Paeds · infectious-diseases
Varicella and herpes zoster
Also known as Chickenpox · Shingles · Varicella-zoster virus infection · Primary varicella · Herpes zoster reactivation · Human herpesvirus 3 infection
Fellowship topic on varicella (chickenpox) and herpes zoster (shingles) in children: the varicella-zoster virus and its neurotropic latency-and-reactivation biology; primary varicella with its crops of vesicles in all stages at once, and the dermatomal unilateral rash of zoster; the host-risk tiers that decide management from supportive care in the healthy child to intravenous aciclovir in the immunocompromised, neonate and pregnant patient; PCR and clinical diagnosis; the complications (pneumonia, encephalitis and cerebellitis, invasive group A streptococcal infection, congenital and neonatal varicella); the differential of vesicular rashes; isolation and exclusion rules; post-exposure prophylaxis with vaccine and varicella-zoster immune globulin; the two-dose live-attenuated varicella vaccine programme and the recombinant zoster vaccine; and ANZ, UK, US and Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
How to tell it is varicella at a glance
Overview & Definition
Picture a three-year-old brought in with a fever and an itchy rash that began on the trunk two days ago and now covers the face and limbs. The mother points out that some spots are red bumps, some are small blisters, and some are already scabbed over — and that is the single most useful bedside observation in paediatrics, because lesions of all stages at once is the signature of varicella. Recognising it instantly triggers the infection-control and public-health response that protects the vulnerable contacts behind this child. [2] [1]
Varicella, or chickenpox, is the primary systemic infection caused by the varicella-zoster virus, a highly contagious human neurotropic herpesvirus spread by respiratory droplets and direct contact with vesicle fluid. After the acute illness resolves, the virus establishes lifelong latency in the dorsal root and cranial-nerve ganglia. Decades later, when cell-mediated immunity wanes, the latent virus can reactivate along a single dermatome to produce herpes zoster, or shingles. The two diseases are therefore one virus observed at two points in a lifetime. [1] [5]
For most healthy children, varicella is a mild, self-limiting febrile illness. The clinician's job has two halves, and the second is what the fellowship examiner tests. The acute half is to confirm the diagnosis, gauge the host-risk tier, treat accordingly, and prevent spread. The preventive half is to deliver the immunisation programme, protect the non-immune high-risk contact after exposure, and understand the latency-and-reactivation biology that connects chickenpox today to shingles in decades to come. [7] [1]
Classification
Classify varicella-zoster virus disease the way it presents at the bedside — by disease phase, by host risk, and by severity — because each lens changes the management. The disease-phase lens separates primary varicella, the first systemic encounter, from herpes zoster, the dermatomal reactivation that appears years to decades later after a period of ganglionic latency. Most clinical encounters in children are with primary varicella, but a clinician who understands that zoster is the same virus reawakening will recognise the unilateral dermatomal rash correctly. [1] [5]
The host-risk lens is the one that matters most for treatment, because the same virus is a nuisance in one host and a killer in another. The immunocompetent child usually has uncomplicated, self-limiting disease managed supportively. The neonate, the immunocompromised child, and the pregnant patient are the high-risk hosts in whom primary varicella can disseminate to the lungs, liver and brain, and in whom intravenous aciclovir is given promptly. Holding the risk tier in mind at the first encounter prevents the dangerous default of treating every case as mild. [1] [6]
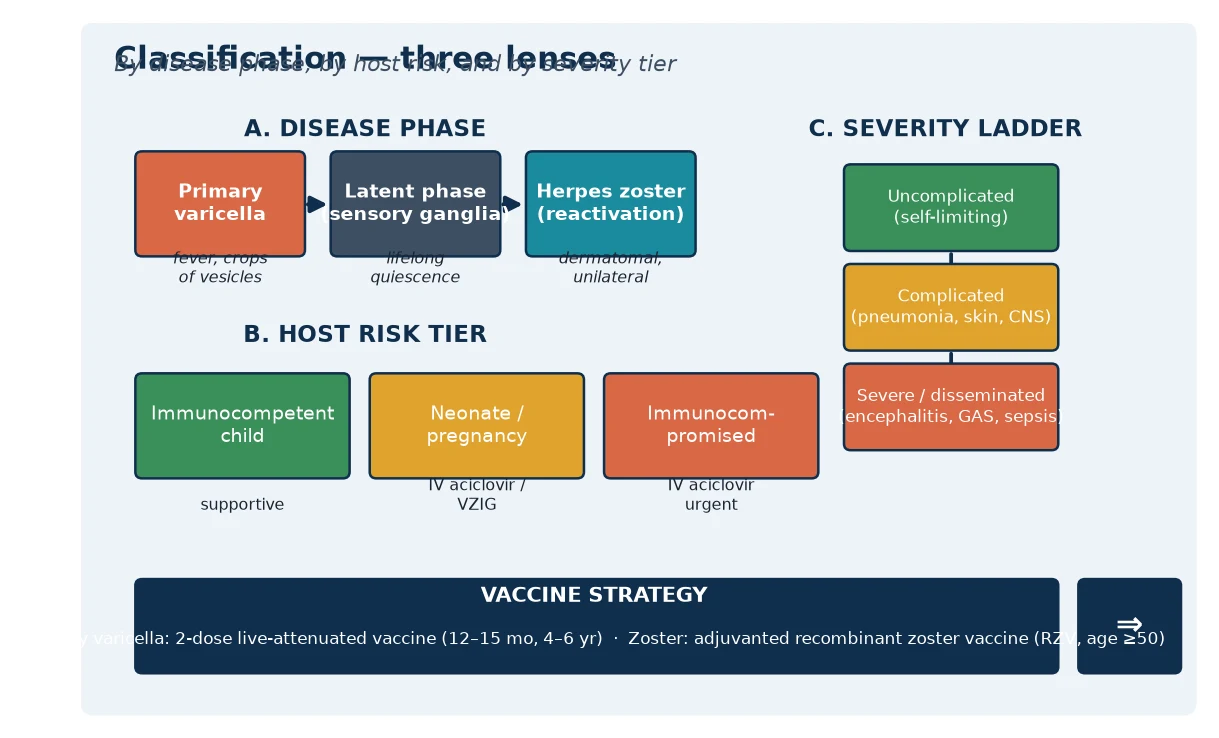
The severity lens sorts the disease from uncomplicated self-limiting infection through complicated disease — pneumonia, secondary bacterial skin infection, cellulitis, encephalitis or cerebellitis — to severe or disseminated disease with visceral involvement, sepsis or invasive group A streptococcal infection. A child who moves up this ladder needs escalation of monitoring, antiviral therapy and often admission, and the move is signalled by fever persisting, new respiratory or neurological signs, or a lesion that becomes red, hot and spreading. [2] [7]
A fourth distinction matters for prevention. Breakthrough varicella — disease in a previously vaccinated child — is usually milder, with fewer lesions, little or no fever, and a predominantly maculopapular rather than vesicular rash, and it is far less contagious. Recognising the milder vaccinated phenotype matters both clinically, because it changes the management, and epidemiologically, because it is the expected, not alarming, consequence of a vaccine that prevents most but not all disease. [9] [7]
Epidemiology & Risk Factors
Where does varicella sit, and who does it hurt? In countries without routine vaccination it is a near-universal childhood infection, with peak incidence in preschool and early school-age children and most cases occurring before adolescence. The disease is highly contagious, with secondary attack rates approaching ninety percent in susceptible household contacts, so a single case in an unvaccinated community spreads rapidly. Understanding the epidemiology directs both the clinical encounter and the preventive response. [1] [7]
Routine childhood immunisation has transformed the epidemiology wherever it has been implemented. The United States moved to a two-dose schedule after one-dose coverage reduced disease but left a residual burden of mild breakthrough cases, and the two-dose programme further reduced incidence, severity and hospitalisation. The result is a disease that is now uncommon in vaccinated populations but remains common where vaccine is absent, and the epidemiology is read through the lens of local vaccine coverage. [7] [3]
The burden of severe disease falls on the high-risk hosts. Immunocompromised children — those on chemotherapy, high-dose corticosteroids, or with primary immunodeficiency — are at risk of disseminated, fulminant disease. Neonates exposed peripartum can develop severe haemorrhagic or disseminated varicella, and maternal primary infection in pregnancy carries risks both to the mother and, in early pregnancy, to the fetus. Adults and adolescents, including pregnant adolescents, carry a higher risk of varicella pneumonia than young children do. [1] [11]
Under-vaccination and vaccine absence are the dominant individual and population risk factors. A child who has not received the varicella vaccine is fully susceptible, and unvaccinated communities sustain outbreaks. Migrant, refugee and disadvantaged families may have incomplete records or missed opportunities, so verifying immunisation status and offering catch-up vaccination is part of every encounter. The vaccinated child is far less likely to catch or spread the disease, and breakthrough disease, when it occurs, is milder. [7] [3]
Pathophysiology
Why does one virus cause a generalised rash today and a dermatomal rash in fifty years? The answer lies in the neurotropic, latency-and-reactivation biology of varicella-zoster virus. The virus enters through the respiratory mucosa and spreads to regional lymph nodes, where it replicates before a primary viraemia seeds the liver and other organs. A second wave of replication produces a secondary viraemia that carries the virus to the skin, where the characteristic vesicles erupt. [1] [2]
Crucially, during the viraemic phase the virus also reaches the sensory ganglia of the dorsal roots and cranial nerves, where it establishes lifelong latency in the neuronal cells. This is the step that makes herpes zoster possible. The host's cell-mediated immunity, rather than antibody, is what holds the latent virus in check, which is why immunosuppression and ageing — both of which erode cell-mediated immunity — are the principal triggers of reactivation. Antibody alone does not prevent zoster. [5] [1]
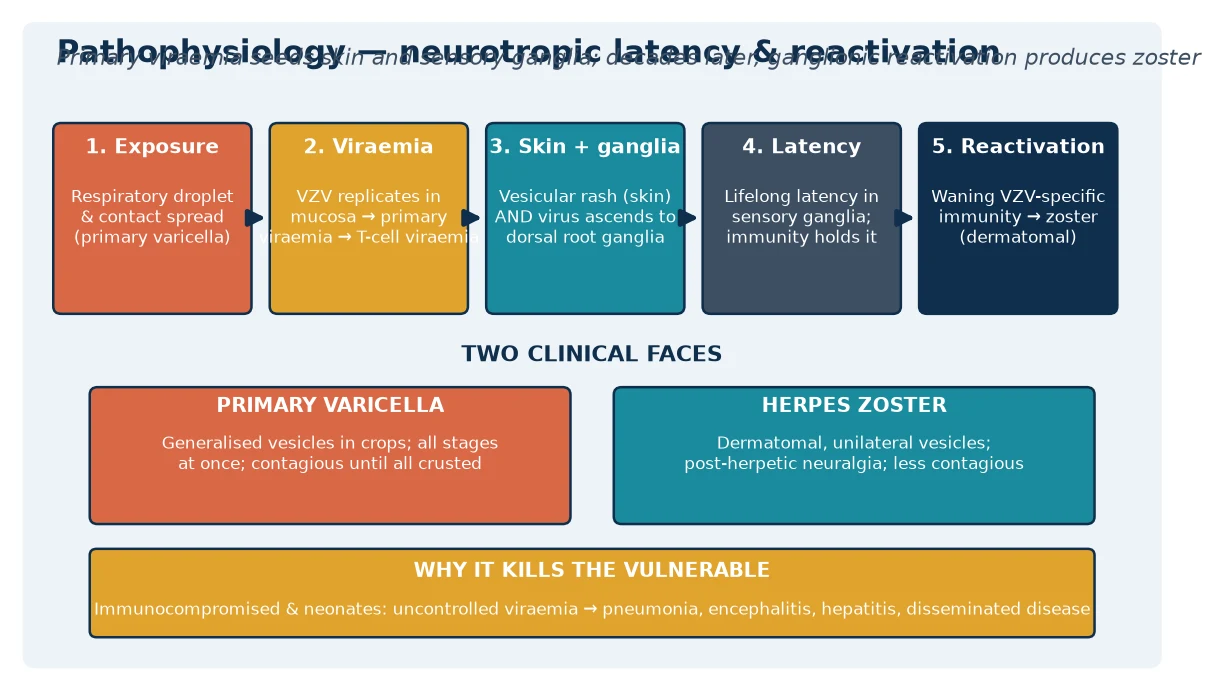
In primary varicella, the skin lesion begins as a papule, becomes a clear vesicle resting on an erythematous base — the "dewdrop on a rose petal" — then progresses to a pustule and finally a crust. Because successive crops of lesions appear over several days, lesions of every stage are visible simultaneously, and this is the clinical signature that distinguishes varicella from rashes with a single uniform stage. The crust marks the end of contagiousness for that lesion, and the child is infectious from one to two days before the rash until every lesion has crusted. [2] [1]
In herpes zoster, reactivation within a single sensory ganglion sends virus down the peripheral nerve to the dermatome it supplies, producing a painful, unilateral, dermatomal cluster of vesicles that does not cross the midline. The pain often precedes the rash by days, and post-herpetic neuralgia — persistent dermatomal pain after the rash resolves — is the feared chronic complication, more common with increasing age. Reactivation in the ophthalmic division of the trigeminal nerve is ophthalmic zoster, a zoster of the eye that threatens vision and needs urgent ophthalmology involvement. [5] [1]
The severe-disease biology follows from uncontrolled viral replication in a host who cannot contain it. In the immunocompromised child or neonate, the virus disseminates beyond the skin to the lungs, causing a haemorrhagic or interstitial pneumonia, to the liver and bone marrow, and to the brain, causing encephalitis. The same cascade that is self-limiting in the healthy child becomes fulminant when cell-mediated immunity is absent, which is exactly why these hosts receive intravenous aciclovir at the earliest suspicion. [1] [6]
Clinical Presentation
The classic presentation of primary varicella is a prodrome of one to two days of mild fever, malaise and sometimes headache or abdominal pain, followed by the rash. The rash begins on the face and trunk and spreads centrifugally to the limbs, and it favours covered areas, sparing the palms and soles. The defining feature is the successive crops: new lesions continue to appear for several days, so papules, vesicles, pustules and crusts coexist, and this polymorphic stage is the bedside key to the diagnosis. [2] [1]
The individual lesion evolves quickly. A small red papule becomes a superficial, thin-walled vesicle on an erythematous base — described classically as a dewdrop on a rose petal — then umbilicates, becomes a pustule, and crusts over. The lesions are intensely itchy, and scratching drives the most common complication, secondary bacterial skin infection. Fever is usually modest, and the child is often surprisingly well between crops, though the itch and the sleep disruption are considerable. [1] [2]
The high-risk presentations are the ones that must not be missed. An immunocompromised child may have a visceral, disseminated or haemorrhagic illness with few skin lesions but pneumonia, hepatitis or encephalitis. A neonate whose mother developed varicella from five days before to two days after delivery can develop severe disseminated neonatal varicella. And an adolescent or adult — including a pregnant adolescent — carries a higher risk of varicella pneumonia, which may present with cough, dyspnoea, tachypnoea and hypoxia alongside the rash. [1] [11]
Herpes zoster in a child is less common than in an adult but does occur, especially in immunocompromised children or those who had primary varicella in infancy. It presents as a unilateral, painful, dermatomal vesicular rash that stops at the midline, often preceded by tingling or burning. A child presenting with a dermatomal rash and pain has zoster until proven otherwise, and immunocompromised children with zoster need assessment for dissemination and antiviral therapy. [5] [1]
The complications are part of the presentation because they often bring the child to care. Varicella pneumonia presents with respiratory distress and hypoxia. Secondary bacterial skin infection, cellulitis or necrotising fasciitis from group A streptococcus presents with a spreading, red, hot, painful lesion and high fever. Acute cerebellar ataxia — the classic VZV neurological complication in children — presents with truncal ataxia and a normal mental state days to weeks after the rash. Encephalitis presents with altered consciousness, seizure or focal signs. A deterioration in any of these directions changes the management and the disposition. [2] [1]
Differential Diagnosis
For the child with a generalised vesicular rash, the differential turns on the stage and distribution of the lesions and the clinical context. Enteroviral rashes, especially hand-foot-and-mouth disease, produce vesicles but on the hands, feet and mouth rather than the trunk. Impetigo produces honey-coloured crusts rather than vesicles in crops. Scabies causes intense itch but with burrows in the finger webs and flexures rather than a generalised vesicular crop. Insect bites and papular urticaria are itchy papules without the vesicular progression. [1] [2]
The serious mimics must be considered and excluded. Eczema herpeticum — disseminated herpes simplex in broken skin — produces monomorphic punched-out erosions rather than crops of all stages, and it needs urgent systemic aciclovir. Molluscum contagiosum produces firm, umbilicated papules, not vesicles. Smallpox, though eradicated, is the historical differential whose uniform-stage lesions contrast with varicella's polymorphic stages, and it is occasionally invoked in bioterrorism teaching. Vaccinia from smallpox vaccination can also mimic. [2] [1]
For the child with a dermatomal rash, the differential of herpes zoster includes contact dermatitis, which is itchy rather than painful and follows a linear exposure pattern, and a bacterial cellulitis, which is red, hot and spreading rather than vesicular. A single-dermatome vesicular rash preceded by pain is zoster until proven otherwise, and in an otherwise healthy child with zoster the question becomes whether there is an underlying immune deficit or a recent varicella in infancy that explains the early reactivation. [5] [1]
For the pregnant adolescent with a varicella contact or rash, the differential also includes the question of immunity. A history of definite prior varicella, or documented vaccination, makes susceptibility unlikely. In the absence of either, serology to determine immune status guides both reassurance and the need for post-exposure prophylaxis. The fetus is at risk of congenital varicella syndrome from primary maternal infection in the first half of pregnancy, and the neonate is at risk from peripartum maternal infection. [11] [1]
Clinical & Bedside Assessment
The assessment begins with a focused history built around the rash and the host. Ask about the onset and evolution of the rash, the presence of successive crops, fever, itch and systemic symptoms. Ask specifically about respiratory, neurological and bleeding symptoms, because cough, breathlessness, ataxia, altered consciousness or a haemorrhagic rash signal a complication that changes the disposition. And ask about the immune status — chemotherapy, corticosteroids, transplantation, primary immunodeficiency — because this is the single most important risk modifier. [1] [2]
Establish the vaccination and contact history precisely. Record the number of varicella vaccine doses and dates, and ask about household, school or childcare contacts with varicella or zoster, and the timing of exposure. For a pregnant or peripartum mother, pin down the date of maternal rash onset relative to delivery, because the peripartum window — five days before to two days after delivery — defines the highest neonatal risk. The contact and immune history frames both the clinical likelihood and the public-health response. [2] [11]
Examine for the red flags that change disposition. Assess the rash for the polymorphic stage, the density of lesions, and any area of cellulitis, necrotising fasciitis or haemorrhagic transformation. Examine the respiratory system for pneumonia, the nervous system for ataxia, meningism or depressed consciousness, and the hydration and feeding tolerance. A child with fever persisting beyond the expected course, new respiratory distress, neurological signs, or a spreading skin lesion is a child who needs escalation. [1] [2]
Document the infection-control and public-health essentials at the bedside, because they drive the response. Record the date of rash onset, calculate the contagious period from two days before the rash until all lesions are crusted, and note school or childcare attendance. Identify the high-risk contacts — pregnant women, neonates, immunocompromised individuals, and non-immune siblings — because these are the people for whom post-exposure prophylaxis is most urgent. A careful contact map at the first encounter prevents the late, disorganised public-health scramble. [7] [2]
Investigations
The diagnosis of primary varicella in a typical case is clinical, and no test is needed. The combination of a prodromal fever, a polymorphic generalised vesicular rash in successive crops, and the characteristic lesion progression is sufficiently specific, and a clinician who orders panels of tests on an obvious case has missed the point. Investigations are reserved for atypical presentations, severe or complicated disease, high-risk hosts, and pregnancy, where confirmation changes management. [1] [2]
When confirmation is needed, PCR is the test of choice. Vesicle fluid, a swab of the lesion base, or a nasopharyngeal sample sent for varicella-zoster virus PCR is sensitive and specific and is preferred over culture, which is slow and less sensitive. PCR distinguishes wild-type virus from vaccine-strain virus — relevant in immunocompromised hosts and in suspected vaccine-related rash — and it confirms zoster when the dermatomal rash is atypical. Serology has a more limited role: IgG determines past immunity and susceptibility for a pregnant contact or pre-vaccination, while IgM can support recent infection but is less reliable than PCR for the acute case. [1] [5]
In Australia and Aotearoa New Zealand, varicella is a nationally notifiable disease in most jurisdictions. PCR of vesicle fluid or a lesion swab is the standard confirmatory test for atypical or severe cases and for high-risk hosts. Serology to determine immune status is used for pregnant women and other high-risk contacts after an exposure. The Australian Immunisation Handbook (ATAGI) and the equivalent New Zealand immunisation schedule set the two-dose varicella programme and the post-exposure prophylaxis guidance. [1]
Basic supportive tests follow the clinical picture. A full blood count may show a lymphocytosis but is not diagnostic. A chest X-ray is indicated when pneumonia is suspected, showing a diffuse interstitial or nodular pattern in varicella pneumonia. Liver function tests assess hepatitis in disseminated disease, and a coagulation screen is warranted if haemorrhagic lesions appear. In the immunocompromised or severely ill child, early and aggressive investigation including PCR on blood is appropriate, because the threshold to treat with intravenous aciclovir in these hosts is deliberately low. [1] [6]
Management — Resuscitation
Resuscitation is about the high-risk or deteriorating host: the immunocompromised child, the neonate, the patient with varicella pneumonia, encephalitis or invasive group A streptococcal infection, and the pregnant adolescent. Any of these is a reason to admit, to monitor closely, and to start intravenous aciclovir promptly. The principle is that delaying antiviral therapy in the host who cannot contain the virus is the avoidable error, so the threshold to treat is low. [1] [6]
Start intravenous aciclovir early in the high-risk host. Immunocompromised children with primary varicella, neonates with high-risk maternal timing, and patients with pneumonia, encephalitis or disseminated disease should receive intravenous aciclovir without waiting for PCR confirmation when the clinical picture is compelling. Intravenous rather than oral therapy achieves the tissue levels needed for visceral and CNS disease, and hydration must be maintained to protect against aciclovir-induced nephrotoxicity. [6] [1]
Supportive airway and breathing care is the mainstay in varicella pneumonia. Give supplemental oxygen for hypoxia, manage fluid balance carefully, and escalate to ventilatory support for respiratory failure. In the child with invasive group A streptococcal infection or sepsis complicating a skin lesion, add empiric intravenous antibiotics covering group A streptococcus and Staphylococcus aureus, including a beta-lactam and consideration of clindamycin for toxin suppression. Surgical review is essential for necrotising fasciitis. [1] [2]
Manage the complications directly as they arise. Encephalitis and cerebellitis receive supportive care with anticonvulsants for seizures and attention to airway and intracranial pressure as needed, alongside aciclovir. Secondary bacterial skin infection receives appropriate antibiotics, and the itching that drives scratching and secondary infection is managed with antihistamines, cool compresses and good skin care. Maintain hydration and nutrition, because a febrile child with a painful, itchy rash often feeds poorly. [1] [2]
Management — Definitive & Stepwise
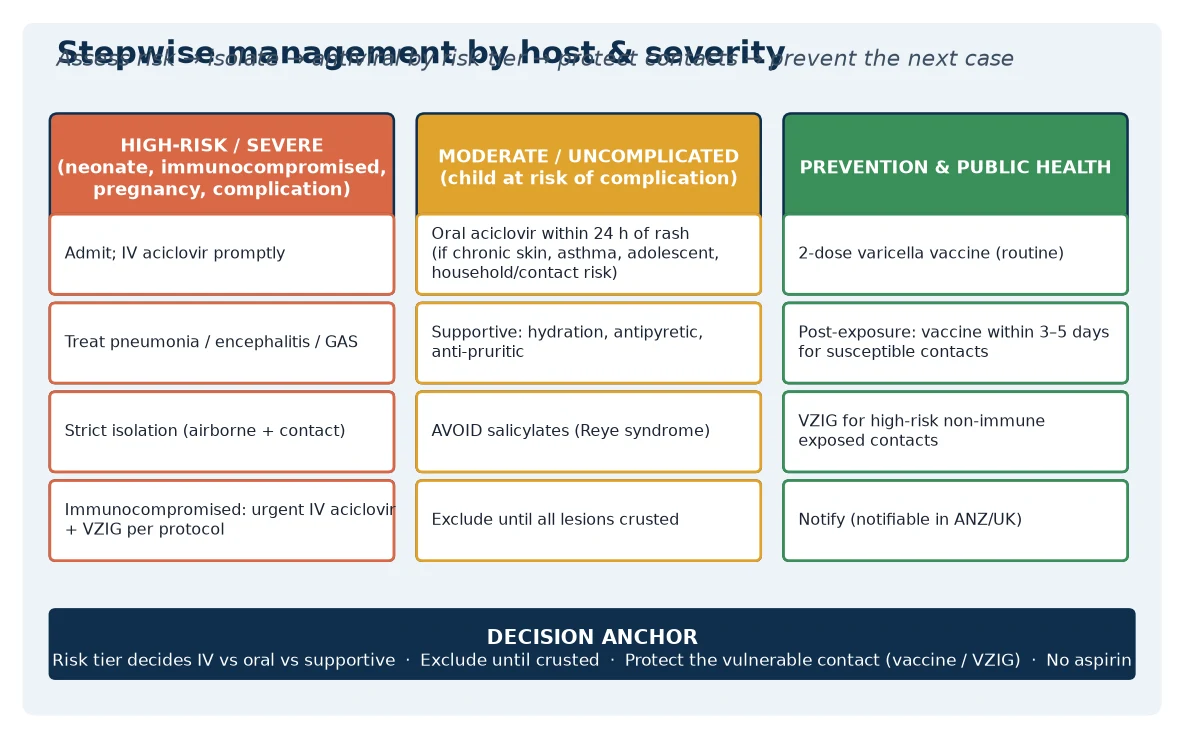
Definitive management is a stepwise pathway matched to the host-risk tier and severity, with supportive care at one end, oral antiviral in the middle, and the public-health layer of isolation, post-exposure prophylaxis and prevention at the other. The healthy child receives supportive care; the child at moderate risk of complication may receive oral aciclovir; and the high-risk host receives intravenous aciclovir. Around the individual, the public-health response protects the contacts and prevents the next case. [1] [7]
The stepwise varicella pathway
Risk-stratify at first contact: healthy child (supportive), at-risk child (consider oral aciclovir), high-risk host (urgent IV aciclovir and admit).
Healthy child: supportive care — antipyretics (paracetamol, NOT aspirin), antihistamines for itch, hydration, skin care; exclude until all lesions crusted.
At-risk child (chronic skin disease, asthma, adolescent, household contact of high-risk person): consider oral aciclovir within 24 hours of rash onset.
High-risk host (immunocompromised, neonate, pregnant, pneumonia, encephalitis, disseminated disease): admit and start IV aciclovir promptly.
Isolate (airborne plus contact precautions in hospital) and exclude from school or childcare until every lesion has crusted.
Notify public health, identify high-risk contacts (pregnant, neonate, immunocompromised, non-immune), and give post-exposure vaccine within 3–5 days or VZIG where vaccine is contraindicated.
For the healthy child, management is supportive. Paracetamol for fever, antihistamines and cool compresses for itch, attention to hydration and skin care, and careful observation for the signs of complication form the core. Aspirin and salicylates must be avoided because of the association with Reye syndrome, and non-steroidal anti-inflammatory drugs are also best avoided in the context of varicella and invasive group A streptococcal risk. Setting the expectation that the child is contagious until every lesion has crusted frames the exclusion and return-to-school advice. [2] [6]
Oral aciclovir has a narrow but defined role. The Cochrane review found that aciclovir shortens the duration of fever and reduces the maximum number of lesions when started within twenty-four hours of rash onset in otherwise healthy children, though the clinical benefit is modest and it does not prevent the rare serious complications. For this reason, routine oral aciclovir for every healthy child is not warranted, but it is reasonable for the child at higher risk of complication — chronic skin disease, chronic lung disease, adolescents, or a household contact who is at high risk. The decision is individualised, not blanket. [6] [1]
Isolation and exclusion form the transmission-control layer. In hospital, use airborne and contact precautions, because the virus spreads by both the airborne and the contact route. Exclude the child from school, childcare and contact with high-risk individuals until every lesion has crusted, which typically takes around five to seven days from the last new lesion. Notify public health according to local requirements, because varicella is notifiable in many jurisdictions, and the notification triggers the contact-tracing and post-exposure prophylaxis response. [7] [2]
Post-exposure prophylaxis protects the vulnerable non-immune contact. The varicella vaccine given within three to five days of exposure can prevent or modify disease in susceptible contacts, and it is the preferred prophylaxis for those in whom the vaccine is not contraindicated. For the high-risk contact in whom the live vaccine is contraindicated — pregnant women, neonates, and immunocompromised individuals — varicella-zoster immune globulin is given to prevent or attenuate severe disease. The aim is always to protect the contact who cannot safely be vaccinated and who cannot safely afford to catch wild-type varicella. [2] [1]
Specific Subtypes & Scenarios
An immunocompromised child with primary varicella. This is the highest-risk presentation. Admit, start intravenous aciclovir promptly, monitor for dissemination to the lungs, liver and brain, and maintain strict isolation. Do not wait for PCR confirmation when the clinical picture is compelling. These children are the ones who die of disseminated disease, and early antiviral therapy is the intervention that changes the outcome. [1] [6]
A neonate exposed to maternal varicella around delivery. When the mother develops varicella from five days before to two days after delivery, the neonate receives little transplacental antibody and a large viral inoculum, and is at risk of severe disseminated neonatal varicella. Give varicella-zoster immune globulin to the neonate, and start intravenous aciclovir if disease develops. Maternal varicella more than a week before delivery allows antibody transfer and is much lower risk. The timing relative to delivery is the decisive fact. [11] [1]
A pregnant adolescent with a varicella contact. Determine immune status first — a reliable history of prior varicella or documented vaccination makes susceptibility unlikely, and serology confirms when the history is uncertain. A non-immune pregnant woman exposed to varicella should receive varicella-zoster immune globulin to prevent or modify maternal disease and its complications, the most serious of which is varicella pneumonia. Primary maternal infection in the first half of pregnancy carries a small risk of congenital varicella syndrome — limb hypoplasia, skin scarring, eye and neurological abnormalities. [11] [1]
An adolescent or adult with varicella pneumonia. This is the severe complication that carries the highest mortality in primary varicella. Admit, give supplemental oxygen, and start intravenous aciclovir. Pregnancy compounds the risk, so a pregnant adolescent with varicella and respiratory symptoms needs urgent assessment and treatment. Varicella pneumonia presents with cough, dyspnoea, tachypnoea and hypoxia, and the chest X-ray shows a diffuse interstitial or nodular pattern out of proportion to the physical findings. [1] [11]
A child with acute cerebellar ataxia after varicella. Acute cerebellar ataxia is the classic VZV neurological complication in children, presenting days to weeks after the rash with truncal ataxia and a normal mental state. It is usually benign and self-limiting, though it warrants assessment to exclude encephalitis. Aciclovir is generally not required for isolated cerebellitis, but the child is assessed for other neurological signs that would broaden the differential and change the management. [2] [1]
A child with a dermatomal rash: herpes zoster. Confirm the diagnosis clinically, assess for dissemination in the immunocompromised, and treat with oral aciclovir if the presentation is severe, disseminated, or ophthalmic. Ophthalmic zoster — reactivation in the ophthalmic division of the trigeminal nerve — threatens vision and needs urgent ophthalmology referral. In an otherwise healthy child with zoster, consider whether there is an underlying immune deficit or a history of early primary varicella that explains the reactivation. [5] [1]
Complications & Pitfalls
Secondary bacterial skin infection is the commonest complication, usually with Staphylococcus aureus or group A streptococcus, and it is driven by scratching. Cellulitis and impetigo are managed with appropriate antibiotics, but the feared progression is invasive group A streptococcal disease — necrotising fasciitis or streptococcal toxic shock — which is a leading cause of varicella-related death. A lesion that becomes red, hot, swollen, exquisitely tender and spreading, with high fever and systemic toxicity, needs urgent surgical and antibiotic management. [2] [1]
Varicella pneumonia is the leading cause of varicella death in adults and a serious complication in adolescents, pregnant women and the immunocompromised. It presents with cough, dyspnoea and hypoxia, sometimes with haemoptysis, and it may progress rapidly. Early intravenous aciclovir and respiratory support are the cornerstones, and pregnancy is a specific high-risk context in which the threshold to treat aggressively is lowest. Recognising pneumonia early and treating it genuinely changes the outcome of severe varicella. [1] [11]
The central neurological complications are acute cerebellar ataxia, encephalitis and, rarely, transverse myelitis or Reye syndrome. Cerebellar ataxia is benign and common; encephalitis is rare but serious and presents with altered consciousness, seizure or focal deficit. Reye syndrome is now rare and is prevented by avoiding aspirin and salicylates in children with varicella — a point an examiner rewards. The diagnostic pitfall is attributing a depressed conscious state to fever or to the prodrome rather than to encephalitis. [2] [1]
The biggest management pitfall is treating the high-risk host as if they were a healthy child. The immunocompromised child, the neonate and the pregnant adolescent with primary varicella need intravenous aciclovir, admission and close monitoring, and a clinician who applies the supportive-care default to these hosts will miss the window in which antiviral therapy changes the course. Risk-tier thinking at the first encounter is the safeguard against this error. [1] [6]
A second pitfall is giving aspirin. Aspirin and salicylates are contraindicated in children with varicella because of the association with Reye syndrome, the rare but devastating hepatocerebral syndrome. Paracetamol is the safe antipyretic, and the avoidance of aspirin is an absolute, not a preference. Educating families and prescribers about this prevents an avoidable catastrophe. [2] [1]
A third pitfall is forgetting the public-health layer. Failing to isolate, exclude, notify, or protect the non-immune high-risk contact allows ongoing transmission to the people for whom varicella is most dangerous — the pregnant colleague, the immunocompromised classmate, the newborn at home. The clinical encounter does not end when the child is treated; it ends when the contacts have been protected and the exclusion has been communicated. [7] [2]
The final pitfall is vaccine complacency. A vaccinated child can still develop breakthrough varicella, which is milder but contagious, so a suggestive rash in a vaccinated child still warrants assessment, exclusion when appropriate, and contact tracing. Dismissing a rash because "the child is vaccinated" closes the door on diagnosis and on the public-health response at the point it is most needed. [9] [7]
Prognosis & Disposition
Most healthy children recover fully within seven to ten days, with the crusts falling off over the following one to two weeks and leaving, at most, small scars where lesions were scratched. The morbidity in this group is driven by itch, sleep disruption, missed school and the occasional secondary skin infection, and the disposition is usually home management with supportive care and clear safety-netting. [1] [2]
The severe morbidity and the mortality are concentrated in the high-risk hosts. Immunocompromised children, neonates with high-risk maternal timing, pregnant adolescents — especially with pneumonia — and patients with invasive group A streptococcal disease carry the burden of severe and fatal varicella. This concentration of harm is the single most important prognostic fact, and it is why every management strategy and every prevention effort ultimately aims to protect these groups. [1] [11]
Disposition follows the risk tier and severity. Admit to a monitored bed or the paediatric intensive care unit the high-risk host with disseminated disease, pneumonia, encephalitis or sepsis. Admit to the ward the child with significant complication or social concern needing observation and intravenous therapy. Manage at home, with isolation and follow-up, the healthy child with uncomplicated disease. The threshold for admitting a high-risk or deteriorating host is deliberately low. [6] [1]
At discharge, complete the isolation and exclusion until every lesion has crusted, finish the contact tracing and post-exposure prophylaxis, and give the family a clear safety-net for return — fever persisting beyond the expected course, respiratory distress, neurological signs, a spreading or painful skin lesion, or bleeding. Reinforce the immunisation schedule, both for the child and for the household, because the discharge encounter is also a prevention opportunity. [2] [7]
Reinfection is uncommon, and second attacks of varicella, when they occur, are usually milder. The long-term consequence of primary infection is the establishment of latency that may reactivate as zoster decades later, which is the biological bridge between this childhood encounter and the adult disease. The recombinant zoster vaccine, given to older and immunocompromised adults, is the prevention tool that addresses that downstream risk. [5] [10]
Special Populations
Immunocompromised children are the highest-risk group for disseminated, fulminant varicella, and the threshold to investigate, admit and treat with intravenous aciclovir is lowest in these patients. They depend on the immunity of the people around them, because the live varicella vaccine may be contraindicated in severe immunodeficiency, so household vaccination and rigorous post-exposure prophylaxis with varicella-zoster immune globulin after exposure are essential. [1] [6]
Neonates are at risk when maternal varicella occurs in the peripartum window from five days before to two days after delivery, because the neonate receives a large viral inoculum without protective maternal antibody. These neonates receive varicella-zoster immune globulin and, if disease develops, intravenous aciclovir. Congenital varicella syndrome, by contrast, follows maternal primary infection in the first half of pregnancy and produces limb hypoplasia, skin scarring, and eye and neurological abnormalities. [11] [1]
Pregnant adolescents with primary varicella face two risks: their own risk of varicella pneumonia, which is more severe in pregnancy, and the fetal risk of congenital varicella syndrome in early pregnancy. Determine immune status after an exposure, give varicella-zoster immune globulin to the non-immune exposed pregnant woman, and treat maternal disease with intravenous aciclovir when indicated. The live varicella vaccine is contraindicated in pregnancy, so prevention rests on pre-pregnancy vaccination. [11] [1]
Unvaccinated or under-vaccinated children and communities carry higher incidence and severity, and they are the substrate for outbreaks. Address vaccine hesitancy respectfully, offer catch-up vaccination at every opportunity, and recognise that under-immunised pockets are where the disease circulates. The two-dose schedule is the durable protection, and verifying and completing immunisation is part of every paediatric encounter. [7] [3]
Aboriginal and Torres Strait Islander, Maori and other Indigenous children, and refugee, asylum-seeking and migrant families may face barriers to timely immunisation and care, including incomplete records and missed opportunities. Ensure culturally safe, equitable access to vaccination, treat actively when disease is suspected, and use trained interpreters rather than family members. Disadvantage should never be the reason a varicella diagnosis is delayed or a child is left unvaccinated. [1] [7]
Rural and remote children need timely access to diagnosis, treatment and public-health follow-up, often through outreach and telehealth, because distance can delay the care that a sick or high-risk child cannot afford to wait for. The plan for a remote family accounts for what is locally available, and retrieval is mobilised early when a high-risk host deteriorates. [7] [1]
Evidence, Guidelines & Regional Differences
The global standard for varicella vaccination is the WHO position paper, which recommends two doses of varicella vaccine for all children and supports its inclusion in national immunisation programmes. It frames varicella as a vaccine-preventable disease whose burden — severe disease in high-risk hosts and the population morbidity of uncomplicated disease — justifies routine childhood vaccination, and it sets the schedule against which national programmes are compared. [1] [7]
The vaccine effectiveness evidence is robust. The Vazquez et al. New England Journal study found the varicella vaccine highly effective in clinical practice, and the Kuter et al. ten-year follow-up documented durable protection after one and two doses, with the two-dose schedule giving superior protection. The move to a two-dose schedule in the United States followed surveillance showing residual breakthrough disease after one dose, and the two-dose programme further reduced incidence, severity and hospitalisation. [3] [4]
Varicella vaccine effectiveness in clinical practice
Population: Case-control study of healthy children in a community paediatric practice, comparing varicella vaccination history between children with a documented diagnosis of varicella and matched controls without varicella.
Key finding
The varicella vaccine was effective in preventing varicella, with effectiveness increasing and breakthrough disease decreasing among those who had received two doses compared with one dose. Vaccine failure, when it occurred, produced milder disease.
Practice change
Two doses of varicella vaccine provide strong, durable protection; breakthrough disease, when it occurs, is milder. This evidence underpins the two-dose schedule and reassures clinicians and families about vaccinated children who develop a mild rash.
The antiviral evidence is set out in the Cochrane review of aciclovir for varicella in otherwise healthy children. The review found that aciclovir started within twenty-four hours of rash onset modestly shortened fever duration and reduced the maximum number of lesions, but the clinical benefit was small and there was no evidence it prevented serious complications. This is why routine aciclovir is not recommended for every healthy child, while it retains a role for the child at higher risk of complication and the high-risk host who needs intravenous therapy. [6] [1]
The epidemiological impact of the vaccine programme is documented in the US surveillance studies. The Marin et al. review traced the successes and challenges of varicella prevention in the United States, and the Chaves et al. studies showed the decline in infant varicella after vaccine implementation and the clinical and epidemiological characteristics of breakthrough disease among vaccinated persons. Together they describe a programme that transformed the epidemiology of the disease where coverage is high. [7] [8]
For herpes zoster, the Harpaz et al. ACIP recommendations framed the original zoster prevention strategy, and the more recent adjuvanted recombinant zoster vaccine has demonstrated high efficacy in preventing zoster and post-herpetic neuralgia in older and immunocompromised adults. The recombinant vaccine represents a major advance over the earlier live zoster vaccine, and its place is in the adult and immunocompromised population rather than in routine childhood practice. [5] [10]
The regional policy structure is consistent in principle and varies in detail. In ANZ, varicella is notifiable, the Australian Immunisation Handbook (ATAGI) and the New Zealand schedule deliver the two-dose varicella programme — usually as measles-mumps-rubella-varicella combination at eighteen months — and public-health units coordinate notification and prophylaxis. In the UK, varicella vaccine is not currently part of the routine childhood schedule, reflecting a different historical risk-benefit calculation, so most UK children acquire natural immunity; the Green Book and UK Health Security Agency guide post-exposure management. In the US, the CDC and AAP deliver the two-dose schedule, the first at twelve to fifteen months and the second at four to six years. In Canada, the Canadian Immunization Guide and provincial programmes deliver the equivalent two-dose strategy. The principle everywhere is that vaccination prevents disease, and post-exposure prophylaxis protects the vulnerable contact. [1] [7]
The controversies are real and active: whether countries without routine varicella vaccination, such as the UK, should adopt it, weighed against the theoretical concern that reduced childhood circulation might shift disease to older, more severe ages; the optimal use of the recombinant zoster vaccine in immunocompromised children; the management of the non-immune pregnant contact; and the inequities in vaccine access that leave some communities unprotected. The defence against each is the same: high coverage, post-exposure prophylaxis for the vulnerable contact, prompt treatment of the high-risk host, and a public-health layer that does not stop at the bedside. [7] [1]
Exam Pearls
- Varicella-zoster virus causes two diseases: primary varicella (chickenpox) on first infection and herpes zoster (shingles) on reactivation from latency in a sensory ganglion. [1]
- The bedside signature is lesions of all stages at once — papules, vesicles, pustules and crusts — from successive crops; the "dewdrop on a rose petal" describes the vesicle. [2]
- Host-risk tier decides management: healthy child = supportive; at-risk child = consider oral aciclovir; immunocompromised, neonate or pregnant = urgent IV aciclovir. [1] [6]
- Diagnose clinically in the typical case; use PCR of vesicle fluid or lesion swab for atypical, severe or high-risk presentations, and serology to determine immune status in pregnant or high-risk contacts. [1]
- The child is contagious from one to two days before the rash until every lesion has crusted; isolate (airborne plus contact) and exclude until crusted. [2]
- Avoid aspirin and salicylates in children with varicella — the Reye syndrome association; use paracetamol for fever. [2]
- Post-exposure: vaccine within three to five days for susceptible contacts; varicella-zoster immune globulin (VZIG) for the high-risk contact in whom the live vaccine is contraindicated — pregnant, neonate, immunocompromised. [1]
- The complications: secondary bacterial skin infection and invasive group A strep (leading cause of death), varicella pneumonia (commonest severe complication in adults/pregnancy), acute cerebellar ataxia (classic VZV CNS sign in children), encephalitis. [2]
- Breakthrough varicella in vaccinated children is milder — fewer lesions, maculopapular, little fever — but still contagious; two-dose vaccination reduces it. [9] [3]
- Prevention is the two-dose live varicella vaccine; the adjuvanted recombinant zoster vaccine (RZV) prevents zoster and post-herpetic neuralgia in older and immunocompromised adults. [7] [10]
- Peripartum maternal varicella (five days before to two days after delivery) risks severe neonatal varicella; give the neonate VZIG and aciclovir if disease develops. [11]
References
- [1]WHO Varicella and herpes zoster vaccines: WHO position paper, June 2014--Recommendations. Vaccine, 2016.PMID 26723191
- [2]Marin M; Guris D; Chaves SS; Schmid S; Seward JF Prevention of varicella: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep, 2007.PMID 17585291
- [3]Vazquez M; LaRussa PS; Gershon AA; Steinberg SP; Freudigman K; Shapiro ED The effectiveness of the varicella vaccine in clinical practice. N Engl J Med, 2001.PMID 11274621
- [4]Kuter BL; Brown AE; Hesley TM; Chalikonda I; et al Ten year follow-up of healthy children who received one or two injections of varicella vaccine. Pediatr Infect Dis J, 2004.PMID 14872179
- [5]Harpaz R; Ortega-Sanchez IR; Seward JF Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep, 2008.PMID 18528318
- [6]Klassen TP; Belseck EM; Wiebe N; Hartling L Acyclovir for treating varicella in otherwise healthy children and adolescents. Cochrane Database Syst Rev, 2005.PMID 16235308
- [7]Marin M; Meissner HC; Seward JF Varicella prevention in the United States: a review of successes and challenges. Pediatrics, 2008.PMID 18762511
- [8]Chaves SS; Lopez AS; Watson TL; Civen R; et al Varicella in infants after implementation of the US varicella vaccination program. Pediatrics, 2011.PMID 22123875
- [9]Chaves SS; Gargiullo P; Zhang JX; Civen R; et al Varicella disease among vaccinated persons: clinical and epidemiological characteristics. J Infect Dis, 2008.PMID 18419385
- [10]Willer DO; Oostvogels L; de la Torre F; Collins M; et al Efficacy of the adjuvanted recombinant zoster vaccine (RZV) by sex, geographic region, and geographic ancestry/ethnicity: A post-hoc analysis of the ZOE-50 and ZOE-70 randomized trials. Vaccine, 2019.PMID 31537443
- [11]Enders G; Miller E; Cradock-Watson J; Bolley I; Ridehalgh M Consequences of varicella and herpes zoster in pregnancy: prospective study of 1739 cases. Lancet, 1994.PMID 7802767