Paeds · investigations-procedures-and-technology
Audiology and hearing-test interpretation
Also known as Audiogram interpretation · Tympanometry · Otoacoustic emissions · OAE · Auditory brainstem response · ABR / BAER · Newborn hearing screening
Fellowship guide to paediatric hearing-test interpretation. Covers reading the pure-tone audiogram (axes, symbols, air versus bone conduction, the air-bone gap, the pure-tone average) and the paediatric degree-of-loss thresholds normal at or under 15 dB HL through slight, mild, moderate, moderately severe, severe and profound; the Jerger tympanogram types A, B, C, As and Ad using admittance, peak pressure and ear canal volume, and why the 1000 Hz probe tone is preferred under six months; otoacoustic emissions as a test of cochlear outer hair cell function; the auditory brainstem response as a test of the whole pathway to the brainstem; the two-stage newborn screen with OAE then automated ABR and the 1-3-6 early hearing detection and intervention milestones; the age-appropriate behavioural tests; and the patterns that separate otitis media with effusion, congenital cytomegalovirus-related loss and auditory neuropathy spectrum disorder, with the ANZ, UK and North American screening and guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the two-week-old baby who referred on the newborn hearing screen and has just arrived at the clinic, or the three-year-old whose nursery teacher worries he is not turning when his name is called. In both, the question is whether this child can hear well enough to acquire speech — and the audiological tests answer it by interrogating different parts of the hearing mechanism in turn. That is the territory this page owns. [1]
Audiology is the measurement of hearing, and in children it has to match the test to the age and to the part of the pathway in question. The pure-tone audiogram measures the softest sound the cochlea can detect at each frequency and gives the degree and type of loss. Tympanometry measures how the eardrum and middle ear move in response to a pressure change and tells you whether the middle ear is aerated, fluid-filled, or under negative pressure. Otoacoustic emissions (OAE) are the faint sounds generated by the cochlear outer hair cells that leak back out into the ear canal; they test the cochlea. The auditory brainstem response (ABR) is the electrical signature the auditory nerve and brainstem produce a few milliseconds after a click or tone, and it tests the whole pathway from cochlea to brainstem. [1] [5]
What makes paediatric audiology distinct from adult audiology is that the child usually cannot raise a hand to signal a threshold, so the tests divide into physiological measures that need no cooperation (OAE, ABR, tympanometry — used in newborns and infants) and behavioural measures that build cooperation by age (behavioural observation, visual reinforcement audiometry, play audiometry, then conventional pure-tone testing). The fellowship skill being tested is choosing the right test for the age, reading the pattern the tests produce together, and never being reassured by a single test that does not answer the whole question — above all, never accepting an OAE pass as proof of hearing in a child at risk of auditory neuropathy. [1] [11]
Classification
Classify paediatric hearing loss by how much (the degree), by where (the type), and by which test catches it (the modality), because each axis changes the diagnosis, the urgency, and the intervention. [1]
By degree, the paediatric normal threshold is at or under 15 dB HL, lower than the adult 25 dB HL cut-off because even a small loss blurs consonants during the years when speech is being laid down. The pure-tone average (PTA) — the mean of the thresholds at 500, 1000 and 2000 Hz — sorts the loss into slight (16 to 25 dB HL), mild (26 to 40), moderate (41 to 55), moderately severe (56 to 70), severe (71 to 90), and profound (over 90 dB HL). These cut-offs are the standard degree-of-loss categories used in audiology and paediatric practice, and a candidate who quotes 25 dB HL as the paediatric normal will under-call a slight loss that matters. [1]
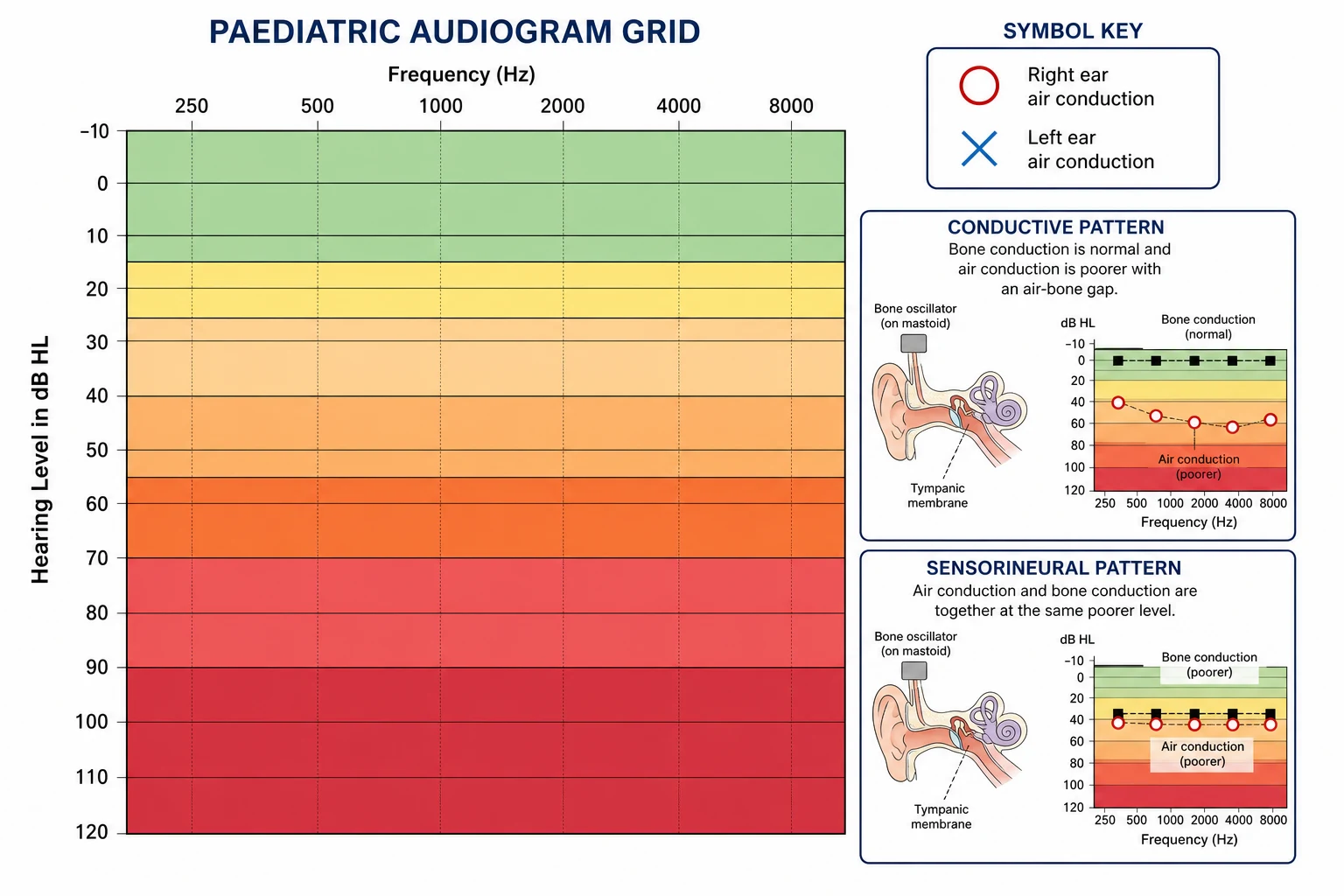
By type, the audiogram separates the loss by where the problem sits along the pathway. A conductive loss sits in the outer or middle ear: bone-conduction thresholds are normal but air-conduction thresholds are reduced, and the gap between them is the air-bone gap, taken to be clinically significant at 15 dB or more. A sensorineural loss sits in the cochlea or the auditory nerve: air and bone thresholds fall together, and there is no air-bone gap. A mixed loss has both a conductive component and a sensorineural component. Reading the air-bone gap before anything else is the single most reliable habit on the audiogram. [1]
By modality, the tests sort into those that need the cochlea alone (OAE), those that need the whole pathway (ABR), and those that measure middle-ear mechanics (tympanometry). The trap that defines this topic is that a child can have preserved OAE and yet have an absent ABR — the cochlea works but the nerve does not conduct. That dissociation is auditory neuropathy spectrum disorder, and classifying a loss by modality is what protects the child from being told the ears are fine when the pathway is impaired. [11] [5]
The numbers that anchor your viva
Epidemiology & Risk Factors
Permanent childhood hearing loss is common enough that universal screening is justified and rare enough that a referred screen is more often a transient than a confirmed loss. Roughly one to three per thousand children are born with permanent bilateral sensorineural hearing loss, and about half of permanent loss is genetic, with the remainder split between environmental causes among which congenital cytomegalovirus (cCMV) is the commonest non-genetic cause. [6] [8]
The children at the highest risk of late-onset or progressive loss after a passed screen are gathered in the JCIH risk-indicator list, and the candidate must know the categories even if not every item: a stay in the NICU of more than five days, or any use of extracorporeal membrane oxygenation or assisted ventilation; treatment with ototoxic medications including aminoglycosides given for more than five days or loop diuretics; hyperbilirubinaemia requiring exchange transfusion; a family history of permanent childhood hearing loss; craniofacial anomalies involving the ear or temporal bone; in-utero infection such as CMV, rubella, toxoplasmosis, herpes or syphilis; a syndrome associated with hearing loss; bacterial meningitis; significant head trauma, especially basal skull fracture; and chemotherapy. These children need surveillance audiometry even when the newborn screen passes, because cCMV in particular can declare a hearing loss months or years later. [6] [2]
On the conductive side, otitis media with effusion (OME) is the dominant cause of mild conductive loss in young children and is most prevalent between one and three years, driven by eustachian tube immaturity. Most effusions resolve spontaneously, but a persistent effusion can hold a child at a 20 to 40 dB conductive loss during the very window when speech is consolidating. [1]
The public-health weakness of newborn screening is loss to follow-up. A referred screen is only useful if the child reaches a diagnostic appointment, and systematic review evidence shows that sociodemographic factors — distance from services, socioeconomic disadvantage, language barriers and rurality — drive the families most likely to be lost. The equity intervention is a single named contact who closes the loop, not another screening device. [10] [12]
Pathophysiology
The teaching model runs from the sound wave at the pinna to the brainstem, and it rests on matching each test to the part of the pathway it interrogates. Read the tests as probes along that pathway and the patterns become logical rather than memorised. [1] [5]
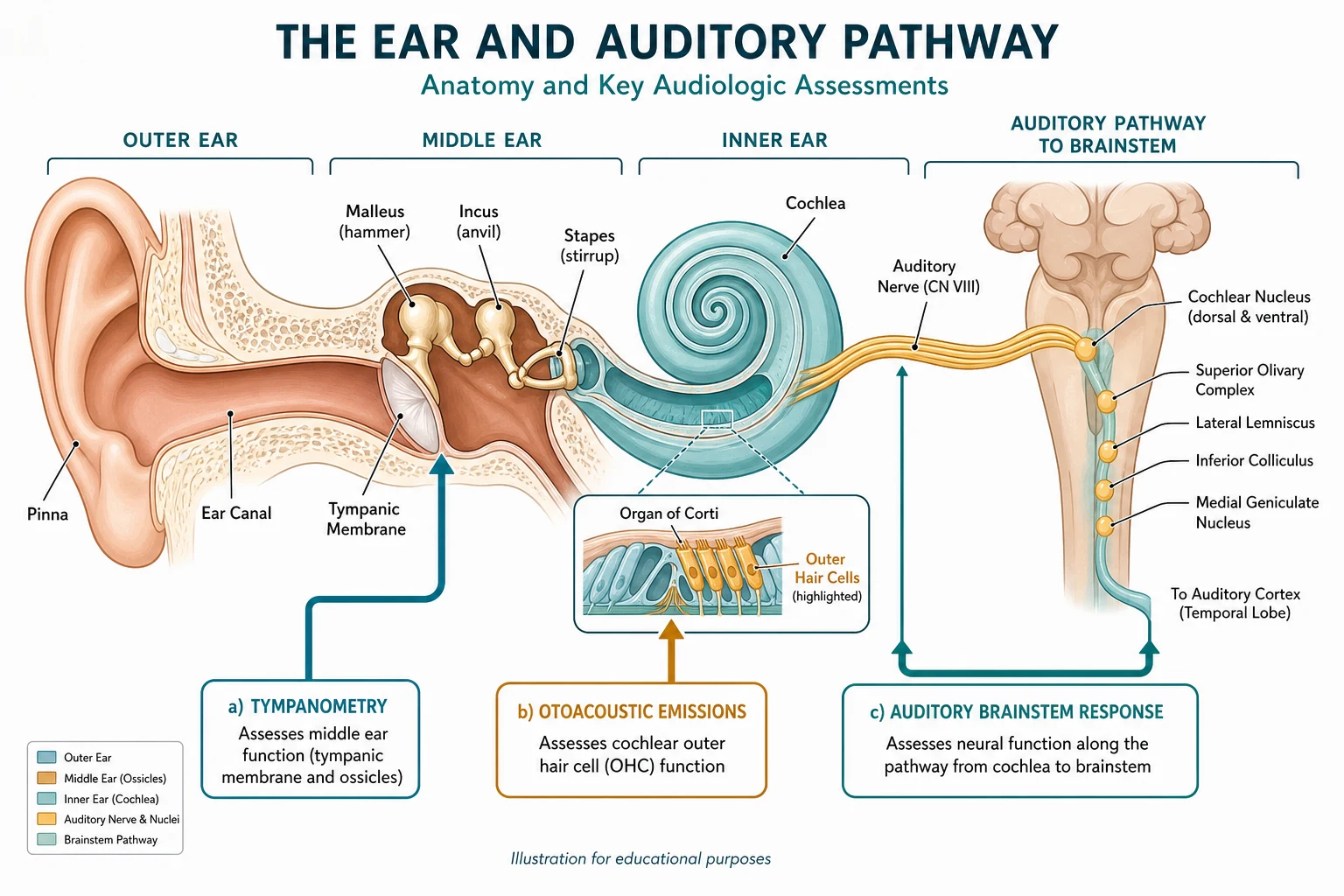
Sound is funnelled by the pinna and ear canal, vibrates the tympanic membrane, and is amplified and impedance-matched by the ossicular chain (malleus, incus, stapes) into the inner ear. This conductive pathway is the part a middle-ear effusion disrupts: fluid in the middle-ear space damps the drum and stiffens the ossicular chain, so the bone-conduction threshold (which bypasses the middle ear) stays normal while the air-conduction threshold drops — producing the air-bone gap of a conductive loss. Tympanometry detects the same mechanics by measuring how the drum admits a probe tone across a sweep of ear-canal pressures, and a fluid-filled middle ear produces a flat trace with no pressure peak. [3]
At the cochlea, the outer hair cells are not passive receptors but biological amplifiers: they generate their own mechanical response — the cochlear amplifier — that sharpens frequency tuning and adds gain. That amplifier is what otoacoustic emissions record. A healthy cochlea emits a faint sound (a transient evoked OAE after a click, or a distortion-product OAE at combination frequencies) that a sensitive microphone in the ear canal can pick up. Present OAE mean functioning outer hair cells; absent OAE mean outer hair cell loss or, equally important, anything that blocks the middle ear and dampens the emission's passage out — which is why an effusion can abolish OAE in a perfectly good cochlea. [1] [11]
The signal then travels along the auditory nerve through a series of brainstem nuclei, and that journey is what the auditory brainstem response records. A click or a tone pip presented through an earphone evokes a series of waves, classically numbered I to V, over the first ten milliseconds; the threshold of wave V is the audiometric estimate. Because the ABR depends on the cochlea, the nerve and the brainstem all working in series, an absent or severely degraded ABR localises the failure anywhere along that chain, which is why the ABR must always be read together with the OAE. [5]
Auditory neuropathy spectrum disorder is the dissociation that sits at the heart of this topic. In ANSD the outer hair cells are intact, so the OAE is present (and the cochlear microphonic is preserved), but the nerve or its synapse fails to conduct a synchronous response, so the ABR is absent or grossly abnormal. Genes such as OTOF, which encodes the synaptic protein otoferlin, produce exactly this picture: a child whose cochlea tests normally on emissions but whose neural conduction is impaired. The behavioural consequence is that the child may detect sound but cannot encode its timing, so speech is audible but unintelligible — a far harder problem than a matched sensorineural loss. [11] [5]
Congenital cytomegalovirus damages the cochlea through a combination of direct viral injury to the stria vascularis and the organ of Corti and an inflammatory vasculopathy, and the damage is often progressive or late-onset rather than present at birth. A child with cCMV can have a normal newborn ABR and still develop a sensorineural loss over the first years of life — which is why cCMV is the single most important reason that a passed screen does not end surveillance. [6] [8]
[11] [5]Clinical Presentation
The clinical scenarios that prompt a hearing test fall into three streams, and the first task is to recognise which stream the child is in, because the test, the urgency and the counselling differ. [1]
The first stream is the newborn or young infant referred from screening. Here the family has been told the screen did not pass, and the child looks entirely well; the job is to move to a diagnostic frequency-specific ABR within the 1-3-6 timeline and to hold the family through the anxiety without either dismissing the refer or alarming them before the diagnosis is confirmed. The second stream is the older infant or toddler with concern about hearing, speech or behaviour — not startling to loud sound, not turning to the parent's voice by nine months, having only a handful of words by eighteen months, or the nursery reporting that the child seems to ignore instructions. The third stream is the child with a known risk factor — a NICU graduate, a craniofacial syndrome, a confirmed cCMV infection, an episode of bacterial meningitis, or a family history — in whom surveillance is mandatory regardless of symptoms. [1] [2]
The OME pattern announces itself through a cluster of clues: a cold two to six weeks earlier, intermittent ear tugging, speech delay that fluctuates, turning the television up, and the classic picture of the two-year-old who seems to hear when close and in a quiet room but loses it in noise. A congenital sensorineural loss more often shows as consistent, non-fluctuating inattention to sound from early infancy and a clear delay in speech milestones. Auditory neuropathy is the subtle one: the child typically responds to sound and may even pass behavioural testing, but has disproportionate difficulty understanding speech, especially in noise — the ears report sound but the brain receives a garbled signal. [1] [11]
The features that should make you worry about progressive or late-onset loss in a child who passed the screen are a parent reporting that hearing seems to be getting worse, a child who is losing speech clarity, an asymmetry on behavioural testing, or new behavioural change around the time of an intercurrent illness. Any child with bacterial meningitis needs a hearing test as soon as the acute illness settles, because the inner-ear damage can be rapid and severe, and a child with confirmed cCMV needs scheduled surveillance because the loss can declare itself over years. [6] [8]
| Pattern | Hearing tests you expect | Where it leads |
|---|---|---|
| Newborn referred on OAE or aABR | Diagnostic frequency-specific ABR | Confirm or exclude PCHL by 3 months; intervene by 6 months |
| Toddler, fluctuating inattention, recent cold | Type B or C tympanogram; mild conductive loss | Otitis media with effusion; watchful waiting then review |
| Consistent speech delay, no startle | Sensorineural loss, symmetric, no air-bone gap | Permanent childhood hearing loss; genetics and cCMV workup |
| Hears sound but cannot understand speech in noise | OAE present, ABR abnormal or absent | Auditory neuropathy spectrum disorder |
| Asymmetrical loss, progressive | Asymmetric sensorineural loss; imaging | cCMV or a vestibular schwannoma in older children; urgent referral |
The trap is the child who passed the newborn screen and is then assumed to hear, when a risk indicator or a subtle developmental signal is being missed. A passed screen is a point-in-time measurement, not a guarantee, and the discipline is to re-test any child whose speech, behaviour or risk profile suggests the screen no longer reflects reality. [2] [6]
Differential Diagnosis
The differential at the bedside is not "is there hearing loss" but what kind, and what is causing it, and the audiogram and the ancillary tests resolve most of it before you reach the history. Frame the differential around four questions and the answer follows. [1]
Conductive
- Air-bone gap of 15 dB or more; bone conduction normal
- Type B or C tympanogram; OAE may be absent from middle-ear damping
- Commonest cause in young children: otitis media with effusion
- Also cerumen impaction, tympanic membrane perforation, ossicular fixation
Sensorineural
- Air and bone fall together; no air-bone gap
- OAE often absent once outer hair cells are lost
- Bilateral: genetic causes (GJB2/Connexin 26) and congenital CMV dominate
- Asymmetric or progressive prompts imaging and cCMV testing
Mixed
- Both an air-bone gap and reduced bone conduction
- Seen in chronic OME superimposed on a permanent loss
- Also in some syndromes and after recurrent infection
- Treat the conductive component to optimise the residual hearing
Auditory neuropathy
- OAE present, ABR absent or grossly abnormal
- Cochlear microphonic preserved
- Behavioural thresholds variable; speech-in-noise disproportionately poor
- OTOF and other synaptic/nerve genes; needs ABR to diagnose
A second layer of differential is what underlies a confirmed sensorineural loss. In a bilateral congenital loss the two commonest answers are a genetic cause — classically GJB2 (Connexin 26) variants, which account for a large share of non-syndromic genetic loss — and congenital cytomegalovirus, which is the commonest non-genetic cause and uniquely able to declare itself late. In an asymmetrical sensorineural loss the differential includes an enlarged vestibular aqueduct, a vestibular schwannoma in older children, and unilateral cCMV, and an asymmetry is the finding that prompts temporal-bone imaging. [8] [6]
The third question is what mimics hearing loss when the ears and the pathway are intact. A child with a developmental language disorder, autism spectrum disorder, or an attention difficulty may present as "not listening", and the discipline is to confirm hearing formally rather than assume the behaviour is explained — but equally, to recognise when a normal audiogram points the evaluation toward development rather than the ear. [1]
Clinical & Bedside Assessment
Assessment before audiology is short and structured: it confirms that the concern is real, screens for a syndromic cause, and ensures the child is sent for the right test at the right age. The aim is never to make the diagnosis at the bedside, but to avoid sending a six-month-old for a behavioural test she cannot do. [1]
Begin with the hearing-specific history. Ask about the newborn screen result and any NICU stay; ask whether the child startles to loud sound, turns to the parent's voice by nine months, babbles with a range of sounds, and has any words by twelve to eighteen months and two-word phrases by two years. Ask specifically whether hearing seems to have worsened, whether speech is regressing, and whether the difficulty is worse in noise. Take a family history of childhood hearing loss and a perinatal history including cCMV risk, NICU admission, ototoxic drugs, hyperbilirubinaemia, and meningitis. [1] [2]
Examine the ears, the face and the systems. Otoscopy looks for a retracted or dull tympanic membrane suggesting an effusion, a perforation, atresia or stenosis of the canal, and cerumen impaction. Look for the dysmorphic features of syndromes associated with hearing loss: the white forelock and heterochromia of Waardenburg, the branchial cysts and renal anomalies of branchial-oto-renal syndrome, the thyroid goitre of Pendred, and the characteristic facies and small ears of Down syndrome, in which both conductive (effusion) and sensorineural loss are over-represented. Examine the neck for branchial cleft remnants and cysts, and consider a developmental assessment, because the impact of the loss shows first in speech and play. [1]
Assess the developmental impact explicitly. A hearing loss in the first three years disrupts the acquisition of speech and language, and the severity of that disruption is itself a reason to act on a mild loss that an adult might tolerate. In the school-aged child, ask about educational progress, attention and fatigue, because an unrecognised mild or unilateral loss can present as inattention or "not trying". [1]
Choosing the right audiological test by age
Birth to around 4-6 months: physiological tests only — diagnostic frequency-specific ABR, OAE, and tympanometry with a 1000 Hz probe tone
Around 6 months to 2.5 years: visual reinforcement audiometry (VRA), supported by OAE and tympanometry
Around 2.5 to 5 years: conditioned play audiometry, with tympanometry; OAE as a screen
From around 5 years: conventional pure-tone audiometry with hand-raise response, as in an adult
Any age with a referred screen or a risk indicator: ABR if the behavioural test is unreliable or the result is equivocal
Investigations
The interpretation of paediatric hearing tests rests on four reads — the audiogram, the tympanogram, the OAE result, and the ABR — and the fellowship candidate must read each correctly and then read them together. [1]
The pure-tone audiogram
The audiogram plots frequency in Hertz on the x-axis (250, 500, 1000, 2000, 4000, 8000 Hz, low to high, left to right) and hearing level in dB HL on the y-axis, with the scale inverted so that better hearing is at the top. The symbols are standard and worth memorising: right ear air conduction is a red circle, left ear air connotation is a blue cross, the bone-conduction symbols are the less-than and greater-than bracket marks for right and left respectively, and masking is shown by drawing a square bracket around the symbol. The pure-tone average is the mean of the air-conduction thresholds at 500, 1000 and 2000 Hz and places the loss into its degree category. Reading the air-bone gap before anything else — comparing the air-conduction against the bone-conduction thresholds — sorts the loss into conductive, sensorineural or mixed. [1]
Tympanometry and the Jerger types
Tympanometry measures three values: the ear canal volume, the static admittance (how much the middle-ear system moves, in millimhos), and the tympanometric peak pressure (the ear-canal pressure at which admittance is greatest, in decaPascals). Read together, these produce the Jerger classification. A type A tympanogram has a peak near atmospheric pressure (within roughly minus 100 to plus 50 daPa) with normal admittance — a normal, aerated middle ear. A type As has a shallow peak with low admittance — a stiff system such as otosclerosis. A type Ad has an abnormally deep peak with high admittance — an overly mobile drum such as ossicular discontinuity. A type B is flat with no identifiable peak — a middle-ear effusion if the ear canal volume is normal, or cerumen impaction or canal atresia if the canal volume is low. A type C has its peak at negative pressure (commonly below minus 150 daPa) — eustachian tube dysfunction, often on the way to or recovering from an effusion. [3] [4]
The probe-tone choice is the infant pitfall. The standard 226 Hz probe tone is reliable in children over about six months and in adults, but the infant middle ear is stiff and mass-dominated, and the 226 Hz tone often yields a flat trace in a perfectly normal infant ear. The 1000 Hz probe tone is the correct choice in infants under six months, and direct comparison with myringotomy findings confirms that the 1000 Hz tone correctly identifies middle-ear effusion where the 226 Hz tone misclassifies normal ears as abnormal. [3] [4]
Otoacoustic emissions and the auditory brainstem response
Otoacoustic emissions are reported as present or absent at each frequency. Present OAE indicate functioning outer hair cells and a clear middle-ear pathway; absent OAE indicate outer hair cell loss, a middle-ear effusion damping the emission, or a problem with probe fit and ambient noise — which is why an absent OAE is interpreted with the tympanogram, not in isolation. [1] [11]
The auditory brainstem response is reported by its wave V threshold, which estimates the degree of hearing loss in dB nHL when the child cannot give a behavioural response. A normal ABR threshold is consistent with normal peripheral hearing; a raised or absent threshold indicates a loss along the cochlea-nerve-brainstem chain. The diagnostic frequency-specific ABR uses tone bursts (rather than a broad-band click) to estimate the audiogram at 500, 1000, 2000 and 4000 Hz, and is the confirmatory test in any infant who refers on a newborn screen. [5]
The patterns that make the diagnosis
The audiological patterns that confirm the common diagnoses are few and worth holding together. Otitis media with effusion shows a type B or type C tympanogram with a mild conductive loss of 20 to 40 dB and often absent OAE from middle-ear damping. Permanent sensorineural loss shows reduced air and bone thresholds with no air-bone gap, and OAE that are absent once the outer hair cells are lost. Congenital cytomegalovirus-related loss is typically sensorineural, may be asymmetrical, and can be progressive or late-onset, which is why the diagnosis rests on cCMV testing (saliva or urine PCR in the neonate, or a dried blood spot in the older infant) rather than on the first audiogram. Auditory neuropathy spectrum disorder shows the dissociation of preserved OAE with an absent or abnormal ABR, often with a preserved cochlear microphonic, and is the one diagnosis that an OAE-only screen is structurally incapable of detecting. [6] [11] [8]
Management — Resuscitation
The resuscitation equivalent in audiology is the time-critical confirmation of a referred screen within the diagnostic window, because every month of delay in the first year is a month of speech input lost. The immediate action when a newborn screen refers is to book the diagnostic frequency-specific ABR, and the target is a confirmed diagnosis by three months of age. [2]
When a screen refers, the most important immediate intervention is accurate counselling that prevents loss to follow-up without catastrophising. Explain that a refer is common — often from middle-ear fluid, vernix or ambient noise in the first day — that it is not a diagnosis, and that the next step is a painless diagnostic ABR while the baby sleeps. The family must leave with a named appointment, a named contact, and a clear date, because the child who is "going to be referred" but never attends is the child the screening programme fails. [10] [12]
When bacterial meningitis is the trigger, the resuscitation principle is that inner-ear damage can evolve within hours to days, so a hearing test is booked as soon as the acute illness settles rather than waiting for routine follow-up — a child deafened by meningitis is a candidate for urgent cochlear implantation assessment, because the bony labyrinth can ossify and close the window for implantation. [1] [8]
If a middle-ear effusion is found at diagnostic testing, the resuscitation question is whether it is preventing a reliable diagnostic ABR. An effusion can abolish OAE and elevate ABR thresholds, so a child may need the effusion managed (observation or, rarely, ventilation tubes) before the permanent-loss question can be answered — but a suspected permanent loss should never be deferred indefinitely behind an effusion, and a diagnostic ABR is pursued in parallel. [1] [3]
Management — Definitive & Stepwise
Once a hearing loss is confirmed, the stepwise pathway runs from diagnosis through habilitation, aetiological work-up, and surveillance, and it is the same pathway whether the loss was found at newborn screening or later. [1] [2]
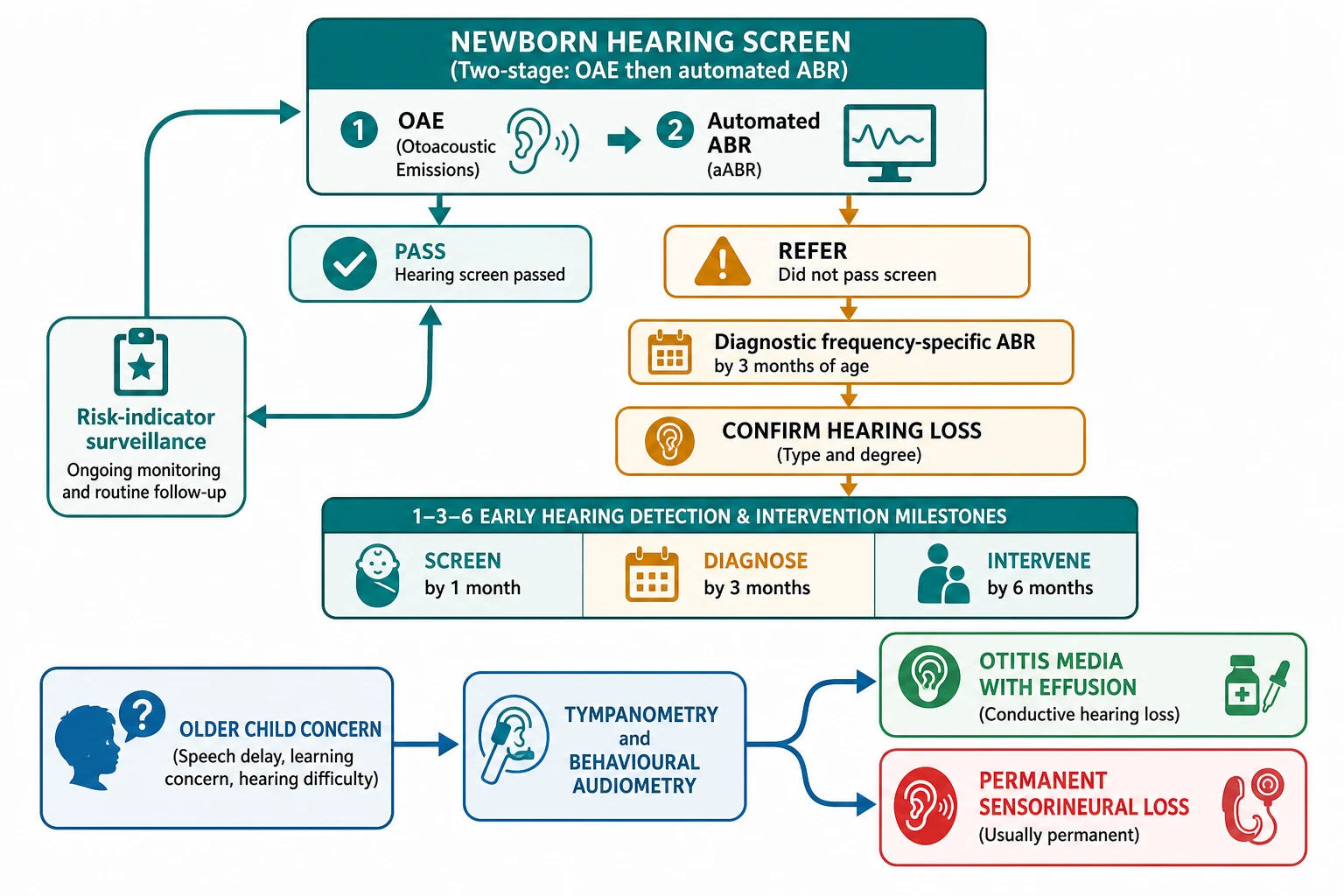
The first milestone is confirmation of the diagnosis with a frequency-specific ABR in the infant, or repeat behavioural testing in the older child, to confirm both the degree and the type of loss. The 1-3-6 framework — screen by one month, diagnose by three months, fit hearing aids and enrol in early intervention by six months — is the operational backbone of early hearing detection and intervention programmes, and the evidence supports that meeting it measurably improves language outcomes. [2] [12]
For otitis media with effusion, the audiological management is watchful waiting in the first instance, because most effusions resolve within three months. Hearing is re-tested at the end of that period, and persistent bilateral OME with a hearing loss of around 20 to 30 dB or more that has lasted at least three months is the threshold at which referral for consideration of ventilation tubes (grommets) is appropriate, in line with national guidance that frames surgery against the natural history. The role of audiology is to document the loss over time and to ensure that a child who is failing to develop speech because of persistent effusion is not left waiting indefinitely. [1]
For permanent sensorineural loss, the definitive management is amplification fitted early — hearing aids for moderate and greater losses, calibrated to the ABR or behavioural thresholds — followed by early intervention services for the family and cochlear implantation for severe-to-profound loss where hearing aids provide insufficient benefit. The candidacy for a cochlear implant is set by the degree of loss and the lack of progress with amplification, and implantation in the first year of life gives the best spoken-language outcomes. [1] [8]
The aetiological work-up that follows a confirmed sensorineural loss looks for the cause and the associated risks. Congenital CMV testing (saliva or urine PCR in the first three weeks of life; a retrospective dried blood spot in the older infant) identifies the child who may benefit from antiviral therapy. Genetic testing including a GJB2 (Connexin 26) panel identifies the commonest non-syndromic genetic cause and informs counselling. Temporal-bone imaging is pursued for an asymmetric loss to look for an enlarged vestibular aqueduct or, in older children, a vestibular schwannoma. An electrocardiogram is performed in the child with a syndrome that includes arrhythmia risk, such as the long-QT associated with Jervell and Lange-Nielsen syndrome. [6] [8]
For auditory neuropathy spectrum disorder, the management diverges from a typical sensorineural loss because amplification may help detection without restoring intelligibility. The child is managed by a multidisciplinary team weighing hearing aids, frequency-modulating (FM) or remote-microphone systems, and, where speech perception remains poor, cochlear implantation, which can be effective when the lesion is the synapse (as in OTOF-related ANSD). The hallmark is that the decision is individualised and audiology-led, not protocol-driven. [11] [8]
Valganciclovir (symptomatic congenital CMV with sensorineural hearing loss, IDSA / consensus)
Specific Subtypes & Scenarios
The approach to paediatric hearing testing changes with the child and the question, and the candidate must adjust the test and the timeline to the subtype. [1]
In the newborn who refers on one ear, the pathway is the same as for a bilateral refer — a diagnostic frequency-specific ABR by three months — but the differential tilts toward a unilateral permanent cause such as an enlarged vestibular aqueduct, a unilateral cCMV infection, or a cochlear malformation. A unilateral loss is easy to underestimate because the child hears with the other ear, but it carries real educational and localisation consequences and is not dismissed. [1] [6]
In the child with otitis media with effusion, the audiological task is to separate the transient conductive overlay from any underlying permanent loss. The tympanogram and the audiogram are repeated over the watchful-watching period; if the loss persists at the same degree after the effusion has resolved, a permanent component is suspected, and an OAE and, in the infant, an ABR are pursued. The danger is over-diagnosing a permanent loss from a transient effusion, and the discipline is to track the loss over time. [1] [3]
In the child with suspected auditory neuropathy, the diagnosis is made by demonstrating preserved OAE (and a preserved cochlear microphonic) alongside an absent or degraded ABR. Because OAE can disappear over time as the outer hair cells are lost, the child with a clear history of "hearing but not understanding" is referred for ABR even when the OAE has become equivocal. [11] [5]
In the child with confirmed congenital cytomegalovirus, the audiological question is not whether there is a loss today but whether one will develop. A child with cCMV and a normal audiogram at birth is still at risk of a late-onset loss, and prognostic work shows that factors present in the neonatal period can stratify that risk. The practical answer is scheduled surveillance — typically at diagnosis and at regular intervals through early childhood — rather than a single reassurance, and a child who develops a loss is considered for valganciclovir in consultation with infectious diseases. [6] [7]
In the child with Down syndrome or a craniofacial syndrome, both conductive and sensorineural loss are over-represented, the ear canals are often stenotic, and the child may not cooperate with behavioural testing. The approach is earlier and more frequent testing, a low threshold for diagnostic ABR when behavioural testing is unreliable, and active management of effusion because even a mild conductive loss compounds the developmental risk. [1]
In the older child with speech delay or school difficulty who passed the newborn screen, the approach is a full behavioural audiogram with tympanometry, looking for a missed mild or unilateral loss, an overlooked effusion, or a progressive loss. The school-entry hearing screen is the safety net for the child who slipped through, and the evidence base supports it as accurate and worthwhile, though it does not replace targeted testing of any child with concern. [9] [1]
Complications & Pitfalls
The complications of audiology are the harms of misinterpretation and of delay, and the discipline is to read every test against the age-appropriate normal and against the other tests, never in isolation. [1]
The dominant harm is undelayed diagnosis. A hearing loss that is missed or confirmed late in the first three years disrupts speech, language, social-emotional development and later literacy, and the developmental cost is the single reason the 1-3-6 timeline exists. The evidence is consistent that children whose loss is identified and managed within the timeline have better language outcomes than those identified later, regardless of the degree of loss. [2] [12]
The common interpretive errors are few and worth naming. Using 25 dB HL as the paediatric normal under-calls a slight loss that matters in a child. Ignoring the air-bone gap misses a conductive loss or mislabels a mixed loss as sensorineural. Reading an absent OAE as cochlear damage without checking the tympanogram over-calls a loss that is simply an effusion damping the emission. OAE-only screening structurally misses auditory neuropathy, because the emissions are preserved. And tying a permanent loss to a transient effusion without follow-up either over-diagnoses or under-diagnoses, depending on the direction of the error. [1] [11]
The infant tympanometry pitfall deserves its own line. Using a 226 Hz probe tone in an infant under six months produces flat traces in normal ears, because the stiff infant middle ear does not respond to the low-frequency tone; the 1000 Hz probe tone is the correct choice, and direct comparison with myringotomy confirms its superior accuracy in this age group. A flat tympanogram in a young infant read with a 226 Hz probe tone is not evidence of effusion. [3] [4]
Prognosis & Disposition
The prognosis of paediatric hearing loss is overwhelmingly a function of how early it is identified and managed and of its underlying cause, and the disposition is built around closing the timeline and setting up surveillance. [1] [2]
For permanent bilateral sensorineural loss, the prognosis for spoken language, literacy and social development is excellent when the loss is identified within the 1-3-6 timeline, hearing is amplified or implanted appropriately, and the family is supported by early intervention. The degree of loss and the presence of additional developmental needs modify the trajectory, but timing of intervention is the single largest modifiable factor. [2]
For otitis media with effusion-related conductive loss, the natural history is resolution of the effusion in the majority within three months, with the hearing returning to normal as the middle ear re-aerates. The disposition is therefore watchful waiting with a planned re-test, reserving surgical referral for the child with persistent bilateral loss and developmental impact. [1]
For congenital cytomegalovirus-related loss, the prognosis depends on whether the loss is stable, progressive or late-onset, and on the response to antiviral therapy where indicated. The disposition is scheduled audiological surveillance through early childhood, because the loss can declare or progress after a normal early assessment, and the family is kept in contact with both audiology and infectious diseases. [6] [7]
The referral map is straightforward. Any referred screen or suspected loss is referred to paediatric audiology; a confirmed permanent loss triggers referral to ear, nose and throat (ENT) surgery, genetics for the child with a likely genetic cause, paediatric infectious diseases for the child with cCMV, and early intervention services for the family. The safety-net for the child with risk indicators who passed the screen is a written surveillance plan, not reassurance alone. [1] [8]
Special Populations
The approach to hearing testing is adjusted for the child in front of you, and the candidate must match the test and the timeline to the population. [1]
In the neonate and young infant, only physiological tests are reliable, and the test of choice for a referred screen is the diagnostic frequency-specific ABR, supported by OAE and 1000 Hz tympanometry. Behavioural testing waits until the infant is old enough for visual reinforcement audiometry, around six months. The risk profile is highest in the NICU graduate, who carries several risk indicators at once. [3] [2]
In the child with Down syndrome or a craniofacial syndrome, hearing loss is common, ear canals are often stenotic, and cooperation with behavioural testing is limited, so the threshold for diagnostic ABR is lower and the surveillance interval shorter. A conductive loss from persistent effusion is actively managed because it compounds the developmental risk. [1]
In the child in a remote or rural setting, the screening and diagnostic pathway is the same in principle but harder to deliver in practice, and the equity intervention is to bring the test to the child through outreach clinics or telehealth-supported models, and to hold the family with a named coordinator so that distance does not become loss to follow-up. [10] [12]
In the child with a disability or neurodevelopmental disorder who cannot cooperate with behavioural testing, the physiological tests (ABR, OAE, tympanometry) carry the diagnosis, and behavioural testing is used as far as the child can manage. The discipline is to obtain an objective measure of hearing before attributing a language or developmental difficulty to cognition alone. [1]
In the child of a migrant or refugee family with limited language access, the risk of a missed screen or loss to follow-up is higher, and the intervention is interpreter-mediated counselling, written information in the family's language, and a coordinator who can hold the family through the diagnostic and intervention pathway. [10]
In the technology-dependent or NICU-graduate child, several risk indicators — ototoxic drugs, hyperbilirubinaemia, ECMO, prolonged ventilation — converge, and surveillance is mandatory even when the screen passes, because the cumulative ototoxic and hypoxic insult can declare a loss later. [2] [1]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric hearing testing rests on three pillars: the screening-programme evidence, the 1-3-6 outcome evidence, and the cCMV treatment evidence, and the regional deltas flow from how each jurisdiction implements them. [1] [2]
The screening evidence is mature. Universal newborn hearing screening identifies the majority of permanent bilateral sensorineural loss in the first months of life, and systematic review evidence has mapped the programme factors — the screening device, the protocol, the timing, and the follow-up infrastructure — that determine referral rates and loss to follow-up. The two-stage protocol (OAE then automated ABR, or ABR with OAE as a screen) reduces false referrals while keeping sensitivity, though OAE-only protocols structurally miss auditory neuropathy. [12] [10]
The 1-3-6 outcome evidence underpins the whole programme. Children whose permanent hearing loss is identified by the milestones, fitted with appropriate amplification, and enrolled in early intervention by six months show measurably better language outcomes than those identified later, and this evidence is the justification for the operational insistence on closing the loop on every referred screen. [2]
The cCMV treatment evidence has moved the field. Antiviral therapy with valganciclovir improves hearing and developmental outcomes in symptomatic congenital CMV, and the question of treating the child with isolated sensorineural loss, and of extending the course, is the live controversy. [8]
Preserved distortion product OAE in OTOF-related hearing impairment (Santarelli et al., Ear Hear 2024)
PMID 37677959
Population: Children with OTOF-related auditory neuropathy spectrum disorder
Comparator: Children with typical sensorineural hearing loss
Key finding
OTOF-related hearing impairment preserves distortion product OAE and the cochlear microphonic while abolishing or degrading the ABR, demonstrating that auditory neuropathy is a neural-synaptic lesion with an intact cochlea — the pattern an OAE-only screen cannot detect.
Where the evidence is weak or contested: the exact age at which to switch from the 1000 Hz to the 226 Hz tympanometry probe tone (commonly placed at around six months, though infant middle-ear mechanics vary); the role of cortical auditory evoked potentials in confirming the audiological diagnosis in complex children; the timing and candidacy of cochlear implantation in auditory neuropathy; and the optimal duration of valganciclovir for the child with cCMV and isolated hearing loss. Each is a defensible viva topic. [3] [8]
Exam Pearls
The fellowship examiner expects a candidate who can read the audiogram, the tympanogram, the OAE and the ABR together, quote the degree-of-loss thresholds for the paediatric range, and defend the screening pathway and the surveillance plan. [1]
The single most testable fact is that the paediatric normal threshold is at or under 15 dB HL, not 25 dB HL, and the degree of loss runs from slight (16 to 25), mild (26 to 40), moderate (41 to 55), moderately severe (56 to 70), severe (71 to 90) to profound (over 90 dB HL), using the pure-tone average of 500, 1000 and 2000 Hz. The air-bone gap of 15 dB or more marks a conductive loss; air and bone falling together marks a sensorineural loss. [1]
The Jerger types in one line each — A normal, As shallow and stiff, Ad deep and discontinuous, B flat and fluid-filled (if canal volume normal), C negative pressure — and the 1000 Hz probe tone under six months, 226 Hz thereafter — are the tympanogram facts that earn marks. [3] [4]
The ANSD signature — preserved OAE with an absent or abnormal ABR — is the pattern an OAE-only newborn screen structurally cannot detect, and it is the reason the two-stage protocol with ABR exists. The 1-3-6 milestones (screen by one month, diagnose by three, intervene by six) and the named risk indicators (NICU stay over five days, ototoxic drugs, family history, craniofacial anomaly, in-utero infection, syndrome, meningitis, head trauma, chemotherapy) are the screening facts. [2] [11]
The classic distractors the exam rewards for naming: accepting 25 dB HL as the paediatric normal; reading an absent OAE as cochlear damage without checking the tympanogram; performing tympanometry with a 226 Hz probe tone in an infant under six months; treating a passed newborn screen as a lifetime guarantee in a child with risk indicators; and using an OAE-only screen in a population at risk of auditory neuropathy. Each is wrong for a specific, citable reason. [1] [3]
References
- [1]Harlor AD Jr, Bower C, Committee on Practice and Ambulatory Medicine, Section on Otolaryngology-Head and Neck Surgery Hearing assessment in infants and children: recommendations beyond neonatal screening Pediatrics, 2009.PMID 19786460
- [2]Awad R, Oropeza J, Uhler KM Meeting the Joint Committee on Infant Hearing Standards in a Large Metropolitan Children's Hospital: Barriers and Next Steps Am J Audiol, 2019.PMID 31084570
- [3]Gellrich D, Eder K, Echternach M, Gröger M, et al A Comparison of 226- and 1000-Hz Probe Tone Tympanometry With Myringotomy Findings in Infants Am J Audiol, 2024.PMID 39413047
- [4]Pilka E, Kochanek K, Jedrzejczak WW, Saczek A, et al Comparison of tympanometry results for probe tones of 226 Hz and 1000 Hz in newborns Int J Pediatr Otorhinolaryngol, 2021.PMID 34175657
- [5]Hunter LL, Blankenship CM, Gunter RG, Keefe DH, et al Cochlear Microphonic and Summating Potential Responses from Click-Evoked Auditory Brain Stem Responses in High-Risk and Normal Infants J Am Acad Audiol, 2018.PMID 29708492
- [6]Buonsenso D, Pedrero-Tomé R, Raimondi F, Salomé S, et al Prognostic Factors of Late-onset Hearing Loss in Infants With Congenital Cytomegalovirus and Normal Audiologic Assessment at Birth Pediatr Infect Dis J, 2026.PMID 40838764
- [7]Chung PK, Schornagel FAJ, Goeman J, Vossen ACTM Predicting mid-term hearing and developmental outcome in clinically inapparent congenital cytomegalovirus infection with hearing loss at birth Early Hum Dev, 2025.PMID 41101277
- [8]Abdul-Hadi S, Choo DI What Is the Most Effective Management of Congenital Cytomegalovirus-Related Hearing Loss? Laryngoscope, 2026.PMID 42370518
- [9]Bamford J, Fortnum H, Bristow K, Smith J, et al Current practice, accuracy, effectiveness and cost-effectiveness of the school entry hearing screen Health Technol Assess, 2007.PMID 17683682
- [10]Atherton KM, Poupore NS, Clemmens CS, Nietert PJ, et al Sociodemographic Factors Affecting Loss to Follow-Up After Newborn Hearing Screening: A Systematic Review and Meta-Analysis Otolaryngol Head Neck Surg, 2023.PMID 36939626
- [11]Santarelli R, Scimemi P, Cama E, Domínguez-Ruiz M, et al Preservation of Distortion Product Otoacoustic Emissions in OTOF-Related Hearing Impairment Ear Hear, 2024.PMID 37677959
- [12]Mackey AR, Bussé AML, Del Vecchio V, Mäki-Torkko E, et al Protocol and programme factors associated with referral and loss to follow-up from newborn hearing screening: a systematic review BMC Pediatr, 2022.PMID 35932008