Paeds · investigations-procedures-and-technology
Bone-marrow aspiration and biopsy principles
Also known as Bone marrow aspirate · Trephine biopsy · Bone marrow examination · Jamshidi needle procedure · Marrow sampling
A fellowship approach to bone marrow aspiration and biopsy in children covering the principle that aspirate and trephine are two complementary samples taken at one sitting (the aspirate for cells in suspension — morphology, flow cytometry, cytogenetics, molecular and culture; the trephine core for cellularity, architecture and infiltration), the posterior superior iliac spine as the standard paediatric site and the reasons the sternum is avoided in young children, the manual Jamshidi and Salah needles and the powered OnControl drill, the stepwise procedure of positioning and landmark, asepsis and local anaesthetic infiltration to the periosteum with lidocaine one per cent three milligrams per kilogram plain or seven milligrams per kilogram with adrenaline, aspirating the first pull for morphology and cytogenetics then taking a trephine core from a new track, the meaning of a dry tap and the need for a trephine, the complications of pain bleeding infection and retropneumoperitoneum, and the staging and risk-stratification decisions that rest on a correctly handled first pull.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a six-year-old referred after a routine count shows a haemoglobin of sixty, a platelet count of twenty, and blasts on the film. The diagnosis is in the marrow, not the blood, and the act that names the disease is the bone marrow examination. For the paediatrician the principle is simple to hold and easy to forget under pressure: the aspirate and the trephine answer different questions, and you take both at the same sitting so the child is not brought back twice. [2] [3]
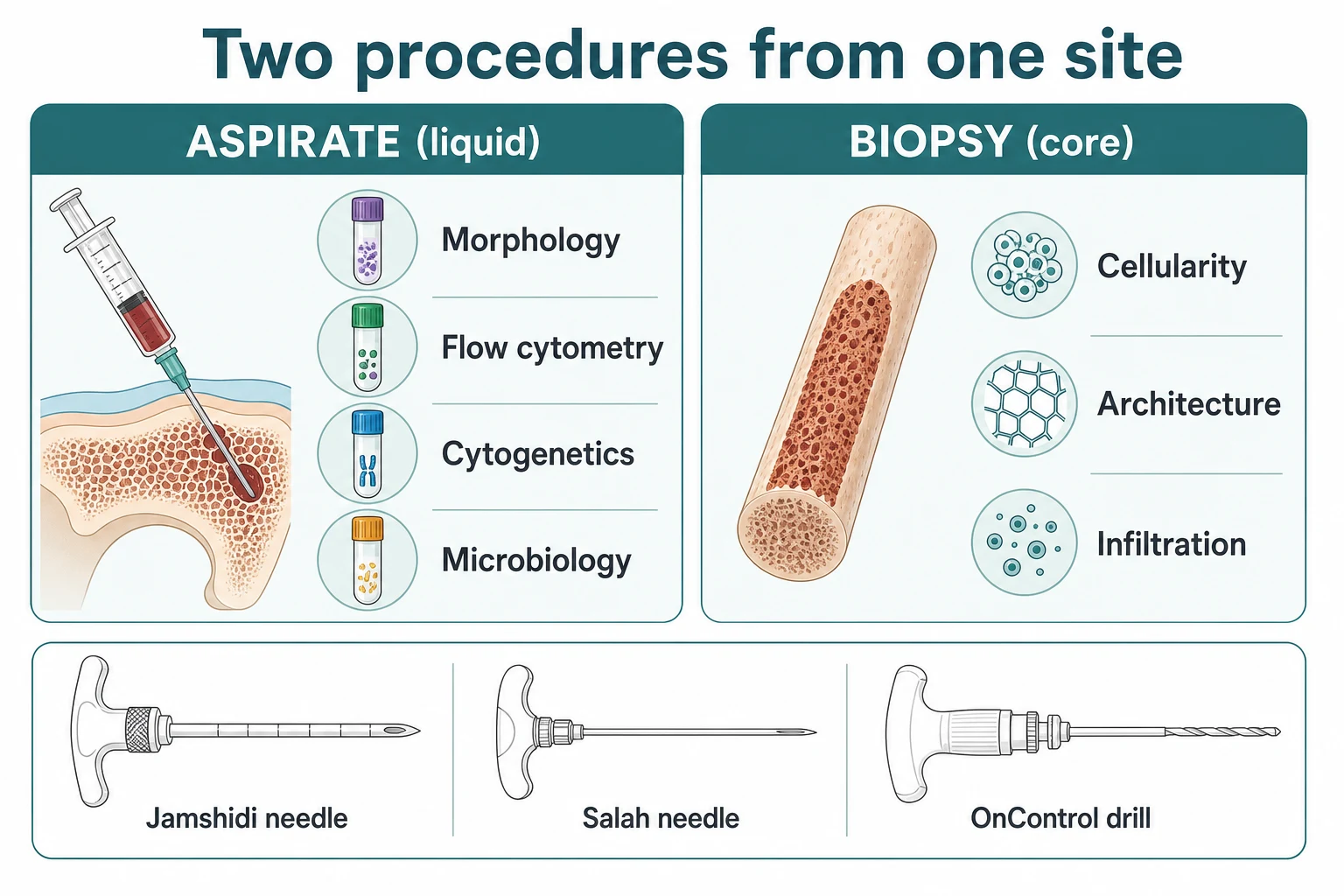
Bone marrow aspiration withdraws liquid marrow from the medullary cavity. It holds the cells in suspension, so it is the sample for anything that needs intact or dividing cells: smear morphology, immunophenotyping by flow cytometry, cytogenetics, molecular studies, and culture. Bone marrow trephine biopsy removes a core of bone that still contains the marrow in its native arrangement, so it is the only sample that shows overall cellularity, the pattern of infiltration, fibrosis, granulomas, and metastatic tumour. [1] [2]
The reason a fellowship candidate must hold both at once is that each sample fails where the other succeeds. A leukaemia may be diagnostic on aspirate flow cytometry but invisible on a trephine core; a severely aplastic marrow may look deceptively normal on a liquid aspirate taken from a surviving pocket, and only the trephine reveals the empty, fatty marrow that defines aplastic anaemia. Sending one without the other is the commonest avoidable error. [1] [10]
Classification
Hold two classifications in mind at once: the sample you take, and the device you take it with. They interact, because the device governs the quality of the core and the comfort of the child. [1] [6]
By sample, the aspirate and the trephine split cleanly along the question each answers. The aspirate is a liquid, and it answers questions about cells as individuals: what they are (morphology), what surface markers they carry (flow cytometry), what chromosomes and genes they hold (cytogenetics and molecular), and whether any organism grows (culture). The trephine is a solid core, and it answers questions about the marrow as a tissue: how full or empty it is (cellularity), whether it is scarred (fibrosis), whether it is invaded (metastases, lymphoma), and whether it carries granulomas or storage material. [2] [3]
By device, three families are in paediatric use. The manual aspiration needle (Salah or Jamshidi type) is twisted gently through the cortex by hand; it remains the workhorse for the aspirate in children of all ages. The manual trephine needle (Jamshidi or Islam) captures a core by hand-advancing over the cortex. The powered drill (OnControl) drives a needle with a stylet through the cortex under motor control; it is faster, more controllable, and less fatiguing, and a 2019 comparison showed its trephine cores were of comparable or better quality than the manual Jamshidi. The drill is used increasingly in older children and adolescents. [6]
Epidemiology & Risk Factors
Bone marrow examination is one of the commonest invasive diagnostic procedures in paediatric haematology and oncology. Nearly every child with suspected acute leukaemia, with unexplained marrow failure, or undergoing staging of a solid tumour or lymphoma will have one, and the procedure is safe in trained hands with major complication rates well under one per cent. [1] [10]
The children who need it cluster around a few diagnoses. The child with unexplained cytopenias — a falling haemoglobin, a platelet count drifting down, a neutrophil count that will not recover — heads the list. So does the child with blasts or abnormal cells on the blood film, the child being staged for neuroblastoma, lymphoma, rhabdomyosarcoma or Ewing sarcoma, the immunocompromised child with fever and a mystery, and the child with hepatosplenomegaly and a storage or histiocytic disorder. [2] [5]
Risk concentrates in two directions. Bleeding risk sits with the thrombocytopenic or coagulopathic child whose marrow has failed or whose chemotherapy has suppressed the count. Infection risk sits with the neutropenic child and the child with indwelling lines. Both are predictable and both are managed before the needle goes in, not after. [10] [11]
Newly suspected leukaemia
Blasts on film, cytopenias
- Aspirate is the diagnostic test: morphology, flow, cytogenetics, molecular
- First pull reserved for morphology and cytogenetics — it sets the risk group
- Trephine supports cellularity and infiltration pattern
- Platelet and clotting support before the trephine if cytopenic
Pancytopenia, cause unknown
Aplastic versus infiltrative
- Trephine is decisive: cellularity under 25 per cent defines severe aplastic anaemia
- Aspirate alone is misleading — surviving marrow pockets look normal
- Add cytogenetics and a diepoxybutane breakage test for Fanconi
- Dry tap is common in fibrosis — take the trephine
Solid tumour or lymphoma staging
Neuroblastoma, rhabdomyosarcoma, Ewing
- Bilateral trephines — a unilateral biopsy can miss focal marrow disease
- Aspirate for morphology plus trephine for architecture
- Send for flow cytometry in lymphoma
- Coordinate with imaging and the staging protocol
Critically ill child in PICU
HLH, overwhelming infection
- Bedside procedure with full monitoring and an anaesthetist
- Aspirate for haemophagocytosis and culture
- Trephine for infiltration and cellularity
- Balance diagnostic urgency against bleeding risk
Pathophysiology
The marrow is the factory of the blood. Haematopoietic stem cells sit in the medullary cavity of the flat and long bones and produce the red cells, white cells and platelets that circulate, so a sample of the marrow reads the factory floor directly. When the blood count fails, the marrow shows why: a clonal expansion of leukaemic blasts, an empty fatty marrow of aplasia, a fibrous scar, or a metastatic deposit. [1] [2]
The aspirate and the trephine read that factory in two different ways. The aspirate is drawn from the medullary sinusoids and holds the cells as a suspension — ideal for any assay that needs the cells intact or dividing. The trephine core keeps the marrow in its native architecture, so it is the only sample that shows how full the factory is and how the cells are arranged. [2] [3]
One physiological fact governs everything about sample handling: the first pull is the only pull that is not diluted by peripheral blood. As soon as the cortex is breached, venous blood mixes with the marrow, and every later pull is progressively haemodiluted. A paediatric ALL study showed that the way the aspirate is taken changes the measured blast percentage and may shift the therapy stratification, which is the reason the first one to two millilitres is reserved for morphology and cytogenetics and the later pulls go to flow, molecular and culture. [4]
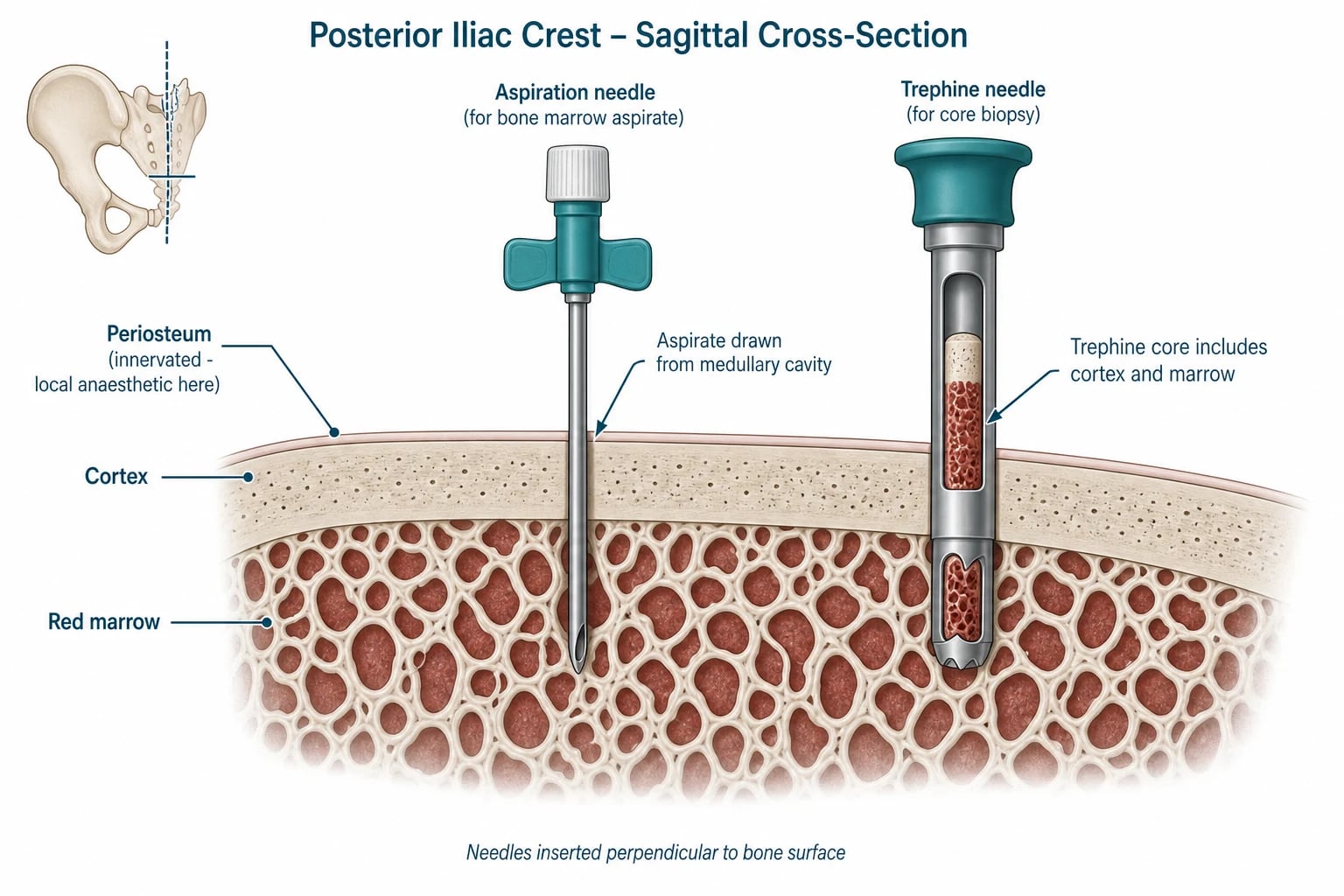
A second fact governs pain. The periosteum and the marrow cavity are richly innervated, so the procedure is genuinely painful and restraint alone is not acceptable. The skin, the subcutaneous tissue and the periosteum must each be infiltrated with local anaesthetic, and the child is given procedural sedation on top. The combination is what makes the examination humane as well as diagnostic. [7] [8]
Clinical Presentation
A child rarely presents asking for a bone marrow examination. The presentation is the abnormal count or film that points to the marrow, and the procedure is the next step the paediatrician takes. The triggers fall into a small number of recognisable patterns. [2] [3]
The commonest is the unexplained cytopenia: a haemoglobin that has fallen, a platelet count drifting down, or a neutrophil count that will not recover, alone or together as a pancytopenia. Close behind is the abnormal film — blasts, nucleated red cells, or bizarre forms that declare a leukaemia or a myelodysplasia and demand a confirmatory marrow. The third is staging: the child with a newly diagnosed solid tumour or lymphoma whose protocol requires a marrow sample to complete the staging and set the treatment intensity. [4] [5]
The child may also arrive through the back door. The dry tap — a needle in the right place from which no marrow can be aspirated — is itself a clinical sign. It points to marrow fibrosis, a marrow packed so full of cells that none will aspirate (as in some acute leukaemias), or a technical error, and it converts the trephine from a supporting sample into the diagnostic one. [1] [10]
Differential Diagnosis
The differential here is not of the procedure but of the reason for it. The candidate should hold two: the differential of the indication, and the differential of a failed sample. [2]
The differential of pancytopenia splits into four families that a marrow examination separates. Marrow failure — acquired aplastic anaemia and the inherited marrow failure syndromes — gives an empty, fatty trephine. Marrow infiltration — acute leukaemia, myelodysplasia, storage disease — gives a hypercellular marrow overrun by a single clone or a storage material. Nutritional and megaloblastic causes give a hypercellular megaloblastic picture. Peripheral consumption or sequestration — hypersplenism, haemolysis, immune destruction — leaves the marrow normal or reactive. The trephine and the aspirate, read together, place the child in one of these four boxes. [1] [2]
The differential of a failed sample is procedural, and it carries its own corrective action. A dry tap points to fibrosis or a packed marrow; the action is a trephine. A haemodiluted aspirate points to a late pull; the action is to send the first pull for morphology. A crushed or fragmented trephine points to technique; the action is a properly advanced Jamshidi or the powered drill. A core too short to assess cellularity points to an inadequate length; the action is a second core at least one to one and a half centimetres long. [3] [6]
Clinical & Bedside Assessment
The bedside assessment happens before the needle is inserted, and it decides whether the procedure is safe to do now. Confirm the indication, read the count and the clotting, examine the child, and choose the site by palpation rather than by eye. [1] [3]
Confirm the indication in one sentence and write it on the consent. Review the full blood count and coagulation screen and check a group and hold when the child is cytopenic. Examine for hepatosplenomegaly and lymphadenopathy, because a massively enlarged spleen or a mediastinal mass changes both the diagnosis and the sedation plan. Decide whether the trephine is needed at all today or whether an aspirate alone will answer the question, because the trephine is the part that bleeds. [2] [10]
The site is chosen by palpation. Run your fingers along the iliac crest to the firm prominence of the posterior superior iliac spine, and mark the point one to two centimetres below and lateral to it, where the bone is broadest and flattest. That point sits safely away from the sacroiliac joint, the sciatic notch, and any pelvic or abdominal structure. The anterior superior iliac crest is an alternative in the larger child; the sternum is avoided in young children because the thin cortex admits the needle into the mediastinum. [1] [2]
Site and sample order
Investigations
The investigations are of two kinds: the tests done before the procedure, and the handling of the samples taken during it. Both matter, because a mishandled sample wastes the procedure and the child's sedation. [3]
Before the needle, send a full blood count, coagulation screen and group and hold. Read the film again and review any peripheral flow cytometry, because a peripheral flow that is already diagnostic of acute leukaemia may change what the marrow is taken for. Decide on platelet and clotting-factor support from the count and the INR. [2] [11]
During the procedure, the aspirate is divided at the bedside. Make immediate smears from the first pull and send them for morphology; aliquot later pulls into EDTA for flow cytometry, heparin for cytogenetics and molecular testing, and a culture bottle when infection is suspected. The trephine core is handled differently: take touch imprints for rapid cytology, then fix the core immediately in formalin for decalcification and histology. No imaging is required before a standard posterior iliac procedure; ultrasound or CT guidance is reserved for a difficult or repeat site, an obese child, or an anterior approach. [1] [3]
Post-procedure, observe the puncture site and the child's vital signs for bleeding and for recovery from sedation. Check a count only if bleeding is suspected. The laboratory's report comes back over days to weeks depending on the assay — morphology within hours, flow within a day, cytogenetics over one to two weeks — so set the family's expectation and arrange a clear follow-up. [2] [9]
Management — Resuscitation
The resuscitation of a bone marrow procedure is preparation and safety, not an emergency drill. Before the needle is inserted, the consent, the fasting status, the monitoring, the site, the available blood-product support, and the sample-handling plan must all be in place. [1] [9]
Pain control is twofold and both arms are required. Local anaesthetic is infiltrated into the skin, the subcutaneous tissue and the periosteum — the layer that actually hurts — using lidocaine one per cent at three milligrams per kilogram plain or seven milligrams per kilogram with adrenaline, waiting for onset before advancing the needle. Procedural sedation is added on top: a ketamine–midazolam regimen, or an alfentanil–remifentanil–midazolam combination under monitored sedation, both shown to be safe and effective in children undergoing marrow procedures. Sedation is given by trained staff with full monitoring and a reversal agent to hand. [7] [8]
Lidocaine 1 per cent (local infiltration to the periosteum)
Dose
3 mg per kilogram plain (without adrenaline); 7 mg per kilogram with adrenaline
For the child who is critically ill or profoundly thrombocytopenic, give a platelet transfusion before the trephine and have blood ready. Have the sedation-reversal agents — flumazenil and naloxone — drawn up and to hand, and run the procedure where resuscitation drugs and equipment are immediately available. If bleeding occurs at the site, apply firm sustained pressure, elevate, and recheck the count and clotting; bleeding that will not settle is a reason to look for a deeper vessel injury and to involve haematology and surgery. [10] [11]
Management — Definitive & Stepwise
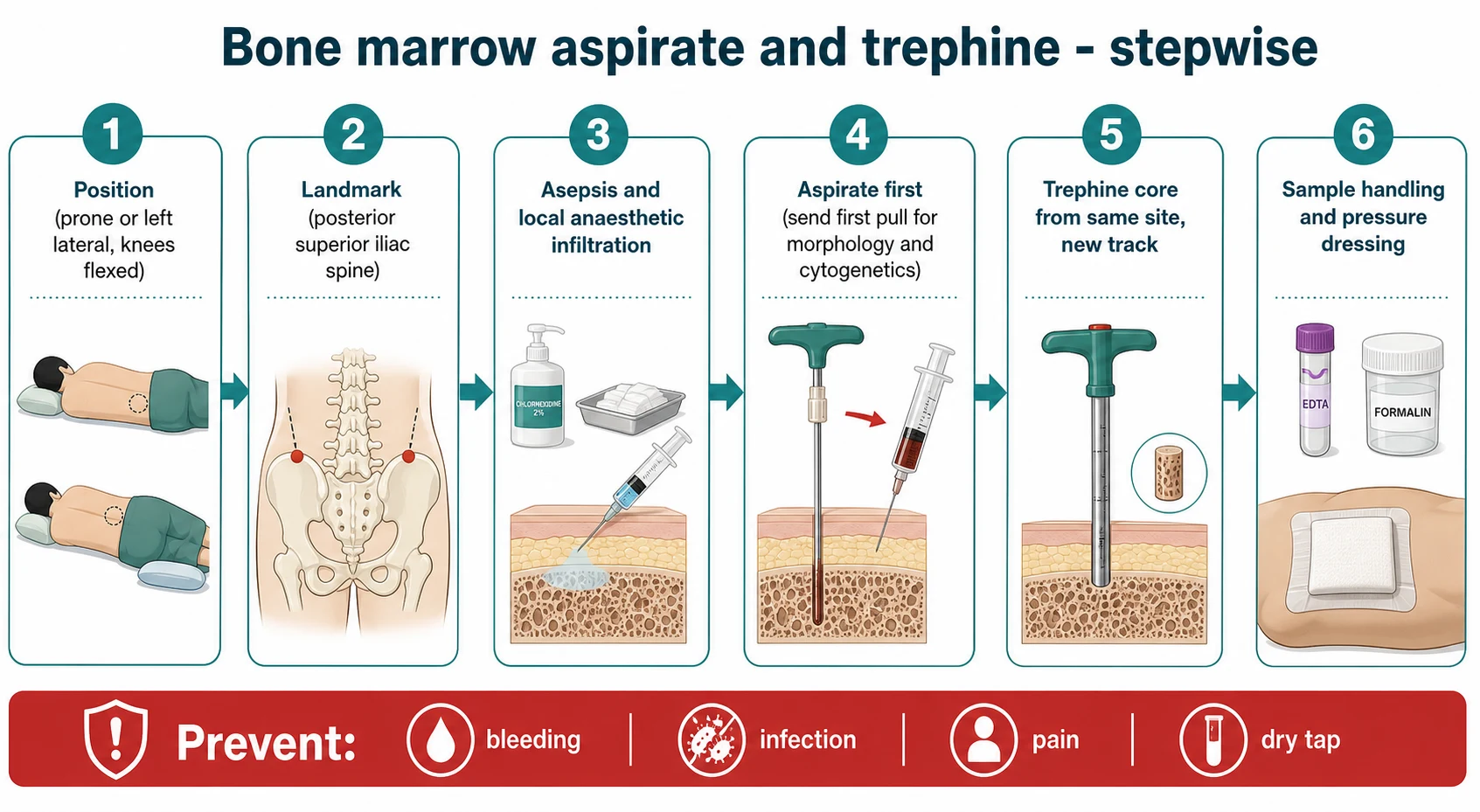
Once the preparation is done, the procedure itself runs in six ordered steps. Run them the same way every time, so that nothing about the sample-handling is left to the moment. [1] [2]
The aspirate-and-trephine procedure, in order
1 · Consent and preparation
Explain the procedure, the risks (pain, bleeding, infection, dry tap) and the sedation plan. Confirm nil-by-mouth status and attach monitoring. Check the count and clotting and give blood-product support if needed.
2 · Position and landmark
Prone or left lateral with the knees flexed to expose the posterior superior iliac spine. Mark one to two centimetres below and lateral to the PSIS on the broadest, flattest part of the bone.
3 · Asepsis and local anaesthetic
Sterile skin preparation and draping. Raise a skin wheal and infiltrate lidocaine one per cent down to and onto the periosteum (3 mg per kg plain, 7 mg per kg with adrenaline). Wait for onset.
4 · Aspirate first
Make a small skin stab. Advance the aspiration needle through the cortex with a gentle twisting motion until a give is felt. Confirm position, aspirate the first 0.5 to 2 mL, and make immediate bedside smears.
5 · Trephine core
Through the same skin puncture but a slightly different track, advance the trephine needle. Capture a core at least 1 to 1.5 cm long. Take touch imprints, then fix the core immediately in formalin.
6 · Sample handling and aftercare
Label and dispatch all aspirate aliquots (EDTA, heparin, culture) with a clear request. Apply firm pressure then a sterile pressure dressing. Observe the child and the site, document the procedure and the samples, and review before discharge.
A few technique points separate a diagnostic sample from a wasted one. Aspirate before the trephine, and from the same site, because a trephine taken first disrupts the marrow and dilutes the aspirate. Reserve the first pull for morphology and cytogenetics — it is the only pull not haemodiluted, and it is the pull that drives the leukaemia risk group. Take the trephine from a slightly different track through the same skin puncture, so the core is not fragmented by the aspirate hole. And fix the core immediately, because delay degrades the architecture the trephine exists to show. [4] [6]
| Question | Aspirate (liquid) | Trephine (core) |
|---|---|---|
| Cell identity — what is it? | Yes (morphology, flow cytometry) | Limited (histology) |
| Chromosomes and genes | Yes (cytogenetics, molecular) | No (unless decalcified special studies) |
| Overall cellularity | Misleading — surviving pockets look normal | Yes — the decisive sample |
| Fibrosis, granulomas, metastases | Often missed | Yes — architecture preserved |
| Microbiology (culture) | Yes — aspirate into culture bottle | Limited |
[1] [2] Both samples are taken at the same sitting so the child is not brought back; the aspirate is taken first because the trephine disrupts and dilutes the marrow.
Specific Subtypes & Scenarios
Four scenarios recur in fellowship vivas and OSCE stations, and each turns on a single decision. The first is the child with newly suspected acute leukaemia. The marrow aspirate with morphology, flow cytometry and cytogenetics is the diagnostic test and the basis of risk stratification, and the technique of the first pull matters: a haemodiluted pull changes the measured blast percentage and may shift the assigned risk group. Take the first pull cleanly, send it for morphology and cytogenetics, and let the later pulls go to flow and molecular. [4]
The second is the child with aplastic anaemia or an inherited marrow failure syndrome. Here the trephine is the decisive test, because cellularity under twenty-five per cent defines severe aplastic anaemia and a liquid aspirate taken from a surviving pocket can look deceptively normal. A generous trephine, read with the aspirate cytogenetics and a diepoxybutane breakage test for Fanconi anaemia, is what places the child in the right diagnostic and treatment box. [1] [2]
The third is the child being staged for a solid tumour or lymphoma. A unilateral trephine can miss focal marrow disease, so the staging protocol calls for bilateral trephines. The aspirate is sent for morphology and, in lymphoma, for flow cytometry, and the trephines show the pattern of infiltration. Missing a marrow deposit understages the tumour and undertreats the child, which is why bilateral sampling is the standard. [5]
The fourth is the dry tap. A needle in the right place from which no marrow can be aspirated is not a failed procedure — it is a sign. It points to marrow fibrosis, a marrow so packed with cells that none will aspirate, or a technical error, and the correct response is a trephine biopsy. The trephine, read with the clinical picture, shows the fibrosis or the packed marrow that explains the dry tap and often delivers the diagnosis the aspirate could not. [1] [10]
Complications & Pitfalls
Complications are uncommon when the procedure is done well, and the candidate must be able to name and prevent each one, because pain and bleeding are directly under the operator's control. [1] [10]
Pain is the commonest complication and the most preventable. The periosteum is innervated, and a child held down without adequate local anaesthetic and sedation is harmed as well as frightened. The treatment is local anaesthetic infiltrated to the periosteum plus procedural sedation; restraint alone is not acceptable practice. [7] [8]
Bleeding is more likely after a trephine than after an aspirate, and it concentrates in the thrombocytopenic and coagulopathic child. A 2017 review of CT-guided biopsies in thrombocytopenic patients confirmed that the procedure can be done safely when the count and clotting are corrected, which is why most centres transfuse platelets to keep the count above twenty to fifty for a trephine, and above fifty when the child is also coagulopathic. Firm pressure and site observation catch the rest. [11]
Infection — cellulitis, osteomyelitis, septic arthritis — is rare with sterile technique, but the risk rises with neutropenia and indwelling lines. Retropneumoperitoneum and injury to pelvic or abdominal structures are rare but serious, the result of over-penetration at the posterior iliac crest; they are prevented by a correct perpendicular angle and by stopping the moment the cortex gives way. The dry tap and the inadequate sample are procedural complications with their own corrective action: a trephine, a clean first pull, and a core long enough to read. [10]
Prognosis & Disposition
The procedure itself has an excellent prognosis. Most children go home the same day once sedation has recovered and the site is dry, and the puncture site heals quickly. The outcome of the illness is driven by the underlying diagnosis — leukaemia, aplastic anaemia, metastatic disease — and not by the procedure, but the marrow examination changes the outcome by securing the correct diagnosis and the correct risk group. [1] [2]
Disposition is straightforward. Observe the child until sedation has worn off, document the procedure and every sample dispatched, and arrange a clear plan for follow-up of the result. Give the family a safety-net: bleeding that will not stop, a fever, or worsening pain at the site in the days after the procedure all demand urgent review for haematoma, infection, or a deeper injury. [9] [10]
A child who bleeds persistently, who becomes febrile, or whose pain worsens after discharge needs to come back. The marrow examination is a diagnostic act with a small but real procedural risk, and the safety-net is what keeps that risk from becoming harm. [10] [11]
Special Populations
The infant and small child need a shorter needle, a gentle technique, and sedation that assumes no cooperation. The posterior superior iliac spine remains the site, and the procedure is done under full monitoring with staff trained in paediatric sedation, because restraint alone is neither safe nor acceptable. [7] [8]
The adolescent brings consent and autonomy to the forefront. The powered OnControl drill may be used and is well tolerated in the larger adolescent, and the conversation about a painful, intimate procedure must include privacy, a chaperone, and a genuine assent. The critically ill child in the PICU may need a marrow examination to diagnose haemophagocytic lymphohistiocytosis or an overwhelming infection, and the procedure is done at the bedside with full monitoring, an anaesthetist, and the support of a pathologist. [6] [9]
The thrombocytopenic or coagulopathic child needs blood-product cover before the trephine, and the question of whether a trephine is needed at all today should be asked honestly — an aspirate alone is safer when the architecture is not essential. The immunocompromised and oncology child need strict asepsis, a culture sent from the aspirate when infection is in the differential, and a balance struck between the diagnostic need and the risk of bacteraemia. [10] [11]
For Aboriginal, Torres Strait Islander, Māori, and rural or remote children, the procedure should be arranged in a centre with paediatric sedation and a laboratory that can handle the samples, because a marrow taken and handled poorly in a remote setting delays diagnosis rather than advancing it. Distance, family logistics, and the coordination of retrieval are part of the plan, and a fellowship candidate should frame the procedure as an act that closes a diagnostic gap rather than a technical exercise. [1]
Evidence, Guidelines & Regional Differences
The guidelines are strikingly concordant across regions. The Royal Children's Hospital Melbourne, the British Committee for Standards in Haematology, and the major paediatric oncology groups in North America all place the posterior superior iliac spine as the standard site and avoid the sternum in young children, and all require local anaesthetic to the periosteum plus procedural sedation with monitoring. [1] [2]
The strongest recent device evidence is a 2019 comparison of the powered OnControl drill against the manual Jamshidi, which found the drill's trephine cores were of comparable or better quality with less operator fatigue. The drill is used increasingly in older children and adolescents, while the manual needle remains the workhorse in infants and small children. [6]
The evidence on technique is equally pointed. A 2011 paediatric ALL study showed that the way the aspirate is taken changes the measured blast percentage and may shift the therapy stratification, which is the empirical basis for reserving the first pull for morphology and cytogenetics. A 2017 review of CT-guided biopsies in thrombocytopenic patients confirmed the procedure can be done safely when the count and clotting are corrected, supporting the practice of platelet cover before a trephine. [4] [11]
[1] [9]The genuine controversies are narrow. Whether peripheral flow cytometry can replace a diagnostic marrow in some leukaemias is unsettled; whether sedation should be nurse-, haematologist- or anaesthetist-led varies by centre; and the role of routine bilateral trephines in solid-tumour staging is settled in favour of bilateral sampling but varies in practice. The platelet threshold for a trephine is not universal, but most centres transfuse to keep the count above twenty to fifty, and above fifty when the child is coagulopathic. [4] [11]
Exam Pearls
A fellowship candidate should leave the examiner with a small set of sharp, sourced facts. Memorise these and you will answer any question on this topic. [1] [2]
Two samples, one site. The aspirate is for cells in suspension — morphology, flow, cytogenetics, molecular, culture — and the trephine core is for cellularity, architecture and infiltration. Send the first pull for morphology and cytogenetics, because it is the only pull not diluted by peripheral blood, and it is the pull that drives the leukaemia risk group. [4]
The site is the posterior superior iliac spine, one to two centimetres below and lateral to the spine, and the sternum is avoided in young children because the thin cortex admits the needle into the mediastinum. Infiltrate local anaesthetic to the periosteum with lidocaine one per cent, three milligrams per kilogram plain or seven milligrams per kilogram with adrenaline, and add procedural sedation. [7] [8]
A dry tap is not a failed procedure — it points to fibrosis or a packed marrow, and the correct response is a trephine. Severe aplastic anaemia is defined on the trephine (cellularity under twenty-five per cent), not the aspirate. Take bilateral trephines when staging a solid tumour or lymphoma, because a unilateral biopsy can miss focal marrow disease. The complications to name are pain, bleeding, infection, the dry tap, and rarely retropneumoperitoneum from over-penetration, and the powered OnControl drill gives comparable or better trephine quality than the manual Jamshidi with less operator fatigue. [6] [10]
References
- [1]Bhaskar N Bone Marrow Aspiration and Biopsy in Critical Pediatric Patients: A Pathologist's Perspective Cureus, 2021.PMID 34589333
- [2]Riley RS, Hogan TF, Pavot DR, et al A pathologist's perspective on bone marrow aspiration and biopsy: I. Performing a bone marrow examination Journal of Clinical Laboratory Analysis, 2004.PMID 15065211
- [3]Trewhitt KG Bone marrow aspiration and biopsy: collection and interpretation Oncology Nursing Forum, 2001.PMID 11683311
- [4]Helgestad J, Rosthøj S, Johansen P, et al Bone marrow aspiration technique may have an impact on therapy stratification in children with acute lymphoblastic leukaemia Pediatric Blood and Cancer, 2011.PMID 21360660
- [5]Valdés-Sánchez M, Nava-Ocampo AA, Palacios-González RV, et al Diagnosis of bone marrow metastases in children with solid tumors and lymphomas. Aspiration, or unilateral or bilateral biopsy? Archives of Medical Research, 2000.PMID 10767482
- [6]Forwood KM, Lee E, Crispin PJ Comparison of the bone marrow trephine sample quality between OnControl drill system and the Jamshidi needle International Journal of Laboratory Hematology, 2019.PMID 30779423
- [7]Kato Y, Maeda M, Aoki Y, et al Pain management during bone marrow aspiration and biopsy in pediatric cancer patients Pediatrics International, 2014.PMID 24417881
- [8]Antmen B, Saşmaz I, Birbiçer H, et al Safe and effective sedation and analgesia for bone marrow aspiration procedures in children with alfentanil, remifentanil and combinations with midazolam Paediatric Anaesthesia, 2005.PMID 15725319
- [9]Aslam SL, Haque A, Jamil MT, et al Safety and Efficacy of Procedural Sedation and Analgesia in Pediatric Oncology Patients Cureus, 2020.PMID 32351822
- [10]Bain BJ Bone marrow biopsy morbidity: review of 2003 Journal of Clinical Pathology, 2005.PMID 15790706
- [11]Liu B, Limback J, Kendall M, et al Safety of CT-Guided Bone Marrow Biopsy in Thrombocytopenic Patients: A Retrospective Review Journal of Vascular and Interventional Radiology, 2017.PMID 29042170