Paeds · infectious-diseases
Viral upper respiratory tract infection and the common cold
Also known as Common cold · Viral upper respiratory tract infection (URTI) · Acute viral rhinitis · Acute nasopharyngitis · Viral rhinosinusitis · Coryza · Head cold · Acute viral sore throat with coryza
Fellowship guide to viral upper respiratory tract infection and the common cold in children. Covers the viral aetiology and seasonal patterns, the pathophysiology of acute mucosal inflammation, the typical seven-to-ten-day course and why cough lingers, the bedside assessment for red flags and complications, the evidence against antibiotics and the safety of over-the-counter cough and cold preparations, the symptomatic care that does work (analgesia, honey, saline), and the regional guideline differences for antimicrobial stewardship and school exclusion.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
The common cold is an acute, self-limiting viral inflammation of the mucosa of the upper respiratory tract — the nose, nasopharynx and throat — that produces the familiar cluster of nasal congestion, rhinorrhoea, sneezing, sore throat and cough. Most episodes resolve within seven to ten days, though a cough often lingers for two to three weeks as the airway recovers its normal reactivity. [1]
It is the most frequent illness in humans. A normal preschool child has six to eight colds each year, and a child in daycare or with older siblings may have up to ten or twelve, because so many different viruses circulate and immunity to one does not protect against another. Adults, by contrast, average only two to four colds a year. The sheer frequency is what makes the cold a core general-paediatrics topic: it is the everyday presentation behind most fever, cough and "is this serious?" consultations. [1] [2]
The fellowship trap is treating the cold as trivial. Most are, but the same viruses cause bronchiolitis, croup, pneumonia and acute otitis media, and a child who starts with a cold can deteriorate. The paediatrician's job is to recognise the self-limiting majority, give effective symptom relief, avoid antibiotics and unsafe over-the-counter drugs, and pick up the minority who need escalation. [1] [15]
Classification
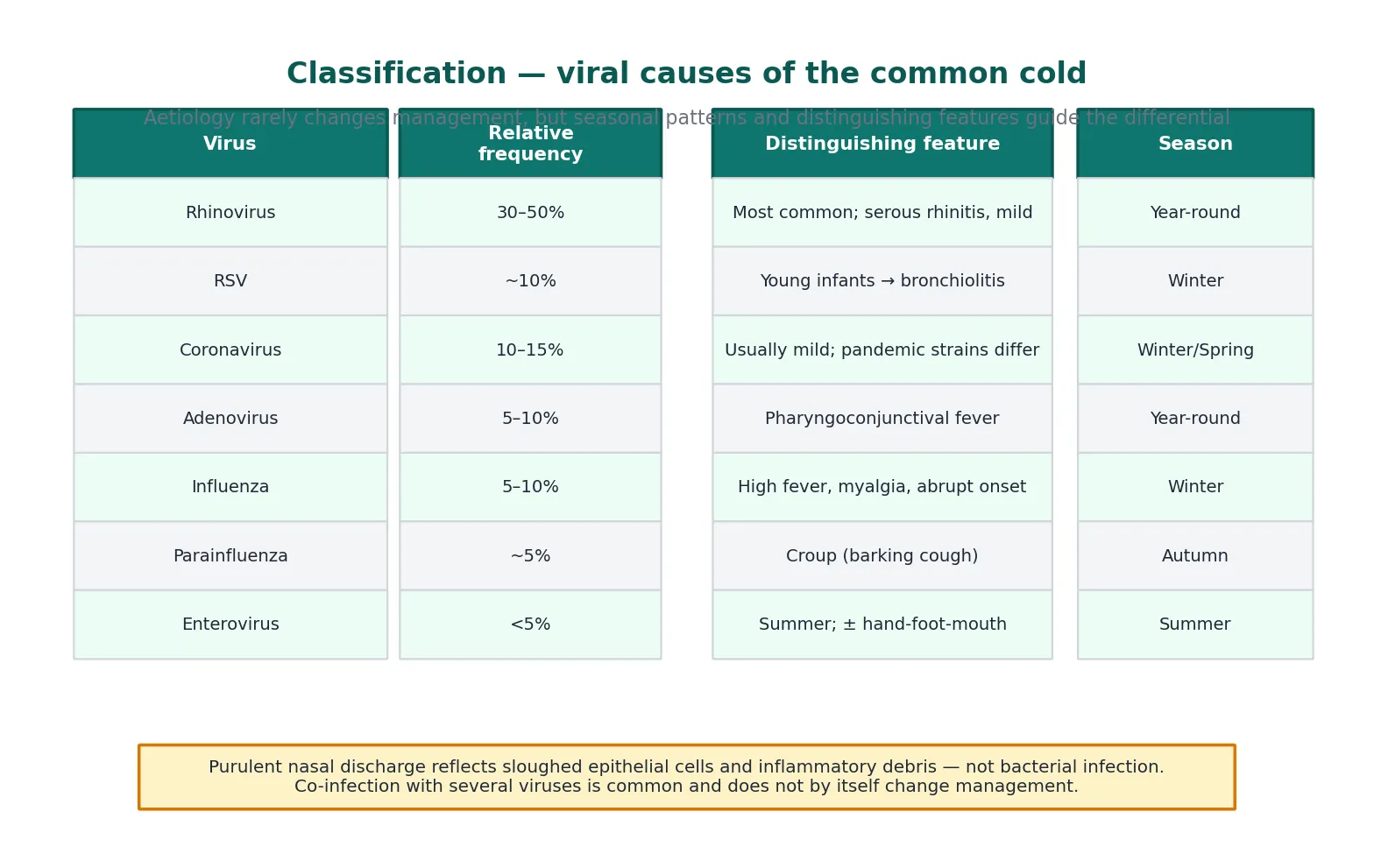
A cold is one clinical syndrome produced by many viruses, so classification matters less for treatment than for epidemiology and the differential. Knowing which viruses circulate in which season helps you anticipate complications — RSV in a winter infant points toward bronchiolitis, parainfluenza in autumn toward croup — and reminds you that co-infection with two or more viruses is common and does not by itself worsen the outlook. [1]
Rhinovirus is the dominant cause, accounting for roughly 30 to 50 per cent of colds, and it circulates year-round with peaks in autumn and spring. Respiratory syncytial virus (RSV), coronaviruses, adenoviruses, influenza and parainfluenza viruses, enteroviruses, human metapneumovirus and human bocavirus make up most of the remainder. Each tends to favour a season and an age group, which is why cold epidemiology shifts through the year in a busy clinic. [1] [2]
The more useful clinical classification separates the uncomplicated cold from the cold complicated by a bacterial or lower-airway extension — acute otitis media, sinusitis, pneumonia, croup or bronchiolitis. This complication-aware framing is what drives your examination and your safety-net, because the cold itself needs no treatment but its complications do. [15]
Epidemiology & Risk Factors
Children carry the burden of colds because they are immunologically naive and physically close to each other. A typical child has six to eight colds per year in the first decade of life, with the highest counts in children attending daycare or preschool and in those with school-age siblings. Frequency falls with age as immunity accrues, dropping to the adult rate of two to four episodes per year. [1] [2]
Transmission is efficient and multimodal. Viruses spread through large respiratory droplets from coughing and sneezing, through direct hand-to-hand or hand-to-surface contact, and via fomites, because rhinovirus survives for hours on skin and surfaces. The incubation period is short — one to three days for rhinovirus — which is why colds sweep through classrooms and households so quickly. Children shed virus for days before and after symptoms, so exclusion is only partially effective. [1]
[1] [2]Recognised risk factors for more frequent or more severe colds include daycare attendance, passive smoke exposure, household crowding, and having older siblings. In children with chronic lung disease, asthma, cystic fibrosis, immunocompromise or congenital heart disease, the same virus that causes a trivial cold in a healthy child can trigger a serious lower-respiratory exacerbation. These groups justify a lower threshold for review. [1]
Pathophysiology
A cold begins when a virus lands on the nasopharyngeal mucosa and binds to receptors on ciliated epithelial cells, most famously the intercellular adhesion molecule-1 (ICAM-1) used by the major rhinovirus receptor group. The virus enters, replicates, and the infected cells release inflammatory mediators — bradykinin, cytokines such as interleukin-6 and interleukin-8, and histamine — that drive the symptoms rather than the virus itself. [1]
These mediators increase vascular permeability and glandular secretion, so the nasal mucosa swells and produces copious mucus. Patients experience the swelling as congestion and the mucus as rhinorrhoea and post-nasal drip. The increased blood flow and nerve stimulation produce the scratchy sore throat and sneezing. Viral clearance over seven to ten days relies on innate defences and the cell-mediated immune response, and the cough that lingers beyond the cold reflects persistent vagal afferent sensitivity in the recovering airway. [1]
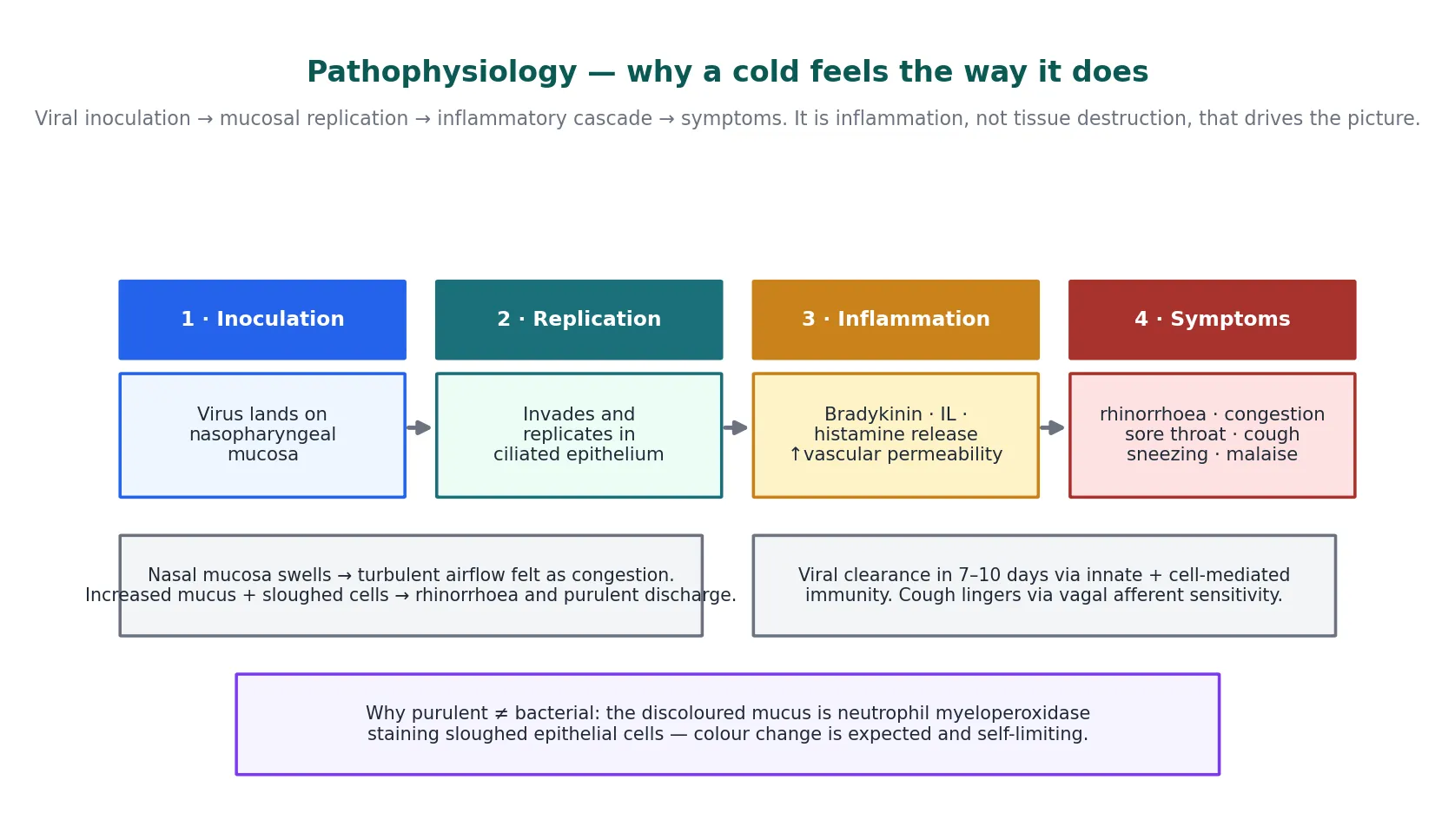
The mechanism explains the single most misunderstood feature of a cold: the discoloured nasal discharge. As neutrophils migrate into the mucus, their myeloperoxidase stains the sloughed epithelial cells and inflammatory debris green or yellow. A change from clear to purulent discharge is an expected part of the natural history and does not indicate bacterial infection or warrant an antibiotic. [5]
Clinical Presentation
The textbook cold unfolds over a week. Nasal congestion, clear rhinorrhoea and sneezing usually begin first, joined within a day by a scratchy or sore throat and a dry cough. Symptoms peak on days two to three and then ease. Young children often run a low-grade fever in the first one to two days — sometimes higher in infants — and are mildly irritable with reduced appetite. [1] [2]
Cough is common and often the symptom that brings the family in. It tends to persist after the nasal symptoms settle, and a post-viral cough lasting two to three weeks is normal; it does not signal a new infection. In an internet-based symptom surveillance study of children with colds, the median symptom duration fell within the expected seven-to-ten-day window, and a minority had cough persisting well beyond it. [2]
The child with an uncomplicated cold looks well between febrile episodes, plays, drinks, and has a normal or mildly raised respiratory rate. On examination the nasal mucosa is inflamed, there may be mild pharyngeal erythema, and cervical lymph nodes are often small and tender. The chest is clear or has only an upper-airway transmitted sound. This "well child with a snotty nose" picture is what reassures you. [1] [3]
What changes the picture is a complication. Tugging at an ear or new fever suggests acute otitis media; increased work of breathing or wheeze points to bronchiolitis or virus-induced wheeze; a barking cough and stridor signal croup; and tachypnoea, recession or grunting raises pneumonia. The history and a focused examination separate the cold from its complications, and this is the heart of bedside assessment. [15]
Differential Diagnosis
The cold sits at the centre of a broad differential because nasal symptoms, sore throat and cough are common to many childhood illnesses. The task is not to prove the cold — it is the default — but to exclude the mimics and the extensions that change management. Allergic rhinitis comes first: it causes chronic or recurrent clear rhinorrhoea, sneezing and nasal itch, often with a personal or family atopy history, and it lacks the fever and the seven-day arc. [1]
Infectious mimics matter more. Influenza presents with abrupt high fever, myalgia and malaise out of proportion to the nasal symptoms; pharyngeal group A streptococcus causes fever and an exudative tonsillitis without coryza; and the prodrome of measles, with coryza, cough and conjunctivitis, precedes the rash by days. Pertussis is the cough that persists and paroxysms. A unilateral, foul-smelling or blood-stained nasal discharge in a preschool child is a nasal foreign body until proven otherwise. [1] [15]
[1] [15]The final branch of the differential is the complication — acute otitis media, sinusitis, pneumonia, croup and bronchiolitis. These are not so much separate diagnoses as the cold's lower-airway or bacterial extensions, and they announce themselves through the red flags assessed in the next section. [15]
Clinical & Bedside Assessment
Bedside assessment of a cold is a search for the few children who are not simply snotty. Start with the airway, breathing and circulation and a set of vital signs, because the history of "just a cold" can conceal early respiratory distress. Watch the child undressed: rate, effort and work of breathing tell you more than any single number. [1] [15]
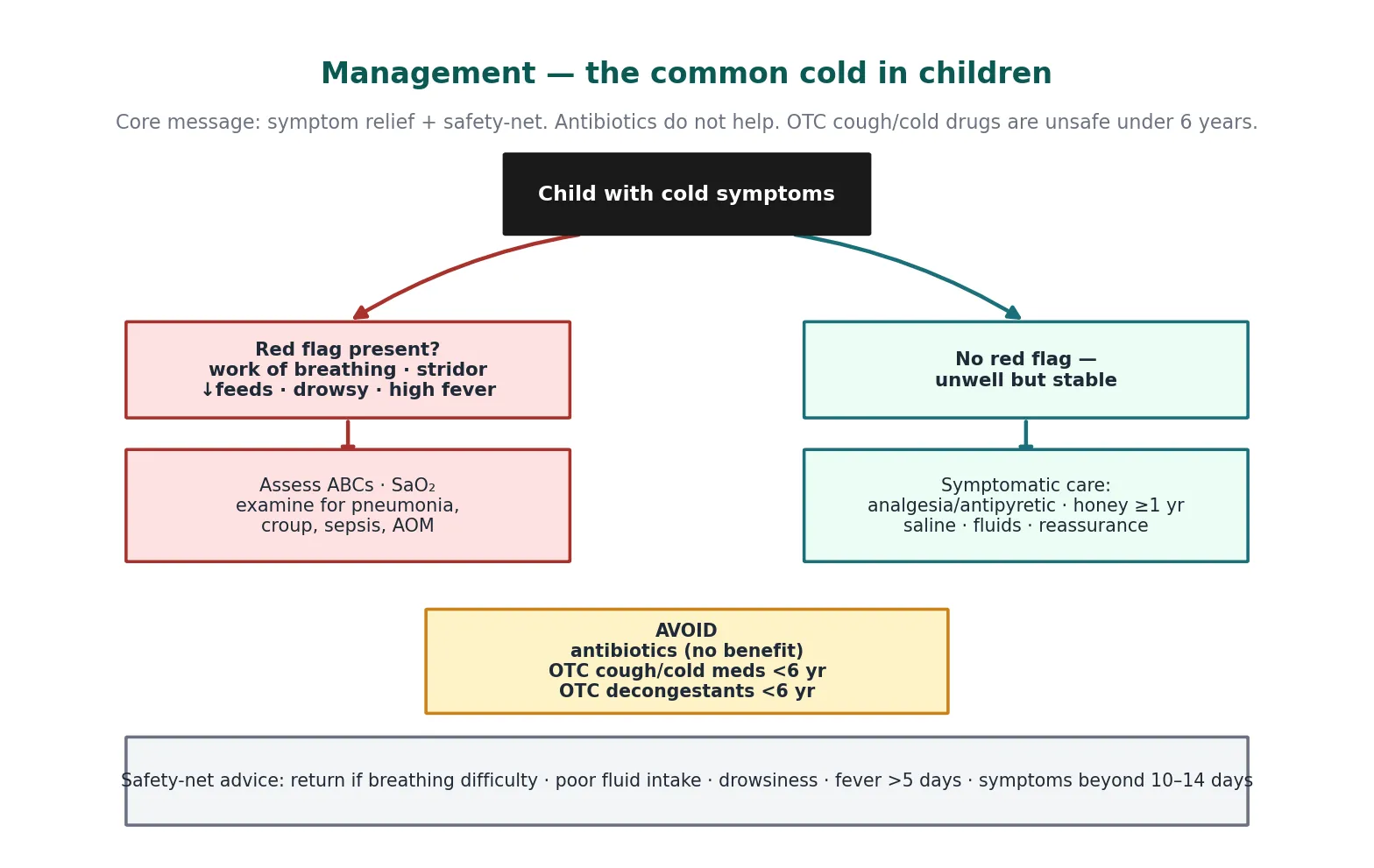
The red-flag examination targets breathing, hydration and the ears. Look for recession, nasal flaring, tracheal tug, grunting and stridor; count the respiratory rate and feel for the effort; and check oxygen saturation if any of these are abnormal. Assess feeding, urine output and capillary refill for dehydration, and always examine the tympanic membranes, because acute otitis media is the commonest complication and is easily missed without pneumatic otoscopy. [15]
When a cold is NOT just a cold — the SAFETY signs
For the well child, a focused examination confirms the diagnosis and reassures the family. Note the inflamed nasal mucosa, assess the throat and ears, palpate the cervical nodes, and listen to the chest to exclude a complication. Document that the child is well, drinking, and has no red flags, because this documentation anchors your safety-net advice. [1]
Investigations
An uncomplicated cold needs no investigation, and ordering tests is itself a source of error: a full blood count adds nothing, and a C-reactive protein cannot separate viral from bacterial illness in the early days. The diagnosis is clinical, and the absence of red flags is sufficient to manage the child symptomatically. [1] [3]
Testing becomes appropriate only when the picture departs from the uncomplicated cold. A respiratory viral polymerase chain reaction panel is justified in the admitted or immunocompromised child, in an infant under three months with fever, or to confirm RSV, influenza or SARS-CoV-2 when the result changes isolation, cohorting or specific therapy. In the child with red flags, blood cultures, urine and a chest radiograph target the suspected complication rather than the cold itself. [1] [15]
The temptation to swab a well child "to prove it is viral" should be resisted. A positive swab confirms a virus but does not exclude a bacterial complication, and a negative swab does not exclude a cold. Reserve testing for the child whose management changes because of the result. [3]
Management — Resuscitation
The cold itself almost never needs resuscitation, because the airway is patent and the child is cardiovascularly stable. The only resuscitation question is whether the cold has become a lower-airway or systemic illness, and that decision belongs to the red-flag assessment above. A child with grunting, severe recession, oxygen saturation below 92 per cent, or signs of shock needs immediate assessment, oxygen, and the septic-workup pathway rather than cold management. [1] [15]
For the overwhelming majority, the "resuscitation" phase is reassurance: confirm the child is well, drinking, and has no red flags, and tell the family what to expect. This first conversation prevents the later antibiotic request, because parents who understand the natural history are far less likely to re-present expecting a prescription. [3] [4]
Management — Definitive & Stepwise
Definitive management of the cold is symptomatic and supportive, and the evidence is clear about what works and what does not. Antibiotics have no place: a Cochrane review found no benefit for antibiotics in the common cold or in acute purulent rhinitis, with no shortening of illness and no prevention of complications, while adding the burden of side effects and resistance. [4] [5]
The agents that do help are modest and safe. Paracetamol at 15 mg per kg per dose every four to six hours (maximum 60 mg per kg per day) or ibuprofen at 10 mg per kg per dose every six to eight hours relieve fever and discomfort. A single 2 to 5 mL dose of honey before bed reduces nocturnal cough in children one year and over. Saline nose drops or spray ease congestion, particularly before feeds in infants. Vapor rub may help nocturnal cough in children over two years when applied to the chest and neck, never the face or nares. [3] [9] [10] [11]
Paracetamol
Dose
15 mg/kg/dose
What to avoid matters as much as what to give. Over-the-counter cough and cold preparations — antitussives, expectorants, decongestants and antihistamine combinations — are not recommended in children under six years and are of unproven benefit in older children. They account for a meaningful number of emergency department visits for unsupervised ingestion and adverse effects, particularly in toddlers. Honey is contraindicated under one year because of the risk of infant botulism. [6] [7] [8]
The popular supplements do not change practice. A Cochrane review found routine vitamin C does not prevent colds in the general population and only modestly shortens duration in those who take it regularly; zinc lozenges have inconsistent benefit and unacceptable taste and nausea in children; and heated, humidified air showed no convincing benefit. None justifies routine recommendation in children. [12] [13] [14]
Specific Subtypes & Scenarios
The infant under three months with fever and coryza. Do not attribute the fever to the cold. An infant under three months with any fever (38°C or above) is at meaningful risk of serious bacterial illness and is investigated on the febrile-infant pathway — blood and urine cultures, and often cerebrospinal fluid — regardless of nasal symptoms. The cold may be the incidental finding, not the explanation. [1] [15]
The cold that triggers wheeze. In the preschool child, the same viruses that cause colds — particularly rhinovirus and RSV — are the commonest trigger of virus-induced wheeze and asthma exacerbations. A child with a cold who develops wheeze and work of breathing is managed for the wheeze (bronchodilator response, oxygen if needed), not for the cold, and a positive response supports a reactive airway. [1]
The cold in the child with chronic disease. In cystic fibrosis, chronic lung disease of prematurity, congenital heart disease, immunocompromise or a tracheostomy, a respiratory virus can precipitate a serious lower-respiratory decline. These children warrant a lower threshold for review, viral testing, and specialist involvement, and their families usually have an action plan to use early. [1]
The recurring "always snotty" child. A child who seems to have a permanent cold may instead have allergic rhinitis, enlarged adenoids, or — with chronic purulent discharge — a nasal foreign body or immune deficiency. Persistence beyond the expected ten to fourteen days, absence of fever, or a clearly atopic pattern should prompt a different line of assessment rather than repeated antibiotic courses. [1]
Complications & Pitfalls
The commonest complication of a cold is acute otitis media, which follows eustachian-tube dysfunction and viral-bacterial interaction in roughly 5 to 30 per cent of young children with a cold. It presents with new ear pain or fever, otoscopic findings of a bulging, opaque tympanic membrane with reduced mobility, and sometimes a spontaneous perforation. The diagnosis requires the bulging membrane, not the cold alone, and the AAP guideline frames expectant observation or antibiotic choice around age, severity and reassurance access. [15]
Other complications extend the inflammation down the airway. Sinusitis presents with persistent purulent nasal discharge and cough beyond ten days without improvement, or with worsening after initial improvement. Pneumonia declares itself through tachypnoea, recession and focal findings; croup through barking cough and stridor; and bronchiolitis through wheeze, crackles and work of breathing in the young infant. Rare but serious bacterial complications include peritonsillar and retropharyngeal abscess. [1] [15]
Cold complications at a glance
The most common pitfall, though, is iatrogenic: prescribing an antibiotic for an uncomplicated cold or for purulent nasal discharge. This exposes the child to side effects such as rash, diarrhoea and candidiasis, selects for resistant organisms, and consumes resources — all for no clinical gain. A close second is recommending an over-the-counter cough and cold preparation in a young child, which risks dosing error, sedation and toxicity. Both errors are avoidable with evidence-based counselling. [4] [6] [7]
Prognosis & Disposition
The prognosis of an uncomplicated cold is excellent: symptoms resolve within seven to ten days, and a post-viral cough settling over two to three weeks is the norm rather than a sign of recurrence. Most children are managed entirely at home, need no follow-up, and return to normal activity once they feel well. The disposition decision rests on the red-flag assessment, not on the diagnosis itself. [1] [2]
School and childcare exclusion balances contagion against practicality. Because children shed virus before and after symptoms and because exclusion does not reliably interrupt spread, the practical rule is to keep a child home while febrile or unwell, and to allow return once they are well enough to participate and have been afebrile for 24 hours without antipyretics. Good hand hygiene and respiratory etiquette are the measures that actually reduce transmission. [1]
What to tell every family before they leave
Tell parents three things. First, the cold will last about a week, and a cough for up to three weeks is normal. Second, antibiotics will not help and may cause side effects, so the plan is paracetamol or ibuprofen for discomfort, honey (over one year) for the cough, saline for the nose, fluids, and rest. Third — and this is the safety-net — return promptly if breathing gets harder, fluids or wet nappies drop, the child becomes drowsy, the fever lasts beyond five days, or things get worse after first improving. [1] [3]
Special Populations
Indigenous and remotely living children. Aboriginal and Torres Strait Islander children and Māori and Pacific children in Aotearoa New Zealand carry a higher burden of respiratory complications, driven by crowding, earlier and denser viral exposure, and barriers to timely care. A cold in these children deserves particular attention to complications, up-to-date immunisation, and timely review, with a low threshold for inhaled bronchodilator assessment and follow-up. [1]
Immunocompromised and technology-dependent children. Children on chemotherapy, post-transplant, or with primary immune deficiency may clear respiratory viruses poorly and progress to lower-respiratory disease. Viral testing, early antiviral therapy where specific agents exist, and a low threshold for admission shape their management, usually in partnership with their specialist team. [1]
Children with asthma, cystic fibrosis and chronic lung disease. In these children the cold is the trigger, not the disease. The priority is the early management of the underlying condition — stepping up asthma therapy, increasing airway clearance in cystic fibrosis — and recognising that a "minor" cold can destabilise a marginal respiratory baseline. Their action plans should specify when to start extra therapy and when to seek review. [1]
Socioeconomically disadvantaged families. Crowding, smoke exposure, and limited access to care all worsen cold frequency and complications, and they make the safety-net conversation harder. A clear, written return plan, attention to immunisation status, and practical advice on fluids and simple symptom relief matter most where resources are tight. [1]
Evidence, Guidelines & Regional Differences
The evidence base for the common cold is dominated by Cochrane reviews that confirm the futility of antibiotics and the limited role of supplements. Antibiotics provide no benefit for the common cold or for acute purulent rhinitis. Honey is more effective than no treatment for acute cough in children. Saline nasal irrigation gives modest benefit. Vitamin C does not prevent colds in the general population, zinc has inconsistent benefit, and heated humidified air shows no convincing effect. [4] [8] [11] [12] [13] [14]
Guidelines converge on the same message across regions. NICE guidance on self-limiting respiratory tract infections (NG190) advises a no-antibiotic strategy with a safety-net for the common cold. The Australian Therapeutic Guidelines reserve antibiotics for documented bacterial complications. Choosing Wisely campaigns in Australia, the United Kingdom and North America all list "no antibiotics for an uncomplicated cold" as a core recommendation. The agreement is the point: regional practice varies far less here than in conditions like sore throat or otitis media. [1] [4]
[1] [4]Where regions do differ is in the practical scaffolding around the no-antibiotic message. The UK formalises the safety-net as a written delayed or back-up prescription strategy. Australia and New Zealand lean on the medical home and on telehealth review for remotely living families. North American guidance, including the AAP, emphasises the risk of over-the-counter preparation harm and the role of vaccination against influenza, SARS-CoV-2 and RSV to reduce the burden and complications of viral respiratory illness. [1] [6] [15]
Exam Pearls
The highest-yield facts for the common cold cluster around stewardship and safety. Antibiotics do not shorten the illness or prevent complications in the common cold, and purulent nasal discharge is not a sign of bacterial infection — it reflects sloughed epithelial cells and neutrophil debris. These two points alone answer a large share of written questions. [1] [4] [5]
Know the age cut-offs cold-cold. Over-the-counter cough and cold preparations are not recommended under six years; honey is contraindicated under one year because of infant botulism; and an infant under three months with fever is investigated for serious bacterial illness regardless of coryza. The expected duration — seven to ten days for most symptoms, two to three weeks for cough — frames the "when to worry" questions. [6] [8] [1]
For viva and clinical encounters, structure your answer around the two questions: is this child unwell enough to escalate, and what is the safety-net? Name the effective symptomatic measures, refuse the antibiotic with a clear rationale, and demonstrate you can spot acute otitis media, bronchiolitis, croup and pneumonia. Examiners reward the candidate who manages the parent as skilfully as the child — the antibiotic conversation is a communication station in disguise. [3] [15]
References
- [1]Heikkinen T, Järvinen A. The common cold. Lancet, 2003.PMID 12517470
- [2]Troullos E, Baird L, Jayawardena S, et al. Common cold symptoms in children: results of an Internet-based surveillance program. Journal of medical Internet research, 2014.PMID 24945090
- [3]Fashner J, Ericson K, Werner S. Treatment of the common cold in children and adults. American family physician, 2012.PMID 22962927
- [4]Kenealy T, Arroll B. Antibiotics for the common cold and acute purulent rhinitis. Cochrane database of systematic reviews, 2013.PMID 23733381
- [5]Arroll B, Kenealy T. Are antibiotics effective for acute purulent rhinitis? Systematic review and meta-analysis of placebo controlled randomised trials. BMJ, 2006.PMID 16861253
- [6]Shefrin AE, Goldman RD. Use of over-the-counter cough and cold medications in children. Canadian family physician Medecin de famille canadien, 2009.PMID 19910592
- [7]Mital R, Lovegrove MC, Schillie SF, et al. US emergency department visits for acute harms from over-the-counter cough and cold medications, 2017-2019. Pharmacoepidemiology and drug safety, 2022.PMID 34757641
- [8]Oduwole O, Udoh EE, Oyo-Ita A, et al. Honey for acute cough in children. Cochrane database of systematic reviews, 2018.PMID 29633783
- [9]Paul IM, Beiler J, McMonagle A, et al. Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Archives of pediatrics & adolescent medicine, 2007.PMID 18056558
- [10]Paul IM, Beiler JS, King TS, et al. Vapor rub, petrolatum, and no treatment for children with nocturnal cough and cold symptoms. Pediatrics, 2010.PMID 21059712
- [11]King D, Mitchell B, Williams CP, et al. Saline nasal irrigation for acute upper respiratory tract infections. Cochrane database of systematic reviews, 2015.PMID 25892369
- [12]Hemilä H, Chalker E. Vitamin C for preventing and treating the common cold. Cochrane database of systematic reviews, 2013.PMID 23440782
- [13]Singh M, Das RR. Zinc for the common cold. Cochrane database of systematic reviews, 2011.PMID 21328251
- [14]Singh M, Singh M. Heated, humidified air for the common cold. Cochrane database of systematic reviews, 2013.PMID 23733382
- [15]Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics, 2013.PMID 23439909