Paeds · infectious-diseases
Paediatric sepsis: diagnosis, antimicrobial treatment and source control
Also known as Paediatric sepsis · Septic shock in children · Phoenix sepsis criteria · Paediatric sepsis bundle · Source control in sepsis
A fellowship approach to paediatric sepsis covering Phoenix-criteria diagnosis, the first-hour recognition-to-resuscitation bundle, empiric and de-escalated antimicrobial therapy, judicious fluid and vasoactive support, source control, reassessment loops, special populations, and regional guideline boundaries.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A febrile child who has stopped interacting, a toddler with cold mottled limbs and a racing heart, and a neonate who will not feed are the clinical faces of paediatric sepsis. The diagnosis does not wait for microbiological proof. Sepsis is a syndrome: the child's own dysregulated response to infection has begun to injure their organs, and the team's job is to recognise that injury, reverse it, and treat the cause before it becomes irreversible. [1] [2] [12]
The 2024 Phoenix criteria redefined paediatric sepsis as suspected infection together with life-threatening organ dysfunction measured by a validated score. A child meets sepsis when the Phoenix score is two or more points, and meets septic shock when at least one of those points comes from cardiovascular dysfunction. These definitions replaced the old systemic inflammatory response syndrome (SIRS) framework because SIRS was too sensitive — many well children met it, and some dying children did not. [1] [2] [5]
Four ideas run through this whole topic and bind it together. Recognise the syndrome early and escalate. Resuscitate the failing circulation and breathing. Treat the organism with timely, appropriate antimicrobials. Control the source by draining, debriding, or removing the infected focus. The four pillars must run in parallel, not sequence, and each is reassessed against the child's response rather than against a fixed target. [3] [10] [11]
From suspicion to source control in the first hour
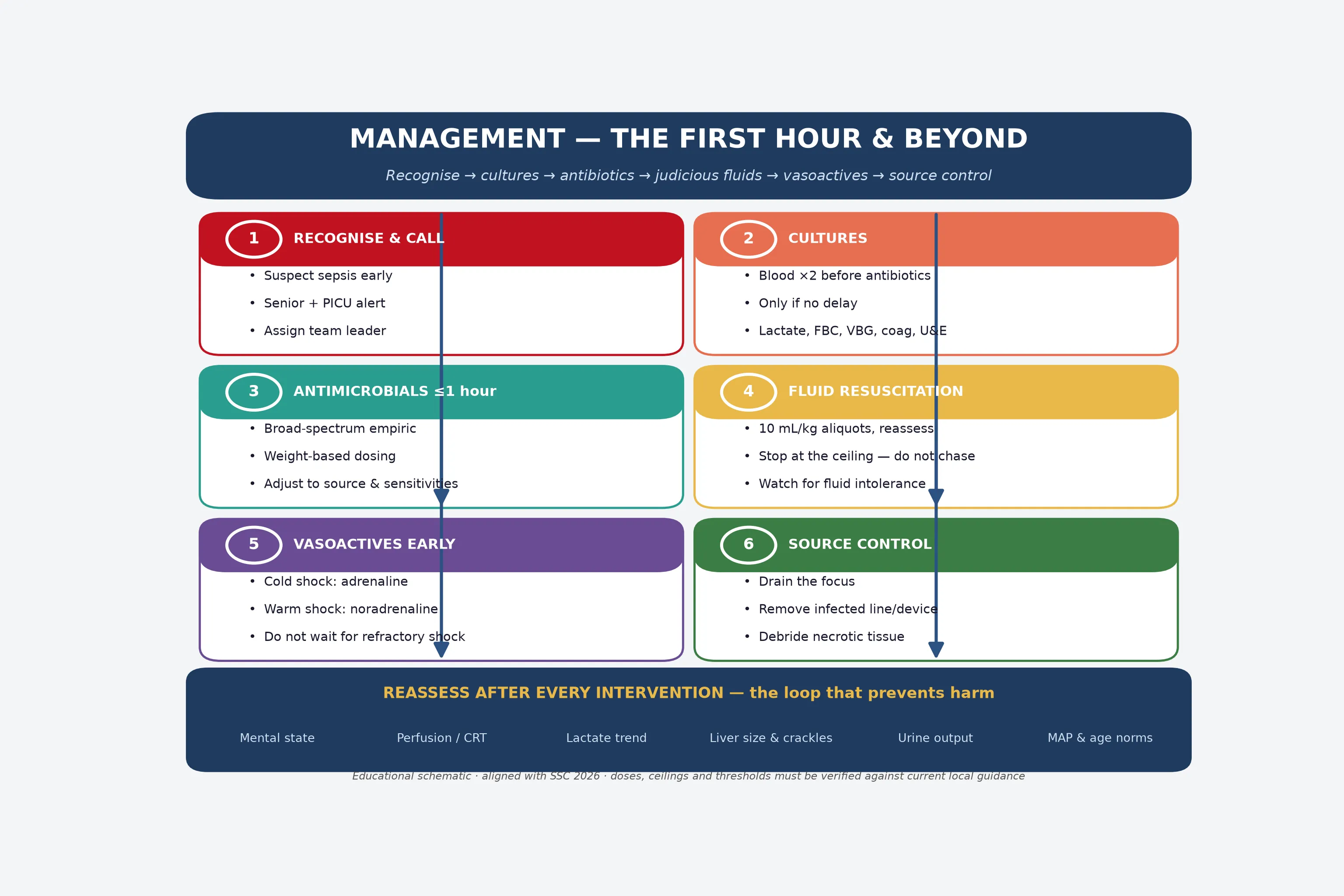
0–15 min: recognise
Suspect sepsis from infection plus illness severity. Assign a leader, attach monitoring, weigh or estimate weight, and alert senior and PICU or retrieval teams.
15–30 min: sample and drug
Draw blood cultures and a lactate before antibiotics only if it does not delay them. Give the first broad-spectrum, weight-based antimicrobial within one hour of recognition.
30–60 min: resuscitate
Give judicious fluid aliquots for shock, reassessing after each and stopping at the ceiling. Start vasoactives early for cold or warm shock rather than waiting for refractory shock.
60 min and beyond: source and reassess
Identify and control the source by imaging, drainage, debridement or device removal. De-escalate antimicrobials to the organism and sensitivities, and reassess after every intervention.
Classification
Severity is classified along a ladder that maps to escalating intervention. Infection alone is suspected or proven microbes without organ dysfunction. Sepsis adds life-threatening organ dysfunction captured by a Phoenix score of two or more. Septic shock is sepsis with cardiovascular dysfunction — at least one Phoenix cardiovascular point. Refractory shock persists despite adequate fluids and vasoactives, and heralds multi-organ failure and mortality. [1] [2] [12]
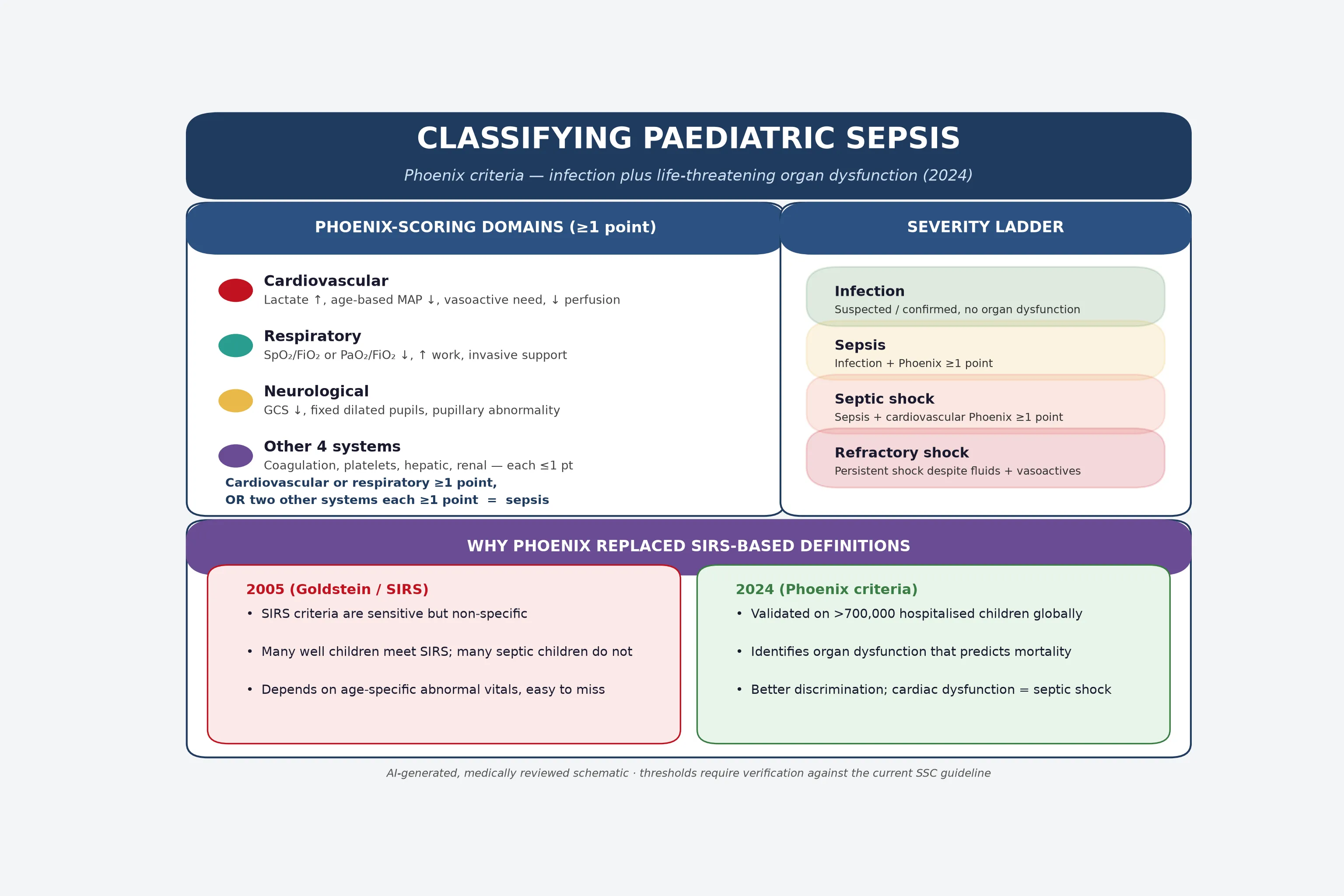
The Phoenix score rewards knowing where the points come from. Cardiovascular points come from lactate elevation, age-inappropriate mean arterial pressure, need for vasoactives, or impaired perfusion. Respiratory points reflect worsening oxygenation (SpO₂-to-FiO₂ or PaO₂-to-FiO₂ ratios), increased work, or invasive support. Neurological points follow reduced Glasgow Coma Scale, fixed pupils, or other pupillary abnormality. Four further systems — coagulation, hepatic, renal, and haematological — each contribute at most one point. [1] [2]
The rule that converts the score into a diagnosis is worth stating plainly. Cardiovascular or respiratory dysfunction of one point or more equals sepsis; alternatively, dysfunction in two of the other four systems also equals sepsis. When the qualifying points include cardiovascular dysfunction, the label becomes septic shock. This single move — tying shock to cardiovascular organ failure — is what makes Phoenix more discriminating than the old blood-pressure-dependent definitions. [1] [2]
Epidemiology & Risk Factors
Sepsis remains a leading cause of paediatric death worldwide, and the burden falls unevenly. The global SPROUT study of more than 6,000 children with severe sepsis or septic shock found a hospital mortality around 25 per cent, with most cases occurring in children with comorbid conditions (though previously healthy children still present) and in lower-resource settings. Mortality and morbidity cluster in the youngest infants, in children with chronic complex conditions, and in families facing social disadvantage. [7] [13]
The risk of sepsis rises whenever the host, the exposure, or the access to care is disadvantaged. Host factors include infancy (especially neonates and ex-preterm infants), immunocompromise from malignancy, transplant, or immunosuppressive therapy, indwelling central venous or urinary catheters, complex congenital heart disease, neurodisability, and skin breakdown. Exposure factors include recent surgery, trauma, burns, incomplete immunisation, and community-acquired infections such as meningococcaemia, pneumonia, or urinary tract infection. [7] [12]
Previously healthy
Community-acquired
- Often pneumonia, UTI, meningitis, meningococcaemia, or primary bacteraemia
- Sepsis may be the first sign of infection
- Good outcomes with early bundles
- Trust caregiver concern and trend
Complex / chronic
Healthcare-associated
- Central lines, devices, immunosuppression
- Resistant organisms and atypical pathogens
- Baseline physiology may mask deterioration
- Use the child's own baseline, not population norms
Neonate
Highest mortality
- Non-specific signs: poor feeding, temperature instability, apnoea
- Maternal and perinatal risk shape the differential
- Treat as sepsis until proven otherwise
- Early neonatal and PICU involvement
Equity matters at the bedside and in the answer. A large quality-improvement cohort showed that children from neighbourhoods with a lower Child Opportunity Index were recognised and treated for sepsis later than their more advantaged peers. Naming disadvantage, indigenous status, language access, and distance from definitive care is not an aside — these factors change who gets the bundle on time. [13]
Pathophysiology
Sepsis begins with a trigger — a bacterium, virus, fungus, toxin, or injured tissue — but the damage is done by the host's response to that trigger. Pathogen-associated and damage-associated molecular patterns activate innate immune cells, releasing a storm of pro- and anti-inflammatory mediators at the same time. Endothelium activates, glycocalyx sheds, coagulation and fibrinolysis fall out of balance, and the microcirculation becomes leaky and obstructed. [6] [12]
The macroscopic consequences of that molecular chaos are what the clinician sees and treats. Vasoplegia and capillary leak produce warm or cold shock and hypovolaemia. Cellular and metabolic failure — mitochondrial dysfunction and cytopathic hypoxia — explains the rising lactate and the organ that fails even when perfusion looks adequate. Reversible myocardial dysfunction lowers cardiac output, and disordered coagulation tips toward microthrombi and bleeding. [6] [12]
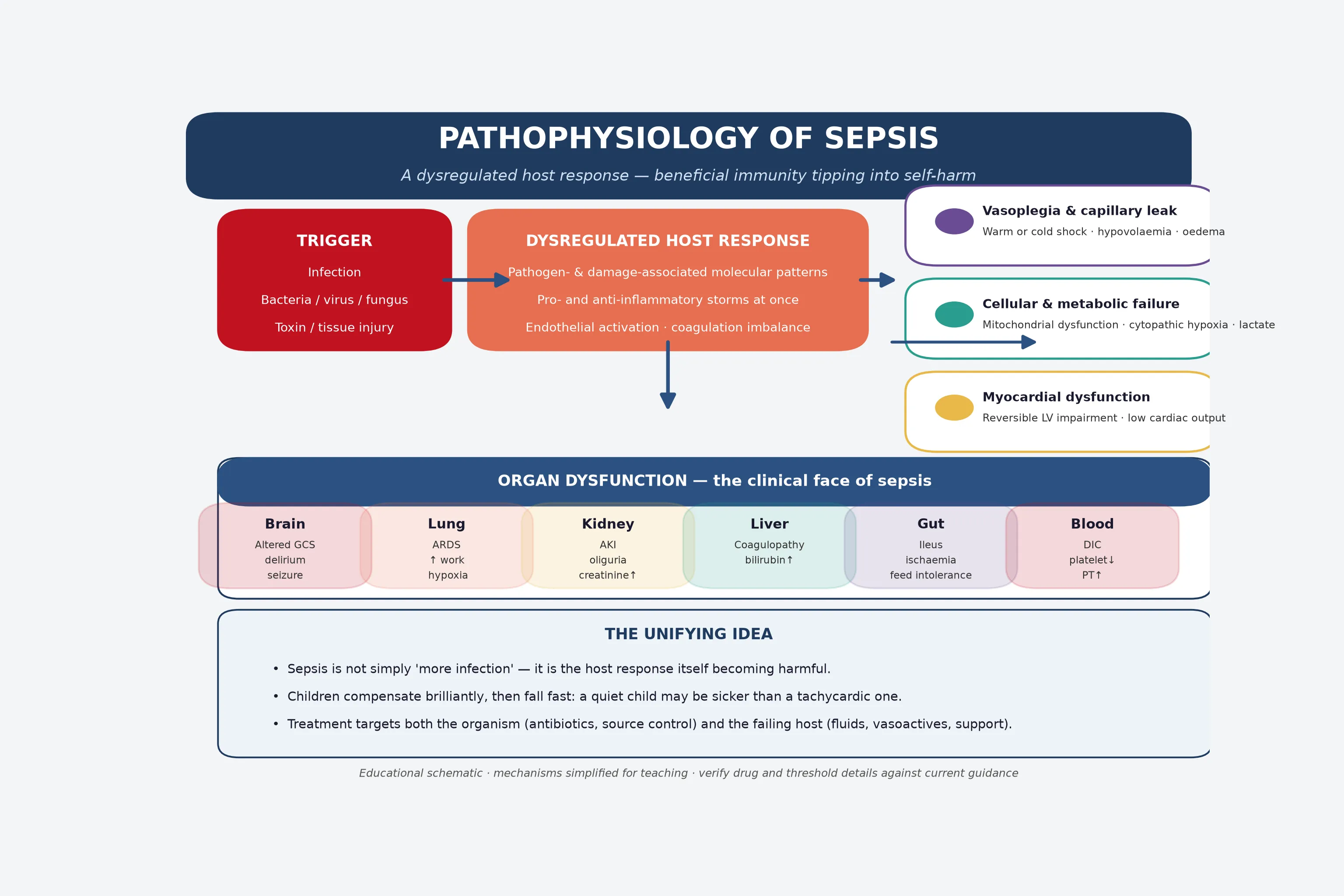
Two physiological lessons shape how you resuscitate. First, the child who compensated with tachycardia and vasoconstriction can decompensate abruptly when those reserves are exhausted — the shock you see is late. Second, the same capillary leak that causes hypovolaemia also floods the interstitium, so aggressive fluid can worsen pulmonary and tissue oedema without improving perfusion. Both lessons explain why reassessment after each aliquot, and early vasoactive support, matter more than reaching a fixed fluid volume. [8] [9] [12]
Clinical Presentation
Presentation spans a spectrum from subtle behavioural change to cardiovascular collapse, and the early signs are often behavioural. A febrile child who is less interactive, harder to console, or has a weak cry; an infant who stops feeding or develops temperature instability; or a school-age child who is confused or unusually quiet — each may be the first signal of sepsis. Trust these cues, especially when the caregiver says the child is not themselves. [12] [14]
Circulatory signs confirm a failing circulation and predict shock. Look for tachycardia out of proportion to fever, weak or bounding pulses, prolonged capillary refill, mottled or pale cool skin, reduced urine output, and altered mentation. Tachypnoea may reflect metabolic acidosis or the primary respiratory source. A non-blanching rash or rapidly evolving purpura demands immediate empiric treatment for meningococcaemia before any further investigation. [5] [12]
| Feature | Cold shock (common) | Warm shock (less common) |
|---|---|---|
| Extremities | Cold, mottled, prolonged capillary refill | Warm, flushed, brisk capillary refill |
| Pulses | Weak, thready | Bounding, wide pulse pressure |
| Mechanism | Low cardiac output, vasoconstriction | Vasodilation with relative hypovolaemia |
| First vasoactive | Adrenaline (epinephrine) to raise output | Noradrenaline (norepinephrine) to restore tone |
| Fluid response | Often improves with aliquots | May need early vasoactive, less fluid-tolerant |
Neonates and infants present differently and are the highest-risk group. Poor feeding, hypothermia or fever, irritability or lethargy, apnoea, grunting, a bulging or full fontanelle, and jaundice can each be the only sign of serious bacterial infection. Treat any unwell neonate as sepsis until proven otherwise, and involve neonatal or paediatric intensive care early. [12]
Differential Diagnosis
The differential splits into three questions the clinician must hold at once: is this sepsis, what else could mimic it, and where is the source? Sepsis itself is a syndrome, so the harder work is naming the likely organism and focus to guide empiric therapy. Common sources in children include pneumonia, urinary tract infection, meningitis or encephalitis, primary bacteraemia, intra-abdominal infection, skin and soft tissue infection, osteoarticular infection, and device-related infection. [3] [12]
Mimics of sepsis must be considered so that time-critical alternatives are not missed. Cardiogenic shock from myocarditis or a congenital heart lesion, hypovolaemic shock from haemorrhage or severe dehydration, anaphylaxis, tension pneumothorax, cardiac tamponade, and metabolic or endocrine crises such as adrenal insufficiency or diabetic ketoacidosis can all resemble septic shock. A rapid toxicological and metabolic screen, an electrocardiogram, and focused bedside ultrasound help separate these. [12]
The febrile child without organ dysfunction is not sepsis, and over-labelling risks unnecessary investigation and admission. Conversely, a well-appearing child with high-risk features — abnormal behaviour, age under three months, immunocompromise, an indwelling device, or caregiver concern — still warrants careful observation and a low threshold to treat. The Phoenix score and structured early-warning tools help here, but they assist judgement; they never replace it. [14] [15]
Clinical & Bedside Assessment
Bedside assessment follows the standard primary survey, but the priorities are weighted toward circulation and disability because that is where septic children die. Begin at the doorway with a first impression of appearance, work of breathing, and circulation to skin. Then move through airway, breathing, and circulation, attaching monitoring, estimating weight, and measuring capillary refill, pulse quality, blood pressure, perfusion, mentation, and a bedside glucose. [12]
Circulatory assessment in septic shock is a synthesis, not a single number. Combine heart rate and pulse quality, capillary refill measured under standard conditions, skin temperature and colour, blood pressure relative to age, urine output, mentation, and the trend over time. A normal blood pressure alone never excludes shock, and a single normal capillary refill never excludes serious illness. The direction of change is more informative than any isolated reading. [12] [5]
A focused history targets the source, host risk, and the trajectory. Ask about onset, fever pattern, focal symptoms, intake and urine output, immunisation status, recent surgery or device manipulation, immune status, underlying conditions, medications, exposures and travel, and exactly what the caregiver has noticed change. Examine for the focus — chest, abdomen, skin, joints, central nervous system, ears and throat, and any device or line — without delaying resuscitation. [3] [12]
Investigations
Investigations serve two purposes: to confirm the syndrome and to find the cause. Confirming the syndrome requires a lactate (the metabolic signature of tissue hypoperfusion), a venous or arterial blood gas, full blood count and differential, coagulation, electrolytes, urea, creatinine, liver function, and glucose. Calculate the Phoenix score from the results as they return, because the score drives both the diagnosis and the disposition. [1] [3]
Finding the cause means microbiology before antimicrobials, but never at the cost of delaying the first dose. Draw two blood cultures from separate sites, and add cultures of urine, cerebrospinal fluid, and any drainable focus when clinically indicated and safe to obtain. A lumbar puncture is deferred if the child is unstable, has coagulopathy, or has signs of raised intracranial pressure, and empiric meningitis treatment proceeds regardless. Molecular and rapid antigen tests refine the differential within hours. [3] [4]
SEPSIS bundle in the first hour
Imaging is targeted to the suspected source and to safety. A chest radiograph is routine; abdominal ultrasound or computed tomography follows localising abdominal signs or a positive peritoneal examination; echocardiography assesses cardiac function and volume status when shock is refractory or fluid-intolerant. Bedpoint ultrasound helps assess volume responsiveness and cardiac function, but it does not replace repeated clinical reassessment. [3] [12]
Management — Resuscitation
Resuscitation and antimicrobials run together and begin the moment sepsis is recognised. Assign a team leader, call for senior and critical-care help, attach full monitoring, and estimate weight using a validated method. State, before each intervention, the response you expect; then check whether you achieved it. This closed-loop discipline is what separates a bundle that works from a checklist that does not. [3] [10]
Airway and breathing are stabilised first because hypoxaemia and hypercapnia worsen the shock state. Give high-flow oxygen to the hypoxaemic child, and escalate to positive-pressure support when work of breathing is excessive, fatigue is developing, or gas exchange is failing. For the child in refractory shock or respiratory failure, secure the airway early with skilled support, using age- and weight-appropriate equipment and drugs. [3] [12]
Fluid resuscitation is the single most contested intervention in paediatric sepsis, and the evidence demands humility. For septic shock with impaired perfusion, give a 10 mL/kg crystalloid aliquot and reassess immediately — checking perfusion, mentation, liver size, breath sounds, and work of breathing. Repeat only if shock persists and the child remains fluid-responsive, and stop at a locally agreed ceiling rather than chasing a target. The FEAST trial showed that bolus fluids increased mortality in some African children with severe infection, and the Fluids in Shock pilot established the feasibility of a restricted-bolus strategy; both shape a cautious, reassessment-driven approach. [8] [9]
Balanced crystalloid and 0.9% saline have been compared head-to-head. The 2026 PRoMPT BOLUS trial found that, in children with septic shock, balanced fluids and 0.9% saline gave similar outcomes, settling a long debate and leaving the clinician free to follow local protocol. Whichever fluid is chosen, the discipline of aliquots, reassessment, and a ceiling is what protects the child from fluid harm. [16]
Vasoactive support should begin early rather than being held in reserve for refractory shock. For cold shock with low cardiac output, adrenaline (epinephrine) is the first-line vasoactive; for warm shock with vasodilation and a wide pulse pressure, noradrenaline (norepinephrine) restores vascular tone. Start the infusion, titrate to perfusion and mean arterial pressure targets appropriate for age, and escalate to a second agent as needed. The old practice of waiting until several litres of fluid have failed delays effective therapy. [3] [4]
Adjuncts address reversible metabolic threats. Treat hypoglycaemia promptly and recheck; correct clinically significant electrolyte derangements; and consider stress-dose hydrocortisone for catecholamine-resistant shock, especially in children with known or suspected adrenal insufficiency. Blood product transfusion follows standard thresholds, not sepsis-specific triggers, and is reserved for the child who needs it. [3] [12]
Management — Definitive & Stepwise
Definitive management converts the empiric bundle into targeted therapy as information arrives. The aims are to narrow the antimicrobial to the organism, to control the source definitively, and to support each failing organ until recovery. This phase belongs to the paediatric intensive care team for the sickest children, but the general paediatrician must drive the transition deliberately. [3] [11]
Antimicrobial therapy de-escalates from broad empiric cover to the narrowest effective regimen as soon as an organism and its sensitivities are known. The initial choice depends on the suspected source, host risk, local resistance patterns, and immunisation status. Cover broadly for the previously well child — for example, a third-generation cephalosporin with or without vancomycin depending on local resistance and suspicion of resistant organisms — and add anti-pseudomonal, antistaphylococcal, antiviral, or antifungal cover when the host or focus demands it. Stewardship principles require a documented indication, a planned duration, and a daily review to stop or narrow therapy. [3] [4]
Empiric antimicrobial principles (verify against current local guidance)
The usual duration of antimicrobial therapy for uncomplicated sepsis is around seven to ten days, but it is individualised to the organism, source, clinical response, and whether source control was achieved. Stop therapy promptly when an alternative non-infective diagnosis is confirmed, and shorten the course when the child recovers quickly with good source control. Daily stewardship review prevents the harm of unnecessary, prolonged, or broad therapy. [3] [11]
Source control is definitive therapy and is often definitive diagnosis as well. It means draining an abscess or empyema, removing an infected central venous or urinary catheter, debriding necrotic tissue, relieving an obstructed and infected viscus, or decompressing a compartment. Imaging defines the focus, and surgical, interventional radiology, or urological teams deliver control — ideally within hours of recognition for unstable children. Antibiotics alone rarely cure a drainable focus. [3] [12]
Specific Subtypes & Scenarios
Different sources demand different first moves. Meningococcaemia with a purpuric rash needs immediate empiric antibiotics and fluids, with early vasoactives for shock and a low threshold for intubation. Pneumonia with sepsis requires antibiotics, targeted oxygen and respiratory support, and drainage of any effusion or empyema. Urinary tract infection with sepsis responds to antibiotics and fluids, and an obstructed pyonephrosis needs urgent urological drainage. [3] [12]
The toxic-shock and toxin-mediated syndromes are time-critical and demand source control alongside antibiotics that suppress toxin production. Staphylococcal toxic shock and streptococcal toxic-shock-like syndrome present with fever, rash, hypotension, and multi-organ involvement. Combine fluid resuscitation, clindamycin (and intravenous immunoglobulin in severe cases), and aggressive surgical debridement of any necrotising focus. [12]
Recognise-to-definitive-care pathway
Sepsis in the technology-dependent child turns on the personal baseline. A ventilator-dependent or central-line-dependent child whose caregiver reports that the child is not themselves must be assessed against their usual observations, tone, and interaction. Device-related infection is high on the differential, and device removal is often both treatment and diagnosis. Specialist teams and the child's personal emergency plan guide escalation. [12]
Complications & Pitfalls
The complications of sepsis and of its treatment overlap, and both must be sought actively. Untreated or late-treated sepsis causes multi-organ failure, disseminated intravascular coagulation, acute kidney injury, acute respiratory distress syndrome, neurological injury, and death. Treatment-related harm includes fluid overload with pulmonary oedema, electrolyte disturbance, secondary infection, antimicrobial adverse effects, and line and procedure complications. [3] [12]
The common cognitive pitfalls cluster around three failures. Failure to recognise happens when abnormal behaviour is attributed to fever, anxiety, or crying, or when a normal single value reassures the team. Failure to act happens when antibiotics are delayed for imaging or for a lumbar puncture the child is too unstable to tolerate. Failure to stop happens when fluids continue past the ceiling or when broad antimicrobials are never narrowed. Each failure is preventable with structured reassessment and stewardship. [8] [9] [11]
Recognise
- Infection plus organ dysfunction
- Calculate a Phoenix score
- Behaviour change is an early cue
- Call for help early
First hour
- Cultures before drug, only if no delay
- Broad-spectrum antibiotic within 1 hour
- Fluid aliquots, reassess each
- Vasoactives early for shock
Source control
- Drain the focus
- Remove infected device
- Debride necrotic tissue
- Antibiotics alone do not cure a drainable focus
Reassess
- Mental state, perfusion, lactate trend
- Liver size and crackles signal overload
- Stop fluids at the ceiling
- De-escalate antimicrobials daily
Boundaries
- No universal fluid target
- Blood pressure is late in paediatric shock
- FEAST restrains bolus enthusiasm
- Equity changes who is treated on time
“Phoenix sepsis → first-hour bundle (cultures, antibiotic ≤1 h, judicious fluids, early vasoactives) → source control → reassess after every intervention → de-escalate antimicrobials → safe disposition.”
Pitfalls in communication and handover cause harm at the boundaries of care. A septic child transferred to imaging or to another ward can deteriorate out of sight of the resuscitation team. Structured handover that carries the diagnosis, the timed interventions, the trend, the pending results, and the specific deterioration plan prevents the loss of momentum that kills children. [11] [12]
Prognosis & Disposition
Prognosis depends on early recognition more than on any single drug or device. Children who receive a complete first-hour bundle, source control, and organ support in a timely sequence have markedly better survival than those who do not. Quality-improvement collaboratives such as the New York mandate and the IPSO network have demonstrated that protocolised bundles reduce paediatric sepsis mortality across many hospitals at once. [10] [11]
Disposition follows severity and trajectory, not a diagnosis label alone. Any child with septic shock, persistent organ dysfunction, or a need for vasoactives or invasive ventilation belongs in paediatric intensive care. The child who responds quickly to a fluid aliquot and antibiotics may be observed in a high-dependency or acute ward with clear escalation criteria. Retrieval services should be engaged before the child exceeds local capability, and transfer decisions weigh distance, weather, escort skill, and the receiving unit's capacity. [11] [12]
Recovery is not the end of the episode. Survivors of severe sepsis face ongoing morbidity — new or worsened organ dysfunction, prolonged weakness, psychological distress, and disrupted schooling and family life. Follow-up must address the underlying diagnosis, antimicrobial adverse effects and duration, pending microbiology results with named ownership, rehabilitation needs, and a written safety net the family can act on. A brief improvement never discharges a child whose trend or concerns remain unresolved. [3] [12]
Special Populations
The immunocompromised child can deteriorate with muted signs and atypical organisms. Neutropenia from chemotherapy, recent transplant, primary immunodeficiency, and immunosuppressive therapy each broaden the differential to include resistant bacteria, viruses, and fungi. Cover broadly from the outset, remove any infected central line, and involve the oncology, transplant, or immunology team early, because their input shapes both the empiric regimen and the source-control plan. [3] [12]
The neonate is a population unto itself. Non-specific behavioural, feeding, and temperature changes may be the only signs of sepsis, and the differential is shaped by maternal risk, perinatal events, and gestation. Use neonatal-specific antimicrobial regimens, weigh fluid boluses carefully given the immature myocardium, and engage neonatal intensive care from the first suspicion. [12]
Australia and Aotearoa New Zealand: the Surviving Sepsis Campaign 2026 children's guideline is the international evidence base; the Royal Children's Hospital Melbourne Sepsis guideline and the Australian Commission on Safety and Quality in Health Care sepsis program translate it into local pathways. State and territory retrieval, escalation, and antimicrobial-formulary rules vary and must be checked against the current local source. Care for Aboriginal and Torres Strait Islander and Māori children must be culturally safe, with whānau participation and earlier escalation given the documented inequity in sepsis outcomes. [3] [13]
Global and low-resource settings: the WHO global report on sepsis documents the disproportionate burden in lower-resource settings. The FEAST trial's finding — that fluid boluses increased mortality in African children with severe infection — is population-specific and restrains uncritical bolus enthusiasm where intensive-care rescue is limited. Apply the principles of recognition, antimicrobials, and source control, but tailor fluid strategy and escalation thresholds to the resources that can actually rescue the child. [8]
Evidence, Guidelines & Regional Differences
The evidence underpinning paediatric sepsis care has matured rapidly, and a candidate should know where it is strong and where it is contested. The 2024 Phoenix criteria were derived and validated on more than 700,000 hospitalised children across multiple continents and provide a robust, mortality-predictive definition that supersedes SIRS. The Surviving Sepsis Campaign 2026 children's guideline collates the current evidence and is the primary international reference for resuscitation, antimicrobials, and source control. [1] [2] [3]
Bundle delivery works. Both the New York state sepsis-care mandate, studied in a large JAMA analysis, and the multicentre IPSO collaborative showed that protocolised recognition and first-hour care reduce paediatric sepsis mortality across hospitals. Clinical decision support can help front-line clinicians apply the bundle, though its effect depends on how the tool fits local workflow. [10] [11] [15]
Fluids remain the area of greatest debate. FEAST demonstrated harm from bolus fluids in one African population, the Fluids in Shock pilot established that a restricted-bolus strategy is feasible, and the 2026 PRoMPT BOLUS trial found balanced and saline fluids equivalent in children with septic shock. The synthesis is a cautious, reassessment-driven approach with a ceiling rather than a target, applied differently in low-resource settings without intensive-care rescue. [8] [9] [16]
Board and assessment distinctions
RACP current PREP curriculum candidates in 2026 must keep current learning objectives separate from the renewed curriculum goals applying to first-year trainees from 2027. RCPCH Progress+ outcomes are curriculum expectations, while MRCPCH Foundation of Practice, Theory and Science, and Applied Knowledge in Practice are theory classifications and the Clinical stations are assessment formats. The ABP General Pediatrics Content Outline classifies written examinations, while ACGME Pediatrics Milestones govern residency development and are distinct from certification. [3] [13]
| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Interpret a vignette and trend, classify sepsis with Phoenix, and choose the safest first-hour action |
| RACP DCE long case | Integrate host risk, source, organ failure, devices, family context and a resuscitation-to-disposition plan |
| MRCPCH clinical / video | Recognise septic shock from bedside and video signs, and state the next action |
| ABP | Apply content domains and universal tasks to recognise, resuscitate and treat sepsis |
| RCPSC structured oral | Manage evolving septic shock across rural or tertiary contexts with reassessment and escalation |
Exam Pearls
Viva: the child whose lactate is rising despite fluids
Do not continue to bolus. Reassess for fluid intolerance — hepatomegaly, gallop, crackles — and start or escalate vasoactives, because a rising lactate with worsening perfusion signals refractory shock and ongoing anaerobic metabolism. State the ceiling you have reached, request early PICU involvement, and consider stress-dose hydrocortisone for catecholamine-resistant shock. Source control proceeds in parallel. [3] [9] [12]
Structured oral: rural recognition and retrieval
State the Phoenix score and shock status, summarise the first-hour bundle already delivered, and call retrieval before local capability is exceeded. Agree the destination, the monitoring and escort required, what the local team can safely continue, the deterioration plan, and the family communication. Do not invent a universal transport trigger or wait until all local options have failed. [11] [13]
References
- [1]Sanchez-Pinto, L Nelson; Bennett, Todd D; DeWitt, Peter E Development and Validation of the Phoenix Criteria for Pediatric Sepsis and Septic Shock. JAMA, 2024.PMID 38245897
- [2]Schlapbach, Luregn J; Watson, R Scott; Sorce, Lynn R International Consensus Criteria for Pediatric Sepsis and Septic Shock. JAMA, 2024.PMID 38245889
- [3]Weiss, Scott L; Peters, Mark J; Oczkowski, Stephen J W Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2026.PMID 41869844
- [4]Weiss, Scott L; Peters, Mark J; Alhazzani, Waleed Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2020.PMID 32032273
- [5]Goldstein, Bram; Giroir, Brett; Randolph, Adrienne International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine, the World Federation of Pediatric Intensive and Critical Care Societies, and the Latin American Society of Intensive Care, 2005.PMID 15636651
- [6]Singer, Mervyn; Deutschman, Clifford S; Seymour, Christopher W The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA, 2016.PMID 26903338
- [7]Weiss, Scott L; Fitzgerald, Julie C; Pappachan, Joseph Global epidemiology of pediatric severe sepsis: the sepsis prevalence, outcomes, and therapies study. American journal of respiratory and critical care medicine, 2015.PMID 25734408
- [8]Maitland, Kathryn; Kiguli, Sarah; Opoka, Robert O Mortality after fluid bolus in African children with severe infection. The New England journal of medicine, 2011.PMID 21615299
- [9]Inwald, David P; Canter, Robert; Woolfall, Kerry Restricted fluid bolus volume in early septic shock: results of the Fluids in Shock pilot trial. Archives of disease in childhood, 2019.PMID 30087153
- [10]Evans, Ithan D Peltan; Phillips, Greg S; Alpern, Elizabeth R Association Between the New York Sepsis Care Mandate and In-Hospital Mortality for Pediatric Sepsis. JAMA, 2018.PMID 30043064
- [11]Paul, Richard; Niedner, Matthew; Riggs, Roberta Bundled Care to Reduce Sepsis Mortality: The Improving Pediatric Sepsis Outcomes (IPSO) Collaborative. Pediatrics, 2023.PMID 37435672
- [12]Bjorklund, Ashley; Resch, Jacob; Slusher, Tina Pediatric Shock Review. Pediatrics in review, 2023.PMID 37777656
- [13]Rutman, Laila; Richardson, Tyler; Auletta, Joseph Association between Child Opportunity Index and paediatric sepsis recognition and treatment in a large quality improvement collaborative: a retrospective cohort study. BMJ quality & safety, 2026.PMID 40345682
- [14]Alpern, Elizabeth R; Scott, Halden F; Balamuth, Frances Derivation and Validation of Predictive Models for Early Pediatric Sepsis. JAMA pediatrics, 2025.PMID 41082207
- [15]Scott, Halden F; Sevick, Colleen J; Colborn, Kenneth L Clinical Decision Support for Septic Shock in the Emergency Department: A Cluster Randomized Trial. Pediatrics, 2025.PMID 40490252
- [16]Balamuth, Frances; Weiss, Scott L; Long, Eleanor Balanced Fluid or 0.9% Saline in Children Treated for Septic Shock. The New England journal of medicine, 2026.PMID 42028918