Paeds · infectious-diseases
Vaccine-preventable disease outbreak response
Also known as VPD outbreak control · Outbreak response and contact tracing · Post-exposure prophylaxis in VPD outbreaks · Ring vaccination and catch-up campaigns · Epidemic-curve investigation
Fellowship topic on the systematic response to a vaccine-preventable disease outbreak in children: how the basic reproduction number sets the herd-immunity threshold and why measles, with an R₀ of twelve to eighteen, demands coverage above ninety-five per cent; how outbreaks ignite in under-vaccinated clusters and what the epidemic curve tells you about the window for action; the stepwise response — recognise the prodrome, isolate on suspicion, confirm with IgM and PCR with genotyping, notify public health, build the contact list, triage the pregnant woman, infant and immunocompromised contact, deliver post-exposure prophylaxis (MMR within seventy-two hours, immunoglobulin within six days, macrolides, antivirals and VZIG), exclude until non-infectious, and run the ring and catch-up vaccination campaign that lifts coverage back above the threshold; the disease-specific levers for measles, mumps, rubella, pertussis and varicella; the special-population triage that decides who pays for a late response; and the communication and documentation that close the loop and protect the next child.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The outbreak response — DETECT, INTERRUPT, PREVENT
Overview & Definition
Picture a six-year-old brought to the emergency department with four days of fever, a streaming nose, a hacking cough and red eyes, who this morning developed a rash behind the ears spreading down the body. The child has never been vaccinated, and the waiting room is full of infants and pregnant women. This is measles, and the decisions made in the next ten minutes — isolate, confirm, treat, notify, trace — determine whether this is one child's illness or a community outbreak. Vaccine-preventable disease outbreak response is the disciplined, time-critical system that converts that first encounter into protection for everyone around the child. [3] [1]
A vaccine-preventable disease (VPD) is an infection for which a safe, effective vaccine exists and is routinely recommended — in childhood these are principally measles, mumps, rubella, pertussis, varicella, poliomyelitis, Haemophilus influenzae type b, pneumococcal disease, rotavirus, hepatitis B, diphtheria and tetanus. An outbreak is the occurrence of cases above the expected baseline in a defined place, time and population. The response is the coordinated set of clinical and public-health actions taken to contain the outbreak, interrupt transmission, prevent further cases, and reinforce the immunisation programme so the next imported case does not ignite another one. [1] [6]
The clinician's work has three faces. The acute face is to recognise the individual child with a VPD, treat and isolate them, and trigger the response. The contact face is to build and triage the contact list, delivering prophylaxis to those who need it most within the narrow windows that work. And the population face is to run the vaccination campaign — ring and catch-up dosing that lifts coverage back above the herd-immunity threshold — because the outbreak ends when the susceptible pool is closed, not when the first child recovers. [2] [11]
Classification
Classify the outbreak response the way it plays out — by the agent, because each VPD dictates its own R₀, incubation period, exclusion rule and post-exposure lever, and by the phase of the response, because the same contact is managed differently in the contain, interrupt and prevent beats. Keeping the agent in the classification is what stops a clinician applying the measles prophylaxis window to a pertussis contact, or the varicella exclusion rule to mumps. [1] [4]
By agent, the common childhood VPDs divide by their transmission efficiency and their prophylactic levers. Measles, with an R₀ of twelve to eighteen, is airborne and the most contagious; its prophylaxis is MMR within seventy-two hours for susceptible contacts and immunoglobulin within six days for high-risk contacts. Pertussis, with a similarly high R₀, is droplet-spread and its prophylaxis is a macrolide for high-risk contacts. Varicella is airborne and contact-spread, excluded until lesions are crusted, with vaccine within three to five days and VZIG for the immunocompromised and pregnant. Mumps and rubella complete the MMR-preventable group. [2] [4]
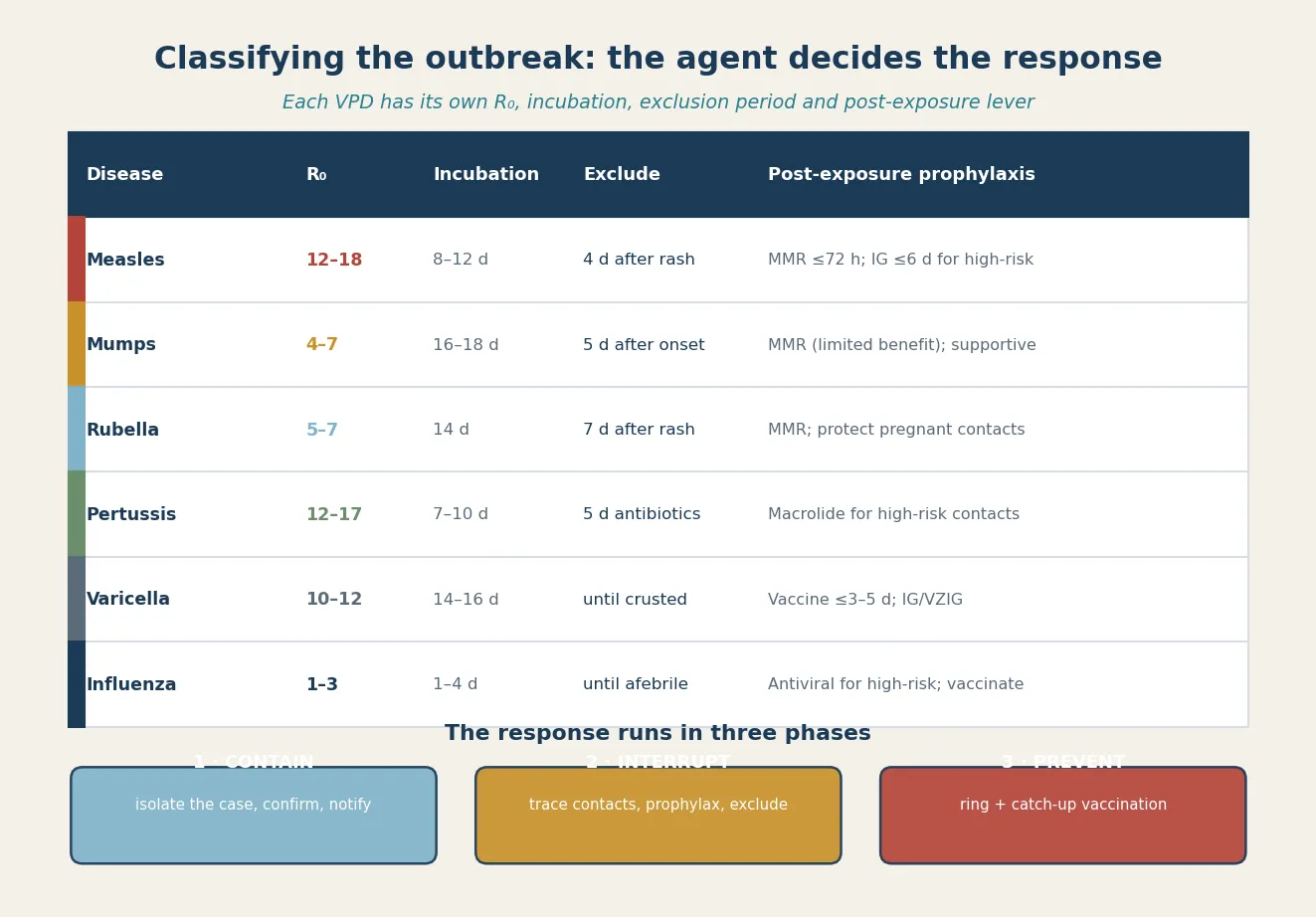
By response phase, the same outbreak is managed in three sequential but overlapping beats. Contain begins the moment a case is suspected — recognise, isolate, confirm, notify. Interrupt is the contact-tracing and prophylaxis beat — build the list, triage, prophylax, exclude. Prevent is the vaccination beat — ring and catch-up dosing, communication and documentation that close the loop and protect the next imported case. These phases are not bureaucratic stages; they are the temporal logic of an outbreak, because the early beats decide how many contacts the later beats have to chase. [1] [7]
Epidemiology & Risk Factors
Where do VPD outbreaks occur, and who do they hurt? Outbreaks recur in countries that have interrupted endemic transmission whenever vaccination coverage falls below the herd-immunity threshold and an imported case meets a susceptible pool. The measles outbreak in an underimmunised Amish community in Ohio illustrated the mechanism precisely: a single imported case in a community with low coverage produced sustained transmission, and the response depended on ring and catch-up vaccination that lifted coverage back above the threshold. The global partnership against measles and rubella has driven enormous progress, but that progress is fragile — it reverses wherever coverage dips. [7] [12]
The dominant risk factor at every level is under-vaccination — whether from parental refusal, missed doses, access barriers, or waning immunity. A review of measles and pertussis resurgences in the United States found that vaccine refusal was associated with an elevated risk of both diseases, and that under-vaccination — in clusters defined by geography, belief or access — is the substrate on which outbreaks ignite. Outbreaks do not occur at random in a well-vaccinated population; they find the clusters. [6] [3]
The epidemiology of each disease shapes its outbreak pattern. Measles, with its extreme R₀, demands the highest coverage and produces the largest outbreaks from the smallest coverage gaps. Mumps resurges in young-adult and adolescent populations whose vaccine-induced immunity has waned, as documented in outbreaks in close-contact settings such as universities and religious communities; a third MMR dose has been recommended in outbreak settings to blunt transmission. Pertussis resurges cyclically because acellular-vaccine immunity wanes faster than whole-cell immunity, sustaining transmission in adolescents and adults who infect the infants they care for. Varicella outbreaks continue in settings with one-dose or low coverage, and the two-dose strategy has been shown to improve effectiveness in preventing community transmission. [8] [10] [9]
Pathophysiology
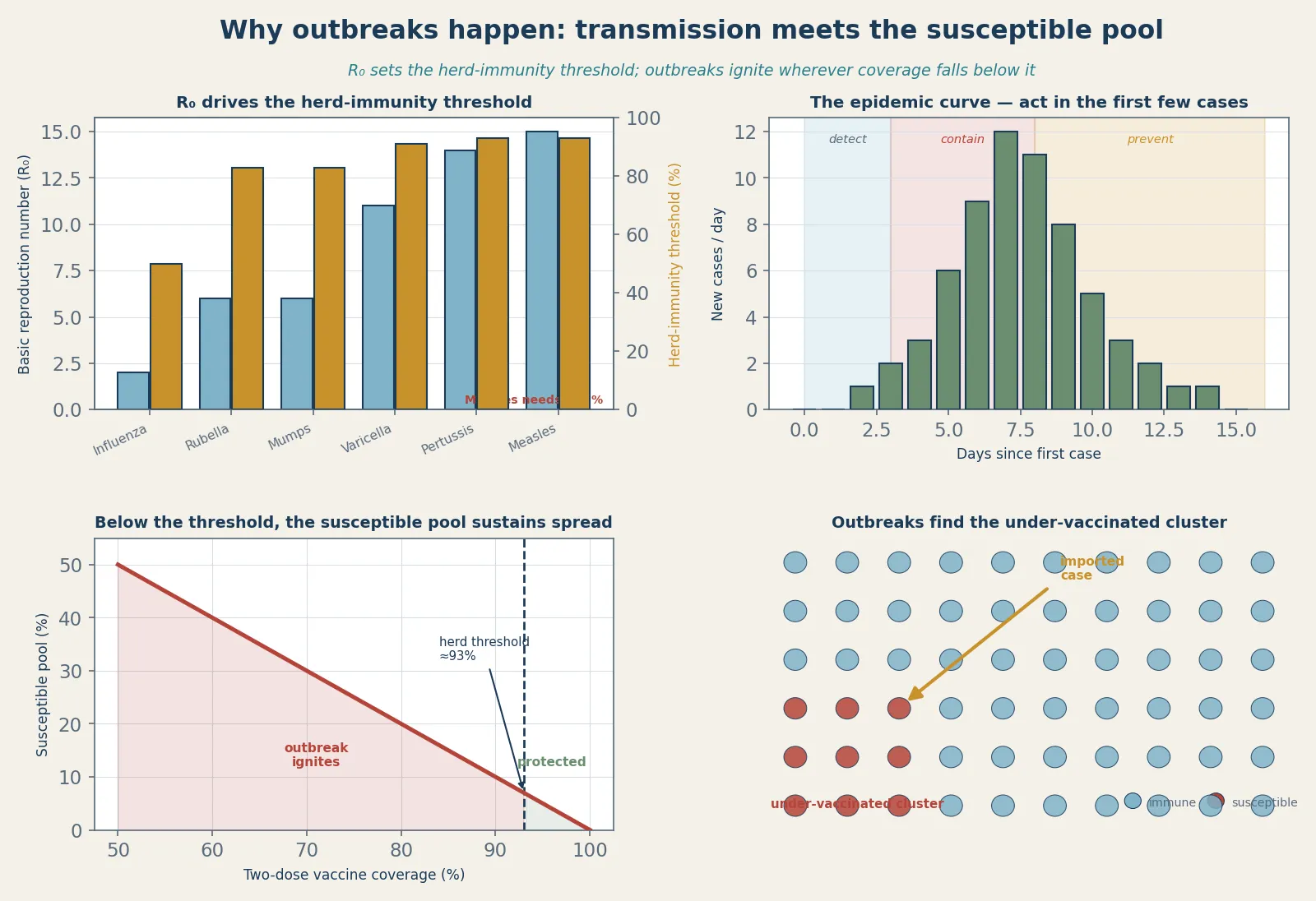
Why do VPD outbreaks happen at all, and why is measles so hard to control? The answer lies in the arithmetic of transmission. The basic reproduction number, R₀, is the average number of secondary cases produced by one case in a fully susceptible population. Measles has the highest R₀ of any human pathogen — twelve to eighteen — which means a single case in a fully susceptible population infects up to eighteen others. The herd-immunity threshold — the fraction of the population that must be immune to prevent sustained transmission — rises with R₀: roughly one minus one over R₀, which for measles is about ninety-three to ninety-five per cent. This is why measles is the disease that punishes every dip in coverage. [3] [11]
The herd-immunity threshold is not a single number for a population; it is a local property. When a community, a school, or a clinic's catchment falls below the threshold, a susceptible pool accumulates — a cohort of non-immune children who sustain transmission once an imported case arrives. Combining serological and contact data shows that the target immunity level needed to achieve and maintain elimination depends on both the contact structure and the existing immunity, which is why even national coverage above the threshold cannot protect an under-vaccinated cluster embedded within it. Outbreaks are local failures of a global average. [11] [6]
Waning immunity is a second mechanism that sustains VPD transmission even in vaccinated populations. For mumps and pertussis, vaccine-induced protection declines over years, so that adolescents and adults become susceptible again — not severely ill, but infectious enough to sustain transmission and to infect the infants and immunocompromised who cannot be fully protected by their own vaccination. The mumps outbreaks in close-contact young-adult settings and the recommendation for a third MMR dose in outbreak response are the operational consequences of waning. The outbreak response therefore has two prevention levers: closing the coverage gap in the never-vaccinated, and topping up the waning immunity of the previously vaccinated. [8] [10]
Measles adds a third mechanism that makes its outbreaks especially damaging: immune amnesia. Measles infects and depletes memory B and T lymphocytes, erasing the child's existing immune memory and driving a two-to-three-year rise in overall childhood infectious-disease mortality. This means a measles outbreak is not only an outbreak of measles — it is an immunological reset of a cohort of children that leaves them vulnerable to other infections for years. Preventing the outbreak prevents this invisible, delayed harm. [5] [3]
Clinical Presentation
The clinical presentation of a VPD outbreak begins with the index case — the child whose illness is recognised and reported. The fellowship skill is to recognise the prodromes of the common VPDs and to act before confirmation, because the contagious window of most VPDs precedes the pathognomonic sign. A febrile, unvaccinated child with cough, coryza and conjunctivitis who is about to develop a cephalocaudal rash is measles until proven otherwise, and the child is most infectious in the prodrome, before the rash appears. [3] [1]
Pertussis presents differently by age. In an older child it is the classic paroxysmal cough with an inspiratory whoop and post-tussive vomiting; in an infant under six months the whoop is often absent and apnoea may be the only — and lethal — sign. A household or childcare cough contact for an infant is pertussis until proven otherwise, and the presentation that should trigger the response is the apnoeic or cyanotic infant in a coughing household. Varicella presents with the characteristic crops of vesicles in different stages; mumps with parotitis; rubella with a mild rash and lymphadenopathy. [4] [9]
The outbreak declares itself in the contact network. A cluster of febrile-rash illness in a school or childcare, a cluster of paroxysmal cough in a household with an infant, or a rise in parotitis in a university are outbreak signals. The clinical task at the index encounter is not only to diagnose the child but to ask the questions that map the outbreak: where has the child been while infectious, who are the pregnant, infant and immunocompromised contacts, and what is the vaccination status of the network? The contact history is the bridge from the bedside case to the community response. [7] [6]
Differential Diagnosis
The differential of a suspected VPD outbreak is the differential of the index presentation, because the response is triggered by the clinical suspicion before laboratory confirmation. For a febrile-rash illness in an unvaccinated child, the differential spans the enteroviral and adenoviral exanthems, roseola infantum, scarlet fever, Kawasaki disease, drug eruption, dengue and other travel-related exanthems — but the operational rule is that any unvaccinated child with fever and a cephalocaudal rash, or with Koplik spots, is managed as measles until PCR excludes it, because the cost of allowing measles transmission far exceeds the cost of temporary isolation. [3] [1]
For a paroxysmal cough, the differential includes viral bronchitis, asthma, foreign-body aspiration, mycoplasma and cystic-fibrosis exacerbation — but an infant with apnoea and a coughing household, or a paroxysmal cough lasting more than two weeks, is managed as pertussis while PCR is pending. For parotitis, the differential includes other viral parotitides, bacterial parotitis, salivary duct obstruction and lymphadenopathy, but in the setting of a mumps outbreak or an under-vaccinated community, mumps is managed presumptively. [4] [8]
[3] [1]The broader point is that the outbreak-response frame changes the threshold for action. In a well-vaccinated child with a non-specific exanthem, the prior probability of measles is low and observation is reasonable. In an unvaccinated child, in an outbreak setting, or with a known exposure, the same presentation demands isolation, testing and notification immediately. The differential is the same; the response threshold is not. [6] [2]
Clinical & Bedside Assessment
The assessment of a suspected VPD case at the bedside is built around three questions: what is the diagnosis, who has the child exposed, and who in the network is at highest risk? Establish the onset of symptoms relative to the infectious period, the vaccination history (documented doses and dates), potential exposures (travel, unvaccinated communities, known outbreaks, healthcare or school contacts in the relevant incubation window), and examine for the disease-specific signs — Koplik spots, parotitis, the vesicle crops of varicella, the paroxysmal cough. [3] [1]
Document the public-health essentials at the bedside because they drive the entire response. Record the date of symptom onset and, for rash illnesses, the date of rash onset; calculate the infectious period (for measles, from four days before to four days after the rash; for pertussis, from catarrhal onset to three weeks of paroxysms or five days of antibiotics); map the school, childcare and healthcare exposures; and begin the contact list with particular attention to pregnant women, infants and immunocompromised contacts. These details determine notification, exclusion, and who needs prophylaxis. [1] [2]
For each contact identified, the bedside assessment asks the triage questions that decide urgency. Who is pregnant, and at what gestation — because rubella, varicella and pertussis in pregnancy carry fetal or neonatal consequences? Who is under six to twelve months — because infants are the most vulnerable to pertussis and measles and cannot be fully protected by their own vaccination? Who is immunocompromised — because they cannot receive live vaccines and need immunoglobulin? A careful contact triage at the first encounter prevents the late, disorganised public-health scramble that costs the vulnerable contacts their window. [4] [2]
The bedside-to-public-health handover
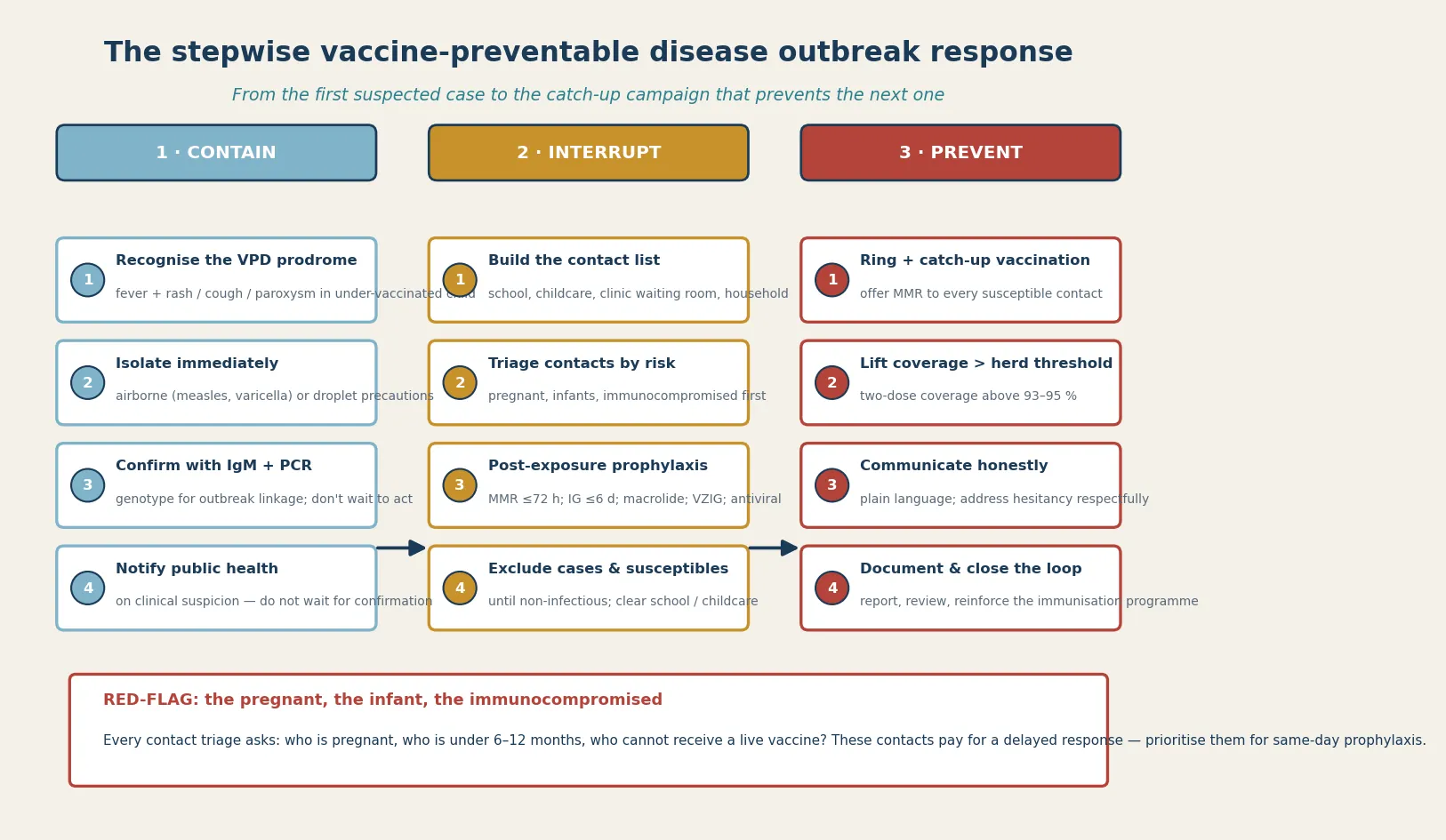
Recognise the VPD prodrome in an under-vaccinated or exposed child and isolate immediately with the correct precautions (airborne for measles and varicella; droplet for pertussis).
Document onset date, rash date, infectious period, and all school, childcare, clinic and household exposures; begin the contact list.
Confirm with the disease-specific test — IgM and PCR with genotype for measles; PCR for pertussis within three to four weeks; PCR or serology for the others.
Notify public health on clinical suspicion; do not wait for laboratory confirmation to start the response.
Triage every contact for the high-risk markers — pregnant, infant under 6–12 months, immunocompromised — and flag them for same-day prophylaxis.
Investigations
Investigation of a suspected VPD outbreak rests on pathogen-specific testing timed to the illness, plus genotyping for outbreak linkage. For measles, the recommended approach is measles-specific IgM on a single serum at first contact together with RT-PCR and virus genotyping on a throat or nasopharyngeal swab and urine in the first few days of the rash; the genotype links cases into a chain and distinguishes imported from endemic transmission. For pertussis, PCR of a nasopharyngeal aspirate or swab is the test of choice in the first three to four weeks, with serology for late presentations. [1] [4]
For mumps, PCR or viral culture of a buccal swab plus serology; for rubella, IgM and PCR; for varicella, PCR of vesicle fluid or scraping is preferred over the older Tzanck method. In an outbreak, the laboratory is not only confirming cases — it is defining the chain of transmission through genotyping and the epidemic curve. A rising count of PCR-positive cases linked by genotype and exposure is the laboratory signature of an outbreak, and it directs the contact-tracing effort to the settings that matter. [8] [9]
In Australia and Aotearoa New Zealand, measles, mumps, rubella, pertussis and varicella are nationally notifiable diseases, and suspected measles is notified on clinical suspicion — do not wait for confirmation. PCR, IgM and genotyping are available through public-health laboratories, and public-health units coordinate the contact-tracing, prophylaxis and outbreak-vaccination response. The Australian Immunisation Handbook (ATAGI) and the New Zealand Immunisation Schedule set the prophylaxis windows, exclusion periods and the outbreak-response framework. [1]
Supportive tests round out the workup as the clinical picture demands. A full blood count in pertussis often shows a marked lymphocytosis; in measles, a lymphopenia consistent with the viral and immunosuppressive nature of the illness. Serology for immunity — measles, varicella and rubella IgG — is essential for defining the susceptible contacts who need prophylaxis or catch-up vaccination, and for the pregnant contact whose immune status determines the urgency of the response. [3] [4]
Management — Resuscitation
Resuscitation in a VPD outbreak is about the contacts and cases who decompensate. For pertussis in an infant, the red flags are apnoea, cyanosis, pneumonia and exhaustion; the infant needs admission to a monitored bed with continuous apnoea and oxygenation monitoring and a low threshold for PICU involvement, because apnoea can be the first and lethal sign. For measles complicated by pneumonia, croup with stridor, dehydration, encephalitis or corneal ulceration, the deteriorating respiratory or neurological status is the trigger to escalate. [4] [3]
Supportive care is individualised to the disease: fluids and nutrition for the child with measles who is dehydrated and anorexic; oxygen, gentle suctioning and minimal stimulation for the infant with pertussis paroxysms; antipyretics and hydration for varicella; and disease-specific treatment — vitamin A for measles, a macrolide for pertussis, antivirals for severe influenza or varicella in the immunocompromised. The resuscitation frame, however, is always two-layered: treat the child, and contain the community, because a child who recovers but infects an infant has not been managed well. [3] [4]
Isolation of the case from the moment of suspicion is the first resuscitative act for the community. Measles and varicella require airborne precautions (negative-pressure where available); pertussis and mumps require droplet precautions. The infectious period, not the recovery, sets the exclusion: four days after the measles rash, five days of effective antibiotic for pertussis, until lesions are crusted for varicella, five days after parotitis onset for mumps. Notifying public health on suspicion triggers the contact-tracing and prophylaxis cascade that protects the rest of the network. [1] [2]
Management — Definitive & Stepwise
Definitive management of a VPD outbreak is a stepwise pathway that runs from the index case through the contact network to the vaccination campaign. The same logic applies to every disease, with disease-specific windows and levers. The sequence is: recognise and isolate the case; confirm with the disease-specific test and genotype; notify public health; build and triage the contact list; deliver post-exposure prophylaxis within its window; exclude cases and susceptible contacts; and run the ring and catch-up vaccination that closes the susceptible pool. [1] [7]
The disease-specific post-exposure prophylaxis levers
Measles: offer MMR within 72 hours of exposure to susceptible contacts; give normal human immunoglobulin within 6 days to high-risk contacts (pregnant, immunocompromised, infants under 6–12 months) who cannot be vaccinated.
Pertussis: offer a macrolide (azithromycin first-line) to high-risk contacts — infants under 12 months, pregnant women, and unvaccinated household contacts.
Varicella: give varicella vaccine within 3 to 5 days to susceptible contacts; give VZIG to the immunocompromised, the pregnant non-immune, and the newborn of a peripartum mother.
Mumps: post-exposure MMR has limited benefit once exposed, but offer it to under-immunised contacts to close future susceptibility; a third dose is recommended in outbreak settings for those at risk.
Rubella: MMR is the lever; the operational priority in a rubella contact is the pregnant woman, whose serology and gestation determine the counselling.
The post-exposure prophylaxis window is the time-critical core of the response, and missing it is the most common failure. MMR given within seventy-two hours of measles exposure can prevent or modify disease in a susceptible contact; immunoglobulin given within six days protects the high-risk contacts who cannot receive the live vaccine. For pertussis, a macrolide given promptly to high-risk contacts limits transmission to the infant at the centre of the household. The principle is that prophylaxis is a race against the incubation period, and the contact list must be built and triaged fast enough to reach people inside the window. [1] [4]
The prevention beat is the vaccination campaign that closes the susceptible pool. Ring vaccination — offering MMR to every susceptible contact around a case — and catch-up vaccination across the affected school or community lift two-dose coverage back above the herd-immunity threshold. The measles outbreak in the underimmunized Amish community was controlled through exactly this mechanism: rapid case identification, isolation and an aggressive vaccination campaign that raised coverage and interrupted transmission. The outbreak ends when the susceptible pool is closed, and the campaign is what closes it. [7] [11]
Specific Subtypes & Scenarios
A measles outbreak in an under-vaccinated school or community. This is the canonical scenario. Isolate each case, confirm with IgM and PCR with genotype, notify public health, trace the school and household contacts, offer MMR within seventy-two hours and immunoglobulin within six days to high-risk contacts, exclude susceptible children until the incubation period clears, and run a catch-up vaccination campaign that lifts coverage above ninety-five per cent. The infants and pregnant women at the edge of the outbreak are the ones who pay for delay. [1] [7]
An infant with apnoea and a household cough contact — pertussis. This is the highest-risk pertussis presentation. Admit for monitoring, confirm with PCR, start a macrolide, isolate with droplet precautions, notify, and prophylax the household — particularly any other infant, any pregnant woman, and any unvaccinated contact. Reinforce maternal Tdap for future pregnancies and catch-up vaccination for the household. The apnoeic infant is the face of pertussis severity and the reason the contact network matters. [4] [6]
A mumps outbreak in a university or close-contact young-adult setting. This is the waning-immunity outbreak. Recognise parotitis, confirm with PCR or serology, isolate and exclude, and — because acellular and single-dose immunity has waned — offer a third MMR dose to the at-risk group, as recommended in outbreak settings. The lesson is that even a well-vaccinated population can sustain mumps transmission when immunity has waned, and the response lever is a targeted booster. [8] [10]
A varicella outbreak in a school or childcare. Confirm clinically and with PCR where needed, exclude until lesions are crusted, offer varicella vaccine to susceptible contacts within three to five days, and give VZIG to the immunocompromised, the pregnant non-immune, and the newborn of a peripartum mother. The two-dose strategy has improved effectiveness in preventing community transmission, so catch-up to two doses is the prevention lever. [9] [2]
A pregnant contact of a measles, rubella, varicella or pertussis case. This is the contact triage that decides the fetal and neonatal outcome. Check the documented immune status, send urgent serology if unknown, deliver the disease-specific prophylaxis within its window, and counsel honestly about the gestation-specific risk. The pregnant contact is the reason the contact list is triaged by risk, not by convenience. [2] [4]
Complications & Pitfalls
The most common and damaging pitfall is waiting for confirmation to act. Because the contagious window of measles, pertussis and varicella precedes the pathognomonic sign, a clinician who waits for PCR to isolate and notify has already allowed transmission. The rule is to suspect, isolate and notify on the prodrome, and to let the laboratory confirm what the response is already managing. This single discipline — act on suspicion — is the difference between a contained case and an outbreak. [3] [1]
A second pitfall is missing the prophylaxis window. The seventy-two-hour window for MMR and the six-day window for immunoglobulin are narrow, and they close while the contact list is still being built. The contact-tracing effort must be fast enough and prioritised enough — pregnant, infant, immunocompromised first — to reach the high-risk contacts inside the window. A contact list that is complete in two weeks but whose infants were identified in two days is a failed list. [2] [4]
A third pitfall is applying the wrong disease-specific rule. The measles exclusion is four days after the rash; the pertussis exclusion is five days of antibiotic; the varicella exclusion is until crusted; the mumps exclusion is five days after parotitis onset. Confusing these — keeping a pertussis case out for the measles window, or releasing a measles case under the pertussis rule — produces both over-exclusion that disrupts families and under-exclusion that perpetuates transmission. The agent decides the rule. [1] [4]
Vaccine refusal and VPD resurgence
Population: Systematic review of measles and pertussis outbreaks in the United States, and a detailed account of a measles outbreak in an underimmunized Amish community.
Key finding
Vaccine refusal was associated with an elevated risk of measles and pertussis, and outbreaks recurrently ignited in under-vaccinated clusters; the Amish outbreak was controlled by rapid identification, isolation and an aggressive vaccination campaign that lifted coverage.
Practice change
Outbreaks are local failures of coverage; the response is detection plus ring and catch-up vaccination that closes the susceptible pool and lifts coverage back above the herd threshold.
A fourth pitfall is forgetting the waning-immunity diseases. Mumps and pertussis can outbreak in well-vaccinated populations because immunity has waned, and a clinician who dismisses parotitis or a prolonged paroxysmal cough in a vaccinated person as non-infectious misses the outbreak. A suggestive presentation warrants testing regardless of vaccination status, and the mumps response may require a third MMR dose. [8] [10]
The final pitfall is treating the outbreak as over when the cases settle. The susceptible pool that allowed the outbreak persists until coverage is restored, and without the catch-up campaign the next imported case ignites the next outbreak. The response is complete only when two-dose coverage is back above the herd-immunity threshold and the programme has learned from the failure. [11] [12]
Prognosis & Disposition
The prognosis of a VPD outbreak is determined by the speed and completeness of the response. An outbreak detected in its first few cases, with rapid isolation, tracing, prophylaxis and vaccination, is contained with few secondary cases; an outbreak detected late, in a large under-vaccinated network, produces dozens to hundreds of cases and the severe complications that follow — measles pneumonia and encephalitis, pertussis apnoea and death in infants, congenital rubella syndrome, and the multi-year immune-amnesia aftermath of measles. The epidemic curve is the prognosis: a curve that bends early is a response that worked. [7] [5]
For the individual case, disposition follows severity: admit the infant with pertussis apnoea, the child with measles pneumonia or encephalitis, and any case with dehydration, respiratory distress or neurological compromise; manage uncomplicated cases at home with isolation, clear safety-netting and the public-health follow-up. For the contacts, disposition is determined by the prophylaxis and exclusion plan: those within the window receive prophylaxis, those susceptible are excluded through the incubation period, and the high-risk contacts are reviewed same-day. [3] [4]
At the population level, the prognosis is the coverage. Where two-dose coverage is sustained above the herd-immunity threshold, imported cases cause limited spread; where it dips, outbreaks recur. The global partnership against measles and rubella has demonstrated that sustained, high-coverage vaccination can drive these diseases toward elimination, but the partnership also shows that the gains reverse rapidly when coverage falls. The disposition of an outbreak, then, is not only its containment but the reinforcement of the immunisation programme that prevents the next one. [12] [11]
Special Populations
Pregnant women are the contact population whose outcome is most altered by the response. A pregnant contact of measles, rubella, varicella or pertussis needs urgent immune-status assessment, disease-specific prophylaxis within its window, and honest gestation-specific counselling. Rubella in the first trimester, varicella in pregnancy, and pertussis in the neonatal period are the fetal and neonatal consequences the response exists to prevent. The pregnant contact is always triaged first. [2] [4]
Infants under six to twelve months are too young to be fully protected by their own vaccination and are among the most vulnerable to severe pertussis and measles. They rely on herd immunity, maternal antibody (for pertussis, transplacentally from maternal Tdap), and — after exposure — immunoglobulin prophylaxis. Protecting the infant is the population point of high coverage and the reason maternal Tdap is given in every pregnancy. [1] [4]
Immunocompromised children cannot receive live vaccines (MMR, varicella) and depend on the immunity of those around them; measles and varicella in this group can be severe or fatal, and immunoglobulin prophylaxis after exposure is indicated within the window. Their protection is a population responsibility, and an exposure in this group is an emergency for the same reason their vaccination is not an option. [1] [9]
Under-vaccinated and vaccine-hesitant communities carry the burden of outbreaks. Address vaccine hesitancy respectfully and with evidence, offer catch-up vaccination at every opportunity, and recognise that under-immunised pockets — geographic, belief-based or access-defined — are where outbreaks ignite most violently. The review of measles and pertussis resurgence makes the case directly: refusal and under-vaccination are the substrate of outbreaks. [6] [7]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families may face barriers to timely immunisation and care. Ensure culturally safe, equitable access to vaccination and outbreak response, use trained interpreters rather than family members, and recognise that disadvantage should never be the reason a contact is identified late or a woman reaches pregnancy non-immune. [1] [12]
Rural and remote children and families need timely access to diagnosis, prophylaxis and public-health follow-up through outreach and telehealth, because distance can delay the response a sick child or a pregnant contact cannot afford to wait for. The plan for a remote family accounts for what is locally available and mobilises retrieval and public-health support early. [1] [2]
Evidence, Guidelines & Regional Differences
The global standard for VPD outbreak response is anchored in the WHO position papers and the ACIP summary recommendations, which set the disease-specific prophylaxis windows, exclusion periods, and the vaccination schedule that underpins herd immunity. The global partnership against measles and rubella has documented the enormous progress toward elimination — and the fragility of that progress when coverage falls. These documents are the operational reference for national programmes worldwide. [1] [12]
The transmission-dynamics evidence underpins the whole response. The herd-immunity threshold rises with R₀, and measles — with the highest R₀ — demands the highest coverage; combining serological and contact data shows that the target immunity level for elimination depends on both contact structure and existing immunity, which is why local coverage gaps matter more than national averages. The immune-amnesia evidence adds a hidden, long-acting cost to every measles outbreak that strengthens the case for prevention. [11] [5]
Herd immunity, target levels and outbreak control
Population: Mathematical and population-level analyses combining serological, contact and mortality data to derive the immunity levels needed for measles elimination and to quantify the post-measles immune-amnesia mortality.
Key finding
The target immunity level for elimination depends on both contact patterns and existing immunity; measles induces a prolonged increase in overall childhood infectious-disease mortality through immune amnesia.
Practice change
Sustain two-dose coverage above the herd threshold locally, not just nationally; preventing measles prevents both the acute outbreak and the multi-year immune-amnesia aftermath.
The disease-specific outbreak evidence shapes the levers. The measles outbreak in the underimmunized Amish community showed that rapid identification and aggressive vaccination control transmission; the mumps outbreaks in close-contact young-adult settings and the recommendation for a third MMR dose showed the waning-immunity lever; the pertussis resurgence and vaccine-refusal review showed the under-vaccination substrate; and the varicella two-dose effectiveness study showed the prevention lever for community transmission. Each disease teaches a different failure mode and a different response lever. [7] [8] [10] [9]
The regional policy structure is consistent in principle and varies in detail. In ANZ, the VPDs are nationally notifiable, the Australian Immunisation Handbook (ATAGI) and the New Zealand Immunisation Schedule set the prophylaxis windows, exclusion periods and the outbreak-response framework, and public-health units coordinate contact tracing and outbreak vaccination. In the UK, UKHSA guidance and the Green Book direct the programme, including the MMR catch-up campaigns that follow outbreaks. In the US, the ACIP/CDC schedule and surveillance deliver the equivalent strategy, with measles elimination declared but periodically challenged by imported cases in under-vaccinated pockets. In Canada, the Canadian Immunization Guide and provincial public health deliver the same strategy. The shared principle is that high two-dose coverage, prompt notification and the disease-specific prophylaxis windows are the universal defence. [1] [2]
The controversies and active issues are real: sustaining the high coverage that herd immunity demands in the face of hesitancy and access barriers; the timing and reach of post-exposure prophylaxis in dispersed or hard-to-reach communities; whether a third MMR dose should be routine or reserved for outbreaks; and the inequities that leave some communities under-vaccinated. The defence against each is the same: high two-dose coverage, prompt notification, disease-specific prophylaxis within its window, and a public-health layer that does not stop at the bedside. [6] [11]
Exam Pearls
- The response is one system: DETECT (recognise, isolate, confirm, notify), INTERRUPT (trace, triage, prophylax, exclude), PREVENT (ring + catch-up vaccination, communicate, document). [1]
- Measles R₀ is 12–18 — the highest of any pathogen — so herd immunity needs two-dose coverage above 95 per cent; outbreaks ignite in under-vaccinated clusters wherever coverage dips. [3] [11]
- Act on suspicion, not confirmation: isolate and notify on the prodrome, because the contagious window precedes the pathognomonic sign. [1]
- Confirm measles with IgM plus RT-PCR with genotype; the genotype links cases into a chain and distinguishes imported from endemic transmission. [1]
- Post-exposure prophylaxis windows are narrow: MMR ≤72 h, normal human immunoglobulin ≤6 d for high-risk measles contacts; macrolide for high-risk pertussis contacts; varicella vaccine ≤3–5 d, VZIG for the immunocompromised and pregnant. [2] [4]
- Triage the contact list by risk first — pregnant, infant under 6–12 months, immunocompromised — because these contacts pay most for a delayed response. [2]
- Exclusion is disease-specific: measles 4 d after the rash, pertussis 5 d of antibiotic, varicella until crusted, mumps 5 d after parotitis onset. [1] [4]
- Waning immunity drives mumps (and pertussis) outbreaks in vaccinated populations — a third MMR dose is recommended in mumps outbreak settings. [8] [10]
- Measles causes immune amnesia — a two-to-three-year rise in overall infectious-disease mortality — so preventing the outbreak prevents hidden, delayed harm. [5]
- The outbreak ends when the susceptible pool is closed: ring and catch-up vaccination lift coverage back above the herd-immunity threshold. [7] [11]
References
- [1]WHO Measles vaccines: WHO position paper. Wkly Epidemiol Rec, 2009.PMID 19714924
- [2]McLean HQ; Fiebelkorn AP; Tempte JL; Wallace GS Prevention of measles, rubella, congenital rubella syndrome, and mumps, 2013: summary recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep, 2013.PMID 23760231
- [3]Perry RT; Halsey NA The clinical significance of measles: a review. J Infect Dis, 2004.PMID 15106083
- [4]WHO Pertussis vaccines: WHO position paper, August 2015--Recommendations. Vaccine, 2016.PMID 26562318
- [5]Mina MJ; Metcalf CJE; de Swart RL; Osterhaus ADME; Grenfell BT Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality. Science, 2015.PMID 25954009
- [6]Phadke VK; Bednarczyk RA; Salmon DA; Omer SB Association Between Vaccine Refusal and Vaccine-Preventable Diseases in the United States: A Review of Measles and Pertussis. JAMA, 2016.PMID 26978210
- [7]Gastañaduy PA; Budd J; Fisher N; Redd SB; et al A Measles Outbreak in an Underimmunized Amish Community in Ohio. N Engl J Med, 2016.PMID 27705270
- [8]Barskey AE; Schulte C; Rosen JB; Handschur EF; et al Mumps outbreak in Orthodox Jewish communities in the United States. N Engl J Med, 2012.PMID 23113481
- [9]Perella D; Wang C; Glynn A; Hoffman K; et al Varicella Vaccine Effectiveness in Preventing Community Transmission in the 2-Dose Era. Pediatrics, 2016.PMID 26977081
- [10]Albertson JP; Clegg WJ; Reyes JD; Cnossen T; et al Mumps Outbreak at a University and Recommendation for a Third Dose of Measles-Mumps-Rubella Vaccine --- Illinois, 2015-2016. MMWR Morb Mortal Wkly Rep, 2016.PMID 27467572
- [11]Funk S; Knapp JK; Lebo E; Reef SE; et al Combining serological and contact data to derive target immunity levels for achieving and maintaining measles elimination. BMC Med, 2019.PMID 31551070
- [12]Strebel P; Cochi S; Grabowsky M; Bilous J; et al Evolution and Contribution of a Global Partnership against Measles and Rubella, 2001-2022. Vaccines (Basel), 2024.PMID 38932422