Paeds · investigations-procedures-and-technology
Airway suction, oxygen devices and nebuliser technique
Also known as Paediatric airway suction · Oxygen delivery devices in children · Nebuliser technique in children · High-flow nasal cannula setup · Inhaled bronchodilator delivery
Fellowship guide to three linked bedside skills: clearing a child's airway by suction, choosing and applying the right oxygen delivery device to a target saturation, and setting up a nebuliser so the drug actually reaches the lung. Covers device classification and FiO2, the entrainment principle and aerosol physics, suction technique and complications, the evidence for high-flow nasal cannula, and the choice between a spacer with a metered-dose inhaler and a nebuliser.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A wheezy, struggling infant, a child who has vomited and is unconscious, and a toddler with an asthma attack all need the same three hands-on skills: clear the airway of whatever is blocking it, give the right amount of oxygen to a chosen target, and deliver a drug as a mist that actually reaches the lung. These skills — airway suction, oxygen devices, and nebuliser technique — are bundled as one topic because they are done together, at the bedside, in the first minutes of caring for a sick child, and because the same physics decides whether each of them works.
[2]Each skill rests on a single idea. Suction removes liquid from the airway so gas can flow again. Oxygen therapy adds oxygen, but how much actually reaches the alveolus depends on the device and on how hard the child is breathing. A nebuliser turns a liquid drug into droplets, and the size of those droplets decides whether the drug lands in the mouth or travels down to the small airways where it acts. Get one idea wrong and the whole effort is wasted, which is why these procedures reward understanding over ritual. [6]
Classification
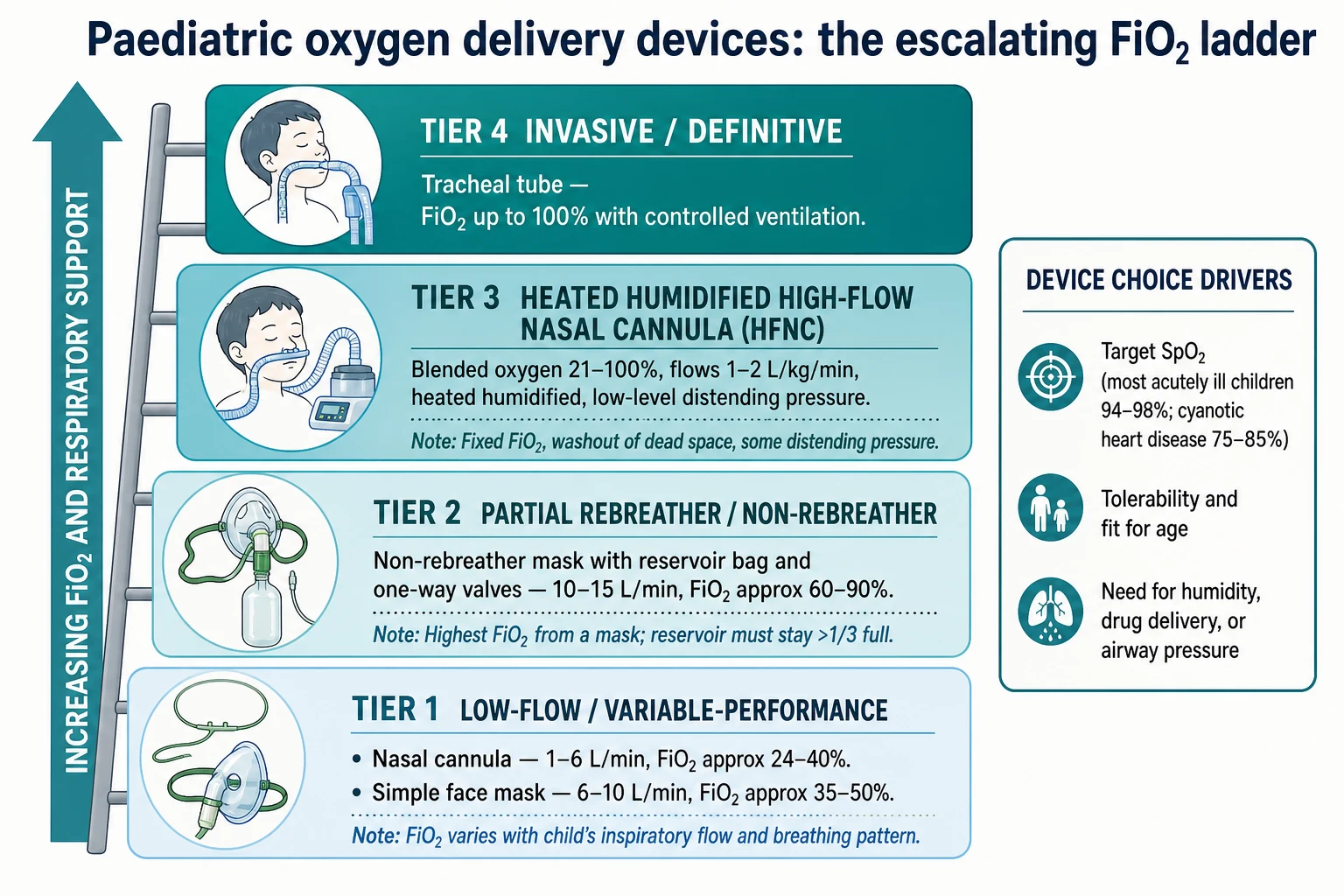
The useful way to classify oxygen devices is by how much oxygen they can reliably deliver, because that decides which device you reach for. A nasal cannula or simple face mask is a variable-performance device: it adds oxygen, but every time the child breathes in, room air is drawn in too and dilutes it, so the actual fraction of inspired oxygen (FiO2) swings up and down with how fast and deep the child breathes. A heated humidified high-flow nasal cannula and a tracheal tube are fixed-performance: they deliver a set FiO2 that does not depend on the child's breathing pattern. [2]
[2]Suction devices sort by where they reach. A rigid Yankauer tip clears the mouth and oropharynx. A soft, flexible catheter reaches the nasopharynx or an artificial airway. Nebulisers sort by how they make the mist: a jet (pneumatic) nebuliser uses a fast gas stream, a vibrating-mesh nebuliser pushes the liquid through a perforated membrane, and an ultrasonic nebuliser uses sound waves — and they do not all deliver the same dose, especially when the child is on respiratory support. [7]
Epidemiology & Risk Factors
Respiratory illness is the commonest reason a child presents acutely, and hypoxaemia from lower airway disease — bronchiolitis, pneumonia, asthma — is the proximate cause of most paediatric arrests, so the demand for these three skills is constant. Infants under one year need the most support because their small airways obstruct within minutes, their oxygen reserve is tiny, and a blocked nose matters more because they are obligate nose-breathers. [2]
Some children need these procedures again and again. Copious secretions come with bronchiolitis, with neuromuscular weakness and cerebral palsy, and with any child who has a tracheostomy. A reduced conscious level loses the cough and gag that normally protect the airway, so vomit and saliva pool and must be suctioned. Syndromic and dysmorphic airways — Down syndrome, Pierre Robin sequence — are harder to manage and oxygenate. The procedures themselves carry risk that clusters around operator error: suction held too long, dry high-flow oxygen run without humidity, and a nebuliser that delivers the wrong dose because the driving flow is slow or the mask leaks. [11]
Indigenous and remote communities carry a higher burden of acute respiratory illness and sit further from tertiary care, which makes a first responder's competence at suction, oxygen and nebuliser therapy genuinely life-saving before retrieval arrives.
[1]Pathophysiology
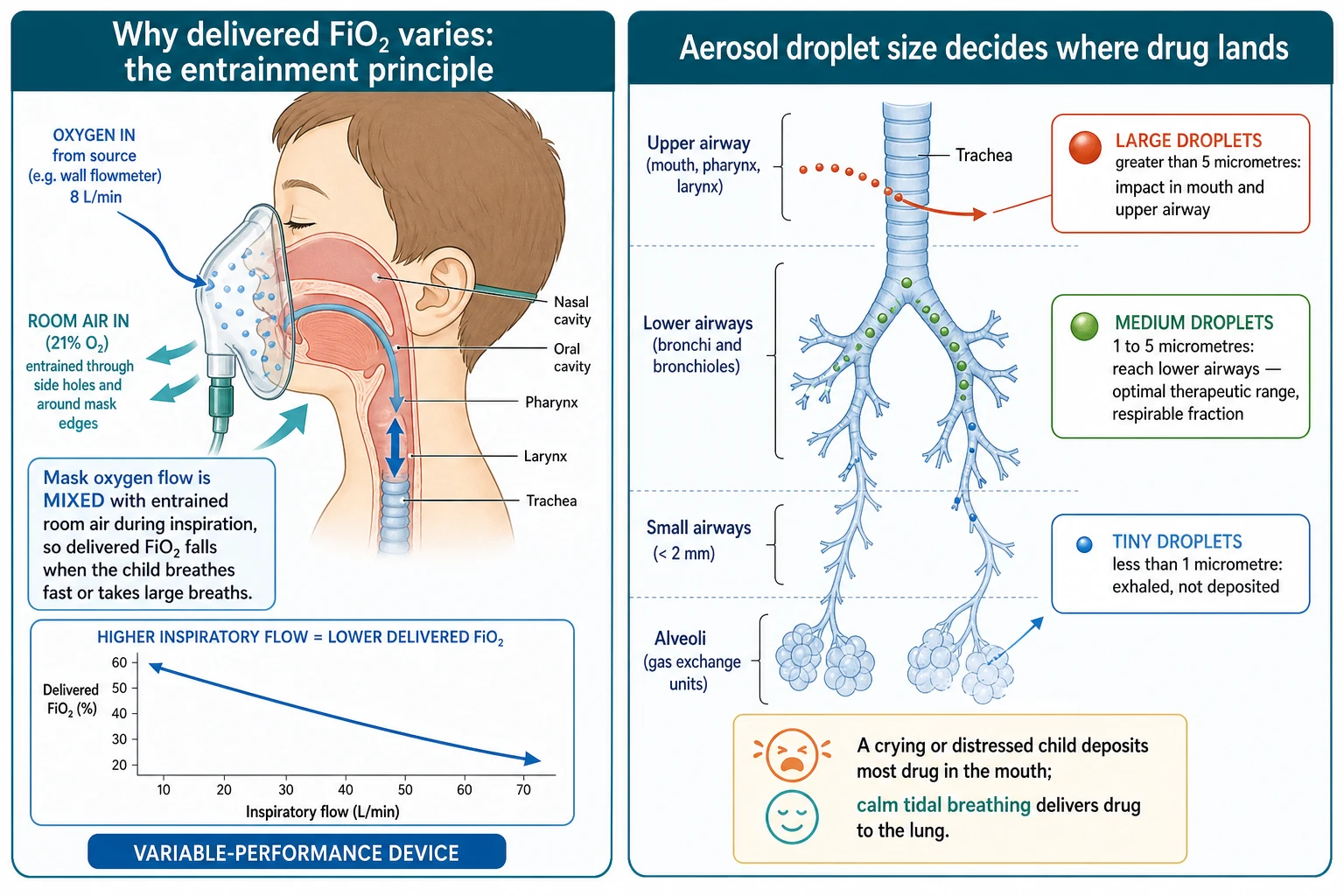
Two pieces of physics explain why these devices behave as they do, and a candidate who holds them can answer almost any question on this topic. The first is the entrainment principle. When a child breathes in through a low-flow mask or nasal cannula, they pull in far more air than the device delivers, so room air (21 percent oxygen) is drawn in through the mask side-holes and around the edges and mixes with the oxygen. The faster and deeper the child breathes, the more room air dilutes the flow, and the lower the real FiO2 at the alveolus. This is the whole reason a nasal cannula is called variable-performance: the quoted FiO2 of 24 to 40 percent is only an estimate that collapses the moment a sick child pants. [2]
The second is aerosol physics. A nebuliser makes droplets, and the size of the droplet (its mass median aerodynamic diameter) decides where it lands. Droplets larger than 5 micrometres are heavy and crash out in the mouth and upper airway. Droplets between 1 and 5 micrometres are light enough to ride the breath down into the lower airways — this is the respirable fraction, the only droplets that do useful work. Droplets smaller than 1 micrometre are so light they drift in and out again and are exhaled. A jet nebuliser's droplet size depends on its driving gas flow: a slow flow makes large, useless droplets, which is why the driving gas must run at 6 to 8 L/min. [6]
Suction earns its place by restoring flow. A child's airway is narrow, and because airway resistance rises steeply as the radius falls, a millimetre of secretion or vomit in a neonate narrows the airway as much as centimetres would in an adult. Removing that liquid reopens the passage so that oxygen and nebulised drug can travel through it. Suction is not an end in itself; it is the act that makes the other two procedures possible. [11]
Clinical Presentation
A child needing one or more of these skills shows it at the bedside, and you read the three needs in turn. The need for suction announces itself audibly: gurgling or rattling breathing, visible vomit, blood or thick secretions in the mouth, or a child too weak to cough and clear the airway. The need for oxygen shows as the familiar signs of hypoxaemia — recession, tracheal tug, nasal flaring, head-bobbing, grunting, agitation or, late and unreliable, cyanosis — with a pulse oximeter reading below the target for age. The need for a nebuliser shows as wheeze, poor air entry, and the increased work of breathing of an asthma attack or bronchiolitis. [8]
The presentation that demands all three at once is the deteriorating infant with bronchiolitis: a nose and pharynx full of secretions, saturations falling, and a chest full of wheeze. Another is the unconscious child who has vomited — liquid in the airway, failing ventilation, and a need for bronchodilator only after the airway and oxygen are sorted. [11]
Watch for the presentations that mislead. The silently hypoxaemic child looks calm while the oxygen runs low, because cyanosis is late and colour lags the failing lung, so judge the child on work of breathing and behaviour, not on colour. The child on home oxygen or a tracheostomy can obstruct behind the very equipment the family manages every day, and the family will know the warning signs before you do. And the child with a cyanotic cardiac lesion lives at a saturation of 75 to 85 percent by design — chasing a "normal" saturation in that child does harm, not good. [8]
Differential Diagnosis
The procedural differential is practical, not pathological, and it runs in three short columns. For suction, decide where the obstruction sits: visible in the mouth (use a Yankauer), in the nasopharynx (use a soft catheter, but never in suspected basilar skull fracture or coagulopathy), or in an artificial airway or tracheostomy (use a sterile, sized catheter). [12]
For oxygen, decide how sick the child is. Mild to moderate hypoxaemia with a normal or only mildly raised work of breathing needs low-flow oxygen, titrated to target. Severe hypoxaemia, or any acutely deteriorating child, needs a non-rebreather mask while you assess. A child with moderate to severe disease who is failing low-flow oxygen is the candidate for high-flow nasal cannula, and the child in refractory respiratory failure needs invasive ventilation. [1]
For a nebuliser, decide what drug you are giving — a bronchodilator (salbutamol, ipratropium), a steroid, hypertonic saline, adrenaline, or an antibiotic — and whether a nebuliser is even the right tool. For most acute asthma, a spacer with a salbutamol metered-dose inhaler is as effective as a nebuliser and works faster, so reach for the nebuliser only when the child cannot use a spacer, needs high-flow oxygen at the same time, or needs a drug that only comes nebulised. [4]
Clinical & Bedside Assessment
Assess before, during and after every procedure, and let the pulse oximeter run throughout. Look, listen and feel at the airway and breathing; grade the work of breathing (recession, tracheal tug, nasal flare); count the respiratory rate; read the SpO2; and judge the child's conscious state and colour. State a target saturation out loud, because oxygen is a drug and a drug without a target is given blindly. [8]
Before suction, pre-oxygenate the child and have the correct catheter ready. A suction catheter should be sized to about half the diameter of the airway lumen, so it can remove liquid without occluding the tube and without causing mucosal trauma. During suction, watch the heart rate and SpO2 on the monitor throughout, because the vagal response is immediate: the moment the heart rate drops, stop and re-oxygenate. [11]
For oxygen, confirm the device and flow against the target, and check the details that decide whether it works. A simple face mask must run at least 5 to 6 L/min so that exhaled carbon dioxide is flushed out rather than rebreathed. A non-rebreather mask needs 10 to 15 L/min and a reservoir bag that stays inflated. For a nebuliser, confirm the drug and dose, that the driving gas is 6 to 8 L/min, that the mask seals and the mist is visible, and that the child is upright and breathing calmly. [6]
Investigations
These are procedural skills, not diagnostic ones, so no investigation precedes clearing an obstructed airway or correcting hypoxaemia. The single essential monitor is the pulse oximeter: confirm a target SpO2 and trend it continuously, but remember that it lags the failing lung and reads the oxygen story only. [8]
When hypoxaemia is severe or the child is tiring, add a blood gas to read the carbon dioxide, because a child who looks more comfortable on oxygen may quietly be retaining carbon dioxide. A chest radiograph, taken once the child is stable, finds the cause — a lobar pneumonia, hyperinflation, a pneumothorax. For a nebulised bronchodilator, the "investigation" is the clinical and physiological response: reduced work of breathing, better air entry, and a rising SpO2, measured against the baseline you recorded before the dose. [4]
One investigation matters for a rare but serious complication of the procedure itself. Deep, blind pharyngeal suction in infants has caused iatrogenic mediastinitis, and a contrast study is what makes that diagnosis after the event — a reminder to suction only what you can see, and never to push a catheter blindly into an infant's pharynx. [12]
Management — Resuscitation
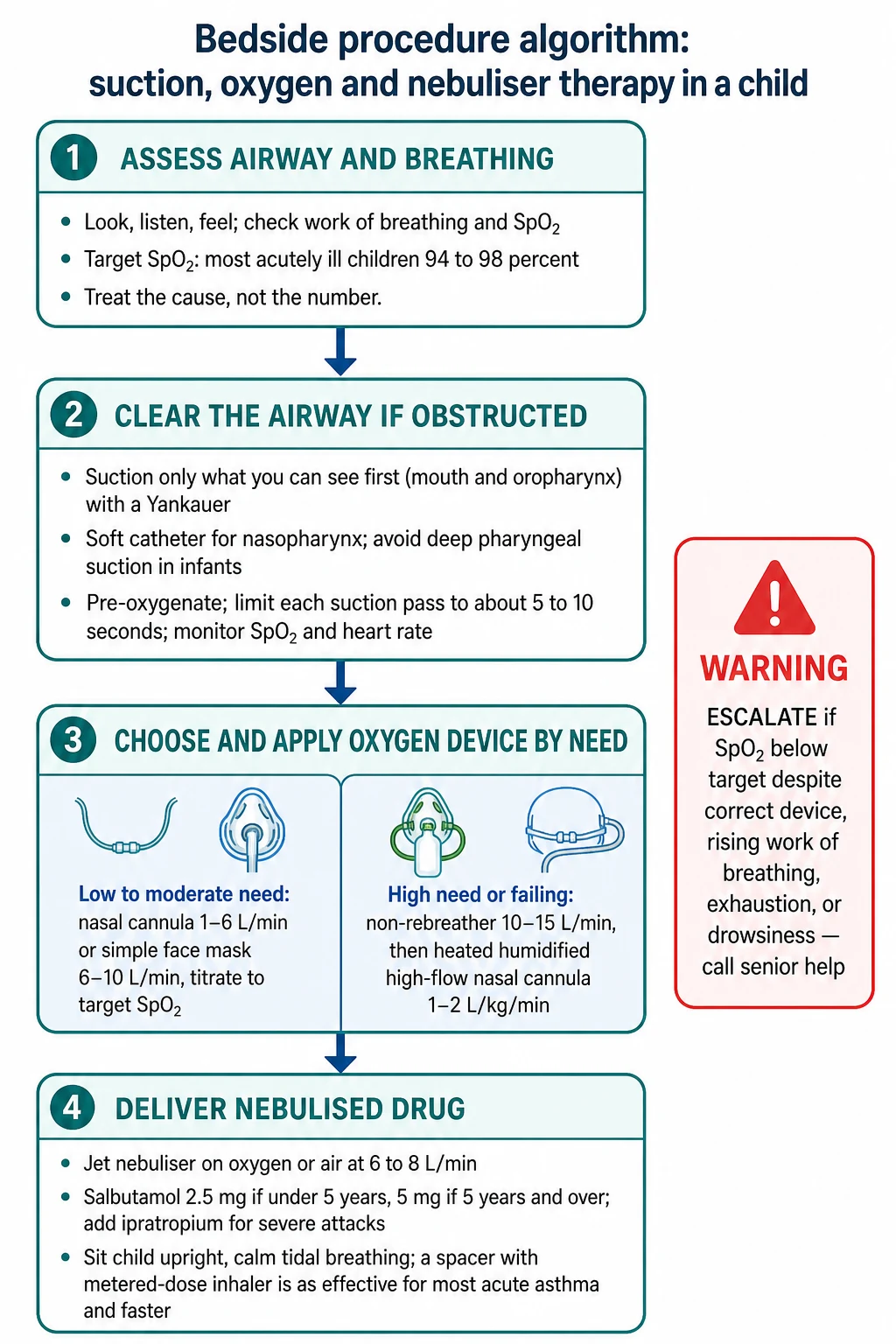
The resuscitation order is airway, then breathing, then drug delivery, done in the first minutes. If the airway is obstructed by liquid, suction what you can see first with a Yankauer, pre-oxygenating before and between passes and limiting each pass to about 5 to 10 seconds while you watch the monitor. Give oxygen by a device matched to severity — nasal cannula or simple mask for mild to moderate hypoxaemia, a non-rebreather for severe — titrated to the target saturation you stated. [11]
Deliver the bronchodilator by the route that works fastest. For most acute asthma that is a spacer with a salbutamol metered-dose inhaler, given one puff at a time into the spacer with the child taking tidal breaths, because it is as effective as a nebuliser and acts faster. Reach for a jet nebuliser when the child cannot use a spacer, needs high-flow oxygen at the same time, or needs a drug that only comes nebulised. [4]
The first-minute respiratory support sequence
Look, listen and feel; check work of breathing, respiratory rate and SpO2
Suction visible liquid from the mouth and oropharynx with a Yankauer, pre-oxygenating and limiting passes
State a target SpO2 and apply oxygen by a device matched to severity
Give salbutamol by spacer-MDI for acute asthma, or by nebuliser if the child needs oxygen or cannot use a spacer
Reassess work of breathing, SpO2 and the child's response
Escalate and call senior help if SpO2 stays below target or work of breathing rises
Call for senior help early — at the point where the saturation will not correct, the work of breathing rises, or the child becomes exhausted or drowsy. The child who is heading for respiratory failure needs intensive care involved while you are still at the bedside, not after a quiet deterioration.
[8]Management — Definitive & Stepwise
Oxygen escalates up a ladder, and you choose the rung by how sick the child is. Begin with low-flow oxygen — a nasal cannula at 1 to 6 L/min or a simple face mask at 6 to 10 L/min — for mild to moderate hypoxaemia, titrated to the target saturation. Step up to a non-rebreather mask at 10 to 15 L/min, with the reservoir kept inflated, for severe hypoxaemia or any acutely deteriorating child. Step up again to heated humidified high-flow nasal cannula at 1 to 2 L/kg/min with blended FiO2 for moderate to severe disease that is failing low-flow oxygen. Step finally to invasive ventilation for refractory respiratory failure. [2]
High-flow nasal cannula is now a well-evidenced rung. The PARIS randomised trial showed that, in infants with bronchiolitis, high-flow nasal cannula reduced the rate of intubation and intensive care admission compared with standard oxygen, and a current review places it squarely between standard oxygen and continuous positive airway pressure. The FIRST-ABC randomised trials then found high-flow nasal cannula non-inferior to CPAP as first-line non-invasive support in paediatric critical care, which is why it has become the default step before intubation for many infants. [1]
Suction has its own ladder. Clear the mouth and oropharynx first with a Yankauer, because what you can see you can remove safely. Then, only if needed, use a soft catheter for the nasopharynx, sized to half the airway lumen and advanced gently without forcing. For a tracheostomy or artificial airway, use a sterile catheter with sterile technique. At every rung, pre-oxygenate before the pass and limit the pass to about 5 to 10 seconds with continuous heart-rate and SpO2 monitoring. [11]
Nebulised therapy for acute asthma follows a drug ladder, and the doses are the facts examiners test. Give salbutamol 2.5 mg nebulised for a child under 5 years and 5 mg for a child of 5 years and over, repeated according to response. For a severe or poorly responding attack add ipratropium 250 microgram nebulised, repeated as needed, because the meta-analytic evidence supports ipratropium on top of salbutamol and systemic steroid for acute asthma. For a life-threatening attack, give salbutamol by continuous nebulisation rather than repeated bolus doses, and move to intravenous bronchodilator with senior intensive care support. Give a systemic corticosteroid early, within the first hour. [5]
Nebulised salbutamol (acute asthma)
Dose
2.5 mg for a child under 5 years; 5 mg for a child 5 years and over, repeated according to response, or given continuously for a severe attack
Two evidence points reshape the way oxygen and drug delivery are calibrated. The Oxy-PICU trial found that, in critically ill children, a conservative oxygen target was as safe as a liberal one and may be safer, which is why the modern practice is to give oxygen to a target and to wean it once the child is stable, rather than to chase a maximal saturation. And the choice of nebuliser device changes the dose a child receives: vibrating-mesh and jet nebulisers deliver drug differently, and the difference widens when the child is on respiratory support, so device choice and driving flow are not trivial details. [8]
Specific Subtypes & Scenarios
The infant with bronchiolitis is the archetype for all three skills, and gentle nasal and oral suction alone often transforms the child, because the obligate nose-breather obstructs behind thick nasal secretions. Add titrated low-flow oxygen, and escalate to high-flow nasal cannula for moderate to severe disease; the evidence for high flow is strongest in this group. [1]
The acute asthma attack is the archetype for nebuliser technique. Begin with a spacer and salbutamol metered-dose inhaler — one puff at a time into the spacer with tidal breathing — for most attacks, because it is as effective as a nebuliser and faster. Move to a nebuliser for the severe attack or the child who needs oxygen at the same time, add ipratropium for severe or poorly responding attacks, give a systemic steroid within the first hour, and use continuous nebulised salbutamol for life-threatening attacks. [5]
The tracheostomy-dependent or technology-dependent child follows their own airway plan, drawn up with the family and the treating team. Use a sterile, appropriately-sized suction catheter, involve the family — who are usually the most expert people at the bedside — and keep the spare tracheostomy tube to hand. The same principles apply: clear, oxygenate, deliver the drug, and escalate. [11]
The neonate and preterm infant need oxygen handled with particular care. Use blended oxygen, set a target saturation defined by the unit (commonly around 91 to 95 percent after the immediate newborn period), and avoid unnecessary high FiO2 because oxygen toxicity causes retinopathy of prematurity and lung injury. Suction gently and only when needed. At altitude, the saturation thresholds for hypoxaemia are lower than at sea level, so apply the altitude-specific definition. [9]
The child with cyanotic congenital heart disease is the one whose saturation you must not "normalise". Their target is 75 to 85 percent by design, and over-oxygenating them can worsen their physiology; set the target to the child's baseline and document it clearly. [8]
Complications & Pitfalls
Suction harms when it is done too hard or too long. Each pass can provoke a vagal bradycardia and a fall in saturation within seconds, which is why you pre-oxygenate, limit each pass to about 5 to 10 seconds, and watch the monitor throughout. A catheter that is too large, or one that is forced, tears the mucosa and bleeds. Deep, blind pharyngeal suction in infants has caused iatrogenic mediastinitis, a serious and avoidable injury that is the reason to suction only what you can see. And non-sterile technique in an artificial airway introduces infection. [12]
Oxygen has its own error set. Under-dosing comes from a low flow or a leaky mask, so the child stays hypoxaemic. A simple face mask run below 5 to 6 L/min lets the child rebreathe exhaled carbon dioxide. Dry, unhumidified high-flow oxygen dries and damages the airway mucosa and thickens secretions, which is why high-flow oxygen must always be heated and humidified. Unnecessary high oxygen causes harm: retinopathy of prematurity in the preterm infant, and now recognised liberal-oxygen injury in critically ill children. Oxygen also feeds fire, a real risk wherever diathermy or a heat source meets a high-flow source. [8]
Nebuliser errors waste the dose or, occasionally, overdose it. A slow driving gas flow makes large droplets that deposit in the mouth, so the drug never reaches the lung. A leaky mask, a near-empty cup, or a crying child each lose the dose. A contaminated device can infect the child. And the largest pitfall of all is failing to recognise that the child is not improving because the drug never arrived — a child who is no better after a nebuliser may simply not have received it, so check the setup before assuming the disease is resistant. [6]
Prognosis & Disposition
When secretions are cleared, hypoxaemia corrected, and bronchodilator delivered promptly, most children recover well, and the outlook is then that of the underlying illness. Gentle suction alone often turns the bronchiolitic infant around. High-flow nasal cannula has reduced intubation rates in moderate bronchiolitis and is a safe first-line non-invasive support, which has shifted many children out of intensive care and onto the ward. [3]
Any child who needs high-flow oxygen, continuous nebulisers, or who has required escalation belongs in a resuscitation or high-dependency area with continuous SpO2 monitoring and, where indicated, carbon dioxide monitoring and senior review. Children retrieved between hospitals need airway- and oxygen-capable staff in transit, because the safest place for a child to deteriorate is not the back of an ambulance. [2]
Discharge is safe only when the child holds the target saturation in air (or on their baseline oxygen), has manageable secretions, a clear and written safety-net, and a follow-up plan. The family must know the warning signs that should bring them back — increasing work of breathing, colour change, drowsiness, poor feeding — because a child who recovered once can decline again. [8]
Special Populations
Neonates and preterm infants are the group most easily harmed by oxygen. Use blended oxygen to a unit-defined target saturation, humidify all flows, and suction gently and only when needed, because over-oxygenation causes retinopathy of prematurity and lung injury and the preterm lung is fragile. [9]
Infants under one year combine every difficulty at once. They are obligate nose-breathers, so a blocked nose obstructs them and nasal suction is disproportionately helpful. Their airways are the smallest, so suction must be gentle and deep pharyngeal suction avoided. And their oxygen reserve is the tiniest, so pre-oxygenate before any procedure. [11]
Children with neurodisability or neuromuscular weakness have a weak cough and copious secretions, so obstruction recurs and the family usually knows the child's airway and suction routine better than anyone at the bedside. Technology-dependent children — tracheostomy, home ventilation, home oxygen — follow their own airway plan; carry the spare tube, use sterile sized catheters, and involve the family in every decision. [11]
Indigenous, remote and rural children across Australia and Aotearoa New Zealand carry a higher burden of acute respiratory illness combined with distance from tertiary services, so the first responder's competence at suction, oxygen and nebuliser therapy is genuinely life-saving before retrieval arrives. Culturally safe, family-inclusive care, interpreter access, reliable retrieval pathways, and a clear written safety-net are all part of equitable respiratory care. [1]
[1]Evidence, Guidelines & Regional Differences
The international guidance converges on the same principles, and the recent trials have hardened the evidence on the points that used to be controversial. Oxygen is given to a target saturation, not to the maximum: the Oxy-PICU trial showed that a conservative target is as safe as a liberal one in critically ill children and may be safer, which underpins the modern practice of targeting and weaning. [8]
High-flow nasal cannula evidence is now mature. The Franklin 2018 PARIS randomised trial showed that high-flow nasal cannula reduces intubation in infants with bronchiolitis compared with standard oxygen. A current review places high flow between standard oxygen and CPAP, and the FIRST-ABC randomised trials found high-flow nasal cannula non-inferior to CPAP as first-line non-invasive support in paediatric critical care. Together these trials justify high flow as the default step before intubation for the deteriorating infant. [3]
Nebuliser and inhaler evidence favours the simpler tool. The Cates Cochrane review found that a spacer with a metered-dose inhaler delivers beta-agonist as effectively as a nebuliser for acute asthma, and faster; the ipratropium meta-analysis supports adding it to salbutamol and steroid for severe attacks; and continuous nebulised salbutamol is preferred for severe attacks. On device physics, vibrating-mesh and jet nebulisers deliver drug differently, and the difference widens under respiratory support, so device choice is a real clinical decision. [7]
[4]Controversies remain. The exact starting flow and weaning strategy for high-flow nasal cannula, the routine use of humidification for low-flow oxygen, the place of nebulised hypertonic saline in bronchiolitis, and the risk-benefit calculation of oxygen in the preterm infant are all still debated. Regional differences are small in principle — ANZ follows RCH Melbourne and ANZCOR, the UK follows the British Thoracic Society and NICE, Canada and the US follow their own societies — and they agree on targets, device classification, and the preference for spacer over nebuliser, while differing in operational detail. [2]
Exam Pearls
Why a nebulised dose misses — DROPS
References
- [1]Franklin D A Randomized Trial of High-Flow Oxygen Therapy in Infants with Bronchiolitis. N Engl J Med, 2018.PMID 29562151
- [2]Alexander EC Effectiveness of high flow nasal Cannula (HFNC) therapy compared to standard oxygen therapy (SOT) and continuous positive airway pressure (CPAP) in bronchiolitis. Paediatr Respir Rev, 2024.PMID 38937210
- [3]Ramnarayan P High-flow nasal cannula therapy versus continuous positive airway pressure for non-invasive respiratory support in paediatric critical care: the FIRST-ABC RCTs. Health Technol Assess, 2025.PMID 40326538
- [4]Cates CJ Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database Syst Rev, 2013.PMID 24037768
- [5]Hamud AA Use of inhaled/nebulised ipratropium bromide in addition to standard first-line treatment with inhaled/nebulised short-acting beta 2-agonist and systemic steroid in the management of acute asthma exacerbations: a systematic review and meta-analysis of randomised controlled trials. Arch Dis Child, 2026.PMID 41224524
- [6]Trend S Current options in aerosolised drug therapy for children receiving respiratory support. Anaesthesia, 2017.PMID 28872662
- [7]MacLoughlin R Vibrating Mesh and Jet Nebulizer Performance in Pediatric Respiratory Support: A Multi-Modality In Vitro Comparison. Pharmaceutics, 2026.PMID 42198269
- [8]Peters MJ Conservative versus liberal oxygenation targets in critically ill children (Oxy-PICU): a UK multicentre, open, parallel-group, randomised clinical trial. Lancet, 2024.PMID 38048787
- [9]Subhi R When should oxygen be given to children at high altitude? A systematic review to define altitude-specific hypoxaemia. Arch Dis Child, 2009.PMID 18829620
- [10]Zulqarnain A Continuous versus intermittent nebulization of salbutamol in acute Severe asthma in children under 12 years of age. Pak J Med Sci, 2026.PMID 41737184
- [11]Ringer CN Physiologic Effects of Nasal Aspiration and Nasopharyngeal Suctioning on Infants With Viral Bronchiolitis. Respir Care, 2020.PMID 32071129
- [12]Le Roch M Iatrogenic mediastinitis in bronchiolitis: Importance of avoiding pharyngeal aspiration. Arch Pediatr, 2019.PMID 31278025