Paeds · infectious-diseases
Pertussis
Also known as Whooping cough · Bordetella pertussis infection · 100-day cough · Pertussis (infant apnoea presentation) · Cough illness due to Bordetella pertussis
Fellowship topic on pertussis (whooping cough) in children: the Bordetella pertussis organism and its toxin-mediated, ciliary-paralysing pathophysiology; the classic catarrhal-paroxysmal-convalescent course in older children and the atypical, life-threatening infant presentation dominated by apnoea; the differential of prolonged cough and of infant apnoea; PCR and serology interpreted by age and duration; stepwise management from PICU support of the young infant through macrolide treatment, isolation, exclusion, notification and contact chemoprophylaxis; the complications (pneumonia, seizures, encephalopathy, apnoea); the DTaP/Tdap, maternal-Tdap and cocoon prevention strategy; waning acellular-vaccine immunity and the resurgence problem; special populations (infants, pregnant women, unvaccinated communities, immunocompromised, Indigenous, rural and refugee children); and ANZ/UK/US/Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The three stages — and why the third one tests you
Overview & Definition
Picture a four-month-old brought to the emergency department after a coughing turn at home in which the mother thought the baby had stopped breathing. The baby is now pink and feeding, but the mother has had a chronic cough for three weeks. There is no whoop here, no classic paroxysm to anchor the diagnosis — yet this is exactly how infant pertussis presents, and it is exactly the presentation that kills. Recognising it early turns a preventable death into a survivable illness. [8] [1]
Pertussis, or whooping cough, is an acute infection of the respiratory tract caused by the Gram-negative coccobacillus Bordetella pertussis, spread by respiratory droplets. In an older immunised child it produces the familiar paroxysmal cough with an inspiratory whoop; in a young infant it may produce nothing more than apnoea. The disease is vaccine-preventable, yet it remains endemic worldwide because immunity — whether from vaccination or from natural infection — wanes over time. [1] [3]
The clinician's job has two halves. The acute half is to recognise the sick infant, support breathing, start a macrolide, and prevent spread through isolation, notification and contact prophylaxis. The preventive half is to deliver the immunisation programme — maternal Tdap in every pregnancy, the childhood DTaP series, the adolescent booster, and cocooning of household contacts — because the infant who never reaches the hospital is the infant the programme has protected. [8] [1]
Classification
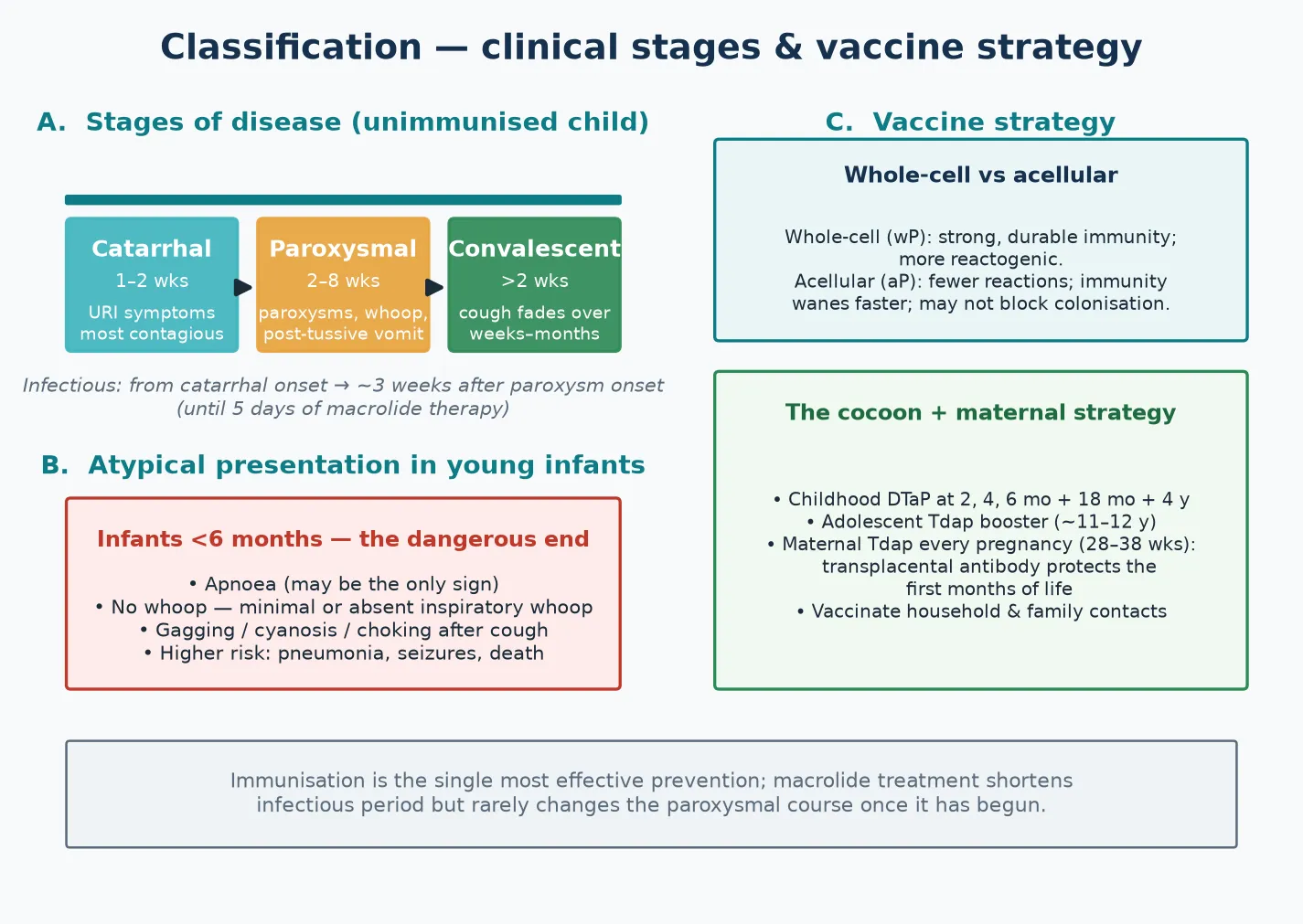
Sort pertussis the way it presents at the bedside — by the stage of the illness, and then by the age of the child, because age changes everything. The classic illness in an older child runs three stages. The catarrhal stage lasts one to two weeks and is indistinguishable from an ordinary viral upper-respiratory infection: rhinorrhoea, low-grade fever and a mild cough. This is when the child is most contagious. The paroxysmal stage follows, lasting two to eight weeks, with explosive runs of coughing that end in the inspiratory whoop and often in post-tussive vomiting. The convalescent stage then sees the cough fade over weeks to months. [1] [3]
The second axis is severity and age. In an older, immunised child the paroxysmal course is unpleasant but rarely dangerous. In an infant under six months the disease is a different beast: apnoea may be the only sign, the whoop is often absent, and the risks of pneumonia, seizures and death are concentrated here. A fellowship answer that classifies only by stage and ignores the age axis misses the point that matters most. [8] [1]
A third distinction, useful in diagnosis and in vaccine science, is between Bordetella pertussis and Bordetella parapertussis. Parapertussis produces a similar but milder cough illness and is not covered by current vaccines, so a vaccinated child with a pertussis-like illness may occasionally have parapertussis instead. For practical management the two are approached the same way, but the distinction explains some "breakthrough" cough illnesses in well-immunised children. [3] [1]
Epidemiology & Risk Factors
Where does pertussis sit, and who does it hurt? The disease remains endemic worldwide, with cyclical epidemics every few years, and the burden falls hardest on the very young. Infants under six months — especially those too young to have completed their primary DTaP series — carry the highest morbidity and mortality, and most pertussis deaths occur in this group. Understanding who is at risk directs both acute care and prevention. [8] [1]
Under-vaccination is the dominant risk factor at the individual level. A child whose parents have declined or delayed vaccination, or who has missed doses through access barriers, has a markedly higher risk of pertussis than a fully vaccinated peer. A case-control study in a large managed-care population found that parental refusal of pertussis vaccination was associated with a substantially increased risk of pertussis infection in the children, a finding that anchors the case for catch-up vaccination and respectful hesitancy response. [5] [1]
The usual source of infant infection is a household or family contact whose own immunity has waned — a parent, sibling or grandparent with a prolonged cough illness. This epidemiological fact is the foundation of two prevention strategies: maternal Tdap, which passes antibody to the infant before birth, and cocooning, which vaccinates the people around the infant. An infant who is too young to be fully vaccinated is protected by the immunity of the people who surround them. [8] [3]
Resurgence is driven by a combination of factors. Immunity after the acellular vaccine wanes faster than after the whole-cell vaccine, so vaccinated adolescents and adults become susceptible again and sustain transmission. Under-vaccinated pockets amplify outbreaks, and improved PCR recognition has raised detection. The result is a disease that did not disappear with the vaccine — it cyclical-resurges, and the response is boosters, the maternal programme, and high coverage. [2] [6]
Pathophysiology
Why does a small Gram-negative coccobacillus produce one of the most violent coughs in medicine? The answer lies in how Bordetella pertussis damages the airway without ever invading deeply. The organism is inhaled in respiratory droplets and adheres to the ciliated epithelium of the nasopharynx and upper airways, using adhesins such as filamentous haemagglutinin, pertactin and fimbriae to anchor itself to the cells whose cilia normally clear secretions. [7] [1]
Having adhered, the organism secretes a set of toxins that do the real damage: pertussis toxin, adenylate cyclase toxin, tracheal cytotoxin and a dermonecrotic toxin. These paralyse the cilia and injure the epithelial cells, so the normal mucociliary escalator stops working. The histopathology of infection in the baboon model — the closest experimental model to human disease — shows precisely this: ciliated epithelium damaged, inflammatory exudate accumulating, and the organism localised to the airway surface rather than invading tissue. [7] [1]
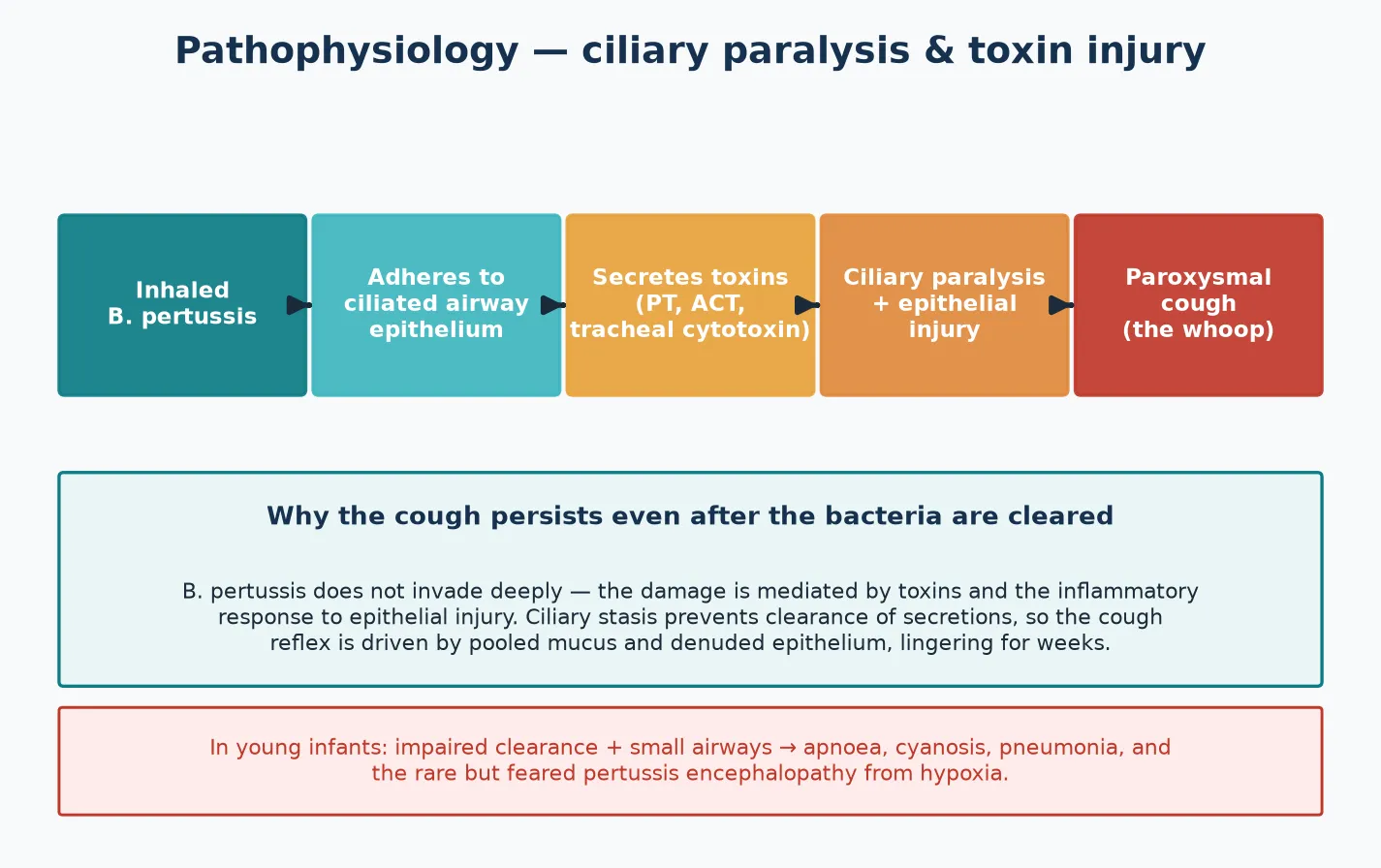
With the cilia paralysed and the epithelium injured, respiratory secretions and debris pool in the airway rather than being cleared. That pooled, irritant material is what drives the explosive paroxysmal cough: the cough reflex fires repeatedly to clear what the cilia can no longer move. This is also why the cough persists for weeks after the bacteria themselves are gone — the injury and inflammation outlast the infection, producing the prolonged convalescent phase that gives pertussis its "hundred-day" reputation. [7] [4]
The infant-specific severity follows from the same mechanism applied to a smaller, less mature system. A young infant has small airways, limited respiratory reserve and an immature immune response. The impaired clearance that produces a prolonged cough in an older child produces apnoea, cyanosis and pneumonia in an infant — and, through hypoxia, the rare but feared pertussis encephalopathy. The biology of the organism is the same; the host turns a nuisance into a threat. [8] [7]
Clinical Presentation
The classic presentation lives in the older child. After a one-to-two-week catarrhal prodrome that looks like any viral cold, the cough changes character: it comes in paroxysms — rapid, consecutive coughs that the child cannot voluntarily stop — ending in a forced inspiration against a narrowed glottis, the whoop, and frequently in vomiting. Between paroxysms the child often looks surprisingly well, which is part of what makes the disease under-recognised. [1] [3]
The infant presentation is the one that must never be missed, and it is the one that does not look like the textbook. An infant under six months may have no whoop at all. Instead, the presentation is dominated by apnoea — which may be the only sign — gagging, choking, cyanotic spells after coughing, and poor feeding. A baby who "stopped breathing" after a cough, or who is feeding poorly with a colour change, with a household cough contact, is pertussis until proven otherwise. This is the presentation that causes the deaths. [8] [1]
In adolescents and adults, including previously vaccinated individuals, the whoop is frequently absent and pertussis presents simply as a prolonged cough illness lasting weeks. Because these individuals often remain functional, they circulate in the community and in households, and they are the reservoir from which infants are infected. A clinician who thinks of pertussis only when the whoop is present will miss most of the transmission. [2] [3]
The complications are part of the presentation because they often bring the child to care. Pneumonia is the commonest serious complication and a leading cause of death, particularly in infants. Seizures and encephalopathy reflect hypoxic injury during severe paroxysms or apnoea. Rib fracture, pneumothorax, hernia and subconjunctival haemorrhage arise from the force of coughing itself. A worsening cough accompanied by fever, respiratory distress, lethargy or a change in conscious state signals a complication that changes the disposition. [1] [8]
Differential Diagnosis
For the older child with a prolonged cough, the differential is broad: viral bronchitis, asthma and asthma exacerbation, mycoplasma pneumonia, foreign-body aspiration, tuberculosis, gastro-oesophageal reflux and upper-airway-cough syndrome all produce cough lasting beyond two weeks. The features that point toward pertussis are the paroxysmal pattern, the whoop, post-tussive vomiting, a nocturnal predominance, and a household contact with a prolonged cough. Asthma is episodic with wheeze and reversibility; mycoplasma is more systemic with fever and malaise; a foreign body is focal and sudden in onset. [1] [3]
For the infant with apnoea or cyanotic spells, the differential is the dangerous one, and pertussis sits firmly within it. Bronchiolitis — especially respiratory syncytial virus — is the commonest mimic in this age group and produces apnoea, wheeze and feeding difficulty. Pneumonia, sepsis, gastro-oesophageal reflux with aspiration, a congenital airway anomaly, and seizures can all present with apnoea or a colour change. The decisive point is that apnoea in an infant without a clear viral cause, or with a household cough contact, should prompt a pertussis test rather than being attributed to a self-limiting virus. [8] [1]
For the adolescent or adult with a prolonged cough, the differential includes chronic post-infectious cough, asthma, gastro-oesophageal reflux, an ACE-inhibitor cough, and smoking-related disease. The duration beyond two to three weeks, a paroxysmal quality, and a known contact or outbreak should keep pertussis on the list even when the whoop is absent — testing this group protects the infants they will otherwise infect. [2] [3]
Clinical & Bedside Assessment
The assessment begins with a focused history built around the cough and its setting. Ask about duration, the paroxysmal pattern, the presence of a whoop, post-tussive vomiting, nocturnal waking, and any apnoea, cyanosis or choking. In an infant, ask explicitly about feeding — how much, how often, and whether feeding triggers cough or colour change. And ask about the household: who has been coughing, for how long, and whether there has been a known pertussis case or outbreak. The contact history is often the clue that swings the diagnosis. [8] [1]
Establish the immunisation status precisely. Record the number of pertussis-containing doses the child has received, with dates, and whether the mother received maternal Tdap in pregnancy. Under-vaccination raises both the likelihood and the severity of disease, and a fully unvaccinated infant with a cough contact is at the highest risk of all. The immunisation history also frames the prevention conversation that follows the acute encounter. [1] [5]
Examine for the red flags that change disposition. Look for apnoea, cyanosis or an acute life-threatening event; for distress or exhaustion after paroxysms; for dehydration from poor feeding or vomiting; and for the signs of pneumonia — fever, tachypnoea, recession, crackles or hypoxia. In the infant, assess work of breathing, oxygenation and feeding tolerance directly, because a young infant can deteriorate quickly between paroxysms that look deceptively mild. [8] [1]
Document the public-health essentials at the bedside, because they drive the response. Record the date of symptom onset, calculate the infectious period, note school or childcare attendance, and begin the list of household and close contacts. These details determine notification, the exclusion period, and who receives chemoprophylaxis. A careful contact list at the first encounter prevents the late, disorganised public-health scramble. [10] [3]
Investigations
PCR is the preferred test early in the illness. A nasopharyngeal aspirate or a flocked nasopharyngeal swab sent for PCR has its highest sensitivity in the first three to four weeks of illness — the catarrhal and early paroxysmal stages — when the organism is present in the airway in greatest numbers. PCR has largely replaced culture for routine diagnosis because it is faster and more sensitive, and it can be combined with respiratory-virus panels when the differential includes bronchiolitis or other viral infections. [1] [8]
Serology takes over when the presentation is late. After two to three weeks of cough, PCR sensitivity falls as the organism is cleared, but the antibody response is strong. A single high-titre anti-pertussis-toxin IgG can support the diagnosis in an adolescent or adult with a prolonged cough, and it is the test that catches the cases PCR misses. The choice between PCR and serology is therefore governed by the duration of illness at the time of presentation — a point an examiner rewards. [1] [2]
In Australia and Aotearoa New Zealand, pertussis is a nationally notifiable disease. PCR on a nasopharyngeal aspirate or swab is the standard diagnostic test in the first few weeks; paired or single high-titre serology is used for the late-presenting prolonged cough. The Australian Immunisation Handbook (ATAGI) and equivalent New Zealand Ministry of Health guidance set the schedule and the public-health response, including exclusion and contact prophylaxis. [1]
Basic supportive tests round out the workup as the clinical picture demands. A full-blood count frequently shows a marked lymphocytosis — a characteristic finding driven by pertussis toxin, and especially striking in infants. A chest X-ray is indicated when pneumonia is suspected, and the unwell infant needs continuous monitoring for apnoea and oxygenation. The lymphocytosis is not diagnostic on its own, but in an infant with apnoea and a cough contact it strengthens the case for pertussis while the PCR is pending. [1] [8]
Management — Resuscitation
Resuscitation is about the infant who is deteriorating. The red flags are apnoea, cyanosis, exhaustion, recurrent desaturation and an acute life-threatening event. An infant with any of these needs admission to a monitored bed or the paediatric intensive care unit, because the margin between a stable paroxysm and a respiratory arrest is narrow in this age group. The decision to admit a young infant with pertussis should be deliberately low-threshold. [8] [1]
Supportive airway and breathing care is the mainstay. Give supplemental oxygen for desaturation, use gentle suctioning to clear secretions, and minimise stimulation that can trigger paroxysms. Severe cases may need respiratory support, up to and including mechanical ventilation, and the team should be ready for apnoea at any point. The aim is to keep the infant oxygenated, feeding and monitored through the period of greatest risk. [1] [8]
Maintain hydration and nutrition deliberately. Paroxysms and post-tussive vomiting make feeding difficult, so use small, frequent feeds, consider nasogastric support, and use intravenous fluids in the infant who cannot feed safely. A child who is losing weight or becoming dehydrated is a child who needs supportive admission regardless of how the paroxysms look in clinic. [1] [8]
Start a macrolide antibiotic early. The macrolide's principal role in an established case is to limit the infectious period and protect contacts — it rarely shortens the paroxysmal course once it has begun — but it should be started promptly so that isolation, exclusion and the return-to-school calculation can proceed. Treating pneumonia, seizures or encephalopathy as complications, and watching for secondary bacterial infection, completes the resuscitation bundle. [4] [1]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway matched to age and severity, with the individual treatment at one end and the public-health response at the other. Supportive and monitored care protects the young infant; a macrolide, isolation and exclusion manage the stable case; and chemoprophylaxis, catch-up vaccination and notification run the public-health layer that prevents the next infant case. [1] [10]
The stepwise pertussis pathway
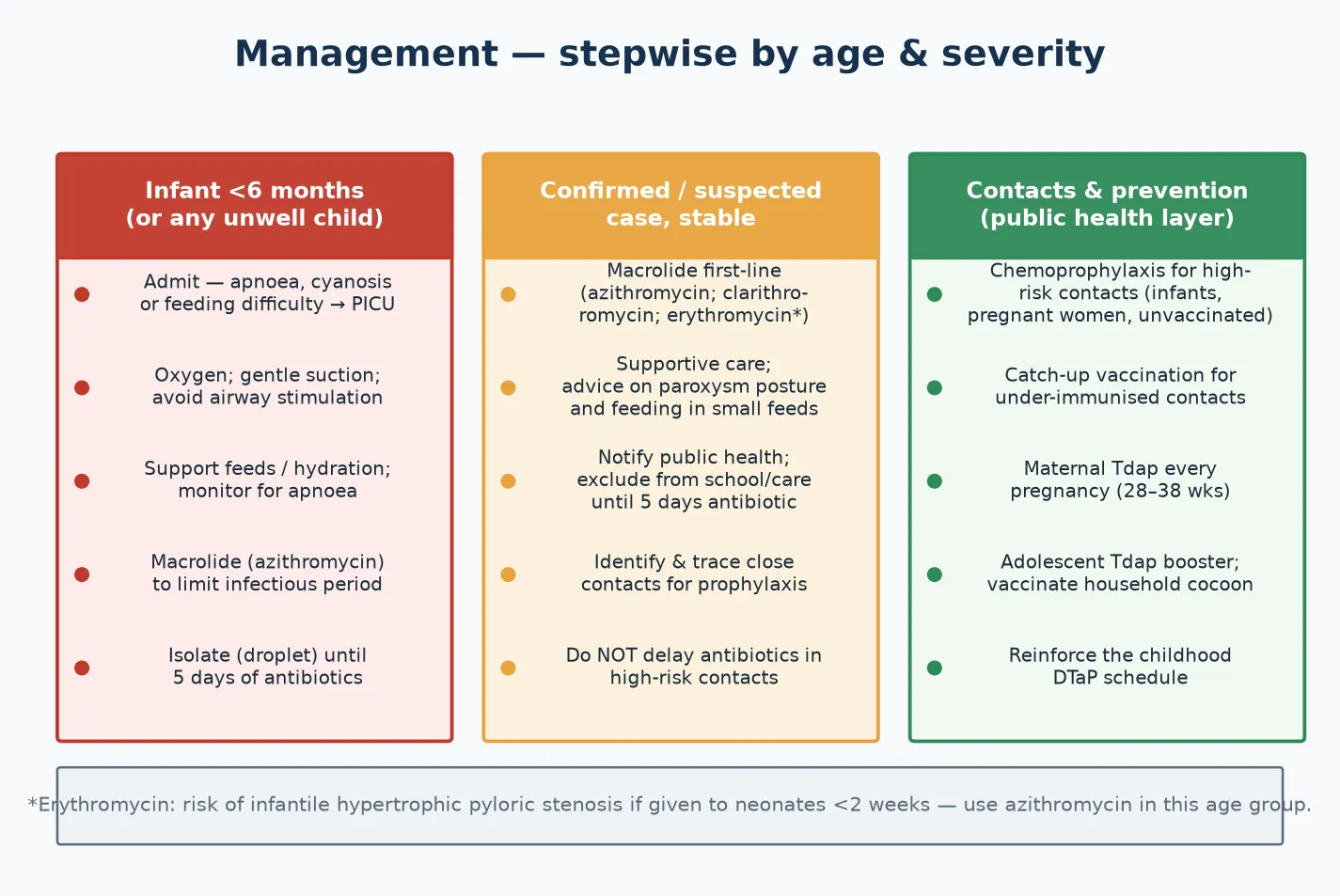
Infant or unwell child: admit for monitoring, give oxygen and gentle suction, support feeds and hydration, and start a macrolide; escalate to PICU for apnoea, cyanosis or exhaustion.
Confirmed or suspected case: give a macrolide — azithromycin first-line, clarithromycin as an alternative, erythromycin with caution in neonates because of pyloric-stenosis risk.
Isolate with droplet precautions and exclude from school or childcare until five days of effective antibiotic, or for three weeks from paroxysm onset if untreated.
Notify public health, and trace household and close contacts; identify who is high-risk.
Offer chemoprophylaxis to high-risk contacts — infants under twelve months, pregnant women, and unvaccinated or under-vaccinated household contacts.
Give catch-up vaccination to under-immunised contacts, and reinforce maternal Tdap, the adolescent Tdap booster and the childhood DTaP schedule.
For the confirmed or suspected case, a macrolide is first-line treatment. Azithromycin is the usual first choice across age groups; clarithromycin is an alternative; and erythromycin remains an option but carries a risk of infantile hypertrophic pyloric stenosis when given to neonates in the first weeks of life, so azithromycin is preferred in that age group. The standard azithromycin course runs for five days, and its purpose is principally to reduce infectiousness — honest expectation-setting with families prevents the disappointment of a cough that outlasts the antibiotics. [4] [1]
Isolation, exclusion and notification form the transmission-control layer. Place the case under droplet precautions, and exclude from school or childcare until five days of an effective antibiotic have been completed — or, if untreated, for three weeks from the onset of paroxysms. Notify public health according to local requirements, because pertussis is notifiable in most jurisdictions, and the notification triggers the contact-tracing and prophylaxis response. [10] [1]
Chemoprophylaxis is targeted at the contacts who matter most. High-risk contacts — infants under twelve months, pregnant women, and unvaccinated or under-vaccinated household contacts — should receive a macrolide promptly after exposure, because prophylaxis given early can prevent or attenuate disease and protects the vulnerable infant at the centre of the cluster. A household study of azithromycin prophylaxis supports its use to prevent pertussis in exposed contacts, and the aim is always to protect the youngest, least-protected member of the household. [10] [8]
Specific Subtypes & Scenarios
A young infant (under six months) with apnoea or cyanotic coughing spells. This is the highest-risk presentation and the commonest cause of death. Admit for monitoring, provide oxygen and supportive care, maintain hydration and nutrition, and start a macrolide. Watch continuously for apnoea, and escalate to PICU for respiratory failure. The earlier the infant is identified and supported, the better the outcome. [8] [1]
A school-age child with classic paroxysms and whoop. Confirm with PCR if within the first few weeks, or serology if later, give a macrolide, and exclude from school until the isolation criteria are met. Identify the household contacts and offer prophylaxis where indicated, and look for the infant at the centre of the household — the school-age child is often the one who brings pertussis home to a younger sibling. [1] [10]
An adolescent or adult with a prolonged cough and no whoop. The absence of a whoop does not exclude pertussis. Test with serology if the cough has lasted beyond two to three weeks, treat to limit transmission, and reinforce the adolescent or adult Tdap booster. This is the group that silently sustains transmission to infants, so identifying and treating them is a public-health act as much as a clinical one. [2] [3]
A pregnant woman at twenty-eight to thirty-eight weeks. Give maternal Tdap in every pregnancy, regardless of prior vaccination history, because the transplacental transfer of antibody protects the infant through the vulnerable first months before the primary series is complete. The timing matters: antibody peaks a few weeks after vaccination, so the late-second to early-third trimester is the window that delivers the most antibody to the baby. [8] [9]
A partially vaccinated household contact of an infant case. Offer chemoprophylaxis and catch-up vaccination to complete the cocoon around the vulnerable infant. The logic of cocooning is that every immune person around the infant is a barrier between the organism and the baby, and a contact who is caught up on vaccination is a contact who is far less likely to transmit. [10] [3]
An outbreak in a school or under-vaccinated community. Coordinate with public health, offer vaccination and prophylaxis as directed, and exclude cases to interrupt transmission. Outbreaks in under-immunised pockets are a reminder that vaccine coverage is a population responsibility, and that the infants at the edge of the outbreak are the ones who pay the price of low coverage. [5] [1]
Complications & Pitfalls
Pneumonia is the commonest severe complication and a leading cause of death, particularly in young infants. It may be a primary pertussis pneumonia or a secondary bacterial infection, and a child whose cough is accompanied by fever, respiratory distress or hypoxia needs assessment for pneumonia and, often, admission. Recognising pneumonia early and treating it is one of the few interventions that genuinely changes the outcome of severe pertussis. [1] [8]
The central diagnostic pitfall is waiting for the whoop in a young infant. The whoop is often absent, and apnoea may be the only sign of a lethal infection. A clinician who requires the textbook triad before testing or admitting an infant will miss the disease at the moment it is most dangerous. The rule that protects against this error is simple: apnoea or a colour change in an infant with a cough contact is pertussis until proven otherwise. [8] [1]
A second pitfall is treating pertussis expecting the antibiotics to shorten the cough. The Cochrane review of antibiotics for whooping cough found that macrolides eradicate the organism and reduce infectiousness, but the evidence that they shorten the paroxysmal course once it is established is weak. Setting this expectation honestly with families prevents the frustration of a cough that outlasts the treatment, and it frames the macrolide correctly as a public-health measure. [4]
A third pitfall is the choice of macrolide in the neonate. Erythromycin carries a risk of infantile hypertrophic pyloric stenosis when given to babies in the first weeks of life, so azithromycin is preferred in this age group. Applying the adult or older-child default to a neonate is an avoidable error, and the age-specific choice is a detail an examiner probes. [4] [1]
Forgetting the public-health layer is the fourth error. Failing to notify, to isolate, to exclude, or to trace and offer prophylaxis to contacts allows ongoing transmission to other vulnerable infants. The clinical encounter does not end when the child is treated; it ends when the contacts have been protected and the cluster has been contained. [10] [3]
The final pitfall is vaccine complacency. Because acellular-vaccine immunity wanes, a vaccinated child can still catch pertussis, and a suggestive cough in a vaccinated child still warrants testing. Dismissing a prolonged cough because "the child is fully immunised" closes the door on the diagnosis at the very point the resurgence epidemiology makes it most plausible. [2] [6]
Prognosis & Disposition
Most older children and adults recover fully, but the cough may last for weeks to months — the "hundred-day cough" — and the morbidity in this group is driven less by danger than by disruption to sleep, feeding, school and work. For these patients the disposition is usually home management with isolation, a macrolide, and clear safety-netting. [1] [3]
The mortality is concentrated in infants under six months, most often from pneumonia, apnoea or encephalopathy, and it is highest in those too young to be vaccinated. This is the single most important prognostic fact in pertussis, and it is why every prevention strategy ultimately aims to protect this age group — through maternal antibody, cocooning, and prompt treatment of the sick infant. [8] [1]
Disposition follows severity. Admit to a monitored bed or PICU the infant with apnoea, cyanosis, desaturation or exhaustion; admit to the ward the younger or dehydrated infant who needs feeding support and observation; and manage at home, with isolation and follow-up, the stable older child. The threshold for admitting a young infant is deliberately low, because the child who looks well between paroxysms can still arrest during one. [8] [1]
At discharge, complete the isolation or five-day antibiotic course, clear the exclusion, finish the contact tracing and prophylaxis, and give the family a clear safety-net for return — worsening apnoea, cyanosis, poor feeding, dehydration or fever. Reinforce the immunisation schedule, both for the child and for the household, because the discharge encounter is also a prevention opportunity. [1] [10]
Recurrence is possible, because neither natural infection nor the acellular vaccine confers lifelong immunity. Boosters and the maternal programme remain necessary across the life course, and a child who has had pertussis still needs to complete and maintain the schedule. The disease does not confer the durable protection that the vaccine programme tries to engineer. [2] [6]
Special Populations
Infants under six months are the highest-risk group, the principal beneficiaries of maternal vaccination and cocooning, and the patients for whom the threshold to test and admit is lowest. Their atypical presentation — apnoea without a whoop — is the single most important clinical fact in pertussis, and every system of care should be designed to catch them early. [8] [9]
Pregnant women should receive maternal Tdap in every pregnancy, optimally between 20 and 32 weeks in Australia (CDC often 27–36 weeks), because transplacental antibody transfer protects the infant through the first months of life. The US infant-pertussis-incidence trends study and the maternal-vaccination antibody-transfer studies underpin this recommendation, and offering Tdap in pregnancy is the single most effective current protection for the newborn. [8] [9]
Unvaccinated or under-vaccinated children and communities carry higher incidence and severity, and they are the substrate for outbreaks. Address vaccine hesitancy respectfully, offer catch-up vaccination at every opportunity, and recognise that under-immunised pockets are where the disease resurges most violently. The parental-refusal evidence is a reminder that individual vaccination decisions have population consequences. [5] [1]
Immunocompromised children may have atypical or prolonged illness and a less robust response to vaccination, so they depend on the immunity of the people around them. Cocooning matters most for these children, and early treatment of disease, with a low threshold for investigation and support, is the right stance. [1] [3]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families may face barriers to timely immunisation and care. Ensure culturally safe, equitable access to vaccination, treat actively when disease is suspected, and use trained interpreters rather than family members. Disadvantage should never be the reason a pertussis diagnosis is delayed or an infant is left unvaccinated. [1] [8]
Rural and remote children need timely access to diagnosis, treatment and public-health follow-up, often through outreach and telehealth, because distance can delay the care that a sick infant cannot afford to wait for. The plan for a remote family accounts for what is actually available locally, and retrieval is mobilised early when an infant deteriorates. [8] [1]
Evidence, Guidelines & Regional Differences
The global standard for pertussis vaccination is the WHO position paper on pertussis vaccines, which sets out the recommended schedule, the place of maternal immunisation, and the use of boosters. It is the reference against which national programmes are compared, and it frames pertussis as a vaccine-preventable disease whose control is a public-health responsibility as much as a clinical one. [1] [3]
The efficacy and limitations of the acellular vaccine are defined by trials and models. The Ward et al. trial in the New England Journal of Medicine established the efficacy of an acellular pertussis vaccine in adolescents and adults, the group that sustains transmission; and baboon-model work comparing whole-cell and acellular vaccines showed that while acellular vaccines prevent disease, they may not block colonisation and transmission as effectively as whole-cell vaccines. This durability and transmission gap is the biological anchor of the resurgence problem. [2] [6]
Maternal Tdap and US infant pertussis incidence
Population: US surveillance of infant pertussis incidence before and after implementation of the maternal tetanus, diphtheria and acellular pertussis (Tdap) vaccination programme.
Key finding
Implementation of maternal Tdap was associated with a reduction in infant pertussis incidence and in pertussis-related hospitalisation in young infants, the age group at highest risk.
Practice change
Vaccinating pregnant women is the single most effective current protection for infants too young to be fully vaccinated; offer Tdap in every pregnancy.
The maternal-vaccination evidence underpins the strongest current prevention. The US infant-pertussis-incidence trends study showed that maternal Tdap implementation was associated with reduced infant incidence and hospitalisation, and the antibody-transfer studies confirmed that maternal vaccination raises infant anti-pertussis antibody concentrations in the first months of life. Together they justify giving Tdap in every pregnancy, ideally between 28 and 38 weeks. [8] [9]
The treatment and prophylaxis evidence is set out in the Cochrane review of antibiotics for whooping cough and in the household-prophylaxis literature. The Cochrane review found that macrolides eradicate the organism and reduce infectiousness but that evidence for shortening the paroxysmal course is weak — so treatment is principally a public-health measure. The household study of azithromycin prophylaxis supports targeted chemoprophylaxis of exposed contacts, and the parental-refusal study confirms that under-vaccination raises individual risk. [4] [10]
The regional policy structure is consistent in principle and varies in detail. In ANZ, pertussis is nationally notifiable, the Australian Immunisation Handbook (ATAGI) and the New Zealand immunisation schedule set the DTaP/Tdap programme and the maternal-Tdap recommendation, and public-health units coordinate notification and prophylaxis. In the UK, the Green Book and UK Health Security Agency guidance direct the programme, including the maternal programme introduced after a large outbreak. In the US, the CDC and AAP set the schedule and surveillance, with maternal Tdap recommended in every pregnancy. In Canada, the Canadian Immunization Guide and provincial programmes deliver the equivalent strategy. In every region the principle is the same: vaccinate in pregnancy, complete the childhood schedule, boost in adolescence, and protect the contacts around the infant. [1] [8]
The controversies are real and active: the durability gap between whole-cell and acellular vaccines and whether to reconsider whole-cell priming; the optimal timing and coverage of maternal vaccination; the balance between treating the individual case and prophylaxing the contacts; and the inequities in vaccine access that leave some communities and infants unprotected. The defence against each is the same: high coverage, boosters, the maternal programme, prompt treatment, and a public-health layer that does not stop at the bedside. [6] [1]
Exam Pearls
- Pertussis is a droplet infection with Bordetella pertussis; the classic course is catarrhal, paroxysmal, convalescent, and the whoop and post-tussive vomiting define the paroxysmal stage. [1]
- Infants under six months may have NO whoop — apnoea, cyanosis, choking or poor feeding may be the only sign, and this is the presentation that kills. [8]
- The hallmark full-blood-count finding is a marked lymphocytosis, especially in infants, driven by pertussis toxin. [1]
- Diagnose with PCR early (catarrhal to early paroxysmal, first three to four weeks) and serology later (more than two to three weeks of cough). [1]
- Treat with a macrolide — azithromycin first-line — for five days; the aim is to limit infectiousness, not to shorten the cough. [4]
- Isolate and exclude until five days of antibiotic (or three weeks from paroxysm onset if untreated); notify public health. [10]
- Give high-risk contacts — infants, pregnant women, the unvaccinated — chemoprophylaxis promptly. [10]
- Prevention is maternal Tdap every pregnancy (20–32 weeks (ANZ) / 27–36 weeks (CDC)), the childhood DTaP schedule, an adolescent Tdap booster, and cocooning. [8]
- Waning acellular-vaccine immunity plus under-vaccination drives resurgence — a vaccinated child can still catch pertussis, so a suggestive cough still warrants testing. [2]
- Pneumonia is the commonest severe complication and a leading cause of death; erythromycin risks infantile hypertrophic pyloric stenosis in neonates under two weeks. [4]
References
- [1]WHO Pertussis vaccines: WHO position paper, August 2015--Recommendations. Vaccine, 2016.PMID 26562318
- [2]Ward JI; Cherry JD; Chang SJ; Partridge S; et al Efficacy of an acellular pertussis vaccine among adolescents and adults. N Engl J Med, 2005.PMID 16221778
- [3]Tan T; Halperin S; Cherry JD; Edwards K; et al Pertussis immunization in the global pertussis initiative North American region: recommended strategies and implementation considerations. Pediatr Infect Dis J, 2005.PMID 15876933
- [4]Altunaiji S; Kukuruzovic R; Curtis N; Massie J Antibiotics for whooping cough (pertussis). Cochrane Database Syst Rev, 2007.PMID 17636756
- [5]Glanz JM; McClure DL; Magid DJ; Daley MF; et al Parental refusal of pertussis vaccination is associated with an increased risk of pertussis infection in children. Pediatrics, 2009.PMID 19482753
- [6]Warfel JM; Zimmerman LI; Merkel TJ Comparison of Three Whole-Cell Pertussis Vaccines in the Baboon Model of Pertussis. Clin Vaccine Immunol, 2016.PMID 26561389
- [7]Zimmerman LI; Papin JF; Warfel J; Wolf RF; et al Histopathology of Bordetella pertussis in the Baboon Model. Infect Immun, 2018.PMID 30126900
- [8]Skoff TH; Deng L; Bozio CH; Hariri S US Infant Pertussis Incidence Trends Before and After Implementation of the Maternal Tetanus, Diphtheria, and Pertussis Vaccine. JAMA Pediatr, 2023.PMID 36745442
- [9]Havers FP; Skoff TH; Rench MA; Epperson M; et al Maternal Tetanus Toxoid, Reduced Diphtheria Toxoid, and Acellular Pertussis Vaccination During Pregnancy: Impact on Infant Anti-Pertussis Antibody Concentrations by Maternal Pertussis Priming Series. Clin Infect Dis, 2023.PMID 35642525
- [10]Alvarez J; Godoy P; Plans-Rubio P; Camps N; et al Azithromycin to Prevent Pertussis in Household Contacts, Catalonia and Navarre, Spain, 2012-2013. Emerg Infect Dis, 2020.PMID 33079034