Paeds · infectious-diseases
Mumps
Also known as Mumps virus infection · Infectious parotitis · Epidemic parotitis · Mumps orchitis · Mumps meningitis
Fellowship topic on mumps in children: the mumps virus (a paramyxovirus) and its tropism for glandular and neural tissue that produces the hallmark parotitis and the complications — orchitis, meningitis, encephalitis, pancreatitis and deafness; the 12–25-day incubation and infectious window; the differential of parotid swelling and of acute scrotum; buccal-swab RT-PCR and IgM serology interpreted by timing and vaccination status; supportive management, isolation and notification; the 5-day exclusion rule; the two-dose MMR schedule and the waning-immunity resurgence problem; the third-dose outbreak-control strategy; special populations (postpubertal adolescents, pregnant women, immunocompromised, under-vaccinated communities, Indigenous and migrant families); and ANZ/UK/US/Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Mumps in five words — and the trap
Overview & Definition
Picture a sixteen-year-old boy brought to the emergency department with three days of fever and tender swelling at the angle of his jaw, now complaining of severe pain and swelling in his right testicle. He had two MMR doses as a child, but he has just started university where a mumps outbreak is circulating. The parotitis is unmistakable, but it is the orchitis — a complication that disproportionately affects postpubertal males — that brings him in, and that will frame the conversation about complications, transmission and prevention. Recognising that parotitis is only the visible tip of a multisystem virus is what turns a simple "swollen gland" encounter into a complete fellowship answer. [1] [6]
Mumps is an acute, contagious viral infection caused by the mumps virus, a single-stranded RNA paramyxovirus of the genus Rubulavirus, transmitted by respiratory droplets, direct contact with saliva, and contaminated fomites. In its classic form it produces acute non-suppurative enlargement of one or both parotid glands — infectious parotitis — but the virus is tropic for glandular epithelium and the central nervous system, so orchitis, oophoritis, pancreatitis, aseptic meningitis, encephalitis and sensorineural deafness are all part of the disease. There is a single serotype, and infection confers lifelong immunity in most cases. [5] [7]
The clinician's job has two halves. The acute half is to recognise parotitis and its complications, confirm the diagnosis where needed, provide supportive care, and prevent spread through isolation and notification. The preventive half is to deliver and reinforce the MMR programme — two doses in childhood, a catch-up for the under-immunised, and a third dose in outbreak settings — because the child who never develops mumps is the child the programme has protected. [1] [5]
Classification
Classify mumps the way it presents and the way it tests you — by the clinical course, by the complication that dominates, and by the host's immune status. The classic clinical course runs incubation through prodrome to parotitis and resolution. After a 12–25-day incubation, a brief one-to-two-day prodrome of fever, headache and malaise precedes the parotitis. The parotid swelling peaks over one to three days, may be unilateral before becoming bilateral, and resolves over five to ten days. The child is infectious from around two days before the parotitis appears until around five days after. [4] [5]
The second axis is the complication, because complications often bring the child to care and frequently dominate the examination answer. Aseptic meningitis is the commonest neurological complication; encephalitis is rare but serious. Orchitis affects up to a third of postpubertal males and rarely threatens fertility. Pancreatitis is usually mild. Sensorineural deafness is uncommon but often permanent. A fellowship answer that describes only parotitis and ignores the complication axis misses what the examiner is probing. [6] [9]
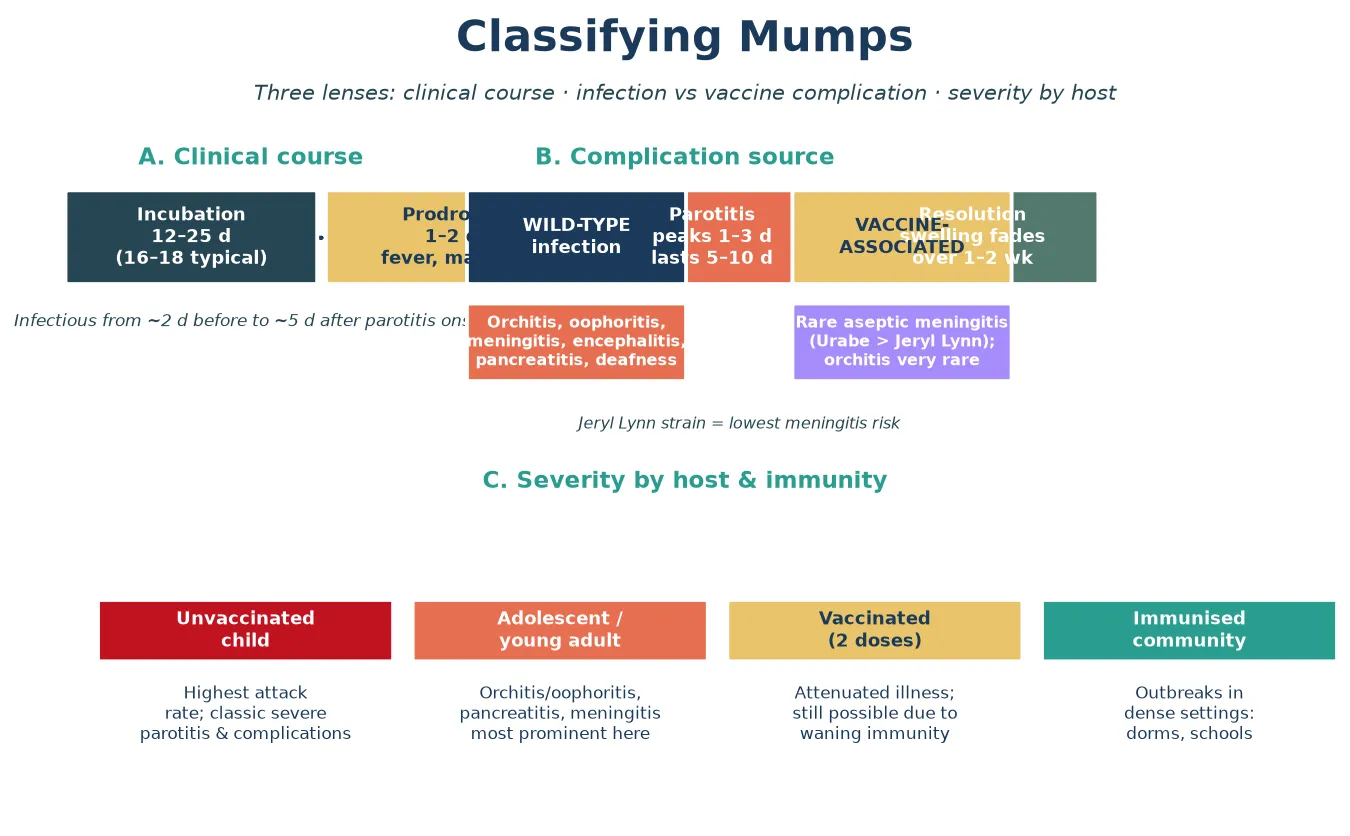
The third distinction, important in vaccine science and in outbreak interpretation, is between wild-type mumps infection and rare vaccine-associated events. The live-attenuated mumps vaccine strains differ in their adverse-event profile: the Urabe strain carries a higher risk of vaccine-associated aseptic meningitis, while the Jeryl Lynn strain used in most current programmes carries the lowest. Outbreaks in vaccinated populations usually reflect waning immunity rather than primary vaccine failure or vaccine-virus circulation, and the Jeryl Lynn-induced antibody has been shown to neutralise heterologous wild-type outbreak strains effectively. [7] [6]
Epidemiology & Risk Factors
Where does mumps sit, and who does it hurt? Before widespread vaccination, mumps was a near-universal childhood infection, but the two-dose MMR programme has dramatically reduced incidence in countries that achieve high coverage. Despite this, mumps has not been eliminated: recurrent outbreaks occur in highly vaccinated populations — in schools, universities, dormitories and tight-knit communities — because immunity wanes over the years after the second dose. Understanding who is at risk directs both acute care and the prevention and outbreak-control response. [2] [6]
Under-vaccination is the dominant individual-level risk factor. A child who has received zero or only one dose of mumps-containing vaccine has a markedly higher attack rate than a fully vaccinated peer, and an unvaccinated child exposed in a household or classroom outbreak is very likely to develop disease. Waning immunity is the dominant population-level driver: seroprevalence studies confirm that antibody to mumps is common in the population, but protection falls over time after vaccination, leaving adolescents and young adults susceptible in the very settings — crowded, social, mixed-household — where transmission thrives. [9] [10]
The usual setting for an outbreak in a vaccinated country is a dense, highly connected group of older adolescents or young adults. The large 2009–2010 outbreak in Orthodox Jewish communities in the United States, reported by Barskey and colleagues, demonstrated that mumps could spread extensively even in a population with high two-dose coverage, because waning immunity and intense exposure overwhelmed residual protection. The French and Canadian experiences reinforce the same lesson: the resurgence is a waning-immunity and coverage problem, not a vaccine-failure problem. [2] [10]
Pathophysiology
Why does a virus that everyone remembers as "swollen glands" also cause meningitis, orchitis and deafness? The answer lies in its tropism for glandular duct epithelium and neural tissue, and in the viraemic spread that carries it beyond the parotid. The mumps virus is inhaled or inoculated onto the respiratory or conjunctival mucosa, infects the epithelial cells of the nasopharynx, and then spreads to the parotid gland via the ductal epithelium of Stensen's duct. [5] [7]
From this initial replication, the virus enters the bloodstream in a primary viraemia and seeds its target organs: the salivary and parotid glands, the testes and ovaries, the pancreas, and the central nervous system. The clinical disease reflects where the virus lands and the immune response it provokes. In the parotid, interstitial oedema and a periductal mononuclear infiltrate produce the tender swelling; in the testes, oedema and pressure within the tunica produce orchitis; in the meninges, a lymphocytic pleocytosis produces aseptic meningitis. [5] [6]
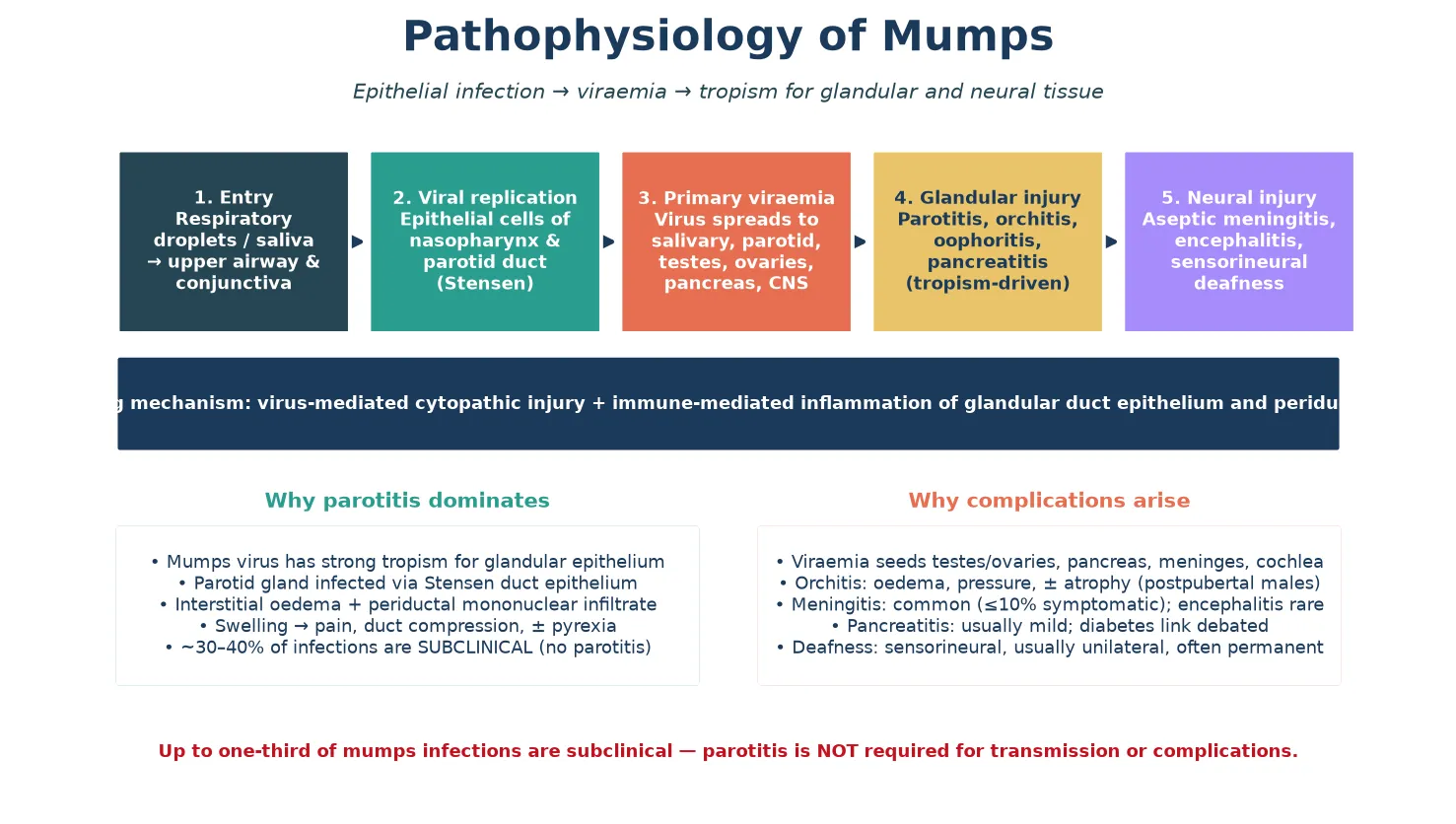
The critical clinical implication of this tropism is that parotitis is not required for transmission or for complications. Up to a third of mumps infections are subclinical — no parotitis at all — yet these individuals still shed virus and can still develop meningitis, orchitis or pancreatitis. This is why a vaccinated young adult with aseptic meningitis during a documented outbreak is mumps until proven otherwise, even without parotid swelling, and why the diagnosis must be considered on clinical and epidemiological grounds rather than on the presence of swollen glands alone. [5] [6]
The complication-specific severity follows from the same mechanism applied to different hosts. In a prepubertal child, orchitis and oophoritis do not occur because the gonadal tissue is immature; in a postpubertal male, the same tropism produces orchitis that can cause pressure, atrophy and, rarely, fertility concern. The biology of the virus is the same; the host turns a nuisance into a complication. The sensorineural deafness, when it occurs, reflects cochlear injury and is usually unilateral and permanent — a rare but important reason to take any sudden hearing loss during mumps seriously. [6] [9]
Clinical Presentation
The classic presentation is the parotitis every clinician recognises. After a one-to-two-day prodrome of fever, headache, malaise and loss of appetite, the child develops tenderness and swelling at the angle of the jaw, lifting the earlobe forward. The swelling is often unilateral for the first one to three days before becoming bilateral in around seven in ten cases, and it is exacerbated by eating — particularly sour or acidic foods that stimulate salivation. Submandibular and sublingual glands may also be involved. The child looks unwell but not toxic, and the illness settles over five to ten days. [5] [4]
The complications are part of the presentation because they often bring the child to care, and because they are what the examination rewards. Aseptic meningitis is the commonest neurological complication: headache, photophobia, neck stiffness and vomiting, with a lymphocytic cerebrospinal-fluid pleocytosis. It is usually self-limiting. Encephalitis is rare but presents with altered consciousness, seizures or focal signs and is life-threatening. Orchitis affects up to a third of postpubertal males, usually after the parotitis, with testicular pain, swelling and fever; atrophy may follow but sterility is rare. Pancreatitis presents with severe epigastric pain and vomiting. Sensorineural deafness is sudden, usually unilateral and often permanent. [6] [9]
In previously vaccinated individuals, the illness may be attenuated and the presentation atypical: milder or unilateral parotitis, an isolated complication such as orchitis or meningitis, or a non-specific viral illness in an outbreak setting. This is the group that tests the clinician, because the classic picture is muted and serology may be blunted by prior vaccination. A clinician who thinks of mumps only when bilateral parotitis is florid will miss the vaccinated outbreak case at the point it most matters for transmission control. [10] [11]
The symptoms that change disposition are the red flags: meningism, severe headache or altered consciousness suggesting CNS involvement; severe scrotal pain and swelling in a postpubertal male (orchitis, but always differentiated urgently from testicular torsion); severe abdominal or back pain suggesting pancreatitis; and any sudden hearing loss. A child with parotitis alone is usually managed supportively at home; a child with any of these features needs assessment and, often, admission. [6] [9]
Differential Diagnosis
For the child with parotid swelling, the differential is broad and the distinction matters for isolation, notification and reassurance. Other viral causes of parotitis include parainfluenza, influenza, coxsackievirus, Epstein–Barr virus, cytomegalovirus and HIV. Bacterial (suppurative) parotitis — usually Staphylococcus aureus — is unilateral, purulent and accompanied by high fever and toxicity, and it requires antibiotics. Salivary duct obstruction by a calculus, cervical lymphadenopathy (which sits below and behind the jaw rather than lifting the earlobe), and recurrent parotitis of childhood are the structural mimics. [5] [11]
For the postpubertal male with acute scrotal pain and swelling, the differential is the surgical emergency: testicular torsion must be excluded because it is time-critical and devastating if missed. Mumps orchitis typically follows parotitis, develops over hours to days rather than the sudden onset of torsion, and is accompanied by the systemic features of viral infection, but the two can overlap and the safest stance is urgent surgical assessment whenever torsion is plausible. Epididymo-orchitis from bacterial urinary-tract infection, torsion of the appendix testis, and trauma complete the list. [6] [9]
For the child with aseptic meningitis during an outbreak, the differential is the other enteroviral and viral causes of lymphocytic meningitis — echovirus, coxsackievirus, herpes simplex, and other respiratory viruses. The decisive point is that mumps meningitis is considered on clinical and epidemiological grounds, supported by CSF and buccal PCR, and that the management is supportive with the public-health layer of isolation and notification layered on top. [5] [6]
Clinical & Bedside Assessment
The assessment begins with a focused history built around the swelling and its setting. Ask about the onset, laterality and progression of the parotid swelling; the prodrome of fever and malaise; exacerbation by eating; and any testicular pain, headache, neck stiffness, photophobia, abdominal pain or hearing change. In an adolescent, ask explicitly about testicular symptoms and about hearing. And ask about the setting: school or university attendance, a known mumps case or outbreak, the child's MMR status with dates, and any pregnant or immunocompromised household contacts. The epidemiological history is often the clue that anchors the diagnosis. [4] [11]
Establish the immunisation status precisely. Record the number of MMR doses the child has received, with dates, and whether any doses were given outside the standard schedule. Under-vaccination raises both the likelihood and the severity of disease, and a child who has received only one dose is at higher risk than a two-dose peer. The immunisation history also frames the catch-up and outbreak-control conversation that follows the acute encounter. [5] [2]
Examine for the red flags that change disposition. Look for meningism, altered consciousness or focal neurological signs; for scrotal swelling, tenderness and the cremasteric and lie findings that distinguish orchitis from torsion; for abdominal tenderness suggesting pancreatitis; and for any hearing loss. Assess hydration and feeding, because parotitis makes eating painful and dehydration is a real risk. In the adolescent with testicular pain, the safest stance is to exclude torsion surgically before attributing the picture to mumps. [6] [9]
Document the public-health essentials at the bedside, because they drive the response. Record the date of parotitis onset, calculate the infectious and exclusion window, note school, university or childcare attendance, and begin the list of close and household contacts. These details determine notification, the five-day exclusion, and who needs review. A careful contact list at the first encounter prevents the late, disorganised public-health scramble. [4] [2]
Investigations
Diagnosis is confirmed by RT-PCR of a buccal or oral swab in the first days of parotitis. A buccal swab (massaging the parotid duct opening at the Stensen duct near the upper second molar) sent for RT-PCR has its highest yield in the first one to three days of parotitis, when viral shedding is greatest, and a British Columbia outbreak investigation confirmed that buccal PCR combined with genotyping is the most informative approach in a partially vaccinated population. PCR can be paired with a respiratory-virus panel when the differential includes other viral causes of parotitis. [8] [11]
Serology supports the diagnosis when PCR is delayed or the presentation is late. A positive mumps IgM supports recent infection, and a fourfold rise in IgG between acute and convalescent samples confirms the diagnosis. The limitation is that IgM may be blunted or absent in previously vaccinated individuals, so a negative IgM does not exclude mumps in a vaccinated person during an outbreak. This is why the diagnosis is built on the clinical picture, the epidemiological setting and PCR together, rather than on a single serological result. [11] [3]
In Australia and Aotearoa New Zealand, mumps is a nationally notifiable disease. Buccal-swab RT-PCR is the preferred diagnostic specimen in the first days of parotitis, with mumps IgM and IgG serology as a supplement, and viral genotyping to distinguish wild-type from vaccine-strain virus when the source is unclear. The Australian Immunisation Handbook (ATAGI) and the equivalent New Zealand immunisation schedule set the MMR programme and the public-health response, including the five-day exclusion and contact tracing. [5]
Basic supportive and complication-directed tests round out the workup as the clinical picture demands. A serum amylase or lipase is elevated in parotitis and in pancreatitis, so it is not specific, but a markedly raised lipase with severe epigastric pain supports pancreatitis. A full-blood count is non-specific. In the child with meningism, cerebrospinal-fluid analysis shows a lymphocytic pleocytosis with a normal glucose and a mildly raised protein, and CSF mumps PCR may be positive. Audiometry is indicated urgently for any hearing loss, because mumps deafness is usually permanent and the window for any intervention is narrow. [6] [9]
Management — Resuscitation
Resuscitation is about the complication that is deteriorating. The red flags are encephalitis, severe orchitis with a possible torsion differential, severe pancreatitis, and significant dehydration. A child with altered consciousness, seizures or focal signs needs urgent assessment, imaging as indicated, and supportive care in a monitored bed; mumps encephalitis is rare but life-threatening. The decision to admit a child with neurological involvement should be deliberately low-threshold. [6] [9]
Supportive care is the mainstay, because there is no antiviral with proven benefit in mumps. Give analgesia and antipyretics (paracetamol or ibuprofen), maintain hydration with oral fluids or intravenous fluids in the dehydrated child, and encourage a soft diet that does not stimulate painful salivation. For orchitis, provide scrotal support, analgesia and rest; severe cases may need admission for pain control, and urological review if torsion cannot be excluded. [5] [6]
There is no role for antibiotics, antivirals, or corticosteroids in uncomplicated mumps. Antibiotics add nothing because the disease is viral; antivirals have no proven benefit; and corticosteroids, though historically used for severe orchitis, lack evidence of benefit and are not routinely recommended. Stating this honestly — that mumps management is supportive and public-health, not pharmacological — is a point an examiner rewards. [5] [6]
Treat the complications as they arise. Aseptic meningitis is managed supportively with analgesia, hydration and observation, and is usually self-limiting. Pancreatitis is managed with analgesia, fluid support and a gradual return to feeding. Sensorineural deafness needs urgent audiology and ENT referral. The child with uncomplicated parotitis and no red flags is managed at home with supportive care, isolation and safety-netting. [6] [9]
Management — Definitive & Stepwise
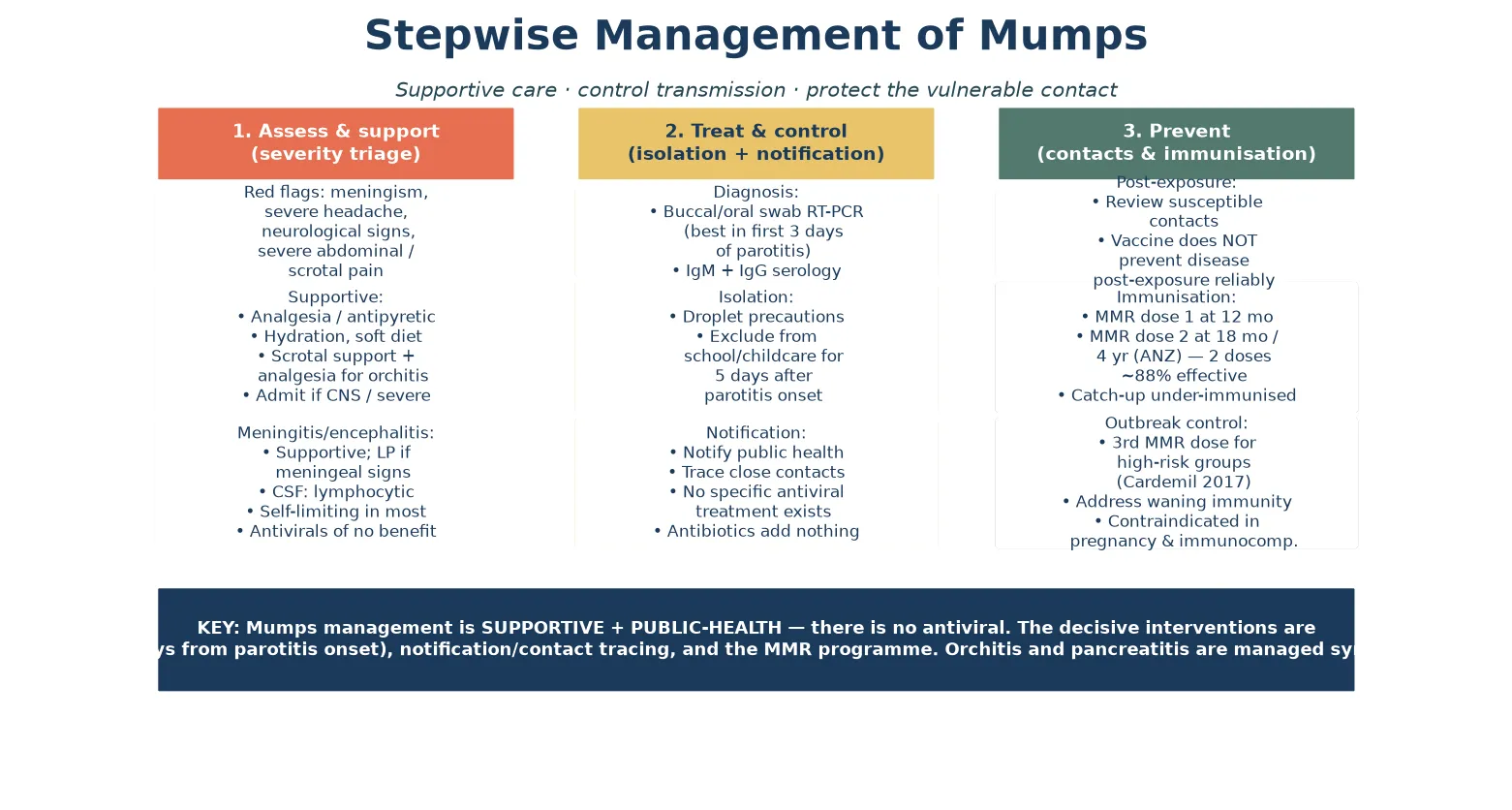
Definitive management is a stepwise pathway with the individual supportive case at one end and the public-health response at the other. Supportive care treats the child; isolation and exclusion interrupt transmission; notification and contact tracing protect the network; and the MMR programme, with a third dose in outbreaks, prevents the next case. There is no antiviral anchor in this pathway — the decisive interventions are behavioural and public-health. [4] [1]
The stepwise mumps pathway
Assess for red flags — meningism or encephalitis, severe scrotal pain (exclude torsion), pancreatitis, hearing loss — and admit any child with these; otherwise manage uncomplicated parotitis at home.
Confirm the diagnosis with a buccal or oral swab for mumps RT-PCR in the first days of parotitis, supplemented by IgM/IgG serology; genotyping distinguishes wild-type from vaccine strain when needed.
Treat supportively: analgesia and antipyretics, hydration, a soft diet, scrotal support for orchitis. There is no antiviral, antibiotic or steroid of proven benefit.
Isolate with droplet precautions and exclude from school, university or childcare for five days from the onset of parotitis swelling.
Notify public health according to local requirements, and trace household and close contacts; identify who is susceptible (under-vaccinated, pregnant, immunocompromised).
Prevent the next case: give catch-up MMR to the under-immunised, reinforce the two-dose schedule, and offer a third MMR dose to high-risk groups during an outbreak.
Isolation, exclusion and notification form the transmission-control layer. Place the case under droplet precautions, and exclude from school, university or childcare for five days from the onset of parotitis swelling — the evidence base for the change from nine to five days was reviewed by Kutty and colleagues. Notify public health according to local requirements, because mumps is notifiable in most jurisdictions, and the notification triggers the contact-tracing and outbreak-control response. The child who is isolated for five days and whose contacts are traced has done their public-health part. [4] [2]
The prevention layer is the MMR programme, which is where the clinician's leverage truly lies. Two doses of MMR are about 88% effective against mumps, but the protection wanes over the years after the second dose, so a vaccinated adolescent is not as protected as a recently vaccinated toddler. Catch-up vaccination of the under-immunised, reinforcement of the two-dose schedule, and — in outbreaks — a third MMR dose for high-risk groups are the tools that close the gap. A third MMR dose has been shown to improve outbreak control, as the Cardemil study demonstrated, and offering it in the right setting is an evidence-based act. [1] [5]
Specific Subtypes & Scenarios
An unvaccinated child with classic parotitis. Confirm with buccal-swab RT-PCR, give supportive care, isolate with droplet precautions and exclude for five days from parotitis onset, notify public health, and trace contacts. Offer catch-up MMR to the child and to under-immunised contacts. The unvaccinated child is the highest-attack-rate presentation, and the encounter is both a treatment and a prevention opportunity. [4] [5]
A postpubertal male with orchitis. Provide scrotal support, analgesia and rest, and exclude torsion surgically whenever the onset is sudden or the picture is equivocal. Orchitis affects up to a third of postpubertal males with mumps, usually follows the parotitis, and may cause testicular atrophy; sterility is rare but possible, so honest discussion and follow-up are warranted. Admit for pain control if needed. [6] [9]
A child with meningism during an outbreak. Assess for encephalitis (altered consciousness, seizures, focal signs), perform a lumbar puncture when safe, and expect a lymphocytic CSF pleocytosis. Mumps aseptic meningitis is usually self-limiting and managed supportively with analgesia and hydration, but the child needs isolation and notification. Distinguish it from other viral and bacterial meningitides on CSF and PCR. [6] [9]
A previously vaccinated young adult with attenuated, atypical illness. The vaccination blunts the parotitis and the serology, so the diagnosis rests on the clinical picture, the outbreak setting, and PCR with genotyping. Test, isolate and notify as for any case, and offer a third MMR dose as part of the outbreak-control response. This is the group that tests the clinician and that sustains the modern resurgence. [10] [2]
An outbreak in a school, university or tight-knit community. Coordinate with public health, offer vaccination and a targeted third dose to high-risk groups, exclude cases for five days, and reinforce the two-dose schedule. Outbreaks in highly vaccinated populations are a reminder that waning immunity and dense exposure can overwhelm residual protection, and that the public-health layer is what contains them. [1] [2]
A pregnant contact of a mumps case. Review the contact's immune status, reassure that mumps in pregnancy is not associated with the same teratogenic risk as rubella or primary cytomegalovirus, and exclude acute infection by serology and PCR if symptomatic. Live MMR vaccine is contraindicated in pregnancy but should be given postpartum if the woman is susceptible. [5] [9]
Complications & Pitfalls
Aseptic meningitis is the commonest neurological complication, and it is usually self-limiting, but encephalitis is the feared one and it is life-threatening. A child with mumps and altered consciousness, seizures or focal signs needs urgent assessment for encephalitis, because supportive and neuroprotective care in a monitored setting is what changes the outcome. Recognising encephalitis early, rather than attributing depressed consciousness to fever or dehydration, is one of the few interventions that genuinely changes outcome in severe mumps. [6] [9]
The central diagnostic pitfall is requiring parotitis to make the diagnosis in a vaccinated young adult. Up to a third of mumps infections have no parotitis, and in an outbreak a compatible illness — meningitis, orchitis, even a non-specific viral illness — warrants testing rather than dismissal. The rule that protects against this error is simple: a compatible illness in an exposed, waning-immunity individual is mumps until proven otherwise, and PCR with genotyping is the test that confirms it. [5] [2]
A second pitfall is missing testicular torsion in the postpubertal male with scrotal pain. Mumps orchitis and torsion can overlap, and torsion is the surgical emergency that cannot wait. The safe stance is urgent surgical assessment whenever torsion is plausible, because attributing acute scrotal pain to mumps without excluding torsion is a devastating, avoidable error. [6] [9]
A third pitfall is over-reliance on serology in a vaccinated individual. Mumps IgM may be blunted or absent in previously vaccinated people, so a negative IgM does not exclude mumps during an outbreak. Building the diagnosis on a single negative serological result, rather than on the clinical picture, the epidemiology and PCR, closes the door on the diagnosis at the point the resurgence epidemiology makes it most plausible. [11] [3]
Forgetting the public-health layer is the fourth error. Failing to isolate, to exclude for five days, to notify, or to trace and offer vaccination to contacts allows ongoing transmission to other susceptible individuals. The clinical encounter does not end when the child feels better; it ends when the contacts have been protected and the cluster has been contained. [4] [2]
The final pitfall is vaccine complacency. Because immunity wanes after two doses, a vaccinated young adult can still develop mumps, and a compatible illness in a vaccinated person still warrants testing. Dismissing a parotitic or meningitic illness because "they have had two MMR doses" closes the door on the diagnosis at the very point the resurgence epidemiology makes it most plausible. [10] [6]
Prognosis & Disposition
Most children with uncomplicated mumps recover fully within one to two weeks, and the morbidity in this group is driven less by danger than by disruption — pain on eating, dehydration, missed school. For these children the disposition is usually home management with supportive care, isolation, exclusion and clear safety-netting for the red flags. [5] [4]
The serious morbidity is concentrated in the complications: orchitis in postpubertal males (testicular atrophy possible, sterility rare), pancreatitis (usually mild), aseptic meningitis (usually self-limiting), encephalitis (rare but potentially fatal or with neurological sequelae), and sensorineural deafness (usually unilateral and permanent). The child with any of these needs assessment and, often, admission, and the prognosis depends on which complication and how promptly it is recognised. [6] [9]
Disposition follows severity. Admit the child with encephalitis or significant meningitis; admit the postpubertal male with severe orchitis or unresolved torsion concern; admit the child with significant dehydration or pancreatitis; and manage at home, with isolation and follow-up, the child with uncomplicated parotitis. The threshold for admitting a child with neurological involvement is deliberately low, because the margin between a self-limiting meningitis and an evolving encephalitis is narrow. [6] [9]
At discharge, complete the five-day exclusion, finish the contact tracing and notification, and give the family a clear safety-net for return — worsening headache, altered consciousness, severe scrotal or abdominal pain, or any hearing loss. Reinforce the MMR schedule, both for the child and for the household, because the discharge encounter is also a prevention opportunity. [4] [1]
Reinfection is rare, because natural infection confers lifelong immunity in most cases, but the waning of vaccine-induced immunity means that a vaccinated young adult remains at risk over time. Boosters and the outbreak third-dose strategy remain necessary across the life course, and a person who has had mumps still needs to maintain the broader immunisation schedule for measles and rubella. [5] [10]
Special Populations
Postpubertal adolescents and young adults are the group that carries the modern outbreak burden, because waning vaccine immunity meets dense social settings, and because their complications — orchitis, pancreatitis, meningitis — are the prominent ones. A low threshold to test, isolate and offer a third MMR dose in outbreak settings is the right stance for this group. [2] [10]
Unvaccinated or under-vaccinated children and communities carry higher attack rates and severity, and they are the substrate for outbreaks. Address vaccine hesitancy respectfully, offer catch-up MMR at every opportunity, and recognise that under-immunised pockets are where the disease transmits most efficiently. The MMR programme is a population responsibility as much as an individual one. [5] [2]
Immunocompromised children are at risk of severe disease if infected and should not receive live MMR vaccine themselves, so they depend on the immunity of the people around them. Cocooning matters most for these children, and exclusion of infectious contacts and early assessment of any compatible illness is the right stance. Live mumps vaccine is contraindicated in significant immunocompromise and in pregnancy. [5] [6]
Pregnant women exposed to mumps should have their immune status reviewed. Mumps in pregnancy is not associated with the same teratogenic risk as rubella, but acute infection can cause illness, and live MMR vaccine is contraindicated during pregnancy and should be given postpartum to susceptible women. Reassurance, serology and postpartum vaccination frame the response. [5] [9]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families may face barriers to timely immunisation and care. Ensure culturally safe, equitable access to MMR vaccination, treat actively when disease is suspected, and use trained interpreters rather than family members. Disadvantage should never be the reason a mumps diagnosis is delayed or a child is left unvaccinated. [5] [2]
Rural and remote children need timely access to diagnosis, complication assessment and public-health follow-up, often through outreach and telehealth, because distance can delay the care that a complicated case cannot afford to wait for. The plan for a remote family accounts for what is actually available locally, and retrieval is mobilised early when a child with encephalitis or severe orchitis deteriorates. [9] [6]
Evidence, Guidelines & Regional Differences
The global standard for mumps vaccination is embedded in the combined measles–mumps–rubella programme, and the Cochrane review of MMR and MMRV vaccines by Di Pietrantonj and colleagues established the effectiveness and safety of the vaccine, including the rare adverse-event profile. It is the reference against which national programmes are compared, and it frames mumps as a vaccine-preventable disease whose control is a public-health responsibility as much as a clinical one. [5] [7]
The effectiveness and limits of two-dose protection are defined by the resurgence epidemiology. The Barskey report of the large Orthodox Jewish community outbreak in the New England Journal of Medicine showed that mumps could spread extensively in a highly two-dose-vaccinated population, and the Cortese antibody-correlate study and the Vygen waning-immunity report from France explained why: antibody and protection fall over the years after the second dose. The Peltola editorial calling for "new thinking on mumps vaccines" framed the waning-immunity problem that the field has since worked to address. [2] [6]
Third-dose MMR for mumps outbreak control
Population: University outbreak in a two-dose-vaccinated population; a targeted third dose of MMR was offered to at-risk students.
Key finding
A third dose of MMR vaccine reduced the risk of mumps in the vaccinated group and improved outbreak control in the high-risk setting.
Practice change
In outbreaks affecting dense, two-dose-vaccinated populations of older adolescents and young adults, a targeted third MMR dose is an evidence-based control measure.
The vaccine-strain and laboratory-diagnosis evidence completes the picture. The Rubin study showed that antibody induced by the Jeryl Lynn vaccine strain effectively neutralises a heterologous wild-type outbreak strain, supporting the conclusion that outbreaks reflect waning immunity rather than escape. The Nunn and Hatchette laboratory studies demonstrated the value of buccal-swab RT-PCR and genotyping in partially vaccinated populations, and the Kutty seroprevalence and isolation-guidance studies set the diagnostic and public-health framework. [7] [8]
The regional policy structure is consistent in principle and varies in detail. In ANZ, mumps is nationally notifiable, the Australian Immunisation Handbook (ATAGI) and the New Zealand immunisation schedule set the two-dose MMR programme (at 12 and 18 months in Australia, with the second dose at 15 months and 4 years historically in New Zealand), and public-health units coordinate notification, contact tracing and outbreak control. In the UK, the Green Book and UK Health Security Agency guidance direct the programme, including the two-dose schedule at 12–13 months and 3 years 4 months. In the US, the CDC and AAP set the schedule (12–15 months and 4–6 years) and surveillance, with a third dose recommended in outbreak settings. In Canada, the Canadian Immunization Guide and provincial programmes deliver the equivalent strategy. In every region the principle is the same: two doses in childhood, catch-up for the under-immunised, isolation and notification of cases, and a targeted third dose in outbreaks. [5] [4]
The controversies are real and active: the durability gap after two doses and whether a routine third dose should be added to the standard schedule; the optimal outbreak-control strategy; the balance between case isolation and the disruption of exclusion; and the inequities in vaccine access that leave some communities unprotected. The defence against each is the same: high coverage, catch-up vaccination, prompt isolation and notification, a targeted third dose in outbreaks, and a public-health layer that does not stop at the bedside. [1] [6]
Exam Pearls
- Mumps is a droplet paramyxovirus infection with hallmark parotitis; incubation is 12–25 days (typically 16–18) and the child is infectious from ~2 days before to ~5 days after parotitis onset. [5]
- Up to a third of infections are subclinical — no parotitis — yet still transmit and can still cause meningitis, orchitis or pancreatitis. [6]
- The feared complications are aseptic meningitis (commonest neurological), encephalitis (rare, serious), orchitis (up to a third of postpubertal males), pancreatitis, and sensorineural deafness (usually unilateral and permanent). [9]
- Diagnose with buccal/oral-swab RT-PCR in the first days of parotitis, supplemented by IgM and rising IgG; IgM may be blunted in the vaccinated, so a negative IgM does not exclude mumps. [8]
- Treatment is supportive only — no antiviral, no antibiotic, no steroid of proven benefit. [5]
- Isolate and exclude for five days from parotitis onset (changed from nine days on the Kutty evidence review); notify public health. [4]
- Two doses of MMR are ~88% effective, but immunity wanes over the years after dose 2 — this, plus under-vaccination, drives resurgence. [10]
- A third MMR dose is evidence-based for outbreak control in dense, two-dose-vaccinated populations (Cardemil 2017). [1]
- Always exclude testicular torsion in the postpubertal male with acute scrotal pain — overlap with mumps orchitis is dangerous. [6]
- Jeryl Lynn is the lowest-meningitis-risk vaccine strain; outbreaks in vaccinated populations reflect waning immunity, not vaccine failure or escape (Rubin 2008). [7]
References
- [1]Cardemil CV; Dahl RM; James L; Wannemuehler K; et al Effectiveness of a Third Dose of MMR Vaccine for Mumps Outbreak Control. N Engl J Med, 2017.PMID 28877026
- [2]Barskey AE; Schulte C; Rosen JB; Handschur EF; et al Mumps outbreak in Orthodox Jewish communities in the United States. N Engl J Med, 2012.PMID 23113481
- [3]Cortese MM; Barskey AE; Tegtmeier GE; Zhang C; et al Mumps antibody levels among students before a mumps outbreak: in search of a correlate of immunity. J Infect Dis, 2011.PMID 21933874
- [4]Kutty PK; Kyaw MH; Dayan GH; Brady MT; et al Guidance for isolation precautions for mumps in the United States: a review of the scientific basis for policy change. Clin Infect Dis, 2010.PMID 20455692
- [5]Di Pietrantonj C; Rivetti A; Marchione P; Debalini MG; et al Vaccines for measles, mumps, rubella, and varicella in children. Cochrane Database Syst Rev, 2021.PMID 34806766
- [6]Peltola H; Kulkarni PS; Kapre SV; Paunio M; et al Mumps outbreaks in Canada and the United States: time for new thinking on mumps vaccines. Clin Infect Dis, 2007.PMID 17638194
- [7]Rubin SA; Qi L; Audet SA; Sullivan B; et al Antibody induced by immunization with the Jeryl Lynn mumps vaccine strain effectively neutralizes a heterologous wild-type mumps virus associated with a large outbreak. J Infect Dis, 2008.PMID 18558869
- [8]Nunn A; Masud S; Krajden M; Naus M; et al Diagnostic Yield of Laboratory Methods and Value of Viral Genotyping during an Outbreak of Mumps in a Partially Vaccinated Population in British Columbia, Canada. J Clin Microbiol, 2018.PMID 29491021
- [9]Kutty PK; Kruszon-Moran DM; Dayan GH; Alexander JP; et al Seroprevalence of antibody to mumps virus in the US population, 1999-2004. J Infect Dis, 2010.PMID 20662720
- [10]Vygen S; Fischer A; Meurice L; Mounchetrou Njoya I; et al Waning immunity against mumps in vaccinated young adults, France 2013. Euro Surveill, 2016.PMID 26987576
- [11]Hatchette T; Davidson R; Clay S; Pettipas J; et al Laboratory diagnosis of mumps in a partially immunized population: The Nova Scotia experience. Can J Infect Dis Med Microbiol, 2009.PMID 21119794