Paeds · infectious-diseases
Urinary tract infection and pyelonephritis
Also known as Paediatric UTI · Febrile UTI · Acute pyelonephritis · Cystitis in children · Recurrent urinary tract infection · Vesicoureteral reflux with infection
Fellowship guide to paediatric urinary tract infection and pyelonephritis: the febrile infant as the great trap, reliable urine sampling by age, urinalysis and culture interpretation, oral versus intravenous therapy, the imaging and prophylaxis debate after a first febrile UTI, vesicoureteral reflux and the RIVUR evidence, and the prevention of renal scarring.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A urinary tract infection is bacterial infection of the bladder, the collecting system, or the renal parenchyma, and it is one of the most common serious bacterial infections of childhood. In infants the presentation is usually non-specific fever alone, which makes UTI the diagnosis that must not be missed in any febrile child under two years. Pyelonephritis is the upper tract form, involving the kidney itself, and it carries the burden of fever, systemic illness, and the risk of permanent renal scarring. [2]
The reason this topic dominates paediatric exams is that the consequences of a missed or delayed diagnosis fall on the youngest patients. Renal scarring after pyelonephritis in a small child can lead to hypertension and chronic kidney disease decades later, so the threshold to sample urine in a febrile infant is deliberately low. The clinician's task is to obtain a reliable urine specimen before antibiotics, confirm the diagnosis with urinalysis and culture, treat promptly, and then decide selectively about imaging and prophylaxis. [1]
Classification
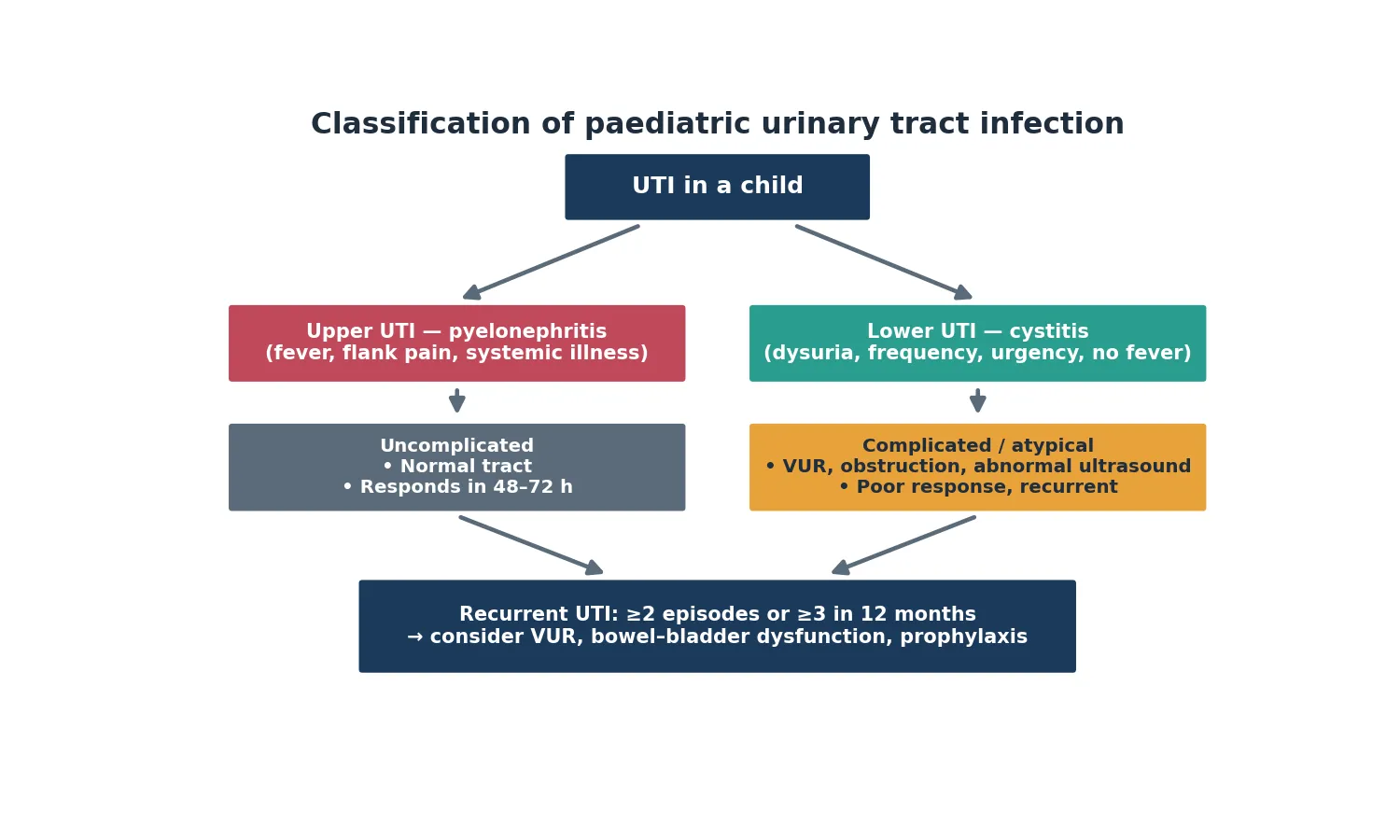
Clinicians first separate lower from upper tract infection. Lower UTI, or cystitis, involves the bladder and presents with dysuria, frequency, urgency, and suprapubic discomfort, often without fever. Upper UTI, or pyelonephritis, involves the renal parenchyma and presents with fever, flank or abdominal pain, vomiting, and systemic illness. Fever is the practical dividing line: a febrile child with a positive urine is treated as having pyelonephritis until proven otherwise, because fever signals parenchymal involvement and scarring risk. [9]
The second axis is whether the infection is uncomplicated or complicated and atypical. An uncomplicated UTI occurs in a child with a structurally normal urinary tract who responds to antibiotics within 48 to 72 hours. An atypical or complicated infection features a poor response to treatment, a raised creatinine, hypertension, a palpable bladder or abdominal mass, infection with unusual or resistant organisms, or recurrence, all of which prompt urgent imaging. This distinction drives the selective imaging strategy after a first febrile UTI. [1]
[9]Recurrent UTI defines a third pattern that changes management. A child with two or more episodes of pyelonephritis, or three or more episodes of any UTI within twelve months, warrants evaluation for vesicoureteral reflux, bowel and bladder dysfunction, and underlying structural abnormality. Recurrent febrile UTI in a young child carries the highest scarring risk and is the scenario in which prophylaxis and imaging are most clearly indicated. [11]
Epidemiology & Risk Factors
Urinary tract infection is the most common serious bacterial infection in children under two years of age. Meta-analytic data place the prevalence of UTI among febrile infants under two months at around 7 to 9 per cent, and among febrile children up to two years at roughly 7 per cent overall, with girls affected more often than boys beyond infancy. Before the age of three months, uncircumcised boys carry a notably higher risk than girls, which is why any febrile young infant, regardless of sex, deserves a urine sample. [7]
The dominant pathogen is Escherichia coli, which causes 80 to 90 per cent of childhood UTIs through uropathogenic strains bearing fimbriae that adhere to uroepithelium. Klebsiella, Proteus, Enterococcus, and coagulase-negative staphylococci account for most of the remainder, with Proteus more common in boys and associated with struvite stones. The recognition of risk factors matters because they identify the children most likely to scar and to recur: age under two years, female sex beyond infancy, uncircumcised foreskin in young boys, vesicoureteral reflux, constipation and bowel and bladder dysfunction, and structural urinary tract abnormality. [11]
Indigenous children in Australia and New Zealand, children in remote communities, and migrant and refugee families with barriers to care experience higher rates of recurrent and complicated UTI and later presentation. Socioeconomic disadvantage, overcrowded housing, limited access to reliable primary care, and reduced continence-related hygiene all amplify risk, so culturally safe assessment, clear safety-net advice, and reliable follow-up pathways are part of management in these populations. [2]
Pathophysiology
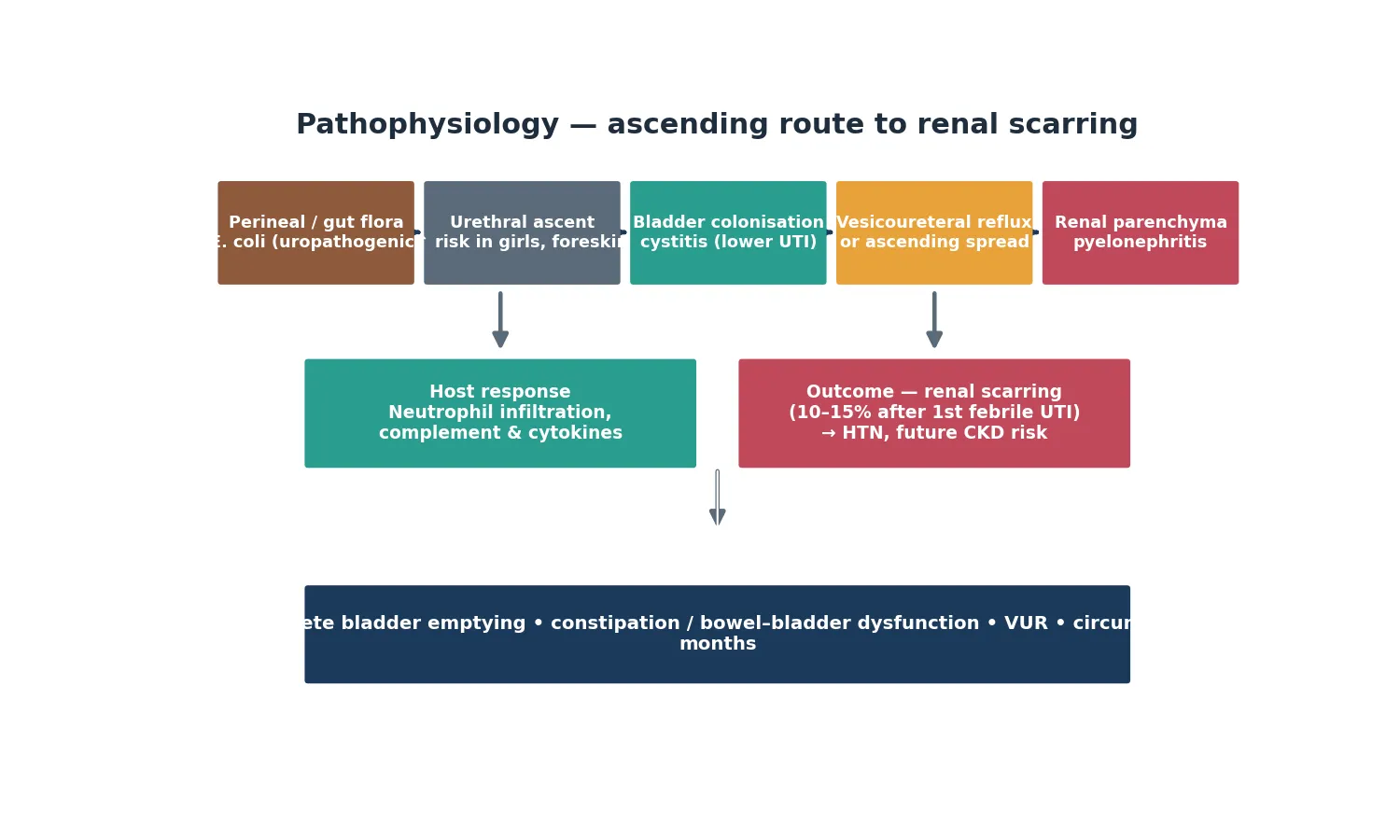
Most childhood UTIs arise by the ascending route. Uropathogenic strains of E. coli from the perineal and gut flora ascend the urethra into the bladder, where they adhere to uroepithelial cells via P-fimbriae and type 1 pili, evade bladder emptying, multiply, and trigger cystitis. Girls are more susceptible because of a short urethra, and uncircumcised boys carry higher risk because the warm subpreputial space favours uropathogen colonisation. [9]
Once established in the bladder, bacteria may ascend to the kidney directly or through vesicoureteral reflux, in which urine flows retrograde from the bladder up the ureters during voiding. Reflux is graded by severity and is found in roughly 30 to 40 per cent of children investigated after a first febrile UTI. Higher grades of reflux and concurrent bowel and bladder dysfunction substantially increase the risk of recurrent pyelonephritis and renal scarring. [3]
The renal injury that examiners probe is scarring. Bacterial invasion of the renal parenchyma recruits neutrophils and activates complement and cytokines, producing oedema, vasoconstriction, and ischaemic injury to the renal tubules and interstitium. The resulting scar is permanent and, when bilateral or extensive, predisposes to hypertension and chronic kidney disease over the long term. Roughly 10 to 15 per cent of children develop a permanent scar detectable on a DMSA scan months after a first febrile UTI, and the risk is highest in the youngest children and those with high-grade reflux. [8]
Risk modifiers turn an isolated infection into a recurrent, scarring illness. Incomplete bladder emptying, dysfunctional voiding, and chronic constipation raise residual urine and bacterial stasis. Vesicoureteral reflux delivers infected urine to the kidney. Structural obstruction, such as posterior urethral valves in boys, creates the conditions for atypical and recurrent infection. Recognising these modifiers is what separates management of a single UTI from prevention of long-term renal damage. [11]
Clinical Presentation
The presentation of UTI in children is highly age-dependent, and the absence of classic urinary symptoms is the rule rather than the exception in the youngest patients. Infants under two years most often present with fever alone, or with non-specific features such as irritability, poor feeding, vomiting, lethargy, or failure to thrive. Jaundice in the neonate can be the only clue. Because the urinary symptoms are absent, UTI enters the differential of every febrile infant, which is why guideline-based urine sampling is built into the febrile infant pathway. [1]
Toilet-trained children and adolescents are more likely to report the textbook symptoms. Dysuria, frequency, urgency, suprapubic pain, and haematuria point to lower UTI, while fever with flank or abdominal pain, vomiting, rigors, and systemic illness point to pyelonephritis. Enuresis in a previously continent child and new-onset daytime wetting are also recognised features. The clinician should ask explicitly about voiding pattern, constipation, fluid intake, and previous UTI, because bowel and bladder dysfunction is the commonest driver of recurrence. [9]
Presenting features by age and level
Infant under 2 years: fever alone, irritability, poor feeding, vomiting, or jaundice
Toilet-trained child: dysuria, frequency, urgency, suprapubic pain, haematuria
Pyelonephritis: high fever, flank or abdominal pain, vomiting, rigors, systemic illness
Recurrent pattern: repeated episodes, daytime wetting, enuresis, constipation, voiding dysfunction
Neonate or toxic child: sepsis-like illness, poor perfusion, lethargy, bacteraemia
A small but important group presents with sepsis from a urinary source. A toxic, lethargic infant with tachycardia, prolonged capillary refill, and hypotension may have urosepsis complicating pyelonephritis, and this child needs immediate resuscitation, parenteral antibiotics, and a search for obstruction. The message for the exam is that UTI ranges from an uncomfortable but benign cystitis in a teenager to a life-threatening sepsis illness in a neonate, and the assessment must match the severity. [2]
Differential Diagnosis
The differential diagnosis of suspected UTI splits into other causes of urinary symptoms and other causes of fever in a young child. Vulvovaginitis, urethritis, balanitis, and pinworm infestation can mimic lower UTI with dysuria and frequency, and sexually transmitted infections enter the differential in adolescents. These conditions produce urinary symptoms without a confirmed culture, so a properly collected and interpreted urine sample resolves most of the confusion. [9]
When the presenting problem is fever in a young child without localising features, the differential is the broad febrile infant differential. Viral upper respiratory infection, otitis media, pneumonia, gastroenteritis, and occult bacteraemia or meningitis all coexist with UTI on the list, which is why urine testing belongs in the workup of any febrile child under two years without an obvious source. A child with a respiratory finding can still have a UTI, so the presence of an alternative explanation must never exempt the clinician from sampling urine. [1]
Non-infectious causes complete the differential. Renal colic from a stone, anatomical obstruction, diabetes mellitus with polyuria and secondary infection, and pelvic or abdominal pathology can present with abdominal or flank pain. In the atypical case that does not respond to antibiotics, or that shows an unusual organism, the clinician must return to the differential and image for obstruction, abscess, or structural abnormality. [2]
Clinical & Bedside Assessment
Begin with an overall judgement of how sick the child is, using the paediatric assessment triangle of appearance, work of breathing, and circulation. A toxic, lethargic, or poorly perfused child needs immediate resuscitation and parenteral antibiotics, regardless of how the workup proceeds. Measure temperature, heart rate, respiratory rate, blood pressure, capillary refill, and oxygen saturation, and weigh the child to calculate any drug dose. Hypertension in a child with a febrile UTI raises concern for underlying renal disease or scarring and mandates imaging. [2]
Examine the abdomen and genitourinary region specifically. Palpate for a distended bladder or an abdominal mass suggesting obstruction, and ballot the kidneys for enlargement or tenderness, though this sign is hard to elicit reliably in a young child. Inspect the external genitalia for vulvovaginitis, balanitis, phimosis, and signs of abuse, and assess for constipation by palpating for faecal loading. A focused neurological and spinal examination is warranted when voiding dysfunction or recurrent UTI raises the possibility of a neurogenic bladder. [9]
Take a targeted history that captures the features that change management. Establish the duration and height of fever, the presence of urinary symptoms, previous UTI episodes, voiding pattern, constipation, fluid intake, and family history of reflux or renal disease. Ask about pregnancy and neonatal history for clues to posterior urethral valves or other structural abnormality, and document vaccination status and any antibiotic exposure in the preceding days, because prior antibiotics lower the culture yield and confound diagnosis. [1]
Investigations
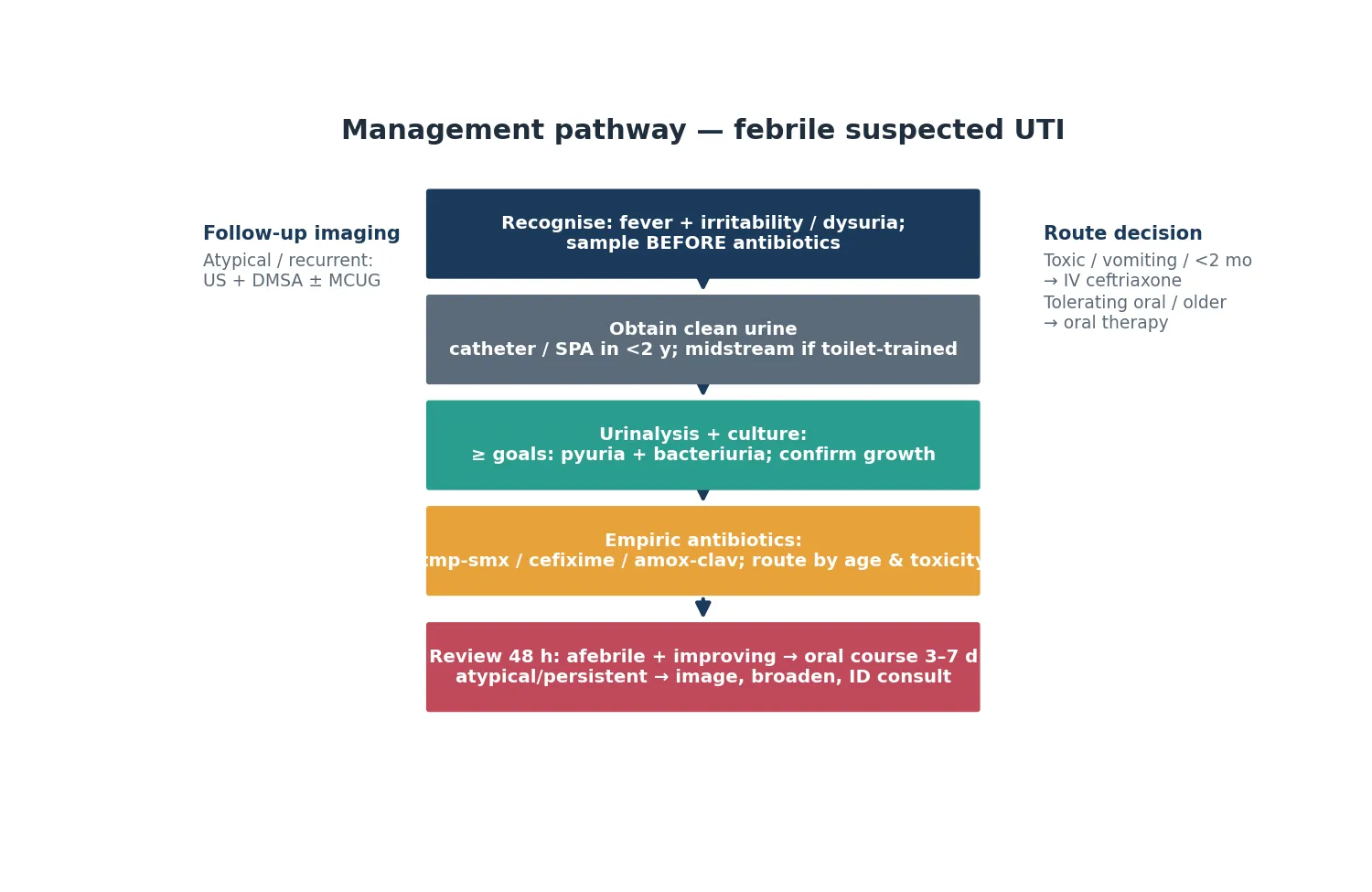
The cornerstone investigation is a properly collected urine specimen, and the method depends on age and continence. In a child under two years, or any child not yet toilet-trained, a clean catch sample has an unacceptably high contamination rate, so urine must be obtained by urethral catheterisation or suprapubic aspiration. Suprapubic aspiration is the gold standard for sterility and is preferred in young infants, while catheterisation is more practical in most settings and is the dominant method in Australasian emergency departments. [1]
In the toilet-trained child, a clean-catch midstream specimen is acceptable after instructing the child and parent in technique. Whatever the method, the sample must be obtained before antibiotics are given. Bag specimens are useful only to exclude infection when negative, because a positive bag culture has a contamination rate so high that it leads to overdiagnosis, unnecessary treatment, and incorrect imaging decisions. A positive bag culture must always be confirmed by catheter or suprapubic sample before acting on it. [1]
Urinalysis provides the immediate answer. Dipstick testing for leucocyte esterase and nitrites, combined with microscopy for pyuria and bacteria, predicts UTI while culture is pending. The combination of pyuria and bacteriuria on an enhanced urinalysis, or a positive leucocyte esterase with nitrites on dipstick, makes UTI highly likely, while the absence of both makes it unlikely. Critically, pyuria must accompany a significant culture growth to confirm UTI, because asymptomatic bacteriuria and contamination can produce a positive culture without pyuria and must not be treated as infection. [1]
Blood tests are reserved for the atypical, toxic, or very young child. A febrile infant under one month, or any child with signs of sepsis, needs blood cultures, a full blood count, electrolytes, urea and creatinine, and C-reactive protein. A raised creatinine or hypertension at presentation mandates urgent ultrasound to exclude obstruction. Blood inflammatory markers do not by themselves diagnose UTI, but a markedly raised C-reactive protein and procalcitonin correlate with pyelonephritis and a higher scarring risk, and they help stratify which children warrant closer imaging follow-up. [2]
Urine culture confirms the diagnosis and guides antibiotic choice. Send the sample for culture and sensitivity regardless of the dipstick result when UTI is suspected, because culture defines the organism, the antibiotic susceptibilities, and the threshold growth that separates true infection from contamination. A culture growing a single uropathogen at or above the threshold for the collection method, in a sample with pyuria, confirms UTI and allows the clinician to narrow or adjust the antibiotic once sensitivities return. [9]
Management — Resuscitation
Most children with UTI are well enough to manage with oral antibiotics as an outpatient, but a small group needs immediate resuscitation. A toxic, lethargic, or poorly perfused child with suspected urosepsis needs an airway, breathing, circulation approach, high-flow oxygen for hypoxia or distress, and rapid intravenous or intraosseous access. Establish access within minutes rather than hunting for a peripheral line. [2]
Give a 10 mL per kilogram bolus of isotonic 0.9 per cent sodium chloride for hypotension or poor perfusion, and reassess the child after each bolus, repeating to a total of 30 to 60 mL per kilogram in septic shock titrated to perfusion and blood pressure. Watch for hepatomegaly and a rising oxygen requirement as signs of volume overload. Avoid hypotonic fluids because of the risk of hyponatraemia. Treat hyperpyrexia with paracetamol 15 mg per kilogram for comfort and to reduce metabolic demand, but recognise that fever itself does not indicate severity. [2]
Resuscitation sequence for the toxic child with suspected UTI or urosepsis
Assess airway, breathing, circulation and give high-flow oxygen
Establish intravenous or intraosseous access within minutes
Obtain catheter urine sample, blood culture, full blood count, CRP, electrolytes
Give first dose of parenteral antibiotic immediately after sampling
Fluid bolus 10 mL/kg 0.9 per cent NaCl for shock, reassess after each
Arrange urgent ultrasound if raised creatinine, hypertension, or poor response
The single most important drug intervention is the first dose of an appropriate antibiotic, given as soon as the urine and blood cultures are sampled. The empiric choice is guided by age, local resistance patterns, and severity. Never let imaging or transport delay the first dose in a sick child, because untreated pyelonephritis progresses to sepsis and renal injury, and the cultures drawn before antibiotics retain their value for the first hours. [6]
Management — Definitive & Stepwise
Empiric oral therapy for an uncomplicated UTI in a child old enough to tolerate oral intake uses a guided choice of trimethoprim-sulfamethoxazole, cefixime, or amoxicillin-clavulanate, with the agent selected against local E. coli resistance patterns. Cefixime 8 mg per kilogram orally daily or amoxicillin-clavulanate are widely used first-line options in Australasia. Nitrofurantoin 3 mg per kilogram per day in divided doses reaches good bladder concentrations and is effective for lower UTI but not for pyelonephritis, because it does not achieve reliable tissue levels. [2]
The route of therapy is a key examinable decision, settled by a landmark trial. Oral and intravenous therapy are equally effective for febrile UTI in young children who are not toxic, so oral therapy is preferred for the child who is tolerating oral intake and is well enough for outpatient care. Reserve intravenous therapy for the toxic or vomiting child, the infant under one to two months, and any child who fails oral therapy. The standard parenteral agent is ceftriaxone 50 mg per kilogram intravenously daily, switching to oral once the child is afebrile and improving. [6]
Empiric antibiotic decisions by scenario
Duration of therapy depends on the level of infection. Lower UTI in an older child is treated for 3 to 5 days, while pyelonephritis and febrile UTI in a young child require 7 to 14 days. Shorter courses carry a higher recurrence risk in young children with pyelonephritis, so 7 to 10 days remains the standard for febrile UTI in infancy. Review the child at 48 hours: a child who is afebrile and improving completes the course orally, while a child still febrile or unwell must be reassessed for resistant organism, obstruction, or complication, and imaged urgently. [1]
Specific Subtypes & Scenarios
The febrile infant under three months is the highest-stakes scenario. These infants have a non-negligible risk of bacteraemia, may deteriorate rapidly, and have immature immune responses, so the standard of care is admission, parenteral antibiotics such as ceftriaxone, and a full sepsis evaluation including blood and cerebrospinal fluid cultures when indicated. Oral therapy is not appropriate in this age group for pyelonephritis, and the threshold for imaging is lower because structural abnormality such as posterior urethral valves is more likely to declare itself here. [2]
Vesicoureteral reflux is the structural scenario that examiners test most relentlessly. Reflux is graded I to V by severity and is found in roughly a third of children imaged after a first febrile UTI. The RIVUR trial established that antimicrobial prophylaxis reduces recurrent UTI in children with reflux, though it does not prevent new renal scarring and carries a small risk of resistant infection. The contemporary approach is to reserve prophylaxis for children with high-grade reflux, recurrent febrile UTI, or bowel and bladder dysfunction, rather than reflexively treating all reflux. [3]
Recurrent UTI is the scenario in which prevention takes over from a single episode. A child with recurrent febrile UTI warrants evaluation for reflux and bowel and bladder dysfunction, aggressive management of constipation, attention to hydration and voiding hygiene, and consideration of continuous antibiotic prophylaxis. Cochrane evidence confirms that long-term prophylaxis modestly reduces the risk of recurrent culture-confirmed UTI, and the benefit is clearest in children with reflux and recurrent disease, weighed against the risk of selecting resistant organisms. [4]
[4]Atypical and resistant UTI demands a different response. Infection with unusual or resistant organisms, a poor response to first-line therapy, or UTI in a child with a structurally abnormal or neurogenic bladder requires broader empiric cover, early imaging, and infectious diseases or nephrology input. Children with spina bifida, posterior urethral valves, or transplanted kidneys fall into this group, and their management is individualised around their anatomy and catheterisation pattern. [2]
Complications & Pitfalls
Renal scarring is the defining long-term complication and the reason the topic matters. Approximately 10 to 15 per cent of children develop a permanent scar detectable on a DMSA scan performed months after a first febrile UTI, and the risk rises with younger age, high-grade reflux, delayed treatment, and recurrent febrile infection. Bilateral or extensive scarring predisposes to hypertension and chronic kidney disease over decades, which is why long-term blood pressure and renal function surveillance belong to the follow-up of a scarred kidney. [8]
Acute complications include bacteraemia and sepsis, particularly in infants under three months, and renal or perinephric abscess in the atypical case that fails to respond. A child still febrile at 48 hours of appropriate therapy must be reassessed for resistant organism, obstruction, abscess, or alternative diagnosis, and imaged. Urosepsis with shock and disseminated intravascular coagulation is the severe end of the spectrum and mandates intensive care support and source control. [2]
The major clinical pitfalls are sampling urine after antibiotics have already been given, acting on a contaminated bag culture, treating asymptomatic bacteriuria without pyuria, defaulting to intravenous therapy for the well child who could take oral medication, and reflexively imaging every child after a first uncomplicated febrile UTI. Omitting follow-up blood pressure surveillance in a scarred child and failing to address bowel and bladder dysfunction in recurrent UTI are additional recurring errors that examiners probe directly. [1]
Prognosis & Disposition
The two determinants of outcome are the speed of starting appropriate antibiotics and the presence of reflux and recurrent infection. Children who receive prompt antibiotics and defervesce within 48 hours generally recover fully, though a scar may still declare itself on a DMSA scan months later. The youngest infants and those with high-grade reflux and recurrent febrile UTI carry the worst prognosis for scarring, while the child with a single uncomplicated lower UTI has an excellent outlook. [8]
Disposition depends on the child's age, toxicity, and response. A well, afebrile child tolerating oral intake completes a short oral course as an outpatient with review at 48 hours. Admission and parenteral therapy are reserved for infants under one to two months, the toxic or vomiting child, the child failing oral therapy, and any child with social or geographic barriers to reliable follow-up. In remote communities, a lower threshold for admission reflects the difficulty of safety-net review and the consequences of deterioration far from care. [2]
Special Populations
Infants under three months are the highest-risk group and warrant a different management pathway. Their immature immunity, higher bacteraemia rate, and non-specific presentation demand admission, parenteral antibiotics, and a full sepsis evaluation. Structural abnormality such as posterior urethral valves is more likely to declare itself in this group, so the threshold for ultrasound is lower. The risk-benefit balance favours investigation and inpatient treatment over oral therapy and watchful waiting. [2]
Children with complex chronic conditions and neurogenic bladders, including those with spina bifida, posterior urethral valves, and renal transplants, are susceptible to atypical and recurrent UTI with resistant organisms. Their management is individualised around their anatomy, catheterisation, and immunosuppression, and they need nephrology and urology involvement. Asymptomatic bacteriuria is common in catheterised children and must be distinguished from true infection by the presence of symptoms and pyuria, because treating colonisation drives resistance without benefit. [2]
In Indigenous and remote communities across Australia and New Zealand, higher rates of recurrent and complicated UTI, later presentation, and greater distance to tertiary care all contribute to worse outcomes. Culturally safe, family-centred care with interpreter access, clear safety-net advice in plain language, and reliable aeromedical and follow-up pathways is essential. In migrant and refugee families, language barriers, incomplete continuity of care, and reduced health literacy shape both risk and presentation, so a written plan and an interpreter-mediated explanation of warning signs and re-presentation reduce missed complications. [4]
[4]Evidence, Guidelines & Regional Differences
The American Academy of Pediatrics 2011 clinical practice guideline, together with the contemporary management review by Mattoo and Shaikh, provides the current framework for diagnosis and management of the initial UTI in febrile infants. These sources converge on reliable urine sampling before antibiotics, the requirement for pyuria plus a significant culture growth to confirm diagnosis, oral therapy for the well child, and a selective imaging strategy that reserves ultrasound, DMSA, and micturating cystourethrography for atypical, recurrent, or complicated infection. [1]
The imaging and prophylaxis debate is the most contested area, and it rests on two landmark trials. The RIVUR trial showed that antimicrobial prophylaxis reduces recurrent UTI in children with vesicoureteral reflux but does not prevent new renal scarring and increases the risk of resistant infection. The earlier Montini trial found that prophylaxis after a first febrile UTI did not reduce recurrent UTI overall. Cochrane review of long-term antibiotics confirms a modest reduction in recurrent culture-confirmed UTI, with the clearest benefit in high-risk groups. The practical synthesis is selective prophylaxis for high-grade reflux and recurrent disease rather than routine use. [3]
[3]Controversies persist around which children need imaging after a first febrile UTI, whether routine DMSA scanning adds value beyond selective use, and how to balance the benefit of prophylaxis against the selection of resistant organisms. The NICE guideline from the United Kingdom favours a more restrictive imaging approach than the AAP guideline, while the Australasian approach aligns with selective imaging and oral-first therapy. Rising antimicrobial resistance in E. coli, the emergence of extended-spectrum beta-lactamase organisms, and the increasing recognition of bowel and bladder dysfunction as a modifiable risk factor keep these questions live. [12]
Exam Pearls
SAMPLE the urine
References
- [1]Roberts KB Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics, 2011.PMID 21873693
- [2]Mattoo TK Contemporary Management of Urinary Tract Infection in Children. Pediatrics, 2021.PMID 33479164
- [3]Hoberman A Antimicrobial prophylaxis for children with vesicoureteral reflux. N Engl J Med, 2014.PMID 24795142
- [4]Williams G Long-term antibiotics for preventing recurrent urinary tract infection in children. Cochrane Database Syst Rev, 2019.PMID 30932167
- [5]Hoberman A Imaging studies after a first febrile urinary tract infection in young children. N Engl J Med, 2003.PMID 12529459
- [6]Hoberman A Oral versus initial intravenous therapy for urinary tract infections in young febrile children. Pediatrics, 1999.PMID 10390264
- [7]Shaikh N Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J, 2008.PMID 18316994
- [8]Shaikh N Identification of children and adolescents at risk for renal scarring after a first urinary tract infection: a meta-analysis with individual patient data. JAMA Pediatr, 2014.PMID 25089634
- [9]Morello W Acute pyelonephritis in children. Pediatr Nephrol, 2016.PMID 26238274
- [10]Montini G Prophylaxis after first febrile urinary tract infection in children? A multicenter, randomized, controlled, noninferiority trial. Pediatrics, 2008.PMID 18977988
- [11]Keren R Risk Factors for Recurrent Urinary Tract Infection and Renal Scarring. Pediatrics, 2015.PMID 26055855
- [12]Williams G Prevention of recurrent urinary tract infection in children. Curr Opin Infect Dis, 2009.PMID 19532083