Paeds · investigations-procedures-and-technology
Chest decompression and intercostal drain insertion
Also known as Needle thoracostomy · Needle decompression · Intercostal catheter insertion · Chest drain insertion · Intercostal drain · Chest tube · Underwater seal drainage
A fellowship approach to chest decompression and intercostal drain insertion in children covering tension pneumothorax as a clinical diagnosis requiring immediate needle decompression at the second intercostal space mid-clavicular line or the fourth or fifth intercostal space at the anterior axillary line within the safe triangle, the safe triangle boundaries (anterior border lateral edge of pectoralis major, posterior border lateral edge of latissimus dorsi, inferior border the fifth intercostal space at the nipple line, apex at the base of the axilla), the rule of inserting above the rib below to avoid the neurovascular bundle that runs in the costal groove along the inferior border of the rib above, the stepwise blunt-dissection drain insertion technique, drain-size selection by content (small-bore 8 to 14 French pigtail for air, medium 16 to 24 French for fluid and empyema, large-bore 28 to 36 French for blood), the underwater seal with the tube tip two centimetres below the water line, the lidocaine 1 per cent maximum three milligrams per kilogram dose, the never-clamp-a-bubbling-drain rule, the complications of bleeding from the intercostal vessels, re-expansion pulmonary oedema, and wrong-side insertion, and the special scenarios of the ventilated neonate, adolescent spontaneous pneumothorax, and complicated parapneumonic empyema with intrapleural fibrinolytics.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a six-year-old hit by a car, now on a ventilator in the emergency department. Half a minute ago he was stable; now his oxygen saturations are crashing, his airway pressure alarm is shrieking, his blood pressure is falling, and the right side of his chest is silent and hyperresonant. Every second you spend confirming what you already know is a second his heart goes without venous return. Chest decompression exists for exactly this moment: to let the trapped air out of the pleural space before it kills him. [3] [10]
Two procedures live under this single topic, and the candidate must hold them apart. Needle thoracostomy (needle decompression) is the emergency, temporary act of pushing a cannula through the chest wall to vent a suspected tension pneumothorax. Intercostal drain (chest tube, ICC) insertion is the definitive act of placing a tube into the pleural space and connecting it to an underwater seal that lets air and fluid out while stopping air going back in. Needle decompression buys minutes; the intercostal drain buys the hours to days the lung needs to heal. A child who needed a needle will need a drain; a child who needs a drain does not always need a needle. [1]
A third, gentler cousin is pleural aspiration (thoracentesis) — draining fluid from the pleural space with a needle or cannula for diagnosis or symptom relief. It uses the same landmarks and the same respect for the neurovascular bundle, but it is not the emergency procedure and it is not what tension pneumothorax is treated with. Throughout this topic the focus is the two emergency procedures, with aspiration appearing where the differential and the technique overlap. [1]
Classification
The candidate should classify chest decompression along three axes at once: the purpose (emergency decompression, definitive drainage, or diagnostic aspiration), the site (mid-clavicular or safe triangle), and the device (cannula, pigtail, or large-bore tube). The three interact, because the device dictates the technique and the site is partly chosen for it. [1]
By purpose, three families exist. Emergency needle decompression is for the child in whom you suspect a tension pneumothorax and cannot wait; it is a temporising act that must always be followed by a drain. Definitive intercostal drainage treats a pneumothorax, pleural effusion, empyema, or haemothorax that is too large, too symptomatic, or too infected to resolve on its own. Pleural aspiration drains fluid for diagnosis or symptom relief without leaving a tube. [1]
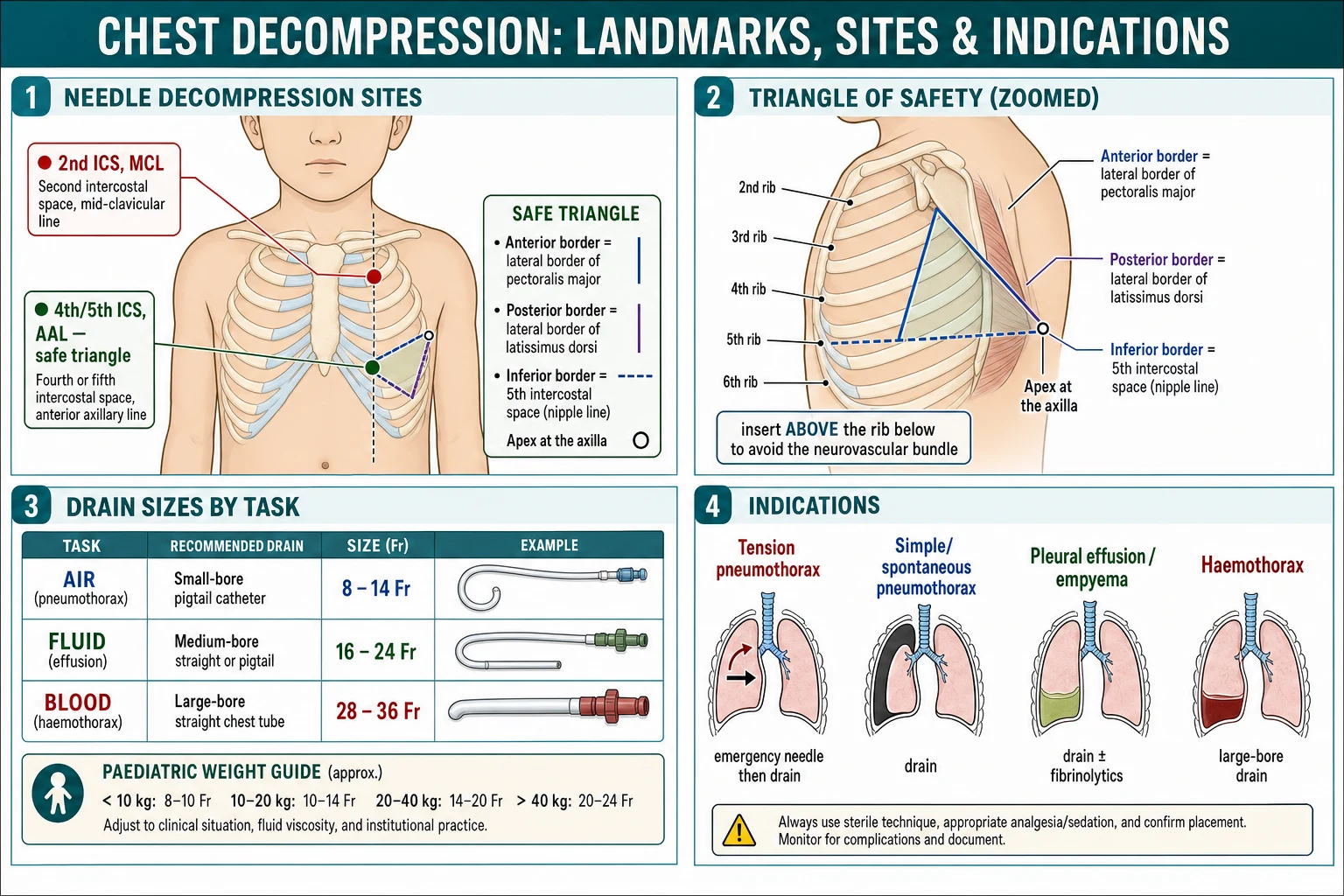
By site, two decompression points coexist in modern teaching and the candidate must know both. The traditional site is the second intercostal space in the mid-clavicular line — taught for decades in ATLS and APLS because it is easy to find and is above the breasts in adults. The preferred site, increasingly recommended in children and in adults, is the fourth or fifth intercostal space in the anterior axillary line, within the safe triangle — the same site used for the definitive drain. The shift matters and is examined: the chest wall is thinner and more consistent at the axillary line, the catheter is more likely to reach the pleural space, the site avoids the internal mammary vessels, and a single incision can become the definitive drain. [4] [5]
By device, three sizes govern practice. A small-bore pigtail catheter (8 to 14 French), placed by Seldinger technique, drains air and simple fluid with less pain and is now first-line for pneumothorax and uncomplicated effusion. A standard intercostal catheter (16 to 24 French) drains thicker fluid, pus, and loculated effusion. A large-bore drain (28 to 36 French) is reserved for blood and large air leaks, because clot blocks a small tube. The cardinal rule is simple: choose the smallest drain that will drain the material. [1] [11]
Epidemiology & Risk Factors
Tension pneumothorax is rare in children but disproportionately lethal, and it clusters in three predictable groups. The first is the ventilated child, above all the premature neonate on positive-pressure ventilation, in whom even a small air leak can become tension physiology within a few breaths. The second is the trauma victim — the blunt chest injury, the rib fracture, the penetrating wound — in whom a pneumothorax or haemothorax can develop fast. The third is the child with severe intrinsic lung disease: an acute severe asthma attack, a cystic fibrosis exacerbation, or a necrotising pneumonia that erodes into the pleura. [3] [10]
A few numbers frame the rest of the topic. Neonatal pneumothorax occurs in roughly 1 to 2 per cent of live births and is symptomatic in a minority; it is far commoner in the ventilated preterm infant and after meconium aspiration. Primary spontaneous pneumothorax peaks in tall, thin adolescent males who smoke, with a recurrence rate that climbs toward 50 per cent after a first episode. Complicated parapneumonic effusion and empyema in children, most often caused by Streptococcus pneumoniae and Staphylococcus aureus, is a leading indication for intercostal drainage worldwide and has risen in regions where pneumococcal conjugate vaccine coverage is incomplete. [2] [8]
One epidemiological fact drives the modern shift in decompression site: the second intercostal space mid-clavicular line fails in a meaningful proportion of adults and older children because the catheter is too short for the chest wall. Paediatric CT and ultrasound studies measure chest wall thickness at 10 to 18 millimetres depending on site and age, thinner and more consistent at the anterior axillary line than at the mid-clavicular line. That single finding is why the safe-triangle site is now preferred in children and increasingly in adults. [5] [6] [7]
Ventilated neonate
Preterm, RDS, meconium
- Tension physiology can develop in a few breaths
- Thin chest wall — use the smallest drain (10 to 12 Fr pigtail)
- Sudden rise in airway pressure is the alarm
- Needle aspiration may be enough for a small pneumothorax
Trauma (child or adolescent)
Blunt or penetrating chest injury
- Decompress at the safe triangle, then large-bore drain
- Look for haemothorax — needs 28 to 36 Fr
- ATLS primary survey in parallel
- Finger thoracostomy if ventilated and needle fails
Adolescent spontaneous pneumothorax
Tall thin smoker
- Small (under 2 cm rim) and stable: observe or aspirate
- Larger or symptomatic: small-bore pigtail
- Recurrence risk high — discuss pleurodesis after second episode
- Counsel on smoking cessation
Complicated parapneumonic effusion
Empyema
- Chest drain plus intrapleural fibrinolytics for loculations
- IV antibiotics covering pneumococcus and staph
- VATS if drainage fails or collections are multiloculated
- Send pleural fluid for culture and PCR
Pathophysiology
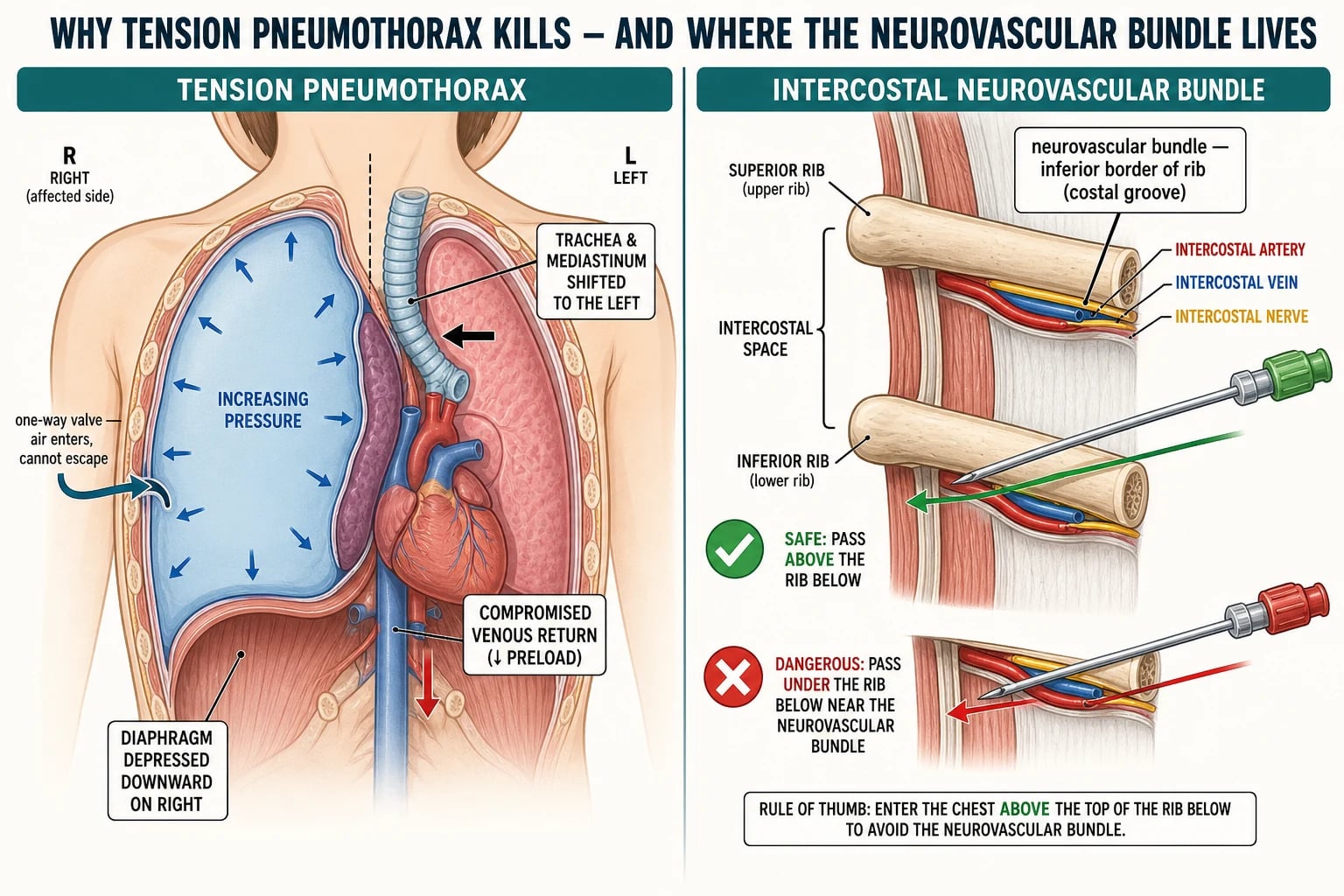
Tension pneumothorax is, mechanically, a one-way valve. Air enters the pleural space — through a ruptured alveolus, a lung laceration, or from the positive-pressure breath the ventilator is pushing in — but it cannot escape. Each breath adds a little more. The intrapleural pressure climbs above atmospheric, and from that single fact every clinical sign follows. [3] [10]
Trace the cascade. Rising pleural pressure pushes the ipsilateral lung flat against the mediastinum and depresses the diaphragm. The mediastinum and trachea shift to the contralateral side, kinking the great veins at the thoracic inlet and compressing the thin-walled right atrium. Venous return to the heart falls, cardiac output falls, and the child becomes hypoxic, then bradycardic, then arrests. The tracheal deviation and the distended neck veins are late signs; the early signs are hypoxia, tachypnoea, and rising ventilator pressures in the intubated child. By the time blood pressure falls, you are close to arrest. [3]
The second anatomical fact that governs the whole technique is the intercostal neurovascular bundle. Between each pair of ribs runs a groove — the costal groove — along the inferior border of the rib above, carrying an intercostal vein, artery, and nerve from superior to inferior. The bundle therefore sits close to the rib forming the top of the intercostal space, not the one forming the bottom. The procedural rule is the inverse: insert the needle or the drain just above the rib below — that is, along the upper border of the lower rib — and you pass well clear of the bundle. This is the rule that every examiner tests. [1]
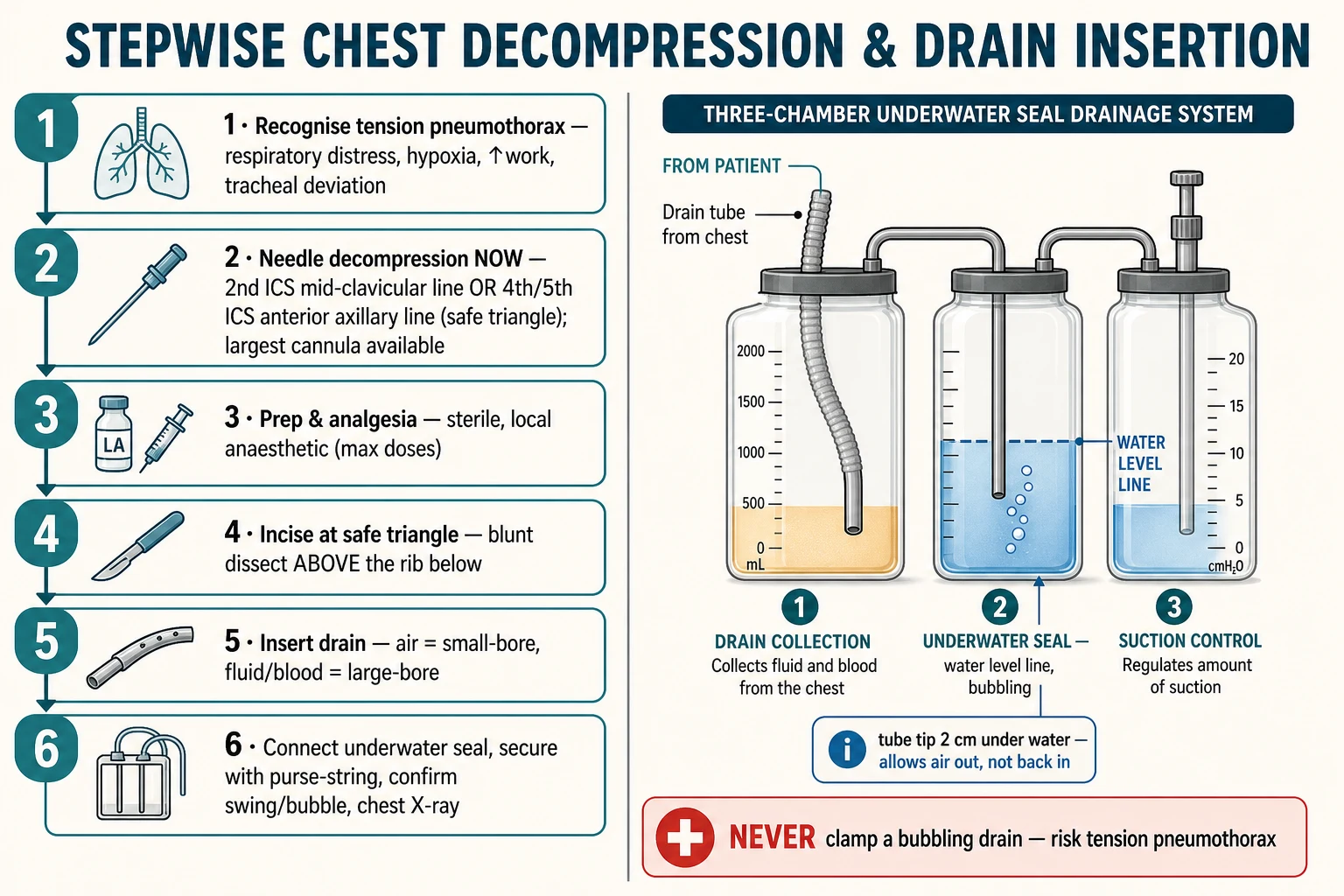
The underwater seal turns the same physics to your advantage. The drain tube tip sits two centimetres below the water line in a sealed chamber. When pleural pressure rises above atmospheric — on expiration, or with a cough, or with positive-pressure ventilation — air and fluid are pushed out through the tube and bubble up through the water. When pleural pressure falls below atmospheric — on inspiration — the negative pressure sucks water up the tube a little (the swing) but cannot pull atmospheric air back in, because the water column blocks it. The seal is therefore a one-way valve in reverse of the one that caused the tension. [1]
One last physiological fact governs the safe drainage of a large effusion. Rapid re-expansion of a chronically collapsed lung damages the pulmonary capillaries and causes re-expansion pulmonary oedema — sometimes fatal. The practical rule is to drain in a controlled way, pausing and reassessing after about 1.5 litres, and to monitor closely. This is why the BTS guideline warns against uncontrolled drainage of very large effusions. [1]
Clinical Presentation
The child who needs chest decompression is recognised by the situation, not by a single sign. Four clinical pictures recur, and the candidate should be able to narrate each. [3]
The first is tension pneumothorax in the spontaneously breathing child. The child is in marked respiratory distress: tachypnoeic, hypoxic, distressed, using accessory muscles. The affected side is expanded, moves less, is hyperresonant to percussion, and is silent on auscultation. As tension builds, the trachea deviates away from the affected side, the neck veins distend, and the child becomes pale, sweaty, and hypotensive — a peri-arrest state. By the time you see tracheal deviation you have little time left. [3]
The second is the ventilated child who suddenly deteriorates. This is the scenario that catches teams out, because the child cannot tell you they are breathless. The clues are objective: rising peak inspiratory and plateau pressures on the ventilator, falling oxygen saturations, hypotension, and reduced chest movement on one side. The ventilated neonate who desaturates and bradycardias within a minute, with a sudden jump in airway pressure, has a tension pneumothorax until proved otherwise. [9] [10]
The third is the trauma victim. The child with a flail segment, a penetrating chest wound, or a high-energy blunt injury may declare a pneumothorax or haemothorax on the primary survey; the haemothorax adds dullness to percussion and signs of hypovolaemia. The fourth is the child with a pleural collection that has declared itself slowly — the pneumonia that has not improved in 48 hours, the empyema with swinging fever and pleuritic pain, the large effusion with breathlessness and dullness. These need drainage, but not in the next 60 seconds. [2] [11]
Differential Diagnosis
There is no differential diagnosis of the procedure itself, but there is a crucial differential of the sudden deterioration in a ventilated child, and there is the differential of a large unilateral pleural collection. Both are examined. [9]
In the ventilated child who suddenly crashes, tension pneumothorax sits at the top of a short list that includes a blocked or kinked endotracheal tube, a mucous plug, mainstem intubation (the tube has slipped down and ventilates one lung), severe bronchospasm, and cardiac tamponade. The discriminating moves are fast: inspect and suction the tube, listen to both lungs, check tube depth, and watch the response to disconnecting the ventilator. A child whose saturations recover when you disconnect — and whose airway pressures fall — points to a tension pneumothorax or a blocked tube; a child who does not recover points to a fixed mechanical problem. Bilateral signs argue against a unilateral pneumothorax. [9]
The differential of a large unilateral pleural collection is the standard radiological one. A complicated parapneumonic effusion or empyema follows pneumonia and is the commonest in children. A transudative effusion complicates heart failure, nephrotic syndrome, hepatic failure, or severe hypoalbuminaemia. A haemothorax follows trauma, a bleeding disorder, or (rarely) a vascular malformation. A chylothorax follows thoracic surgery, central line injury, or lymphoma. A malignant effusion is seen with lymphoma or metastatic disease. Pleural fluid analysis distinguishes them. [2]
The third differential is the apparent failure of an established drain. When a drain stops swinging, stops bubbling, or stops draining, the possibilities are: the tube is blocked or kinked, it has dislodged from the pleural space (check the length outside the chest), it is malpositioned (in a fissure, or in the soft tissue), the underwater seal water level is low, the suction is disconnected, or there is a persistent large air leak indicating a bronchopleural fistula. Each has a corrective action: flush cautiously, reposition, top up the water, reattach suction, or call the surgical team. [1]
Clinical & Bedside Assessment
The bedside assessment has two halves: recognising tension physiology when it is in front of you, and identifying the correct site and a safe approach before you cut. Both are procedural skills as much as cognitive ones. [1]
To recognise a tension pneumothorax, run the same checklist every time. Look: is the child in distress, using accessory muscles, cyanosed? Is one side of the chest expanded and moving less? Feel: is the trachea central or deviated, are the neck veins engorged? Percuss: is the affected side hyperresonant? Listen: is air entry reduced or absent on that side? Add the ventilated child's tell-tale sign: a sudden rise in peak airway pressure with falling saturations and hypotension. If the picture fits, decompress — do not confirm. [3] [10]
To identify the safe triangle, you must be able to draw it on a chest and name its borders from memory. The anterior border is the lateral edge of pectoralis major — run your finger along the outer border of the pectoral muscle. The posterior border is the lateral edge of latissimus dorsi — the posterior axillary line, roughly. The inferior border is a horizontal line drawn at the level of the nipple — the fifth intercostal space, corresponding to the inframammary crease. The apex is the base of the axilla. The drain goes in the fourth or fifth intercostal space within that triangle, in the anterior axillary line. The mnemonic P-L-I-N (Pectoralis, Latissimus, Inferior fifth, Nipple) fixes the borders. [1]
Before incising, count the intercostal space accurately. Start at the angle of Louis (the manubrio-sternal angle), where the second rib and the second intercostal space below it are reliably found. Slide your finger down to the second space, then walk down to the fourth or fifth space, and carry the count to the anterior axillary line. Confirm the side by the clinical signs and, where time permits, by a bedside chest radiograph or lung ultrasound — a wrong-side drain is a never-event. [1]
After insertion, confirm the drain is working with three observations. Swing — the water column in the tube moves up and down with respiration — confirms the tube is in the pleural space and is patent. Bubbling — air bubbling through the water seal on expiration or cough — confirms an ongoing air leak. Drainage — fluid or blood appearing in the collection chamber — confirms the tube is in the right place for fluid. A post-insertion chest radiograph confirms the position and shows whether the lung has re-expanded. [1]
Safe triangle and the bundle rule
Investigations
No investigation is a precondition for emergency decompression — the tension pneumothorax is a clinical diagnosis and the procedure is immediate. Imaging has its place in the stable child, in confirmation after the drain is in, and in the characterisation of a pleural collection before elective drainage. [1]
The chest radiograph remains the standard confirmatory investigation for pneumothorax, effusion, empyema, and haemothorax when the child is stable enough to wait. Look for the pleural line with absent lung markings beyond it (pneumothorax), the meniscus sign or layering (effusion), an air-fluid level (hydropneumothorax or empyema), and the volume of fluid and any mediastinal shift. A supine film in the ventilated child can hide a pneumothorax — the air collects anteriorly — so look carefully or use ultrasound or CT. [9]
Bedside lung ultrasound is the imaging of choice in the ventilated neonate and is increasingly used at the bedside in the emergency department. A pneumothorax abolishes lung sliding and B-lines and shows a lung point where the pleural surfaces re-meet; an effusion or empyema appears as an anechoic or septated collection that can be measured and sampled. Ultrasound avoids ionising radiation and can guide drainage in real time. [7]
When draining an effusion or empyema, send pleural fluid for pH, glucose, lactate dehydrogenase, protein, cell count and differential, Gram stain and culture, and pneumococcal and staphylococcal PCR. In the immunocompromised or the clinically atypical, add acid-fast bacilli, fungal culture, and cytology. Blood tests — full blood count, CRP, blood cultures, and venous blood gas — frame the severity of sepsis, and a group and hold is mandatory before any drainage that may bleed. [2]
CT chest is reserved for complex, loculated empyema (to map the collection and to decide between fibrinolytics and surgery), for suspected bronchopleural fistula, and for retained haemothorax after initial drainage. It is not needed for a straightforward pneumothorax, and the radiation cost in a child is real — use it selectively. [2]
Management — Resuscitation
The resuscitation of a tension pneumothorax is the procedure itself, run in parallel with oxygen and circulation. The order matters and is the single highest-yield fact in this topic. [3] [4]
Give high-flow oxygen, secure intravenous access, support the circulation with a 10 millilitre per kilogram isotonic crystalloid bolus if the child is shocked, and decompress the chest at once. Do both at the same time — assign one team member to the airway and circulation while you decompress. The decompression is the definitive resuscitation act for this problem; the fluids and oxygen are supports that will not work until the tension is relieved. [3]
For the needle decompression, prepare a large-bore cannula — 14 or 16 gauge in the older child and adolescent, and the largest cannula that will reliably reach the pleural space in the smaller child. Choose the site by what is in front of you: the second intercostal space, mid-clavicular line (the traditional site) or the fourth or fifth intercostal space, anterior axillary line within the safe triangle (the increasingly preferred site). Insert perpendicular to the skin, advance until air rushes out (the hiss), then withdraw the needle and leave the cannula in place, securing it. [4] [5]
A hiss of air and the prompt recovery of oxygenation and blood pressure confirm the diagnosis and the benefit. But a needle decompression is only a temporising measure: the cannula kinks, blocks, or dislodges, and the tension will return. A formal intercostal drain must follow, at the safe triangle, within minutes. If the needle decompression does not work and you are still in the peri-arrest window, re-decompress at the other site or, in the ventilated child, proceed at once to a finger thoracostomy — a digital incision into the pleural space at the safe triangle that vents the air directly. [3] [10]
Lidocaine 1% (local infiltration for drain insertion)
Dose
Up to 3 milligrams per kilogram without adrenaline (up to 7 milligrams per kilogram with adrenaline). 1% lidocaine is 10 milligrams per millilitre, so 3 milligrams per kilogram equals 0.3 millilitres per kilogram of 1% solution.
Resuscitate the underlying cause in parallel. In the trauma victim, continue the ATLS primary survey and look for the other life-threats. In empyema, start intravenous antibiotics that cover Streptococcus pneumoniae and Staphylococcus aureus and send cultures. In haemothorax, cross-match blood and prepare for the possibility of thoracotomy if bleeding is heavy. [2] [11]
Management — Definitive & Stepwise
Once the resuscitation decision is made, the intercostal drain itself is eight ordered steps. Run them the same way every time, on a manikin until they are automatic, and they will stay automatic when the child is crashing in front of you. [1]
The intercostal drain procedure, in order
1 · Confirm and consent
Confirm the indication and the side with a pre-procedure pause. In an emergency, implied consent applies and you explain to parents afterwards; for an elective drain, take informed consent.
2 · Prepare and anaesthetise
High-flow oxygen, monitoring, intravenous access, sterile field, skin prep and draping. Infiltrate 1% lidocaine down to the parietal pleura (maximum 3 mg/kg without adrenaline), aspirating before each injection.
3 · Identify the safe triangle
Palpate the borders — pectoralis major anteriorly, latissimus dorsi posteriorly, the fifth intercostal space at the nipple line inferiorly, the axilla at the apex. Mark the fourth or fifth space in the anterior axillary line.
4 · Incise and dissect
Make a small horizontal incision over the rib just below the chosen space. Blunt-dissect through the intercostal muscles just above the rib below, keeping a finger over the track and sweeping the lung away.
5 · Enter the pleural space
Feel the give as the pleura is breached. Keep a gloved finger in the track to confirm entry and to sweep any adhesions before passing the drain.
6 · Pass the drain
Choose the size by content — small-bore 8 to 14 Fr pigtail for air, 16 to 24 Fr for fluid or empyema, 28 to 36 Fr for blood. Direct the tip towards the apex for air or towards the base for fluid.
7 · Connect the underwater seal
Connect immediately to a sterile underwater seal with the tube tip two centimetres below the water line. Confirm swing with respiration, bubbling if there is an air leak, and drainage of fluid.
8 · Secure and confirm
Secure the drain with a purse-string suture and a secure dressing, apply a sterile occlusive dressing, and obtain a post-procedure chest radiograph to confirm position and lung re-expansion.
A few technique points separate a clean insertion from a complication. Always insert above the rib below — the neurovascular bundle runs along the inferior border of the rib above, and a drain placed just below the rib above will hit it. Use blunt dissection, never a trocar, because a sharp trocar can stab the lung, the heart, or the great vessels; the blunt technique with a finger over the track is the safe standard. Keep a finger in the track as you pass the drain to sweep adhesions and to confirm the pleural space. Direct the drain towards the apex for air and towards the base for fluid, because that is where each collects. [1]
| Content / indication | Drain size | Technique | Notes |
|---|---|---|---|
| Pneumothorax (air) | 8 to 14 French pigtail | Seldinger | Less pain than large-bore; first-line for most pneumothoraces |
| Uncomplicated pleural effusion | 12 to 16 French pigtail or small ICC | Seldinger or blunt | Small-bore adequate unless fluid is thick |
| Empyema / complicated parapneumonic effusion | 16 to 24 French | Blunt dissection | Combine with intrapleural fibrinolytics for loculations |
| Haemothorax | 28 to 36 French | Blunt dissection | Large-bore to avoid clot blockage; measure ongoing blood loss |
| Neonatal pneumothorax (symptomatic) | 10 to 12 French pigtail | Blunt or Seldinger | Thin chest wall; use the smallest effective drain |
[1] [2] [11] Drain sizes are guides; always confirm against the current BTS and local paediatric guidance and choose the smallest drain likely to clear the material.
Specific Subtypes & Scenarios
Four scenarios recur in fellowship vivas and OSCE stations, and each carries a specific twist. The first is tension pneumothorax in trauma. The child arrives after blunt or penetrating chest injury with respiratory distress, hypoxia, and shock. The move is immediate needle decompression at the safe triangle, followed by a large-bore intercostal drain, all run in parallel with the ATLS primary survey. Look for the associated injuries — the rib fractures, the pulmonary contusion, the haemothorax, the cardiac tamponade — and reassess the drain output constantly; heavy ongoing blood loss (over 2 millilitres per kilogram per hour) is an indication for thoracotomy. [3] [11]
The second is the ventilated neonate. The premature infant on positive-pressure ventilation is the child most likely to develop tension physiology in a matter of breaths. The clue is sudden deterioration with rising airway pressures and falling saturations. For a small, asymptomatic pneumothorax, needle aspiration may suffice; for a symptomatic or tension pneumothorax, a small 10 to 12 French pigtail drain connected to a low-depth underwater seal is standard. The thin chest wall and fragile lung demand a blunt, gentle technique and the smallest effective drain. [9]
The third is primary spontaneous pneumothorax in the adolescent. The tall, thin teenager who smokes presents with sudden pleuritic chest pain and breathlessness. A small pneumothorax (under a 2 centimetre rim on the chest radiograph) with minimal symptoms may be observed or aspirated; a larger or symptomatic pneumothorax needs a small-bore intercostal drain, often a pigtail. Recurrence is common — around half after a first episode — so counsel on smoking cessation and discuss the role of elective pleurodesis after a second episode. [8]
The fourth is complicated parapneumonic effusion and empyema. The child with pneumonia that has not improved after 48 hours of antibiotics, who has a fever, pleuritic chest pain, and a loculated pleural collection, needs drainage plus intravenous antibiotics that cover pneumococcus and staph. A chest drain combined with intrapleural fibrinolytics (urokinase or tissue plasminogen activator) is effective for loculated collections; recent meta-analytic evidence supports earlier rather than later fibrinolytic use. If drainage fails or the collection is multiloculated, early video-assisted thoracoscopic surgery (VATS) is the next step. [2] [12]
[1] [9]Complications & Pitfalls
Complications are uncommon when the procedure is done well, but two of them — wrong-site insertion and bleeding from the intercostal vessels — are directly under your control and are exactly what an examiner will press. [1] [3]
Pain at insertion is the rule, not the exception: the parietal pleura and the chest wall are richly innervated, and a drain hurts. Prevent it with generous local anaesthetic (infiltrating all the way down to the pleura) and procedural sedation where the child is stable enough. The conscious child who receives no analgesia for a drain insertion has been failed. [1]
Bleeding from the intercostal artery or vein is the classic anatomical complication and is prevented by the single rule: insert above the rib below. The bundle runs in the costal groove along the inferior border of the rib above each space; a drain placed just below the rib above will hit it. Bleeding can be brisk and, in the small child, significant. If it occurs, apply pressure, transfuse as needed, and consider surgical exploration if it does not stop. [1]
Damage to the lung, diaphragm, liver, or spleen follows a sharp trocar or a drain passed too low. The preventions are blunt dissection, a finger in the track, and a site firmly within the safe triangle (above the diaphragm). A drain placed below the fifth intercostal space at the anterior axillary line risks the upper abdomen; a drain placed too medially risks the internal mammary vessels. [1]
Infection — cellulitis at the site, surgical emphysema, an infected haematoma, empyema, or systemic sepsis — is prevented by sterile technique and by removing the drain as soon as it is no longer needed. Wrong-side insertion is a never-event, prevented by a pre-procedure pause and, where time allows, a confirmatory chest radiograph. Re-expansion pulmonary oedema follows rapid drainage of a very large effusion; prevent it by controlled drainage, pausing after about 1.5 litres, and close monitoring. [1]
The mechanical complications of the drain itself — blockage, kinking, dislodgement, and malposition — are suspected when the swing, the bubbling, or the drainage disappears. Check the tube for kinks, confirm the external length has not changed, look at the chest radiograph for position, and consider whether a persistent air leak indicates a bronchopleural fistula that needs surgical review. A persistent large air leak beyond four or five days, or failure of the lung to re-expand, is the trigger to call the thoracic team. [1]
Prognosis & Disposition
A chest drain is a bridge, not a destination. Its job is to keep the pleural space decompressed and draining while the underlying lung heals — over hours for a pneumothorax, over days for an empyema. Once the lung has re-expanded and the leak or the fluid has stopped, the drain comes out. [1]
The removal criteria are three. The lung is re-expanded on the chest radiograph. There is no ongoing air leak — the drain no longer bubbles when the child breathes or coughs, and the swing is preserved. And the fluid drainage is minimal — typically under 50 to 100 millilitres per day. Satisfy all three and the drain is ready to come out. [1]
The removal technique is the inverse of the insertion: cut the purse-string, withdraw the drain in one smooth motion during a Valsalva manoeuvre in the cooperating child, or at end-expiration in the ventilated child, and tie the purse-string closed. Apply a sterile occlusive dressing and obtain a follow-up chest radiograph to confirm the lung stays up. [1]
Disposition depends on the underlying cause. A trauma victim with a drained haemothorax needs ongoing inpatient observation and the rest of the trauma work-up. A child with an empyema needs a full course of intravenous antibiotics and follow-up imaging. A small spontaneous pneumothorax in a stable adolescent may be managed as a short stay or day case. The outcome is driven by the underlying illness; the drain itself rarely determines outcome when it is placed correctly and removed early. [8] [11]
Special Populations
The neonate deserves its own paragraph. The chest wall is thin, the lung is fragile, and the trigger is usually positive-pressure ventilation in a preterm infant with respiratory distress syndrome or meconium aspiration. A symptomatic or tension pneumothorax needs a small 10 to 12 French pigtail drain connected to a low-depth underwater seal, placed by a gentle blunt or Seldinger technique. Asymptomatic small pneumothoraces may resolve without drainage; needle aspiration is an option for the borderline case. A Cochrane review found insufficient evidence to choose between aspiration and tube drainage for neonatal pneumothorax, and practice varies by unit. [9]
The adolescent with primary spontaneous pneumothorax is the other classic paediatric population. Tall, thin, often male, and often a smoker, the adolescent presents with sudden pleuritic chest pain and breathlessness. Counsel on smoking cessation, because smoking multiplies the recurrence risk. After a second episode, discuss elective pleurodesis — chemical or surgical — because recurrence approaches two-thirds after a second pneumothorax. [8]
The child with cystic fibrosis or chronic lung disease is a high-stakes subgroup. Pneumothoraces in these children are larger, often persistent, and carry a higher mortality; the threshold for a surgical opinion and pleurodesis is lower, and lung transplantation may be in the background. The immunocompromised child with a pleural effusion needs a broader differential — bacterial, fungal, mycobacterial, and malignant — and the pleural fluid must go for the full panel including acid-fast bacilli and cytology. [2]
The anticoagulated child or the child with a bleeding disorder can still have a drain in an emergency; insert it and correct the coagulopathy in parallel. For an elective drain, correct the coagulopathy first. For Aboriginal, Torres Strait Islander, Māori, and migrant and refugee children, and children in remote communities, severe pneumonia with empyema and trauma present late, and the rural and retrieval clinician who can place a chest drain in minutes converts a lethal deterioration into a survivable retrieval. Chest-drain competence in the rural and retrieval workforce is an equity issue as much as a clinical one. [2] [10]
Evidence, Guidelines & Regional Differences
The guidelines are strikingly concordant across regions. The British Thoracic Society pleural disease guideline, the BTS paediatric pleural infection guideline, ATLS, APLS, and the European Trauma Course all converge on the same two principles: immediate needle decompression for tension pneumothorax followed by a definitive intercostal drain sited in the triangle of safety, with the drain chosen by content. [1] [3]
The strongest modern debate is the decompression site. A 2025 meta-analysis of the optimal needle length and decompression site for tension pneumothorax concluded that the fifth intercostal space in the anterior axillary line outperforms the traditional second space mid-clavicular line, because the chest wall is thinner and more consistent there and the catheter is more likely to reach the pleural space. Paediatric CT and ultrasound studies of chest wall thickness in children reinforce the same conclusion, and propose the nipple line as a reliable surface landmark for the axillary site. The traditional site remains acceptable, but a fellowship candidate should know the trend and the reason. [4] [5] [6] [7]
On drain size, the BTS 2023 guideline confirms that small-bore drains are as effective as large-bore drains for pneumothorax and uncomplicated effusion and cause less pain. Large-bore drains remain standard for haemothorax and for large air leaks, where clot and viscous material block a small tube. A prospective multicentre cohort analysis of traumatic haemothorax identified the predictors of initial management failure — including a large initial volume and persistent bleeding — that should trigger a large-bore drain or surgical review. [1] [11]
On paediatric empyema, a 2026 systematic review and meta-analysis compared early and late intrapleural fibrinolytic therapy and found a benefit to earlier administration, supporting a low threshold for adding fibrinolytics to the drain once a loculated collection is recognised. The choice between primary fibrinolytics and primary VATS remains debated and partly resource-dependent. On neonatal pneumothorax, a Cochrane review found insufficient evidence to choose between needle aspiration and intercostal tube drainage, and practice varies by unit. [9] [12]
The genuine controversies are narrow. Whether finger thoracostomy should replace needle decompression in the ventilated trauma patient is actively debated, with NAEMSP and several prehospital systems moving toward finger thoracostomy as the first move in ventilated patients. Whether routine prophylactic antibiotics are needed around chest drain insertion in trauma is unsettled; most guidance does not recommend them for the routine insertion but some trauma services do. And whether a small asymptomatic pneumothorax in a stable child should be observed, aspirated, or drained is a judgement call that depends on size, symptoms, and underlying cause. [3] [10]
Exam Pearls
A fellowship candidate should leave the examiner with a small set of sharp, sourced facts. Memorise these and you will answer any question on this topic. [1] [3]
The single highest-yield fact is that tension pneumothorax is a clinical diagnosis — decompress first, radiograph afterwards, in the crashing child. The decompression site is the second intercostal space mid-clavicular line or the fourth or fifth intercostal space in the anterior axillary line within the safe triangle; the axillary site is increasingly preferred, especially in children, because the chest wall is thinner and the catheter more likely to reach the pleura. The safe triangle is fixed by the borders pectoralis (anterior), latissimus (posterior), the fifth intercostal space at the nipple line (inferior), and the axilla (apex). [1] [4]
The bundle rule is the inverse of anatomy: the neurovascular bundle runs along the inferior border of the rib above, so you insert above the rib below. Drain size follows content: 8 to 14 French pigtail for air, 16 to 24 French for fluid or empyema, 28 to 36 French for blood. The underwater seal has its tube tip two centimetres below the water line; swing means the tube is in the pleural space, bubbling means an air leak, and you never clamp a bubbling drain. [1]
For analgesia, lidocaine 1 per cent up to 3 milligrams per kilogram without adrenaline (7 milligrams per kilogram with adrenaline), aspirating before injecting, all the way down to the pleura. To prevent re-expansion pulmonary oedema, do not drain more than about 1.5 litres at once. The ventilated neonate with sudden deterioration and high airway pressures has a tension pneumothorax until proved otherwise. And remember that a needle decompression is always a bridge — the definitive step is the intercostal drain. [1] [9]
References
- [1]Roberts ME, Rahman NM, Maskell NA, et al British Thoracic Society Guideline for pleural disease Thorax, 2023.PMID 37553157
- [2]Balfour-Lynn IM, Abrahamson E, Cohen G, et al BTS guidelines for the management of pleural infection in children Thorax, 2005.PMID 15681514
- [3]Lyng JW, Ward C, Angelidis M, et al Prehospital Trauma Compendium: Traumatic Pneumothorax Care. Position Statement and Resource Document of NAEMSP Prehospital Emergency Care, 2024.PMID 39499620
- [4]Ahmad SJS, Degiannis JR, Head M, et al Meta-analysis of the optimal needle length and decompression site for tension pneumothorax and consensus recommendations on current ATLS and ETC guidelines World Journal of Emergency Surgery, 2025.PMID 40383767
- [5]Terboven T, Heblich LA, Weiss C, et al The nipple as a landmark for needle decompression of tension pneumothorax in children: a CT-based evaluation and proposal of an alternative insertion site Prehospital Emergency Care, 2021.PMID 33026282
- [6]Terboven T, Leonhard G, Wessel L, et al Chest wall thickness and depth to vital structures in paediatric patients: implications for prehospital needle decompression of tension pneumothorax Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 2019.PMID 30992028
- [7]Hossain R, Qadri U, Dembowski N, et al Sound and air: ultrasonographic measurements of pediatric chest wall thickness and implications for needle decompression of tension pneumothorax Pediatric Emergency Care, 2021.PMID 32925707
- [8]Speck KE, Kulaylat AN, Baerg JE, et al Evaluation and management of primary spontaneous pneumothorax in adolescents and young adults: a systematic review from the APSA Outcomes and Evidence-Based Practice Committee Journal of Pediatric Surgery, 2023.PMID 37130765
- [9]Bruschettini M, Romantsik O, Zappettini S, et al Needle aspiration versus intercostal tube drainage for pneumothorax in the newborn Cochrane Database of Systematic Reviews, 2019.PMID 30707441
- [10]Boever JC, Ott MJ, Muldiiarov V, et al Prehospital needle thoracostomy and the need to implement objective criteria for intervention: a retrospective study Injury, 2026.PMID 41436345
- [11]Beyer CA, Byrne JP, Moore SA, et al Predictors of initial management failure in traumatic hemothorax: a prospective multicenter cohort analysis Surgery, 2023.PMID 37500410
- [12]Kaur D, Kumar K, Mishra P, et al Early versus late(r) administration of intrapleural fibrinolytic therapy in children with empyema: a systematic review and meta-analysis Indian Pediatrics, 2026.PMID 42430023