Paeds · infectious-diseases
Undifferentiated fever and fever without a source in infants and children
Also known as Fever without a source · FWS · Febrile infant · Undifferentiated fever · Occult serious bacterial infection · Fever without localising signs
A fellowship-level approach to the infant or child with fever and no localising clinical source. Covers the precise definition of fever, age-stratified risk (neonate through older child), named prediction rules (PECARN, Boston, Rochester, Philadelphia), the NICE traffic-light system, biomarker interpretation, empiric antibiotics, disposition and safety-netting across ANZ, UK, US and Canadian practice.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A febrile child walks through your door. They are hot to touch, irritable, and the parent is worried. There is no runny nose, no obvious rash, no localising story — just fever. This is the single most common paediatric presentation to emergency departments worldwide, and the clinical question is always the same: is this a self-limiting viral illness, or is a serious bacterial infection brewing that will cause harm if I wait? [6] [13]
Fever is defined as a rectal temperature of ≥38 °C (100.4 °F). In clinical practice, axillary, tympanic and oral measurements are used with varying accuracy, but the rectal temperature remains the reference standard in infants and young children. [6] [14]
Fever without a source (FWS) is fever for which history and physical examination do not reveal a clear cause. This is distinct from fever of unknown origin (FUO), which implies prolonged or recurrent fever (typically more than 7–14 days) requiring a different diagnostic workup. The acute undifferentiated fever is what you face in the emergency department: a child who has been febrile for hours to a few days, looks unwell or well, and needs a decision now. [6] [7]
Classification
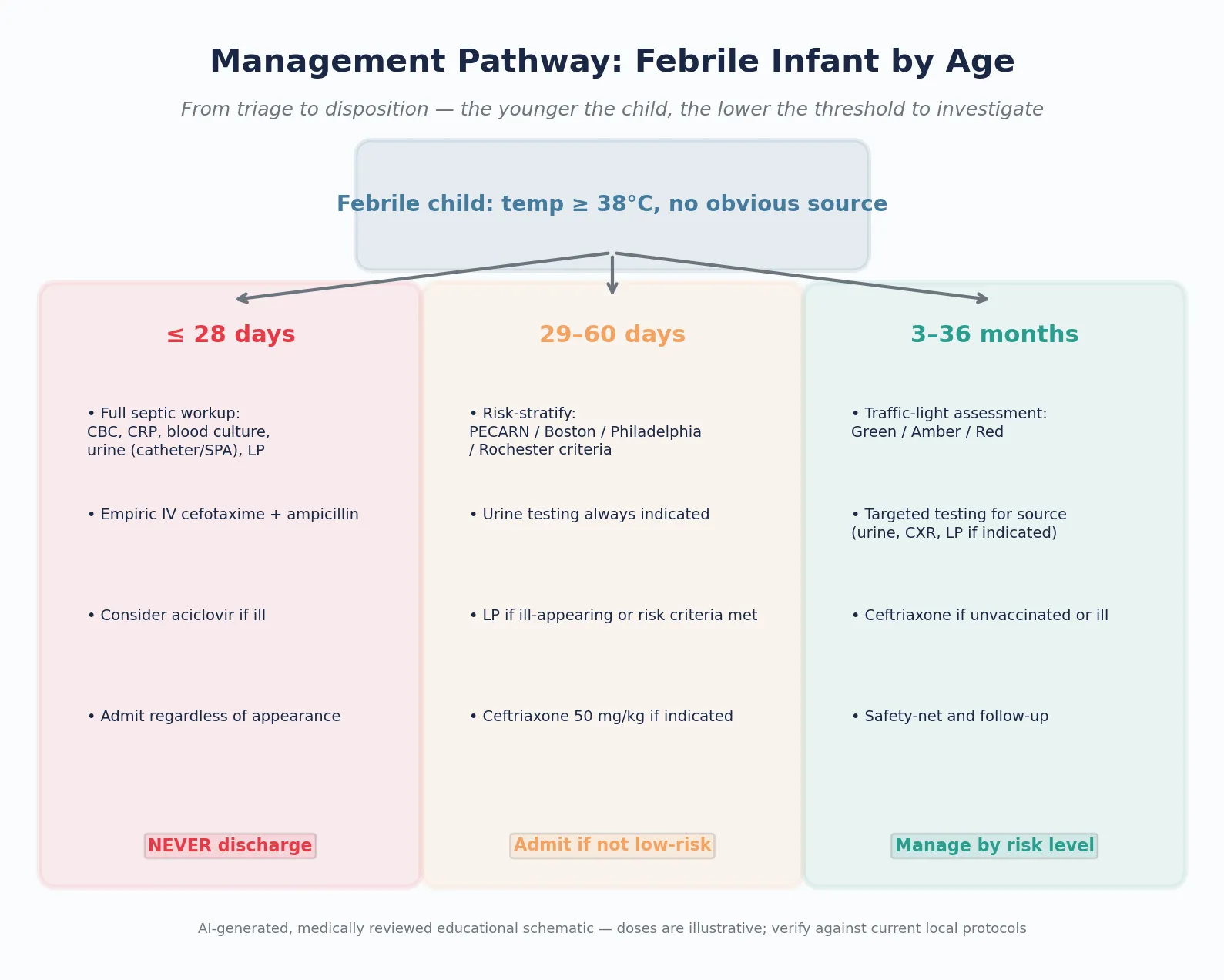
The approach to the febrile child is classified primarily by age, because the risk of SBI and the reliability of clinical assessment change dramatically across age bands. Three age groups drive the decision-making, each with a different balance of risk, investigation and disposition. [6] [13]
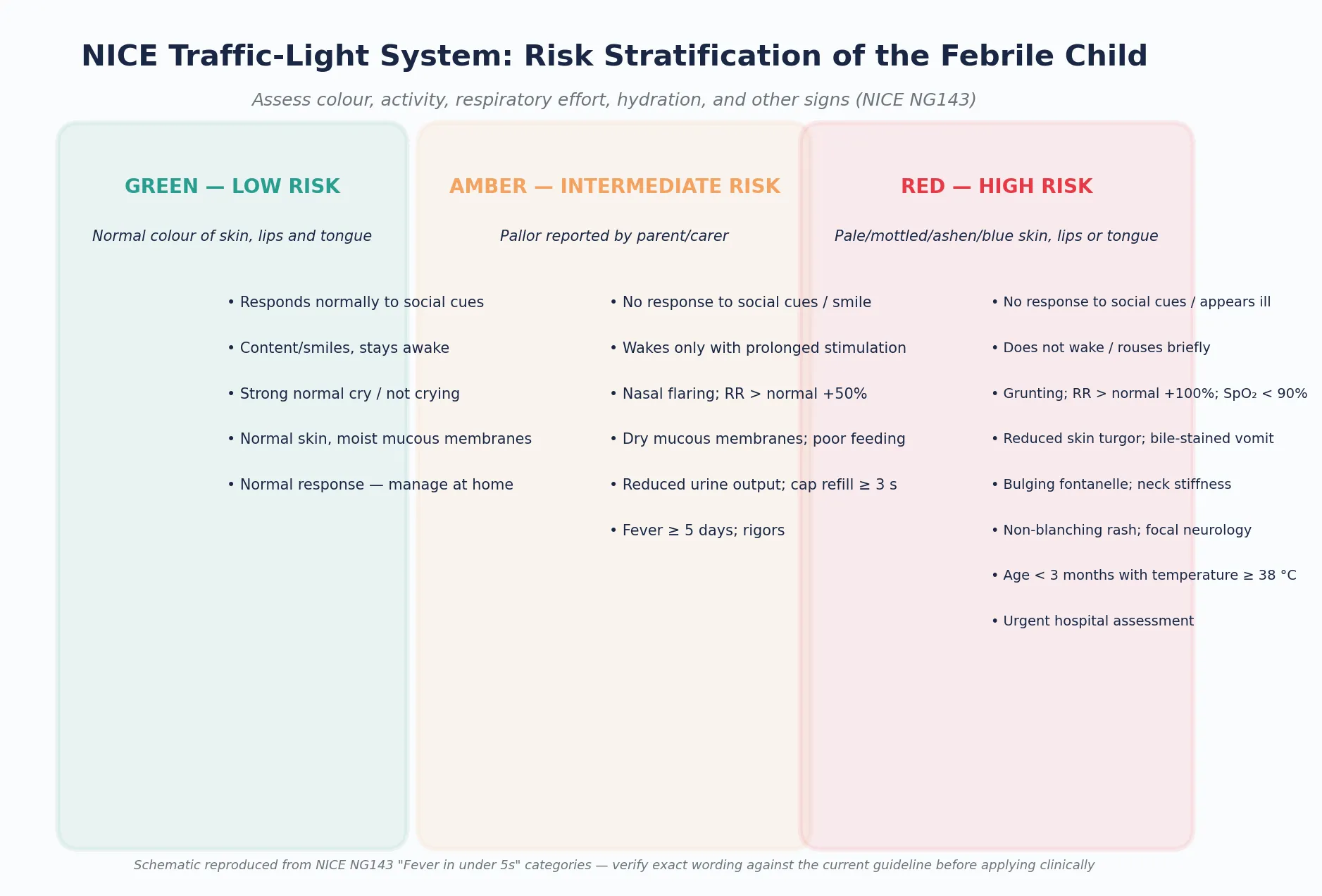
The NICE traffic-light system is the most widely used bedside risk-stratification tool for febrile children under 5. It assesses five domains: colour of skin, lips and tongue; activity and social response; respiratory effort; hydration and mucous membranes; and other specific red-flag signs such as non-blanching rash, neck stiffness, or bulging fontanelle. A child in the green zone may be managed at home with antipyretics and a clear safety-net. An amber child needs same-day assessment by a clinician. A red child needs urgent hospital assessment. [13]
≤28 days
Neonate
- Highest baseline SBI risk (~8-12%)
- Clinical signs unreliable
- Full septic workup mandatory
- Never discharge; always admit and treat empirically
29–90 days
Young infant
- Moderate SBI risk (~3-8%)
- Risk-stratify with PECARN, Boston, Rochester or Philadelphia
- Urinalysis always indicated
- Disposition depends on risk category and local protocol
3–36 months
Infant or young child
- Lower SBI risk in vaccine era (~0.5-2% occult bacteraemia)
- Traffic-light assessment and targeted testing
- Empiric antibiotics only if unvaccinated or ill-appearing
- Safety-net and close follow-up
≥36 months
Older child
- Lowest SBI risk
- Clinical assessment usually localises source
- Investigate based on history and examination
- Most managed as outpatients
Epidemiology & Risk Factors
Fever is the reason for up to 30% of paediatric emergency presentations. The vast majority are viral and self-limiting, but a small proportion harbour SBI. The risk is not uniform: it falls steeply with age, driven by the maturation of the immune system and the accumulation of vaccine-conferred immunity. [6] [13]
Several factors increase the risk that a febrile child has SBI. The most powerful is young age — infants under 90 days have a substantially higher baseline risk, which is why the approach to them is protocol-driven rather than clinician-discretion-based. [1] [11]
Host factors
- Age under 90 days (primary risk driver)
- Prematurity or ex-preterm (corrected age matters)
- Immunocompromise or oncology treatment
- Congenital heart disease or asplenia
- Indwelling central venous catheter or VP shunt
- Incomplete immunisation status
Fever characteristics
- Fever ≥39 °C in infants under 90 days
- Fever duration ≥2 days without improvement
- Rigors or shaking chills
- Very high or very low white cell count
- Elevated CRP or procalcitonin
Clinical appearance
- Ill-appearing or toxic on examination
- NICE red-category signs
- Abnormal paediatric assessment triangle
- Caregiver concern that the child is not right
- Re-presentation within 24-48 hours
Social context
- Rural or remote location with delayed access to care
- Language barriers to safety-netting
- Socioeconomic disadvantage
- Aboriginal, Torres Strait Islander or Māori heritage with higher SBI prevalence
- Out-of-home care or safeguarding concerns
The introduction of conjugate vaccines against Haemophilus influenzae type b (Hib) and Streptococcus pneumoniae (PCV) has transformed the epidemiology. In the pre-vaccine era, occult bacteraemia in well-appearing febrile children 3-36 months occurred in 3-5% and was most commonly caused by S. pneumoniae. In the post-PCV era, this has fallen below 1% in vaccinated populations, fundamentally changing the threshold for empiric antibiotics in this age group. [12] [13]
Pathophysiology
Why are young infants so much more vulnerable to serious bacterial infection? The answer lies in three overlapping vulnerabilities that converge in the first three months of life. [6] [7]
First, the immune system is immature. Neonatal neutrophils have reduced chemotaxis and phagocytic capacity. The alternative complement pathway is less active. Transplacentally acquired maternal IgG — which provides passive protection in the first weeks — nadir at 3-12 weeks of age, creating a vulnerability window before the infant's own antibody production ramps up. This is why infants aged 1-3 months are at particularly high risk. [6] [7]
Second, pathogen exposure is different. In the neonatal period, organisms acquired from the maternal genital tract dominate: Group B Streptococcus, Escherichia coli, and Listeria monocytogenes. As the infant grows, the pathogen profile shifts toward respiratory viruses, S. pneumoniae, uropathogenic E. coli, and community-acquired organisms. [6]
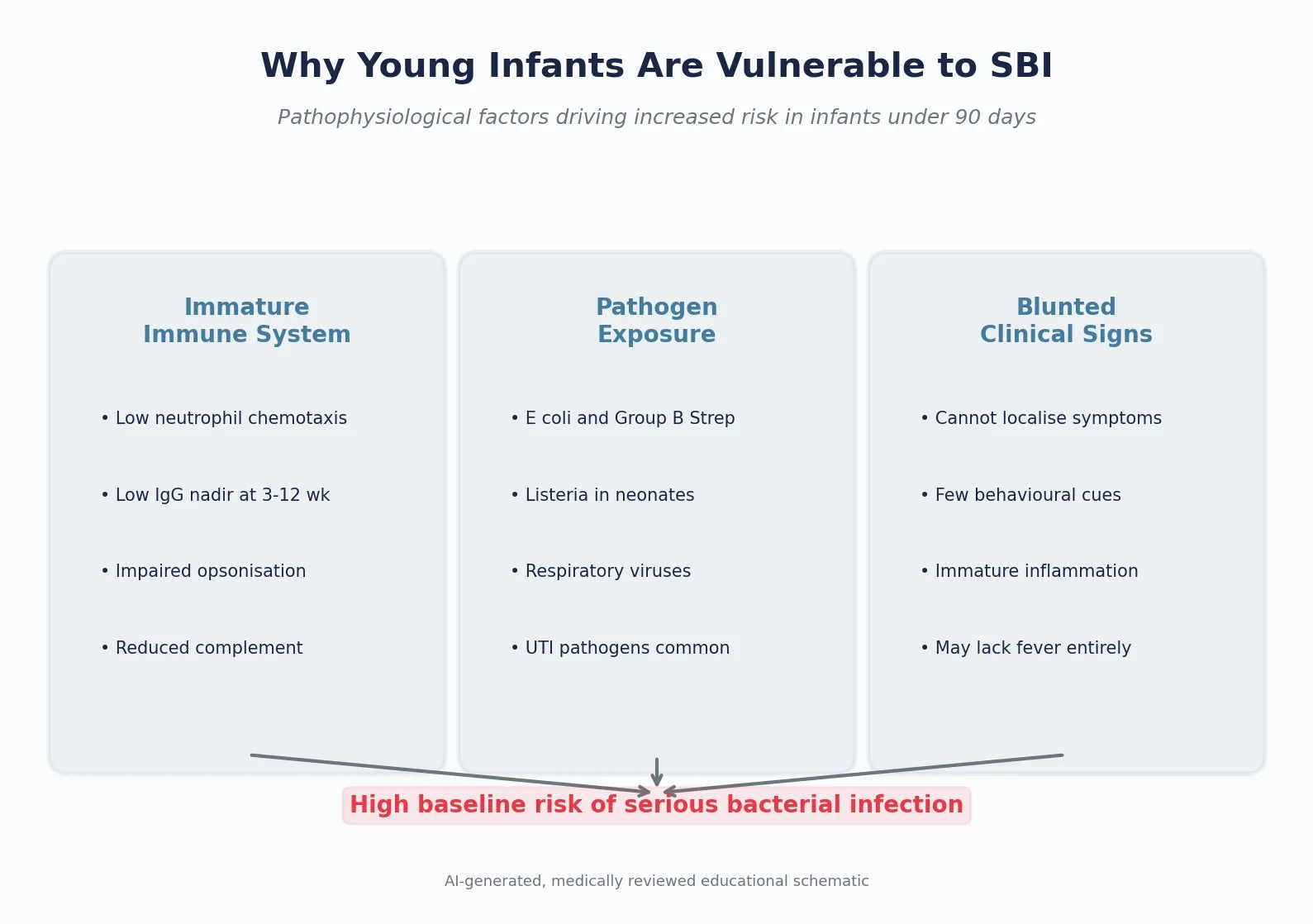
Third, clinical signs are blunted. A neonate with meningitis may not have neck stiffness, bulging fontanelle, or fever — they may simply feed poorly, be irritable, or have an abnormal cry. The immature inflammatory response means the usual signs of sepsis may be attenuated or absent. This is why clinical judgement alone cannot safely exclude SBI in this age group, and why protocol-driven investigation is mandatory. [6]
The febrile response itself is mediated by prostaglandin E2 acting on the hypothalamic thermoregulatory centre, typically in response to pyrogenic cytokines (IL-1, IL-6, TNF-alpha) released during infection. Fever is a host response, not a direct measure of pathogen virulence. Viral infections commonly produce high fever, and bacterial infections may present without fever (particularly in neonates). This disconnect between fever and infection severity is one of the fundamental challenges in the febrile child assessment. [7]
Clinical Presentation
The focused history and examination of the febrile child serve two purposes: to find a source if one exists, and to assess the severity of illness. Both must happen quickly and in parallel with initial stabilisation if the child is unwell. [6] [13]
History
Ask about the duration, height and pattern of fever (continuous versus intermittent), associated symptoms (cough, breathing difficulty, vomiting, diarrhoea, rash, urine output, feeding, activity), immunisation status, sick contacts, recent travel, animal exposure, and any significant past medical history including prematurity, congenital conditions or recurrent infections. Ask what the caregiver is most worried about — caregiver concern is a validated predictor of serious illness. [6] [13]
Examination
Observe before touching. Use the paediatric assessment triangle to form a rapid first impression: Appearance, Work of Breathing, and Circulation to Skin. Then proceed to a head-to-toe examination looking for a source: tympanic membranes, oropharynx, neck (lymph nodes, stiffness), chest (auscultation), abdomen (tenderness, organomegaly), skin (rash, cellulitis), joints (swelling, warmth, reduced movement), and in infants, the fontanelle. [6] [7]
| Domain | Red flag finding |
|---|---|
| Colour | Pale, mottled, ashen or blue |
| Activity | No response to social cues; appears ill to a health professional |
| Consciousness | Does not wake, or rouses only with prolonged stimulation; weak high-pitched cry |
| Respiratory | Grunting; respiratory rate well above normal; moderate or severe chest indrawing; SpO₂ ≤95% in air (NICE intermediate/amber feature; <90% is a higher-risk red feature) |
| Circulation | Reduced skin turgor; capillary refill 3 seconds or more |
| Other | Bile-stained vomiting; age under 3 months with temperature ≥38 °C (red); age 3–6 months with temperature ≥39 °C is amber/intermediate in NICE NG143 rather than red; non-blanching rash; bulging fontanelle; neck stiffness; focal neurology; status epilepticus |
The critical distinction is between well-appearing and ill-appearing. A well-appearing child interacts normally, smiles, plays, has good tone, and has normal colour and perfusion. An ill-appearing child is lethargic, poorly interactive, has abnormal colour or perfusion, or has any red-flag sign. This distinction is central but imperfect — a well-appearing young infant can still have SBI, which is why age overrides appearance in the under-90-day group. [6] [13]
Differential Diagnosis
The differential for the febrile child without a source is broad and spans from trivial to life-threatening. The practical framework is to divide causes into serious bacterial infection, viral infection, and non-infectious causes. [6] [12]
Serious bacterial infection
- UTI — the most common SBI in infants under 2 years
- Bacteraemia — occult or with a focus
- Meningitis or encephalitis — including HSV in neonates
- Pneumonia — may occur without respiratory signs
- Osteomyelitis or septic arthritis — focal bone or joint findings may be subtle in non-verbal children
- Cellulitis or soft-tissue infection
- Gastroenteritis with bacterial cause (Salmonella, Shigella, Campylobacter)
Viral infection
- Enterovirus and parechovirus — common cause of aseptic meningitis in summer
- Respiratory viruses — RSV, influenza, parainfluenza, adenovirus
- Roseola (HHV-6) — high fever followed by rash on defervescence
- Adenovirus — pharyngitis, conjunctivitis, fever
- COVID-19
- Other systemic viral syndromes
Non-infectious causes
- Over-bundling — environmental overheating (resolves on unwrapping)
- Dehydration fever — particularly in neonates
- Kawasaki disease — fever ≥5 days with criteria
- Malignancy — leukaemia, neuroblastoma presenting with fever
- Drug fever or adverse reaction
- Autoimmune or autoinflammatory disease
The most important can't-miss diagnosis in a febrile neonate is HSV encephalitis. Neonatal HSV may present with fever, seizures, vesicular rash (which may be absent), lethargy, or poor feeding — and it can be fatal or devastating if not treated early. Consider empiric aciclovir in any neonate with fever and a concerning presentation (seizure, vesicular lesions, maternal HSV history, CSF pleocytosis, or liver dysfunction). [6] [20]
Enterovirus and parechovirus are the most common causes of aseptic meningitis in young infants, particularly in summer and autumn. While generally self-limiting, they cause significant morbidity (hospitalisation, unnecessary antibiotics) and are an important consideration in the evaluation of the febrile infant with CSF pleocytosis. Enterovirus PCR can shorten hospital stay by confirming a viral cause. [19] [20]
Clinical & Bedside Assessment
The bedside assessment of the febrile child is built on three pillars: the first impression (paediatric assessment triangle), the focused history and examination (to find a source and assess severity), and the serial reassessment (to detect deterioration or confirm improvement). [6] [13]
Temperature measurement requires attention to method. In infants under 6 months, tympanic thermometry is unreliable — use axillary or rectal measurement. Rectal temperature is the gold standard but may not be practical or acceptable in all settings. Document the method used, as this affects interpretation. [6]
The assessment of hydration and perfusion is critical. Look for dry mucous membranes, sunken eyes, reduced skin turgor, delayed capillary refill (3 seconds or more), cool peripheries, and reduced urine output. In the febrile child, tachycardia may reflect fever, dehydration, or early shock — the response to a fluid bolus helps distinguish these. [6] [13]
Structured assessment of the febrile child without a source
First impression
Apply the paediatric assessment triangle. If the child is ill-appearing, call for help and start ABCDE.
History
Fever duration, height, pattern. Associated symptoms. Immunisation status, sick contacts, travel, animals. Past medical history and prematurity. Caregiver concern.
Examination
Head-to-toe: tympanic membranes, oropharynx, neck, chest, abdomen, skin, joints, fontanelle. Look for a source.
Risk stratify by age
Neonate ≤28 days: full workup. 29-90 days: apply prediction rule. 3-36 months: traffic-light system. Older: targeted testing.
Investigate
Urinalysis (catheter or SPA in non-toilet-trained). Bloods if indicated by age or risk. LP if indicated. CXR if respiratory signs.
Decide disposition
Admit, observe, or discharge with a documented safety-net. The safety-net must be specific, written and actionable.
Reassess
Re-examine after every intervention and at handover. If the child returns, start the assessment from the beginning.
Investigations
The investigation strategy is driven by age and clinical appearance. The younger the child, the more comprehensive the workup, because the pre-test probability of SBI is higher and the clinical signs are less reliable. [1] [6]
Febrile neonate (≤28 days)
Every febrile neonate gets a full septic workup: full blood count, blood culture, urinalysis and culture (by catheterisation or suprapubic aspiration — not bag collection, which has an unacceptably high contamination rate), lumbar puncture with CSF cell count, differential, protein, glucose, Gram stain and culture. This is non-negotiable regardless of how well the infant appears. [6] [11]
Febrile young infant (29-90 days)
Risk stratify with a named prediction rule. The most widely validated contemporary rule is the PECARN prediction rule (Kuppermann 2019), which uses a urinary biomarker (urinary neutrophil gelatinase-associated lipocalin, uNGAL), absolute neutrophil count (ANC), procalcitonin and CRP to identify infants at low risk for invasive bacterial infection. The PECARN rule does not require LP for its low-risk definition, though LP remains indicated in ill-appearing infants. [1] [15]
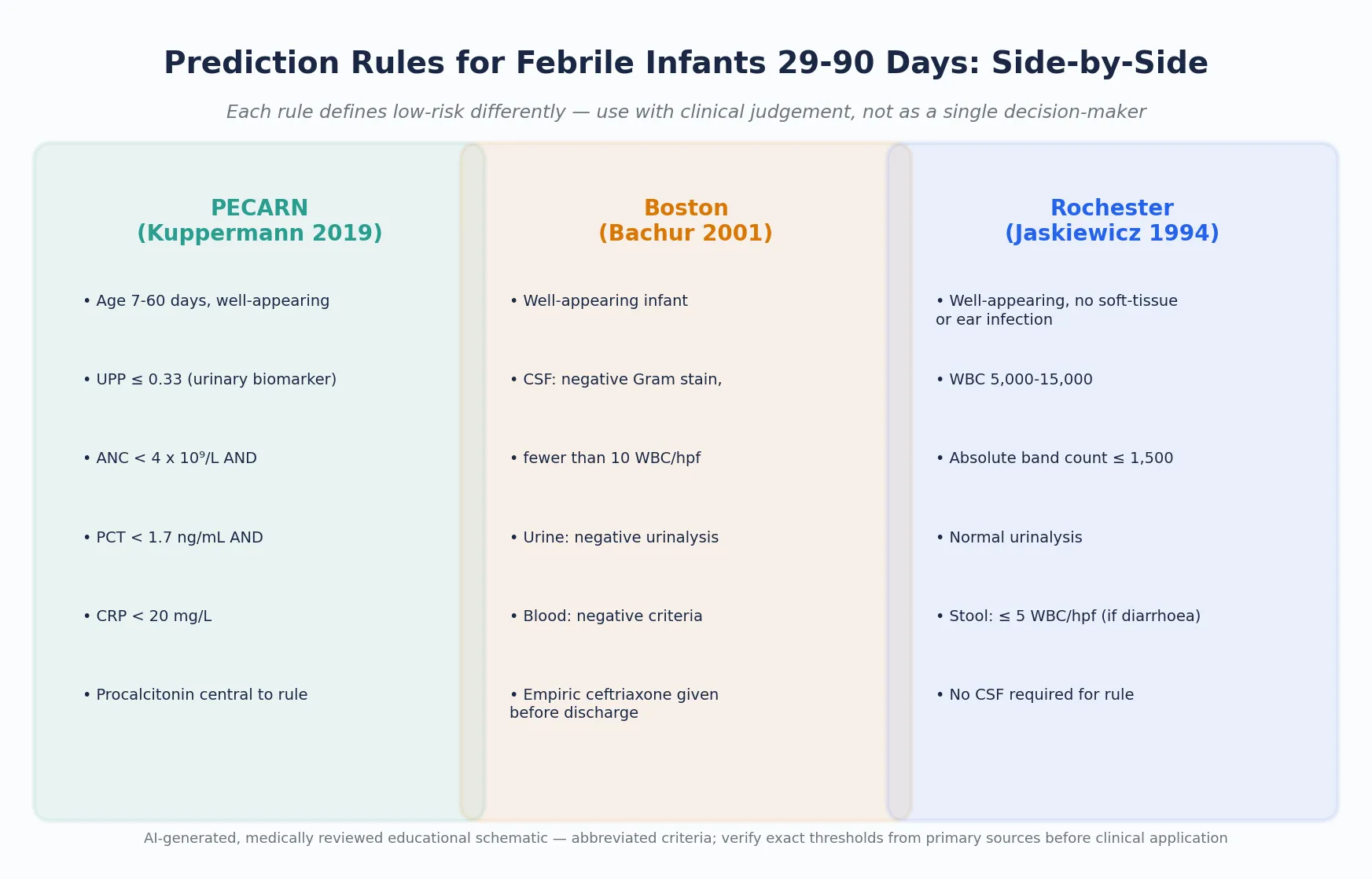
The Rochester criteria define low-risk as: well-appearing, no soft-tissue or ear infection, WBC 5,000-15,000, absolute band count ≤1,500, normal urinalysis, and stool with fewer than 5 WBC/hpf if diarrhoea is present. Importantly, the Rochester criteria do not require LP — a febrile infant meeting Rochester low-risk criteria is managed without LP if the clinician is confident. [2]
The Boston criteria add LP to the evaluation: a low-risk infant must have CSF with negative Gram stain and fewer than 10 WBC/hpf, in addition to normal urinalysis and blood criteria. Boston also gives empiric ceftriaxone before discharge and arranges 24-hour review. [3]
| Feature | Rochester | Boston | Philadelphia | PECARN |
|---|---|---|---|---|
| Year | 1994 | 2001 | 1993 | 2019 |
| Age range | ≤60 days | 28-89 days | 29-56 days | 7-60 days |
| Requires LP | No | Yes | Yes | No |
| Empiric antibiotics | No | Yes (ceftriaxone) | Yes | Per protocol |
| Key biomarkers | WBC, bands | WBC, bands | WBC, bands, ANC | PCT, CRP, ANC, uNGAL |
| Urine testing | Yes (UA) | Yes (UA) | Yes (UA + culture) | Yes (UA + culture) |
| Contemporary relevance | Widely used | Widely used | Historical reference | Most current; incorporates PCT |
Biomarkers
Inflammatory markers help estimate the probability of SBI, but no single marker is perfect. The most studied are procalcitonin (PCT), C-reactive protein (CRP), and white cell count (WCC) with absolute neutrophil count (ANC). [9] [18]
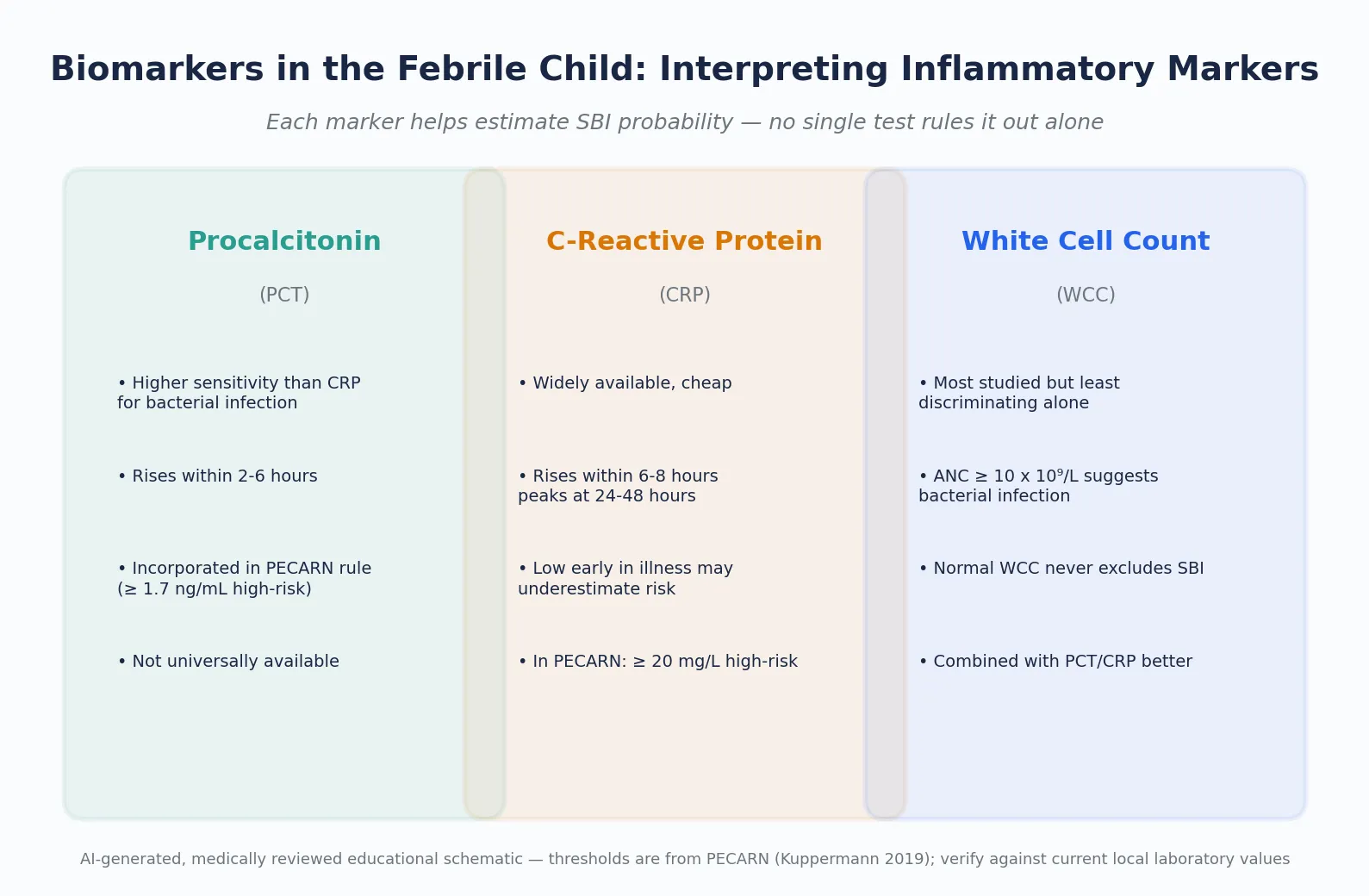
Procalcitonin rises earlier than CRP (within 2-6 hours versus 6-8 hours), giving it better sensitivity for early bacterial infection. A systematic review and meta-analysis by Yo et al. confirmed that PCT outperforms CRP and WCC for detecting SBI in children with fever without a source. However, PCT is not universally available in all settings, which limits its incorporation into routine practice. [9] [18]
Lumbar puncture
LP is indicated when meningitis is suspected — specifically in ill-appearing infants, infants with CSF criteria triggering the prediction rule, or infants with seizures, bulging fontanelle, or altered consciousness. In neonates, LP is part of the mandatory workup. Interpret CSF findings in age-specific context: a neonate normally has higher CSF white cell counts than an older child. [4] [5]
The Bacterial Meningitis Score (BMS), developed by Nigrovic et al. and validated in multiple studies, helps distinguish bacterial from aseptic meningitis in children over 2 months with CSF pleocytosis. A BMS-negative child has a very low (but not zero) probability of bacterial meningitis. [4] [5]
Enterovirus PCR
When available, enterovirus PCR on CSF or blood can identify the cause of aseptic meningitis and shorten hospital stay by reducing unnecessary antibiotics. Aronson et al. demonstrated that enteroviral PCR testing reduced length of stay for febrile infants 60 days or younger. [19]
Blood culture
Blood culture remains the gold standard for detecting bacteraemia. Biondi et al. showed that the majority of positive blood cultures in febrile infants turn positive within 24 hours, supporting the practice of observing for 24-48 hours before declaring a culture negative. [8]
Management — Resuscitation
If the febrile child is ill-appearing, shocked, seizing, or has any red-flag sign, resuscitation takes priority over the diagnostic workup. Follow the age-adapted ABCDE approach: secure the airway, support breathing, establish vascular access, treat shock with fluid boluses (10 mL/kg aliquots of isotonic crystalloid, reassessing after each), check glucose, and give empiric antibiotics without delay. [6] [13]
Cefotaxime
Dose
50 mg/kg per dose IV
The empiric antibiotic regimen depends on age and suspected source. For neonates (≤28 days), the standard is cefotaxime plus ampicillin (to cover Listeria, which cefotaxime does not). Add aciclovir (20 mg/kg/dose IV every 8 hours) if HSV is suspected (seizure, vesicular rash, maternal HSV, CSF pleocytosis, or deranged liver function). Ceftriaxone is avoided in neonates under 28 days because it displaces bilirubin from albumin, increasing the risk of kernicterus. [6] [13]
For infants 29-90 days who require empiric treatment, ceftriaxone (50 mg/kg IV or IM) is the agent of choice, providing coverage against the most likely pathogens (S. pneumoniae, E. coli, N. meningitidis). [6] [13]
Management — Definitive & Stepwise
The definitive management pathway is driven by age and risk category. Each age band has a clear algorithm that balances the risk of SBI against the harms of over-investigation. [6] [13]
Neonate (≤28 days)
Full septic workup (CBC, CRP, blood culture, urinalysis/culture by catheter or SPA, LP with CSF analysis). Empiric IV cefotaxime plus ampicillin. Consider aciclovir. Admit for observation pending cultures. No outpatient management. [6] [11]
Young infant (29-90 days)
Apply a prediction rule (PECARN, Boston, or Rochester per local protocol). All infants in this age group should have urinalysis. If the infant meets low-risk criteria, is well-appearing, and has reliable follow-up, selected infants may be managed without empiric antibiotics or with a single dose of ceftriaxone and 24-hour review. If the infant is ill-appearing, does not meet low-risk criteria, or has abnormal biomarkers, proceed with LP, empiric ceftriaxone and admission. [1] [6] [13]
Infant or child (3-36 months)
Apply the traffic-light system. A green (low-risk) child with a identified or presumed viral source can be managed at home with antipyretics and a safety-net. An amber (intermediate) child needs same-day assessment, targeted testing (urinalysis if under 2 years or if suspected, CXR if respiratory signs), and consideration of empiric antibiotics depending on vaccination status. A red (high-risk) child needs urgent hospital assessment, full workup and empiric antibiotics. [13]
In Australia and New Zealand, the RCH Melbourne Clinical Practice Guidelines guide the approach and align closely with the NICE traffic-light system. Ceftriaxone is the first-line empiric agent for febrile infants 29-90 days. The approach in Aboriginal and Torres Strait Islander and Māori children may need to account for higher rates of SBI and reduced access to follow-up, lowering the threshold for investigation and admission. [6]
Specific Subtypes & Scenarios
Several specific clinical scenarios modify the standard approach to the febrile child and require tailored evaluation. [6]
The febrile infant with a central venous catheter
Any fever in a child with an indwelling central line is treated as line-associated bacteraemia until proven otherwise. Draw blood cultures from the line and peripherally, start empiric broad-spectrum antibiotics (e.g., vancomycin plus a third-generation cephalosporin or antipseudomonal beta-lactam), and consult the oncology or infectious diseases team. [6]
The febrile child with sickle cell disease or functional asplenia
These children are at extremely high risk of overwhelming S. pneumoniae or Haemophilus sepsis due to impaired splenic function. Any fever ≥38.5 °C requires immediate parenteral antibiotics (e.g., ceftriaxone 50 mg/kg IV/IM), blood cultures, and observation, regardless of how well they appear. [6]
The febrile infant with bronchiolitis
A febrile infant under 3 months with a clinical diagnosis of bronchiolitis still has a non-trivial rate of concomitant SBI (particularly UTI). Bronchiolitis does not automatically explain the fever — urinalysis should still be performed, and the young infant risk-stratification rules still apply. [6] [13]
The febrile child with confirmed enterovirus or parechovirus
Documented enterovirus or parechovirus infection in a well-appearing febrile infant can shorten the duration of unnecessary antibiotics and hospital stay. However, it does not negate the initial evaluation, and concomitant SBI must still be excluded. [19] [20]
FEVER
Complications & Pitfalls
The evaluation of the febrile child carries risks at both ends of the spectrum: too little investigation can miss SBI, and too much can cause harm. [6] [13]
Over-investigation leads to unnecessary lumbar punctures (discomfort, post-LP headache, rare complications), hospitalisation (nosocomial infection, cost, family disruption), and antibiotics (adverse reactions, Clostridioides difficile colitis, antimicrobial resistance, disruption of the developing microbiome). Each investigation must be justified by the probability it changes the management decision. [6]
Under-investigation risks missing meningitis, bacteraemia or UTI, leading to delayed treatment, permanent neurological injury, septic shock, or death. The consequences of a missed SBI are catastrophic and asymmetric — this asymmetry is what drives the conservative approach to young infants. [6]
Classic pitfalls include: [6] [9] [17]
- Relying on a normal urinalysis to exclude UTI in a young infant. Bag urine specimens have contamination rates of up to 30%; even catheter specimens can be falsely negative early in infection. A negative urinalysis in a high-risk infant should be confirmed with culture.
- Interpreting a traumatic LP as sterile when bacteria may be present. Use the CSF white-to-red cell ratio as a guide, but treat empirically if there is clinical concern.
- Over-reliance on a single biomarker. A normal CRP early in the illness course does not exclude bacterial infection. Procalcitonin is better early but is not universally available.
- Discharging without a safety-net. A verbal "come back if worried" is inadequate. The safety-net must be specific, written and actionable: "Return immediately if the child has [specific signs], within [specific timeframe], to [specific location]." [6] [9] [17]
Prognosis & Disposition
The prognosis for the vast majority of febrile children is excellent. Most viral fevers resolve within 3-5 days. The prognosis for SBI depends on early recognition and treatment — untreated meningitis has a mortality of up to 10% and a neurological morbidity of 20-30%, while early-treated meningitis has substantially better outcomes. [6] [13]
Disposition is determined by the combination of age, clinical appearance, risk-stratification category, and the results of investigations. The decision to admit, observe, or discharge must account for the feasibility of follow-up and the caregiver's ability to return. [6]
Blood cultures should be observed for 24-48 hours before declaring them negative, as the majority of true positives turn positive within this window. If a culture turns positive after discharge, there must be a protocol for recall, re-evaluation and treatment. [8]
Special Populations
Several groups require modified approaches due to altered baseline risk or impaired ability to mount or express the usual clinical signs. [6]
Immunocompromised children (oncology patients, transplant recipients, primary immunodeficiency) have attenuated inflammatory responses and may present with subtle signs of overwhelming sepsis. Any fever in this group is a medical emergency requiring immediate broad-spectrum antibiotics, blood cultures and admission. [6]
Aboriginal and Torres Strait Islander and Māori children may have higher rates of SBI and reduced access to timely healthcare, particularly in rural and remote settings. Lower the threshold for investigation and admission, and ensure culturally safe communication and follow-up arrangements. [6]
Children with developmental disability or neurodiversity may not express symptoms in typical ways, making clinical assessment less reliable. The caregiver's knowledge of the child's baseline behaviour is particularly important. Use familiar communication methods and avoid unnecessary distress during examination. [6]
Migrant and refugee families may face language barriers, unfamiliarity with the healthcare system, and difficulty enacting safety-nets. Use professional interpreters (not family members), provide written safety-netting in the family's language if possible, and consider social factors in disposition decisions. [6]
Evidence, Guidelines & Regional Differences
The approach to the febrile child has evolved through several landmark studies. The Philadelphia protocol (Baker 1993, not separately PMID-cited here due to verification constraints), Rochester criteria (Jaskiewicz 1994), and Boston criteria (Bachur 2001) were developed in the pre-conjugate vaccine era and defined the framework for risk-stratifying young febrile infants. [2] [3] [14]
The PECARN prediction rule (Kuppermann 2019) is the most contemporary and largest study, derived from over 180,000 febrile infants across 26 US emergency departments. It incorporates procalcitonin and a urinary biomarker (uNGAL) and achieves very high sensitivity for invasive bacterial infection. The PECARN rule has been externally validated in multiple settings, though some European validation studies have found lower performance, highlighting the importance of considering local epidemiology. [1] [15] [16]
PECARN (Kuppermann 2019)
Population: Febrile infants 7-60 days presenting to 26 US emergency departments
Key finding
A prediction rule using ANC, procalcitonin, CRP and uNGAL identified infants at very low risk of invasive bacterial infection (sensitivity ~97.7%) without requiring LP for low-risk determination.
The post-conjugate vaccine era has fundamentally changed the approach to febrile children 3-36 months. With occult pneumococcal bacteraemia now occurring in fewer than 1% of vaccinated well-appearing children, routine empiric blood cultures and antibiotics are no longer recommended for this age group in most developed-world settings. [12] [13]
Exam Pearls
References
- [1]Kuppermann, Nathan A Clinical Prediction Rule to Identify Febrile Infants 60 Days and Younger at Low Risk for Serious Bacterial Infections. JAMA pediatrics, 2019.PMID 30776077
- [2]Jaskiewicz, Julie A Febrile infants at low risk for serious bacterial infection--an appraisal of the Rochester criteria and implications for management. Febrile Infant Collaborative Study Group. Pediatrics, 1994.PMID 8065869
- [3]Bachur, Richard G Predictive model for serious bacterial infections among infants younger than 3 months of age. Pediatrics, 2001.PMID 11483793
- [4]Nigrovic, Lise E Development and validation of a multivariable predictive model to distinguish bacterial from aseptic meningitis in children in the post-Haemophilus influenzae era. Pediatrics, 2002.PMID 12359784
- [5]Nigrovic, Lise E Meta-analysis of bacterial meningitis score validation studies. Archives of disease in childhood, 2012.PMID 22764093
- [6]Ishimine, Paul Fever without source in children 0 to 36 months of age. Pediatric clinics of North America, 2006.PMID 16574521
- [7]Ishimine, Paul The evolving approach to the young child who has fever and no obvious source. Emergency medicine clinics of North America, 2007.PMID 17950137
- [8]Biondi, Eugene A Blood culture time to positivity in febrile infants with bacteremia. JAMA pediatrics, 2014.PMID 25048522
- [9]Yo, Cheng-Hsu Comparison of the test characteristics of procalcitonin to C-reactive protein and leukocytosis for the detection of serious bacterial infections in children presenting with fever without source: a systematic review and meta-analysis. Annals of emergency medicine, 2012.PMID 22921165
- [10]Mahajan, Prashant Serious Bacterial Infections in Young Febrile Infants With Positive Urinalysis Results. Pediatrics, 2022.PMID 36097858
- [11]Palladino, Lauren Febrile infants aged 60 days or younger: evaluation and management in the emergency department. Pediatric emergency medicine practice, 2024.PMID 38266065
- [12]Gomez, Borja Bacteremia in previously healthy children in emergency departments: clinical and microbiological characteristics and outcome. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology, 2015.PMID 25252630
- [13]Baraff, Lawrence J Management of infants and young children with fever without source. Pediatric annals, 2008.PMID 18972849
- [14]Baraff, Lawrence J Management of fever without source in infants and children. Annals of emergency medicine, 2000.PMID 11097701
- [15]Velasco, Ruth Accuracy of PECARN rule for predicting serious bacterial infection in infants with fever without a source. Archives of disease in childhood, 2021.PMID 32816694
- [16]Vos-Kerkhof, Esther Clinical prediction models for young febrile infants at the emergency department: an international validation study. Archives of disease in childhood, 2018.PMID 29794106
- [17]Velasco, Ruth Febrile young infants with altered urinalysis at low risk for invasive bacterial infection. a Spanish Pediatric Emergency Research Network's Study. The Pediatric infectious disease journal, 2015.PMID 25036049
- [18]Lacour, Alain G Procalcitonin, IL-6, IL-8, IL-1 receptor antagonist and C-reactive protein as identificators of serious bacterial infections in children with fever without localising signs. European journal of pediatrics, 2001.PMID 11271398
- [19]Aronson, Paul L Impact of Enteroviral Polymerase Chain Reaction Testing on Length of Stay for Infants 60 Days Old or Younger. The Journal of pediatrics, 2017.PMID 28705656
- [20]Rittichier, Kathryn R Diagnosis and outcomes of enterovirus infections in young infants. The Pediatric infectious disease journal, 2005.PMID 15933567