Paeds · infectious-diseases
Staphylococcal scalded skin syndrome
Also known as Staphylococcal scalded skin syndrome · SSSS · Ritter disease · Pemphigus neonatorum · Lyell disease (staphylococcal) · Generalised bullous impetigo
Fellowship guide to staphylococcal scalded skin syndrome: the toxin-mediated blistering disorder of infants and young children produced when phage-group-II Staphylococcus aureus releases exfoliative toxins A and B that cleave desmoglein 1. Covers the bullous impetigo, scarlatiniform, and generalised (Ritter) phenotypes, the mucosa-sparing superficial split that separates it from Stevens-Johnson syndrome and toxic epidermal necrolysis, the mostly negative blood cultures, anti-staphylococcal antibiotics with clindamycin for toxin suppression, and the child's near-complete recovery without scarring.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A fretful, febrile infant whose skin turns scarlet and then peels off in sheets is one of the most arresting sights in paediatrics, and staphylococcal scalded skin syndrome is the diagnosis that explains it. Phage-group-II Staphylococcus aureus, often colonising a trivial focus such as a sticky eye or an umbilical stump, releases exfoliative toxins A and B that travel in the blood and split the superficial epidermis. The result is tender erythema, fragile blisters, and widespread desquamation that looks like a scald but heals without scarring in a child who is treated promptly. [2]
The illness belongs to the family of staphylococcal exfoliative toxin diseases, which span from localised bullous impetigo at one end to generalised SSSS, also known as Ritter disease, at the other. The dividing line is whether the toxin stays local or reaches the circulation, and that in turn depends on the bacterial strain and on the host's ability to clear the toxin through the kidneys. Infants and children under six years cannot excrete the toxin as efficiently as adults, which is why this is overwhelmingly a disease of the very young. [1]
The single most important clinical point is that the mucous membranes are spared. The toxin cleaves desmoglein 1, which is expressed in the superficial epidermis of skin but is compensated for in mucosa by desmoglein 3, so the mouth, eyes, and genital surfaces remain intact. This single fact separates SSSS from Stevens-Johnson syndrome and toxic epidermal necrolysis, in which mucosal involvement is the rule and the split is full-thickness. Getting that distinction right at the bedside dictates the antibiotic choice, the prognosis, and the conversation with a frightened family. [3]
Classification
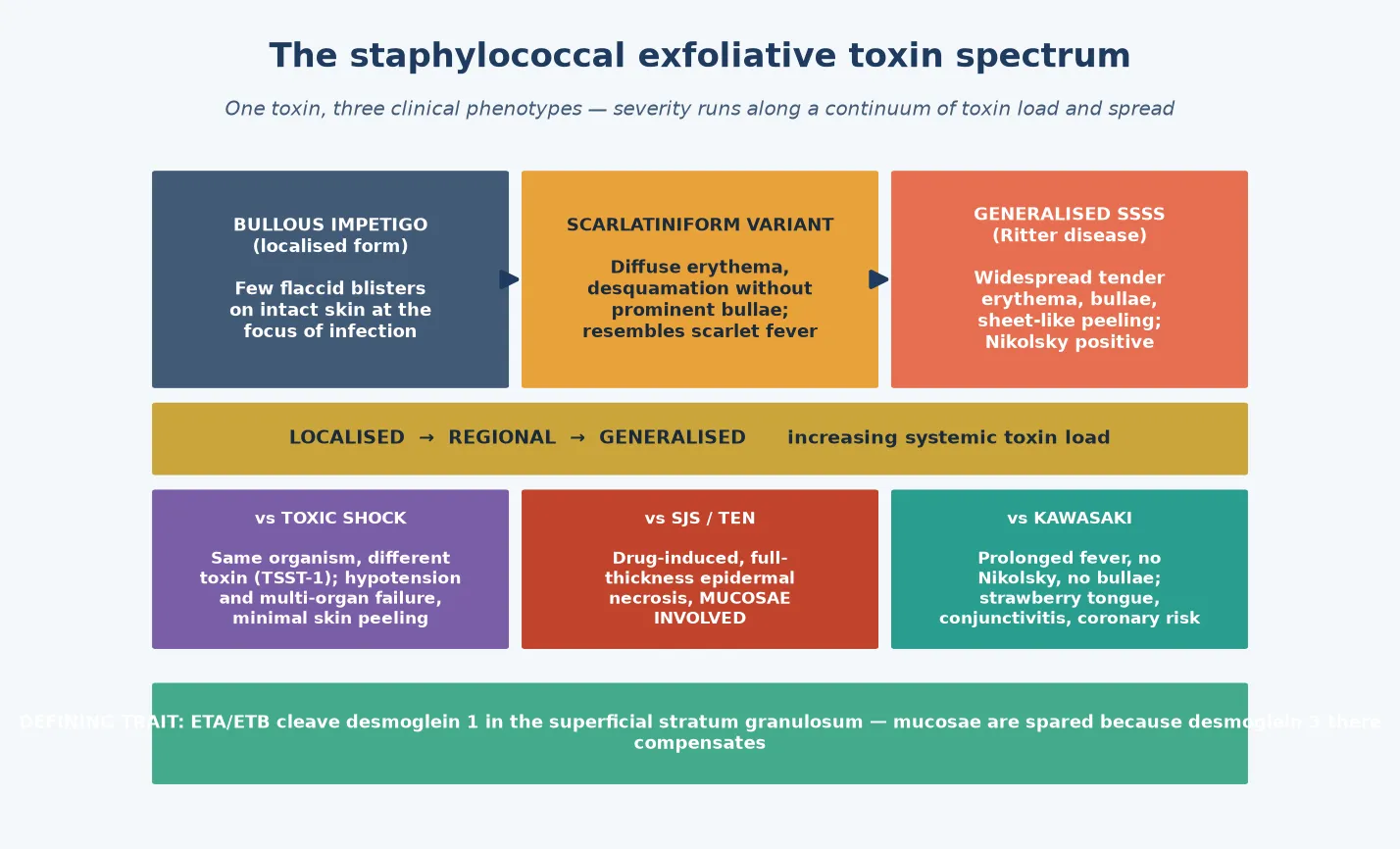
Clinicians group the staphylococcal exfoliative toxin disorders by how far the toxin has spread from its source. Bullous impetigo is the localised form, in which the toxin acts only at the site of infection to produce a few flaccid blisters on otherwise intact skin. Generalised SSSS, or Ritter disease in neonates, is the disseminated form, in which toxin reaches the circulation and the entire skin surface becomes involved. Between these two sits a scarlatiniform variant, in which diffuse erythema and desquamation occur without prominent bullae and the rash can be mistaken for scarlet fever. [5]
The severity of the phenotype reflects the dose of toxin the host absorbs and the efficiency with which the host clears it. The same toxin can produce a single blister in one infant and head-to-toe peeling in another, depending on the strain, the size of the focus, and the maturity of the child's renal clearance. Recognising that these phenotypes are points on a single spectrum prevents the error of treating bullous impetigo as an unrelated disease when the underlying organism and its toxin are the same. [1]
Distinguishing SSSS from its mimics is the central diagnostic task, because the therapy and the prognosis differ sharply. Toxic shock syndrome is caused by the same organism but a different toxin, TSST-1, and presents with hypotension and multi-organ failure rather than blistering. Stevens-Johnson syndrome and toxic epidermal necrolysis are drug-induced, produce full-thickness epidermal necrosis, and involve the mucosae. Kawasaki disease causes prolonged fever, conjunctivitis, and a strawberry tongue but no Nikolsky sign and no bullae. Holding these four diagnoses in mind at every assessment keeps the clinician oriented to the correct one. [3]
Epidemiology & Risk Factors
Staphylococcal scalded skin syndrome is overwhelmingly a disease of infants and young children, with the great majority of cases occurring before the age of six years. Neonates are particularly susceptible because their immature renal function limits clearance of the toxin, and nursery outbreaks are a well-recognised hazard. Beyond early childhood the syndrome becomes rare, because mature kidneys clear the toxin efficiently, and when an adult develops SSSS it usually signals renal failure, immunocompromise, or another failure of toxin clearance that carries a far higher mortality. [2]
Population-based data from Germany recorded an annual incidence of roughly five to ten cases per million children, with a clear preponderance in boys and a winter-to-spring seasonality. Mortality in children is low, in the range of three to four per cent in modern series, but it climbs steeply with delayed presentation, extensive skin involvement, dehydration, or superimposed sepsis. The disease burden falls heaviest on neonates and on children with underlying skin breakdown or immune impairment. [7]
The dominant risk factor is exposure to a toxigenic strain of Staphylococcus aureus, which colonises the conjunctiva, the umbilicus, the nasopharynx, a wound, or the nappy area and then seeds toxin into the bloodstream. Outbreaks in neonatal units trace to a carrier among staff or parents, and the source is often an asymptomatic nasal or fingertip carrier whose organism reaches a vulnerable infant through contact. Chronic kidney disease, immunosuppression, and pre-existing skin disease each raise the risk of progression from colonisation to disseminated disease in older patients. [8]
Pathophysiology
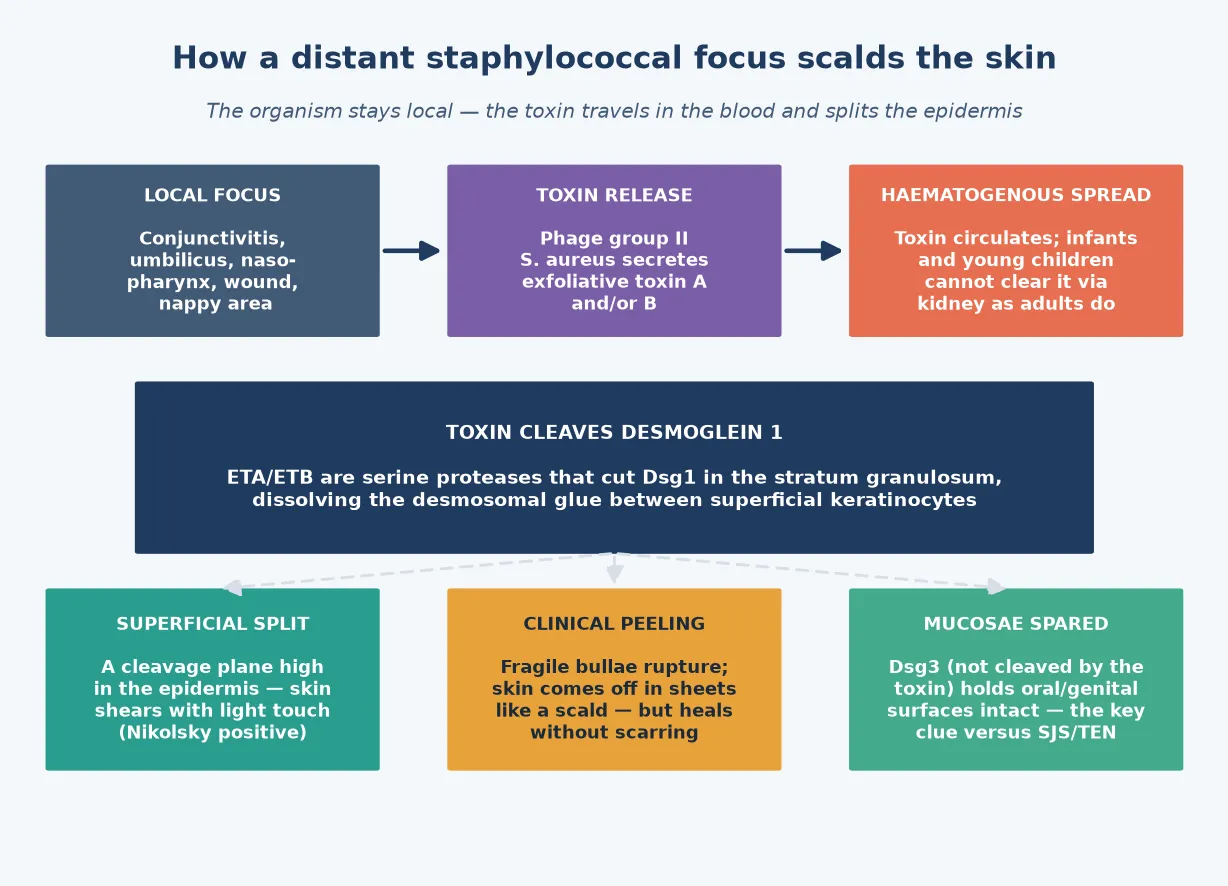
The cascade begins at a local focus where a toxigenic Staphylococcus aureus strain takes hold. The conjunctiva, the umbilical stump, the nasopharynx, a surgical or traumatic wound, or the nappy area each provide a portal, and the organism multiplies there without necessarily causing an obvious local infection. The clinically apparent skin disease is therefore a remote event, generated by toxin that has left the focus and travelled through the blood. [2]
The toxins themselves are the key. Phage-group-II strains of Staphylococcus aureus secrete exfoliative toxin A, which is chromosomally encoded and heat-stable, and exfoliative toxin B, which is plasmid-encoded and heat-labile. Both are serine proteases with a remarkable specificity: they cleave desmoglein 1, the desmosomal adhesion molecule that binds superficial keratinocytes to one another, and they do so at a precise site in the extracellular domain. They do not cleave desmoglein 3, which is the molecular reason the mucosae are spared. [12]
The split occurs in the stratum granulosum, high in the epidermis, which is why the skin peels so superficially and why healing occurs without scarring. Desmoglein 1 loss dissolves the glue between the outermost keratinocytes, so the upper epidermis shears away from the viable layer beneath with the lightest touch, giving the positive Nikolsky sign. In the mucosa, desmoglein 3 takes over the adhesion role, which is why the mouth, eyes, and genital surfaces stay intact even when the surrounding skin is peeling off. [6]
The host determines the phenotype through toxin clearance. Infants and young children excrete the toxin slowly because their renal function is immature, so toxin accumulates and reaches the skin in sufficient concentration to split it. Adults clear the toxin efficiently, which is why adult SSSS is rare and almost always associated with renal failure, immunocompromise, or a hidden source of ongoing toxin production. Blood cultures are typically negative in children because the organism stays at its local focus and only the toxin circulates, which is a point that distinguishes SSSS from a true staphylococcal septicaemia. [1]
Clinical Presentation
The child usually begins with a prodrome of irritability, low-grade fever, and malaise, often dismissed as a minor viral illness before the skin reveals the diagnosis. Within hours the skin becomes tender and erythematous, beginning around the mouth, in the flexures, and at the neck, and then spreading centrifugally over much of the body surface. The erythema has a scarlatiniform, sandpaper quality in some children before the bullae emerge, and the tenderness is striking, with the infant crying when handled. [5]
Flaccid, superficial bullae appear within the erythematous skin over the next day. They rupture easily and leave a moist, glistening, raw surface that looks like a scald, and the surrounding skin shears off on light stroking, giving a positive Nikolsky sign. Large sheets of epidermis peel away, leaving the child with extensive areas of denuded skin that lose fluid, heat, and the barrier against infection. The face often shows perioral fissuring and radial crusting that produces the characteristic sad-man facies, a helpful diagnostic clue. [3]
Throughout all of this the mucous membranes remain intact. The oral mucosa, the conjunctivae, and the genital surfaces show no ulceration or blistering, even when the surrounding facial or perineal skin is severely involved. This sparing is the cardinal feature that separates SSSS from Stevens-Johnson syndrome and toxic epidermal necrolysis, in which mucosal involvement is prominent, and it should be actively sought and documented at every assessment. [2]
The severity ranges from a limited distribution to involvement of the entire skin surface, and the systemic state varies with it. A child with extensive involvement is at risk of dehydration, hypothermia, and secondary infection from the loss of the skin barrier, while a child with limited disease may be only mildly unwell. The skin usually begins to dry and desquamate over three to five days, and complete healing occurs within one to two weeks without scarring, which is the reassuring message that should anchor the conversation with the family. [4]
Evolution of staphylococcal scalded skin syndrome
Prodrome of irritability, low-grade fever, and skin tenderness
Scarlet erythema around the mouth, flexures, and neck, then spreading
Flaccid superficial bullae that rupture to leave a moist raw surface
Positive Nikolsky sign with sheet-like peeling of the epidermis
Perioral fissuring and radial crusting producing the sad-man facies
Desquamation and drying over three to five days with complete healing within two weeks
Differential Diagnosis
The blistering, desquamating infant invites a focused differential, because several serious conditions share features with SSSS and demand a different treatment. Stevens-Johnson syndrome and toxic epidermal necrolysis are the most important mimics, and both are usually drug-induced, produce full-thickness epidermal necrosis, and involve at least two mucosal sites. The presence of oral, conjunctival, or genital ulceration in a blistering child shifts the diagnosis away from SSSS and toward a drug reaction, and the management changes accordingly. [3]
Bullous impetigo sits within the same toxin spectrum as SSSS and is distinguished by its localised nature. The bullae are few, they sit on intact skin at the focus of infection, and the child is usually systemically well. Recognising bullous impetigo matters because localised disease can be treated with topical or oral anti-staphylococcal agents without the need for the supportive care that generalised SSSS requires, though the clinician must watch for progression to the disseminated form. [1]
Toxic shock syndrome is produced by the same organism but a different toxin and presents a different clinical challenge. The child is hypotensive and multi-organ unwell, with a diffuse erythroderma and late desquamation, rather than the acute blistering and peeling of SSSS. Kawasaki disease causes fever, conjunctivitis, strawberry tongue, and a polymorphous rash with later periungual desquamation, but it lacks the acute bullae and the Nikolsky sign. Holding these four diagnoses against the clinical picture at every reassessment keeps the clinician oriented. [3]
[3]Clinical & Bedside Assessment
The assessment begins with a judgement of how sick the child is, using the paediatric assessment triangle and a full set of vital signs. A child with extensive skin loss may be hypothermic from heat loss, dehydrated from fluid loss across the raw surface, or tachycardic from pain or evolving shock, and each of these demands immediate action. Weigh the child, measure the temperature, heart rate, respiratory rate, blood pressure, and capillary refill, and estimate the extent of skin involvement as a percentage of body surface area. [4]
Expose the skin fully and examine the distribution and character of the eruption. Look for the scarlet erythema, the flaccid bullae, the moist raw surface where the epidermis has sheared away, and the perioral fissuring of the sad-man facies. Perform a careful Nikolsky test by applying lateral pressure with a finger on apparently unblistered erythematous skin, and a positive result, in which the superficial epidermis slides off, supports the diagnosis. Mark the extent of involvement and document it, because progression over the next hours guides the level of supportive care. [5]
Examine the mucous membranes deliberately and document what you find. The oral mucosa, the conjunctivae, and the genital surfaces should be intact in SSSS, and their involvement shifts the diagnosis toward SJS or TEN. Look at the umbilicus, the conjunctiva, the nasopharynx, and the nappy area for the staphylococcal focus that is generating the toxin, because identifying and treating that focus is the route to stopping toxin production. Palpate for lymphadenopathy and examine for any source of deeper infection that would explain a positive blood culture if one returns. [2]
Investigations
The diagnosis of SSSS is clinical, and laboratory tests serve to support the impression, to quantify severity, and to search for the focus rather than to confirm the diagnosis. A full blood count, C-reactive protein, and electrolytes are useful in a child with extensive involvement or systemic illness, and they track the degree of dehydration and inflammation. Blood cultures should be drawn but are usually negative, because the organism stays at its local focus and only the toxin circulates. [10]
Swabs of the suspected portal are more revealing than blood cultures. A swab of a sticky eye, an umbilical stump, a nasopharyngeal site, a wound, or the nappy area can grow the toxigenic Staphylococcus aureus that is producing the toxin, and isolating it confirms the source. A skin swab from an unruptured bulla is usually sterile in SSSS, in contrast to bullous impetigo where the fluid is seeded with organisms, and that contrast reinforces the distinction between the localised and the disseminated forms. [5]
A skin biopsy is rarely required in a typical case, because the clinical picture is characteristic and the disease is usually uncomplicated in children. When the diagnosis is uncertain, particularly when SJS or TEN are genuine possibilities, a frozen-section biopsy shows the superficial split in the stratum granulosum of SSSS, in contrast to the full-thickness necrosis of TEN. This single histological distinction can settle a difficult case at the bedside and direct the child to the correct pathway. [3]
Management — Resuscitation
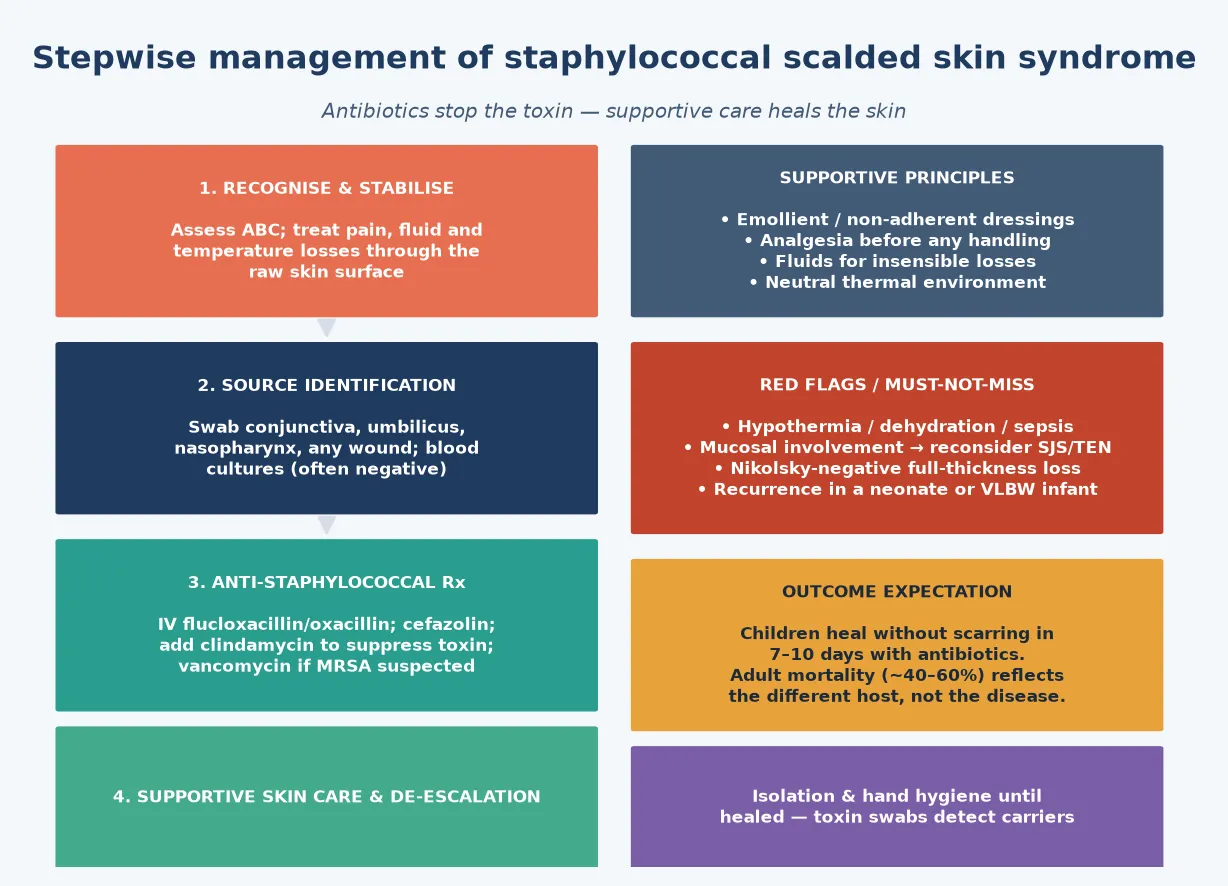
A child with extensive skin loss behaves like a burn patient, and resuscitation begins with attention to fluid, temperature, and pain. Assess the airway and breathing, establish intravenous access, and estimate the extent of skin involvement as a percentage of body surface area, because fluid losses scale with that figure. Give analgesia before any handling of the raw skin, because the denuded surface is exquisitely tender, and titrate opiate analgesia to allow examination and care without distress. [4]
Correct dehydration and electrolyte losses with intravenous fluids, calculated to cover maintenance plus the additional insensible loss across the raw surface, and monitor the response with urine output and clinical perfusion. Maintain the child in a neutral thermal environment, because the loss of the skin barrier promotes heat loss, and check the temperature frequently to detect hypothermia. A child with extensive involvement may need transfer to a burns or intensive-care setting for the level of monitoring and skin care that the surface area demands. [3]
Give the first dose of anti-staphylococcal antibiotic immediately after cultures and swabs are drawn, because halting toxin production is the definitive act of therapy. Do not wait for microbiological confirmation, because the diagnosis is clinical and the antibiotic should be on board within minutes of the decision to treat. Alert the surgeon, the anaesthetist, and the intensive-care team early in a child with extensive involvement, because the level of supportive care may exceed what a general ward can provide. [2]
Resuscitation of the child with extensive SSSS
Assess airway, breathing, circulation and give high-flow oxygen if needed
Establish intravenous access and draw blood cultures and focus swabs
Estimate the extent of skin involvement as a percentage of body surface area
Give analgesia before handling the raw skin, then titrate to comfort
Replace fluid and electrolyte losses, including insensible loss across raw skin
Maintain a neutral thermal environment and give the first anti-staphylococcal dose
Management — Definitive & Stepwise
The definitive therapy is an anti-staphylococcal antibiotic that halts toxin production at the source. In a child with mild disease, oral flucloxacillin or cephalexin may suffice, but most children with generalised SSSS warrant intravenous therapy. Intravenous flucloxacillin or oxacillin, or cefazolin where flucloxacillin is unavailable, is first-line, and the duration is usually seven to ten days guided by the clinical response. Adding clindamycin is rational because it suppresses toxin synthesis through its effect on ribosomal protein production, and it is often included in moderate or severe disease for this reason. [4]
Flucloxacillin (intravenous, first-line SSSS)
Dose
25-50 mg/kg (max 2 g) intravenously every 6 hours for 7-10 days
When methicillin-resistant Staphylococcus aureus is suspected or prevalent locally, vancomycin replaces flucloxacillin as the backbone, and clindamycin is added or substituted if the strain is susceptible. The choice should reflect local resistance patterns, and infectious-disease advice is valuable in a region with high MRSA prevalence or in a child who fails to improve on first-line therapy. Linezolid is an alternative that covers MRSA and suppresses toxin production, and it is reserved for cases where vancomycin cannot be used. [3]
Antibiotic logic for SSSS by severity and resistance
Supportive skin care is the other half of management, and it matters as much as the antibiotic. Apply emollients and non-adherent dressings to the raw areas to reduce fluid loss and pain, handle the child gently to avoid extending the shearing, and use a topical agent such as white soft-paraffin or a barrier cream to protect the healing skin. Steroids are not indicated and may worsen the infection, and topical antibiotics have little role because the focus is systemic. Skin care continues until desquamation is complete and the new epidermis is intact, which is usually within two weeks in a treated child. [5]
Specific Subtypes & Scenarios
Neonatal SSSS, or Ritter disease, is the most dramatic presentation and carries the highest stakes in the youngest infants. A neonate with sticky-eye conjunctivitis or an umbilical focus can progress to generalised desquamation within hours, and the small body surface area makes fluid and heat losses proportionally greater. Management warrants admission to a neonatal unit, intravenous anti-staphylococcal therapy, meticulous skin care, and close monitoring for dehydration and hypothermia, and the search for a carrier among staff and parents is part of the response to every case. [8]
Nosocomial nursery outbreaks are a recognised pattern, and they demand both case management and epidemiological control. Investigation seeks the source among staff, parents, or shared equipment, with nasal and fingertip swabs to identify asymptomatic carriers of the toxigenic strain. Once a carrier is found, eradication therapy and reinforcement of hand hygiene interrupt transmission, and affected infants receive anti-staphylococcal therapy and supportive care. A single case in a neonatal unit should trigger a search for further cases and for the source, because clusters can follow a missed carrier. [8]
Recurrent SSSS is uncommon but well described, and it most often reflects an ongoing source of toxin in a child whose clearance is impaired. A very low birth weight infant with immature renal function experienced repeated episodes that resolved only when the carrier focus was eradicated, illustrating that recurrence signals persistent exposure and an inability to clear the toxin. When a child presents with recurrence, the clinician should search again for a hidden focus, assess renal and immune function, and involve infectious diseases to plan eradication. [11]
[9]Complications & Pitfalls
The complications of SSSS arise from the loss of the skin barrier and from the systemic effects of the toxin. Dehydration and electrolyte disturbance follow fluid loss across the raw surface, hypothermia follows heat loss, and secondary bacterial or fungal infection can colonise the denuded skin. In a small infant, septicaemia from a skin focus or from the original portal can complicate the picture, and a child who deteriorates after initial improvement should be reassessed for sepsis rather than assumed to be following the expected course. [2]
The mortality in children is low, in the range of three to four per cent in modern series, and it rises with delay, extensive involvement, dehydration, or sepsis. The mortality in adults is far higher, at forty to sixty per cent, because adult disease reflects toxin-clearance failure rather than the benign paediatric host, and that contrast is worth remembering when the same diagnosis appears in a different age group. The prognosis in children who are treated promptly is excellent, with complete healing and no scarring, and that is the message the family needs to hear. [7]
The major pitfalls are misdiagnosis, delayed antibiotic therapy, and undertreatment of fluid and temperature losses. Confusing SSSS with SJS or TEN leads to withdrawal of the wrong drug and a failure to give anti-staphylococcal therapy, while the reverse error exposes a child with SJS to unnecessary antibiotics. Treating the skin without estimating the fluid and heat losses leaves a child hypovolaemic and hypothermic, and failing to search for and treat the focus invites recurrence. Each of these errors is preventable by a structured approach that confirms the diagnosis, treats the source, and supports the skin. [3]
Prognosis & Disposition
The two determinants of outcome are the speed of antibiotic therapy and the adequacy of supportive care. A child who receives prompt anti-staphylococcal antibiotics, fluid and temperature support, and skin care typically heals completely within one to two weeks, with desquamation peaking at three to five days and new epidermis forming beneath. Scarring does not occur because the split is superficial, in the stratum granulosum, and the hair follicles and sweat glands that hold the regenerative cells remain intact. This excellent prognosis is the anchor of the conversation with a frightened family. [4]
Disposition depends on the extent of involvement and the age of the child. A neonate, an infant, or any child with extensive skin loss warrants admission for intravenous antibiotics, fluid and temperature monitoring, and skin care, often in a neonatal or paediatric intensive-care setting. A child with limited disease who is systemically well may be managed with oral antibiotics and close outpatient review, provided the family has a clear safety-net for return. The threshold for admission is low in the very young, because their small body surface area makes fluid and heat losses proportionally greater. [2]
Follow-up focuses on confirming complete healing, identifying any persistent focus that could drive recurrence, and addressing any underlying renal or immune impairment in an older child. In a nursery outbreak, follow-up extends to the unit itself, with ongoing surveillance for new cases and confirmation that the carrier has been treated and that hand hygiene has been reinforced. The family should leave with written advice about the expected course, the signs of deterioration, and the reassuring fact that complete healing without scarring is the norm in a treated child. [5]
Special Populations
Neonates and very low birth weight infants are the most vulnerable group, because their immature renal function limits toxin clearance and their small body surface area amplifies fluid and heat losses. A neonate with SSSS warrants admission to a neonatal unit for intravenous antibiotics, fluid and temperature monitoring, and skin care, and the search for a carrier among staff and parents is part of the response. Recurrence in a very low birth weight infant signals persistent exposure and an inability to clear the toxin, and it should prompt a renewed search for the focus and a plan for eradication. [11]
Immunocompromised children, including those on chemotherapy, after transplantation, or on immunosuppressive biologics, may develop SSSS with a broader range of staphylococcal strains and a higher risk of progression to sepsis. The threshold for intravenous therapy and for admission is lower, and the antibiotic regimen should cover resistant organisms with early infectious-disease input. Children with chronic kidney disease or renal failure are also at higher risk, because they cannot clear the toxin as a healthy child does, and they may need renal-adjusted antibiotic dosing alongside the standard supportive care. [3]
In Indigenous and remote communities across Australia and New Zealand, the higher burden of staphylococcal skin disease, later presentation, and distance from tertiary care all shape the clinical picture. Culturally safe, family-centred care with interpreter access, healthy skin education, and reliable aeromedical retrieval pathways is essential, and empiric vancomycin with clindamycin is reasonable where MRSA prevalence is high. In migrant and refugee families, overcrowded housing and unfamiliarity with the health system may delay presentation, so a clear safety-net in the family's language is part of safe care. [9]
[9]Evidence, Guidelines & Regional Differences
The foundational understanding of SSSS rests on the work of Ladhani and colleagues, who synthesised the clinical, microbial, and biochemical aspects of the exfoliative toxins in a landmark review. Their work established that exfoliative toxins A and B are serine proteases with a precise specificity for desmoglein 1, that the split occurs in the superficial stratum granulosum, and that the sparing of mucosae reflects the compensatory role of desmoglein 3. These molecular insights explain every clinical feature of the disease and underpin the modern approach to diagnosis and management. [1]
The epidemiology of SSSS has been documented in several population-based studies, including a German national survey that reported an annual incidence of roughly five to ten cases per million children, a clear preponderance in boys, a winter-to-spring seasonality, and a child mortality of three to four per cent. Recent single-centre series from tertiary paediatric centres confirm the continued predominance of methicillin-susceptible strains in most regions but document rising MRSA prevalence that influences empiric antibiotic choice. These data calibrate the clinician's expectation of the disease and its prognosis. [7]
[3]Controversies persist around the routine addition of clindamycin for toxin suppression, the duration of intravenous therapy, and the threshold for admission in limited disease. The evidence for clindamycin is mechanistic rather than derived from large trials, because it suppresses ribosomal toxin synthesis, and most authorities include it in moderate or severe disease despite the limited trial data. The duration of therapy is usually seven to ten days, guided by the clinical response, and the threshold for admission is lowest in neonates and in any child with extensive involvement. Rising MRSA prevalence keeps the empiric antibiotic choice a locally calibrated decision. [4]
Exam Pearls
TOXIN signs that anchor the diagnosis
References
- [1]Ladhani S Clinical, microbial, and biochemical aspects of the exfoliative toxins causing staphylococcal scalded-skin syndrome. Clin Microbiol Rev, 1999.PMID 10194458
- [2]Ladhani S Staphylococcal scalded skin syndrome. Arch Dis Child, 1998.PMID 9534685
- [3]Handler MZ Staphylococcal scalded skin syndrome: diagnosis and management in children and adults. J Eur Acad Dermatol Venereol, 2014.PMID 24841497
- [4]Patel GK Treatment of staphylococcal scalded skin syndrome. Expert Rev Anti Infect Ther, 2004.PMID 15482221
- [5]Patel GK Staphylococcal scalded skin syndrome: diagnosis and management. Am J Clin Dermatol, 2003.PMID 12627992
- [6]Hanakawa Y Mechanisms of blister formation by staphylococcal toxins. J Biochem, 2004.PMID 15671483
- [7]Mockenhaupt M Epidemiology of staphylococcal scalded skin syndrome in Germany. J Invest Dermatol, 2005.PMID 15816826
- [8]El Helali N Nosocomial outbreak of staphylococcal scalded skin syndrome in neonates: epidemiological investigation and control. J Hosp Infect, 2005.PMID 16009455
- [9]Soti Khiabani M Ten-Year Epidemiology and Antimicrobial Susceptibility of Pediatric Staphylococcal Scalded Skin Syndrome: A Retrospective Study From a Tertiary Referral Center. Pediatr Dermatol, 2026.PMID 42219159
- [10]Ladhani S Isolating Staphylococcus aureus from children with suspected Staphylococcal scalded skin syndrome is not clinically useful. Pediatr Infect Dis J, 2003.PMID 12664881
- [11]Duijsters CE Recurring staphylococcal scalded skin syndrome in a very low birth weight infant: a case report. J Med Case Rep, 2009.PMID 19830179
- [12]Ladhani S Understanding the mechanism of action of the exfoliative toxins of Staphylococcus aureus. FEMS Immunol Med Microbiol, 2003.PMID 14625102