Paeds · infectious-diseases
Meningitis and encephalitis
Also known as Bacterial meningitis · Viral meningitis · Aseptic meningitis · Herpes simplex encephalitis · Acute meningoencephalitis
Fellowship guide to paediatric meningitis and encephalitis: bacterial versus viral patterns, age-specific pathogens, the time-critical assessment of the febrile child with headache or altered consciousness, lumbar puncture and CSF interpretation, empiric antibiotic and aciclovir selection with doses, dexamethasone and steroid controversies, complications including hearing loss, and neurodevelopmental outcomes.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Meningitis is inflammation of the meninges, the membranes lining the brain and spinal cord, and encephalitis is inflammation of the brain parenchyma itself. The two overlap as meningoencephalitis when both are involved, and the distinction drives both prognosis and treatment. In children these are time-critical diagnoses: a febrile infant or child with headache, neck stiffness, or altered consciousness must be presumed to harbour a central nervous system infection until proven otherwise. [3]
The clinician's first job is to separate bacterial meningitis, which carries a mortality of 5 to 10 per cent even with treatment and leaves up to a third of survivors with permanent disability, from viral meningitis, which is usually self-limiting. Herpes simplex encephalitis occupies a special place because it is the most common cause of severe sporadic viral encephalitis, it is treatable with aciclovir, and it is missed easily when doctors assume a febrile drowsy child simply has a viral illness. [6]
The cardinal principle is that antibiotics and, when appropriate, aciclovir must be given early. Every hour of delay in starting antibiotics in bacterial meningitis is associated with a measurable rise in mortality and morbidity, so investigations including lumbar puncture must never delay the first dose. Cultures guide later narrowing of therapy, but they do not gate the decision to treat. [2]
Classification
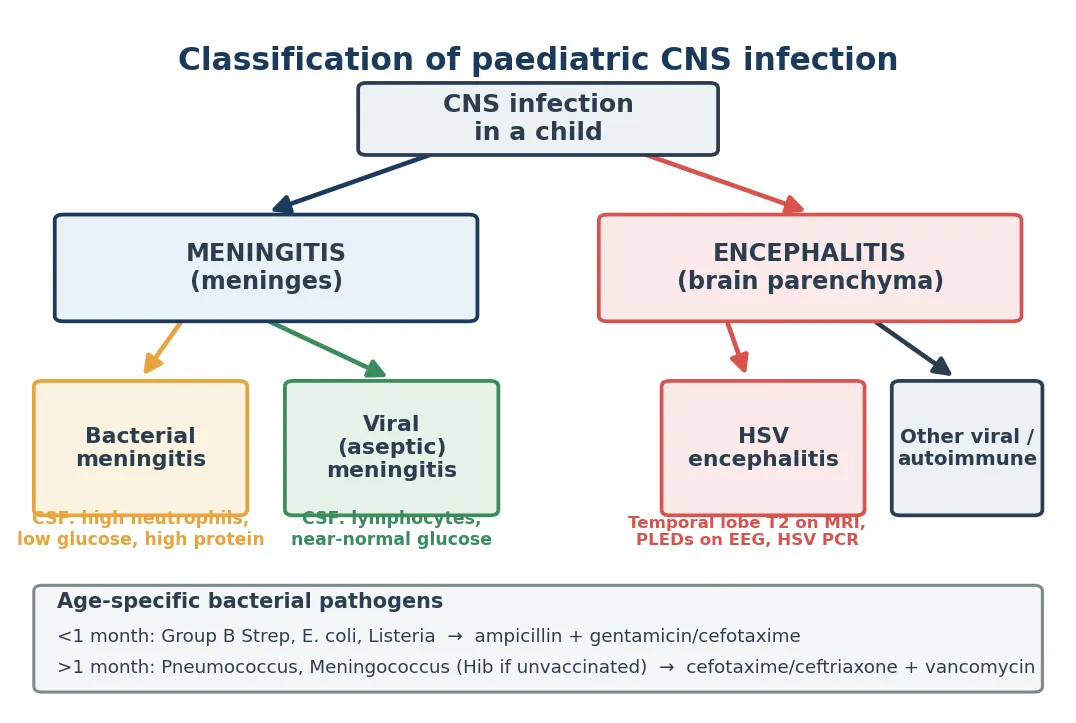
The classification of central nervous system infection turns on two axes: the anatomical site, which separates meningitis from encephalitis, and the organism class, which separates bacterial from viral and the less common fungal and parasitic causes. Bacterial meningitis produces a neutrophilic pleocytosis with low glucose and high protein in the cerebrospinal fluid. Viral meningitis and encephalitis produce a lymphocytic pleocytosis with near-normal glucose, though early viral CSF can show neutrophils. [1]
[1]Age refines the likely pathogen in bacterial meningitis. In neonates under one month, group B Streptococcus, Escherichia coli, and Listeria monocytogenes dominate. In older infants and children beyond the neonatal period, Neisseria meningitidis and Streptococcus pneumoniae are the chief organisms, with Haemophilus influenzae type b now rare in vaccinated populations. Knowing the age-specific pathogen profile determines the empiric antibiotic regimen. [3]
Epidemiology & Risk Factors
The introduction of conjugate vaccines against Haemophilus influenzae type b, pneumococcus, and meningococcus has transformed the epidemiology of bacterial meningitis in children. Where these vaccines are used routinely, the incidence of bacterial meningitis has fallen dramatically, and pneumococcus and meningococcus have become the dominant residual causes in older infants and children. In settings without universal vaccination, Haemophilus influenzae type b remains a major cause of childhood meningitis. [1]
The overall incidence of bacterial meningitis in high-income countries is now roughly 1 to 2 per 100,000 children per year, a fraction of its pre-vaccine level. Despite this decline, bacterial meningitis remains a leading cause of death and permanent neurodisability in children worldwide, and survivors face substantial rates of hearing loss, epilepsy, cognitive impairment, and developmental delay. [2]
The dominant risk factors are young age, incomplete or absent vaccination, immunocompromise, cochlear implants and other central nervous system hardware, basilar skull fractures with cerebrospinal fluid leak, and asplenia or functional hyposplenism. Children with complement deficiency or those receiving eculizumab carry a markedly elevated risk of meningococcal disease. Socioeconomic disadvantage, overcrowded housing, and late presentation amplify risk and worsen outcomes, particularly in Indigenous and remote communities. [12]
Pathophysiology
Most bacteria reach the meninges by haematogenous spread, crossing the blood-brain barrier at the choroid plexus or cerebral capillaries after colonising the nasopharynx. A smaller proportion reach the central nervous system by direct extension from a contiguous focus such as sinusitis, mastoiditis, or a basilar skull fracture with cerebrospinal fluid leak. Once in the subarachnoid space, organisms multiply rapidly because cerebrospinal fluid has low levels of complement and immunoglobulin. [11]
The bacterial cell wall components, particularly pneumococcal teichoic and peptidoglycan, trigger a brisk inflammatory cascade in the subarachnoid space. Tumour necrosis factor, interleukin-1, and interleukin-6 recruit neutrophils, increase blood-brain barrier permeability, and produce the protein-rich exudate that fills the subarachnoid space. This inflammation underlies the characteristic cerebrospinal fluid findings of neutrophilia, low glucose, and raised protein. [11]
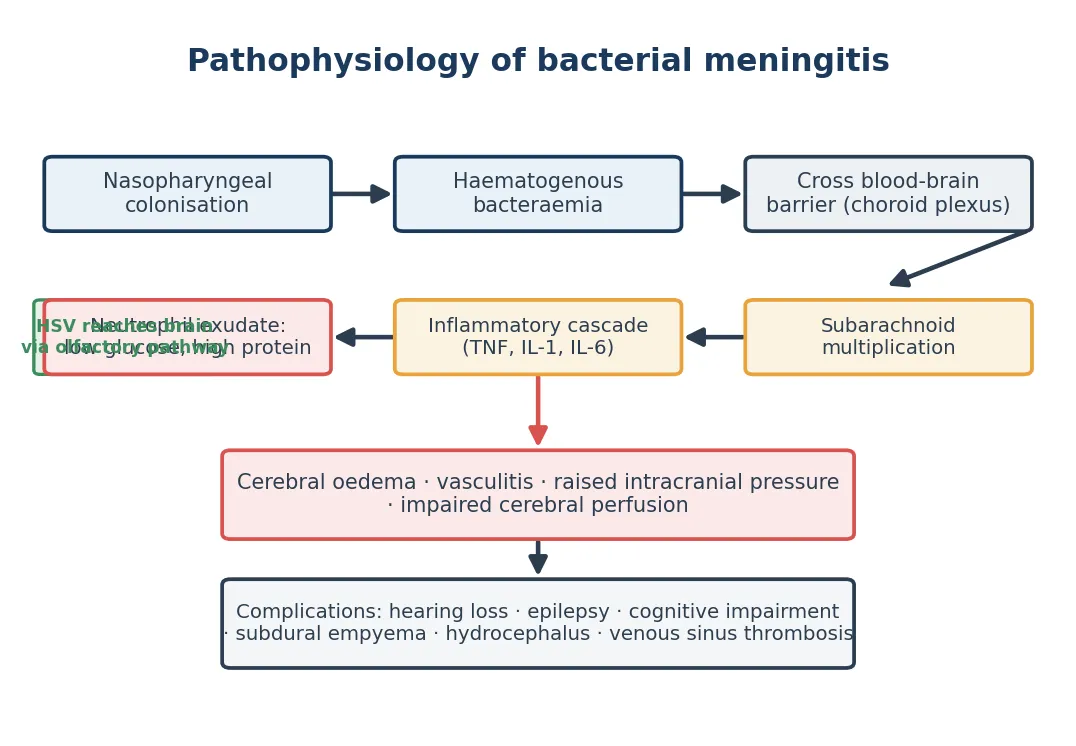
The consequences of this inflammation drive both the clinical features and the complications. Cerebral oedema, vasculitis, and impaired cerebrospinal fluid flow raise intracranial pressure and reduce cerebral perfusion. Cortical vein and dural sinus thrombosis, subdural empyema, and hydrocephalus may follow. In herpes simplex encephalitis, the virus reaches the brain along the olfactory pathway and causes haemorrhagic necrosis with a predilection for the temporal and frontal lobes, producing the characteristic clinical and imaging picture. [6]
Clinical Presentation
The classical triad of bacterial meningitis is fever, headache, and neck stiffness, but the full triad appears in only about half of children, and infants rarely show it. In older children and adolescents the presentation may also include photophobia, nausea and vomiting, altered mental state, and signs of shock with a purpuric rash in meningococcal disease. Neck stiffness on passive flexion is the most useful single sign beyond infancy. [1]
Infants and young children present differently and more subtly. The signs to watch for are fever or hypothermia, irritability, a high-pitched cry, poor feeding, vomiting, lethargy, a tense or bulging fontanelle, and seizures. A bruised, irritable infant who resists handling may have meningitis even without neck stiffness, so the absence of a single sign must never reassure the clinician. [3]
Encephalitis presents with fever alongside altered mental state, behavioural change, seizures, or focal neurological deficits. The red flag that separates encephalitis from uncomplicated viral meningitis is any disturbance of brain function: confusion, drowsiness, dysphasia, hemiparesis, or focal seizures. Herpes simplex encephalitis often presents with fever, altered consciousness, and temporal lobe features such as complex partial seizures or memory disturbance, but in young children the picture is frequently non-specific. [6]
Presenting features by frequency in children
Fever, irritability, or lethargy in any age group
Headache, neck stiffness, and photophobia beyond infancy
Vomiting, poor feeding, and a bulging fontanelle in infants
Altered mental state, confusion, or behavioural change
Focal neurological signs or new seizures suggesting encephalitis
Petechial or purpurial rash and shock in meningococcal disease
Differential Diagnosis
The differential diagnosis for a febrile child with headache, neck stiffness, or altered consciousness is broad, and several non-infectious causes must be excluded alongside infection. The most urgent non-infectious mimic is subarachnoid haemorrhage, which can present with sudden severe headache and neck stiffness, though this is uncommon in children. Intracranial abscess, subdural empyema, and venous sinus thrombosis can mimic meningitis or encephalitis and require imaging. [9]
Septicemia without meningitis, particularly meningococcal septicaemia, may coexist with or masquerade as meningitis, and the priorities of fluid resuscitation and early antibiotics are identical. A simple febrile convulsion can present with fever and a reduced conscious state post-ictally, but any child who does not recover full consciousness within an hour, or who has focal features, must be evaluated for central nervous system infection. [3]
Viral and autoimmune causes dominate the differential of encephalitis. Enteroviruses, parechoviruses, and arboviruses cause seasonal viral encephalitis, while autoimmune encephalitides such as anti-N-methyl-D-aspartate receptor encephalitis present with psychiatric disturbance, movement disorder, and seizures. Migraine, Todd paresis, and metabolic encephalopathy from hypoglycaemia, electrolyte disturbance, or inborn errors of metabolism all enter the differential of the altered febrile child. [7]
Clinical & Bedside Assessment
Begin every assessment with an overall judgement of how sick the child is, using the paediatric assessment triangle of appearance, work of breathing, and circulation. A child who is drowsy, poorly perfused, or in compensated shock needs immediate resuscitation and empiric antibiotics regardless of how long the examination takes. Measure temperature, heart rate, respiratory rate, blood pressure, capillary refill, and oxygen saturation. [2]
Examine specifically for neck stiffness by attempting passive flexion of the neck, and look for the Kernig and Brudzinski signs, which are useful when present but imperfect when absent. Inspect the skin carefully for petechiae and purpura, and apply the glass test: a petechial rash that does not blanch under pressure is meningococcal disease until proven otherwise. Assess for rash, otitis media, upper respiratory infection, and any source of fever that might explain the presentation. [1]
Perform a full neurological examination. Document the Glasgow Coma Scale or a paediatric equivalent, pupil size and reactivity, and any focal deficit. Check the fontanelle in infants. Look specifically for signs of raised intracranial pressure such as a falling conscious level, abnormal posturing, Cushing triad of bradycardia with hypertension and irregular respirations, or papilloedema, because these signs change the urgency and the imaging strategy. [6]
Investigations
Blood culture must be obtained before antibiotics whenever it can be done without delaying treatment, and a full blood count, C-reactive protein, and electrolytes including glucose and sodium are sent at the same time. Hyponatraemia is common in meningitis from syndrome of inappropriate antidiuretic hormone and influences fluid management. Blood gas and lactate help assess perfusion and acid-base status in the unwell child. [2]
Lumbar puncture for cerebrospinal fluid analysis is the definitive investigation when it is safe to perform. Send the fluid for cell count and differential, glucose with a simultaneous blood glucose, protein, Gram stain, culture, and meningococcal and pneumococcal polymerase chain reaction. Hold an extra tube for viral studies including herpes simplex polymerase chain reaction, which is the diagnostic test for herpes simplex encephalitis, though early results can be falsely negative and a repeat sample several days later may be needed. [6]
Neuroimaging before lumbar puncture is required when there are signs of raised intracranial pressure, focal neurological deficits, a reduced or rapidly falling conscious level, new-onset seizures, a bleeding disorder, or skin infection over the puncture site. In these children, start antibiotics and aciclovir first, image urgently, and then perform lumbar puncture if it is safe. A normal computed tomography scan does not exclude raised pressure, so the decision to tap rests on clinical stability. [9]
Management — Resuscitation
A child with suspected meningitis and signs of shock or raised intracranial pressure needs immediate resuscitation using an airway, breathing, circulation approach. Secure the airway and give high-flow oxygen for hypoxia, respiratory distress, or a falling conscious level. Establish intravenous or intraosseous access rapidly and do not spend more than a few minutes hunting for a peripheral line before going to the intraosseous route. [2]
Give a 10 mL per kilogram bolus of isotonic crystalloid, 0.9 per cent sodium chloride, for hypotension or poor perfusion, and reassess the child after each bolus. Repeat boluses to a total of 30 to 60 mL per kilogram may be required in septic shock, titrated to perfusion and blood pressure, while watching for hepatomegaly and rising oxygen need as signs of volume overload. Avoid hypotonic fluids because of the risk of hyponatraemia and cerebral oedema. [2]
Resuscitation sequence for suspected CNS infection
Assess airway, breathing, circulation and give high-flow oxygen
Establish intravenous or intraosseous access within minutes
Draw blood culture, full blood count, CRP, glucose, and electrolytes
Give first dose of empiric antibiotics immediately, before imaging or LP
Start aciclovir if encephalitis or HSV is suspected
Fluid bolus 10 mL/kg 0.9 per cent NaCl for shock, reassess after each
The single most important drug intervention is the first dose of an appropriate antibiotic, given as soon as intravenous access is secured. The choice is guided by age and immune status, and the dose must be meningitis-appropriate because standard doses achieve inadequate cerebrospinal fluid concentrations. If lumbar puncture must be deferred, antibiotics come first, and cultures obtained afterwards still retain value for the first few hours. [3]
Management — Definitive & Stepwise
Empiric antibiotic therapy for bacterial meningitis in a child older than one month is a third-generation cephalosporin, cefotaxime 50 mg per kilogram intravenously 6-hourly or ceftriaxone 50 to 100 mg per kilogram intravenously daily, combined with vancomycin 15 mg per kilogram intravenous loading then 6-hourly to cover penicillin-resistant pneumococcus. Add ampicillin if the child is under three months, immunocompromised, or older than fifty years, to cover Listeria. [3]
For neonates under one month, the empiric regimen is ampicillin plus an aminoglycoside such as gentamicin, or ampicillin plus cefotaxime, because third-generation cephalosporins do not treat Listeria and gentamicin extends Gram-negative cover. Start aciclovir 20 mg per kilogram intravenously 8-hourly for a term neonate whenever herpes simplex encephalitis or disseminated neonatal herpes is suspected, because the cost of missing it is catastrophic and the cost of treating unnecessarily is modest. [3]
Dexamethasone 0.15 mg per kilogram intravenously 6-hourly for four days, given with or just before the first antibiotic dose, reduces hearing loss and neurological sequelae in Haemophilus influenzae type b meningitis, with probable benefit in pneumococcal meningitis. The benefit is lost if steroids are given after antibiotics, so the decision and the dose belong at the front of the management sequence. In children, the evidence that dexamethasone or glycerol reliably relieves hearing impairment remains limited, which is why many units give steroids routinely for suspected bacterial meningitis but counsel families that hearing outcome is still uncertain. [8]
Empiric regimens by age
Once an organism is identified and sensitivities are known, narrow the antibiotic spectrum and confirm an adequate duration. Uncomplicated meningococcal meningitis requires 7 days, pneumococcal meningitis 10 to 14 days, and group B streptococcal or Gram-negative neonatal meningitis at least 14 to 21 days. Herpes simplex encephalitis requires at least 14 to 21 days of intravenous aciclovir, and a repeat lumbar puncture to confirm clearance of viral DNA before stopping is advocated by some centres for the youngest infants. [9]
Specific Subtypes & Scenarios
Meningococcal meningitis and septicaemia present the most dramatic scenario, with rapid progression from fever to purpuric rash and shock within hours. The priorities are immediate parenteral antibiotics, aggressive fluid resuscitation for shock, and early transfer to a paediatric intensive care setting. Prophylaxis of close contacts with rifampicin or ciprofloxacin, and notification to public health, are essential after a confirmed case. [2]
Pneumococcal meningitis carries the highest case fatality and the highest rate of permanent neurological sequelae among the bacterial causes. It can complicate cochlear implants, basilar skull fractures, and asplenia, and it is the pathogen for which vancomycin is added empirically to cover resistant strains. Subdural effusion or empyema and hydrocephalus are recognised complications that may require neurosurgical drainage. [11]
Herpes simplex encephalitis is the archetype of treatable viral encephalitis and the diagnosis examiners test most relentlessly. The presentation in older children is fever with altered consciousness and temporal lobe features, but in infants and young children the picture is often non-specific. Magnetic resonance imaging shows T2 hyperintensity in the temporal and frontal lobes, the electroencephalogram shows periodic lateralised epileptiform discharges, and the cerebrospinal fluid herpes simplex polymerase chain reaction confirms the diagnosis, though early negative results warrant repeat sampling and continued aciclovir. [6]
Enteroviral and parechoviral meningitis are the most common causes of viral meningitis in infants, often presenting with fever and irritability in the summer months. They are generally self-limiting and require supportive care, but parechovirus type 3 in neonates can cause a severe sepsis-like illness with white matter injury. Autoimmune encephalitis, particularly anti-N-methyl-D-aspartate receptor encephalitis, presents with psychiatric symptoms, movement disorder, seizures, and autonomic instability, and requires immunotherapy rather than antivirals. [7]
[12]Complications & Pitfalls
Mortality from bacterial meningitis in treated children is approximately 5 to 10 per cent, and a further 20 to 33 per cent of survivors develop permanent neurological sequelae. Sensorineural hearing loss affects 10 to 30 per cent and may be progressive, mandating audiology assessment early and again before discharge. Epilepsy, cognitive impairment, developmental delay, cerebral palsy, and visual impairment contribute to the long-term burden, and the youngest infants carry the greatest risk. [10]
Acute complications include raised intracranial pressure, cerebral oedema, subdural effusion or empyema, cerebral venous sinus thrombosis, hydrocephalus, and syndrome of inappropriate antidiuretic hormone causing hyponatraemia and seizures. Septic shock and disseminated intravascular coagulation complicate meningococcal disease in particular. Recognising and treating raised intracranial pressure, with head elevation, hypertonic saline or mannitol, and neurosurgical referral when needed, is part of acute care. [11]
The major clinical pitfalls are delaying antibiotics while awaiting tests or transport, deferring lumbar puncture without then returning to complete it, anchoring on a benign viral diagnosis, omitting aciclovir in a child with encephalitis, and underdosing antibiotics with non-meningitis regimens. Failing to arrange audiology follow-up, missing progressive hearing loss, and giving hypotonic fluids that worsen hyponatraemia are additional recurring errors that examiners probe directly. [12]
Prognosis & Disposition
The two determinants of outcome are the speed of starting appropriate antibiotics and the causative organism. Children who receive antibiotics promptly and who recover fully within days generally have an excellent prognosis, though even well children need audiology and developmental surveillance because hearing loss can be delayed. Pneumococcal meningitis and neonatal Gram-negative meningitis carry the worst prognoses, while uncomplicated meningococcal meningitis generally has the best. [10]
After herpes simplex encephalitis, outcome depends on how early aciclovir is started. Children treated promptly may recover fully, but delays are associated with substantial rates of cognitive impairment, epilepsy, and behavioural change. All survivors require structured neuropsychological and developmental follow-up, and many benefit from rehabilitation services. Repeat cerebrospinal fluid polymerase chain reaction to document viral clearance is advocated for the youngest infants before stopping therapy. [6]
Disposition requires confirming that the child is clinically stable, afebrile, and tolerating oral intake, with a clear plan for completing the antibiotic course and follow-up. Every child treated for bacterial meningitis needs an audiology assessment before discharge and developmental surveillance over the following year. Provide families with a written safety-net explaining warning signs and when to re-present, because the consequences of a missed relapse or complication are severe. [12]
Special Populations
Neonates are the highest-risk group for both bacterial meningitis and disseminated herpes simplex infection. Their muted, non-specific signs and their distinct pathogen profile, with group B Streptococcus, E. coli, and Listeria dominating, demand a lower threshold for evaluation and a different empiric regimen. The addition of aciclovir to the neonatal workup whenever herpes is plausible reflects the cost of a missed diagnosis. [3]
Immunocompromised children, including those on chemotherapy, after transplantation, with primary immunodeficiency, or on immunosuppressive biologics, are susceptible to a broader range of organisms including Listeria, cryptococcus, and enteroviruses, and they may present with less inflammation in the cerebrospinal fluid. Empiric regimens must extend to cover these pathogens, and infectious diseases input is essential early. Children with cochlear implants have a markedly elevated risk of pneumococcal meningitis and benefit from vaccination and prompt evaluation of any febrile illness. [9]
In Indigenous and remote communities across Australia and New Zealand, higher rates of invasive bacterial disease, later presentation to health services, and greater distances to tertiary care all contribute to worse outcomes. Culturally safe, family-centred care with interpreter access, clear safety-net advice, and reliable aeromedical retrieval pathways is essential. In migrant and refugee families, incomplete vaccination, exposure to organisms uncommon in the host country, and language barriers all shape both risk and presentation. [12]
[12]Evidence, Guidelines & Regional Differences
The 2017 Infectious Diseases Society of America guidelines for healthcare-associated ventriculitis and meningitis, together with the broader community-acquired disease literature summarised in disease primer and review articles, provide the current framework for diagnosis and treatment. These sources converge on early empiric antibiotics, cerebrospinal fluid analysis when safe, adjuvant dexamethasone for Haemophilus and pneumococcal disease, and aciclovir for suspected herpes simplex encephalitis. [9]
The bacterial meningitis score, derived and validated in large multicentre cohorts, helps distinguish bacterial from aseptic meningitis in children with cerebrospinal fluid pleocytosis. A child with none of the score's high-risk features, namely a positive Gram stain, cerebrospinal fluid protein above 0.8 g per litre, cerebrospinal fluid neutrophils above 1000, blood neutrophils above 10, and a seizure history, is at very low risk of bacterial meningitis and can often be observed without antibiotics. [4]
[4]Controversies persist around whether dexamethasone reliably prevents hearing loss in children, whether routine repeat lumbar puncture is needed in neonatal Gram-negative meningitis, the optimal duration of aciclovir for the youngest infants, and how to balance antibiotic stewardship against the small residual risk in low-risk aseptic meningitis. Rising antimicrobial resistance in pneumococci and enteric Gram-negatives, and the emergence of vaccine-escape strains, keep these questions live. [12]
Exam Pearls
MENINGES red flags
References
- [1]Brouwer MC Epidemiology, diagnosis, and antimicrobial treatment of acute bacterial meningitis. Clin Microbiol Rev, 2010.PMID 20610819
- [2]van de Beek D Community-acquired bacterial meningitis. Nat Rev Dis Primers, 2016.PMID 27808261
- [3]Kim KS Acute bacterial meningitis in infants and children. Lancet Infect Dis, 2010.PMID 20129147
- [4]Nigrovic LE Clinical prediction rule for identifying children with cerebrospinal fluid pleocytosis at very low risk of bacterial meningitis. JAMA, 2007.PMID 17200475
- [5]Nigrovic LE Development and validation of a multivariable predictive model to distinguish bacterial from aseptic meningitis in children in the post-Haemophilus influenzae era. Pediatrics, 2002.PMID 12359784
- [6]Venkatesan A Case definitions, diagnostic algorithms, and priorities in encephalitis: consensus statement of the international encephalitis consortium. Clin Infect Dis, 2013.PMID 23861361
- [7]Glaser CA Beyond viruses: clinical profiles and etiologies associated with encephalitis. Clin Infect Dis, 2006.PMID 17109290
- [8]de Gans J Dexamethasone in adults with bacterial meningitis. N Engl J Med, 2002.PMID 12432041
- [9]Tunkel AR 2017 Infectious Diseases Society of America's Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis. Clin Infect Dis, 2017.PMID 28203777
- [10]Peltola H Hearing impairment in childhood bacterial meningitis is little relieved by dexamethasone or glycerol. Pediatrics, 2010.PMID 20008417
- [11]Mook-Kanamori BB Pathogenesis and pathophysiology of pneumococcal meningitis. Clin Microbiol Rev, 2011.PMID 21734248
- [12]Peltola H Improving the outcomes in children with bacterial meningitis. Curr Opin Infect Dis, 2009.PMID 19369866