Paeds · investigations-procedures-and-technology
Central venous and arterial access in children
Also known as Paediatric central line insertion · Central venous catheterisation in children · Paediatric arterial line · Ultrasound-guided vascular access in children
A fellowship approach to central venous and arterial access in children: choose the site by indication and bleeding risk, use ultrasound to identify the target vessel and its companion artery, run the Seldinger sequence (needle, guidewire, dilator, catheter), aim the central catheter tip at the cavoatrial junction, and prevent the complications of arterial puncture, pneumothorax, haematoma, thrombosis and central line-associated bloodstream infection with a full sterile insertion bundle and a daily review of line necessity.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A 3-year-old in septic shock needs reliable access to run adrenaline and draw frequent blood gases. A peripheral cannula will not deliver concentrated vasoactives safely, and repeated attempts only burn her veins. The decision to place a central or arterial line is the decision to give a sick child a stable bridge for the next hours to weeks, and the next few minutes — choosing the site, finding the vessel with ultrasound, and running the Seldinger sequence without injuring the artery or dropping a pneumothorax — are where the line is made safe or harmful. This page teaches the whole procedure: the sites, the technique, the sizing, and what to do when it goes wrong. [1] [8]
Seldinger in six words
Overview & Definition
Imagine you must put a large-bore line into a central vein of a sick child, or an arterial line to watch her blood pressure beat by beat. The veins are small, they roll and collapse under a probe, and an artery lies beside every central vein you want. Central venous and arterial access is the set of techniques built to place these lines safely despite those obstacles. A central venous access device is any catheter whose tip ends in a great vein near the heart — the cavoatrial junction — so that irritant, concentrated, or vasoactive infusions are diluted in a high-flow vessel rather than burning a small peripheral vein. An arterial line is a cannula placed in a systemic artery to transduce continuous pressure and allow frequent blood-gas sampling. [1] [8]
The defining principle of modern paediatric access is ultrasound. The international evidence-based recommendations on ultrasound-guided vascular access, and the Cochrane reviews that support them, moved paediatric central cannulation from a landmark-and-hope technique to one in which the operator sees the vessel, confirms it is a vein by its compressibility and non-pulsatile flow, and watches the needle enter it. Lamperti and colleagues framed ultrasound guidance as the standard of care, and that framing is the lens through which the whole procedure is now taught and examined. [1] [2]
The key idea a candidate must hold is the compressibility and the artery. In an elective adult line a landmark technique sometimes works; in a child the vessels are small enough that feeling for a pulse and guessing the vein underneath it is a gamble. Ultrasound answers two questions before the needle moves: is the target vessel present and patent, and where does the artery lie relative to it. Every decision that follows — site, approach, the response to bright blood — flows from those two answers. [4]
Classification
Sort paediatric access by what is being put where and for how long, because that drives both the site and the device. [7] [8]
A central line is first sorted by its intended duration and whether it is tunnelled. A non-tunnelled acute central venous catheter is placed at the bedside for the sick child who needs vasoactive drugs, concentrated infusions, or reliable access for days to a week or two. A tunnelled catheter (such as a Hickman or Broviac line) is surgically tunnelled under the skin for the oncology or intestinal-failure child who needs months of chemotherapy or parenteral nutrition. A totally implantable port sits under the skin and is accessed through the skin with a needle, suiting the child who needs intermittent long-term access and wants to swim and live normally between treatments. A peripherally inserted central catheter (PICC) is threaded from an arm vein to the cavoatrial junction and offers a less invasive central option for intermediate-duration therapy. The choice among them is driven by the duration of therapy, the irritancy of the infusate, and the child's lifestyle. [7]
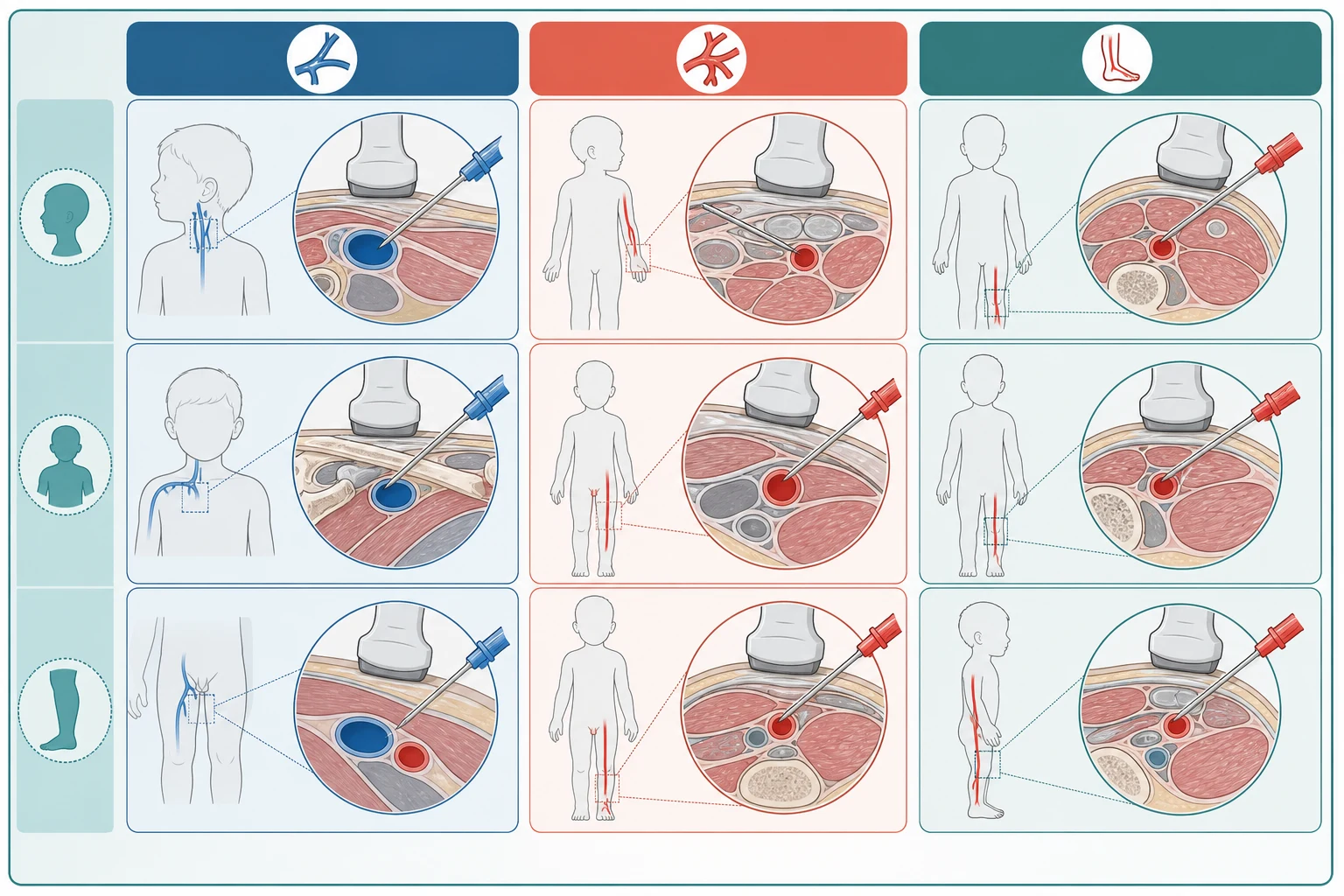
The second sort is by site. The central venous sites are the internal jugular vein, the subclavian vein, and the femoral vein; the arterial sites are the radial artery (first-line), the femoral artery, the posterior tibial and dorsalis pedis arteries, and, less often, the axillary or brachial. The site is chosen against the indication and the child's risks — compressible sites for the bleeding child, ultrasound-friendly sites for the small child, and sites that spare the pleura when pneumothorax would be catastrophic. [1]
A useful refinement is the contrast with peripheral and intraosseous access. A peripheral cannula suffices for short-term, non-irritant therapy in a child with good veins; an intraosseous needle is the emergency bridge when there is no time to cannulate. A central line is the answer when the infusate demands central dilution or the access must be reliable for more than a few days. The sister pages on intraosseous access and umbilical venous and arterial catheterisation carry the emergency and neonatal detail. [8]
Device purposes follow APLS and the international ultrasound-guided vascular access recommendations. [1] [8]
Epidemiology & Risk Factors
Paediatric central access is common in intensive care, oncology, and procedural settings, and its complications are predictable enough that a prepared team prevents most of them. Duesing and colleagues framed central venous access in the paediatric population around its complications and the prevention strategies that reduce them, and that framing — anticipate, prevent, and recognise early — is how the topic is examined. The risk is not uniform: the smallest, the sickest, and the most coagulopathic children carry the highest burden. [8]
Age and size are the strongest anatomical risk multipliers. Infants and small children have small-calibre vessels that collapse under the ultrasound probe, a thin subcutaneous layer that lets vessels roll away from the needle, and less physiological reserve if the procedure provokes vagal slowing or desaturation. The coagulopathic child — the thrombocytopenic oncology patient, the child in disseminated intravascular coagulation, or the anticoagulated child — carries a much higher risk of a catastrophic haematoma, especially at a non-compressible site. Ullman and colleagues documented that paediatric central venous access devices carry substantial practice variation, performance differences, and cost, with device failure and complication clustering in the most complex children. [7]
Who performs the line changes the outcome. Operators trained in ultrasound-guided access, working with a full sterile team and a planned approach, achieve higher first-pass success and fewer arterial punctures than those relying on landmarks. In retrieval and small units, this is the argument for either calling a team that can place the line safely or accepting a single femoral line over repeated internal jugular attempts that burn vessels and risk the pleura. [1] [4]
The dwell time of a line is itself a risk factor. Each day a central line stays in raises the cumulative probability of a central line-associated bloodstream infection and of catheter-related thrombosis, which is why a daily review of line necessity — and prompt removal the moment the line is no longer needed — is a core safety practice rather than an administrative tick. [12]
Pathophysiology
Children are harder to cannulate centrally than adults for mechanical reasons, and those reasons explain why ultrasound changed paediatric practice so completely. A child's central veins are small in calibre, they lie close to their companion artery, and they are mobile within a thin subcutaneous layer, so a probe pressed too firmly obliterates the very vein being sought. Where an adult internal jugular vein might tolerate a landmark guess, a child's rarely does, and the cost of a wrong guess — an arterial puncture, a haematoma, a pneumothorax — is paid in a smaller body with less reserve. [1] [4]
The internal jugular anatomy is the foundation of the most common approach. The internal jugular vein runs within the carotid sheath, lateral and superficial to the carotid artery, deep to the sternocleidomastoid, and it is reached at the apex of the triangle formed by the two heads of the muscle. In a child the vein often lies anterior to the artery in part of its course, which is exactly why a short-axis ultrasound view — confirming the vein is the compressible, non-pulsatile lateral structure before any needle moves — is non-negotiable. The right side is usually preferred because the route to the superior vena cava is straight and the thoracic duct is on the left. [1] [2]
The femoral anatomy underpins the emergency site. Below the inguinal ligament the femoral sheath contains, from lateral to medial, the nerve, artery, vein, and lymphatics — the relationship remembered as the NAVL arrangement. The vein therefore lies medial to the pulsatile artery, the site is fully compressible against the pubic ramus if the artery is hit, and there is no pleura to puncture, which is why the femoral vein is the safest first site in the emergency or coagulopathic child. [3]
The Seldinger principle is the mechanical heart of the whole procedure. A small needle finds the vessel, a guidewire is passed through the needle into the lumen, the needle is withdrawn leaving the wire, the tract is dilated, and the catheter is railroaded over the wire into the vessel. Each step is irreversible: once the wire is in, the operator must never lose control of its distal end, and once the catheter is in, the wire must be out before the line is flushed. The radial artery owes its safety to collateral circulation — the ulnar artery completes the superficial and deep palmar arches — which is why an intact ulnar collateral supply, confirmed by an Allen test, lets the radial artery be sacrificed to a line with low risk to the hand. [5] [6]
Clinical Presentation
The child who needs a central or arterial line presents through one of a few clear doors, and reading which door the child is at tells you both whether a line is needed and which line and site. [8]
The venous indication most often met in intensive care is the need to deliver a drug or fluid that a peripheral vein cannot safely carry. Concentrated vasoactive infusions such as adrenaline or noradrenaline, hypertonic or irritant infusions such as parenteral nutrition, and the demands of haemofiltration or plasmapheresis all call for central dilution at the cavoatrial junction. The bedside picture is the shocked child on rising vasoactive support through a tenuous peripheral cannula, or the technology-dependent child whose peripheral access has run out. [8]
The arterial indication is the child who needs beat-to-beat pressure or frequent gases. A child in severe shock on high vasoactive support, a child on a ventilator with severe respiratory failure needing tight carbon dioxide control, or a child in diabetic ketoacidosis needing hourly gases all benefit from an arterial line that spares repeated peripheral stabs and gives continuous pressure. The bedside clue is the child who is already being stabbed too often, or whose non-invasive pressure is unreliable because of a poor cuff fit or a low output state. [5]
Anticipated duration and lifestyle shape the device. A child who needs weeks of chemotherapy, a child on long-term parenteral nutrition for intestinal failure, and a child who wants to swim between treatments each push toward a tunnelled catheter or an implantable port rather than a bedside acute line. The distressed, agitated, or moving child is a procedural risk in themselves, because a sudden jerk converts a careful needle approach into an arterial puncture; recognising that, and preparing holding, distraction, or procedural sedation, is part of reading the child. [7]
Differential Diagnosis
Before committing to a central or arterial line, ask whether a less invasive option would meet the need, or whether a different access altogether is the answer. The differential here is a list of access strategies, not of diseases. [8]
Peripheral access is the first alternative. A well-placed peripheral cannula suffices for short-term, non-irritant therapy in a child with good veins, and the decision to escalate to a central line turns on whether the infusate demands central dilution or the access must be reliable beyond a few days. For the child who needs intermediate-duration therapy but tolerates a peripheral approach, a PICC threads a central tip from an arm vein and avoids a neck or groin procedure. [7]
Intraosseous access is the emergency alternative. When a child has collapsed and there is no time to cannulate, an intraosseous needle into the proximal tibia or humerus gives a route for fluids and drugs that reaches the central circulation within seconds. It is a bridge, not a definitive line, and is converted to a central or peripheral line once the child is stabilised. The sister page on intraosseous access carries the technique. [8]
Reversible or alternative problems deserve a final thought before the procedure. A child who "needs a line for fluids" may in fact need the underlying shock treated; a child who "needs an arterial line for gases" may need less frequent sampling and a better-run insulin infusion. The line supports the child while the real treatment happens, and the decision to place it should never be automatic. [8]
Clinical & Bedside Assessment
The bedside assessment for central or arterial access is almost entirely about preparation, because the procedure is won or lost before the needle moves. Work through equipment, ultrasound, sizing, and roles as a checklist. [1] [8]
Start with the ultrasound. A high-frequency linear probe is essential for paediatric access, and the first action is to identify the target vessel and its companion artery in a short-axis view. For the internal jugular, confirm the vein is the lateral, compressible, non-pulsatile structure relative to the carotid, and watch it return after compression. For the femoral vein, confirm it lies medial to the artery in the groin. For the radial artery, identify the pulsatile vessel lateral to the flexor carpi radialis tendon. Seeing these relationships before draping is what separates a safe line from a guess. [1]
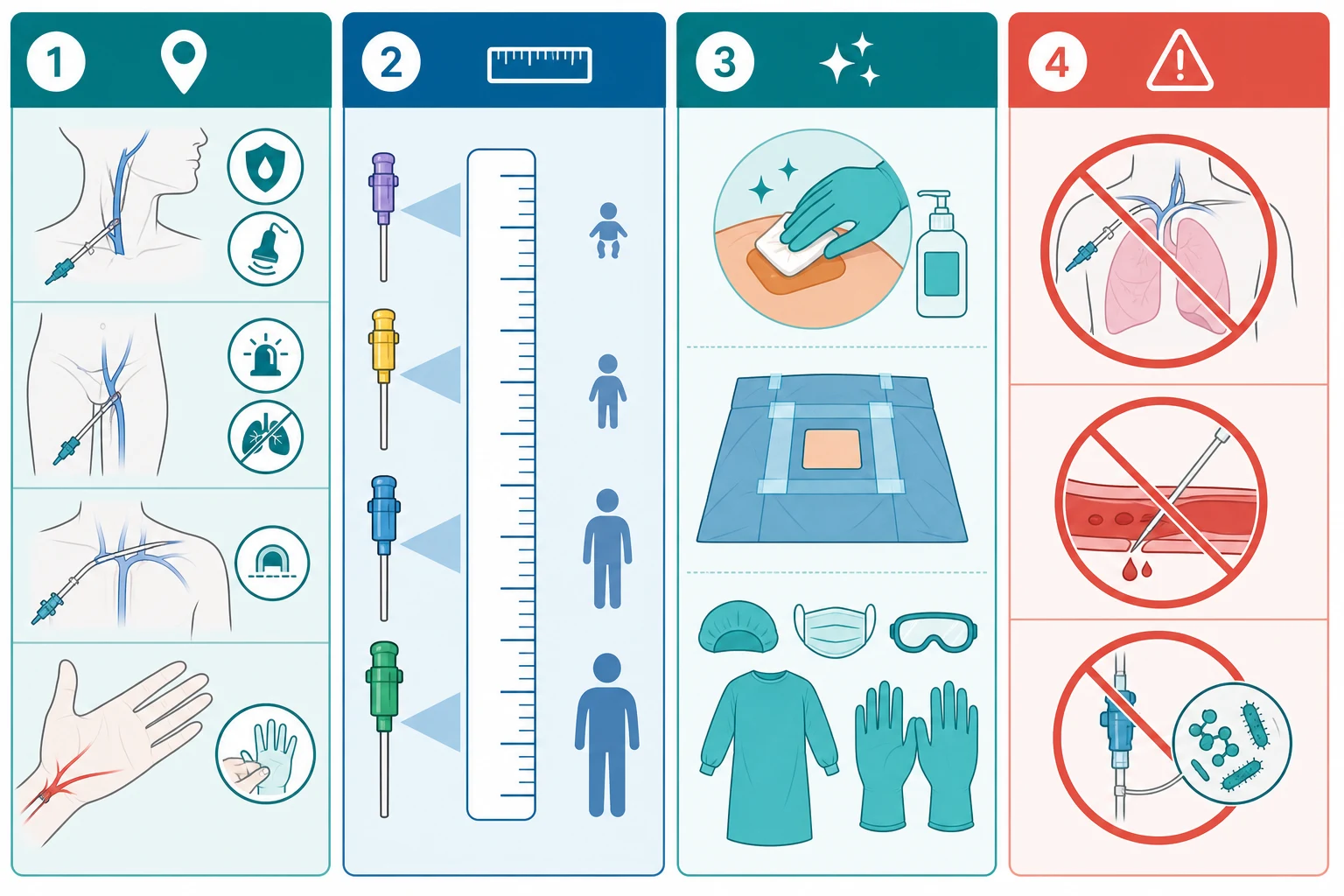
The equipment trolley carries the sterile pack, chlorhexidine skin preparation, the chosen catheter or cannula with its guidewire and dilator, a scalpel blade, suture, flushing saline, a transducer and pressure tubing for an arterial line, and drawn-up local anaesthetic. Full barrier precautions — cap, mask, sterile gown and gloves, and a large sterile drape — are applied for every central line, because the strongest evidence for preventing central line-associated bloodstream infection sits in the insertion bundle. [12]
Catheter and cannula sizing — by age and weight
Local anaesthetic for skin wheal: lidocaine 1 per cent, maximum 3 mg/kg without adrenaline (4.5 mg/kg with adrenaline), given slowly and aspirated to avoid intravascular injection. [8]
The radial arterial line begins with the Allen test. Compress both the radial and ulnar arteries at the wrist, ask the child to clench and open the fist to blanch the palm, then release the ulnar artery and watch for reperfusion of the palm within seconds. A brisk flush confirms an intact ulnar collateral supply and makes the radial artery a safe choice; a delayed or absent flush should prompt a different site. The wrist is then dorsiflexed and ulnar-devoted, and the artery is approached under ultrasound, often with an acoustic-shadowing technique that aids visualisation in the young child. [5] [6]
Pre-insertion bedside checklist
Ultrasound machine with a high-frequency linear probe; target vessel and artery confirmed in short axis before draping
Full barrier precautions: cap, mask, sterile gown and gloves, large sterile drape
Chlorhexidine skin preparation applied and allowed to dry
Catheter or cannula sized to the child, with guidewire and dilator; scalpel, suture, flush ready
Local anaesthetic drawn up; sedation and holding plan agreed for the child
Roles assigned: operator, ultrasound assistant, drug and flush assistant, scribe
Plan for failure stated aloud: what to do if the artery is hit, the wire will not pass, or the child desaturates
Investigations
Most investigations must not delay a line that is needed, but a few bedside tests change the plan. The single most important "investigation" is the ultrasound itself, which answers, before the needle moves, whether the target vessel is present and patent and where the companion artery lies. [1]
A coagulation screen and platelet count matter when a central line is planned in a child with a bleeding risk, and they shape the site. A low platelet count or a deranged coagulation screen pushes the operator away from the subclavian site — whose bleeding cannot be compressed — toward the femoral or internal jugular vein, and may prompt correction of the coagulopathy by local protocol before the procedure. The exact thresholds for safe central access vary by centre, so the candidate should name the local protocol while stating the principle: compressible sites for the bleeding child. [8]
After insertion, the functional tests are the proof. A central venous line should aspirate venous blood and flush freely from every lumen, and its tip is confirmed on a chest radiograph or by ultrasound-based tip navigation. An arterial line is confirmed by a crisp arterial waveform on the transducer and bright pulsatile blood that matches the child's pulse; a damp trace or venous-coloured blood means the line is not truly arterial and must be reassessed. [11]
Management — Resuscitation
The resuscitation phase is the moment of insertion, and it begins the instant the decision is made. Assemble the team, bring the ultrasound and a full sterile set, confirm consent and any sedation, allocate roles, and state a plan for failure aloud: what to do if the artery is hit, the wire will not pass, or the child deteriorates. A short team brief turns a fumbled attempt into a coordinated one. [1] [8]
Prepare the skin with chlorhexidine antisepsis and allow it to dry, because the antiseptic only works once dry and a wet field breaks the sterile barrier. Apply full barrier precautions — cap, mask, sterile gown and gloves, and a large drape — for every central line, not only the elective ones. Hold the child safely and still: swaddle an infant, use distraction or sucrose in the toddler, arrange procedural sedation where appropriate, and assign a trained assistant to immobilise the limb or head without compromising the airway. A moving child is the most common cause of an arterial puncture. [12]
The response to an arterial puncture during a venous attempt is a rehearsed manoeuvre, not a moment of panic. Withdraw the needle, apply firm sustained proximal pressure over the artery for several minutes — longer than feels necessary — reassess the vessel under ultrasound, and reposition before reattempting. For a femoral site the pressure is straightforward because the artery is compressible against bone; for a subclavian puncture the bleeding is invisible and uncompressible, which is the reason the site is avoided in the bleeding child. [8] [9]
The single most important resuscitation rule during the procedure is this: if the child deteriorates, stop. Bradycardia, desaturation, or hypotension during an attempt demand that the needle comes out, the team returns to airway and circulation priorities, and the child is stabilised before the procedure resumes. Completing the line is never more important than the child in front of you. [8]
Management — Definitive & Stepwise
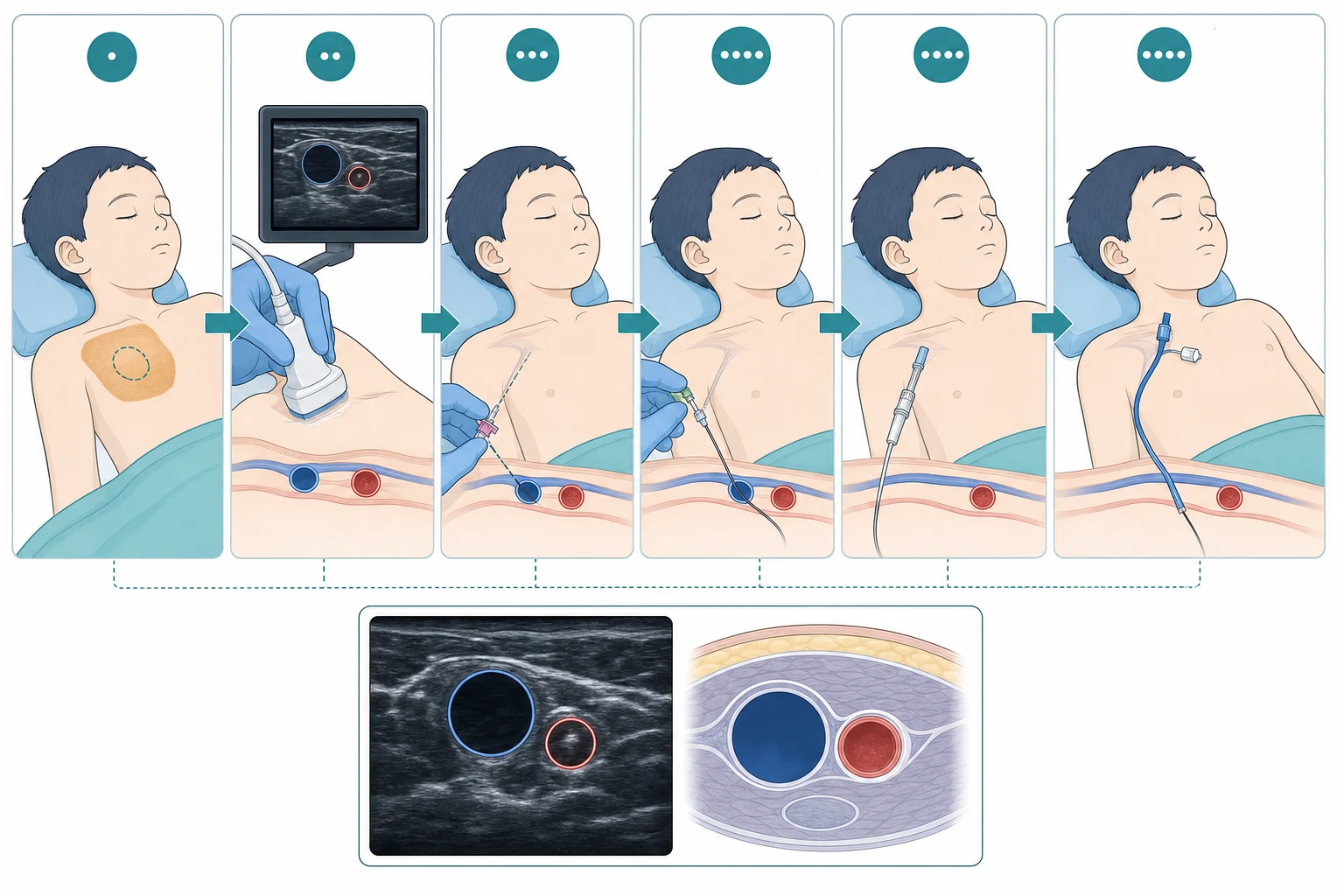
The definitive management is the Seldinger sequence executed under ultrasound, with the right device for the right child. State each step by name and its reason. [1] [11]
Begin by identifying the target vessel and its companion artery in a short-axis view, confirming the vein is compressible and non-pulsatile. Raise a skin wheal with local anaesthetic, then advance the needle to the vessel under ultrasound, watching the needle tip in the lumen. Confirm venous return by the dark, non-pulsatile blood that aspirates gently, then pass the guidewire through the needle into the vessel, holding the wire at all times so its distal end is never lost. Withdraw the needle over the wire, make a small skin nick, dilate the tract, and railroad the catheter over the wire into the vessel. Remove the wire, aspirate and flush every lumen to confirm free flow and venous blood, secure the line, and confirm the tip. [1]
Central venous site — choose by indication and bleeding risk
Arterial site first-line is the radial artery after an Allen test; the femoral artery is used for shock or when the radial is exhausted. [3] [8]
The site is chosen against the child's indication and risks. The internal jugular vein is ultrasound-friendly and is the common acute site, with the right side preferred for its straight run to the superior vena cava; its risks are carotid puncture and pneumothorax. The femoral vein is the first choice in the emergency or coagulopathic child because it is compressible and spares the pleura, with the trade-off of higher infection and thrombosis rates with long dwell times. The subclavian vein is preferred for long-term tunnelled access in the stable child but is avoided in coagulopathy because the subclavian artery cannot be compressed. [2] [3]
Arterial cannulation follows the same principle. After the Allen test and ultrasound identification, the radial artery is approached with an in-plane or out-of-plane needle, and a guidewire-assisted or direct cannula technique is used to place a 22 to 24 gauge cannula. The femoral artery is reserved for the child in shock or when the radial sites are exhausted. After placement, transduce the line to confirm a crisp arterial waveform, secure it well to prevent dislodgement, and monitor distal perfusion of the limb. [5] [6]
Post-insertion care is mandatory and is where candidates often stop too early. Secure the line, label each lumen, aspirate and flush all lumens, transduce an arterial line to a clean waveform, document the procedure and its complications, and arrange tip confirmation. Arrange the appropriate level of monitoring and admission — a freshly placed central line belongs in an intensive-care or high-dependency setting, not on an unmonitored ward. [7] [11]
Specific Subtypes & Scenarios
Different children need a tailored line, and the exam rewards the candidate who can match the site and device to the scenario. [7]
The infant and small child is the most technically demanding scenario. Vessels are small and collapse under the probe, the catheter is a tight fit, and the child is exquisitely sensitive to sedation and to a brief loss of the airway. Ultrasound is essential rather than helpful, the femoral and internal jugular sites dominate, and a fully prepared team with holding and sedation planned is the rule. Small drug and flush volumes demand careful checking, because a flush into a central line reaches the heart in seconds. [4]
The oncology child is the scenario where device choice is long-term. A tunnelled Hickman or Broviac catheter, or a totally implantable port, gives reliable access for months of chemotherapy and spares the child repeated cannulation. Thrombocytopenia and chemotherapy-induced mucositis raise both the bleeding and the infection risk, so the subclavian site is avoided when the platelet count is low and the insertion bundle is applied with extra rigour. Ullman and colleagues documented the substantial cost and performance variation of these devices, which is why their choice and care are centralised in oncology services. [7]
Site choices follow the international ultrasound-guided recommendations and the Cochrane evidence on each site. [1] [3]
In the child on high vasoactive support or needing very frequent blood gases, an arterial line becomes essential rather than convenient. The radial artery is first-line after an Allen test; the femoral artery is used in shock or when the radial sites are exhausted. Distal perfusion is checked hourly, because the threat is a thrombosis that ischaemia the hand or foot, and the line is removed the moment it is no longer needed. [5]
The bleeding-risk child — a coagulopathy, a low platelet count, or active anticoagulation — changes the site but not the technique. Choose a compressible site, the femoral or internal jugular, avoid the subclavian, and correct or accept the coagulopathy by local protocol. The retrieval or remote setting often asks who should place the line and where; a single femoral line placed safely by an experienced operator is better than repeated internal jugular attempts in a small unit, and intraosseous access remains the bridge when there is no time. [8]
Complications & Pitfalls
Complications of paediatric central and arterial access are predictable and cluster around a few failures, and knowing them in advance is how a team avoids them. [8]
Arterial puncture is the most common immediate complication of a central venous attempt, and its management is rehearsed rather than improvised: withdraw the needle, hold firm proximal pressure for several minutes, reassess under ultrasound, and reposition. The danger is not the puncture itself but a failure to recognise it and a failure to hold pressure long enough; a missed arterial puncture at a non-compressible site becomes a haemothorax or a catastrophic haematoma. Pneumothorax follows internal jugular and subclavian attempts, and is excluded by a post-procedure chest radiograph and by watching the child for sudden desaturation, dyspnoea, or hypotension that suggests a tensioning pneumothorax. [2] [9]
D.R.I.P. — when the line goes wrong
Venous air embolism is the rare but feared complication of a central line, and it is prevented by keeping the child head-down for an internal jugular or subclavian insertion, by occluding every lumen and the needle hub at all times, and by never leaving an open catheter to air. Sudden hypotension, desaturation, or a "mill wheel" murmur during or after insertion should raise the suspicion of air embolism; the response is to position the child head-down and left-lateral, give oxygen, and aspirate air from the line if possible. [8]
Central line-associated bloodstream infection is the dominant late complication, and its prevention is an insertion-and-maintenance bundle rather than a single act. Full barrier precautions at insertion, chlorhexidine skin antisepsis, chlorhexidine-impregnated dressings, scrub-the-hub hub care before each access, avoidance of routine flushing, and a daily review of line necessity with prompt removal are the elements Buetti and colleagues updated for acute-care hospitals. Arterial lines carry a lower infection rate but the same aseptic discipline, and their distinctive pitfall is distal limb ischaemia from thrombosis — a cold, pale, pulseless hand or foot demands immediate line removal and escalation. [12]
Catheter malposition and a guidewire advanced too far are the pitfalls most tied to inattention. A central catheter tip that sits in the internal jugular, the contralateral subclavian, or a ventricle must be repositioned or replaced, because an irritant infusion delivered there can thrombose or perforate the vessel. A wire advanced too far provokes atrial or ventricular ectopy on the monitor, and the response is to withdraw the wire until the ectopy resolves; measuring the wire depth to the child's size before insertion prevents the error. Never lose sight of the wire's distal end, and never fail to confirm, at the end of the case, that the wire has been removed. [8] [11]
Prognosis & Disposition
Every child who receives a fresh central line is monitored in an intensive-care or high-dependency setting, or in theatre, because the first hours after insertion are when the pneumothorax, the haematoma, and the malposition declare themselves. An unmonitored ward is not a safe place for a freshly placed central line, and a child who needs a line for a ward-level problem usually needs a PICC or a peripheral approach instead. [7]
The dwell time of a line is the single strongest modifiable factor in its long-term risk. Each additional day raises the cumulative probability of a central line-associated bloodstream infection and of catheter-related thrombosis, which is why the daily review of line necessity — asking, every day, whether the line is still needed — is a core safety practice and a quality target, not a paperwork exercise. The line that is no longer needed should be removed, with the child positioned head-down for an internal jugular or subclavian line to prevent air embolism, and with pressure and a sealed dressing over the exit site. [12]
After insertion, ongoing monitoring is continuous. An arterial line is watched for a crisp waveform, a clean blood-gas trace, and a well-perfused distal limb; a central line is watched for lumen patency, dressing integrity, and exit-site signs of infection. The line is removed the moment its purpose is served, and the child who will need long-term access is transitioned to the most suitable device — a tunnelled catheter or a port — rather than nursing an acute line past its useful life. [8]
It is worth saying plainly to a family that the long-term outcome depends far more on why the child needed the line than on the line itself. The line is a bridge for the infusions, the monitoring, and the chemotherapy that treat the underlying illness; owning the procedure's risks — an arterial puncture, a pneumothorax, a line infection — while framing the line as the access that lets the real treatment happen is honest and steadying communication. [7]
Special Populations
Some children carry an access risk that changes the procedure from the first phone call, and recognising them early is the mark of safe practice. [8]
The technology-dependent child — one with a long-term tunnelled line, a port, or a known difficult venous access from a chronic condition — should have a pre-existing line-care plan documented in the record and, ideally, on the family. Find that plan, involve the teams who know the child, use the device that has worked before, and avoid burning new peripheral veins that the child will need for years. These children are often the hardest access in the hospital, and routine approaches fail them. [7]
A child with a bleeding disorder or on anticoagulation turns the site choice into a safety decision. Haemophilia, a low platelet count, or a therapeutic anticoagulant all push the operator toward a compressible site — femoral or internal jugular — and away from the subclavian, and may prompt factor correction by protocol before the procedure. Knowing the child's bleeding risk before the site is chosen prevents the cardinal error of an uncompressible bleed. [8]
The immunocompromised or oncology child needs heightened prevention of central line-associated bloodstream infection and a strong preference for a tunnelled device or port over repeated acute lines, because each acute line carries its own cumulative infection risk. A child with developmental disability or autism benefits, when time allows, from preparation, distraction, child-life involvement, and, where appropriate, procedural sedation, because a calm child is a safer line. [12]
In remote and retrieval settings, the question is often who should place the line and where. A small unit with a single junior doctor and no ultrasound expertise faces a high-risk line; the safer answer may be to bridge with intraosseous access and call a retrieval team that can place the line in a controlled way. Moving the skill and the ultrasound to the child is often safer than moving the child to repeated attempts. [8]
Evidence, Guidelines & Regional Differences
The guidelines that anchor paediatric central and arterial access — the international ultrasound-guided vascular access recommendations of Lamperti, the Cochrane reviews of Brass and Aouad-Maroun, the RCH Melbourne guidelines, and the CLABSI prevention strategies of Buetti — converge on ultrasound guidance, a sterile insertion bundle, and a daily review of necessity, but a few evidence questions are worth knowing for the exam. [1] [12]
The clearest evidence is for ultrasound guidance of the internal jugular vein. Brass and colleagues' Cochrane review found that, compared with anatomical landmarks, ultrasound guidance reduced the number of failed attempts, the number of arterial punctures, and the number of haematomas for internal jugular cannulation, and Sigaut's earlier paediatric meta-analysis reached the same conclusion in children and infants. This is why ultrasound guidance is now the standard of care for paediatric internal jugular access. [2] [4]
The evidence for subclavian and femoral ultrasound guidance is more measured. Brass's second Cochrane review found that ultrasound guidance offered no clear advantage over the landmark technique for subclavian or femoral cannulation in adults, though it did not negate ultrasound's role in children, where the small-vessel problem remains. Nardi and colleagues reported the effectiveness and complications of ultrasound-guided subclavian cannulation in children and neonates, and Pang's randomised trial found ultrasound guidance non-inferior to fluoroscopy for subclavian catheterisation in children with haematologic disease, supporting ultrasound as a practical, radiation-sparing approach. [3] [9] [10]
Ultrasound-guided arterial cannulation in children is an evolving area. Aouad-Maroun's Cochrane review found only low- or very-low-quality evidence that ultrasound improved arterial cannulation in children, with a trend toward benefit that fell short of certainty, and Quan's study of the acoustic-shadowing technique showed how ultrasound could facilitate radial artery cannulation in young children. The pragmatic position is that ultrasound is used for paediatric arterial access despite the limited randomised evidence, because the anatomical case is the same as for central veins. [5] [6]
Tip navigation and device selection are newer evidence strands. Zito Marinosci and colleagues described the ECHOTIP-Paed protocol, a structured approach to ultrasound-based tip navigation and tip location during central venous access device placement in children, which reduces reliance on fluoroscopy and post-procedure radiography. Ullman's data on paediatric central venous access device practice, performance, and costs documented the substantial variation in device choice and failure across services, framing device selection as a system decision as much as a clinical one. [7] [11]
Exam Pearls
The exam will test three things above all: the sites and their trade-offs, the Seldinger sequence, and the recognition of when a line is going wrong. Have these ready to say aloud. [1] [8]
State the sites precisely: central venous sites are the internal jugular (ultrasound-friendly, right side preferred, risk of pneumothorax and carotid puncture), the subclavian (long-term tunnelled access, avoided in coagulopathy because the bleeding is non-compressible), and the femoral (emergency and coagulopathy first choice, compressible, pneumothorax-free). Arterial sites are the radial (first-line, after an Allen test), the femoral (for shock or when the radial is exhausted), and the posterior tibial. [2] [3]
Know the Seldinger sequence cold: needle to vessel under ultrasound, confirm venous blood, guidewire through needle, withdraw needle, dilate, railroad catheter over wire, withdraw wire, aspirate and flush every lumen, secure, and confirm the tip at the cavoatrial junction. State the catheter tip target — the cavoatrial junction, confirmed on a chest radiograph or by ultrasound-based tip navigation — and never forget to confirm, at the end, that the wire has been removed. [1] [11]
Know the complication bundle: arterial puncture (withdraw and hold firm pressure), pneumothorax (exclude on chest radiograph, watch for tension), venous air embolism (head-down, occlude lumens, treat head-down left-lateral), central line-associated bloodstream infection (full barrier, chlorhexidine, chlorhexidine dressing, scrub-the-hub, daily review, prompt removal), and distal limb ischaemia from an arterial line (remove immediately). Know the CLABSI prevention bundle and the rule that the subclavian site is avoided in coagulopathy because the bleeding site cannot be compressed. [9] [12]
Finally, have the DRIP and the Seldinger mnemonics on the tip of your tongue, and be able to talk through what you do when bright pulsatile blood returns on a venous attempt: withdraw the needle, hold firm proximal pressure for several minutes, reassess under ultrasound, and reposition before reattempting. The candidate who can describe the calm, prepared, ultrasound-guided approach with a rehearsed plan for failure is the one who passes this topic. [8]
References
- [1]Lamperti M International evidence-based recommendations on ultrasound-guided vascular access. Intensive Care Med, 2012.PMID 22614241
- [2]Brass P Ultrasound guidance versus anatomical landmarks for internal jugular vein catheterization. Cochrane Database Syst Rev, 2015.PMID 25575244
- [3]Brass P Ultrasound guidance versus anatomical landmarks for subclavian or femoral vein catheterization. Cochrane Database Syst Rev, 2015.PMID 25575245
- [4]Sigaut S Ultrasound guided internal jugular vein access in children and infant: a meta-analysis of published studies. Paediatr Anaesth, 2009.PMID 19863734
- [5]Aouad-Maroun M Ultrasound-guided arterial cannulation for paediatrics. Cochrane Database Syst Rev, 2016.PMID 27627458
- [6]Quan Z Acoustic Shadowing Facilitates Ultrasound-guided Radial Artery Cannulation in Young Children. Anesthesiology, 2019.PMID 31634245
- [7]Ullman AJ Pediatric central venous access devices: practice, performance, and costs. Pediatr Res, 2022.PMID 35136199
- [8]Duesing LA Central Venous Access in the Pediatric Population With Emphasis on Complications and Prevention Strategies. Nutr Clin Pract, 2016.PMID 27032770
- [9]Nardi N Effectiveness and complications of ultrasound-guided subclavian vein cannulation in children and neonates. Anaesth Crit Care Pain Med, 2016.PMID 26924612
- [10]Pang H A Randomized Trial of Ultrasound- versus Fluoroscopy-Guided Subclavian Vein Catheterization in Children with Hematologic Disease. Indian J Pediatr, 2019.PMID 31332603
- [11]Zito Marinosci G ECHOTIP-Ped: A structured protocol for ultrasound-based tip navigation and tip location during placement of central venous access devices in pediatric patients. J Vasc Access, 2023.PMID 34256613
- [12]Buetti N Strategies to prevent central line-associated bloodstream infections in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol, 2022.PMID 35437133