Paeds · investigations-procedures-and-technology
Bag-mask ventilation and basic airway adjuncts
Also known as Paediatric bag-mask ventilation · BMV in children · Self-inflating bag ventilation · Oropharyngeal airway insertion · Guedel and nasopharyngeal airway · Two-person mask ventilation
Fellowship guide to the two skills that stand between a hypoxic child and a cardiac arrest: ventilating through a face mask, and holding a blocked airway open with an adjunct. Covers manual ventilation device classification, one- and two-person technique, ventilation rates for rescue breathing and arrest, oropharyngeal and nasopharyngeal airway sizing and insertion, the laryngeal mask airway as a rescue device, the paediatric difficult-mask-ventilation predictors, gastric insufflation, and the neonatal T-piece resuscitator.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A floppy, blue infant pulled from a swimming pool, a bronchiolitic baby who has finally exhausted, and a child who has stopped breathing after a seizure all need the same two hands-on skills, and they need them in the next ten seconds: open the airway, and squeeze air into the lungs through a mask held tight to the face. These skills — bag-mask ventilation and the basic airway adjuncts that hold a blocked airway open — are bundled as one topic because they are done together, at the bedside, in the first minutes of every paediatric resuscitation, and because the same small set of anatomy and physics decides whether each of them works. They are also the most decisive skills in paediatrics: respiratory failure and apnoea, not primary cardiac events, cause the great majority of paediatric arrests, so the provider who can ventilate a child keeps the heart beating. [3]
Each skill rests on one idea. Bag-mask ventilation moves gas into the lungs by squeezing a bag through a sealed mask, and whether it works depends almost entirely on whether the airway is open and the mask sealed — not on the bag. An airway adjunct is a shaped piece of plastic that lifts the tongue off the back of the throat when the head position cannot, holding open the passage that the bag then fills. Get the airway open and the seal right and almost any child can be ventilated; get either wrong and the most expensive bag in the hospital delivers nothing to the lung. [1]
Classification
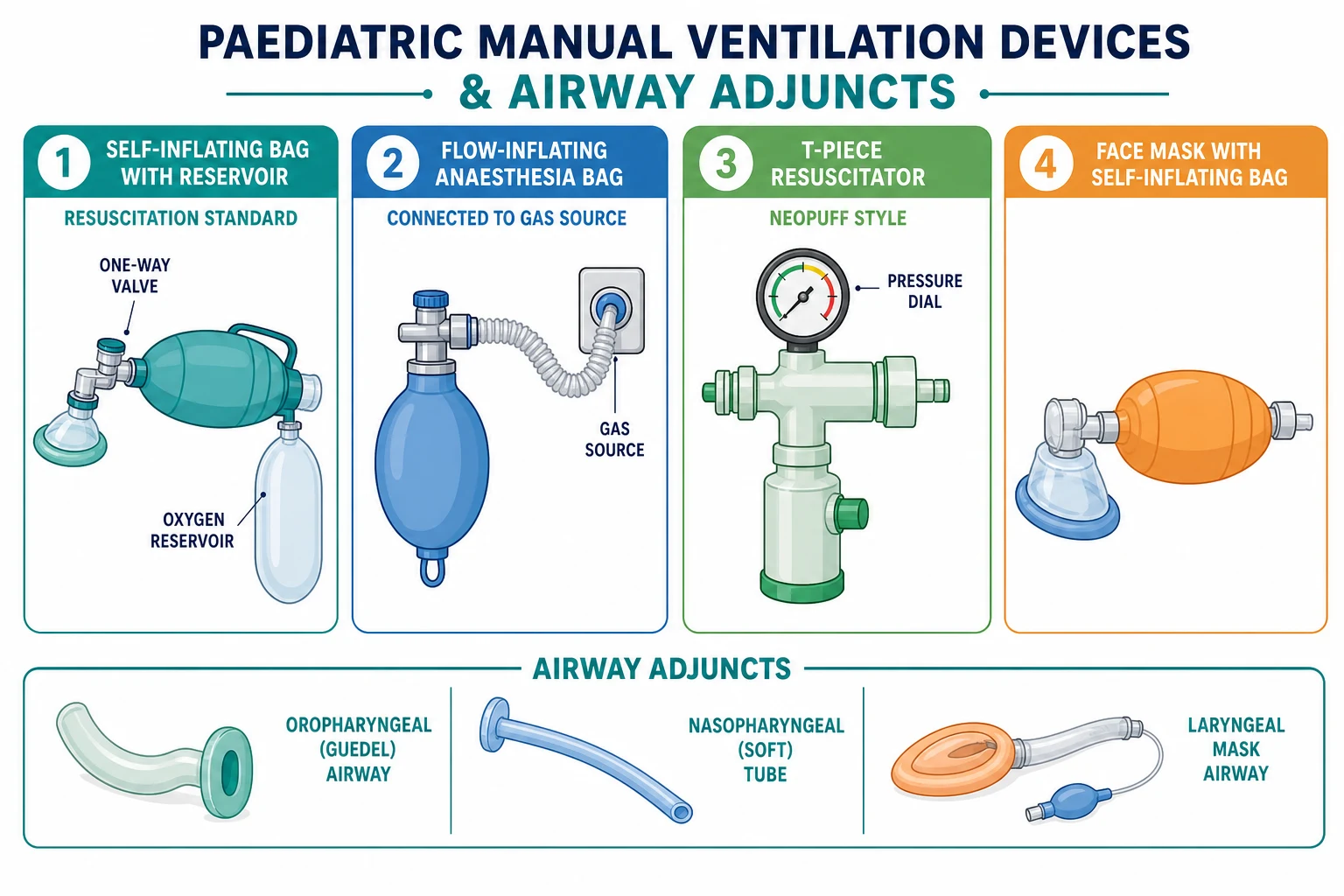
The useful way to classify the ventilation devices is by how they generate the breath, because that decides where you reach for each one. A self-inflating bag re-expands on its own after every squeeze whether or not it is connected to oxygen or pressed to a face, so it is the only device that works in the hands of a single rescuer at an arrest, and it is the resuscitation standard. A flow-inflating bag, the anaesthesia bag, only inflates when it is connected to a continuous flow of gas and sealed to the airway, so it needs a gas source and a tight circuit and is the tool of the anaesthetist. A T-piece resuscitator, such as the Neopuff, connects a gas source to the mask or tube through a fixed-pressure circuit that delivers a set peak inspiratory pressure and a consistent positive end-expiratory pressure, which is why it is the neonatal standard for controlled, gentle ventilation. [8]
[8]The adjuncts sort by where they sit and who they are for. An oropharyngeal airway (a Guedel) is curved plastic that follows the contour of the tongue and holds it off the posterior pharyngeal wall, but only in a child so unconscious they have lost the gag reflex, because a Guedel in a gagging child provokes vomiting. A nasopharyngeal airway is a soft tube passed through the nostril to sit behind the tongue, for the semi-conscious child who still has a gag. A supraglottic airway, the laryngeal mask airway, sits above the glottis and seals around it, and it is the bridge between failed mask ventilation and a definitive tube. [10]
Epidemiology & Risk Factors
Respiratory failure is the path to most paediatric arrests, so the demand for competent bag-mask ventilation is constant across every acute setting — delivery room, emergency department, ward, intensive care, and the back of a retrieval vehicle. Infants under one year need the skill most often, because their airways are smallest, their tongues largest relative to the mouth, their oxygen reserve tiniest, and their chest walls most compliant, so they obstruct and desaturate within seconds. [1]
Some children are hard to ventilate before you even begin, and recognising them is half the battle. Difficult mask ventilation clusters in the infant with a small face and large tongue, the obese adolescent, and the child with a congenital or syndromic airway — Pierre Robin sequence with micrognathia and glossoptosis, Treacher Collins, Down syndrome, and the mucopolysaccharidoses. Limited mouth opening, a short thyromental distance, restricted neck movement, and upper-airway obstruction from laryngomalacia or a peritonsillar and retropharyngeal abscess each raise the chance that a mask will not seal and the airway will not stay open. The skill itself is fragile: bag-mask quality decays quickly without practice, and even trained relatives and providers commonly deliver breaths that never move the chest. [11]
Indigenous, remote and rural children across Australia and Aotearoa New Zealand carry a higher burden of acute respiratory illness and sit further from intensive care, so the first responder's competence at bag-mask ventilation in the minutes before retrieval arrives is genuinely life-saving.
[1]Pathophysiology
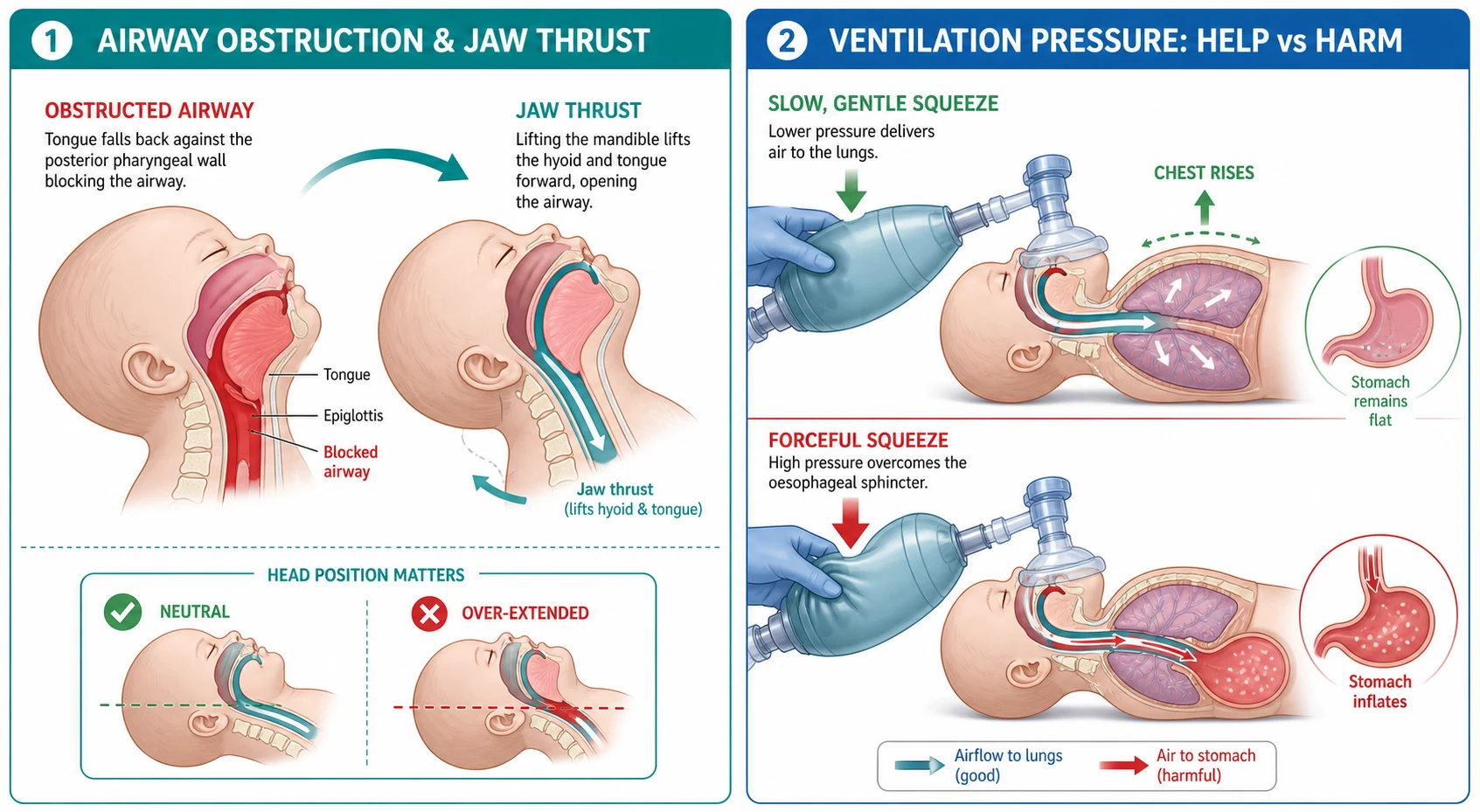
Three paediatric anatomical facts explain why mask ventilation is both powerfully effective and surprisingly hard, and a candidate who holds them can answer almost any question on this topic. The first is the tongue. An infant's tongue is large relative to a small oral cavity, and the occiput is large, so the head flexes and the tongue falls back against the soft, high anterior posterior pharyngeal wall to obstruct the airway. A chin lift, a jaw thrust, the right head position, or an adjunct each work by lifting that tongue off the wall, which is the single act that reopens the airway. [3]
The second is the compliant chest and the high-resistance airway. A child's chest wall is soft, so a small leak at the mask dumps the whole tidal volume without a visible chest rise, and a millimetre of obstruction or oedema in a small airway multiplies the resistance so that the pressure needed to move gas climbs steeply. The cricoid ring, not the glottis, is the narrowest point of a child's airway, so subglottic narrowing or oedema raises the pressure that the bag must generate. The third is the lower oesophageal sphincter, which a forceful or too-rapid squeeze overcomes, pushing gas into the stomach instead of the lung. [11]
The physics of the devices follows directly from this. A self-inflating bag delivers its tidal volume only if the mask seals and the airway is open; squeeze it too fast or too hard and the peak inspiratory pressure climbs until it exceeds the oesophageal closing pressure, and the gas takes the path of least resistance into the stomach. A stomach full of air splints the diaphragm, reduces the tidal volume further, and sets up regurgitation and aspiration. This is why the technique is to squeeze slowly over about one second and to use the smallest volume that moves the chest. A T-piece resuscitator sidesteps the problem by delivering a set pressure: gas flows only to the resistance of the lung and not, at correct pressures, into the stomach, which is why it is the neonatal standard. [8]
Clinical Presentation
A child needing bag-mask ventilation shows it at the bedside, and the signs are read in seconds. The clearest is apnoea or agonal gasping, but the deteriorating infant also shows a falling heart rate and loss of tone, which together are the pre-terminal signature of hypoxia. The tiring child with bronchiolitis, asthma, pneumonia or neuromuscular weakness shows exhaustion and decreasing respiratory effort before the breathing stops, with recession giving way to a shallow, slow, ineffective pattern. The airway obstruction is often audible before it is visible: snoring or stertorous breathing from the tongue, gurgling from liquid or vomit, and stridor or retractions from laryngeal or subglottic obstruction. [1]
The presentation that demands immediate ventilation is the bradycardic, hypoxic, unresponsive infant, because a slow heart rate in a sick child is the heart's response to hypoxia and ventilation usually reverses it within seconds. Recognising this converts a "cardiac arrest" call into a "ventilate the child" action and is the single most important bedside judgement in paediatric resuscitation. The chest compressions come only if the heart rate stays slow despite effective ventilation with oxygen. [1]
Watch for the presentations that make ventilation hard from the start. The child with a dysmorphic airway — micrognathia, a small mouth, a large tongue — will not seal easily and should have a two-person technique and a supraglottic airway ready. The obese adolescent and the child with limited neck movement need a jaw thrust and an adjunct. The trauma patient in a collar must never have head tilt, because a cervical spine injury may sit beneath it. And the technology-dependent child with a tracheostomy who collapses is most often obstructed behind their own tube, so the first move is to suction or replace the tube and ventilate through the stoma before resorting to the mouth. [11]
Differential Diagnosis
The differential here is practical, not pathological: it is the short list of reasons ventilation is failing, each with its fix. When the chest is not rising, run through them in order. A poor seal — a mask that is too large or too small, or a single-hand grip that leaks — is corrected by choosing the size that spans the bridge of the nose to the mental prominence of the chin and by switching to a two-person grip. An obstructed airway — the tongue, vomit, or blood — is corrected by a jaw thrust, suction, and an adjunct. [10]
Wrong head position is the silent cause. Over-extending an infant's neck folds the high anterior airway and obstructs it, where the same extension opens an older child's airway; the fix is a neutral position in the infant, supported by a shoulder roll. Device failure is the avoidable one: a self-inflating bag disconnected from oxygen, a missing or jammed one-way valve, or an anaesthesia bag with the gas turned off. Anatomical difficult mask ventilation — the syndromic airway or the obese child — is the reason to move early to a two-person technique and a supraglottic airway. [11]
[10]The can't-miss diagnoses are the ones where more ventilation makes the child worse. A tension pneumothorax and a blocked tracheostomy tube are each relieved by decompression, not by harder squeezing, and a solid foreign body in the larynx is dislodged or bypassed, not pushed deeper. When the chest will not rise despite a correct mask, a seal, an open airway, and an adjunct, the diagnosis has shifted from technique to obstruction, and the rescuer must stop squeezing and find it.
[10]Clinical & Bedside Assessment
Assess before, during and after every breath, and let the monitors run continuously. Look, listen and feel at the airway and breathing: is the chest rising — the single most important sign of effective ventilation — is obstruction audible, is there vomit or blood? Attach pulse oximetry and, wherever it is available, waveform capnography, because exhaled carbon dioxide confirms that gas is reaching the lungs and quantifies the rate. [3]
Position the head before you pick up the bag. The infant is held neutral, because over-extension obstructs the airway, often with a small shoulder roll to counter the large occiput; the older child is placed in the sniffing position, head slightly extended. Pre-oxygenate with high-flow oxygen if there is even a few seconds to spare. Choose the correct mask — the one that spans from the bridge of the nose to the chin without pressing on the eyes or tucking under the chin — because a wrong mask size is the commonest reason a seal fails. [1]
During ventilation, confirm bilateral chest rise with each breath, watch the heart rate and the SpO2 trend, and reassess after 10 to 20 seconds. A rising heart rate and colour, with visible chest rise, mean effective ventilation. A heart rate that stays slow despite a correct mask, an open airway, and an adjunct means either that ventilation is still ineffective or that the child is in cardiac arrest and needs chest compressions. State the plan out loud — the technique, the rate, and the trigger for escalation — because structured thinking is what examiners and the team at the bedside both reward. [4]
Investigations
Bag-mask ventilation is a resuscitation procedure, so no investigation precedes it and none is allowed to delay it. The essential monitor is pulse oximetry, to confirm and trend the oxygen saturation, and waveform capnography is added wherever possible because exhaled carbon dioxide confirms that the breath reaches the lungs and tells you the rate. [3]
A blood gas, taken once the child is stabilised, reads the carbon dioxide and pH that pulse oximetry cannot, and it is how you discover the child who looked comfortable on a mask but was quietly retaining carbon dioxide. For the neonate, the pre-ductal oxygen saturation is the target that guides oxygen titration. The real "investigation" of ventilation effectiveness, though, is clinical: bilateral chest rise, a rising heart rate, and improving colour and saturation, each measured against the baseline before ventilation began. No test substitutes for watching the chest. [5]
One diagnostic caveat matters. A child who cannot be ventilated despite a correct mask, a seal, an open airway, and an adjunct must be reassessed for a treatable obstruction — a tension pneumothorax, a blocked tracheostomy, or a solid foreign body — rather than ventilated harder. Persisting with the bag when the diagnosis has shifted from technique to obstruction is the classic avoidable error.
[5]Management — Resuscitation
The resuscitation order is open the airway, then ventilate, then reassess, all within seconds. Position the head (neutral infant, sniffing child), clear any visible obstruction by suction, and apply the correctly-sized mask with a C-E grip. Squeeze the self-inflating bag slowly over about one second to produce visible chest rise, deliberately avoiding the forceful or rapid squeezing that insufflates the stomach. [1]
The rate follows the context, and the numbers are the facts examiners test. For a child with a pulse but no or inadequate breathing — rescue breathing — give one breath every 2 to 3 seconds, about 20 to 30 breaths per minute. For a child in cardiac arrest with a single rescuer, give 30 compressions and then 2 breaths; with two rescuers, give 15 compressions and 2 breaths. Once an advanced airway is in place, deliver about 10 breaths per minute (one breath every 6 seconds) with continuous chest compressions at 100 to 120 per minute. Use 100 percent oxygen during active resuscitation and wean to a target saturation once return of spontaneous circulation is achieved. [1]
The first-minute airway and ventilation sequence
Open the airway: jaw thrust (or head tilt-chin lift if no trauma); position the infant head neutral
Suction any visible vomit, blood or secretions from the mouth and oropharynx
Apply the correctly-sized mask with a C-E grip and seal it to the face
Squeeze the bag slowly over about one second to produce visible bilateral chest rise
Set the rate: rescue breathing one breath every 2 to 3 seconds; CPR 30:2 or 15:2
If the chest does not rise, escalate: two-person technique, add an adjunct, then a supraglottic airway
Reassess heart rate, SpO2 and chest rise every 10 to 20 seconds and call for senior help
If one-person ventilation is failing, escalate immediately and in order: move to the two-person technique, add an oropharyngeal or nasopharyngeal airway, then reach for a supraglottic airway, and call for senior and intensive care help. The child who cannot be ventilated and oxygenated is the failed airway, and the algorithm for it should start from the first minute, not after a quiet deterioration. [11]
Management — Definitive & Stepwise
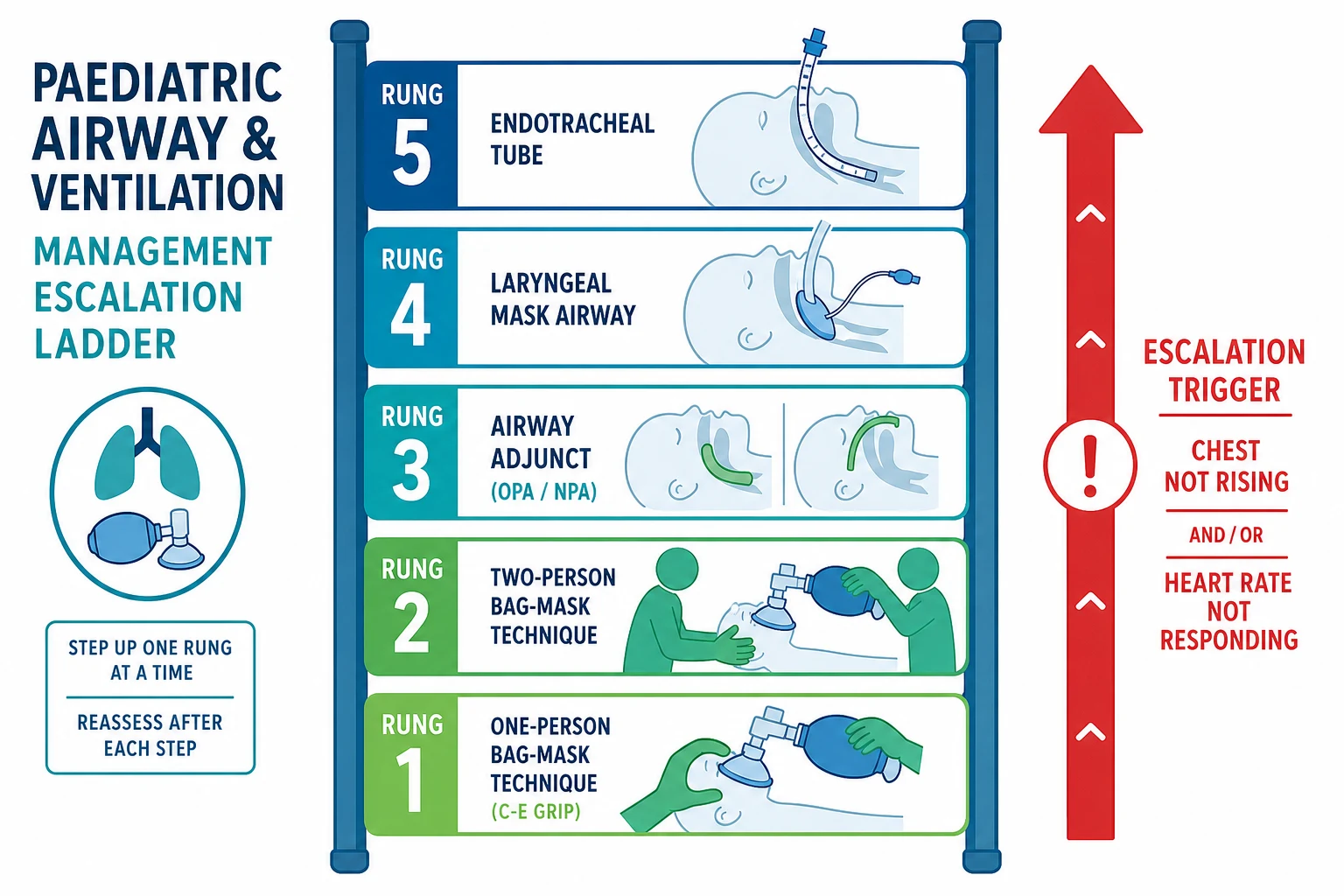
Ventilation escalates up a clear ladder, and you choose each rung by whether the chest is rising and the heart rate is responding. The first rung is one-person bag-mask: a C-E seal with one hand, squeeze with the other, correct for most children. The second rung is the two-person technique, and it is the single most effective improvement, so it should be reached early rather than late: one rescuer performs a two-handed jaw thrust and forms a tight mask seal with the thenar eminences while the second squeezes the bag. [10]
The third rung is the airway adjunct. An oropharyngeal airway, for the deeply unconscious child with no gag, is sized from the angle of the mouth to the angle of the jaw and inserted to follow the curve of the tongue; in the infant and small child it is passed directly along the curve rather than rotated 180 degrees, because the rotation of an adult technique can push the tongue back and worsen the obstruction. A nasopharyngeal airway, for the semi-conscious child with a gag, is sized from the nostril to the tragus and lubricated before gentle insertion, and it is contraindicated in suspected basilar skull fracture or a coagulopathy. [12]
[12]The fourth rung is the supraglottic airway, the laryngeal mask airway, and it is the rescue device when bag-mask ventilation fails or intubation is unsuccessful. The Cochrane review found the laryngeal mask as effective as bag-mask or intubation for neonatal resuscitation, and a randomised trial in Uganda showed that a laryngeal mask airway reduced the need for further resuscitation and was feasible where intubation skill was scarce, which together justify it as the bridge to a definitive tube. The fifth rung is endotracheal intubation by a skilled provider, followed by mechanical ventilation. [6]
Oxygen during bag-mask resuscitation
Dose
100 percent during active resuscitation and arrest; wean to a target SpO2 of 94 to 98 percent once return of spontaneous circulation is achieved. For the neonate, start with blended oxygen — 21 percent for term and late-preterm infants, 21 to 30 percent for the very preterm — and titrate to the pre-ductal saturation target.
At every rung, the trigger to escalate is the same: failure to achieve chest rise and a rising heart rate within seconds. A child who is not being ventilated is not buying time on the lower rungs; the rescuer climbs the ladder until the chest moves.
[10]Specific Subtypes & Scenarios
The neonate in the delivery room follows the neonatal resuscitation sequence and has its own device and numbers. Dry, warm, and stimulate, and assess tone, breathing and heart rate. If the infant is apnoeic or gasping, open the airway and ventilate with a T-piece resuscitator at a peak inspiratory pressure of about 20 to 25 cm of water, at 40 to 60 breaths per minute, starting with blended oxygen and titrating to the pre-ductal saturation target. The T-piece gives a controlled pressure and a consistent positive end-expiratory pressure that a self-inflating bag cannot, which is why it is the neonatal standard; a self-inflating bag remains the fallback where a gas source is absent. [2]
The infant with bronchiolitis or pneumonia who is tiring on the ward needs bag-mask ventilation as a bridge to high-flow nasal cannula or intubation. The technique is the same — slow squeeze, visible chest rise, a rate that keeps the saturation up — but the child is often easier to ventilate than the rescuer fears, because the problem is fatigue rather than obstruction. Gentle breaths avoid gastric insufflation in a child whose stomach is already full of secretions and milk. [1]
The trauma child needs a jaw thrust without head tilt and manual in-line stabilisation of the cervical spine, because head tilt-chin lift is unsafe when a cervical spine injury is possible. The mask and the rate are unchanged, but the airway manoeuvre and the team around the collar are different. The child with a dysmorphic or difficult airway — Pierre Robin sequence, Down syndrome — should have a two-person technique and a supraglottic airway ready from the start, because one-person ventilation is likely to fail and the early rescue saves time. [11]
The technology-dependent child with a tracheostomy who obstructs is managed by the tracheostomy algorithm: suction the tube, pass the spare tube, and if neither works, ventilate through the stoma with a paediatric mask before resorting to mouth ventilation. The family usually knows the child's airway and the spare tube better than anyone at the bedside, so involve them from the first breath. [10]
Why the chest is not rising — DOPE
Complications & Pitfalls
Gastric insufflation is the cardinal complication, and it follows directly from the physics of the squeeze. A forceful or too-rapid bag generates a high peak inspiratory pressure that overcomes the lower oesophageal sphincter and pushes air into the stomach; the distended stomach splints the diaphragm, reduces the tidal volume, and precipitates regurgitation and aspiration. The prevention is a slow, controlled squeeze over about one second and the smallest volume that moves the chest, and the neonatal evidence behind the corrective steps for mask ventilation reinforces that gentle, well-sealed breaths are the technique. [9]
Hypoventilation is the commonest error and the silent killer. It comes from a poor mask seal, a blocked airway, or an infant self-inflating bag too large for the child so the one-way valve does not open, and its sign is a chest that never rises while the rescuer believes they are ventilating. The fix is to watch the chest and to escalate the technique, not to squeeze harder. Eye trauma comes from a mask pressed onto the orbits, and barotrauma and volutrauma follow over-zealous ventilation, especially in the stiff-lung neonate. [11]
Cricoid pressure, once routine, is not recommended during paediatric cardiac arrest and remains contentious even during induction, because it can obstruct the airway of a child and there is no strong evidence of benefit. The largest pitfall of all is persisting with ineffective one-person ventilation when a two-person technique, an adjunct, or a supraglottic airway was available from the first minute. The rescuer who climbs the ladder the moment the chest stops rising is the one who keeps the child alive. [11]
Prognosis & Disposition
When the airway is opened and the chest rises promptly, the hypoxic bradycardic infant usually recovers within seconds, and the outlook is then that of the underlying illness. Competent bag-mask ventilation alone, even without intubation, sustains the great majority of children through a resuscitation, which is precisely why it is the skill that matters most — most children do not need a tube in the first minutes, they need a ventilator who can make the chest rise. [1]
Any child who has needed bag-mask ventilation belongs in a high-dependency or intensive care area with continuous pulse oximetry and capnography monitoring. Those who remain dependent on ventilation, who needed a supraglottic airway, or who failed to respond promptly need definitive airway management by a skilled provider and, often, retrieval to a tertiary centre. Children moved between hospitals must travel with staff able to ventilate and manage the airway in transit, because the safest place for a child to deteriorate is not the back of an ambulance without an airway-capable provider. [3]
The family must leave with a clear written safety-net, because a child who obstructed or hypoventilated once can do so again. They should know the warning signs that bring them back — colour change, abnormal breathing, drowsiness, poor feeding — and the plan for the next episode, written down so it survives the fear of the moment.
[3]Special Populations
Neonates and preterm infants are the population most at risk from over-ventilation. Use a T-piece resuscitator with a controlled peak inspiratory pressure and a consistent positive end-expiratory pressure, blended oxygen to a unit-set target saturation, and the gentlest breaths that move the chest, because excessive pressure and oxygen cause pneumothorax, lung injury and retinopathy of prematurity. The pre-ductal saturation, not the colour, is the target. [2]
Infants under one year combine every difficulty at once: the smallest face and the largest tongue, the most compliant chest, and the tiniest oxygen reserve. Reach the two-person technique and an oropharyngeal airway early in this group, hold the head neutral, and pre-oxygenate whenever a few seconds allow. Children with neurodisability or neuromuscular weakness have weak respiratory muscles and copious secretions, so they obstruct and hypoventilate readily, and the family usually knows the child's mask and airway routine better than anyone at the bedside. [10]
Technology-dependent children with a tracheostomy are managed through their stoma with the child's own airway plan to hand, the spare tube ready, and the family involved in every decision. Indigenous, remote and rural children across Australia and Aotearoa New Zealand sit furthest from intensive care, so the first responder's competence at bag-mask ventilation and airway adjuncts in the minutes before retrieval arrives is genuinely life-saving, and culturally safe, family-inclusive care with reliable aeromedical retrieval is part of equitable airway management. [1]
[3]Evidence, Guidelines & Regional Differences
International guidance converges on the same principles, and the recent evidence has hardened the points that used to be debated. The 2025 American Heart Association and American Academy of Pediatrics guidelines for paediatric and neonatal resuscitation, the 2021 European Resuscitation Council paediatric life support guideline, and the 2020 and 2022 International Liaison Committee on Resuscitation consensus statements teach the two-person technique, a ventilation rate of 20 to 30 breaths per minute for rescue breathing and about 10 per minute once an advanced airway is in place during arrest, 100 percent oxygen during active resuscitation weaned after return of circulation, and early use of a supraglottic airway when bag-mask fails. [4]
The evidence for the supraglottic airway is now mature. The Cochrane review found the laryngeal mask airway as effective as bag-mask ventilation or endotracheal intubation for neonatal resuscitation, and a randomised trial in Uganda showed the laryngeal mask reduced the need for further resuscitation where intubation was not available — together they justify the laryngeal mask as the rescue device of choice when bag-mask fails or intubation is unsuccessful, particularly where intubation skill is scarce. [7]
The neonatal device evidence favours the T-piece resuscitator, which delivers a more controlled peak pressure and a consistent positive end-expiratory pressure than a self-inflating bag, and the corrective-steps review for neonatal mask ventilation reinforces that mask seal, head position, and a slow gentle breath are the technique that works. [8]
Pejovic 2020 — Laryngeal Mask in Neonatal Resuscitation
Key finding
In a randomised trial of neonatal resuscitation in Uganda, a laryngeal mask airway reduced the need for further resuscitation compared with bag-mask ventilation alone, and was feasible where intubation skill was scarce.
Practice change
The laryngeal mask airway is a supported rescue device when bag-mask ventilation fails or intubation is not available, particularly in resource-limited settings.
Controversies remain around the routine use of cricoid pressure, the starting oxygen concentration in preterm resuscitation, and the exact role of capnography during mask ventilation. Regional differences are small in principle — ANZ follows ANZCOR and aligns with AHA and ERC, the UK follows the Resuscitation Council UK, Canada and the US follow their own societies — and they agree on rates, technique, and the supraglottic airway as rescue, while differing in operational detail. [5]
Exam Pearls
Difficult mask ventilation in a child — BONES
References
- [1]Joyner BL Jr, Dewan M, Bavare A, de Caen A, DiMaria K, Donofrio-Odmann J, et al Part 6: Pediatric Basic Life Support: 2025 American Heart Association and American Academy of Pediatrics Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2025.PMID 41122891
- [2]Lee HC, Strand ML, Finan E, Illuzzi J, Kamath-Rayne BD, Kapadia V, et al Part 5: Neonatal Resuscitation: 2025 American Heart Association and American Academy of Pediatrics Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2025.PMID 41122887
- [3]Van de Voorde P, Turner NM, Djakow J, de Lucas N, Martinez-Mejias A, Biarent D, et al European Resuscitation Council Guidelines 2021: Paediatric Life Support. Resuscitation, 2021.PMID 33773830
- [4]Wyckoff MH, Greif R, Morley PT, Ng KC, Olasveengen TM, Singletary EM, et al 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation, 2022.PMID 36325905
- [5]Maconochie IK, Aickin R, Hazinski MF, Atkins DL, Bingham R, Bittencourt Couto T, et al Pediatric Life Support 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Pediatrics, 2021.PMID 33087557
- [6]Grein AJ, Weiner GM Laryngeal mask airway versus bag-mask ventilation or endotracheal intubation for neonatal resuscitation. Cochrane Database Syst Rev, 2005.PMID 15846656
- [7]Pejovic NJ, Myrnerts Höök S, Byamugisha J, Alfvén T, Lubulwa C, Cavallin F, et al A Randomized Trial of Laryngeal Mask Airway in Neonatal Resuscitation. N Engl J Med, 2020.PMID 33252870
- [8]Hawkes CP, Ryan CA, Dempsey EM Comparison of the T-piece resuscitator with other neonatal manual ventilation devices: a qualitative review. Resuscitation, 2012.PMID 22227500
- [9]Gaertner VD, Mileder LP, Springer L, Wagner M, Dvorsky R, Rüegger CM, et al Corrective steps during neonatal mask ventilation - a narrative review of the evidence behind the MR SOPA acronym. Resuscitation Plus, 2026.PMID 41909182
- [10]Miller KA, Nagler J Advances in Emergent Airway Management in Pediatrics. Emerg Med Clin North Am, 2019.PMID 31262416
- [11]Miller KA, Goldman MP, Nagler J Management of the Difficult Airway. Pediatr Emerg Care, 2023.PMID 36790950
- [12]Nemeth M, Ernst M, Asendorf T, Richter J, von Gottberg P, Brandes IF, et al Working with estimation-formulas to predict nasopharyngeal airway insertion depth in children: Looking at magnetic resonance images - A prospective observational study (WEND:LI-Study). Resuscitation, 2021.PMID 34600970