Paeds · investigations-procedures-and-technology
Developmental, cognitive and behavioural assessment tools
Also known as Developmental screening · Cognitive assessment · Bayley Scales · Ages and Stages Questionnaire · M-CHAT-R/F · Strengths and Difficulties Questionnaire · Developmental surveillance
A fellowship approach to the developmental, cognitive and behavioural assessment tools used across childhood, built on the single principle that surveillance, screening and diagnostic assessment are three different acts answering three different questions. Surveillance is the longitudinal, opinion-based monitoring done at every health visit. Screening is a brief, standardised tool applied to the whole population at scheduled ages to find the child who needs a closer look. Diagnostic assessment is the lengthy, trained-administered evaluation that confirms and quantifies a disorder. Hold the schedule of developmental screen at nine, 18 and 30 months and autism screen at 18 and 24 months, layered on surveillance at every visit. Know the broadband developmental screens (Ages and Stages Questionnaires, Parents' Evaluation of Developmental Status, Denver II), the gold-standard cognitive tools (Bayley, Griffiths, Wechsler), the autism screen (M-CHAT-R/F, CHAT) and the behavioural scales (Strengths and Difficulties Questionnaire, Child Behavior Checklist, Vanderbilt, Conners). Hold the psychometric model: standard score mean 100, standard deviation 15, a score of 70 or below two standard deviations below the mean; developmental quotient equals developmental age divided by chronological age times 100. A positive screen is never a diagnosis; low prevalence lowers positive predictive value, so diagnostic confirmation always follows. Always check hearing and vision, because sensory impairment is the reversible mimic, and escalate regression or loss of any skill to urgent diagnostic referral.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture an eighteen-month-old whose mother says he has no words and does not point. Your job is not to label him at the desk; it is to choose the right instrument for the right question, and to know what its number means. That choice — and the honest interpretation that follows — is what this topic tests. [1]
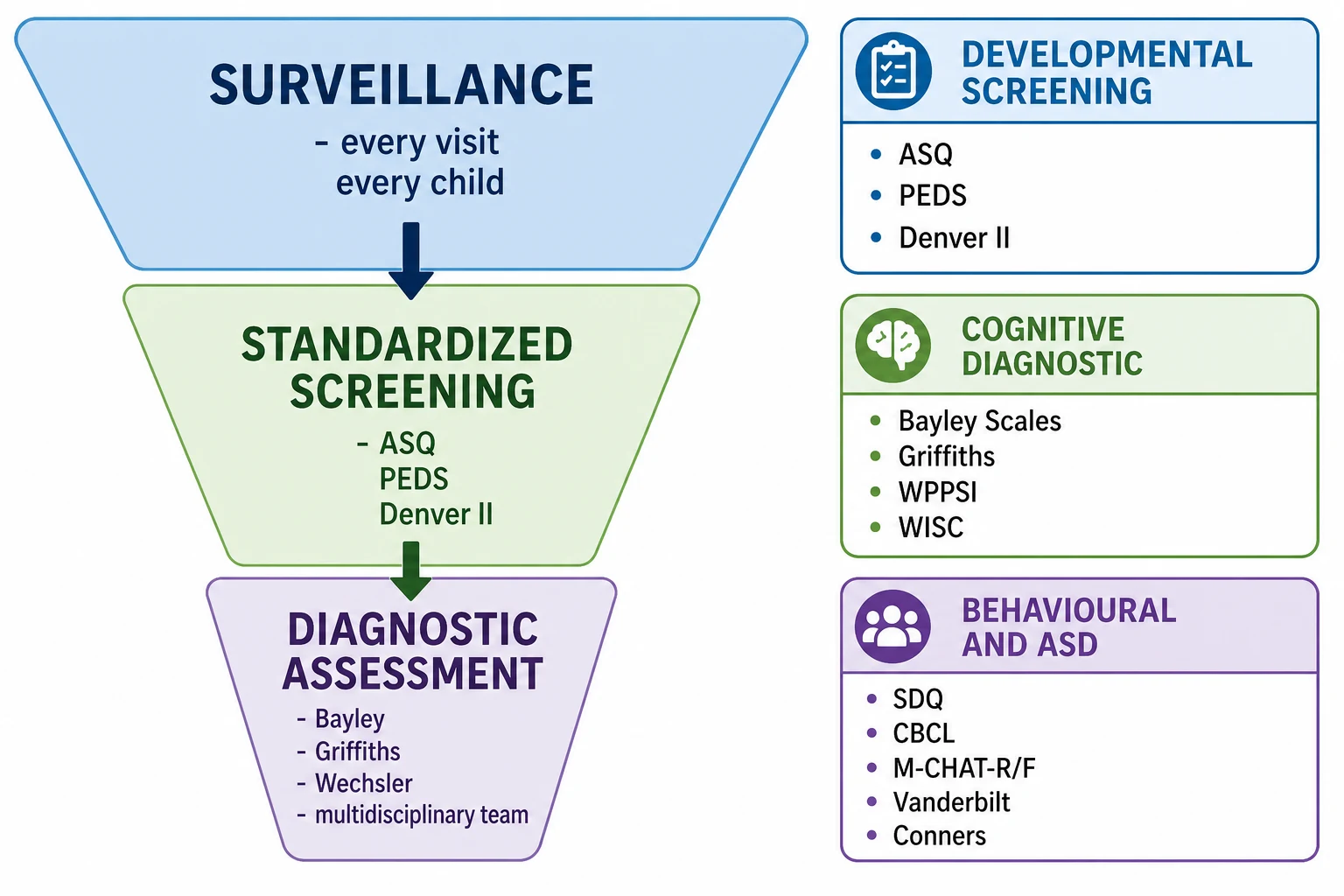
The single idea that holds the whole topic together is that surveillance, screening and diagnostic assessment are three different acts. Surveillance is the longitudinal, opinion-based monitoring you perform at every health contact: you take the history, observe the child at play, elicit the parent's concerns, and follow the trajectory over time. Screening is a brief, standardised tool you apply to the whole population at scheduled ages, whether or not anyone is worried, to find the child who needs a closer look. Diagnostic assessment is the lengthy, trained-administered evaluation that confirms and quantifies a disorder. A screening tool is fast and population-scale; a diagnostic tool is slow and individual; and a screen can never do the diagnostic tool's job. [1]
The reason a fellowship candidate must hold all three at once is that they fail in predictable ways when confused. Treating a screen as a diagnosis over-labels a well child whose false-positive score sits in a low-prevalence population; treating surveillance as a screen misses the child whose clinician's "gut feeling" reassured everyone but never put a number on the concern; and skipping the diagnostic step leaves a family with a worry and no answer. The schedule, the tools and the psychometric model exist to keep these three acts in their lanes. [10]
Classification
Sort the tools along two axes: the question they answer, and the person who answers it. Both matter, because a tool's accuracy depends on who gives it and what you are looking for. [1]
By question, the tools fall into three families. The broadband developmental screens look for delay across the milestone domains: the Ages and Stages Questionnaires (ASQ-3), the Parents' Evaluation of Developmental Status (PEDS) and the Denver II. The gold-standard cognitive and developmental assessments confirm and quantify delay and ability: the Bayley Scales of Infant and Toddler Development, the Griffiths Mental Development Scales, and the Wechsler scales (WPPSI for preschool children, WISC for school-age). The behavioural and autism-specific scales measure behaviour, emotion and social communication: the Strengths and Difficulties Questionnaire and the Child Behavior Checklist as broadband measures, the M-CHAT-R/F for autism, and the Vanderbilt and Conners scales for ADHD. [3] [5]
By informant, the broadband screens are mostly parent-completed — ASQ, PEDS, SDQ, M-CHAT-R — which is what makes them fast enough for a population schedule, while the diagnostic tools are directly administered by a trained psychometrist or developmental paediatrician under standardised conditions. A parent-completed tool trades a little precision for reach; a directly administered tool trades reach for the precision a diagnosis needs. [9]
Epidemiology & Risk Factors
Developmental and behavioural difficulty is common, and that fact is the whole rationale for screening an apparently well population. Around one in six children has a developmental disability, so waiting to assess only the children someone happens to worry about detects far fewer than a scheduled screen. [1]
The children who need formal assessment cluster around a few presentations and a few risk factors. The presentations are the parental or professional concerns: delayed speech, not walking, not pointing, poor social engagement, behaviour that is hard to manage, or a child struggling at school. The risk factors are prematurity and very low birthweight, socio-economic disadvantage, parental mental ill-health, hearing or vision impairment, a neurogenetic syndrome, in-utero alcohol or toxin exposure, and a family history of autism, intellectual disability or learning difficulty. [9]
A single epidemiological fact governs how you read a screening result: the positive predictive value of a screen falls as the prevalence falls. In a general-practice population the chance that any one screen-positive child truly has the disorder is modest, because well children outnumber unwell children by a wide margin. That is why a positive screen is a reason to refer, not a reason to label — the diagnostic step exists to separate the true from the false positive. [10]
General-practice population
Low prevalence, routine screen
- Whole-population screen at 9, 18 and 30 months plus autism at 18 and 24 months
- Modest positive predictive value — most screen-positives are false positives
- Parent-completed broadband screens (ASQ, PEDS) are fast and reach every child
- A positive screen triggers referral, not a diagnosis
High-risk follow-up clinic
Premature, VLBW, post-encephalopathy
- Higher prevalence raises positive predictive value
- Go straight to a diagnostic tool (Bayley at corrected age) rather than relying on a screen
- Scheduled Bayley assessment drives early-intervention and school-support planning
- Interpret the first two years against corrected age
Referred developmental clinic
Concern already raised
- Diagnostic assessment is the task, not re-screening
- Bayley, Griffiths or Wechsler confirm and quantify, plus audiology and vision
- Multidisciplinary team assembles the developmental, medical and family picture
- Regression or loss of skill is escalated the same day
Pathophysiology
There is no disease mechanism in this topic; the "mechanism" is the psychometric model that lets a tool convert a child's observed behaviour into a number comparable to other children of the same age. Once you hold that model, every tool in the topic reads the same way. [7]
The standard-score model is the spine of cognitive assessment. A standard cognitive score has a mean of 100 and a standard deviation of 15, so the average child scores near 100, about two-thirds of children score between 85 and 115, and a score of 70 or below sits two standard deviations below the mean and marks significant concern. Subtest scaled scores use a smaller version of the same model, with a mean of 10 and a standard deviation of 3. The developmental quotient (DQ) is the older, simpler relative of the standard score: it equals developmental age divided by chronological age times 100, so a DQ below 70 means the child is performing below two standard deviations and flags global developmental delay or intellectual disability in the young child. [9]
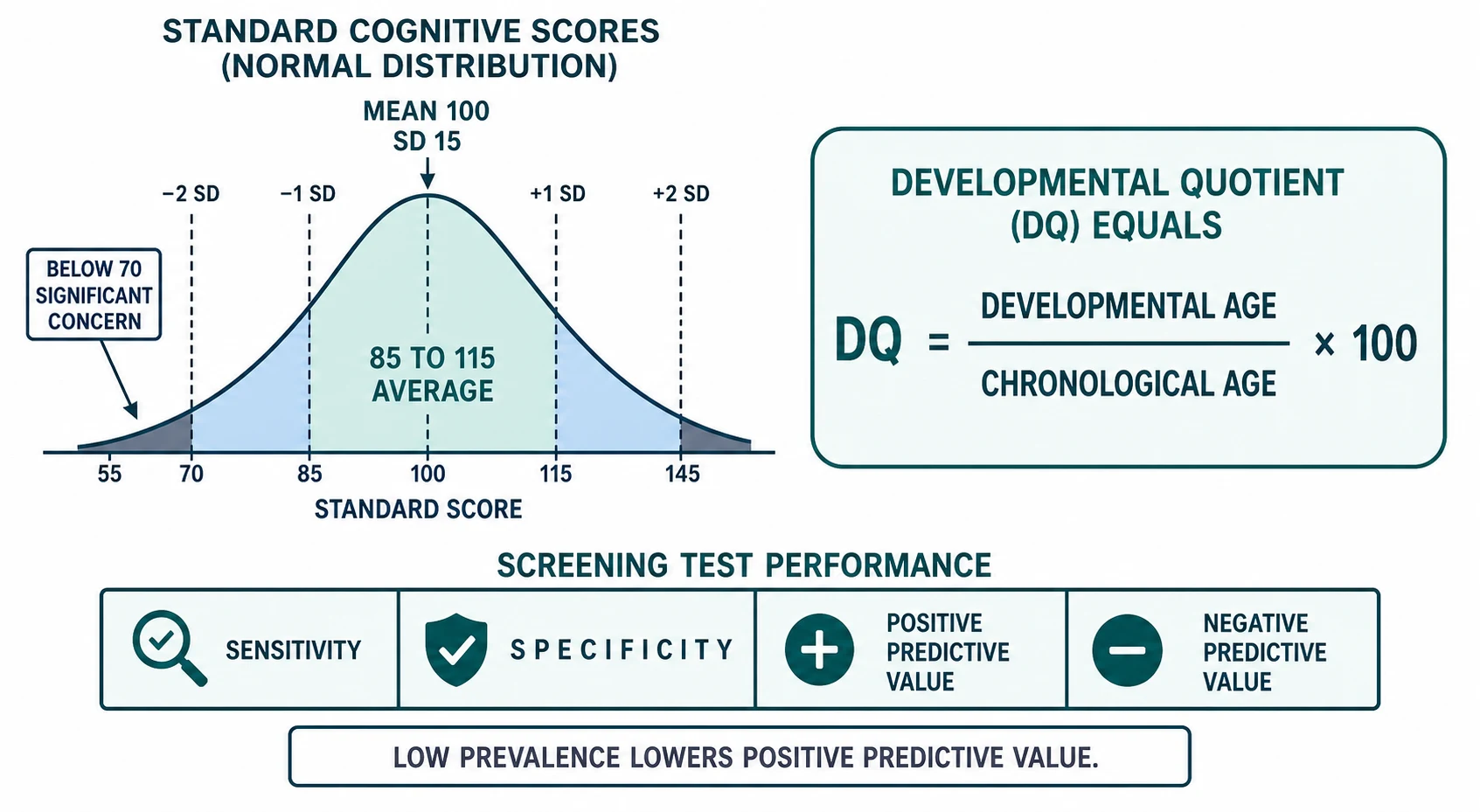
The screening-test model explains why a screen and a diagnostic test behave so differently. A screen is governed by its sensitivity (the proportion of truly delayed children it flags) and its specificity (the proportion of typically developing children it passes), and by the prevalence-dependent positive and negative predictive values. In a low-prevalence general-practice population, even a sensitive screen generates many false positives, because there are far more well children than unwell children. A diagnostic tool minimises both errors by using standardised administration, basal and ceiling rules, and age-stratified norms — which is exactly why a screen cannot stand in for a Bayley or a Wechsler when a diagnosis is needed. [10]
Clinical Presentation
A child rarely arrives asking for an assessment. The presentation is the concern that surfaces in the consultation — the parent's worry, the nurse's observation, the teacher's note — and the act of assessment is what you do next. [1]
The classic triggers for a developmental screen are the missed milestones on surveillance, the parent who reports that the child is not talking or not walking, and the routine nine, 18 and 30 month screening visits. The classic triggers for an autism-specific screen are the social-communication concerns: poor eye contact, no pointing or joint attention by around 12 to 15 months, no words by 18 months, or any loss of social or language skill. These trigger an M-CHAT-R/F and an audiology check, and they are not reassuring variants to watch. [5]
The behavioural presentation is different in kind. Here the concern is function: inattention, impulsivity and hyperactivity that impair the child across home and school, or emotional and conduct difficulty that is hard to manage. The informant is usually the parent and the teacher together, because behaviour that impairs in only one setting is not the same as behaviour that impairs everywhere — a distinction the ADHD scales are built to capture. [8]
Differential Diagnosis
The differential here is not of a procedure but of a concern: a failed screen or a parental worry has a list of possible causes, and the assessment separates them. Hold two differentials — the differential of a failed developmental screen, and the differential of a positive behavioural screen. [1]
The differential of a failed developmental screen splits into the causes of delay. Global developmental delay — delay in two or more domains — often reflects an intellectual disability or a static encephalopathy and needs a diagnostic cognitive assessment plus a directed work-up for an underlying cause. Isolated speech and language disorder affects communication with otherwise typical development and needs audiology first. Autism spectrum disorder presents with social-communication impairment and restricted, repetitive behaviour, often alongside language delay. Motor disorder — cerebral palsy, a neuromuscular condition — shows in the motor domain. And sensory impairment, hearing loss or a refractive error, mimics language and social delay and is reversible, which is why audiology and vision belong in every work-up. [9]
The differential of a positive behavioural screen localises the concern to its domain. ADHD shows as inattention and hyperactivity impairing function across settings, documented by parent and teacher scales. An emotional disorder — anxiety or depression — shows on the emotional scale of a broadband tool. Conduct disorder shows on the conduct scale. Autism can present first as behaviour that is hard to manage. And an unrecognised learning or sensory problem can drive the behaviour, which is why a behavioural screen is a starting point, not an endpoint. [7] [8]
Clinical & Bedside Assessment
Before you reach for a tool, take the developmental history and watch the child. The tool objectifies what you find; it does not replace the finding. [1]
The history is the milestones, the trajectory, and any regression. Ask whether the child has lost any skill, because regression changes the urgency. Take the perinatal and family history — prematurity, neonatal encephalopathy, a family history of autism, intellectual disability or learning difficulty — and ask what the parent, the teacher or the child-health nurse sees in different settings, because a child who functions differently in different places is telling you something. [5]
Observe the child directly, because unstructured play reveals more than a single test item. Watch how the child communicates, attends and moves, how they relate to the parent, and how they approach a novel toy. Then choose the right tool for the question: a broadband developmental screen (ASQ, PEDS) for general delay, the M-CHAT-R/F for autism concern, the SDQ or CBCL for emotional and behavioural concern, and the Vanderbilt or Conners for ADHD — and refer for Bayley, Griffiths or Wechsler when a diagnosis and a number are needed. [3] [7]
Choose the right tool for the question
Investigations
In developmental and behavioural assessment, the "investigation" is the standardised tool itself. Choosing the right one and reading its number is the act. [1]
The broadband developmental screens sit at the population level. The Ages and Stages Questionnaires (ASQ-3) are parent-completed for ages one to 66 months across five domains — communication, gross motor, fine motor, problem-solving and personal-social — with cut-offs near two standard deviations below the mean. The Parents' Evaluation of Developmental Status (PEDS) elicits ten parental concerns across nought to eight years and maps them to risk paths. The Denver II is directly administered across birth to six years in four domains — personal-social, fine motor, language and gross motor — but its real-world sensitivity is variable, which is why the parent-completed screens have largely displaced it in many services. [2] [3] [4]
The gold-standard cognitive and developmental assessments sit at the diagnostic level. The Bayley Scales of Infant and Toddler Development (Bayley-4) are the reference standard for infants and toddlers up to 42 months, yielding cognitive, language and motor composites on the standard-score model (mean 100, standard deviation 15). The Griffiths Mental Development Scales and the Wechsler scales — WPPSI for the preschool child, WISC for the school-age child — are the diagnostic standards for the older child. A 2024 systematic review and meta-analysis compared parent and caregiver-completed screening tools with Bayley as the reference standard and supported their use as screens, not as substitutes for the diagnostic assessment. [9]
The autism-specific screens are narrower. The M-CHAT-R/F is a 20-item parent report for ages 16 to 30 months: a child screens positive if they fail three or more of the twenty items, or two or more critical items, and the Follow-Up Interview then confirms the risk and lowers the false-positive rate. The CHAT is the earlier, lower-sensitivity 18-month instrument that showed autism could be flagged in toddlers but missed many cases. [5] [6]
| Tool | Question it answers | Informant and age range | Role |
|---|---|---|---|
| ASQ-3 | Broadband developmental delay | Parent-completed, 1 to 66 months | Screening |
| PEDS | Broadband developmental and behavioural risk | Parent-completed, 0 to 8 years | Screening |
| Denver II | Broadband developmental delay | Clinician-administered, birth to 6 years | Screening |
| Bayley-4 | Confirm and quantify infant cognitive, language, motor ability | Psychometrist, up to 42 months | Diagnostic |
| Griffiths, Wechsler (WPPSI, WISC) | Confirm and quantify cognitive ability | Psychometrist, preschool to school-age | Diagnostic |
| M-CHAT-R/F | Autism risk | Parent-completed, 16 to 30 months | Screening |
| SDQ | Broadband emotional and behavioural | Parent, teacher, self, 3 to 17 years | Screening |
| CBCL | Broadband behavioural syndromes | Parent, 1.5 to 18 years | Screening |
| Vanderbilt, Conners | ADHD symptoms and impairment | Parent and teacher, school-age | Screening |
The behavioural scales complete the set. The Strengths and Difficulties Questionnaire (SDQ) is a free, 25-item broadband measure for ages three to 17 years with five subscales — emotional, conduct, hyperactivity, peer problems and prosocial — each scored nought to ten, completed by parent, teacher and, in the older child, self-report. The Child Behavior Checklist (CBCL) gives broadband and syndrome T-scores (mean 50, standard deviation 10). The Vanderbilt and Conners scales are the disorder-specific ADHD measures, used with parent and teacher informants to document impairment across home and school. [7] [8]
Two investigations belong in every developmental work-up regardless of the screen result. Audiology and vision assessment must be checked in any child who fails a developmental or autism screen, because unrecognised hearing loss or refractive error is a reversible mimic of language, social and behavioural delay. Sending a child for cognitive assessment before audiology is to investigate in the wrong order. [6]
Management — Resuscitation
There is no acute resuscitation in this topic; the immediate act is the correct response to a raised concern. Do not dismiss a parental worry, complete a structured screen, and escalate regression or loss of skills the same day to diagnostic referral. [1]
The immediate safety-net is urgency. A child with loss of language, social or motor skill, or with no social engagement, needs urgent referral for diagnostic developmental and autism assessment plus audiology, not a wait-and-see at the next routine visit. The window for early intervention in autism and developmental disorder is real, and delay at this point is the avoidable harm. [5]
Communicate the result honestly. Explain that a positive screen is not a diagnosis but a reason to look further, and arrange the diagnostic assessment, the hearing and vision check, and the early-intervention referral while the work-up proceeds. Begin non-directive support at once: refer to early intervention — speech, occupational and physiotherapy — on the basis of need, because intervention does not have to wait for a confirmed diagnosis, and parental support and education begin at the first visit. [1] [9]
Management — Definitive & Stepwise
Once the concern is raised and the immediate safety-net is in place, the work runs in six ordered steps. Run them the same way every time, so that no child is lost between a screen and a diagnosis. [1]
The developmental assessment pathway, in order
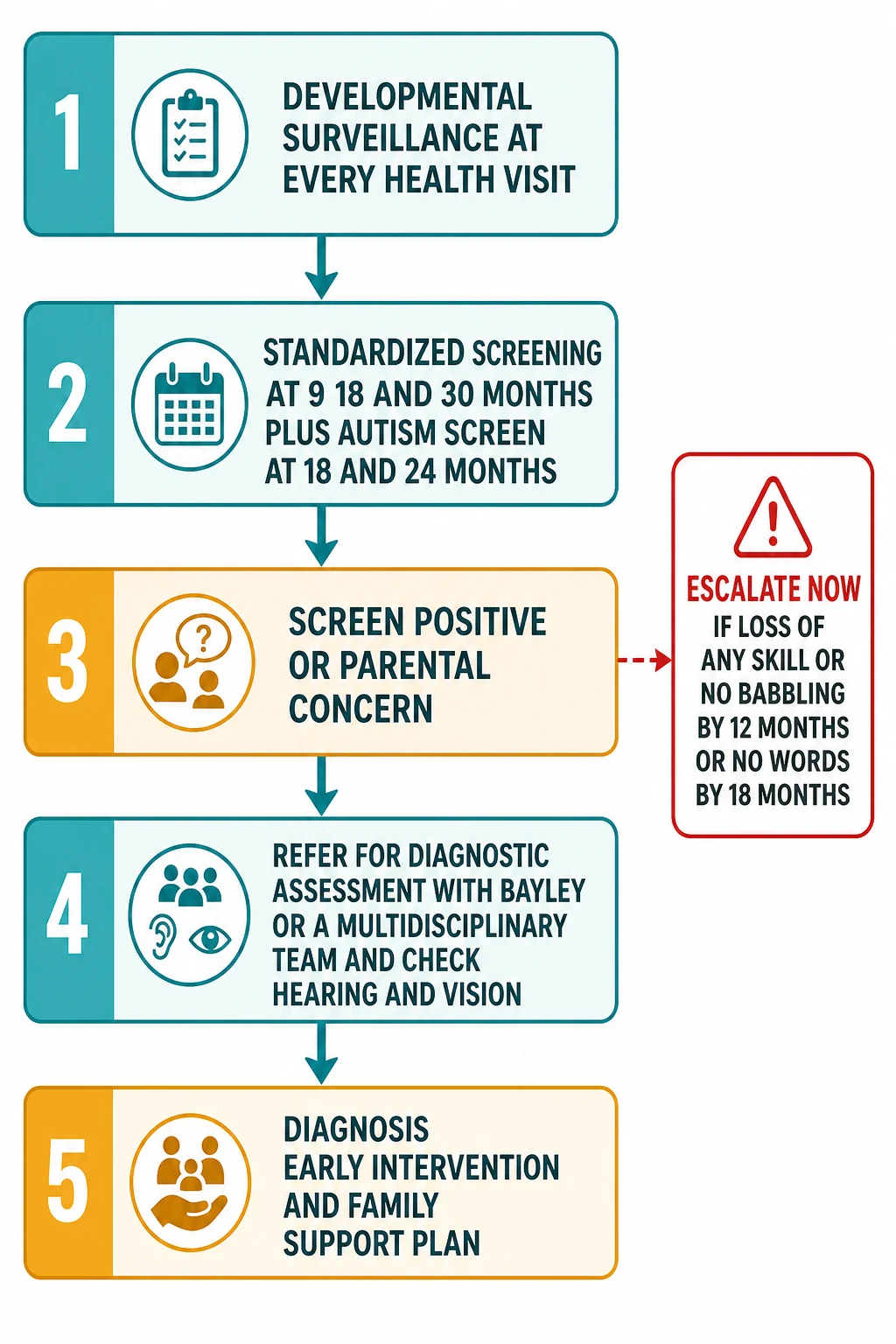
1 · Surveillance at every health visit
Take the history, observe the child at play, elicit the parental concern, and record the milestones and trajectory over time. Surveillance is the foundation on which screening is layered, and it happens at every contact, not only at scheduled screens.
2 · Standardised screening at scheduled ages
Perform a broadband developmental screen at nine, 18 and 30 months and an autism-specific screen (M-CHAT-R/F) at 18 and 24 months, in addition to ongoing surveillance. The scheduled screen reaches the children no one is yet worried about.
3 · Act on a positive screen or concern
Repeat or confirm the screen if there is doubt, check hearing and vision, and refer for diagnostic cognitive assessment (Bayley, Griffiths or Wechsler) and multidisciplinary evaluation. A screen-negative child with a persistent parental concern is still referred.
4 · Diagnostic assessment by a trained team
The psychometrist or developmental paediatrician administers the gold-standard tool under standardised conditions and reports a standard score, a confidence interval and a clinical interpretation, assembled with the medical, audiology and family picture.
5 · Diagnosis, early intervention and family support
Communicate the diagnosis, link the family to early-intervention and education services, and set up longitudinal monitoring. Needs change as the child grows, and the school transition often unmasks learning difficulty.
6 · Re-screen and re-assess over time
Development and behaviour change, a single score is a snapshot, and repeat assessment guides whether intervention is working and whether new concerns have emerged. The pathway is longitudinal, not a single encounter.
A few points separate a pathway that works from one that loses children. Surveillance is continuous, so a missed screen at one visit is caught at the next by the watchful clinician. A positive screen is a referral, not a label, so the diagnostic step is never optional in a low-prevalence population. And intervention does not wait for a diagnosis, so speech, occupational and physiotherapy are started on need while the work-up proceeds, because earlier intervention improves outcome. [10]
Specific Subtypes & Scenarios
Six scenarios recur in fellowship vivas and OSCE stations, and each turns on a single decision. The first is the child with global developmental delay — delay in two or more domains before the age of five. This child needs a broadband screen, then a Bayley or Griffiths diagnostic assessment, audiology and vision, and a directed work-up for an underlying cause. The number from the diagnostic tool, read with the medical picture, places the child in the right diagnostic and support box. [9]
The second is the child with isolated speech and language delay. Here audiology comes first, because hearing loss is the reversible mimic of language delay; then a language-specific assessment follows. An M-CHAT-R/F is added if any social-communication concern coexists, because autism presents with language delay and a language-only lens will miss it. [5]
The third is the child with autism spectrum disorder concern. The M-CHAT-R/F screens at 18 and 24 months, and a positive screen plus clinical concern triggers a diagnostic autism assessment — using instruments such as the ADOS and the ADI-R — and early intervention. Earlier intervention improves outcome, which is the entire rationale for the universal autism screen. [5] [6]
The fourth is the child with ADHD concern. When inattention or hyperactivity impairs function across home and school, use the parent and teacher Vanderbilt or Conners scales to document cross-setting impairment, then apply the diagnostic criteria. Behaviour that impairs in only one setting is not the same as behaviour that impairs everywhere, and the dual-informant scales are built to make that distinction. [8]
The fifth is the child with a behavioural or emotional concern. Use the broadband SDQ or CBCL to localise the problem to an emotional, conduct, hyperactivity or peer domain, then target the assessment and intervention to that domain rather than treating "behaviour" as a single thing. [7]
The sixth is the high-risk infant — premature, very low birthweight, or post-neonatal encephalopathy. Scheduled Bayley assessment at corrected age detects the cognitive and motor deficits that drive early-intervention and school-support planning, with scores interpreted against corrected age in the first two years. [9]
Complications & Pitfalls
The complications here are errors of reasoning, and the candidate must be able to name and avoid each one, because the harm is a child assessed late or labelled wrong. [1]
The first error is equating a screen with a diagnosis. A positive screen is a reason to refer, not a diagnosis, and a near-normal screen in a child with parental concern or regression does not exclude disorder. The corrective action is the diagnostic step, every time. [10]
The second is relying on informal clinical impression alone. Clinician judgement without a structured screen misses more children than it catches, and it is the commonest reason a developmental disorder is detected late. The corrective action is to layer a standardised screen onto surveillance at the scheduled ages. [11]
The third is forgetting hearing and vision. Unrecognised sensory impairment is a reversible mimic of developmental and behavioural delay, and a child sent for cognitive assessment before audiology is investigated in the wrong order. The corrective action is to check hearing and vision in every child who fails a screen. [6]
The fourth is applying a tool outside its age range or without standardised administration, which invalidates the score. Standard scores depend on correct basal and ceiling administration and on age-stratified norms, so a tool given outside its range produces a number that means nothing. The fifth is treating a single score as a fixed destiny: cognitive and behavioural scores are snapshots that respond to intervention, illness, sleep, mood and rapport, and must be read in context. [9]
Prognosis & Disposition
A screening result does not determine prognosis; the diagnosis, the underlying cause, the age at intervention and the child's environment together determine outcome. The tools set the child on the pathway; they do not predict its end. [1]
Earlier detection and earlier intervention improve outcome in autism, speech and language disorder, and global developmental delay, which is the entire rationale for routine surveillance and scheduled screening. A child whose delay is found at 18 months and supported from 19 months has a different trajectory from one whose delay is found at school entry, and the assessment pathway exists to make that difference. [5]
Disposition follows the pathway. A screen-positive child is referred for diagnostic assessment, audiology and vision, and early intervention while the work-up proceeds. A screen-negative child with a persistent parental concern is still referred, because the parent knows the child best. Long-term monitoring is essential, because needs change with age, the school transition unmasks learning difficulty, and repeat assessment guides whether intervention is working and whether the family needs more support. [9]
Special Populations
The high-risk infant — premature, very low birthweight, or post-neonatal encephalopathy — is assessed on a scheduled pathway. Bayley assessment at corrected age detects the cognitive and motor deficits that drive early intervention, and the first two years are interpreted against corrected age, not chronological age, so that prematurity is not mistaken for delay. [9]
The child with established disability and neurodiversity needs an assessment that focuses on function, strengths and support needs rather than a single deficit score. The tools are chosen to be accessible to the child's communication and motor profile, and the goal is a support plan, not a rank. [7]
The child from a culturally and linguistically diverse background needs tools that account for language and cultural context. Norms derived from one population may not transfer to another, so a single low score is not over-interpreted; an interpreter and a cultural broker are part of the assessment, and the clinical picture, not the number alone, carries the decision. [11]
For Aboriginal, Torres Strait Islander, Māori, and rural or remote children, coordinate screening through the child-health schedule — such as the Well Child Tamariki Ora schedule — use telehealth-supported assessment where distance is a barrier, and address access and equity so that distance does not delay detection. The child in out-of-home care, and the child exposed to adversity, carries a high burden of developmental and behavioural difficulty, and developmental and behavioural screening is part of the health assessment for these children. [1]
The adolescent is reached by extending the behavioural and emotional tools into this age: the SDQ self-report, and depression and anxiety scales, carry the assessment forward, and transition planning carries cognitive and learning assessments into adult services. [7]
Evidence, Guidelines & Regional Differences
The guidelines are strikingly concordant across regions on the structure, if not on every detail. The AAP algorithm recommends developmental surveillance at every visit plus standardised screening at nine, 18 and 30 months and autism screening at 18 and 24 months, and this structure is mirrored across the ANZ, UK and Canadian child-health schedules. [1]
The strongest recent evidence concerns how these tools perform in the real world. A 2023 meta-analysis of the real-world accuracy of children's developmental screening tests found that pooled sensitivity and specificity varied widely by tool and setting and were lower than the developers' figures — a finding that underlines the gap between a validation study and a busy clinic. A 2024 systematic review and meta-analysis compared parent and caregiver-completed screening tools with Bayley as the reference standard and supported their use as screens, not as substitutes for diagnostic assessment. [9] [10]
The Denver II has well-documented variable real-world sensitivity and has been criticised for both over-referral and under-referral, which is why the broadband parent-completed tools such as ASQ and PEDS have largely displaced it in many services. [2] [11]
[1] [10]The genuine controversies are narrow. Whether universal autism screening at 18 and 24 months reduces long-term harm is unsettled — the US Preventive Services Task Force found insufficient evidence to assess the balance of benefit and harm of universal autism screening in low-risk toddlers, even as the AAP continues to recommend it. The optimal interval for repeat screening, and how best to adapt norms to culturally and linguistically diverse populations, remain open questions. What is settled is the structure: surveillance at every visit, scheduled screening, and diagnostic confirmation of every positive screen. [5]
Exam Pearls
A fellowship candidate should leave the examiner with a small set of sharp, sourced facts. Memorise these and you will answer any question on this topic. [1]
Three acts, three questions. Surveillance is longitudinal and every visit; screening is brief, standardised and scheduled; diagnostic assessment is lengthy, gold-standard and confirms the disorder. A positive screen is a referral, never a diagnosis. [10]
The schedule: developmental surveillance at every visit, plus a standardised developmental screen at nine, 18 and 30 months and an autism screen at 18 and 24 months. The broadband developmental screens are the ASQ-3 (parent-completed, one to 66 months, five domains), PEDS (parent-completed, nought to eight years, ten concerns) and the Denver II (directly administered, birth to six years, variable sensitivity). [2] [3]
The standard-score model: mean 100, standard deviation 15; a score of 70 or below is two standard deviations below the mean and marks significant concern; the developmental quotient equals developmental age divided by chronological age times 100. The Bayley-4 is the gold-standard infant and toddler tool to 42 months; Griffiths and the Wechsler scales (WPPSI, WISC) are the diagnostic standards for the older child. [9]
The M-CHAT-R/F is a 20-item parent report for 16 to 30 months; screen-positive if three or more items failed or two or more critical items failed, confirmed by the Follow-Up Interview. The SDQ is free, 25 items, three to 17 years, five subscales scored nought to ten each. Always check hearing and vision in any child who fails a screen. Regression or loss of any skill is a red flag and demands urgent diagnostic referral, not a repeat screen. [5] [7]
References
- [1]Council on Children With Disabilities, Section on Developmental Behavioral Pediatrics, Bright Futures Steering Committee, et al Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening Pediatrics, 2006.PMID 16818591
- [2]Frankenburg WK, Dodds J, Archer P, Shapiro H, Bresnick B The Denver II: a major revision and restandardization of the Denver Developmental Screening Test Pediatrics, 1992.PMID 1370185
- [3]Squires J, Bricker D, Potter L Revision of a parent-completed development screening tool: Ages and Stages Questionnaires Journal of Pediatric Psychology, 1997.PMID 9212550
- [4]Glascoe FP Parents' evaluation of developmental status: how well do parents' concerns identify children with behavioral and emotional problems? Clinical Pediatrics, 2003.PMID 12659386
- [5]Robins DL, Casagrande K, Barton M, Chen CM, Dumont-Mathieu T, Fein D Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F) Pediatrics, 2014.PMID 24366990
- [6]Baird G, Charman T, Baron-Cohen S, Cox A, Swettenham J A screening instrument for autism at 18 months of age: a 6-year follow-up study Journal of the American Academy of Child and Adolescent Psychiatry, 2000.PMID 10846303
- [7]Goodman R Psychometric properties of the strengths and difficulties questionnaire Journal of the American Academy of Child and Adolescent Psychiatry, 2001.PMID 11699809
- [8]Wolraich ML, Lambert W, Doffing MA, Bickman L Psychometric properties of the Vanderbilt ADHD diagnostic parent rating scale in a referred population Journal of Pediatric Psychology, 2003.PMID 14602846
- [9]Balasubramanian H, Ahmed J, Ananthan A, Srinivasan L Comparison of parent or caregiver-completed development screening tools with Bayley Scales of Infant Development: a systematic review and meta-analysis Archives of Disease in Childhood, 2024.PMID 38811056
- [10]Rah SS, Jung M, Lee K, Kang H Systematic Review and Meta-analysis: Real-World Accuracy of Children's Developmental Screening Tests Journal of the American Academy of Child and Adolescent Psychiatry, 2023.PMID 36592715
- [11]Arefadib N, Stewart B, Crespo-Gonzalez C, Coghill D Umbrella Review and Meta-Analysis: Screening Tools for the Identification of Developmental Delay in Early Childhood Journal of the American Academy of Child and Adolescent Psychiatry, 2026.PMID 40975434