Paeds · infectious-diseases
Measles, rubella and congenital rubella
Also known as Measles (rubeola) · Rubella (German measles) · Congenital rubella syndrome · Koplik-spot illness · CRS triad (deafness, cataracts, cardiac)
Fellowship topic on measles, rubella and congenital rubella syndrome: the morbillivirus and rubivirus organisms and their lymphotropic and teratogenic mechanisms; the classic measles prodrome-rash course with Koplik spots and the immune-amnesia aftermath; the mild postnatal rubella illness versus the devastating first-trimester congenital rubella syndrome (deafness, cataracts, cardiac and neurodevelopmental deficit); the differential of febrile-rash illness in a child; IgM/PCR diagnosis timed to the illness; stepwise management of the measles case from vitamin A and supportive care through notification and isolation; prevention through the two-dose MMR schedule, antenatal rubella screening and the herd-immunity threshold above 95 per cent; the special populations (infants, pregnant non-immune women, immunocompromised and under-vaccinated communities); and ANZ/UK/US/Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The measles prodrome — remember the 3 C's
Overview & Definition
Picture a five-year-old brought to the emergency department with four days of fever, a streaming nose, a hacking cough and red, watery eyes, who this morning developed a blotchy red rash behind the ears that is now spreading down the body. The child has never been vaccinated. This is textbook measles, and the decision you make in the next five minutes — isolate, confirm, treat, notify — protects both the child and everyone who shared the waiting room. Recognising it early is what turns a preventable death into a survivable illness. [5] [1]
Measles, or rubeola, is an acute, highly contagious viral infection caused by the measles morbillivirus, a paramyxovirus spread largely by the airborne route. It is one of the most transmissible human pathogens known: a single case in a susceptible population can infect twelve to eighteen others, and the virus lingers in the air of a room for up to two hours after an infectious person has left it. Rubella, or German measles, is caused by the rubella rubivirus and is a far milder illness in children — but its teratogenic effect on the first-trimester fetus makes it one of the most consequential infections in pregnancy. Congenital rubella syndrome (CRS) is the constellation of permanent defects that follows maternal rubella in early pregnancy. [6] [1]
The clinician's work has three faces. The acute face is to recognise the child with measles, support them through the illness, give vitamin A, and prevent spread through isolation and notification. The obstetric face is to confirm or exclude rubella in early pregnancy and counsel honestly about CRS risk. And the population face is to run the immunisation programme — two MMR doses, antenatal screening, postpartum catch-up — because the child who never catches measles and the fetus who never meets rubella are the children the programme has protected. [8] [2]
Classification
Sort these infections the way they present at the bedside — by organism and by who is actually at risk, because the same virus does very different things in different hosts. Measles is one disease with a single classic course. Rubella is really two diseases depending on the host: a trivial illness in a child or adult, and a catastrophic teratogenic infection in the first-trimester fetus. Congenital rubella syndrome is the permanent consequence of that fetal infection. Keeping the host in the classification is what stops a clinician dismissing a rubella-like rash in a pregnant woman as "just German measles". [6] [2]
Measles classifies by its clinical course. After an incubation of eight to twelve days, the prodrome runs three to five days of fever with the 3 C's and Koplik spots — small white lesions on an erythematous buccal mucosa that are the most specific early sign. The rash then appears, a maculopapular eruption starting at the hairline and behind the ears and spreading cephalocaudally, while the fever typically peaks and then falls. Recovery follows over one to two weeks, but the immune-amnesia aftermath means the child remains vulnerable to other infections for years. [5] [3]
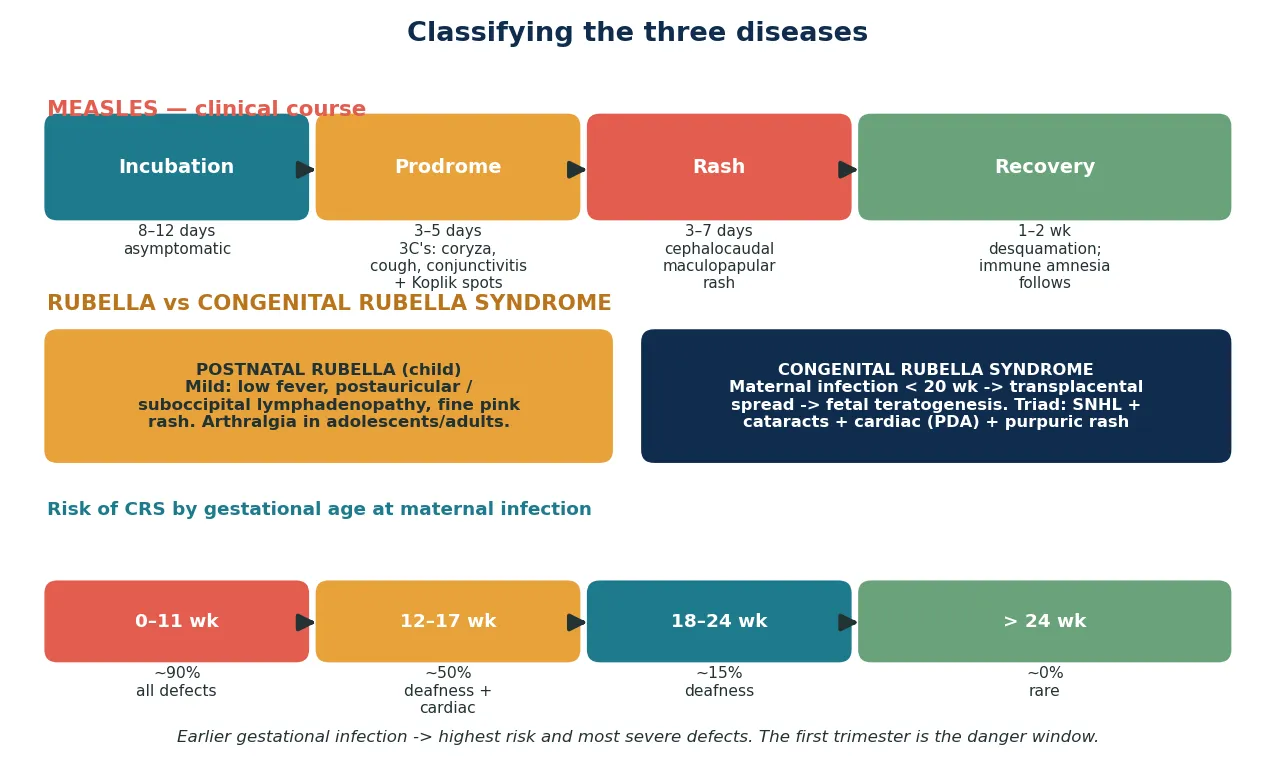
Rubella classifies by the host and, for the fetus, by the gestation. Postnatal rubella in a child or adult is mild. Congenital infection, by contrast, is graded by the timing of maternal infection: the risk of any defect and of multiple defects is highest in the first trimester, falls through the second, and is rare after 20 to 24 weeks. This gestational gradient is the single most important fact in CRS counselling, because it converts a frightening probability into a dated, decision-relevant number. [6] [7]
Epidemiology & Risk Factors
Where do these diseases sit, and who do they hurt? Measles remains endemic in many regions and surges wherever vaccination coverage falls below the herd-immunity threshold. Worldwide progress toward elimination is real but fragile, and outbreaks recur in under-vaccinated pockets even in countries that had interrupted transmission. The burden of severe disease and death falls on young, unvaccinated children and on the malnourished, in whom vitamin A deficiency, pneumonia and blindness compound each other. [1] [5]
The dominant risk factor at the individual level is under-vaccination — whether by parental refusal, missed doses, or access barriers. A child who has received fewer than two documented MMR doses is susceptible, and measles finds these gaps with ruthless efficiency because of its extraordinary transmissibility. Malnutrition, vitamin A deficiency and immunocompromise raise the severity of measles once caught, turning a self-limiting illness into a lethal one. [5] [4]
Rubella and CRS epidemiology follow vaccine coverage in women of childbearing age. Where coverage is high and sustained, CRS becomes rare; where it is patchy, infection can circulate without enough disease in children to warn the community, leaving a cohort of women reaching pregnancy non-immune — the "susceptible pool" that produces CRS. Global progress toward rubella and CRS control continues, but many countries have not yet introduced rubella-containing vaccine, and CRS persists as a preventable cause of deafness, blindness and cardiac disease. [10] [2]
Pathophysiology
Why is measles so contagious, and why does a rash illness cause years of vulnerability to other infections? The answer lies in how the virus uses the immune system itself as its route in. Measles is inhaled in airborne droplets and infects immune cells that express its receptors — CD150 (SLAM) on immune cells and nectin-4 on epithelial cells — so the virus enters through the very cells meant to defend the airway, then spreads systemically through lymphoid tissue. [3] [5]
This lymphotropic spread matters because it sets up the virus's most distinctive and dangerous feature: immune amnesia. Measles infects and depletes memory B and T lymphocytes, erasing the child's hard-won immunological memory of previous infections and vaccinations. Population-level analysis of pre-vaccination-era data showed that measles infection was associated with a long increase in overall childhood infectious-disease mortality lasting two to three years — not because measles itself persisted, but because the child had been immunologically reset. The vaccine prevents this reset; the disease causes it. [3] [5]
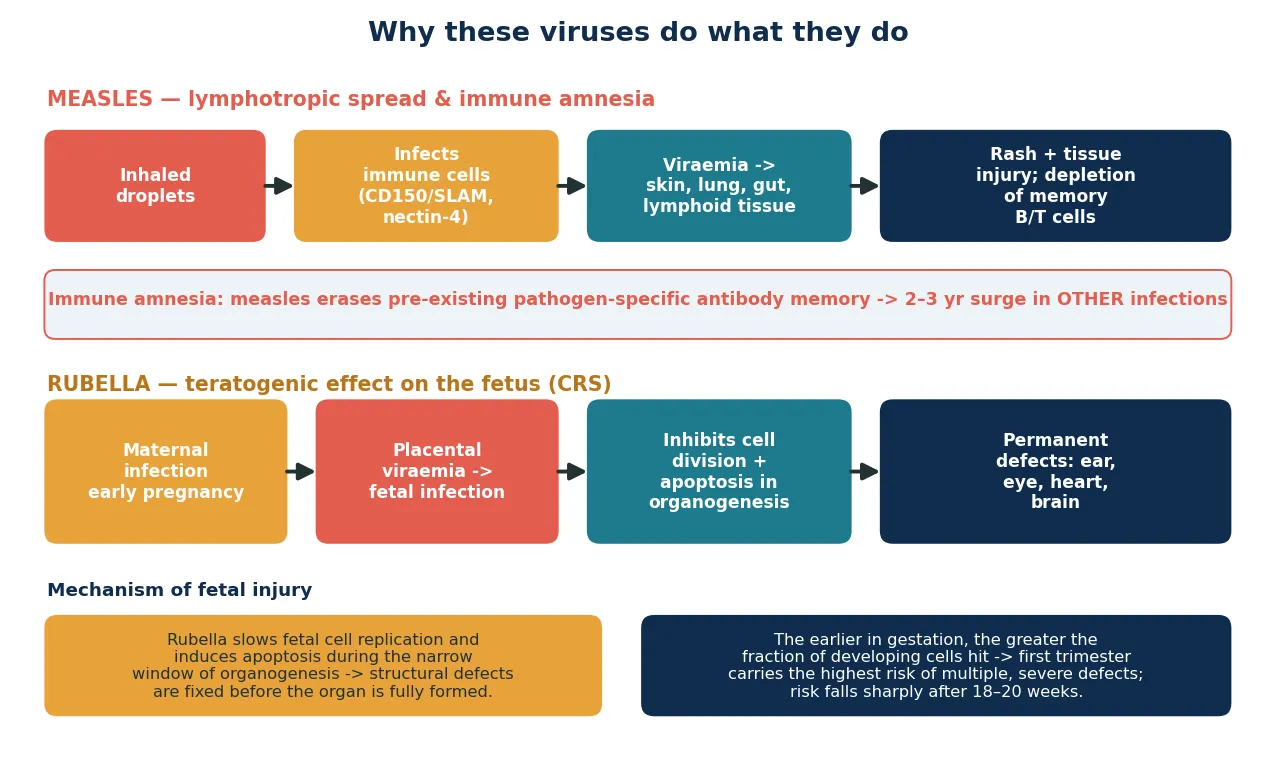
Rubella's mechanism is entirely different and entirely about timing. When a woman catches rubella in early pregnancy, viraemia seeds the placenta and the virus reaches the fetus. The developing fetus has limited capacity to clear the virus, and rubella slows fetal cell division and induces apoptosis precisely during the narrow window of organogenesis — when organs are being built. The earlier in gestation this happens, the larger the fraction of still-forming cells that are hit, which is why the first trimester carries the highest risk of multiple, severe defects. The structural damage is fixed before the organ finishes forming. [7] [6]
The persistence of the rubella virus in fetal tissue also explains some late features of CRS, including late-onset endocrine disease (diabetes) and progressive rubella panencephalopathy, mirroring the way measles can persist in the brain to cause subacute sclerosing panencephalitis years after the original infection. Both viruses can establish persistence; the clinical lesson is that CRS is not a single event but a lifelong condition, and the child needs long-term surveillance. [6] [12]
Clinical Presentation
The classic measles presentation is unmistakable once you have seen it, and the examiner rewards the registrar who can describe it in order. After the incubation, the prodrome is dominated by fever and the 3 C's — cough, coryza and conjunctivitis — with the child looking miserable and photophobic. Koplik spots appear on the buccal mucosa in the prodrome: small, white, grain-like lesions on an erythematous base, and they are the single most specific sign that the rash about to appear is measles. [5] [1]
The measles rash then erupts at the hairline and behind the ears, spreads down the face, trunk and limbs over two to three days, and classically becomes confluent on the upper body. The fever peaks as the rash appears and then falls as the rash fades, leaving a fine desquamation. Crucially, the child is most infectious in the prodrome, before the rash makes the diagnosis obvious — which is why waiting for the rash to isolate the child is waiting too long. [5] [1]
The complications are part of the presentation because they often bring the child to care. Pneumonia is the commonest cause of measles death, whether viral (giant-cell pneumonia) or secondary bacterial. Croup and stridor, otitis media, diarrhoea and dehydration, keratoconjunctivitis with corneal ulceration (especially with vitamin A deficiency), and acute encephalitis are the acute threats. Weeks to years later, subacute sclerosing panencephalitis — a progressive, fatal degenerative brain disease — can follow measles, with recent surveillance showing a surge of early, fulminant cases where measles has re-emerged. [5] [12]
Postnatal rubella in a child is deliberately undramatic: a brief low-grade fever, tender postauricular and suboccipital lymphadenopathy, and a fine pink maculopapular rash that spreads from the face downward and fades in days. Arthralgia is common in adolescent and adult women. The illness is so mild that the real clinical task is not managing the child but identifying the pregnant contact and acting on her. [6] [7]
Congenital rubella syndrome presents in the newborn and infant through its defects. The classic triad is sensorineural deafness (the commonest single defect), eye disease (cataracts, congenital glaucoma, pigmentary retinopathy) and cardiac disease (patent ductus arteriosus, pulmonary artery stenosis). Add the transient "blueberry-muffin" purpura of dermal extramedullary haematopoiesis, hepatosplenomegaly, thrombocytopenia, microcephaly, developmental delay and later-onset diabetes, and the picture of multi-system fetal injury is complete. A review of CRS experience found that hearing loss is often the most disabling and most easily missed defect at birth, making universal newborn hearing screening essential. [11] [6]
Differential Diagnosis
For the child with a febrile rash illness, the differential is broad and the discriminator is the pattern and tempo of the rash with the accompanying features. Measles is distinguished by the prodrome of the 3 C's, Koplik spots, and a cephalocaudal maculopapular rash with the child appearing unwell and febrile. The common mimics include enteroviral and adenoviral exanthems, roseola infantum (high fever that defervesces before the rash appears), scarlet fever (a fine sandpaper rash with a strawberry tongue and palatal petechiae), Kawasaki disease (prolonged fever, conjunctival injection, strawberry tongue, extremity changes), drug eruption, dengue and other travel-related exanthems, and — where the child is unvaccinated — rubella itself. [5] [1]
[5] [1]For the pregnant woman with a rubella-like rash, the differential includes parvovirus B19, enteroviruses, measles itself, drug eruption and even a mild allergic reaction — but the operational rule is that any rubella-like illness or contact in pregnancy must be serologically confirmed or excluded, because the cost of missing true rubella in the first trimester is catastrophic and irreversible. Never reassure a pregnant woman on clinical grounds alone. [6] [7]
For the newborn with multiple congenital anomalies suggesting CRS, the differential is the broader TORCH group — cytomegalovirus (the commonest congenital infection, often with petechiae, sensorineural hearing loss and calcifications), toxoplasmosis (intracranial calcifications, chorioretinitis), syphilis, and enteroviral infection — distinguished by the specific pattern of defects (cataracts and PDA strongly favour CRS), maternal serology and the neonatal PCR/IgM profile. [7] [6]
Clinical & Bedside Assessment
The assessment of the suspected measles case begins with a focused history built around the rash and its setting. Establish the onset of fever relative to the rash, the presence of the 3 C's, any Koplik spots, vaccination history (number and dates of MMR doses), and potential exposures — travel, unvaccinated communities, known outbreaks or contacts in the seven-to-eighteen-day window. In the examination, look specifically at the buccal mucosa for Koplik spots, the conjunctivae, and the rash's distribution and character, and screen for complications: respiratory distress or stridor suggesting pneumonia or croup, dehydration, otoscopic signs, and any change in conscious state suggesting encephalitis. [5] [1]
Document the public-health essentials at the bedside because they drive the response. Record the date of symptom onset and of rash onset, calculate the infectious period (from prodrome to four days after the rash), note school, childcare and healthcare exposures, and begin the contact list — paying particular attention to pregnant women, infants and immunocompromised contacts. These details determine notification, exclusion, and who needs post-exposure prophylaxis. A careful contact list at the first encounter prevents the late, disorganised public-health scramble. [1] [8]
For the pregnant woman with a possible rubella exposure or rash, the bedside assessment is precise and time-critical. Establish the gestational age exactly, the date and nature of the exposure or illness, and the documented antenatal rubella serology. Confirm immune status from the booking bloods: a documented rubella IgG-positive result means she is immune; an equivocal, negative, or unknown result demands urgent serology now. Never defer this — the window for confirmatory testing and counselling is narrow, and the consequence of delay is an irreversible fetal injury. [6] [7]
For the infant with suspected CRS, examine systematically for the defect pattern: ophthalmology for cataracts, congenital glaucoma and pigmentary retinopathy; cardiology for a murmur of PDA or pulmonary stenosis; audiology, recognising that sensorineural hearing loss may be the only or the most disabling defect; and a developmental and neurological assessment. A coordinated multi-disciplinary evaluation defines the burden of injury and sets the surveillance plan. [11] [6]
Investigations
Diagnosis of measles and rubella rests on serology and PCR timed to the illness. For measles, the recommended approach is measles-specific IgM on a single serum sample taken at first contact (it is positive in most cases from the first day of the rash) together with RT-PCR and virus genotyping on a throat or nasopharyngeal swab and urine, ideally within the first few days of the rash. PCR is particularly useful early, when IgM may still be negative, and genotype results support outbreak tracing. Paired sera showing a rise in IgG can confirm a late or atypical case. [1] [8]
For rubella, diagnosis in a child or adult follows the same logic: rubella-specific IgM on an acute serum, with PCR confirming where needed. In pregnancy, the approach is staged and urgent. Confirm the booking serology; if susceptibility is confirmed or status unknown, take an acute serum for IgM and IgG immediately, and arrange repeat serology at the appropriate interval if the first is negative but exposure was recent. PCR on amniotic fluid, performed by the fetal-medicine team after the relevant gestational age, can confirm fetal infection when maternal serology is positive. The principle is that maternal infection must be laboratory-confirmed before life-altering counselling or decisions are made. [6] [7]
In Australia and Aotearoa New Zealand, measles and rubella are nationally notifiable diseases, and suspected measles is notified on clinical suspicion — do not wait for confirmation. PCR and IgM are available through public-health laboratories, with genotyping for outbreak linkage. The Australian Immunisation Handbook (ATAGI) and the New Zealand Immunisation Schedule set the two-dose MMR programme and the public-health response, including post-exposure prophylaxis. [1]
Supportive tests round out the workup as the clinical picture demands. A full blood count in measles often shows a lymphopenia consistent with the viral and immunosuppressive nature of the illness. A chest X-ray is indicated when pneumonia is suspected. For the CRS infant, send neonatal rubella IgM (which does not cross the placenta, so it confirms congenital infection), throat or urine PCR, a full blood count for thrombocytopenia, and arrange the ophthalmology, cardiology and audiology evaluations. Imaging and developmental assessment follow the clinical burden. [11] [6]
Management — Resuscitation
Resuscitation in measles is about the child with complications. The red flags are respiratory distress, stridor, hypoxia, dehydration, a change in conscious state and corneal ulceration. A child with any of these needs admission, supplemental oxygen, fluid and electrolyte support, and a low threshold for intensive care if the work of breathing is escalating. Most measles deaths are from pneumonia and its consequences, so the deteriorating respiratory status is the trigger to escalate. [5] [4]
Supportive care is the mainstay. Maintain hydration and nutrition — measles suppresses appetite and worsens with dehydration and malnutrition — give antipyretics for comfort, treat secondary bacterial infection with antibiotics when present, and protect the eyes, recognising that corneal ulceration and blindness are strongly associated with vitamin A deficiency. The child with measles is a child who needs feeding and fluid support as deliberately as a child with any severe infection. [4] [5]
Give vitamin A to every child with measles. A randomised controlled trial in children with severe measles showed that vitamin A reduced mortality and complications, and the Cochrane review of vitamin A for treating measles confirmed that it reduces measles-related morbidity and mortality. Give two doses of vitamin A twenty-four hours apart (age-appropriate doses), because this single, cheap, safe intervention changes outcomes in the children most at risk — the young, malnourished and vitamin A deficient. [4] [9]
Isolate the case from the moment measles is suspected. Measles is airborne and extraordinarily contagious, so the child needs airborne precautions (negative-pressure where available) and a surgical mask on anyone moving them, and contacts in the waiting room must be identified and managed. Isolation in the community and exclusion from school or childcare runs from the prodrome until four days after the rash appears. Notifying public health on suspicion triggers the contact-tracing and post-exposure prophylaxis response. [1] [8]
Management — Definitive & Stepwise
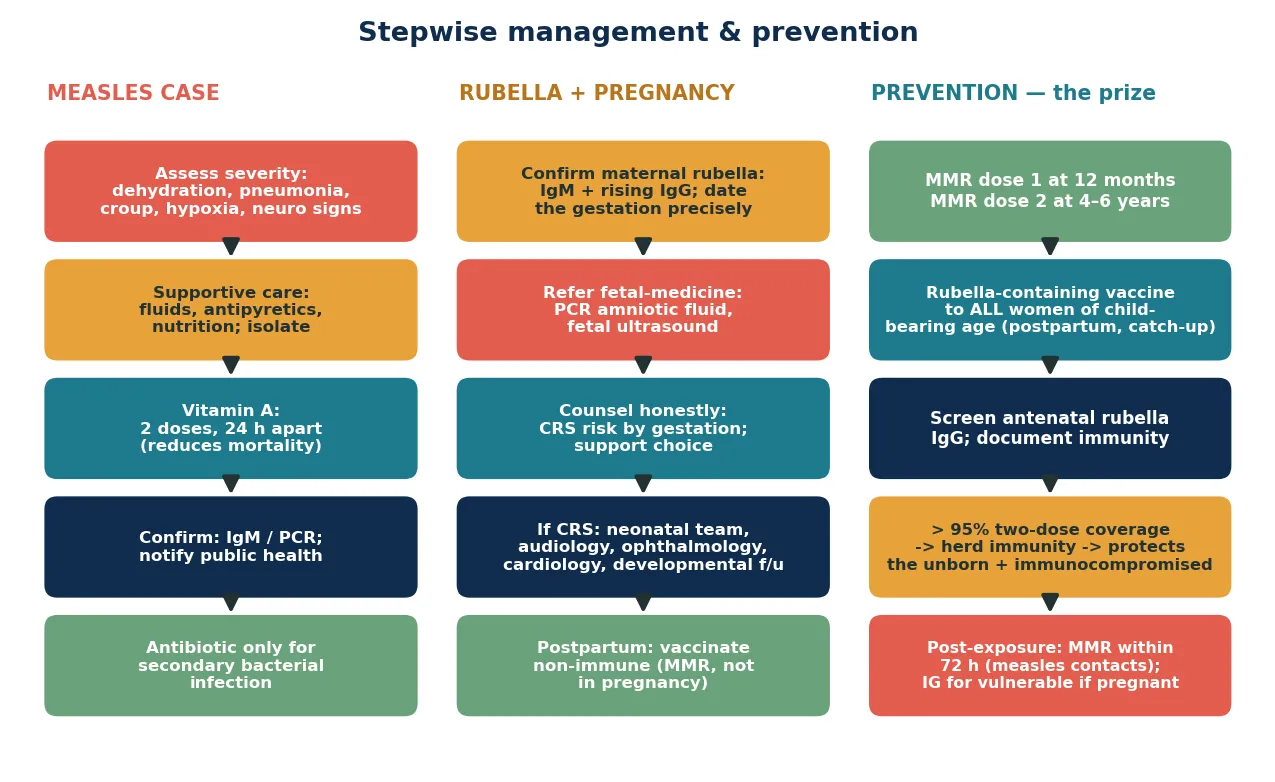
Definitive management is a stepwise pathway matched to the disease and the host: supportive care, vitamin A and isolation for the measles case; urgent confirmation and honest counselling for rubella in pregnancy; and a coordinated, lifelong surveillance plan for the child with CRS. At the population end, the programme — two-dose MMR, antenatal screening, postpartum catch-up and the herd-immunity threshold — does the work that no individual encounter can. [1] [8]
The stepwise measles pathway
Assess severity: airway, breathing, hydration, neurological status and eyes; admit any child with respiratory distress, dehydration, stridor, encephalitis or corneal ulceration.
Give vitamin A in two age-appropriate doses 24 hours apart — the single intervention proven to reduce measles mortality.
Provide supportive care: fluids, antipyretics, nutrition; treat secondary bacterial pneumonia or otitis media with antibiotics when present.
Confirm the diagnosis: measles IgM plus RT-PCR on throat/nasopharyngeal swab and urine, with genotyping for outbreak linkage.
Isolate with airborne precautions and exclude from school or childcare until four days after the rash onset; notify public health on suspicion.
Trace contacts; offer post-exposure MMR within 72 hours to susceptible contacts, and immunoglobulin to high-risk contacts (pregnant, immunocompromised, infants) per protocol.
For rubella in pregnancy, the stepwise pathway is one of confirmation, counselling and choice. Confirm maternal infection with serology; date the gestation precisely; involve fetal medicine for amniotic-fluid PCR where appropriate; and counsel the woman honestly about the gestation-specific CRS risk, supporting her decision within the medicolegal framework of her jurisdiction. The CRS risk falls sharply with gestational age, so the single number she needs is the risk attached to her gestation. Vaccinate non-immune women postpartum, because MMR is contraindicated in pregnancy but the next pregnancy needs to be protected. [6] [7]
For the child with CRS, management is multidisciplinary and lifelong. Neonatal team support in the acute phase; early ophthalmology for cataract surgery; cardiology for the PDA or pulmonary stenosis; audiology with hearing aids or cochlear implantation for the sensorineural loss; and developmental, educational and endocrine surveillance, including screening for later-onset diabetes. The principle is that CRS is not a single insult but a chronic multi-system condition, and the child needs a coordinated team and a long-term plan. [11] [6]
Specific Subtypes & Scenarios
A febrile, unvaccinated child with a cephalocaudal rash and Koplik spots. This is classic measles. Isolate on suspicion, confirm with IgM and PCR, give vitamin A, provide supportive care, and notify public health. Screen for pneumonia, croup, dehydration and encephalitis, and admit any child with complications or risk factors for severe disease. The contact tracing begins at the bedside. [5] [1]
A pregnant woman with a rubella-like rash in the first trimester. This is the encounter where speed and precision determine the fetal outcome. Confirm the gestation, check the booking serology, send urgent IgM and IgG, and refer to fetal medicine for confirmation and counselling. Do not reassure on clinical grounds — the stakes are irreversible. Vaccinate her postpartum if she proves non-immune. [6] [7]
A newborn with purpura, a heart murmur and cloudy corneae. This is congenital rubella syndrome until proven otherwise, and it signals maternal infection earlier in the pregnancy. Confirm with neonatal rubella IgM and PCR, mobilise ophthalmology, cardiology and audiology, and establish the long-term developmental plan. Ask the question the presenting sign demands: which other defects coexist? [11] [6]
An adolescent or adult with a prolonged cough after measles. This may represent the immune-amnesia aftermath — a susceptibility to other respiratory infections for months to years after the measles itself has resolved. The clinical task is to investigate and treat the intercurrent illness while recognising its immunological root, and to ensure the household is fully vaccinated. [3] [5]
A child with progressive myoclonus and cognitive decline years after measles. Consider subacute sclerosing panencephalitis, a fatal degenerative consequence of persistent measles virus in the brain. Recent surveillance shows a surge of early, fulminant cases where measles has re-emerged, so a previously measles-infected child with neurological deterioration needs urgent assessment. SSPE is the long shadow of measles — and another reason to prevent it. [12] [5]
An outbreak in an under-vaccinated community or school. Coordinate with public health, offer MMR to susceptible contacts within 72 hours of exposure, exclude cases, and run catch-up vaccination to lift coverage above the herd-immunity threshold. Outbreaks are the visible cost of under-vaccination; the infants and the unborn at the edge of the outbreak are the ones who pay it. [1] [8]
Complications & Pitfalls
Pneumonia is the commonest severe complication of measles and the leading cause of measles death in children — whether giant-cell viral pneumonia or secondary bacterial. Croup with stridor, otitis media, diarrhoea and dehydration, keratoconjunctivitis progressing to corneal ulceration and blindness (especially with vitamin A deficiency), and acute encephalitis are the acute threats, while subacute sclerosing panencephalitis looms years later. Recognising and treating pneumonia early, and giving vitamin A, are two of the few interventions that genuinely change the measles outcome. [5] [4]
The central diagnostic pitfall is waiting for the rash to make the diagnosis. Koplik spots and the 3 C's in the prodrome are measles until proven otherwise, and the child is most infectious precisely in this pre-rash window — so a clinician who waits for the rash to isolate has already allowed transmission. The rule that protects against this error is to suspect, isolate and notify on the prodrome. [5] [1]
A second pitfall is forgetting vitamin A. It is cheap, safe, and proven to reduce measles mortality and morbidity, and omitting it from the management bundle is an avoidable error in the children who need it most — the young, the malnourished, and the vitamin A deficient. Give it to every child with measles, in two age-appropriate doses twenty-four hours apart. [4] [9]
A third pitfall is reassuring a pregnant woman with a rubella-like rash on clinical grounds. Postnatal rubella is mild and non-specific, and the cost of missing true first-trimester rubella is irreversible fetal injury. Every rubella-like illness or exposure in pregnancy must be laboratory-confirmed, and the gestational CRS risk must be stated explicitly before any decision is made. [6] [7]
The fourth pitfall is treating CRS as a single event rather than a lifelong condition. The defects are permanent, hearing loss may declare itself late, and endocrine disease such as diabetes can appear years later. Discharging the CRS infant without a long-term surveillance plan abandons the child to the late consequences of the infection. [11] [6]
The final pitfall is vaccine complacency. Because measles is so contagious, coverage must be very high — above 95 per cent with two doses — to sustain herd immunity, and even small dips produce outbreaks. Dismissing the possibility of measles in an under-vaccinated child, or of CRS in a community with patchy coverage, closes the door on the diagnosis at the very moment the epidemiology makes it most likely. [1] [8]
Prognosis & Disposition
Most well-nourished, vaccinated-era children recover fully from measles, but the disease carries a real mortality in the young, the malnourished and the immunocompromised, most often through pneumonia, encephalitis or dehydration. Vitamin A, supportive care and early treatment of complications change this prognosis, and the disposition follows severity: admit the child with respiratory distress, dehydration, neurological compromise or risk factors for severe disease; manage the uncomplicated case at home with isolation and clear safety-netting. [5] [4]
The immune-amnesia aftermath means the measles survivor remains vulnerable to other infections for two to three years, a prognosis that is invisible at the bedside but visible at the population level. The family should be counselled that the child's immunity to other illnesses may be impaired, and vigilance for intercurrent infection is warranted for months to years. [3] [5]
For CRS, the prognosis is governed by the burden of defects. Sensorineural hearing loss is the commonest and most disabling single defect; cardiac disease is treatable; cataract surgery restores vision where the eye is structurally salvageable; and developmental outcome depends on the neurological injury. Lifelong surveillance — including endocrine screening for diabetes — is part of the prognosis, because CRS is a chronic condition. [11] [6]
At discharge from the measles encounter, complete the isolation and exclusion period, finish the contact tracing and prophylaxis, reinforce catch-up vaccination for the family, and give the family a clear safety-net for return — worsening respiratory distress, dehydration, neurological change or eye symptoms. The discharge encounter is also a prevention opportunity: vaccinate the susceptible household to close the gap that allowed the case. [1] [8]
Special Populations
Infants under twelve months are too young to have completed their MMR series and are among the most vulnerable to severe measles; they rely on herd immunity, maternal antibody, and — after exposure — post-exposure prophylaxis with immunoglobulin under protocol. Protecting them is the population point of high coverage. [1] [8]
Pregnant women with no documented rubella immunity are the population CRS prevention targets. Screen every pregnancy for rubella IgG at booking, vaccinate non-immune women postpartum (MMR is live and contraindicated in pregnancy), and confirm any rubella-like illness or exposure in pregnancy serologically. The unborn child is protected by the mother's immunity and by the community's coverage. [6] [8]
Immunocompromised children cannot receive live vaccines and depend on the immunity of those around them; measles in this group can be severe or fatal, and immunoglobulin prophylaxis after exposure is indicated under protocol. Their protection is a population responsibility. [1] [8]
Unvaccinated or under-vaccinated children and communities carry the burden of measles outbreaks and the CRS that follows patchy rubella coverage. Address vaccine hesitancy respectfully, offer catch-up vaccination at every opportunity, and recognise that under-immunised pockets are where both diseases resurge most violently. [5] [1]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families may face barriers to timely immunisation and care. Ensure culturally safe, equitable access to vaccination, treat measles actively when suspected, and use trained interpreters rather than family members. Disadvantage should never be the reason a case is delayed or a woman reaches pregnancy non-immune. [1] [10]
Rural and remote children and women need timely access to diagnosis, treatment and public-health follow-up through outreach and telehealth, because distance can delay the care a sick child or a pregnant contact cannot afford to wait for. The plan for a remote family accounts for what is locally available and mobilises retrieval early when needed. [1] [8]
Evidence, Guidelines & Regional Differences
The global standard for measles and rubella vaccination is the WHO position papers, which set the two-dose schedule, the herd-immunity principle and the elimination goals. The ACIP (CDC) summary recommendations consolidate the measles, rubella, CRS and mumps prevention guidance into one operational reference, and these documents anchor national programmes worldwide. [1] [2]
The immune-amnesia evidence transformed the understanding of measles. Population-level analysis of pre-vaccination-era data showed that measles infection was associated with a long increase in overall childhood infectious-disease mortality lasting two to three years — not because measles persisted, but because it erased immunological memory. This reframes measles as more than an acute rash illness: it is an immunological reset whose consequences outlast the infection, and it strengthens the case for prevention. [3] [5]
Vitamin A for severe measles
Population: Children hospitalised with severe measles, in randomised controlled trials and a systematic review.
Key finding
Vitamin A given in two doses reduced measles mortality and morbidity, including pneumonia and hospital stay; the Cochrane review confirmed a reduction in measles-related deaths.
Practice change
Give vitamin A to every child with measles, in two age-appropriate doses 24 hours apart — a cheap, safe, proven intervention.
The CRS prevention evidence is the coverage argument. Global surveillance of rubella and CRS control shows that where rubella-containing vaccine coverage is high and sustained, CRS becomes rare, but where coverage is patchy, a susceptible pool of non-immune women sustains CRS. Reviews of CRS clinical experience, such as the Vietnam series, confirm that hearing loss is the commonest and most disabling defect, anchoring the case for universal newborn hearing screening alongside high-coverage vaccination. [10] [11]
The regional policy structure is consistent in principle and varies in detail. In ANZ, measles and rubella are nationally notifiable, the Australian Immunisation Handbook (ATAGI) and the New Zealand Immunisation Schedule set the two-dose MMR programme and the antenatal rubella-screening requirement, and public-health units coordinate notification and post-exposure prophylaxis. In the UK, NHS and UKHSA guidance and the Green Book direct the programme, including the MMR catch-up campaigns that follow outbreaks. In the US, the ACIP/CDC schedule and surveillance deliver the equivalent strategy, with measles elimination declared but periodically challenged by imported cases in under-vaccinated pockets. In Canada, the Canadian Immunization Guide and provincial programmes deliver the same. In every region the principle is the same: two MMR doses, antenatal screening, postpartum catch-up, and coverage above 95 per cent. [1] [8]
The controversies and active issues are real: sustaining the high coverage that herd immunity demands in the face of hesitancy and access barriers; the timing and reach of post-exposure prophylaxis; whether to pursue regional elimination versus global control; and the inequities that leave some communities and women non-immune. The defence against each is the same: high two-dose coverage, antenatal screening, prompt treatment and notification, and a public-health layer that does not stop at the bedside. [1] [3]
Exam Pearls
- Measles is the most contagious infection in medicine (twelve to eighteen secondary cases per case); herd immunity needs two-dose coverage above 95 per cent. [1]
- The measles prodrome is the 3 C's — cough, coryza, conjunctivitis — plus Koplik spots on the buccal mucosa; the rash then spreads cephalocaudally, and the child is most infectious before the rash. [5]
- Immune amnesia — measles erases pathogen-specific immune memory, driving a two-to-three-year surge in other infections. [3]
- Give vitamin A — two doses 24 hours apart — to every child with measles; it reduces mortality. [4]
- Pneumonia is the commonest cause of measles death; SSPE is the late, fatal brain consequence. [5] [12]
- Diagnose with measles IgM plus RT-PCR on throat/nasopharyngeal swab and urine; isolate with airborne precautions and exclude until four days after the rash; notify on suspicion. [1]
- Rubella is trivial in a child but teratogenic before 20 weeks: sensorineural deafness + cataracts + PDA is the CRS triad; risk is ~90 per cent in the first trimester, falling toward zero after 24 weeks. [6]
- Screen every pregnancy for rubella IgG; vaccinate non-immune women postpartum (MMR is live — contraindicated in pregnancy). [8]
- Never reassure a pregnant woman with a rubella-like rash on clinical grounds — confirm serologically. [6]
- Post-exposure: offer MMR within 72 hours to susceptible measles contacts; immunoglobulin for high-risk contacts (pregnant, immunocompromised, infants). [8]
References
- [1]WHO Measles vaccines: WHO position paper. Wkly Epidemiol Rec, 2009.PMID 19714924
- [2]WHO Rubella vaccines: WHO position paper. Wkly Epidemiol Rec, 2011.PMID 21766537
- [3]Mina MJ; Metcalf CJE; de Swart RL; Osterhaus ADME; Grenfell BT Long-term measles-induced immunodulation increases overall childhood infectious disease mortality. Science, 2015.PMID 25954009
- [4]Hussey GD; Klein M A randomized, controlled trial of vitamin A in children with severe measles. N Engl J Med, 1990.PMID 2194128
- [5]Perry RT; Halsey NA The clinical significance of measles: a review. J Infect Dis, 2004.PMID 15106083
- [6]Banatvala JE; Brown DWG Rubella. Lancet, 2004.PMID 15064032
- [7]Best JM Rubella. Semin Fetal Neonatal Med, 2007.PMID 17337363
- [8]McLean HQ; Fiebelkorn AP; Tempte JL; Wallace GS Prevention of measles, rubella, congenital rubella syndrome, and mumps, 2013: summary recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep, 2013.PMID 23760231
- [9]Huiming Y; Chaomin W; Mei M Vitamin A for treating measles in children. Cochrane Database Syst Rev, 2005.PMID 16235283
- [10]Zimmerman LA; Stanley CP; Goswami ND; Reef SE Progress Toward Rubella and Congenital Rubella Syndrome Control and Elimination — Worldwide, 2012-2020. MMWR Morb Mortal Wkly Rep, 2022.PMID 35143468
- [11]Toizumi M; Motomura H; Dinh Sy T; Takahashi K; et al Clinical manifestations of congenital rubella syndrome: A review of our experience in Vietnam. Vaccine, 2019.PMID 30503658
- [12]Lam T; Lillie J; Orr D; Stodden R; et al A recent surge of fulminant and early onset subacute sclerosing panencephalitis (SSPE) in the United Kingdom: An emergence in a time of measles re-emergence. Eur J Paediatr Neurol, 2021.PMID 34388650