Paeds · investigations-procedures-and-technology
Blood gas, electrolyte and acid-base interpretation
Also known as Blood gas analysis · Arterial blood gas · Capillary blood gas · Venous blood gas · Acid-base balance · Anion gap
A fellowship approach to blood gas, electrolyte and acid-base interpretation in children covering the five-step systematic method (pH, PaCO2, HCO3, compensation, anion gap), the normal paediatric arterial values of pH 7.35 to 7.45, PaCO2 35 to 45 mmHg and bicarbonate 22 to 26 mmol per litre, the anion gap as sodium minus chloride plus bicarbonate with a normal range of 8 to 12 mmol per litre, the compensation rules including Winter's formula of expected PaCO2 equals 1.5 times bicarbonate plus 8 plus or minus 2 for metabolic acidosis, the choice between arterial, venous and capillary samples with venous pH and bicarbonate closely matching arterial values, the high anion gap metabolic acidosis of diabetic ketoacidosis defined by pH below 7.3 and bicarbonate below 15, the hypochloraemic hypokalaemic metabolic alkalosis of pyloric stenosis, the dysnatraemias and their slow correction rates of no more than 8 to 10 mmol per litre per day, and the use of isotonic maintenance fluids to prevent hospital-acquired hyponatraemia.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a three-year-old brought in breathing fast and drowsy with the smell of ketones on the breath. The glucose is high, the gas shows a pH of seven point oh seven and a bicarbonate of six, and the anion gap is twenty-eight. The gas does not make the diagnosis of diabetic ketoacidosis on its own, but it is the single test that tells you how sick the child is, how hard the body is working to compensate, and how fast you must act. Interpretation is a skill the paediatrician uses in the resuscitation bay, the ward and the PICU, and it rests on a method that is the same every time. [6] [7]
A blood gas is a sample of whole blood analysed at the point of care or in the laboratory for pH, the partial pressures of oxygen and carbon dioxide, the bicarbonate concentration, the base excess, and often the electrolytes, glucose, lactate and haemoglobin on the same cartridge. The gas captures two things at once: how well the lungs move oxygen and carbon dioxide, and how well the kidneys and buffers hold the pH. Together they tell you about oxygenation, ventilation and the metabolic state in under a minute. [3] [4]
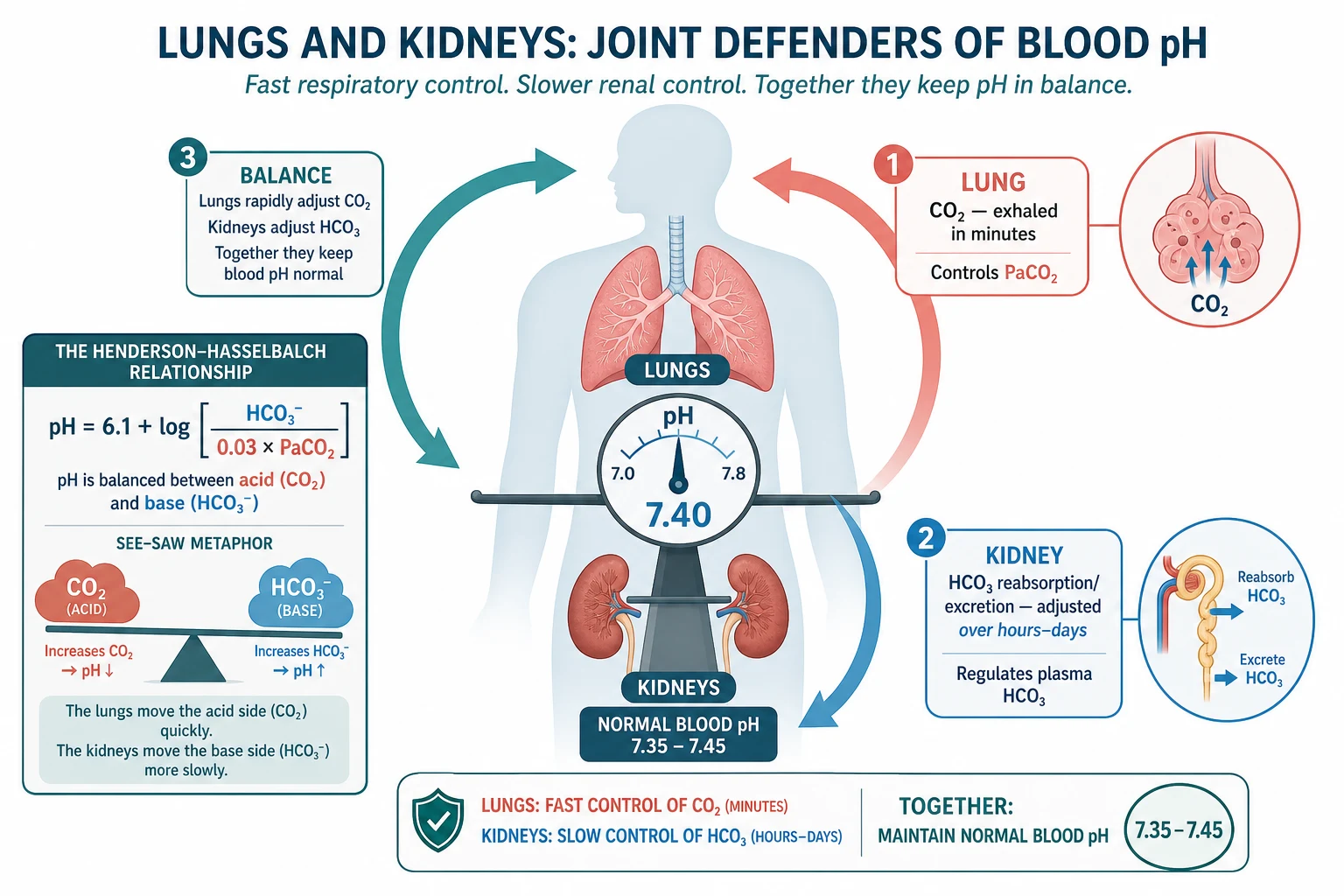
Acid-base balance is the defence of the hydrogen-ion concentration of the blood within the narrow range that lets enzymes work. The healthy arterial pH sits between 7.35 and 7.45, and the body holds it there by pairing a weak acid, carbonic acid from carbon dioxide, against its buffer bicarbonate. The Henderson-Hasselbalch relationship fixes the pH at the ratio of bicarbonate to dissolved carbon dioxide, so a change in either lung or kidney side of the ratio moves the pH. Disturbances are named for the side that drives them and for the direction of the pH. [2] [11]
Electrolytes travel with the gas because sodium, chloride, potassium and bicarbonate are the ions that determine the anion gap, the osmolality and the rhythm of the heart. A child who is acidotic is almost always also deranged in one or more electrolytes, and reading the two together is what turns a number on a printout into a treatable diagnosis. [1] [10]
Classification
Hold two classifications in mind at once: the acid-base disturbance the gas reveals, and the sample you took to reveal it. They interact, because the sample sets the limits of what you can claim. [4] [5]
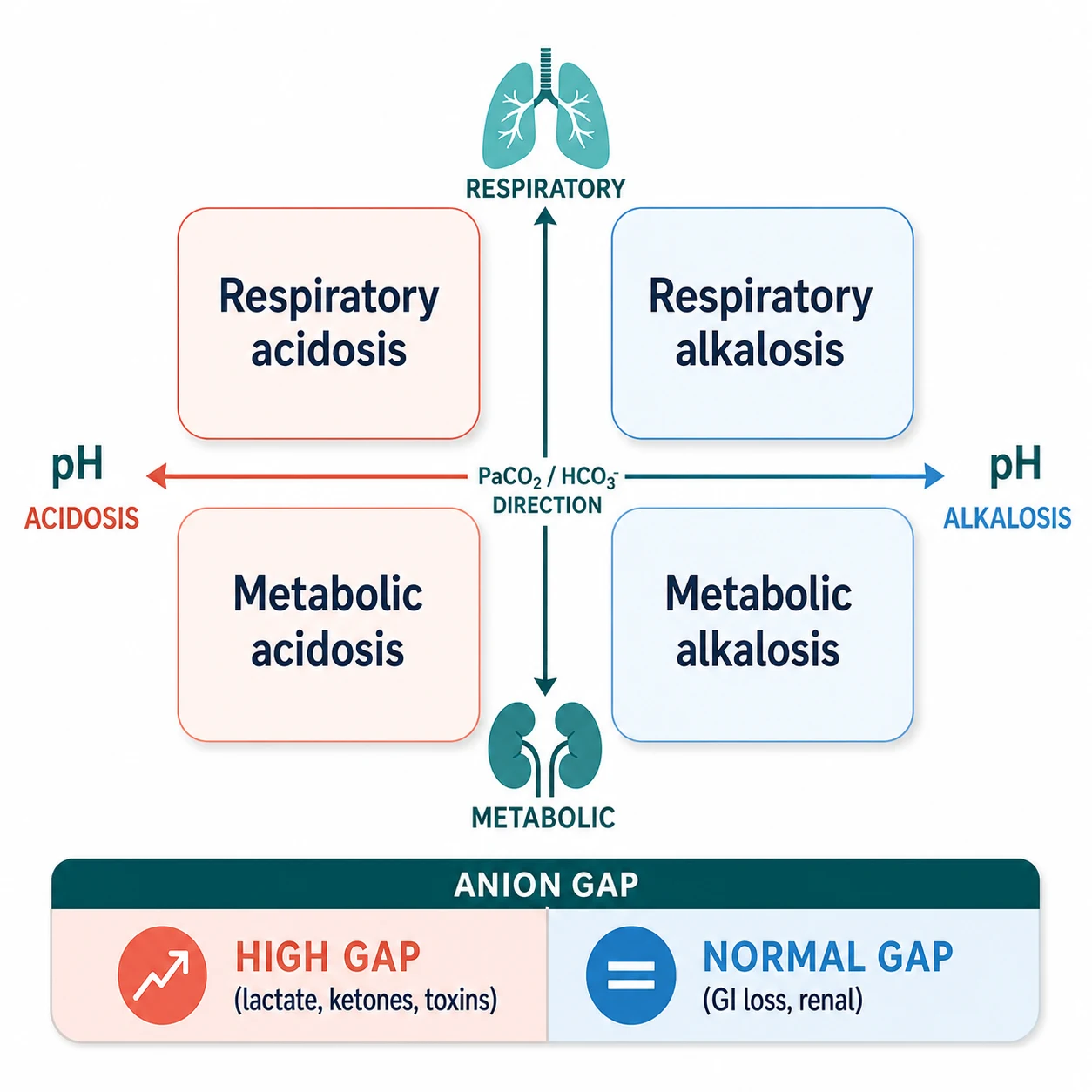
By disturbance, every acid-base problem splits first on the pH into acidosis (pH below 7.35) or alkalosis (pH above 7.45), and then on the driving side into respiratory or metabolic. A respiratory disturbance moves PaCO2 in the same direction as the pH fault: PaCO2 rises in respiratory acidosis and falls in respiratory alkalosis. A metabolic disturbance moves bicarbonate against the pH fault: bicarbonate falls in metabolic acidosis and rises in metabolic alkalosis. Mixed disturbances are common in the sick child, which is exactly why the compensation step matters. [11] [12]
By sample, three sources are in paediatric use, and each answers a slightly different question. The arterial sample is the gold standard: it measures PaO2 and the exact PaCO2, pH and bicarbonate, and it is the only sample that tells you about oxygenation. The venous sample, drawn from a central line or a free-flowing peripheral vein, gives a pH within about 0.03 of the arterial and a bicarbonate that tracks closely, with a PaCO2 that runs three to eight mmHg higher; it cannot assess oxygenation but it is excellent for following an acid-base trend. The capillary sample, taken from a warmed heel or finger prick, mirrors the arterial pH and bicarbonate and is the workhorse in the infant and young child, though its PaCO2 is a little higher and its oxygen value is unreliable. [4] [5]
Epidemiology & Risk Factors
Blood gas and electrolyte derangement is one of the commonest laboratory findings in acutely ill children, because almost any severe illness touches the lungs, the kidneys or the gut that hold the balance. The child in shock, the infant with bronchiolitis, the toddler with gastroenteritis, the new-onset diabetic and the PICU patient on a ventilator all generate gases, and the numbers drive fluid, insulin, ventilation and electrolyte decisions hour by hour. [3] [10]
The children at greatest risk of a dangerous derangement cluster around a few presentations. The child with diabetic ketoacidosis carries a high-gap metabolic acidosis and the risk of cerebral oedema, and it is the commonest endocrine emergency of childhood. The child with severe gastroenteritis loses chloride, potassium and bicarbonate through vomiting and diarrhoea and arrives with dehydration, a metabolic acidosis from hypoperfusion, and sometimes a hypernatraemia or hyponatraemia. The child with bronchiolitis or asthma retains carbon dioxide as exhaustion sets in, and the gas tells you when to escalate respiratory support. The post-operative and PICU child on balanced or unbalanced fluids drifts into dysnatraemia or hyperchloraemic acidosis if the fluid is not chosen with care. [6] [9]
Hospital-acquired hyponatraemia is the iatrogenic hazard that the modern fluid guidelines target. Hypotonic maintenance fluids, once standard, drive the sodium down in the child with non-osmotic antidiuretic hormone release, and the result can be seizures and death. The 2018 AAP guideline shifted maintenance fluids toward isotonic solutions for this reason, and a fellowship candidate must know why. [8] [9]
Pathophysiology
The body defends pH with a chemical buffer, the lung and the kidney, working on three timescales. The buffer system, bicarbonate paired with carbonic acid, works in seconds. The lung adjusts the carbon dioxide it excretes in minutes. The kidney adjusts the bicarbonate it reclaims and the acid it excretes over hours to days. Every disturbance you read on a gas is the net result of these three arms fighting each other. [2] [11]
Carbon dioxide is a volatile acid. The more the lung fails to clear it, the more carbonic acid forms and the pH falls, producing a respiratory acidosis. Conversely, the more a child hyperventilates — in pain, anxiety, sepsis or high altitude — the more carbon dioxide is blown off and the pH rises, producing a respiratory alkalosis. The metabolic side moves through the kidney. A fall in bicarbonate from a buffered acid, from gut loss or from a renal tubular fault produces a metabolic acidosis. A gain of bicarbonate, or a loss of hydrogen and chloride from vomiting, produces a metabolic alkalosis. [2] [4]
Compensation is the side that is not at fault trying to pull the pH back toward normal, and it is never complete. In a metabolic disturbance the lung does the fast work, so PaCO2 should fall in metabolic acidosis and rise in metabolic alkalosis. In a respiratory disturbance the kidney does the slow work, so bicarbonate should rise over hours in chronic respiratory acidosis and fall in chronic respiratory alkalosis. The compensation rules let you tell whether the response is appropriate, too much, or too little — and that is how you catch a mixed disorder. [11] [12]
The anion gap exists because the blood must stay electrically neutral. Sodium is the dominant cation, and chloride plus bicarbonate are the measured anions that balance most of it. The gap between them is the room left for the unmeasured anions — albumin, phosphate and the organic acids — and a normal gap runs from eight to twelve mmol per litre. When a new unmeasured acid appears, as lactate in shock, ketones in DKA, oxalate and glycolate in ethylene glycol poisoning, or sulphate in renal failure, the gap widens. The gap therefore sorts a metabolic acidosis into a search for a cause. [1] [6]
Electrolytes are inseparable from the gas because they are the ions the gap is built from, and because they carry their own danger. Sodium sets the osmolality and the risk of cerebral oedema or demyelination when it is corrected too fast. Potassium sets the cardiac rhythm, and both extremes stop the heart. Chloride, when it is given in excess in normal saline, can itself produce a hyperchloraemic metabolic acidosis that mimics the acidosis of shock — one of the reasons balanced fluids were introduced. [1] [2]
Clinical Presentation
The child who needs a gas is almost always sick enough that the gas explains a clinical sign you can already see. The presentation is the respiratory pattern, the perfusion and the consciousness, and the gas is the confirmation. [10] [12]
A child in metabolic acidosis breathes deeply and rapidly to blow off carbon dioxide: the Kussmaul pattern, seen at its most striking in DKA. The breath may carry the fruity smell of ketones. A child in respiratory acidosis from exhaustion or obstruction breathes shallowly and grows drowsy, and the PaCO2 climbs as the effort fails. A child in respiratory alkalosis from pain, anxiety or early sepsis hyperventilates and may complain of tingling fingers from a falling ionised calcium. A child in metabolic alkalosis from prolonged vomiting, classically the infant with pyloric stenosis, is dehydrated with a low chloride and potassium and a compensatory hypoventilation that is easy to miss. [6] [10]
Electrolyte derangement shows itself in the heart, the gut and the brain. Hyperkalaemia above six brings peaked T waves, a widened QRS and the risk of a sine-wave arrest; hypokalaemia brings muscle weakness, ileus and U waves. Hyponatraemia presents with headache, vomiting and seizures when it falls fast; hypernatraemia presents with irritability, a high-pitched cry and seizures, and it signals severe free-water loss. The gas and the electrolytes together, read with these signs, point to the cause and the urgency. [1] [8]
Differential Diagnosis
The differential is the differential of the acid-base disturbance, and it is built from the anion gap. A high-gap metabolic acidosis asks four questions, summed up as the mnemonic KULT: ketones (DKA, starvation), uraemia (renal failure), lactate (shock, sepsis, hypoxia), and toxins (methanol, ethylene glycol, salicylates). A normal-gap metabolic acidosis is loss of bicarbonate or gain of hydrogen through gut or kidney — diarrhoea, renal tubular acidosis, and the hyperchloraemic acidosis of excess saline. [6] [12]
A metabolic alkalosis splits into chloride-responsive and chloride-resistant. The chloride-responsive group loses hydrogen and chloride from the stomach (vomiting, pyloric stenosis, nasogastric suction) or the kidney after diuretics, and it corrects when chloride and fluid are given back. The chloride-resistant group holds onto chloride and is driven by mineralocorticoid excess, and it is rare in children outside of hyperaldosteronism and Cushing syndrome. A respiratory acidosis is anything that under-ventilates — obstruction, exhaustion, neuromuscular weakness, opiates — and a respiratory alkalosis is anything that over-ventilates — pain, anxiety, fever, early sepsis, hypoxia, salicylates. [4] [11]
KULT — the four causes of a high anion gap
Clinical & Bedside Assessment
The bedside assessment decides whether the gas is an emergency or a trend, and it happens before the numbers come back. Look at the work of breathing, the perfusion, the consciousness and the rhythm, and let those signs tell you how hard to push the interpretation. [10] [12]
Begin with the airway and breathing. Count the respiratory rate, watch for recession and accessory-muscle use, listen for stridor or wheeze, and feel for the exhaustion that precedes collapse. A rising respiratory rate with a falling effort is the sign that the child is tiring, and a gas taken at that moment shows a climbing PaCO2 even when the child looks as if it is breathing hard. Assess the circulation: capillary refill, pulse volume, skin temperature and blood pressure. A cold, mottled child with a prolonged refill is in shock, and the gas will show a metabolic acidosis from a rising lactate. [10]
Check the conscious level with the AVPU scale or Glasgow coma scale, because a falling conscious level in an acidotic child points to decompensation or cerebral oedema. Run an ECG when the potassium is high or low, because the rhythm is the danger and it can change between the gas and the laboratory result. Take a focused history for polyuria, polydipsia and weight loss in the new diabetic; for vomiting, diarrhoea and intake in the dehydrated child; and for ingestion in the toddler with an unexplained high-gap acidosis. [1] [6]
Investigations
The gas is the first investigation, and the electrolytes, glucose and lactate usually travel with it on the same cartridge. The modern point-of-care analyser reports pH, PaCO2, PaO2, bicarbonate, base excess, sodium, potassium, chloride, ionised calcium, glucose, lactate and haemoglobin from a few drops of blood, and a study of paediatric patients showed close agreement between the cartridge and the central laboratory for haemoglobin and the electrolytes when the sample is handled well. [3] [11]
Choose the sample for the question. Use an arterial sample when oxygenation or an exact PaCO2 matters — the critically ill child, the child on a ventilator, the child with severe respiratory disease. Use a venous sample to follow the acid-base trend in DKA, shock or gastroenteritis, accepting that venous pH runs about 0.03 lower and venous PaCO2 three to eight mmHg higher than arterial. Use a capillary sample from a warmed heel or finger in the infant and young child, where it mirrors arterial pH and bicarbonate but cannot judge oxygenation. The AARC guideline stresses a warmed, well-perfused puncture site and a free-flowing, heparinised sample, because a poorly taken capillary gas underestimates pH and overestimates PaCO2. [4] [5]
Always read the gas with the concurrent electrolytes, because the anion gap, the corrected sodium and the potassium all depend on them. Calculate the anion gap as sodium minus chloride plus bicarbonate. Correct the sodium for hyperglycaemia, because glucose draws water into the vascular space and dilutes the measured sodium: the corrected sodium is the measured sodium plus one point six mmol per litre for every 5.5 mmol per litre of glucose above normal. Send a lactate to quantify the high-gap acidosis of shock, and a beta-hydroxybutyrate when ketones are in doubt. [1] [8]
Management — Resuscitation
The first response to a deranged gas is resuscitation of the child, not correction of the number. An acidotic child is usually a child in shock, in respiratory failure, or in diabetic ketoacidosis, and the gas tells you which arm of resuscitation to lead with. [6] [10]
For the child in shock with a lactic metabolic acidosis, restore the circulation with boluses of isotonic crystalloid, ten to twenty mL per kilogram, reassessing after each, and treat the cause — sepsis, haemorrhage, cardiogenic failure. The lactate clears as perfusion returns, and the pH follows it. Do not give bicarbonate to a child whose acidosis is from shock alone, because the bicarbonate generates carbon dioxide that the lung must clear and it does not fix the perfusion. [1] [12]
For the child in respiratory failure with a respiratory acidosis, support the ventilation — high-flow nasal cannula, continuous positive airway pressure, or intubation — and clear the obstruction. The PaCO2 falls as ventilation improves, and the pH recovers within minutes. For the child in diabetic ketoacidosis, follow the structured fluid and insulin protocol: an initial ten to twenty mL per kilogram of isotonic saline to restore perfusion, then a weight-based insulin infusion at nought point oh five to nought point one unit per kilogram per hour, and fluids that avoid rapid shifts. The bicarbonate falls in DKA because it is consumed by ketoacids, and it recovers as insulin shuts off ketogenesis. [7] [12]
For the hyperkalaemic child with ECG change, stabilise the myocardium first. Give calcium gluconate nought point five mL per kilogram of the ten per cent solution to protect the heart, then drive potassium into the cell with insulin and glucose, with nebulised salbutamol, and with sodium bicarbonate if the child is acidotic. Remove potassium with the gut or the kidney once the rhythm is safe. [1]
Management — Definitive & Stepwise
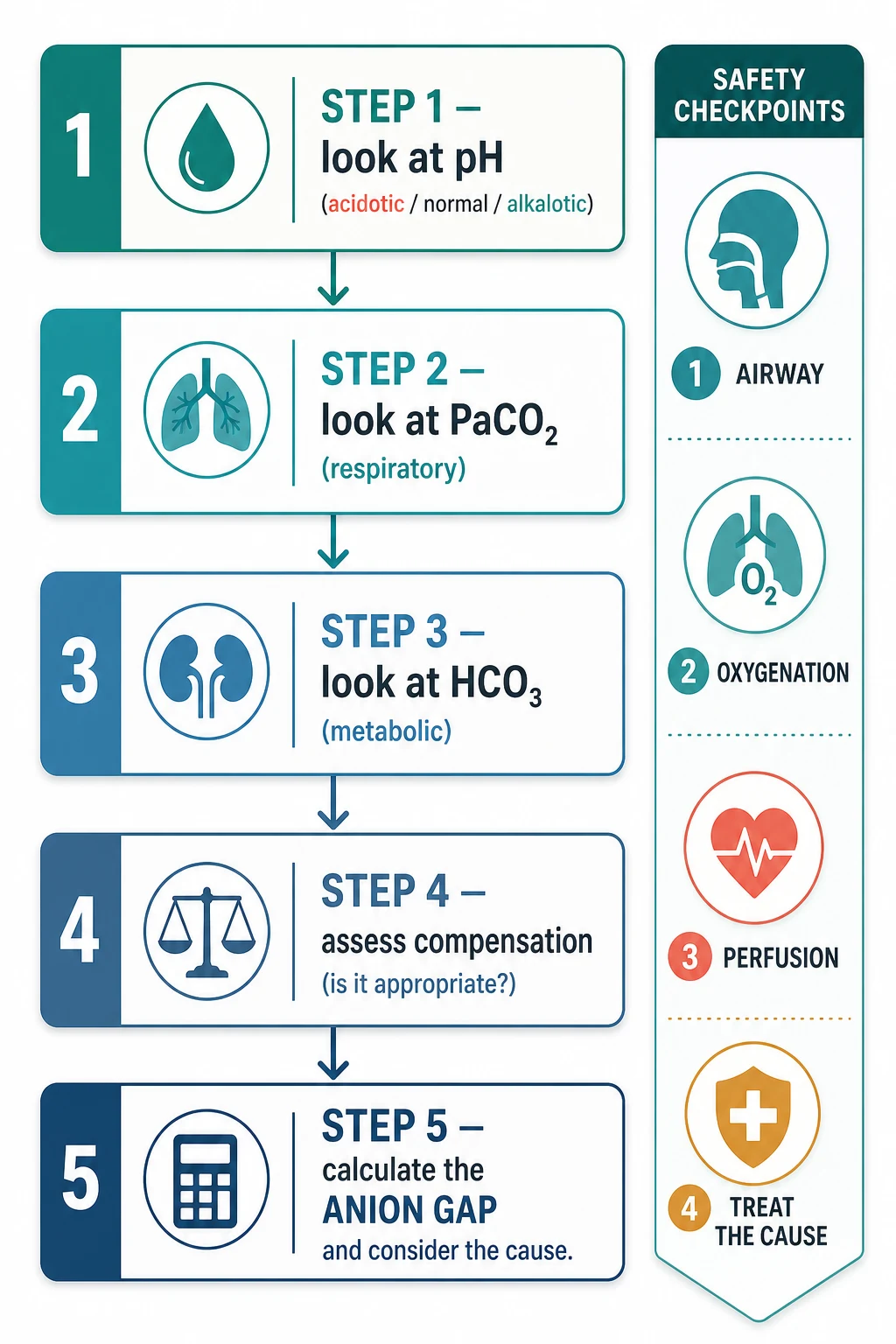
The definitive management is the five-step method applied to the whole picture, and it is the structure that earns marks in any viva. Walk through it the same way every time, on every gas, in this order. [4] [11]
The five-step systematic gas interpretation
1
2
3
4
5
Once the disturbance is named and the gap is calculated, treat the cause. A high-gap acidosis from sepsis needs antibiotics and fluids; from DKA needs insulin and structured fluids; from a toxin needs the specific antidote or clearance. A normal-gap acidosis from diarrhoea needs fluid and chloride replacement; from renal tubular acidosis needs bicarbonate and potassium. A metabolic alkalosis from vomiting needs chloride, potassium and fluid. A respiratory disturbance needs the airway, the ventilator or the cause of the drive. [6] [12]
The compensation rules at a glance
Specific Subtypes & Scenarios
Five scenarios recur in fellowship vivas and OSCE stations, and each turns on a single decision. The first is the child with diabetic ketoacidosis. The gas shows a high-gap metabolic acidosis with a pH below 7.3 and a bicarbonate below 15, and the glucose is above 11 mmol per litre. Winter's formula tells you whether the child is compensating; a PaCO2 higher than expected means the child is tiring and may need ventilatory support. The danger is cerebral oedema from rapid fluid shifts, and the management is structured fluids, a low-dose insulin infusion, and a watch on the sodium and the conscious level. Bicarbonate is reserved for the child with a pH below 7 and haemodynamic collapse. [7] [12]
The second is the infant with pyloric stenosis. Weeks of projectile vomiting lose hydrogen and chloride, and the kidney wastes potassium and bicarbonate to keep the sodium, so the gas shows a hypochloraemic, hypokalaemic metabolic alkalosis with a compensatory hypoventilation. The correction is chloride, potassium and fluid before anything else; the alkalosis resolves as the chloride returns. A candidate who misses the potassium or corrects too fast loses marks. [1] [10]
The third is the child with severe gastroenteritis and dehydration. The gas shows a metabolic acidosis from hypoperfusion and bicarbonate loss through the gut, and the electrolytes show the sodium picture — isonatraemic, hyponatraemic or hypernatraemic. The fluid plan follows the sodium: isotonic fluid for shock, then rehydration over twenty-four to forty-eight hours, and never a correction of more than ten to twelve mmol per litre per day in the hypernatraemic child. [9] [10]
The fourth is the child in respiratory failure. The gas shows a respiratory acidosis with a climbing PaCO2 as the effort fails, and the decision is whether to escalate respiratory support. A respiratory acidosis that does not correct with non-invasive support is an indication for intubation, and the gas taken after intubation confirms the PaCO2 is falling. The same child who hyperventilates from anxiety or early sepsis shows a respiratory alkalosis, and the falling PaCO2 is the early warning that something is wrong. [4] [11]
The fifth is the child with a mixed disorder. A septic child with DKA who is also hyperventilating from pain shows a metabolic acidosis with a respiratory alkalosis; a child with vomiting and diarrhoea shows a metabolic alkalosis and a metabolic acidosis together. The delta ratio catches these: a ratio above two means a metabolic alkalosis is layered on the high-gap acidosis, and a ratio below nought point eight means a normal-gap acidosis rides alongside. The five-step method is what finds them. [1] [11]
Complications & Pitfalls
The complications of interpretation are the mistakes that change management for the worse, and the candidate must name each one and how to avoid it. [4] [11]
Treating the number, not the child, is the commonest error. A normal-looking pH can hide a mixed acidosis and alkalosis, and a child who looks well can have a gas that is about to decompensate. Always read the gas with the clinical picture, and act on the child first. Using a venous or capillary gas to judge oxygenation is the second: only an arterial sample measures PaO2, and weaning oxygen on a capillary oxygen value risks hypoxia. Use venous and capillary gas for the acid-base trend, and reserve the arterial stick for oxygenation. [4] [5]
Correcting sodium too fast, in either direction, is the error that causes cerebral harm. In hyponatraemia a rise of more than eight to ten mmol per litre in twenty-four hours causes osmotic demyelination; in hypernatraemia a fall of more than ten to twelve causes cerebral oedema. Measure the sodium often and slow the correction when it moves too fast. Giving bicarbonate for a number is the fourth error: in DKA and lactic acidosis bicarbonate lowers the cerebrospinal fluid pH and generates carbon dioxide, and it is reserved for the child with a pH below seven and haemodynamic collapse. [6] [8]
Misreading compensation as a second disorder, or missing a second disorder because compensation looked adequate, is the interpretive pitfall that the five-step method exists to prevent. Always apply Winter's formula in metabolic acidosis, and use the delta ratio when the gap is high. Forgetting the corrected sodium in hyperglycaemia is the last: the measured sodium is falsely low, and the corrected value is what guides fluid choice in DKA. [1] [11]
Prognosis & Disposition
The prognosis of a deranged blood gas is the prognosis of the cause, because the gas is a window on the illness and not the illness itself. A high-gap acidosis from septic shock resolves as the shock is treated; the acidosis of DKA resolves over hours as insulin shuts off ketogenesis; the alkalosis of pyloric stenosis resolves as chloride is replaced. The gas that fails to improve, or that worsens despite treatment, is the signal that the cause is not controlled. [6] [12]
Disposition follows the severity and the trend. A child with a pH below 7.2, a potassium above 6.5 with ECG change, a sodium outside 120 to 155, or a gas that is worsening needs a high-acuity setting — PICU, HDU or retrieval. A child with a resolving trend and a stable cause can step down to the ward with serial gases. The family should have a clear safety-net for worsening breathing, drowsiness or reduced urine output, because the child who looks well can decompensate quickly. [1] [10]
Special Populations
The neonate needs capillary or arterial gas read against neonatal ranges, because the neonatal PaCO2 is a little higher and the bicarbonate is a little lower than the older child. The preterm infant on the ventilator is at risk of both permissive hypercapnia and a rapid alkalosis from over-ventilation, and the gas is titrated to protect the immature lung and brain. [5]
The infant with bronchiolitis needs a capillary gas to track the carbon dioxide as the work of breathing rises, because a climbing PaCO2 is the sign that non-invasive support is failing. The child with a chronic respiratory or metabolic disorder — cystic fibrosis, chronic renal failure, a metabolic condition — may live with a compensated gas that looks abnormal to the untrained eye, and the candidate must distinguish the chronic baseline from the acute change. [4] [11]
The critically ill and PICU child needs arterial and venous gases read together, often hourly, to titrate ventilation, fluids and inotropes. The child with diabetic ketoacidosis needs the gas and the electrolytes read together at every step, with the corrected sodium guiding the fluid plan and the conscious level driving the fear of cerebral oedema. [7]
For Aboriginal, Torres Strait Islander, Māori, and rural or remote children, the point-of-care gas is the only test available in many settings, and the staff who take and read it must be trained and supported. A clear escalation pathway, with the numbers that demand retrieval and the place of the child in the system, closes the distance between the remote gas and the intensive-care bed. [10]
Evidence, Guidelines & Regional Differences
The guidelines are strikingly concordant across regions. The Royal Children's Hospital Melbourne, the American Academy of Pediatrics, the ISPAD consensus and the major paediatric intensive-care societies all teach the five-step systematic method, all hold the normal arterial pH at 7.35 to 7.45 and the bicarbonate at 22 to 26 mmol per litre, and all reserve the arterial sample for oxygenation. [4] [9]
The strongest recent shift in practice is the move to isotonic maintenance fluids. The 2018 AAP clinical practice guideline recommended isotonic solutions with potassium chloride for maintenance in children aged 28 days to 18 years, because hypotonic fluids cause hospital-acquired hyponatraemia in the child with non-osmotic antidiuretic hormone release. The same logic underpins the use of balanced crystalloids over normal saline to avoid a hyperchloraemic acidosis, because the chloride in saline is itself an acid load. [2] [9]
The evidence on point-of-care reliability is reassuring. A 2023 study of paediatric patients showed close agreement between the cartridge and the central laboratory for haemoglobin and the electrolytes, and a 2021 validation of an automated interpretation tool showed that a rules-based engine can read a gas as well as a trained clinician — though the tool does not replace the clinical judgement that decides what to do with the number. [3] [11]
[2] [9]The genuine controversies are narrow. Whether balanced crystalloids improve outcomes over normal saline in all paediatric resuscitation is still being refined; the rate of sodium correction in the dysnatraemias is agreed in principle but varies in detail; and the role of automated interpretation tools alongside the clinician is unsettled. The principle that the child is treated and not the number is not controversial. [1] [11]
Exam Pearls
A fellowship candidate should leave the examiner with a small set of sharp, sourced facts. Memorise these and you will answer any question on this topic. [4] [11]
Five steps in fixed order: pH to name the primary disturbance, PaCO2 for the respiratory side, bicarbonate for the metabolic side, a compensation check, and the anion gap. The normal arterial pH is 7.35 to 7.45, PaCO2 is 35 to 45 mmHg, bicarbonate is 22 to 26 mmol per litre, and base excess is minus 2 to plus 2. [11]
The anion gap is sodium minus chloride plus bicarbonate, normal 8 to 12 mmol per litre. A high gap means an unmeasured acid — KULT: ketones, uraemia, lactate, toxins. The delta ratio of the change in anion gap over the change in bicarbonate catches a second metabolic disorder: above two a metabolic alkalosis rides alongside, below nought point eight a normal-gap acidosis rides alongside. [6]
Winter's formula for metabolic acidosis: expected PaCO2 equals 1.5 times the bicarbonate plus 8, within plus or minus 2. A measured PaCO2 outside that band means a respiratory disorder is layered on top. Corrected sodium in hyperglycaemia: measured sodium plus 1.6 mmol per litre for every 5.5 mmol per litre of glucose above normal. [1]
DKA is a high-gap metabolic acidosis with pH below 7.3, bicarbonate below 15, glucose above 11 mmol per litre. Treat with structured isotonic fluid and insulin 0.05 to 0.1 unit per kilogram per hour; the danger is cerebral oedema. Pyloric stenosis is a hypochloraemic, hypokalaemic metabolic alkalosis. Sodium correction must not exceed 8 to 10 mmol per litre in twenty-four hours. Bicarbonate is reserved for a pH below 7 with haemodynamic collapse. Arterial gas for oxygenation; venous and capillary for the trend. [6] [7]
References
- [1]Zieg J, Ghose S, Raina R Electrolyte disorders related emergencies in children BMC Nephrology, 2024.PMID 39215244
- [2]Hoorn EJ Intravenous fluids: balancing solutions Journal of Nephrology, 2017.PMID 27900717
- [3]Konuksever D, Yucel SP, Bölük O, et al Compatibility levels between blood gas analysis and central laboratory hemoglobin and electrolyte tests in pediatric patients: A single-center experience Paediatric Anaesthesia, 2023.PMID 36178754
- [4]Sheikholeslami D, Dyson AE, Villarreal EG, et al Venous blood gases in pediatric patients: a lost art? Minerva Pediatrics, 2022.PMID 34530585
- [5]Evans DL, Volsko TA, Capellari E, et al AARC Clinical Practice Guidelines: Capillary Blood Gas Sampling for Neonatal and Pediatric Patients Respiratory Care, 2022.PMID 36002161
- [6]Dhatariya KK, Glaser NS, Codner E, et al Diabetic ketoacidosis Nature Reviews Disease Primers, 2020.PMID 32409703
- [7]Wolfsdorf JI, Glaser N, Agus M, et al ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic ketoacidosis and the hyperglycemic hyperosmolar state Pediatric Diabetes, 2018.PMID 29900641
- [8]Saba L, Hanna C, Creo AL Updates in hyponatremia and hypernatremia Current Opinion in Pediatrics, 2024.PMID 38174733
- [9]Feld LG, Neuspiel DR, Foster BA, et al Clinical Practice Guideline: Maintenance Intravenous Fluids in Children Pediatrics, 2018.PMID 30478247
- [10]Powers KS Dehydration: Isonatremic, Hyponatremic, and Hypernatremic Recognition and Management Pediatrics in Review, 2015.PMID 26133303
- [11]Rodríguez-Villar S, Poza-Hernández P, Freigang S, et al Automatic real-time analysis and interpretation of arterial blood gas sample for Point-of-care testing: Clinical validation PLoS One, 2021.PMID 33690724
- [12]Calimag APP, Chlebek S, Lerma EV, et al Diabetic ketoacidosis Disease-a-Month, 2023.PMID 35577617