Paeds · infectious-diseases
Tuberculosis in children
Also known as Childhood tuberculosis · Paediatric TB · Tuberculosis infection in children · Intrathoracic TB in children · Tuberculous meningitis · TB disease and TB infection in children
A fellowship approach to tuberculosis in children: the exposure → TB infection → TB disease spectrum; the age-and-immunity pathophysiology that makes infants and immunocompromised children progress to disseminated and CNS disease; the symptom-and-contact history, chest radiograph, gastric-aspirate-or-sputum Xpert MTB/RIF and TST/IGRA workup; weight-based treatment of non-severe disease (4-month regimen per the SHINE trial), 6-month treatment of severe disease and tuberculosis preventive treatment of infection; tuberculous meningitis as the highest-mortality form; and notification, contact tracing and source-case finding across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A four-year-old boy is brought in thin, tired and coughing for six weeks, and his uncle was recently diagnosed with pulmonary tuberculosis. This is the everyday face of childhood TB: a contact history, an indolent symptom, and a chest radiograph showing lymph-node enlargement. The fellowship skill the case tests is moving correctly along the spectrum \u2014 exposure, infection, disease \u2014 and treating the right thing. [1]
Tuberculosis is the disease caused by Mycobacterium tuberculosis complex. In children the decisive idea is that most who are infected never develop disease: they have TB infection (formerly called latent TB), in which viable bacilli are contained by cell-mediated immunity and the child is well, but remain at lifelong \u2014 usually low \u2014 risk of progression. TB disease is the symptomatic and/or radiological illness that follows when that containment fails. [1] [2]
Why children are a distinct clinical problem is the combination of paucibacillary disease and rapid progression. Children swallow sputum rather than expectorate it, produce few bacilli, and are therefore smear-negative and hard to confirm microbiologically; at the same time, their immature cell-mediated immunity lets the few bacilli they have progress quickly to disseminated, miliary and meningeal disease, especially in the first few years of life. [1]
The clinician's role is therefore threefold: find the child with disease (and treat it correctly), find the child with infection (and offer preventive treatment), and find the source case (and break the transmission chain). All three rest on the same foundation \u2014 a contact history, a chest radiograph and a microbiological sample \u2014 and all three carry a public-health responsibility. [1]
Classification
Begin by deciding where the child sits on the spectrum, because that single decision dictates everything that follows: observe, treat infection, or treat disease. The spectrum runs from exposure (the child has shared air with an infectious case but tests are not yet positive), through TB infection (infected and well, with a positive tuberculin skin test or interferon-gamma release assay), to TB disease (symptoms and/or radiological signs of active illness). [1] [2]
Exposure
Contact, not yet infected
- Shared air with an infectious source case
- Symptom screen negative; tests pending
- Under-5 and immunocompromised contacts get presumptive therapy
- Reassess and screen at 8–12 weeks
TB infection
Infected, well
- Positive TST or IGRA; normal chest radiograph
- No symptoms of active disease
- Viable bacilli contained; low lifelong progression risk
- Offer tuberculosis preventive treatment to high-risk children
TB disease
Active illness
- Symptoms and/or radiological signs
- Intrathoracic: lymph-node, complicated, cavitary, pleural
- Extrapulmonary: CNS, miliary, lymphatic, bone, abdominal
- Treat with weight-based anti-TB regimen; notify
Once the child has TB disease, classify where it is and how severe it is, because both drive regimen length. Intrathoracic disease is described by the radiological pattern proposed by Marais and colleagues \u2014 from uncomplicated lymph-node enlargement, through complicated lymph-node disease (airway compression or cavitation), to pleural TB and adult-type cavitary disease in older children. Extrapulmonary disease is named by site, with tuberculous meningitis and miliary disease marking the highest-mortality, most urgent forms. [3]
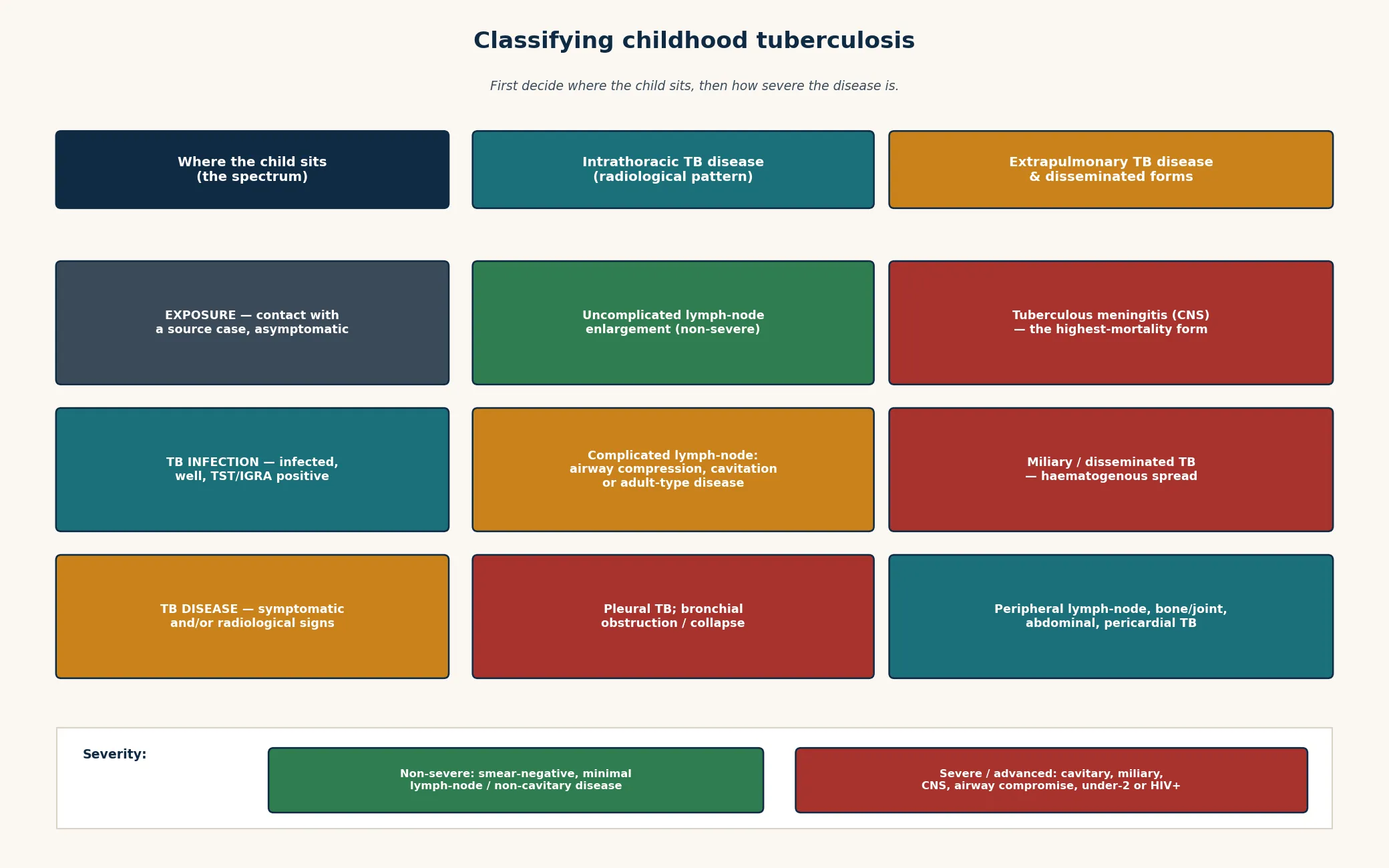
Severity matters because it is now a treatment decision. The SHINE trial defined non-severe TB as minimal, lymph-node or non-cavitary disease (often smear-negative) and showed it can be cured with a shorter 4-month regimen. Severe or advanced disease \u2014 cavitary, miliary, CNS, airway compromise, or disease in an infant, malnourished or HIV-positive child \u2014 still needs the full 6-month course. Naming severity at the bedside is therefore no longer academic; it chooses the regimen. [7]
Epidemiology & Risk Factors
Childhood tuberculosis is common wherever adult TB is common, and it is a disease of inequity. Mathematical modelling by Dodd and colleagues estimates that hundreds of thousands of children develop TB and tens of thousands die of it each year, with the burden concentrated in high-TB-incidence countries and in the most disadvantaged children within them. [4]
In Australia, Aotearoa New Zealand, the UK, the US and Canada, childhood TB is concentrated in children born in or visiting high-incidence countries, in children of migrant and refugee families, and in Indigenous and remote communities \u2014 populations where the upstream adult burden is higher and access to early diagnosis is harder. Recognising who is at risk is the first step to finding disease early. [1]
The contact is the single most powerful risk factor. A child living with an infectious adult is far more likely to be both infected and to progress, and the younger and more immunocompromised the child, the faster that progression. The risk modifiers an examiner expects you to name are young age (especially under five), malnutrition, HIV and other immunocompromise, recent infection (the first two years carry the highest progression risk), and measles. [1] [2]
Pathophysiology
The clinical picture makes sense once you see the central event: inhaled droplet nuclei reach the terminal airway, are taken up by alveolar macrophages, and establish the primary (Ghon) focus. Bacilli then drain to the regional lymph nodes, and the focus plus its draining node form the primary (Ghon) complex \u2014 the hallmark of recent infection in a child. [1] [2]
From there, the outcome depends on whether cell-mediated immunity contains the bacilli. When containment holds, the child has TB infection \u2014 well, with a positive immune test and usually a normal radiograph, harbouring a contained reservoir that only rarely reactivates in childhood. When containment fails, the child develops progressive primary disease within weeks to months: enlarging lymph nodes that compress airways, cavitation, pleural disease, or haematogenous spread to miliary and meningeal disease. [2]
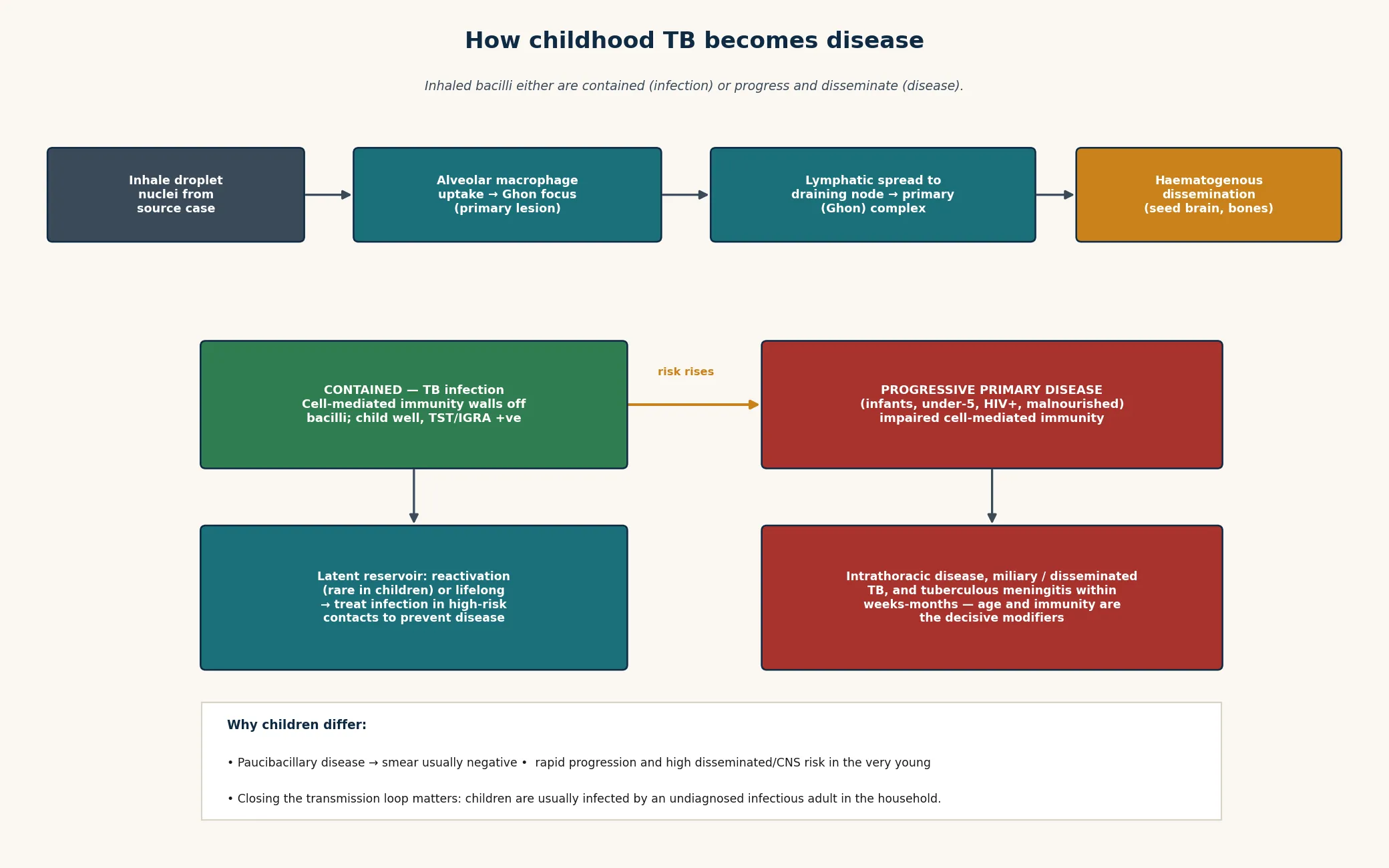
Why infants and immunocompromised children behave so differently is the immaturity or impairment of that cell-mediated response. A two-month-old or a child with HIV cannot wall off the bacilli, so the same inoculum that produces silent infection in an older child produces miliary or meningeal disease in weeks. This is the mechanism behind the rule that an exposed under-five or immunocompromised contact receives presumptive preventive therapy even before infection is confirmed. [1]
Haematogenous dissemination is the route to the two forms an examiner will press you on. Miliary TB follows widespread blood-borne seeding and presents with fever, wasting and diffuse fine nodular shadowing; tuberculous meningitis follows seeding of the meninges and basal ganglia and presents with insidious then progressive neurological decline. Both are diseases of failed containment, and both are emergencies. [6] [2]
Finally, remember that children are usually infected by an undiagnosed infectious adult in the household. The child is rarely the source of transmission \u2014 paucibacillary disease makes children poor transmitters \u2014 which is why finding and treating the source case is how you protect the next child. [1]
Clinical Presentation
A child with TB disease may present in three ways: with an indolent respiratory illness (persistent cough, low-grade fever, failure to thrive over weeks), with an acute severe illness (the febrile, breathless child with miliary disease, or the drowsy child with tuberculous meningitis), or asymptomatically, found through contact screening. The indolent presentation is the common one, and the trap is dismissing weeks of cough as recurrent viral illness. [1]
Intrathoracic TB typically shows a persistent cough and fever for more than two weeks, failure to thrive or weight loss, reduced energy, and sometimes wheeze from airway compression by an enlarged node. Young children may simply stop growing; an older child may report night sweats and haemoptysis. The clue is duration and a compatible contact \u2014 a cough that has not resolved deserves a chest radiograph, not another antibiotic. [1] [3]
Tuberculous meningitis is the presentation you must not miss. It unfolds in stages: a prodrome of vague malaise, irritability and headache (often mistaken for a viral illness), then headache, vomiting and meningism with cranial nerve signs and drowsiness, and finally coma, seizures and focal deficits. Survival and long-term outcome depend on treating in the prodrome, not in the coma \u2014 a febrile, irritable child with a TB contact and a reduced conscious level is presumed TBM until proven otherwise. [6]
Miliary and disseminated TB presents with fever, wasting, hepatosplenomegaly and respiratory distress, with diffuse fine nodular shadowing on the chest radiograph. It is most often seen in infants and immunocompromised children, and it overlaps with septicaemia clinically \u2014 hold sepsis and disseminated TB in the same frame in an ill, febrile child with a TB contact. [1] [2]
The contact screening presentation is the one that rewards a good history: a well child brought in because an adult in the household has been diagnosed with pulmonary TB. Here the child may have no symptoms at all, and the task is to classify (exposure, infection, or unsuspected disease) and to act on that classification. [1]
Differential Diagnosis
The core diagnostic skill is telling apart the three points on the spectrum \u2014 exposure, TB infection and TB disease \u2014 and, once disease is suspected, distinguishing TB from its imitators. A persistent cough and lymph-node radiograph overlap with bacterial and atypical pneumonia, and TB must be held alongside recurrent bacterial infection, foreign-body aspiration, and, in the right child, malignancy involving the mediastinum. [1] [3]
Failure to thrive in a child with TB can be attributed to the wrong cause. Malnutrition itself impairs immunity and is both a risk factor for and a consequence of TB, so the wasted child needs TB considered alongside primary nutritional, endocrine and malabsorptive causes \u2014 and investigated rather than assumed. [1]
Fever in a child from a TB-endemic region demands that imported infection be held in the same frame as common childhood illness. TB, malaria, typhoid and other imported infections overlap, and a child with prolonged fever and a TB contact must not be labelled "a virus" without excluding TB. [1]
Tuberculous meningitis mimics other causes of subacute meningitis and encephalitis \u2014 partially treated bacterial meningitis, viral encephalitis, and fungal meningitis \u2014 and, in its later stages, any cause of raised intracranial pressure. The basal exudate, hydrocephalus and stroke of TBM, plus the CSF lymphocytosis with low glucose and the chest radiograph and contact, are the discriminating features. [6]
[5] [1]Clinical & Bedside Assessment
Open every assessment with the contact, because in childhood TB the contact history is often the most specific finding you will get. Ask specifically who in the household or close circle has had a chronic cough, has been diagnosed with TB, or has died of a respiratory illness; record the source case's drug-susceptibility result if known, because it may decide the child's empiric regimen. [1]
Take a symptom and growth history calibrated to the spectrum. For a contact, screen with the standard four (cough, fever, night sweats, weight loss or failure to thrive) and confirm immunisation including BCG. For a child with suspected disease, map the illness over time \u2014 onset, duration, weight trajectory, and any prior empirical antibiotics \u2014 and ask about the risk modifiers: age, nutrition, HIV status, and recent travel to or residence in a high-incidence country. [1] [4]
Examine for the disease and its complications. Look for wasting, pallor and lymphadenopathy; listen for focal findings, wheeze or stridor from airway compression; palpate for hepatosplenomegaly in suspected disseminated disease; and perform a full neurological assessment for any child with a TB contact and headache, irritability or reduced conscious level. The chest is often quieter than the radiograph suggests \u2014 in a child, the radiograph carries more weight than the stethoscope. [1] [3]
Synthesise a problem representation before you investigate: for example, "a thin four-year-old with six weeks of cough and fever, a household TB contact, and a chest radiograph showing right paratracheal lymph-node enlargement \u2014 suspected intrathoracic TB disease, paucibacillary." That representation decides the sampling strategy and the empiric decision. [1]
Communicate from the first visit that TB is treatable and that the whole household is now part of the plan \u2014 because contact tracing, adherence support and source-case finding all depend on the family trusting the team. Use a trained interpreter for migrant and refugee families; never use the child as interpreter. [1]
Investigations
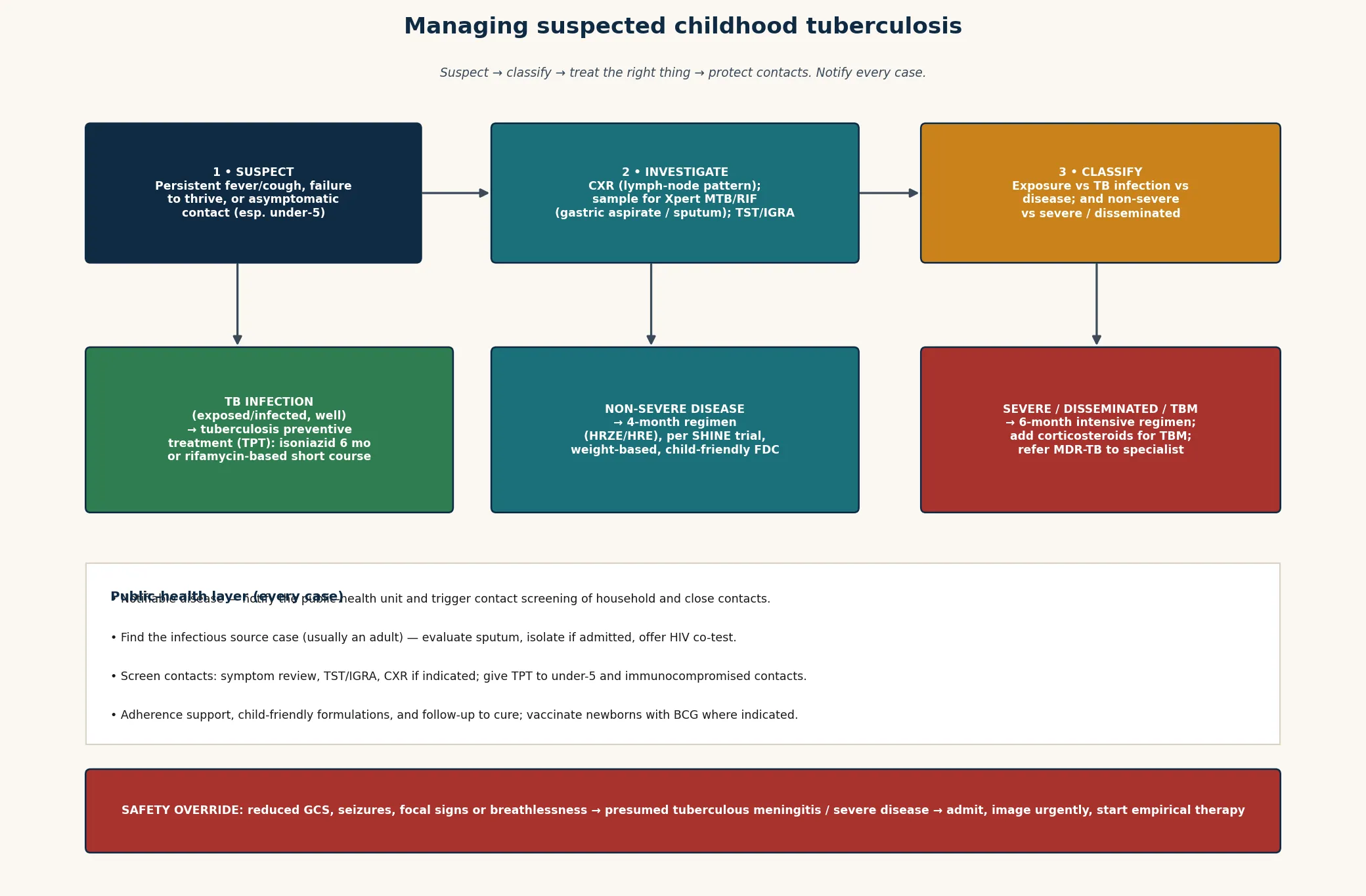
The investigation strategy has three limbs: confirm the disease microbiologically where possible, image the chest (and other sites as indicated), and use immune-based tests (TST or IGRA) to establish infection in a well contact. Each limb answers a different question, and confusing them is a common error. [1] [5]
Microbiology first. Obtain a respiratory sample for Xpert MTB/RIF (or Xpert MTB/RIF Ultra) \u2014 a molecular test that detects M. tuberculosis DNA and rifampicin resistance within hours. In a young child who cannot expectorate, collect an early-morning gastric aspirate (two to three samples) or, where available, an induced sputum or stool sample. Xpert is more sensitive than smear in children, but a negative result does not exclude disease because childhood TB is paucibacillary. Culture and phenotypic drug-susceptibility testing remain the reference standard and should be sent in parallel. [5]
Imaging. The chest radiograph is central and often diagnostic in a child: look for lymph-node enlargement (especially hilar or paratracheal), the primary complex, segmental or lobar collapse from airway compression, cavitation in older children, and the diffuse fine nodular pattern of miliary disease. Use the radiological classification to describe what you see. A computed tomography scan adds detail for complicated airway disease; for suspected tuberculous meningitis, brain imaging shows basal exudate, hydrocephalus and infarction, and must be combined with lumbar puncture. [3] [6]
Immune-based tests. The tuberculin skin test (TST, Mantoux) and the interferon-gamma release assay (IGRA) indicate TB infection, not disease, and they are used to screen contacts and to support a disease diagnosis. Neither can rule TB in or out on its own. IGRA does not cross-react with BCG and needs a single visit, which suits older children; TST remains useful, especially in young children. A systematic review confirms that IGRA performs better than a single TST but should be interpreted alongside the clinical picture, not in isolation. [8]
Which sample, in which child?
- Suspected intrathoracic TB disease: two to three early-morning gastric aspirates (or induced sputum/stool) for Xpert MTB/RIF Ultra plus culture; chest radiograph; TST or IGRA; HIV test.
- Well contact (screening): symptom screen, TST and/or IGRA, and chest radiograph if infection is confirmed or symptoms are present; children under five and immunocompromised contacts get chest radiograph and presumptive therapy early.
- Suspected tuberculous meningitis: urgent brain imaging, lumbar puncture (CSF for cell count, protein, glucose, AFB, Xpert and culture), and a chest radiograph and contact screen; treat empirically on suspicion.
- Suspected miliary/disseminated TB: chest radiograph, blood and sample cultures, and consideration of ocular fundoscopy (choroid tubercles) and imaging of other seeded sites.
Always test for HIV in any child with confirmed or suspected TB, because co-infection changes both risk and management, and screen household contacts regardless of the child's own result. Interpret the immune-based test against the child's BCG status, age and immune function, and never let a single negative test delay treatment of a clinically compatible disease. [1] [8]
Management — Resuscitation
The resuscitation step in childhood TB is the immediate-life-threat override: the child who cannot wait for the routine diagnostic pathway. Reduced consciousness, seizures or focal signs in a febrile child with a TB contact is presumed tuberculous meningitis \u2014 image urgently, send CSF, and start empirical anti-TB therapy with corticosteroids without waiting for confirmation. [6]
Miliary or disseminated TB with respiratory distress and hepatosplenomegaly is treated as both sepsis and disseminated TB: resuscitate, take cultures including samples for Xpert, begin empirical anti-TB therapy on suspicion, and manage respiratory and haemodynamic failure in parallel. Hold sepsis and disseminated TB in the same frame in the ill, febrile at-risk child. [1]
Airway compromise from a complicated lymph-node complex \u2014 stridor, severe wheeze, or acute collapse \u2014 is a respiratory emergency: assess and stabilise the airway, image, and involve ENT and infectious diseases, because manipulation of a compressing node mass can precipitate complete obstruction. [1] [3]
Stabilise and treat, then organise the public-health response in the same breath: notify, identify and isolate the source case if admitted, and trigger contact tracing, because the child's acute presentation is also a signal that an infectious adult is still transmitting in the household. [1]
Management — Definitive & Stepwise
Definitive management is decided entirely by where the child sits on the spectrum, so re-state the classification before you prescribe. TB infection in a high-risk child receives tuberculosis preventive treatment; non-severe TB disease receives a 4-month regimen; severe TB disease receives a 6-month regimen; tuberculous meningitis receives a longer intensive phase with corticosteroids. [1] [7]
The treatment pathway by classification
Exposure (high-risk contact)
Under-five or immunocompromised household contact: presumptive preventive therapy after excluding disease, then re-screen at 8–12 weeks.
TB infection (well, test-positive)
Tuberculosis preventive treatment for high-risk children — isoniazid for the classic course or a shorter rifamycin-based regimen per WHO/NICE — to prevent future disease.
Non-severe TB disease
Weight-based 4-month regimen (intensive phase then continuation) with child-friendly fixed-dose combinations, validated by the SHINE trial for minimal, lymph-node or non-cavitary disease.
Severe / advanced TB disease
Weight-based 6-month regimen (two-month intensive phase with four drugs then continuation); add corticosteroids for tuberculous meningitis; refer MDR-TB to a specialist service.
Use child-friendly, weight-based fixed-dose combinations and adjust to weight at every visit, because children outgrow their dose during months of therapy and under-dosing drives resistance and relapse. Adherence is the single biggest determinant of cure, so build in directly-observed support, family education, and a clear follow-up plan from the first dose. [1]
For tuberculous meningitis, start a longer intensive regimen immediately and add corticosteroids, which reduce mortality and severe disability; manage raised intracranial pressure and hydrocephalus with neurosurgical input. The outcome hinges on how early treatment begins, which is why TBM is treated on suspicion. [6]
Anti-TB therapy in children \u2014 the principle, not the milligram
For drug-resistant TB, do not improvise: involve an infectious-disease or TB specialist service, design the regimen around the source case's susceptibility pattern and the child's own results, and use child-friendly formulations of the second-line and newer agents that paediatric programmes now make available. [1]
Specific Subtypes & Scenarios
Intrathoracic (pulmonary) TB is the commonest form and the one you will manage most. Confirm microbiologically where possible, classify severity, and choose the 4- or 6-month regimen accordingly. The chest radiograph showing lymph-node enlargement in a symptomatic child with a contact is, in practice, enough to treat when samples are negative. [1] [3]
Tuberculous meningitis is the highest-mortality, most examinable form. Treat on suspicion with an extended intensive regimen and corticosteroids, control intracranial pressure, and counsel the family honestly about outcome \u2014 because even with optimal care, mortality and long-term disability remain substantial, and early treatment is the only modifiable factor. [6]
Miliary and disseminated TB in an infant or immunocompromised child is an emergency that overlaps with sepsis: admit, take samples for Xpert and culture, begin empirical therapy, and search for other seeded sites. The diffuse nodular radiograph and hepatosplenomegaly in a febrile, wasted child are the signature. [1] [2]
Peripheral lymph-node TB presents with painless, matted cervical adenopathy; diagnosis rests on aspiration or biopsy for Xpert, culture and histology, and treatment is medical with the standard regimen \u2014 surgery is reserved for diagnostic sampling or refractory cases. [1]
The under-five and immunocompromised contact is a scenario that tests whether you know the spectrum. These children receive presumptive preventive therapy after disease is excluded, because their risk of rapid progression to severe disease outweighs the small cost of treatment. [1]
The adolescent with adult-type cavitary TB behaves more like an adult: higher bacillary load, smear-positive, genuinely infectious, and at risk of reactivation later. Treat with the full regimen, counsel about transmission, and address adherence and the developmental drivers of it. [1]
Congenital and neonatal TB are rare but lethal when missed, arising from haematogenous or aspirated spread in a mother with TB; they present with non-specific sepsis-like illness, hepatosplenomegaly and respiratory failure in the first weeks of life, and demand a high index of suspicion in an infant whose mother has TB. [1]
Complications & Pitfalls
The most dangerous pitfall is withholding treatment while waiting for microbiology. Because childhood TB is paucibacillary, smears and even Xpert are often negative; treating on a compatible clinical and radiological picture with a supportive contact, after collecting the best samples, is correct practice \u2014 not a shortcut. [5] [1]
Missing tuberculous meningitis in its prodrome is the pitfall with the highest cost. A febrile, irritable child with a TB contact and any neurological sign is presumed TBM until proven otherwise; the cost of imaging and treating on suspicion is small, and the cost of waiting is death or severe disability. [6]
[6]Diagnostic overshadowing cuts both ways. Attributing weeks of cough to recurrent viral illness, or weight loss to malnutrition alone, delays TB diagnosis; conversely, over-calling non-specific radiological findings as TB in a child with another cause wastes time. Anchor on the contact, the duration, the radiograph and the microbiology together. [1]
Under-dosing during therapy is a silent pitfall: children gain weight across months of treatment, and a fixed dose that was correct at diagnosis becomes sub-therapeutic \u2014 a recognised driver of relapse and resistance. Re-weigh and adjust the dose at every visit. [1]
Failing to notify, trace contacts and find the source case leaves the transmission loop open. The next child in the household is the one who will present with miliary or meningeal disease, so the public-health response is part of the treatment, not an afterthought. [1]
Finally, overlooking drug resistance \u2014 by not asking for the source case's susceptibility result or not sending the child's own samples for culture and susceptibility \u2014 means treating a resistant organism with a susceptible regimen, which fails. Always design the regimen with resistance in mind. [1] [5]
Prognosis & Disposition
Prognosis in childhood TB is excellent when disease is treated early with an adherent, weight-based regimen \u2014 cure rates for drug-susceptible disease are high. The modifiers of a poor outcome are severe or disseminated disease, tuberculous meningitis, infancy, immunocompromise, malnutrition, drug resistance, and any failure of adherence. [1] [7]
Tuberculous meningitis is the prognosis that defines the topic. Mortality and long-term neurological disability remain substantial even with optimal therapy, and the single most important determinant is the stage at which treatment begins \u2014 which is why TBM is treated on suspicion. Counsel families honestly and early. [6]
Routine disposition is outpatient therapy with directly-observed or supported adherence for uncomplicated disease, after the diagnostic samples are collected and the public-health notification is made. Admit any child with miliary or disseminated disease, airway compromise, tuberculous meningitis, severe malnutrition, or a social situation that cannot support adherence. [1]
Safety-net explicitly: review in days for any new neurological symptom, respiratory distress or deterioration; monitor weight, adherence and adverse effects at planned intervals; and confirm microbiological and susceptibility results as they return, adjusting the regimen if needed. [1]
Long-term, treated TB infection and cured TB disease carry an excellent outlook, and the family does best when the contact tracing, source-case treatment and preventive care are completed together rather than abandoned once the index child improves. [1]
Special Populations
Infants and children under five. Their immature cell-mediated immunity drives rapid progression to severe, disseminated and meningeal disease, so an exposed under-five contact receives presumptive preventive therapy after disease is excluded, and any disease is treated as higher-risk. [1] [2]
Immunocompromised children (HIV, primary immunodeficiency, immunosuppression). Progression is faster, disease is more often disseminated and atypical, and immune-based tests may be falsely negative, so maintain a low threshold to investigate and treat empirically, and coordinate HIV and TB care together. [1]
Migrant, refugee and asylum-seeking children. Born in or transiting high-incidence countries, they carry a higher background burden and may have incomplete BCG and records; apply the catch-up TB screen (symptom review, TST/IGRA, chest radiograph as indicated) within the broader on-arrival health assessment, using a trained interpreter. [4]
Indigenous and remote-community children. Higher upstream adult burden, later presentation, and fragmented access combine to worsen outcomes; build deliberate pathways including telehealth-supported TB care and culturally safe contact tracing. [4]
Malnourished children. Malnutrition is both cause and consequence of TB, worsens outcome, and changes weight-based dosing, so address nutrition and TB together and re-weigh frequently. [1]
Adolescents with adult-type disease. Higher bacillary load makes them genuinely infectious; treat the full regimen, counsel about transmission, and attend to the developmental and adherence challenges that drive poor outcomes in this group. [1]
Evidence, Guidelines & Regional Differences
The comprehensive review. Perez-Velez and Marais's New England Journal of Medicine review of tuberculosis in children remains the single best fellowship-level anchor for the spectrum, the pathophysiology and the approach to diagnosis and treatment. [1]
The natural history and the radiograph. Marais and colleagues' pre-chemotherapy-era reconstruction of the natural history of childhood intra-thoracic TB, and their proposed radiological classification, define how we still think about lymph-node disease, airway compression and progression. [2] [3]
The burden, quantified. Dodd and colleagues' mathematical modelling study established the scale of childhood TB mortality and concentrated global attention on a previously under-counted disease. [4]
Diagnosis \u2014 molecular and immunological. The Cochrane review of Xpert MTB/RIF and Xpert MTB/RIF Ultra in children underpins the move to gastric-aspirate and sputum molecular testing, while the systematic review of interferon-gamma release assays in children anchors the place of IGRA alongside the TST. [5] [8]
Turkova et al, 2022 \u2014 the SHINE trial
Multicentre randomised controlled non-inferiority trial
Population: African and Indian children and adolescents with non-severe (minimal, lymph-node or non-cavitary) tuberculosis
Key finding
A 4-month treatment regimen was non-inferior to the standard 6-month regimen for non-severe TB in children.
Practice change
Classify severity at the bedside and use the shorter 4-month regimen for non-severe disease, reserving the 6-month course for severe or disseminated TB.
Tuberculous meningitis. Seddon and colleagues' review of the global situation for TBM sets out the epidemiology, diagnostics, treatment and outcomes of the highest-mortality form, anchoring the case for early empirical treatment with corticosteroids. [6]
ANZ: Australia and New Zealand run TB through public-health units and specialist TB services; notification is mandatory, contact tracing is centralised, BCG is offered to high-risk neonates, and CDNA guidance frames the national response. UK: NICE NG33 sets investigation and management for children and young people, with a strong public-health and contact-tracing infrastructure; BCG is offered to high-risk neonates. US: the CDC frames TB testing and treatment in children and adolescents, with state and local public-health departments running contact investigation; BCG is not used routinely. Canada: provincial TB programmes lead, with the Canadian Tuberculosis Standard guiding care; BCG policies vary by province and northern programme.
State the principle and verify the operational detail. Regimen composition, exact mg/kg doses, weight-band tables and preventive-therapy choices follow current WHO Module 5 and NICE NG33 guidance \u2014 check the live national guideline before prescribing, because these evolve. [1]
Exam Pearls
- Open every answer with the spectrum \u2014 exposure, infection, disease \u2014 because misclassifying the child is the root of every wrong decision. [1]
- A febrile, irritable child with a TB contact and any neurological sign is tuberculous meningitis until proven otherwise; treat on suspicion. [6]
- Childhood TB is paucibacillary \u2014 a negative smear or Xpert does not exclude disease; treat on a compatible picture. [5]
- Non-severe disease now gets a 4-month regimen (SHINE); severe and uncomplicated miliary disease usually get 6 months; CNS (TB meningitis) still requires 12 months (2HRZE/10HR), with a conditional WHO 2022 6-month intensive alternative (6HRZEto) for carefully selected non-HIV cases. [7]
References
- [1]Perez-Velez CM, Marais BJ Tuberculosis in children. N Engl J Med, 2012.PMID 22830465
- [2]Marais BJ, Gie RP, Schaaf HS, et al The natural history of childhood intra-thoracic tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis, 2004.PMID 15141729
- [3]Marais BJ, Gie RP, Beyers N, et al A proposed radiological classification of childhood intra-thoracic tuberculosis. Pediatr Radiol, 2004.PMID 15300340
- [4]Dodd PJ, Yuen CM, Sismanidis C, Seddon JA, Jenkins HE The global burden of tuberculosis mortality in children: a mathematical modelling study. Lancet Glob Health, 2017.PMID 28807188
- [5]Kay AW, Chileshe C, Vargas D, et al Xpert MTB/RIF and Xpert MTB/RIF Ultra assays for active tuberculosis and rifampicin resistance in children. Cochrane Database Syst Rev, 2020.PMID 32853411
- [6]Seddon JA, Tugume L, Solomons R, et al The current global situation for tuberculous meningitis: epidemiology, diagnostics, treatment and outcomes. Wellcome Open Res, 2019.PMID 32118118
- [7]Turkova A, Wobudeya E, Waja W, et al Shorter Treatment for Nonsevere Tuberculosis in African and Indian Children. N Engl J Med, 2022.PMID 35263517
- [8]Machingaidze S, Wiysonge CS, Gonzalez-Angulo Y, et al The utility of an interferon gamma release assay for diagnosis of latent tuberculosis infection and disease in children: a systematic review and meta-analysis. Pediatr Infect Dis J, 2011.PMID 21427627