Paeds · infectious-diseases
Parasitic infections in children
Also known as Intestinal parasites in children · Helminthiasis · Soil-transmitted helminth infection · Giardiasis · Enterobiasis · Scabies · Pediculosis capitis · Toxocariasis
Fellowship topic on parasitic infections in children: the broad landscape of protozoa (Giardia), soil-transmitted helminths (Ascaris, hookworm, Strongyloides), schistosomiasis, toxocariasis, cutaneous larva migrans, and the ectoparasites scabies and pediculosis; the faecal-oral, skin-penetration and direct-contact routes of acquisition; the clinical patterns from anal pruritus and chronic diarrhoea to iron-deficiency anaemia, visceral toxocariasis and creeping eruption; diagnosis by stool microscopy, antigen testing, tape test, skin scraping and clinical recognition; and the stepwise management from mebendazole and albendazole for intestinal worms to tinidazole for giardiasis, ivermectin for strongyloidiasis and scabies, permethrin for ectoparasites, and the essential public-health principles of treating households, checking glucose-6-phosphate dehydrogenase status, and avoiding steroids alone in Strongyloides infection.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Parasitic infections in children encompass a broad group of diseases caused by protozoa, helminths, and ectoparasites that remain among the most common infections of childhood worldwide. In resource-rich settings such as Australia and New Zealand they are frequent in primary care and emergency presentations, while in resource-limited settings they contribute significantly to malnutrition, anaemia, impaired growth, and lost educational opportunity. The paediatric vulnerability arises from immature hygiene behaviours, oral exploration, close physical contact in childcare and school, and exposure to soil, sandpits, and animals. [1]
The organisms divide cleanly into three functional groups that dictate how the clinician thinks at the bedside. Protozoa such as Giardia lamblia are single-celled organisms acquired by the faecal-oral route that colonise the intestinal lumen. Helminths include the soil-transmitted roundworms Ascaris lumbricoides, hookworm, and Strongyloides stercoralis, the pinworm Enterobius vermicularis, the tissue-migrating Toxocara species, and the blood fluke Schistosoma. Ectoparasites, principally the scabies mite Sarcoptes scabiei and the head louse Pediculus humanus capitis, live on the skin or hair and cause disease through burrowing and hypersensitivity. [2]
The cardinal principle is that most parasitic infections are treatable with simple, safe, oral or topical therapy, but the diagnosis is missed because the clinician did not think of it. A child with chronic diarrhoea may be labelled irritable bowel syndrome when Giardia antigen was never sent. A child with iron-deficiency anaemia may be given iron supplements alone when stool microscopy would have found hookworm ova. The travel history, household and animal exposures, and the recognition of classic clinical patterns are the hinge of every encounter. [3]
Classification
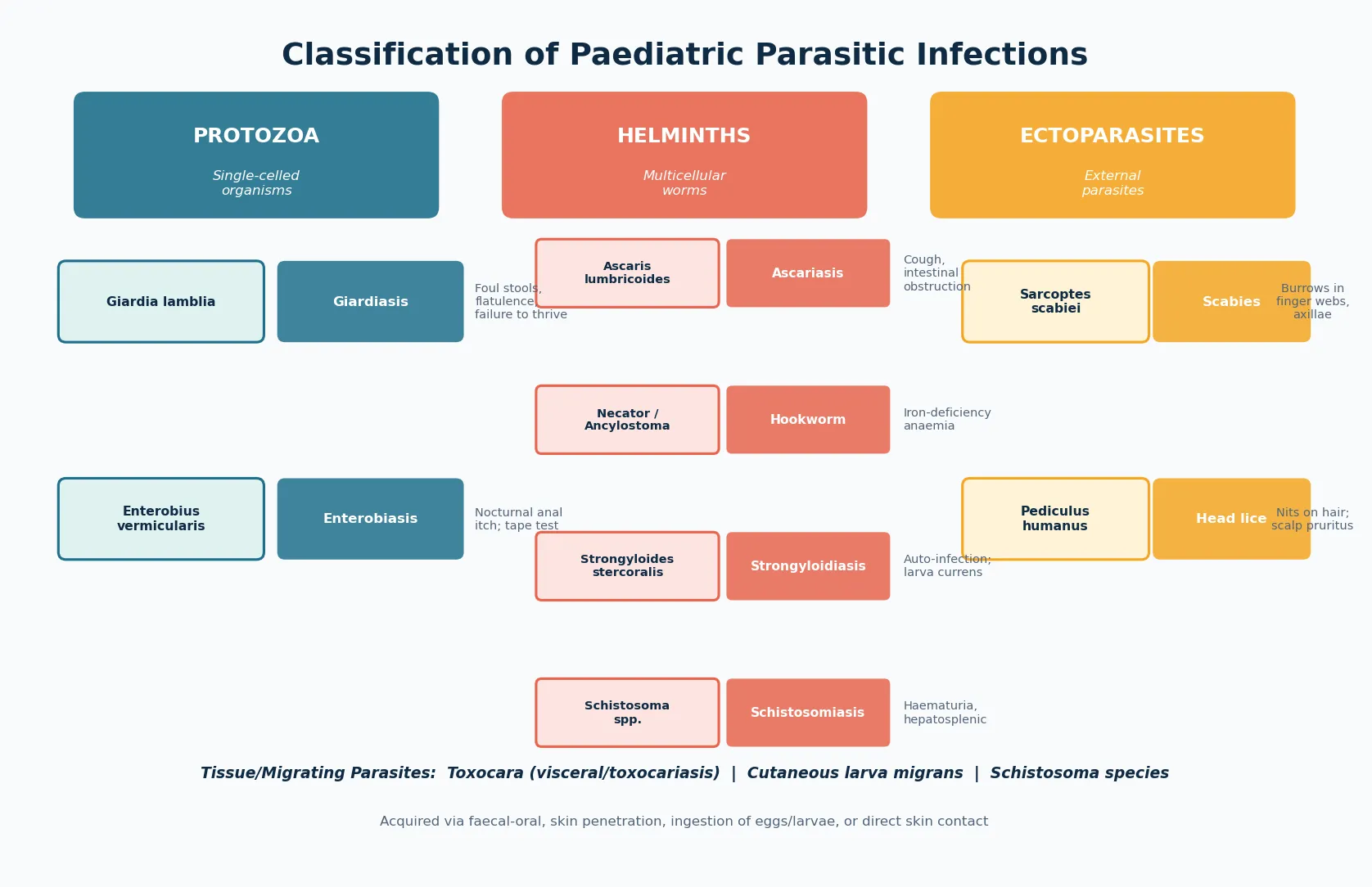
The most useful clinical classification groups parasites by organism type and route of acquisition, because these two factors determine both the presenting syndrome and the diagnostic approach. Protozoa are acquired faecal-orally and present with diarrhoea and malabsorption. Soil-transmitted helminths are acquired by ingesting eggs from contaminated soil or by larval skin penetration, and they present with abdominal symptoms, anaemia, or migration phenomena. Ectoparasites are acquired by direct skin-to-skin or fomite contact and present with intense pruritus and characteristic skin or scalp findings. [1]
The helminths themselves divide into those that complete their life cycle in the intestinal lumen and those that migrate through tissues. Ascaris lumbricoides, the large roundworm, ingested as eggs, undergoes a hepatopulmonary migration loop, is coughed up and swallowed, and matures in the small intestine. Hookworm and Strongyloides larvae penetrate intact skin, travel through the lungs, and settle in the gut, but Strongyloides uniquely can complete its entire cycle internally through auto-infection, allowing it to persist for decades. Enterobius vermicularis, the pinworm, lives in the caecum and lays eggs on the perianal skin at night, causing intense anal pruritus. [2]
[1] [5]Epidemiology & Risk Factors
Soil-transmitted helminths infect well over a billion people globally, with the heaviest burden in children in tropical and subtropical regions where sanitation is limited. Ascaris, hookworm, and Trichuris trichiura together cause malnutrition, growth faltering, cognitive impairment, and iron-deficiency anaemia in children. Mass drug administration programmes with albendazole or mebendazole in endemic countries have reduced prevalence, but reinfection is rapid when sanitation and clean water remain inadequate. [1]
Giardiasis is the most common intestinal parasitic infection in the developed world and a frequent cause of travellers diarrhoea and waterborne outbreaks in childcare centres. Children under five carry the highest prevalence because of faecal-oral spread in diapers, shared toys, and inadequate handwashing. Day-care attendance, untreated drinking or swimming water, and household contact with an infected person are the dominant risk factors in Australia and New Zealand. [3]
Scabies affects an estimated two hundred million people globally at any time, and children in crowded conditions are the most affected. In remote Australian Indigenous communities, scabies prevalence in children has historically exceeded fifty per cent, and the resulting streptococcal skin infection drives the high rates of acute rheumatic fever and rheumatic heart disease. Head lice are nearly universal in primary school children wherever children congregate, with outbreaks managed through school-based policies rather than individual treatment alone. [5]
The dominant risk factors are environmental and behavioural. Oral exploration and geophagia in toddlers, playing in soil or sandpits contaminated by dog or cat faeces, walking barefoot on contaminated ground, close bodily contact in crowded housing, childcare and school attendance, untreated water, and travel to or migration from endemic regions all increase risk. Children who are immunocompromised, on corticosteroids, or malnourished face greater severity, and Strongyloides in particular can become life-threatening in these groups. [2]
Pathophysiology
The pathophysiology of parasitic infections follows the route of acquisition, the life cycle within the host, and the immune response mounted against the organism. Giardia lamblia cysts are ingested in contaminated water or food, excyst in the small intestine, and adhere to the duodenal and jejunal mucosa through a ventral sucking disc. The trophozoites do not invade the tissue, but their blanket adherence disrupts the brush border, impairs disaccharidase activity, and causes malabsorption of fat and fat-soluble vitamins, producing the foul-smelling, greasy stools and flatulence that are the clinical signature. [3]
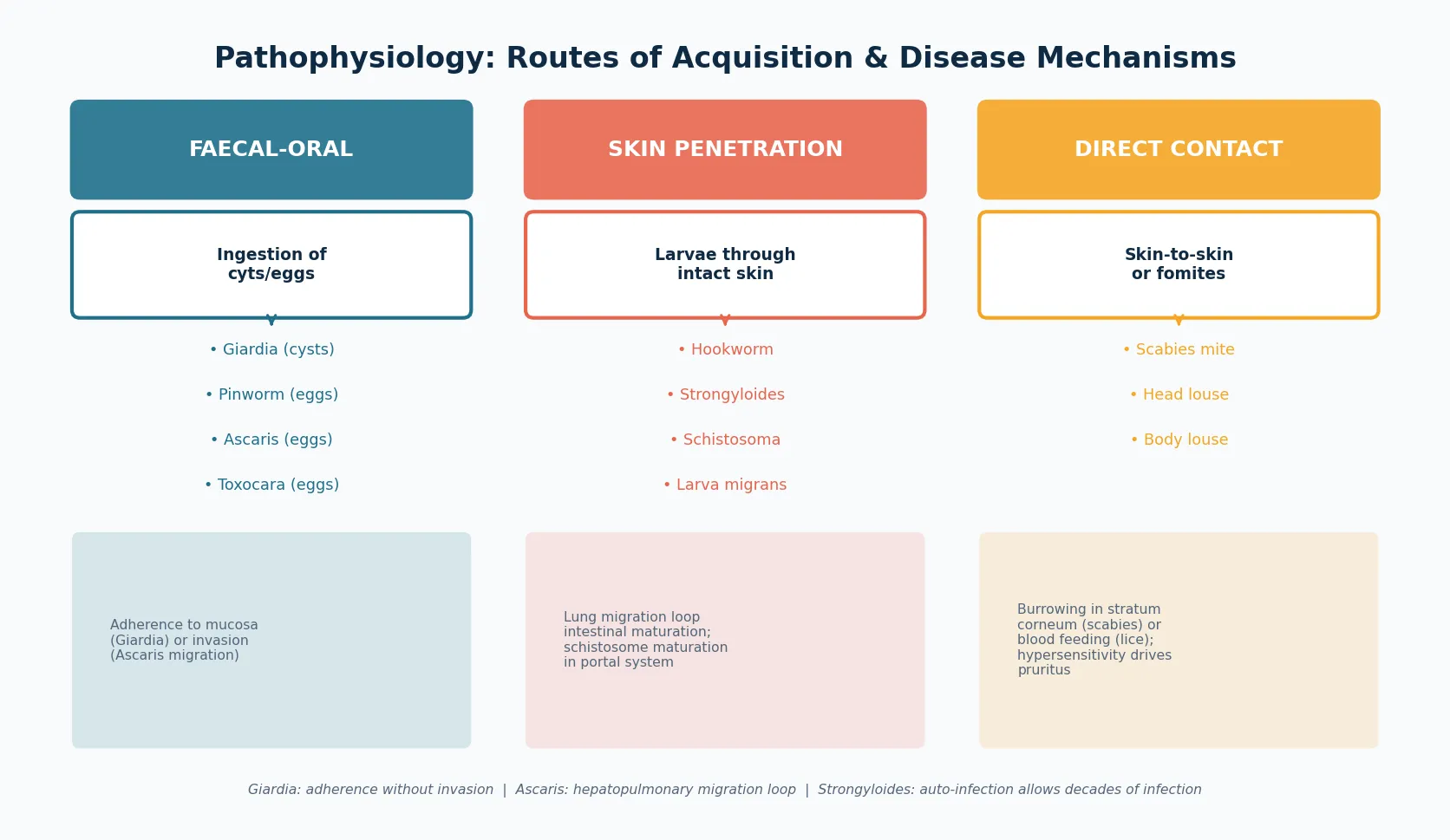
Soil-transmitted helminths follow more complex life cycles that determine their clinical features. Ascaris eggs hatch in the small intestine, and larvae penetrate the intestinal wall, travel via the bloodstream to the liver and then the lungs, ascend the airways, and are swallowed back into the intestine where they mature into adult worms. The pulmonary migration phase can cause a transient cough, wheeze, and eosinophilic pneumonitis known as Loeffler syndrome, while heavy adult worm burdens can cause intestinal obstruction or biliary obstruction. Hookworm and Strongyloides larvae penetrate intact skin, usually through the feet, and follow the same hepatopulmonary loop before settling in the small intestine, where hookworm feeds on blood and causes iron-deficiency anaemia. [2]
The unique and dangerous feature of Strongyloides stercoralis is auto-infection. Larvae produced in the intestine can develop into infective filariform larvae within the gut lumen, penetrate the intestinal wall or perianal skin, and repeat the migration cycle without leaving the host. This allows infection to persist for decades after the original exposure, and it explains why immunosuppression, particularly with corticosteroids, can trigger explosive hyperinfection with larvae disseminating to every organ, carrying enteric bacteria and causing Gram-negative sepsis. This auto-infection cycle is the single most important parasitological concept for the fellowship exam. [11]
Toxocara species, the roundworms of dogs and cats, follow a dead-end pathway in children. Eggs ingested from soil contaminated by animal faeces hatch in the intestine, and larvae penetrate the wall and migrate through tissues, most commonly the liver, lungs, and eye, provoking an intense eosinophilic inflammatory response known as visceral larva migrans. Because the larvae cannot complete their life cycle in a human host, they wander through tissues for months, causing fever, hepatomegaly, wheeze, and, when the retina is involved, ocular toxocariasis that can mimic retinoblastoma. [8]
Schistosoma species, acquired when cercariae in freshwater penetrate the skin during swimming or wading, mature in the portal venous system and migrate to the mesenteric or bladder venules, where adults lay eggs that lodge in tissues and provoke granulomatous inflammation. The species determines the clinical syndrome: Schistosoma haematobium causes urinary schistosomiasis with haematuria and eventual bladder cancer, while Schistosoma mansoni and japonicum cause intestinal and hepatosplenic disease with portal hypertension. [10]
Ectoparasites cause disease through mechanical disruption and hypersensitivity. The scabies mite burrows into the stratum corneum, lays eggs, and triggers a type four hypersensitivity response to mite products that produces intense pruritus, worse at night. The head louse feeds on blood from the scalp, and the immune response to louse saliva drives pruritus and excoriation. In crusted scabies, an inadequate cellular immune response allows millions of mites to proliferate, producing hyperkeratotic crusts that are extraordinarily infectious. [6]
Clinical Presentation
Giardiasis presents with chronic diarrhoea that is typically foul-smelling, greasy, and bulky, accompanied by abdominal cramps, bloating, flatulence, and weight loss or failure to thrive. Acute symptoms begin one to two weeks after exposure, but the infection often becomes chronic, and the child may present with weeks of loose stools and faltering growth before the diagnosis is considered. Vomiting and fever are less prominent than in bacterial enteritis, and the absence of blood or mucus in the stool helps distinguish giardiasis from invasive bacterial diarrhoea. [3]
Enterobiasis, or pinworm, presents with nocturnal anal pruritus, restlessness, and sleep disturbance in an otherwise well child. The adult female worm migrates from the caecum to the perianal skin at night to lay eggs, and the child scratches, reinfects via the oral route, and spreads eggs to bedding and household contacts. Vulvovaginitis in young girls can result from worm migration, and rarely appendicitis or mesenteric adenitis can be associated, but the vast majority present simply with anal itch in a well child. [4]
Ascariasis is frequently asymptomatic, but heavy infections cause abdominal pain, distension, and, in the migration phase, a transient cough, wheeze, and low-grade fever with eosinophilia. Rare but important complications include intestinal obstruction from a bolus of worms, biliary obstruction with jaundice, and pancreatitis. A worm may be passed in the stool or vomited, which is understandably distressing to the family and often the trigger for presentation. [2]
Hookworm infection is insidious and presents with the consequences of chronic occult blood loss: pallor, fatigue, poor exercise tolerance, and, in children, growth faltering and impaired cognitive development. The ground itch of larval skin penetration may be recalled, and a peripheral blood count reveals a microcytic, hypochromic anaemia with eosinophilia. Strongyloidiasis is often asymptomatic or causes vague abdominal pain, diarrhoea, and intermittent larva currens, a rapidly migrating urticarial skin track, but the critical presentation is hyperinfection in the immunosuppressed child with fever, sepsis, pneumonia, and Gram-negative shock. [9]
Clinical clues that should trigger parasite testing
Chronic foul-smelling diarrhoea with flatulence and weight loss: consider Giardia antigen
Nocturnal anal pruritus in a well child: perform a perianal tape test for pinworm
Iron-deficiency anaemia with eosinophilia in a child from or travelled to an endemic area: stool microscopy for hookworm
Toddler with hepatosplenomegaly, eosinophilia, and wheeze after soil exposure: Toxocara serology
Intense nocturnal pruritus with burrows in finger webs and a household contact: scabies
Returned traveller with haematuria or hepatosplenic disease and eosinophilia: schistosomiasis serology
Toxocariasis presents in two distinct patterns. Visceral larva migrans occurs in young children, typically aged one to four years, and causes fever, hepatosplenomegaly, cough, wheeze, and a striking eosinophilia. Ocular toxocariasis presents in older children with unilateral visual impairment, strabismus, or a leukocoria from a retinal granuloma, and it must be distinguished from retinoblastoma to avoid unnecessary enucleation. Schistosomiasis presents acutely with Katayama fever, a serum-sickness-like illness with fever, urticaria, and eosinophilia weeks after freshwater exposure, or chronically with haematuria, dysuria, abdominal pain, and hepatosplenomegaly. [8]
Scabies presents with intense pruritus that is worse at night and after hot showers, with characteristic burrows in the finger webs, flexor surfaces of the wrists, axillae, waist, and genitalia. In infants and young children, the palms, soles, head, and neck are commonly involved, unlike in adults. Household contacts frequently have the same rash. Crusted scabies presents with thick, scaly, hyperkeratotic plaques over the extremities and trunk, often in children with Down syndrome, immunocompromise, or disability, and the child is highly infectious. Head lice present with scalp pruritus, excoriation, cervical lymphadenopathy, and visible nits attached to the hair shaft. [5]
Differential Diagnosis
The differential diagnosis of chronic diarrhoea in a child is broad, and giardiasis sits alongside coeliac disease, cow's milk protein allergy, chronic non-specific diarrhoea of childhood, irritable bowel syndrome, inflammatory bowel disease, lactose intolerance, and cystic fibrosis. The foul-smelling, greasy quality of the stool, the presence of flatulence and bloating, and the exposure history to untreated water or a childcare outbreak point toward Giardia, and the stool antigen test is diagnostic. [3]
The differential of iron-deficiency anaemia includes dietary deficiency, malabsorption from coeliac disease, and occult blood loss from a Meckel diverticulum or inflammatory bowel disease. Hookworm should be considered in any child from or travelled to an endemic area, and stool microscopy for ova is a simple, cheap test that is often omitted. The presence of eosinophilia alongside the anaemia is a strong pointer toward a helminth cause. [9]
The differential of eosinophilia itself is important, because a high eosinophil count in a child is a clue to tissue helminth migration. Toxocariasis, Strongyloides, schistosomiasis, hookworm, and filarial infections all cause eosinophilia, while protozoal infections like Giardia typically do not. Non-parasitic causes include allergic disease, drug reactions, hypereosinophilic syndrome, and some malignancies, but in a child with relevant exposure, parasitic causes must be excluded first. [8]
The differential of a generalised pruritic rash includes eczema, contact dermatitis, atopic dermatitis, drug eruption, and viral exanthems, and scabies is frequently misdiagnosed as eczema, particularly in children who already have an atopic tendency. The keys to scabies are the distribution in finger webs, wrists, and axillae, the worsening at night, and the presence of a household contact with itch. The differential of scalp pruritus includes seborrhoeic dermatitis, atopic dermatitis of the scalp, and tinea capitis, and head lice is confirmed by finding live lice or viable nits. [5]
Clinical & Bedside Assessment
Begin every assessment with an overall judgement of how well the child is, because most parasitic infections present in a well child and the priority is diagnostic clarity rather than resuscitation. A child who is febrile, toxic, or in shock is not presenting with uncomplicated giardiasis or pinworm, and the clinician should consider a complication such as Strongyloides hyperinfection, intestinal obstruction from Ascaris, or invasive bacterial co-infection. Measure temperature, heart rate, respiratory rate, blood pressure, and weight, and plot the weight to assess growth faltering. [1]
Take a focused exposure history that covers the key routes of parasite acquisition. Ask about water sources, including untreated drinking water, swimming or camping water, and travel to areas with unsafe water. Ask about soil exposure, including playing in dirt or sandpits, geophagia, walking barefoot, and contact with dogs and cats whose faeces may contaminate play areas. Ask about childcare or school attendance and outbreaks, household contacts with similar symptoms, and recent travel or migration from tropical regions. The history of a child with a pruritic rash must include close contacts and the timing and distribution of the itch. [3]
Perform a focused abdominal examination, palpating for tenderness, distension, and hepatosplenomegaly. Examine the perianal area for excoriation and, if pinworm is suspected, apply clear adhesive tape to the perianal skin first thing in the morning and examine it microscopically for eggs. Examine the skin thoroughly for the burrows of scabies, the creeping tracks of cutaneous larva migrans, and the urticarial rash of strongyloidiasis. Check the scalp for nits and live lice, and palpate for cervical lymphadenopathy. [5]
In the returned traveller or recently arrived refugee, take a structured travel history covering the countries and regions visited, the dates relative to symptom onset, the activities undertaken including freshwater exposure, and the preventive measures used. This history drives the diagnostic pathway: freshwater swimming in Africa points to schistosomiasis, barefoot walking in the tropics points to hookworm and Strongyloides, and soil exposure from dog faeces points to toxocariasis. Newly arrived refugees should have routine screening stool microscopy and Strongyloides serology as part of their arrival health assessment. [11]
Investigations
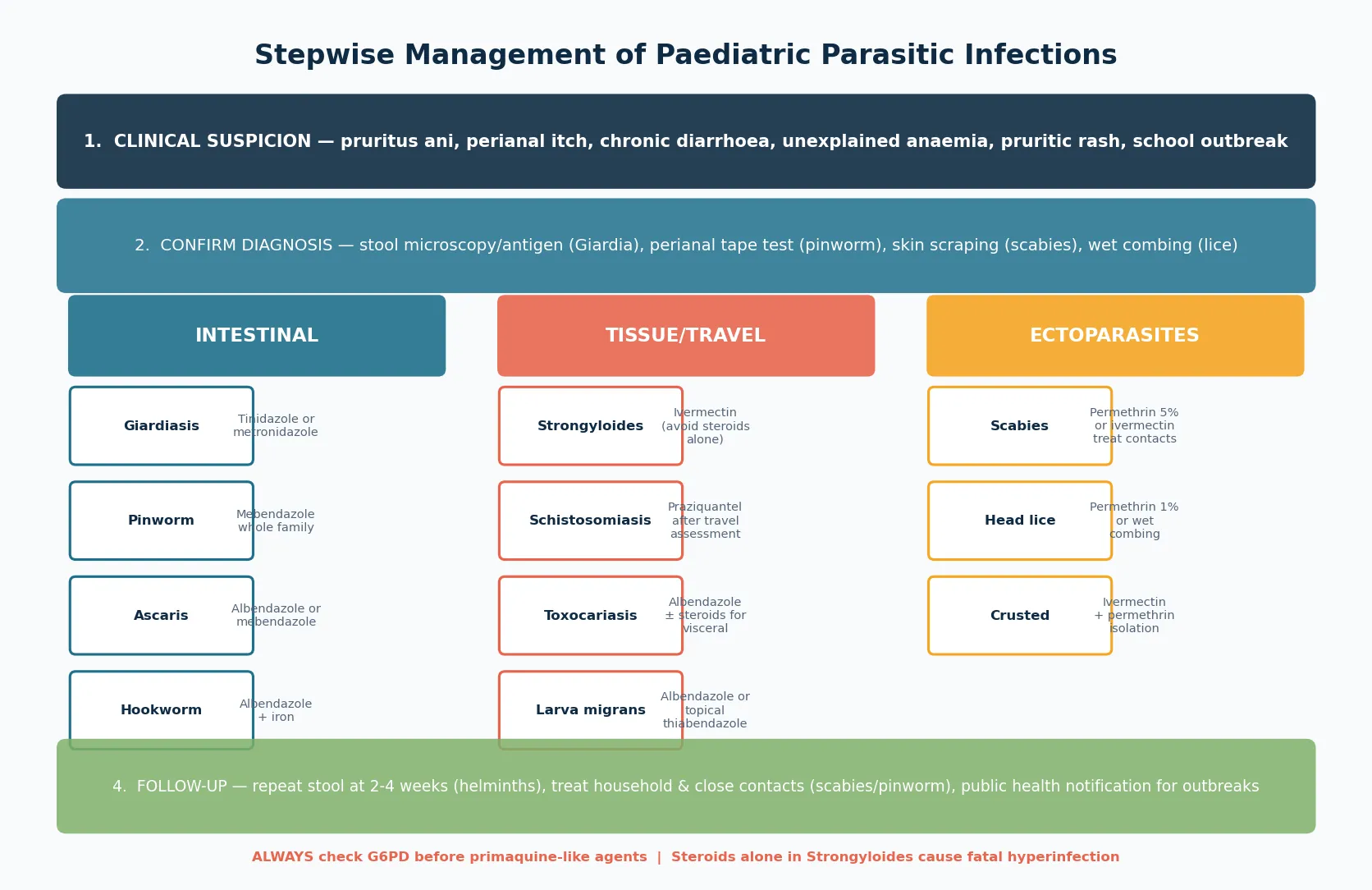
The diagnostic approach to parasitic infection is organism-specific, and the clinician must request the correct test for the organism the history suggests. Giardiasis is best diagnosed by a stool antigen test, which is more sensitive and specific than microscopy and does not require the multiple samples that microscopy does. A single stool antigen test detects over ninety per cent of infections, while routine stool culture does not detect Giardia at all. [3]
Stool microscopy for ova, cysts, and parasites remains the workhorse for intestinal helminths, including Ascaris, hookworm, and Trichuris. A single stool sample may miss light infections, and three samples collected on separate days improve sensitivity. Enterobius is diagnosed by the perianal tape test rather than stool microscopy, because the eggs are laid on the perianal skin and are rarely present in stool. The tape is pressed onto the perianal skin in the morning before bathing, mounted on a slide, and examined for the characteristic asymmetric eggs. [4]
Strongyloidiasis is difficult to diagnose by stool microscopy because larval output is low and intermittent. Serology is the preferred screening test, with a sensitivity of approximately ninety per cent, and it is the test to request before immunosuppression in any child with relevant exposure. Toxocariasis is diagnosed by serology in the context of a compatible clinical picture with eosinophilia, and imaging of the liver or eye supports the diagnosis. Schistosomiasis is diagnosed by microscopy of urine or stool for eggs, depending on the species, with serology useful for returned travellers who may have light infections. [10]
A full blood count is essential in any child with suspected helminth infection, because eosinophilia is a hallmark of tissue migration. Eosinophilia is expected in Toxocara, Strongyloides, hookworm, and schistosomiasis, but it is characteristically absent in Giardia and pinworm. Iron studies confirm the iron-deficiency anaemia of hookworm, and liver function tests may be mildly abnormal in visceral toxocariasis and schistosomiasis. In scabies and head lice, the diagnosis is clinical, with a skin scraping or wet combing providing confirmation when needed. [8]
Management — Resuscitation
Most paediatric parasitic infections present in a well child and do not require resuscitation, but the clinician must recognise the situations that do. A child with severe anaemia from hookworm may present with pallor, tachycardia, and a flow murmur, and needs assessment for transfusion alongside antiparasitic therapy and iron replacement. A child with intestinal obstruction from a heavy Ascaris burden may present with abdominal distension, vomiting, and colicky pain, and requires surgical assessment, fluid resuscitation, and nasogastric decompression. [2]
The most time-critical resuscitation scenario is Strongyloides hyperinfection in the immunosuppressed child. This child presents with fever, septic shock, pneumonia, and Gram-negative bacteraemia or meningitis, as migrating larvae carry enteric bacteria through the gut wall. Management requires intravenous fluids and broad-spectrum antibiotics for the bacterial sepsis, urgent stool and sputum examination for larvae, and treatment with ivermectin, often with a prolonged course, alongside reduction of immunosuppression where possible. The mortality is high, and early recognition of the syndrome in a child on steroids with a tropical exposure history is the only way to improve outcome. [11]
Resuscitation sequence for severe parasitic presentations
Assess airway, breathing, circulation for any child who is toxic or in shock
Treat severe hookworm anaemia with transfusion if haemodynamically unstable, then iron and albendazole
Recognise Ascaris intestinal obstruction: nasogastric decompression, fluids, surgical consult
Suspect Strongyloides hyperinfection in any immunosuppressed child with sepsis and tropical exposure: start ivermectin and broad antibiotics
Arrange admission and paediatric infectious disease input for complex or severe presentations
A child with crusted scabies may need admission for isolation and intensive treatment because of the extreme infectivity, and any child with a parasitic infection and severe malnutrition or growth faltering needs nutritional rehabilitation alongside antiparasitic therapy, because the infection and the undernutrition compound each other. [6]
Management — Definitive & Stepwise
Giardiasis is treated with tinidazole as a single dose or metronidazole for five to seven days, both of which are highly effective. The meta-analysis of nitroimidazole compounds in children confirmed excellent cure rates, and treatment of household contacts and childcare contacts is indicated in outbreak settings. Children with persistent symptoms after treatment should be re-evaluated for reinfection, treatment failure, or an alternative diagnosis, and a second course with a different agent may be needed. [12]
Enterobiasis is treated with a single dose of mebendazole, repeated after two weeks to kill worms hatched from eggs laid since the first dose. Because eggs are ubiquitous in the household environment and auto-infection is the rule, the entire household should be treated simultaneously, regardless of symptoms. Concurrent measures include washing bed linen and nightclothes in hot water, trimming fingernails, and encouraging handwashing, though the drug treatment is the mainstay. Albendazole is an alternative. [4]
Ascariasis, hookworm, and Trichuris are all treated with albendazole or mebendazole as a single dose or short course, which kills the adult worms and interrupts egg deposition. Hookworm-associated iron-deficiency anaemia additionally requires iron replacement for several months to replete stores. Periodic deworming in endemic populations is recommended by the World Health Organization as a public health measure, and mass drug administration programmes with albendazole or mebendazole have reduced the global burden of soil-transmitted helminths. [1]
Mebendazole / Albendazole / Tinidazole / Ivermectin / Permethrin
Dose
Mebendazole 100 mg PO once (pinworm; repeat in 2 wk); Albendazole 400 mg PO once (STH); Tinidazole 50 mg/kg PO once (Giardia); Ivermectin 200 mcg/kg PO x1-2 days (Strongyloides); Permethrin 5% cream apply overnight (scabies)
Strongyloidiasis is treated with ivermectin, which is more effective than albendazole and is the drug of choice. A two-day course of ivermectin achieves high cure rates for chronic infection, and hyperinfection requires a longer course until larvae are cleared. Albendazole is less effective but is an alternative when ivermectin is unavailable. The essential principle is that Strongyloides must be found and treated before any immunosuppression is given, because the consequences of untreated hyperinfection are catastrophic. [11]
Toxocariasis is treated with albendazole for five days for visceral larva migrans, with the addition of corticosteroids when there is significant organ inflammation, cardiac, or central nervous system involvement. Ocular toxocariasis is managed in collaboration with ophthalmology, because systemic anthelmintic therapy may not reach intraocular larvae, and intraocular inflammation may worsen with parasite death. Schistosomiasis is treated with praziquantel, which is highly effective against all species, and corticosteroids are added for acute Katayama syndrome to suppress the hypersensitivity response. [8]
Antiparasitic by organism class
Scabies is treated with permethrin five per cent cream applied to the entire body from the neck down and washed off after eight to fourteen hours, with a repeat application after one to two weeks. Oral ivermectin is an alternative for crusted scabies, immunocompromised children, or when topical therapy fails. The critical management principle is that all household and close contacts must be treated simultaneously, regardless of symptoms, because asymptomatic carriers perpetuate the cycle. Bedding and clothing should be washed in hot water or bagged for several days. Crusted scabies requires isolation, oral ivermectin combined with topical permethrin, and prolonged treatment. [5]
Head lice are treated with a topical pediculicide such as permethrin one per cent or a dimeticone-based product, applied according to the product schedule and repeated after seven to ten days to kill nymphs hatched from surviving eggs. Wet combing with a fine-toothed nit comb every three to four days for two weeks is a non-chemical alternative that is effective when done thoroughly. Treatment failure is most often reinfestation from an untreated contact rather than true resistance, and the whole family should be checked. Children do not need to be excluded from school after the first treatment. [7]
Specific Subtypes & Scenarios
Giardiasis in the childcare setting is a common outbreak scenario that requires public health involvement and concurrent treatment of affected children and staff. The cysts are resistant to standard chlorination of water, which is why waterborne outbreaks from swimming pools and untreated drinking water occur, and hand hygiene is the mainstay of prevention. Children with selective immunoglobulin A deficiency or common variable immunodeficiency are particularly susceptible to chronic giardiasis and should be considered when the infection is persistent or recurrent. [3]
The returned traveller with possible schistosomiasis is a scenario that demands a structured approach. Ask specifically about freshwater exposure in Africa, the Middle East, or Southeast Asia, including swimming, wading, or rafting in lakes and rivers. Schistosoma haematobium causes haematuria and dysuria, while the intestinal species cause abdominal pain and hepatosplenomegaly. Serology is the most useful initial test in returned travellers, and praziquantel is the treatment. The long-term consequence of untreated infection is portal hypertension or bladder cancer, which is why diagnosis and treatment matter even when the child is asymptomatic. [10]
Visceral toxocariasis in a toddler is a frequently missed diagnosis because the clinical picture of fever, hepatomegaly, wheeze, and eosinophilia mimics many other conditions. The key is the exposure to puppies or soil contaminated by dog faeces, and the finding of a marked eosinophilia on the blood count. The condition is generally benign and self-limiting, but albendazole accelerates recovery, and corticosteroids are added when there is significant organ involvement. Ocular toxocariasis is an emergency because of the risk of permanent vision loss, and any child with unilateral visual symptoms and a retinal lesion must be referred to ophthalmology urgently to distinguish it from retinoblastoma. [8]
Cutaneous larva migrans, the creeping eruption, presents as a intensely itchy, serpiginous, migrating skin track acquired when a child walks or sits bare-skinned on sand or soil contaminated by dog or cat hookworm larvae. The track advances one to two centimetres per day, and the diagnosis is clinical. Treatment is with oral albendazole, oral ivermectin, or topical thiabendazole, and the condition resolves without treatment over weeks to months, though the pruritus is severe and treatment is preferred. [8]
[1]Complications & Pitfalls
The complications of untreated parasitic infection are predominantly those of chronicity rather than acute severity. Hookworm causes iron-deficiency anaemia that impairs growth, cognition, and exercise tolerance, and in severe cases cardiac failure. Chronic giardiasis causes malabsorption and failure to thrive, and Ascaris can cause intestinal or biliary obstruction requiring surgery. Untreated schistosomiasis causes portal hypertension with variceal bleeding, or bladder cancer decades later. These long-term complications are why early diagnosis and treatment matter even in an asymptomatic child. [2]
The most dangerous complication of any paediatric parasitic infection is Strongyloides hyperinfection syndrome, which occurs when immunosuppression allows the auto-infection cycle to accelerate. The child develops pneumonia, Gram-negative septicaemia, meningitis, and shock, and the mortality without treatment approaches one hundred per cent. Even with treatment the mortality remains high, which is why the emphasis must be on prevention through screening and treatment before immunosuppression. Any child from a tropical area who is to receive corticosteroids for any reason, including asthma exacerbations and autoimmune disease, should be screened first. [11]
The major clinical pitfalls are failing to think of a parasitic diagnosis, requesting the wrong test, and not treating the household. Giardiasis is missed because routine stool culture does not detect it, and the specific antigen test must be requested. Pinworm recurs because only the symptomatic child is treated while the asymptomatic household carriers reinfect. Scabies persists because contacts are not treated simultaneously. Strongyloides is missed because the clinician did not ask about past tropical residence before prescribing steroids. Each of these errors is common, and each is preventable. [1]
Prognosis & Disposition
The prognosis of treated parasitic infection is excellent for the great majority of children. Giardiasis resolves within days of tinidazole or metronidazole, and enterobiasis clears after the two-dose mebendazole course with household treatment. Soil-transmitted helminths respond to a single dose of albendazole or mebendazole, and the iron-deficiency anaemia of hookworm recovers with iron supplementation over months. Scabies and head lice resolve with correct topical therapy and contact treatment, though reinfestation from untreated contacts is the most common reason for apparent treatment failure. [1]
The prognosis is determined by the duration of infection before treatment and by whether complications have developed. A child with chronic hookworm anaemia may have irreversible cognitive effects from prolonged iron deficiency, and a child with untreated schistosomiasis faces the long-term risk of portal hypertension or bladder cancer. This is why screening of at-risk groups, including refugees, migrants, and children in remote Indigenous communities, is an essential part of preventive paediatrics. [10]
Disposition from hospital is straightforward for most parasitic infections, because the treatment is oral or topical and the child is managed in the community. Admission is indicated for Strongyloides hyperinfection, severe hookworm anaemia requiring transfusion, intestinal obstruction from Ascaris, crusted scabies requiring isolation and intensive treatment, and any child with significant malnutrition or systemic illness. Follow-up stool examination at two to four weeks confirms clearance of helminths, and Strongyloides serology should be checked at intervals after treatment to confirm cure. [11]
Special Populations
Newly arrived refugees and migrant children should undergo routine screening for parasitic infection as part of their arrival health assessment. Stool microscopy for ova, cysts, and parasites, Strongyloides serology, schistosomiasis serology for children from endemic regions, and a full blood count for eosinophilia and anaemia are standard components. Treatment of detected infections prevents long-term complications and is a quality marker of refugee health care. [11]
Children in remote Indigenous communities in Australia carry a disproportionate burden of scabies and streptococcal skin infection, and the link between scabies, group A streptococcal pyoderma, acute post-streptococcal glomerulonephritis, and acute rheumatic fever is one of the most important parasitic connections in Australian paediatrics. Community-based scabies control programmes, including mass drug administration with ivermectin or permethrin, have reduced prevalence and the burden of downstream streptococcal disease. Crusted scabies in these communities is a severe, recurrent condition requiring aggressive treatment and public health management. [6]
Immunocompromised children are uniquely vulnerable to Strongyloides hyperinfection, and the screening and treatment of at-risk children before transplantation, chemotherapy, or biologic therapy is essential. Children on long-term corticosteroids for nephrotic syndrome, inflammatory bowel disease, or autoimmune conditions who have tropical exposure must be screened. Selective immunoglobulin A deficiency and common variable immunodeficiency predispose to chronic giardiasis, and these children should be tested for Giardia when they present with chronic diarrhoea. [11]
[1]Evidence, Guidelines & Regional Differences
The World Health Organization guidelines on soil-transmitted helminths recommend periodic preventive chemotherapy with albendazole or mebendazole for preschool and school-age children in endemic areas, delivered through schools and child health days. This strategy is based on evidence that periodic deworming reduces worm burden, improves haemoglobin and growth, and reduces school absenteeism, though the magnitude of cognitive benefit remains debated. [1]
The evidence for ivermectin over albendazole in strongyloidiasis is well established, and ivermectin is the drug of choice for both chronic infection and hyperinfection. For scabies, permethrin five per cent cream remains first-line for typical infection, with oral ivermectin reserved for crusted scabies, immunocompromised patients, and institutional outbreaks. The systematic review of scabies treatment failure confirms that most apparent failures are reinfestation from untreated contacts rather than drug resistance, which reinforces the importance of simultaneous household treatment. [5]
[1]Two live areas of debate shape contemporary practice. The first is the long-term benefit of community deworming programmes, with some Cochrane reviews questioning the magnitude of developmental and cognitive benefits beyond nutritional improvement, which has led to refinement of the mass drug administration strategy to target high-prevalence communities. The second is the emergence of scabies and head lice resistance to permethrin in some regions, which has driven the development of oral ivermectin for scabies and dimeticone-based and oral therapies for head lice as alternatives to traditional pediculicides. [5]
Exam Pearls
Antiparasitic drug matching
References
- [1]Jourdan PM; Lamberton PHL; Fenwick A; Addiss DG Soil-transmitted helminth infections. Lancet, 2018.PMID 28882382
- [2]Bethony J; Brooker S; Albonico M; Geiger SM; Loukas A; Diemert D; Hotez PJ Soil-transmitted helminth infections: ascariasis, trichuriasis, and hookworm. Lancet, 2006.PMID 16679166
- [3]Leung AKC; Leung AA; Wong AH; Sergi CM; Kam JK Giardiasis: An Overview. Recent Pat Inflamm Allergy Drug Discov, 2019.PMID 31210116
- [4]Leung AKC; Lam JM; Hon KL; Barankin B; Leung AAA Pinworm (Enterobius Vermicularis) Infestation: An Updated Review. Curr Pediatr Rev, 2025.PMID 38288810
- [5]Sunderkötter C; Wohlrab J; Hamm H Scabies: Epidemiology, Diagnosis, and Treatment. Dtsch Arztebl Int, 2021.PMID 34615594
- [6]Fernando DD; Mounsey KE; McCarthy JS Scabies. Nat Rev Dis Primers, 2024.PMID 39362885
- [7]Leung AK; Fong JH; Pinto-Rojas A Pediculosis capitis. J Pediatr Health Care, 2005.PMID 16286223
- [8]Ma G; Holland CV; Wang T; Hofmann A; Fan CK; Maizels RM; Hotez PJ; Gasser RB Human toxocariasis. Lancet Infect Dis, 2018.PMID 28781085
- [9]Loukas A; Hotez PJ; Diemert D; Yazdanbakhsh M; McCarthy JS; Correa-Oliveira R; Croese J; Bethony JM Hookworm infection. Nat Rev Dis Primers, 2016.PMID 27929101
- [10]Colley DG; Bustinduy AL; Secor WE; King CH Human schistosomiasis. Lancet, 2014.PMID 24698483
- [11]Buonfrate D; Bradbury RS; Gobbo F; Sequi M; Esposto AD; Giorli G; Torresi J; Oskam L; Krolewiecki A; Bisoffi Z Human strongyloidiasis: complexities and pathways forward. Clin Microbiol Rev, 2023.PMID 37937980
- [12]Escobedo AA; Almirall P; Alfonso M; Pitueles P; Teran G; Cordovi RA; Nunez FA Efficacy of 5-nitroimidazole compounds for giardiasis in Cuban children: systematic review and meta-analysis. Infez Med, 2019.PMID 30882380