Paeds · investigations-procedures-and-technology
Endotracheal intubation and emergency airway equipment
Also known as Endotracheal tube · ETT placement · Paediatric intubation · Rapid sequence intubation · Definitive airway
A fellowship approach to endotracheal intubation and emergency airway equipment in children covering the indication (respiratory failure, loss of airway reflexes, severe shock, cardiac arrest), the age-based tube sizing formulas (uncuffed internal diameter equals age divided by 4 plus 4, cuffed equals age divided by 4 plus 3.5, depth at the lips equals age divided by 2 plus 12), the straight Miller blade for infants versus the curved Macintosh blade for older children, the infant airway anatomy that drives technique, the seven-step rapid sequence intubation procedure, the role of video laryngoscopy, waveform capnography as the standard for confirming tracheal placement, and the prevention of hypoxia, oesophageal intubation, right main bronchus intubation and post-extubation stridor.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a four-year-old brought to the emergency department with severe bacterial tracheitis, drooling, sitting forward, retracting hard, and now beginning to get drowsy. The airway that was holding is about to be lost. Endotracheal intubation is the act that converts that closing airway into a secured one: a tube passed through the mouth, between the vocal cords and into the trachea, so that the airway is open, protected from aspiration, and connected to a ventilator. It is the definitive airway. [9] [11]
The reason a clinician reaches for the tube is that the alternatives have run out. A bag-mask keeps most sick children alive while you prepare, but it does not protect the lungs from vomit, it fatigues the operator, and it cannot deliver high airway pressures reliably. A laryngeal mask airway rescues the cannot-intubate-cannot-ventilate child, but it is not a definitive airway. Only a tube through the cords does all three jobs at once — opens, protects, and ventilates. [9] [10]
The skill is taught the same way across Australia and New Zealand, the United Kingdom and North America: a structured rapid sequence intubation, rehearsed on a manikin until the steps are automatic, with waveform capnography as the non-negotiable confirmation. The fellowship candidate is expected to know when to intubate, how to size the tube and choose the blade, how to perform the procedure, and — above all — how to prevent the two complications that kill children: hypoxia and an unrecognised tube in the oesophagus. [5] [11]
Classification
Hold two classifications in mind at once: the tube you choose and the device you use to see the cords. The two interact, because the tube must be small enough for the airway but the device must be the right shape for the child's anatomy. [1] [11]
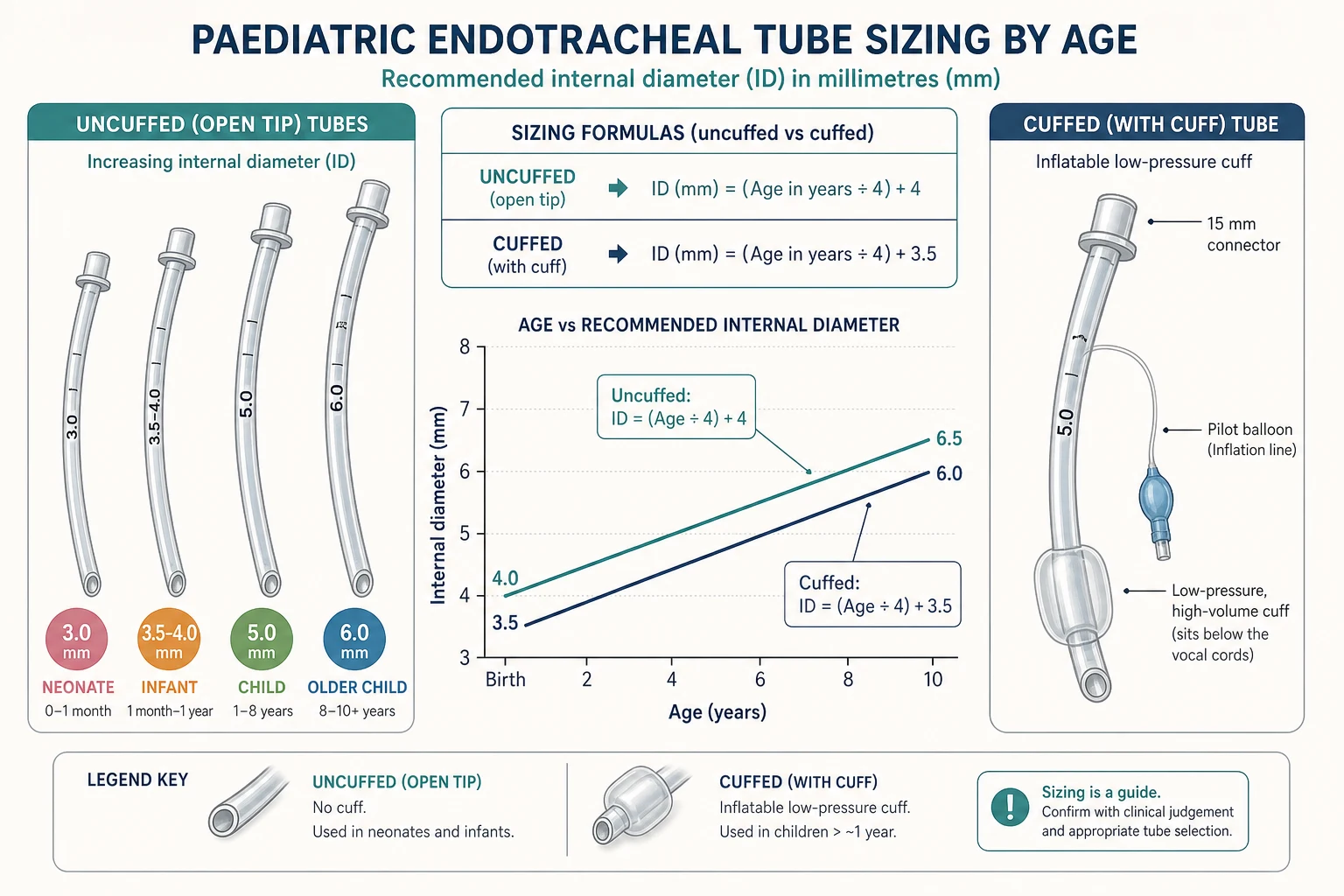
By tube, the modern choice is between uncuffed and cuffed. For decades the paediatric teaching was uncuffed only, on the grounds that the cricoid is the narrowest part of the infant airway and a cuff there risks ischaemic injury. That teaching has changed. Two Cochrane reviews — one in children aged eight years and under, one in neonates — found no increase in post-extubation stridor or reintubation when a modern high-volume low-pressure or microcuff tube was used and sized correctly. Cuffed tubes are now acceptable at every age, provided the cuff pressure is kept low and the tube is not over-sized. [1] [2]
By route, the first choice in an emergency is orotracheal — faster, easier to perform under direct vision, and the standard for rapid sequence intubation. Nasotracheal intubation is reserved for selected ward, PICU or surgical situations and is not first-line in arrest or the unstable child. By device, the choice is direct laryngoscopy with a straight or curved blade, or video laryngoscopy with a device such as a GlideScope or C-MAC that puts a camera on the blade tip. [3] [11]
Epidemiology & Risk Factors
Intubation is one of the commonest high-acuity procedures in paediatrics, performed in the emergency department, the PICU and NICU, theatre and retrieval. The single epidemiological fact that shapes practice is that adverse events rise with the number of attempts: every additional laryngoscopy increases the risk of desaturation, bradycardia and oesophageal intubation. Desaturation is the most frequent adverse event, and the infant is the child at greatest risk. [11]
The infant and small child are the hardest group for three physiological reasons. Their functional residual capacity is small and their oxygen consumption per kilogram is roughly double the adult value, so they desaturate within a minute of apnoea. Their tongue is large relative to the oral cavity, and their larynx is high and anterior, so the cords are harder to bring into view. And their epiglottis is long, soft and angled, so it falls over the glottis unless it is lifted directly. [11]
Previously well infant
Bronchiolitis, exhaustion
- Small functional residual capacity, rapid desaturation
- Straight Miller blade, external laryngeal manipulation
- Preoxygenase fully before the first attempt
- Stop and bag-mask ventilate if saturation falls
School-age child
Pneumonia or status epilepticus
- Curved Macintosh blade, sniffing position
- Cuffed tube at age divided by 4 plus 3.5
- Rapid sequence with rocuronium 1 mg per kg
- Confirm with waveform capnography
Syndromic child
Pierre Robin, Down syndrome
- Anticipated difficult airway — call senior help
- Video laryngoscopy first line
- Laryngeal mask airway ready as rescue
- In-line immobilisation if cervical instability
Neonate in delivery room
Failure of mask ventilation
- 2.5 mm tube if under 1000 g, 3.5 mm if term
- Straight Miller size 1 blade
- Neutral position, large occiput
- Cuffed tubes not used routinely in the newborn
The risk factors for a genuinely difficult airway are the ones an examiner rewards you for naming: craniofacial syndromes (Pierre Robin with micrognathia, Treacher Collins, Goldenhar), mucopolysaccharidoses, cervical spine limitation or instability, neck mass or deep neck infection (retropharyngeal abscess, epiglottitis), upper airway oedema from burns or anaphylaxis, obesity, and the previously intubated or chronically ventilated child with subglottic narrowing. Each is a reason to call for senior or anaesthetic help before the first attempt and to have a supraglottic airway open on the trolley. [9] [10]
Pathophysiology
The reason intubation technique changes with age is a set of anatomical facts about the infant airway. Four features matter, and each has a direct consequence for what you do at the bedside. [11]
First, the infant's occiput is large, so when the child lies supine the neck flexes forward and the airway tends to close. That is why an infant is intubated in a near-neutral position, often with a small towel under the shoulders, rather than the sniffing position used in the older child. Second, the tongue is large relative to the mouth, so it obstructs the view unless it is swept aside by the blade. Third, the larynx sits high and anterior — the glottis lies opposite the first to third cervical vertebrae in the infant, descending to the fourth to sixth in the adult — which is why the cords hide behind the tongue and benefit from external laryngeal manipulation. [11]
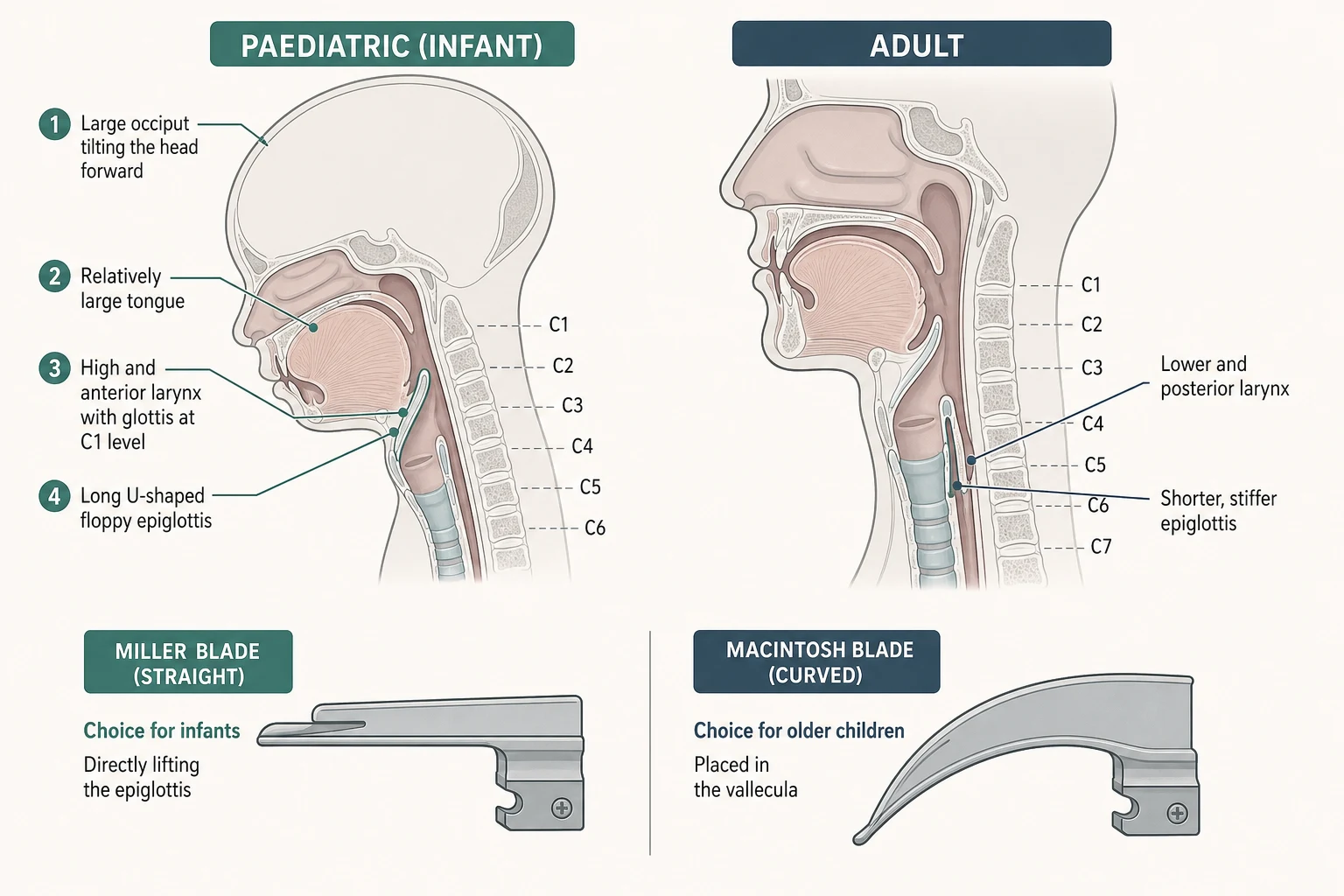
Fourth, the epiglottis is long, soft and U-shaped, and it falls backwards over the glottis like a trapdoor. This single feature explains the blade choice. A straight (Miller) blade is slid beneath the epiglottis and lifts it directly, exposing the cords — the right tool for the infant and small child. A curved (Macintosh) blade is placed in the vallecula, in front of the epiglottis, and lifts it indirectly through the hyoepiglottic ligament — effective once the larynx has descended in the older child. [11]
One further anatomical fact governs tube choice. The cricoid cartilage is the only complete ring in the trachea and is the narrowest point of the infant airway. An uncuffed tube that passes the cords can still be too tight at the cricoid, and a cuffed tube inflated to a high pressure can ischaemic the cricoid mucosa. This is the reason a cuffed tube, when used, must be sized correctly and the cuff pressure kept low — the anatomical basis for the post-extubation stridor and subglottic stenosis that follow over-sized or over-inflated tubes. [1] [11]
Clinical Presentation
The child who needs a definitive airway rarely announces it with a single sign. You recognise the need by recognising that the airway is failing, the breathing is failing, or the brain is no longer protecting the airway. Four presentations dominate. [9] [11]
The first is respiratory failure — the pneumonia, bronchiolitis, asthma or acute neuromuscular weakness in which the work of breathing is exhausting the child and the gas exchange is failing. The second is the loss of protective reflexes, classically a Glasgow Coma Scale of 8 or less, where the child cannot guard the airway and will aspirate. The third is severe shock that will need ventilation, and the fourth is cardiac arrest, where a tube allows uninterrupted chest compressions and reliable drug delivery. [11] [12]
Pre-emptive intubation is the registrar-level judgement that examiners probe. The child who is tiring — rising respiratory rate and heart rate, falling effort, altered consciousness — is the child you intubate before the arrest, not after it. The same applies to the child with severe croup or epiglottitis and impending obstruction, and to the unstable child about to be retrieved between hospitals, where a tube placed in calm conditions is far safer than one placed in a moving ambulance. [9]
The contexts that set up a difficult intubation are worth naming explicitly, because they change the plan. Syndromic facies, micrognathia, limited mouth opening, a stiff or unstable neck, stridor at rest, drooling and a tripod posture all warn you to call for senior help, lead with video laryngoscopy, and have a laryngeal mask airway ready before the first laryngoscopy. [9] [10]
Differential Diagnosis
There is no differential diagnosis of intubation itself — it is a procedure you perform or you do not. The question the clinician holds is which alternative airway adjunct is realistic in the time available, and what is going wrong when the laryngoscopy fails. [9]
The realistic alternatives to a definitive tube are a bag-mask, the skill that keeps almost every sick child alive and must be mastered first; oropharyngeal and nasopharyngeal airways, which relieve soft-tissue obstruction; and the supraglottic airway or laryngeal mask, the rescue device when intubation fails and bag-mask ventilation becomes inadequate. The decision rule keeps the differential practical: bag-mask is the bridge, the laryngeal mask is the rescue, and the tube is the destination. [9] [10]
The more useful differential in practice is the cause of a poor laryngoscopic view. When you cannot see the cords, run through the correctable causes: inadequate positioning, a blade that is too short or too long for the child, a floppy epiglottis not lifted, secretions or blood obscuring the field, the oesophageal inlet mistaken for the glottis, and an anterior larynx that needs external laryngeal manipulation — backwards, upwards, rightward pressure (BURP) applied by an assistant. Each has a corrective action, and naming them is what an examiner wants. [11]
The differential of failed confirmation matters just as much. A flat capnography trace means oesophageal intubation until proved otherwise; asymmetric chest movement means a tube too deep in the right main bronchus; a persistent leak means a cuff failure or an under-sized tube; and a tube that was right but now causes high pressures may be blocked, kinked or dislodged. Capnography and a stethoscope settle most of these at the bedside. [5] [6]
Clinical & Bedside Assessment
The bedside assessment has two parts: predict the difficult airway before you induce, and position the child correctly. Both are done by looking and feeling, not by investigation. [9] [11]
Assess the airway the moment you meet the child. Look for micrognathia and a small jaw, limited mouth opening, a short or stiff neck, any mass or swelling at the front of the neck, and the signs of upper airway obstruction — stridor, drooling, tripod posture, retractions. A child with any of these is an anticipated difficult airway: call for senior or anaesthetic help, prepare video laryngoscopy, and open a laryngeal mask airway on the trolley before you induce. [9]
Positioning is the single most underrated skill in intubation. The older child is placed in the sniffing position — neck slightly flexed, head extended on the atlanto-occipital joint — which aligns the oral, pharyngeal and laryngeal axes into a single line and brings the cords into view. The infant is different: the large occiput already flexes the neck, so the infant is laid nearly neutral, often with a small towel under the shoulders so that the external auditory meatus and the anterior shoulder lie on the same horizontal line. Over-extending an infant's neck collapses the airway and is a classic error. [11]
When the Cormack-Lehane view is poor, apply external laryngeal manipulation — the operator or an assistant presses backwards, upwards and to the right (BURP) on the larynx to bring an anterior glottis into the line of sight. This is not the same as cricoid pressure: BURP improves the view, cricoid pressure (Sellick) is intended to prevent regurgitation and is no longer routinely recommended in children because it can worsen the view. [11]
Tube size, blade, depth and confirmation
Investigations
No investigation is required before an emergency intubation — the decision is clinical and the procedure immediate. A bedside blood gas, glucose and electrolytes can be drawn once vascular access is secured, and they guide the ventilation target rather than the decision to intubate. [11]
The investigation that matters at the moment of intubation is the confirmation of tube position. Waveform capnography is the standard: a sensor in the circuit measures exhaled carbon dioxide breath by breath and displays a trace. A correctly placed tracheal tube produces a square-wave trace that rises briskly in expiration and returns to baseline in inspiration, sustained over six breaths. An oesophageal intubation produces no sustained trace, and a tube in the right main bronchus shows a falling trace as the left lung fails to exchange gas. [5] [6]
A colorimetric carbon dioxide detector — a small disposable device that changes colour in the presence of exhaled carbon dioxide — is a reasonable secondary check where waveform capnography is unavailable, but it is less reliable in low cardiac output states and cardiac arrest, where pulmonary blood flow is too low to deliver carbon dioxide to the lungs. In arrest, a flat colorimetric detector does not exclude tracheal placement, but a flat waveform capnography trace, combined with poor chest rise, should. [6] [12]
After intubation, a chest radiograph confirms the tube tip sits in the mid-trachea — roughly at the level of the clavicles to just above the carina — and rules out right main bronchus intubation, kinking and pneumothorax. The chest film does not confirm tracheal versus oesophageal placement; that is the job of capnography. Ongoing monitoring after intubation is continuous waveform capnography — the target end-tidal carbon dioxide is 35 to 45 mmHg in the perfusing child — with continuous oxygen saturation and a ventilator set to age-appropriate pressures. [5] [6]
Management — Resuscitation
Intubation is itself a resuscitation procedure, and the resuscitation moves are short. Prepare, preoxygenate, position, induce, paralyse, intubate, confirm — the sequence that converts a chaotic arrest into a controlled one. [9] [11]
Preparation means the equipment is open and checked before induction: the chosen endotracheal tube plus one half-size larger and one half-size smaller, a laryngoscope with a working light and a spare bulb or battery, a Yankauer sucker, a stylet, a syringe to inflate the cuff if a cuffed tube is used, securing tape, and the capnography sensor connected. Preoxygenation with 100 per cent oxygen for two to three minutes denitrogenates the lungs and extends the safe apnoea time; in the infant this single act is the difference between a calm intubation and a frantic one. [11]
For rapid sequence intubation, give a sedative — etomidate 0.3 mg per kg, ketamine 1 to 2 mg per kg, or propofol 2 to 4 mg per kg — immediately followed by a neuromuscular blocker: succinylcholine 1 to 2 mg per kg or rocuronium 1 mg per kg. Rocuronium is increasingly preferred because it avoids the succinylcholine contraindications — hyperkalaemia, burns, muscle disease and malignant hyperthermia — and a 2026 paediatric emergency comparison found comparable intubating conditions. [7] [8]
Rocuronium (rapid sequence paralysis)
Dose
1 mg per kilogram
Succinylcholine (rapid sequence paralysis)
Dose
1 to 2 mg per kilogram
Confirmation is the act that separates a safe intubation from a lethal one. As soon as the tube is through the cords, attach the circuit and look at the waveform capnography. A square-wave carbon dioxide trace over six breaths, with chest rise and equal breath sounds, confirms tracheal placement. Inflate the cuff only to a seal — cuff pressure below 25 cm of water — if a cuffed tube is used, then secure the tube and re-check the depth. [5] [11]
Management — Definitive & Stepwise
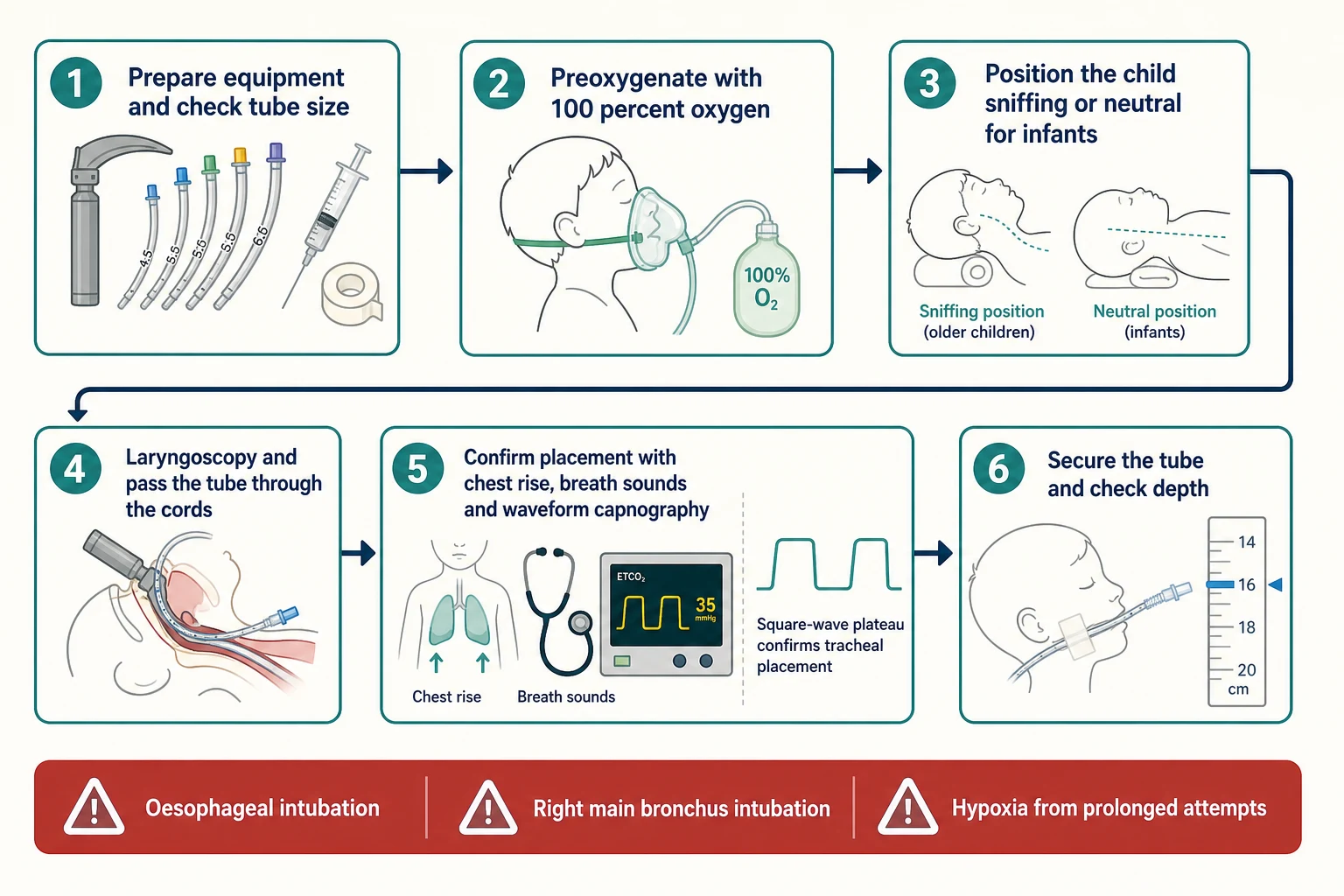
Once the resuscitation sequence is set, the procedure itself is seven ordered steps. Run through them the same way every time, on a manikin until they are automatic. [9] [11]
The intubation procedure, in order
1 · Prepare and check
Confirm the indication. Assemble the team and name roles. Check the tube size plus one half-size up and down, the laryngoscope light, the suction, the stylet, the cuff syringe, the securing tape and the capnography sensor.
2 · Preoxygenase
100 per cent oxygen for two to three minutes (or four to eight high-flow breaths in the emergency). Apply apnoeic oxygenation with high-flow nasal cannula if available to extend safe apnoea time.
3 · Position
Older child in the sniffing position; infant neutral with a small towel under the shoulders so the tragus and anterior shoulder line up horizontally.
4 · Induce and paralyse
Rapid sequence: sedative then neuromuscular blocker at paediatric weight-based doses. Cricoid pressure is not routine; release it if it impairs the view.
5 · Laryngoscopy and intubation
Insert the blade, lift (do not lever on the teeth) to expose the glottis — directly under the epiglottis with a Miller blade, via the vallecula with a Macintosh blade. Pass the tube through the cords under direct vision and withdraw the stylet.
6 · Confirm
Waveform capnography is the standard: square-wave trace over six breaths, with chest rise and equal air entry. Inflate the cuff only to a seal if used.
7 · Secure and verify depth
Secure the tube, confirm the depth at the lips (age divided by 2 plus 12 centimetres, or about three times the internal diameter), and order a confirmatory chest radiograph.
A few technique points separate a clean intubation from a failed one. Lift, do not lever — levering the blade on the upper teeth fractures them and does not improve the view. Stop after two failed attempts and ventilate with a bag-mask: continuing into a third attempt with a falling saturation is the pathway to arrest. And use video laryngoscopy early for the anticipated difficult airway. A 2024 New England Journal of Medicine trial in newborns and a 2025 British Journal of Anaesthesia systematic review found video laryngoscopy improved glottic visualisation and first-attempt success in infants and neonates, with the clearest benefit when the airway was predicted to be hard. [3] [4]
| Age group | Uncuffed ID (mm) | Cuffed ID (mm) | Blade | Depth at lips (cm) |
|---|---|---|---|---|
| Neonate under 1000 g | 2.5 | not routine | Miller 0 or 1 | 6 to 7 |
| Term neonate | 3.0 to 3.5 | not routine | Miller 1 | 9 to 10 |
| Infant (under 1 year) | 3.5 to 4.0 | 3.0 to 3.5 | Miller 1 | 10 to 11 |
| Child (1 to 2 years) | 4.0 to 4.5 | 3.5 | Miller 1 or 2 | 12 |
| Older child (5 years) | 5.0 | 4.5 | Macintosh 2 | 15 |
| Adolescent (10 years) | 6.5 | 6.0 | Macintosh 3 | 17 to 18 |
[1] [11] Uncuffed internal diameter equals age divided by 4 plus 4; cuffed equals age divided by 4 plus 3.5; depth at the lips equals age divided by 2 plus 12. Neonatal sizes follow weight and gestation rather than the formula.
Specific Subtypes & Scenarios
Five scenarios recur in fellowship vivas and OSCE stations, and each has its own twist. The first is the neonate in the delivery room. A term newborn usually takes a 3.5 mm uncuffed tube; a preterm infant under 1000 grams or 28 weeks takes a 2.5 mm tube; the 1000 to 2000 gram infant takes a 3.0 mm tube. Use a straight Miller size 1 blade and a neutral position. Intubate for failure of mask ventilation, prolonged positive-pressure ventilation, chest compressions, congenital diaphragmatic hernia, or to give surfactant. Note that routine intubation of the non-vigorous meconium-stained infant is no longer recommended. [3] [11]
The second is the infant and small child with respiratory failure. The short apnoeic reserve makes full preoxygenation and a calm first attempt essential. A straight blade and external laryngeal manipulation deliver the view, and desaturation with bradycardia is the constant threat — stop and ventilate with a bag-mask the moment the saturation falls, rather than pushing on into a third attempt. [11]
The third is the older child and adolescent, where a curved Macintosh blade and the sniffing position apply and a cuffed tube is standard. Video laryngoscopy comes into its own for the anticipated difficult airway — the syndromic child, the obese adolescent, and any child with limited neck movement — and should be the first device, not the last resort. [3] [4]
The fourth is the child in cardiac arrest. Place the tube without interrupting chest compressions, and confirm with waveform capnography. In arrest, capnography does double duty: it confirms tracheal placement and it monitors the quality of compressions, because end-tidal carbon dioxide is a surrogate for cardiac output. A persistently low end-tidal carbon dioxide suggests poor perfusion, and an abrupt rise can signal the return of spontaneous circulation. [5] [12]
The fifth is the anticipated difficult airway. Call for senior help early, open a laryngeal mask airway on the trolley, lead with video laryngoscopy, and follow a structured difficult-airway algorithm — the Difficult Airway Society 2025 guidelines, the APSA and the ASA 2022 guidelines all converge on the same logic: prepare, optimise the first attempt, and have a rescue plan declared before you begin. Repeating failing direct attempts is the error the algorithms exist to prevent. [9] [10]
Complications & Pitfalls
Complications are uncommon when the procedure is done well, but two of them — hypoxia and unrecognised oesophageal intubation — are directly under your control, and naming them is what an examiner wants. [5] [11]
The commonest significant complication is hypoxia from prolonged or failed attempts. Every additional laryngoscopy raises the risk of desaturation, bradycardia and arrest. The single act that prevents it is full preoxygenation; the single act that halts it is stopping after a failed attempt to ventilate with a bag-mask before the next try. Unrecognised oesophageal intubation is the catastrophe, and it is entirely preventable: waveform capnography is the standard that confirms tracheal placement, and a tube should never be assumed correctly sited from chest rise alone. [5] [6]
Right main bronchus intubation happens when the tube is passed too deep. The right main bronchus is wider and more vertical than the left, so an over-deep tube preferentially enters it, collapsing the left lung and over-distending the right. The fix is to withdraw the tube until breath sounds are equal — listening over the left axilla is the quick test — and to confirm the depth on a chest radiograph. Bradycardia in the infant is the vagal and hypoxic response to laryngoscopy; stop, ventilate with 100 per cent oxygen, and begin chest compressions if the rate stays low and the child is poorly perfused. [11] [12]
Local trauma completes the list: lip, tongue and dental injury from the blade, and — with repeated, over-sized or over-inflated tubes — post-extubation stridor and subglottic stenosis. These are prevented by correct sizing, a cuff pressure kept low (below 25 cm of water), and the discipline of minimising attempts. Other complications include aspiration of gastric contents, pneumothorax from barotrauma, hypotension from induction and positive pressure, and accidental extubation or tube blockage during transport. [1] [11]
Prognosis & Disposition
Intubation is a bridge to definitive care, not a treatment in itself. Once the tube is secure and confirmed, attention turns to the underlying illness, to lung-protective ventilation, and to a safe plan for transfer or weaning. The outcome of the episode is driven by the cause of the respiratory failure — sepsis, pneumonia, status epilepticus, cardiac arrest — and by the quality of the resuscitation, not by the act of intubation. [9] [11]
A confirmed, secured tube with continuous waveform capnography and a ventilator set to age-appropriate pressures is the minimum standard before an inter-hospital transfer. A tube displaced in transit is a recurrent and avoidable cause of harm, so the tube is secured firmly, the depth is documented, and the transfer team carries a spare laryngoscope and a laryngeal mask airway. The retrieval services across Australia and New Zealand treat a secured, monitored airway as a precondition for moving a ventilated child. [9]
After extubation, watch the child for post-extubation stridor — the sign of airway oedema — and treat it with humidity, nebulised adrenaline and, in the moderate case, dexamethasone. Feed back the learning from any difficult intubation, and document the airway plan, the tube size and the blade used so the next encounter begins informed rather than blind. [11]
Special Populations
The neonate deserves a separate line. Tube sizes follow weight and gestation rather than the age formula: 2.5 mm under 1000 grams or 28 weeks, 3.0 mm for 1000 to 2000 grams, and 3.5 mm over 2000 grams or at term. A straight Miller size 1 blade and a neutral position are standard, and the resuscitation follows the Neonatal Resuscitation Program. Cuffed tubes are not used routinely in the newborn. [3] [11]
The syndromic and craniofacial child — Pierre Robin with micrognathia, Treacher Collins, Goldenhar, the mucopolysaccharidoses — is an anticipated difficult airway. Plan ahead, call for senior or anaesthetic help, lead with video laryngoscopy, and have a supraglottic airway open on the trolley. The child with Down syndrome and suspected cervical instability needs in-line cervical immobilisation during laryngoscopy and a careful first attempt, often with video laryngoscopy, because both the airway anatomy and the cervical spine raise the difficulty. [9] [10]
The immunocompromised and oncology child often has fragile mucosa and a friable airway, so the technique is gentle, the cuff pressure is low, and the smallest effective tube is chosen. Weigh early intubation before exhaustion in this group, because the reserve is narrow. The obese adolescent presents a difficult mask and a harder view — ramp the position, preoxygenate thoroughly, prefer a cuffed tube, and have video laryngoscopy available. [11]
For Aboriginal, Torres Strait Islander, Māori, and migrant and refugee children, and for children in remote communities, respiratory failure from pneumonia, bronchiolitis and sepsis presents late, and the nearest clinician who can secure an airway may be hours away. Intubation competence in the rural and retrieval workforce is an equity skill as much as a clinical one — it is what closes the gap between a lethal deterioration and a survivable retrieval. [9]
Evidence, Guidelines & Regional Differences
The guidelines are strikingly concordant across regions. The Advanced Paediatric Life Support course used across Australia and New Zealand, the American Heart Association Pediatric Advanced Life Support guidance, the European Resuscitation Council, the Difficult Airway Society 2025 guidelines, and the ASA 2022 difficult-airway guidelines all treat the endotracheal tube as the definitive emergency airway and waveform capnography as the confirmation standard. [9] [12]
The cuffed versus uncuffed question is now settled at the level of evidence. Two Cochrane reviews — one in children aged eight years and under, one in neonates — found no increase in post-extubation stridor or reintubation with modern cuffed tubes when they were sized correctly and the cuff pressure was monitored. The practical teaching has followed: cuffed tubes are acceptable at every age, with the caveat that the cuff is inflated only to a seal and the pressure kept below 25 cm of water. [1] [2]
[1] [12]The video versus direct laryngoscopy question is moving the same way. A 2024 New England Journal of Medicine randomised trial in newborns found video laryngoscopy improved glottic visualisation and first-attempt success, and a 2025 British Journal of Anaesthesia systematic review extended the benefit to infants and children, with the clearest gain in the anticipated difficult airway. The take-home is precise: video laryngoscopy is not a panacea, but it is the right first device when the airway is predicted to be hard. [3] [4]
The rocuronium versus succinylcholine question has tilted towards rocuronium. A 2026 paediatric emergency comparison found comparable intubating conditions, and rocuronium avoids the succinylcholine contraindications — hyperkalaemia, burns more than 24 hours old, denervation, muscle disease and malignant hyperthermia. The genuine controversies are narrow: whether routine cricoid pressure helps (the evidence is weak and it can worsen the view), whether atropine should be given routinely before intubation in infants (current resuscitation guidance does not mandate it), and the optimal apnoeic-oxygenation technique in the smallest children. [7] [8]
Exam Pearls
A fellowship candidate should leave the examiner with a small set of sharp, sourced facts. Memorise these and you will answer any question on this topic. [9] [11]
The tube-size formulas are the single highest-yield fact: uncuffed internal diameter in millimetres equals age divided by 4 plus 4, cuffed equals age divided by 4 plus 3.5, and the depth at the lips in centimetres equals age divided by 2 plus 12. The neonatal sizes are by weight: 2.5 mm under 1000 grams, 3.0 mm for 1000 to 2000 grams, 3.5 mm at term, with a straight Miller size 1 blade. [1] [11]
The blade choice is straight Miller for the infant (lifting the long floppy epiglottis directly) and curved Macintosh for the older child (placed in the vallecula). The infant larynx is high and anterior and the narrowest point is the cricoid, a complete ring — the anatomical basis for both the difficult view and the risk of subglottic stenosis from an over-inflated cuff. [11]
Confirmation is waveform capnography — a square-wave carbon dioxide trace over six breaths is the standard, and colorimetric is secondary. The rapid sequence drugs are a sedative (etomidate 0.3 mg per kg, ketamine 1 to 2 mg per kg, or propofol 2 to 4 mg per kg) followed by a neuromuscular blocker (succinylcholine 1 to 2 mg per kg or rocuronium 1 mg per kg). [5] [7]
The most common complication is hypoxia from prolonged attempts; the most dangerous is unrecognised oesophageal intubation, prevented by capnography. Preoxygenate, position, and confirm with capnography every time — and stop after a failed attempt to ventilate with a bag-mask before you try again. Video laryngoscopy is the right first device for the anticipated difficult airway, and a laryngeal mask airway is the rescue when intubation fails. [3] [5]
References
- [1]de Orange FA, Andrade RL, Vasconcelos G, et al Cuffed versus uncuffed endotracheal tubes for general anaesthesia in children aged eight years and under Cochrane Database of Systematic Reviews, 2017.PMID 29149469
- [2]Dariya V, Nanavati RN, Patil V, et al Cuffed versus uncuffed endotracheal tubes for neonates Cochrane Database of Systematic Reviews, 2022.PMID 35073407
- [3]Geraghty LE, Zierden J, Deakins K, et al Video versus Direct Laryngoscopy for Urgent Intubation of Newborn Infants New England Journal of Medicine, 2024.PMID 38709215
- [4]Koepp-Medina G, Vásquez JL, Aprea L, et al Videolaryngoscopy versus direct laryngoscopy for paediatric tracheal intubation: a systematic review with meta-analysis and trial sequential analysis British Journal of Anaesthesia, 2025.PMID 41046172
- [5]Bullock A, Pallin D, Foster M, et al Capnography Use During Intubation and Cardiopulmonary Resuscitation in the Pediatric Emergency Department Pediatric Emergency Care, 2017.PMID 27455341
- [6]Selby ST, Hsu M, Wainsztein N, et al An Update on End-Tidal CO2 Monitoring Pediatric Emergency Care, 2018.PMID 30507754
- [7]Mendez D, Patel P, Groth M, et al Succinylcholine Versus Rocuronium for Pediatric Rapid Sequence Intubation in the Emergency Department Pediatric Emergency Care, 2026.PMID 41489184
- [8]Ching KY, Baum CR Newer agents for rapid sequence intubation: etomidate and rocuronium Pediatric Emergency Care, 2009.PMID 19287283
- [9]Black AE, Flynn PE, Smith HL, et al Development of a guideline for the management of the unanticipated difficult airway in pediatric practice Paediatric Anaesthesia, 2015.PMID 25684039
- [10]Jagannathan N, Bayman L, Patel R, et al Difficult Airway Society 2025 guidelines for tracheal intubation: thoughtful preparation for success and systematic management of failure British Journal of Anaesthesia, 2026.PMID 41339170
- [11]Hsu G, Koka R, Ballard HO, et al Pediatric airway management Current Opinion in Anaesthesiology, 2021.PMID 33935175
- [12]Merchant RM, Topjian AA, Panchal AR, et al Part 1: Executive Summary: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Circulation, 2020.PMID 33081530