Paeds · investigations-procedures-and-technology
Gastrostomy, tracheostomy and central-line troubleshooting
Also known as Paediatric enteral and airway device troubleshooting · Gastrostomy tube complications in children · Tracheostomy emergency management in children · Central venous catheter occlusion and breakage in children
A fellowship approach to troubleshooting the three devices a technology-dependent child lives with — the gastrostomy, the tracheostomy and the central venous catheter. Recognise and resolve the common failure modes: the leaking or buried gastrostomy and the dislodged tube in an immature tract; the obstructed or decannulated tracheostomy run through the National Tracheostomy Safety Project algorithm; and the occluded, broken or infected central line managed with the right lock — sterile water and warm flush, a thrombolytic dwell for a clot, and an immediate clamp-and-repair for a fracture.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A 4-year-old with cerebral palsy, a gastrostomy button and a tracheostomy for chronic lung disease is admitted overnight with increased secretions and desaturation. The bedside nurse cannot pass the suction catheter. This child is exactly the patient this page is written for: the technology-dependent child whose safety lives in whether the team can recognise a mucus plug, a dislodged tube or an occluded line in the first minute. The decision in each case is the same — resuscitate the child, then read the device — and the algorithms are learnable, exact and examinable. This page teaches the three devices side by side, the failure modes of each, and the bedside responses that separate a controlled resolution from an arrested deterioration. [1] [4]
D.O.P.E. — why a device fails
Overview & Definition
Imagine you are called to a child who is attached to one or more of three devices — a gastrostomy for feeding, a tracheostomy for breathing, and a central venous catheter for intravenous therapy. Each device keeps the child alive or nourished, and each has a small, predictable set of ways in which it stops working. Device troubleshooting is the recognition of those failure modes and the bedside response to them. The gastrostomy fails by leaking, by growing granulation, by burying its internal bumper, by becoming infected, or by falling out. The tracheostomy fails by obstructing with secretions, by falling out, by bleeding, or by developing a cuff leak. The central line fails by occluding, by fracturing, by becoming infected, or by dislodging. [1] [4]
The defining principle of device troubleshooting is that the child comes before the hardware. In every device emergency the first action is to assess and support airway, breathing and circulation, and only then to read the device. The second principle is that each device has a learned algorithm, and the team that has rehearsed it resolves the emergency calmly while the team that has not improvises dangerously. The National Tracheostomy Safety Project algorithm, the gastrostomy replacement logic of tract maturity, and the central-line occlusion categorisation are the three algorithms a general paediatrician must be able to recite. [3] [8]
The key idea a candidate must hold is tract maturity. A gastrostomy tract takes roughly six to eight weeks to mature, and a tracheostomy tract takes about seven to ten days; before those thresholds the tract will close within hours, and blind instrumentation is both futile and dangerous. After the threshold, replacement at the bedside is expected and safe. That single distinction — mature versus immature tract — governs the entire emergency response to a dislodged tube, and inverting it is one of the most dangerous errors in paediatric device care. [1] [3]
Classification
Sort device failure by which device has failed and by the type of failure, because the response is driven by both. The three devices divide naturally, and within each the failure modes cluster into mechanical, obstructive, infectious and bleeding categories. [1] [8]
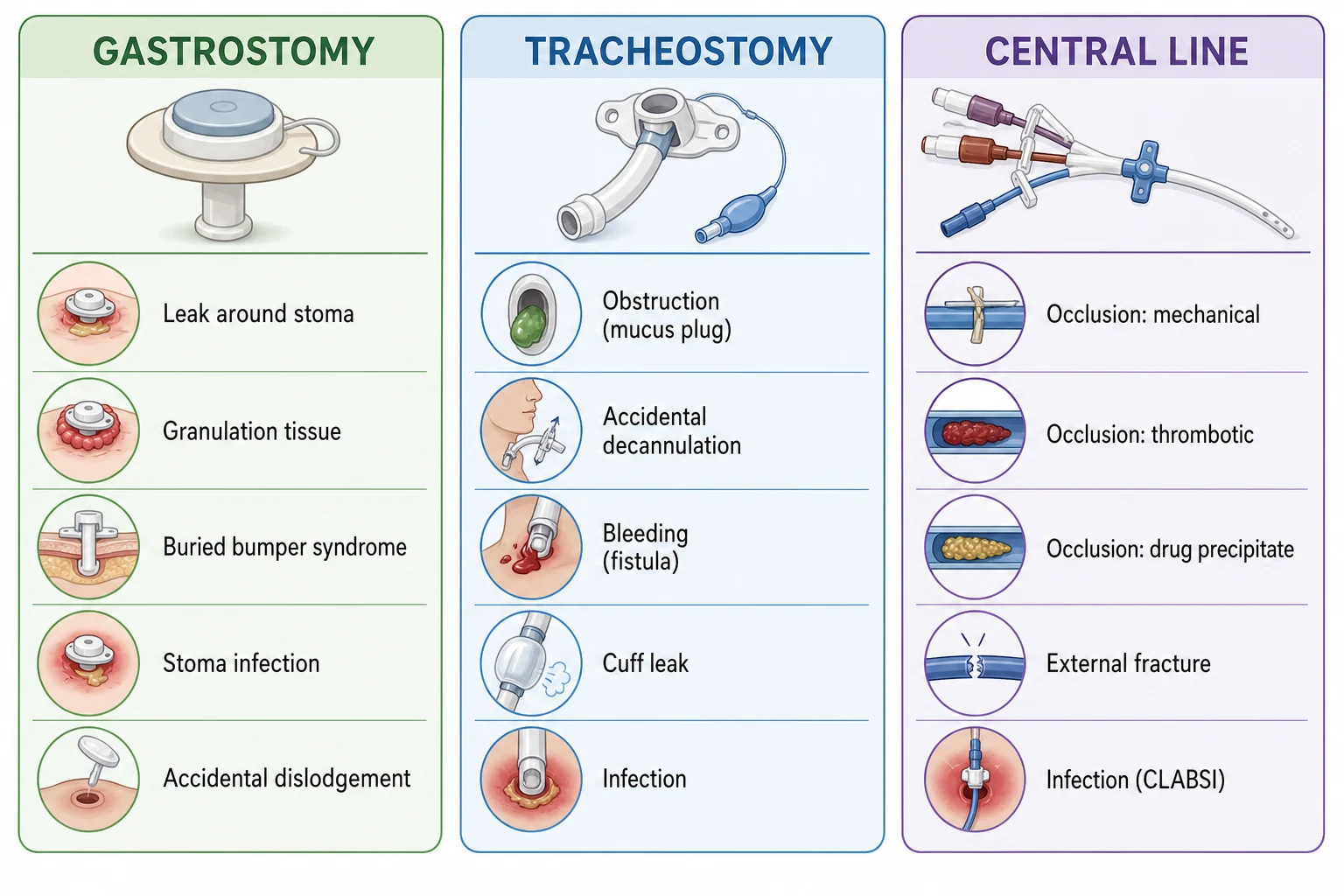
The gastrostomy fails by leak around the stoma, by granulation tissue at the skin, by buried bumper syndrome, by stoma infection or cellulitis, and by accidental dislodgement. The tracheostomy fails by obstruction with a mucus plug or crust, by accidental decannulation, by bleeding (minor from granulation or major from a tracheoinnominate fistula), by cuff leak, and by infection. The central venous catheter fails by occlusion (mechanical, thrombotic, or drug precipitate), by external fracture or breakage, by dislodgement or migration, by air embolism, and by central line-associated bloodstream infection. [2] [7] [8]
The three devices and their headline failure mode
Epidemiology & Risk Factors
Device complications are common in the technology-dependent child because the devices are in constant use and because the children who carry them are medically complex. A child with a tracheostomy, a gastrostomy and a central line carries the accumulated risk of all three, and the team that looks after such a child will meet every failure mode in a career of practice. [1] [4]
For the tracheostomy, accidental decannulation is the most studied complication because it is the most dangerous. Wynings and colleagues' prospective cohort of inpatient paediatric tracheostomies recorded accidental decannulations that were concentrated in the youngest children, in the first weeks after insertion, and in children managed outside an intensive-care setting — all features that mark the newly tracheostomised child as the highest-risk patient on the ward. The lesson is operational: the first week after tracheostomy is a guarded period, the bedside must hold a spare tube of the same size and one smaller, and a low threshold to call for help. [3]
For the central line, occlusion is the single most common non-infectious complication, occurring in a substantial fraction of long-term paediatric catheters, and it is the entry point to thrombosis and to catheter removal if not managed. Giordano and colleagues, writing for the Italian Association of Pediatric Hematology and Oncology, framed central-line occlusion and thrombosis as paired problems that share a management pathway, and that framing is the one the exam expects. The risk rises with long dwell time, oncology and intensive-care use, and parenteral nutrition. [8] [11]
For the gastrostomy, complications cluster in the first months after insertion and in the child with high gastric outputs or reflux; leak, granulation and infection are the day-to-day problems, while buried bumper syndrome and tube dislodgement from an immature tract are the emergencies. Sutherland and colleagues surveyed paediatric gastrostomy practice around making safer and cleaner choices at insertion, because many late complications trace to technique at the outset. [2]
Pathophysiology
Each device fails for mechanical and biological reasons, and knowing those reasons explains the algorithms. [1] [8]
The gastrostomy leaks when the balloon is under-inflated or over-inflated, when the external bolster is too loose or too tight against the abdominal wall, or when the tract has dilated from chronic infection or pressure. Granulation tissue forms because the stoma is a chronic wound bathed in gastric secretions; the body responds with exuberant capillary proliferation that bleeds on contact and weeps. Buried bumper syndrome occurs when the internal retention balloon or bumper migrates forward through the gastric wall and becomes embedded in the gastric mucosa or abdominal wall, so that feeds meet a wall of tissue and leak back. The tract itself is a fistula that closes by secondary intention if the tube is removed before it has matured. [1] [2]
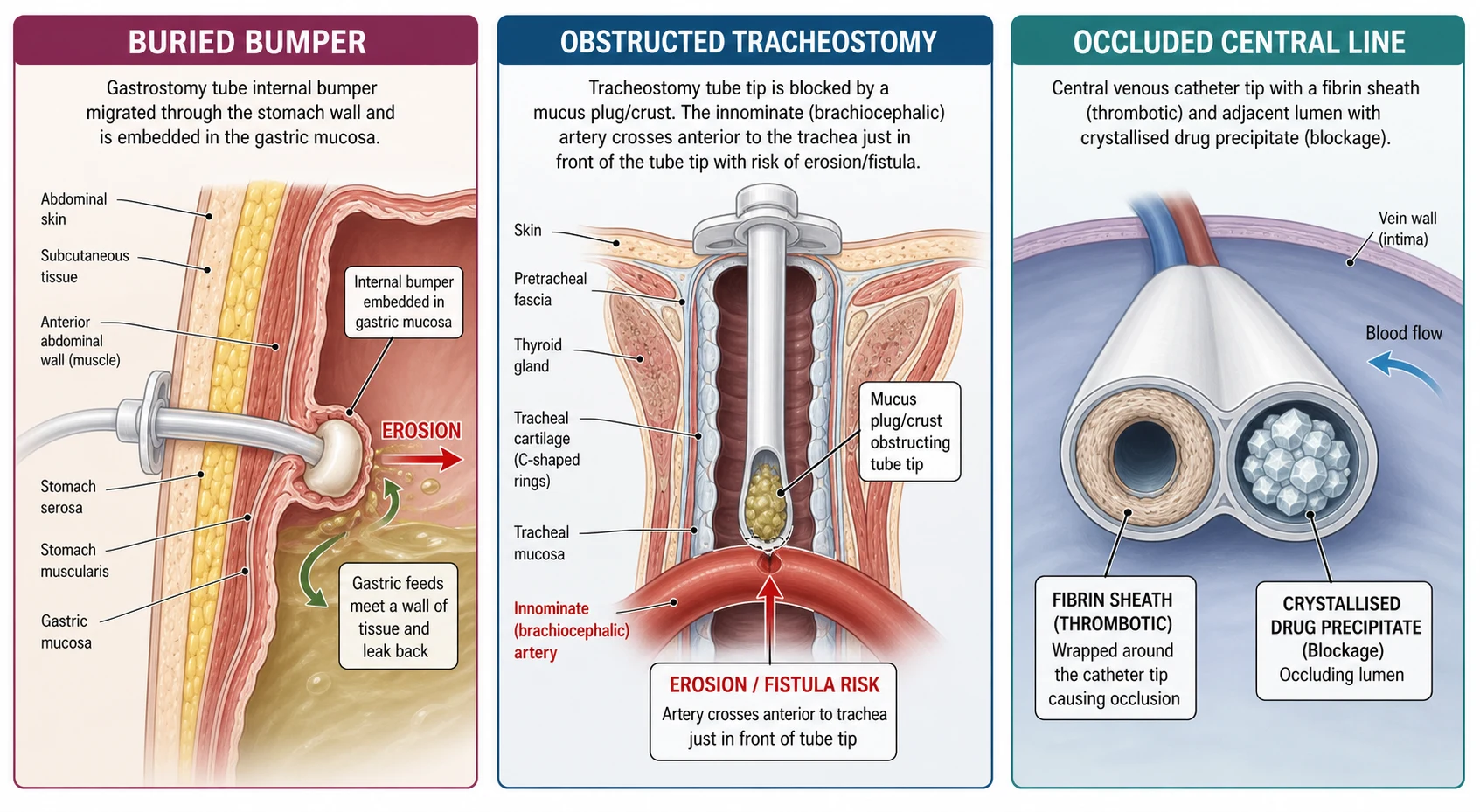
The tracheostomy obstructs because the airway of a child with a tracheostomy is chronically loaded with secretions that are thicker and more abundant than normal, and a crust or mucus plug can occlude the lumen or the distal tip in minutes. Decannuation occurs when the tube is dislodged by movement, suctioning, or a poorly secured flange. Bleeding from a tracheostomy is minor when it arises from granulation at the stoma or the tracheal mucosa, and catastrophic when it arises from a tracheoinnominate fistula — an erosion between the trachea and the innominate (brachiocephalic) artery, which crosses anterior to the trachea and is eroded by pressure from the tube tip or cuff, classically presenting two to six weeks after insertion with a small sentinel bleed followed by massive haemorrhage. [5] [6]
The central venous catheter occludes mechanically when the line is kinked, sutured too tightly, clamped, or abutting a vessel wall; thrombotically when a fibrin sheath or intraluminal clot blocks flow; and by drug precipitate when incompatible or high-pH infusions such as calcium, phenytoin or concentrated parenteral nutrition crystallise in the lumen. A line fractures from mechanical fatigue at the suture wing, the hub, or where it is clamped repeatedly; an external fracture opens the line to air (embolism) and blood (loss), and an internal fracture can embolise a fragment. Infection seeds from the skin down the external catheter tract or up the lumen, forming a biofilm. [8] [11]
Clinical Presentation
The child with a failing device presents through a small number of recognisable patterns, and reading the pattern tells you which device and which failure mode before you touch it. [1] [4]
The gastrostomy presents with feed or gastric contents leaking around the stoma, with an angry, bleeding granulation tissue at the skin, with pain on feeding or resistance to flushing (buried bumper), with spreading erythema and pus (infection), or with the tube lying on the bed (dislodgement). The buried bumper is suspected when there is new leakage with pain or resistance to feeding in a child whose tube has been in place for weeks, and it is a surgical or endoscopic problem, not a bedside one. [1]
The tracheostomy presents with acute desaturation, increased work of breathing, an inability to pass the suction catheter, or a tube that is visibly dislodged or has fallen out. The child with a tracheostomy who deteriorates is obstructed until proven otherwise. Bleeding may be minor and localised to the stoma, or it may be bright, brisk and voluminous — the presentation that demands an immediate suspicion of a tracheoinnominate fistula, especially in the second to sixth week after tracheostomy. A cuff leak presents as a loss of the ventilator circuit seal and a falling tidal volume. [4] [6]
The central line presents with an inability to flush or withdraw (occlusion), with a visible crack or leak in the external segment (fracture), with erythema, pus or tenderness along the tunnel or at the exit site (infection), with fever and no other source (line-associated bloodstream infection), or with the line having fallen back or migrated (dislodgement). The single most useful bedside distinction in occlusion is between a line that will neither flush nor withdraw (complete obstruction), one that flushes but will not withdraw (fibrin flap or tip against the wall), and one with positional flow (tip abutting a vessel wall). [8] [12]
Differential Diagnosis
Before acting on a device, consider what the failure could be and, equally, what non-device cause could explain the child's deterioration. The differential here is a structured list of failure modes plus a short list of mimics. [4] [8]
For the tracheostomy child who deteriorates, run DOPE down the device first (displacement, obstruction, pneumothorax, equipment), then consider that the deterioration may be from the lungs beyond the tracheostomy (consolidation, effusion, bronchospasm), from the heart (arrhythmia, shock), or from a new problem such as sepsis or a seizure. The discipline is to clear the device before blaming the child. [4]
For the occluded central line, the differential is mechanical versus thrombotic versus drug precipitate. A line that occludes immediately after a positional change or that has blood return in one position is mechanical; a line that occludes gradually and will not withdraw but flushes is thrombotic (a fibrin sheath or flap); a line that occludes shortly after an infusion of calcium, phenytoin or concentrated parenteral nutrition is a drug precipitate. Each leads to a different lock or manoeuvre, so the categorisation is the management. [8] [9]
For the gastrostomy, the differential of leakage is between a simple mechanical cause (balloon volume, bolster position), an infective or inflammatory cause (stoma cellulitis, granulation), and the surgical emergency of a buried bumper. Leakage alone is common and usually mechanical; leakage with pain and resistance to feeding is a buried bumper until excluded. [1] [2]
Clinical & Bedside Assessment
The bedside assessment of a device problem is a short, ordered examination that begins at the child and ends at the device. Work through the child, the device, and the consumables as a sequence. [1] [4]
For the gastrostomy, inspect the stoma for leak, erythema, granulation and pus; check the balloon volume against the device specification by aspirating and measuring; check the external bolster position (a fingerbreadth of play between the bolster and the skin is the rule of thumb); attempt to flush and to aspirate to gauge resistance; and compare the device in place with the size and type recorded in the chart. For a tube that has fallen out, the decisive question is the age of the tract, counted in weeks since insertion. [1] [2]
For the tracheostomy, assess airway and breathing first; then attempt to pass a suction catheter, which both clears secretions and tests patency; remove and clean the inner cannula if the tube has one; check the cuff if the child is ventilated; and inspect the stoma for bleeding, granulation and the tube's position. Have at the bedside a spare tracheostomy tube of the same size and one size smaller, a suction unit, a self-inflating bag, an oxygen source, and the bedhead emergency algorithm. [3] [7]
For the central line, assess the child for signs of sepsis or embolism; inspect the external segment for a crack, leak or blood; check the clamps and the dressing; attempt to flush and withdraw each lumen; and review the recent infusion history for drugs that precipitate. Confirm the line is still secure and sutured. A line that cannot be flushed should not be forced, because force can rupture the catheter or dislodge a clot. [8] [11]
Investigations
Most device problems are diagnosed at the bedside, but a few investigations change the plan, and they must not delay the emergency management of an obstructed airway or a bleeding fistula. [8]
The single most important investigation for a central line is the contrast injection or fluoroscopy that confirms whether an occlusion is mechanical or thrombotic, and that defines catheter tip position when a malposition or migration is suspected; a chest radiograph confirms tip position and excludes a pleural effusion from a migrated line. For suspected line infection, paired peripheral and line-drawn blood cultures before antibiotics are the diagnostic and the discriminative test, and they guide the decision to salvage or remove the line. [12]
For the tracheostomy, a bedside assessment of patency by suction catheter is both investigation and treatment; bronchoscopy defines the cause of persistent bleeding, a retained mucus plug, or suspected fistula, and it is the definitive investigation of a tracheoinnominate erosion when the child is stabilised. For a suspected cuff leak, a ventilator leak test localises the problem to the cuff, the circuit, or the connection. [5] [6]
For the gastrostomy, a contrast study through the tube confirms intragastric position before feeding a re-placed tube when the tract is mature, and it is the definitive investigation of a suspected buried bumper when the tube will not flush. Ultrasound and, increasingly, structured imaging can define the buried bumper and the balloon position within the gastric wall. [1]
Management — Resuscitation
The resuscitation phase of a device emergency is the minute in which the child is rescued, and it begins with airway, breathing and circulation — not with the device. State the sequence aloud. [4] [6]
For the obstructed or decannulated tracheostomy, run the National Tracheostomy Safety Project algorithm in order. Assess the child; suction via the tracheostomy; if the suction catheter will not pass, remove the inner cannula; if still obstructed, deflate the cuff; if the child is still not oxygenating, remove the tracheostomy tube and ventilate — by a bag-valve-mask over the face if the upper airway is patent and the stoma covered, or by a mask or paediatric face mask held over the stoma if the upper airway is not patent. Call for senior airway help early. The cardinal error is to persist with a non-functioning tube while the child deteriorates. [4] [7]
For an accidentally decannulated tracheostomy, the response turns on tract maturity. In a mature tract — generally more than seven to ten days after surgical tracheostomy — reinsert a tracheostomy tube of the same size, with the obturator in place, gently and without force; if resistance is met, use a tube one size smaller; if neither passes, ventilate and call for help. In an immature tract — within the first seven to ten days — do not force a tube blindly down the stoma, because the tract can create a false passage in the pretracheal tissues; instead, ventilate by face mask if the upper airway is patent, cover the stoma, and call the surgeon or anaesthetist who created it. [3] [6]
For a fractured central line, clamp the line immediately between the child and the fracture using a specialised slide clamp (not a haemostat that can crush the catheter), place the child head-down on the left side to limit air embolism if air entry is suspected, and prepare for repair or replacement. For a gastrostomy that has fallen out of an immature tract, replace the device without delay — even a Foley catheter as a temporising measure to keep the tract open — because the tract closes within hours, and do not feed until position is confirmed. [1] [8]
Management — Definitive & Stepwise
The definitive management is the application of the device-specific algorithm, and it should be stated step by step with the reason for each. [1] [8]
For the occluded central line, first categorise the occlusion, because the lock depends on the cause. A mechanical occlusion is resolved by releasing a clamp, loosening an over-tight suture, repositioning the arm or the child, or, if the tip is malpositioned, repositioning the line under imaging. A thrombotic occlusion is resolved by a thrombolytic dwell: instil alteplase in a volume that fills the lumen, at a weight-based dose (commonly 0.5 to 2 mg, with the lower dose reserved for the child under 10 kg), leave it to dwell for two to four hours, then aspirate and flush; repeat once if the first dwell fails. Anderson's review and the Baskin data established this regimen as effective and safe in children, restoring flow in the large majority of occluded lines. A drug precipitate is resolved by the matching solvent — sodium bicarbonate for an alkaline drug such as calcium or phenytoin, or hydrochloric acid for an acidic precipitate — and a lipid residue by an ethanol lock. [9] [10]
For a fractured external central line, after clamping, repair the line with a manufacturer-specific repair kit if one is available and the fracture is clean; otherwise replace the line, because a repaired line carries a higher risk of infection and further fracture. For suspected line infection, take cultures, start empiric antibiotics guided by local protocol and the likely organism (Gram-positive skin organisms most often), and discuss removal with the infectious diseases or oncology team, since tunneled lines are salvaged when possible but removed when the child has septic shock, a tunnel infection, or a persistent bacteraemia. [8] [12]
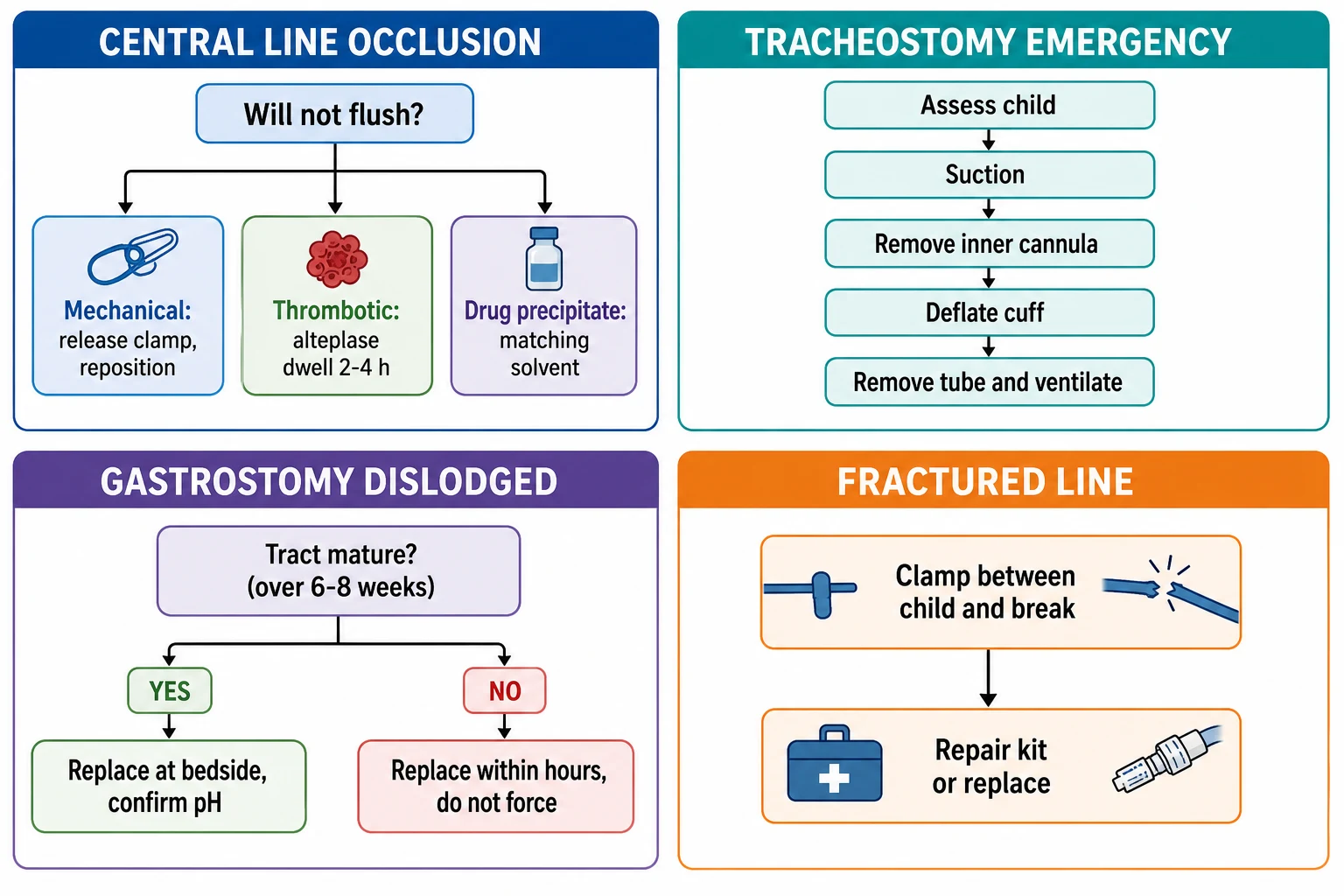
For the gastrostomy, manage a leak by checking and correcting the balloon volume, adjusting the external bolster, protecting the skin with a barrier film or cream, and treating any overlying infection; manage granulation with a topical corticosteroid and, if persistent, silver nitrate cauterisation by the team trained to do it; manage an infected stoma with oral or topical antibiotics directed at skin flora, with intravenous antibiotics for spreading cellulitis; and manage the suspected buried bumper by stopping feeding, decompressing, and arranging endoscopic or surgical correction — never by forcing the tube. For a tube that has fallen out of a mature tract, reinsert it and confirm position with a pH check of aspirate (a gastric pH of 5.5 or below confirms gastric placement) or a contrast study before feeding. [1] [2]
For the tracheostomy, definitive management beyond the emergency algorithm is to identify and treat the cause: humidification and regular suction to prevent mucus plugs, treatment of stoma cellulitis, bronchoscopic removal of a retained crust or plug, and surgical management of a tracheoinnominate fistula once the child is stabilised. The cuff leak is managed by adding air to the cuff to the minimum volume that seals, by checking the tube size, and by replacing the tube if the leak persists. [5] [6]
Specific Subtypes & Scenarios
Different children need a tailored response, and the exam rewards the candidate who can match the algorithm to the scenario. [3] [8]
The newly tracheostomised child (within the first seven to ten days) is the highest-risk patient: the tract is immature, the team is unfamiliar with the child, and the spare tubes may not yet be at the bedside. The response to accidental decannulation in this period is to ventilate by face mask and call the surgeon, not to reinsert blindly. The same child, six months later, with a mature tract, is managed by bedside replacement by the ward team. [3]
The oncology child with a long-term tunnelled central line (Hickman or Broviac) presents the classic occlusion scenario, and the thrombolytic dwell is first-line; the same child with a fever and no focus needs paired cultures and a low threshold to treat for a line infection, with salvage attempted and removal reserved for the deteriorating or persistently bacteraemic child. The neonate with a central line presents the thrombosis scenario — Park and colleagues described the diagnosis, management and outcome of neonatal central venous catheter thrombosis — and the small lumen volumes make weight-based, low-dose alteplase essential. [8] [11]
The child with cerebral palsy who carries both a gastrostomy and a tracheostomy is the patient who brings the two algorithms together: a mucus plug in the tracheostomy may coexist with a leaking gastrostomy, and the priority is always the airway. The technology-dependent child at home or in a rural setting is managed by a written emergency plan, a carer trained in basic troubleshooting, and a clear escalation pathway to the nearest emergency department, because the first responder is often a parent. [1] [7]
Complications & Pitfalls
Device complications are predictable, and the pitfalls are the errors a prepared team avoids. State them by name. [1] [4]
T.R.A.C.T. — the dangerous pitfalls in device care
The buried bumper is the gastrostomy pitfall: a tube that has migrated is forced to feed against tissue, causing pain, leakage and, ultimately, gastric perforation or peritonitis. The response is to stop feeding and refer, never to push. The tracheoinnominate fistula is the tracheostomy pitfall: a late sentinel bleed dismissed as granulation, followed by fatal haemorrhage; the response is a high index of suspicion, cuff hyperinflation, and surgical referral. The fractured central line left unclamped is the line pitfall: air embolism or exsanguination from a few centimetres of exposed, broken tubing; the response is an immediate clamp between the child and the break. [2] [5] [8]
A further pitfall is to confuse a cuff leak with tube obstruction: a ventilated child with a falling tidal volume from a cuff leak is not obstructed and should not have the tube removed; instead, the cuff is reinflated to the minimum sealing volume. The reverse error — attributing true obstruction to a cuff leak — delays the life-saving removal of a blocked tube. The distinction is made by passing a suction catheter: if it passes freely and the child remains difficult to ventilate, suspect a cuff leak; if it will not pass, suspect obstruction. [4] [7]
Prognosis & Disposition
The disposition of a child after a device emergency is set by the severity of the event and the maturity of the device. A child who has been decannulated, obstructed, or who has lost a central line to a fracture or infection belongs in a high-dependency or intensive-care setting for observation, because the recurrence risk is highest in the hours immediately after. [3] [8]
A child with a freshly re-placed gastrostomy in a mature tract, with position confirmed and feeding tolerated, may stay on the ward with a clear plan and spare devices at the bedside. A child with a repaired central line is monitored for further fracture and infection, and a decision is made to replace an irreparable line. A child with a tracheostomy who has been re-cannulated after an obstruction or decannulation is observed for recurrent obstruction, for the cause of the event (thicker secretions, inadequate humidification, a poorly secured tube), and for any hypoxic injury sustained during the arrest. [4] [6]
The long-term prognosis is excellent once the device is functioning and the cause is addressed, but the technology-dependent child is a patient for years, and the quality of their care depends on the team's preparation: a written plan, a rehearsed algorithm, a stocked bedside, and a clear escalation pathway. [1] [7]
Special Populations
Some children carry a device risk that changes the response from the first contact, and recognising them is the mark of safe practice. [4] [8]
The complex, technology-dependent child — typically a child with severe neurodisability, chronic lung disease, or a metabolic or oncological condition — is the patient who carries several devices at once and whose carer knows the devices better than the on-call team. The safest response is to listen to the carer, to use the child's written emergency plan, and to call the child's usual team for the device specifications and the spare equipment. [1] [7]
The immunocompromised child with a central line has a higher risk of line infection and a lower threshold for empirical antibiotics; the decision to remove a tunnelled line weighs the risk of losing long-term access against the risk of persistent bacteraemia, and it is made with the oncology or infectious diseases team. The neonate with a central line has a small lumen volume, a high thrombosis risk, and a low tolerance for volume, so the thrombolytic dose is weight-based and the dwell is aspirated rather than flushed. [8] [11]
The child in a rural or remote setting, or at home, is managed by a written plan, a trained carer, and a clear pathway to the nearest emergency department, with the basic algorithms (replace a mature gastrostomy, suction and remove an obstructed tracheostomy, clamp a fractured line) executable before transfer. The retrieval team must be told exactly which device has failed and what has been done. [3] [4]
Evidence, Guidelines & Regional Differences
The guidelines that anchor device troubleshooting — the National Tracheostomy Safety Project algorithm, the RCH Melbourne gastrostomy and tracheostomy guidelines, the AIEOP central-line occlusion and thrombosis recommendations of Giordano, the thrombolytic dwells of Anderson and Baskin, and the CLABSI prevention strategies of Buetti — converge on rehearsed algorithms, weight-based drugs, and a daily review of device necessity, but a few evidence points are worth knowing for the exam. [8] [12]
The thrombolytic dwell for a thrombotic central-line occlusion is supported by the Baskin data and Anderson's paediatric review, which showed alteplase restoring flow in the large majority of occluded paediatric lines with a low rate of complications; the regimen is weight-based, with a dwell of two to four hours, repeated once. The AIEOP recommendations extend this to a structured occlusion and thrombosis pathway for the oncology child, pairing the lock with a decision about anticoagulation when thrombosis rather than occlusion is the problem. [9] [10]
In ANZ, the National Tracheostomy Safety Project algorithm and the RCH Melbourne guidelines set the tracheostomy and gastrostomy standards; the CLABSI bundle is embedded in PICU and oncology practice with a daily review of line necessity. In the UK, the NTSP is the primary tracheostomy emergency reference, and NICE and RCPCH guidance converge on rehearsed algorithms and weight-based thrombolysis. In North America, PALS and the CDC converge on the same resuscitation-first and CLABSI-prevention principles. Where guidelines differ on a dose, a dwell time, or a dressing, name the guideline you are following and state both values with the regional label rather than invent a compromise. [4] [12]
Exam Pearls
The exam will test three things above all: the tracheostomy emergency algorithm, the distinction between mature and immature tracts, and the categorisation of central-line occlusion by cause. Have these ready to say aloud. [3] [8]
For the tracheostomy, recite the National Tracheostomy Safety Project algorithm in order: assess, suction, remove the inner cannula, deflate the cuff, remove the tube and ventilate. State the tract-maturity rule: a tract is immature for the first seven to ten days, and an immature tract must not be re-instrumented blindly. For a late tracheostomy bleed, name the tracheoinnominate fistula, cuff hyperinflation, and surgical referral. [4] [5]
For the central line, categorise occlusion as mechanical, thrombotic, or drug precipitate; give the thrombolytic dwell as weight-based alteplase for two to four hours repeated once; and clamp a fractured line between the child and the break before repair. For the gastrostomy, state that a tube out of an immature tract (under six to eight weeks) must be replaced within hours, that a buried bumper presents with leakage and resistance to feeding, and that a re-placed tube in a mature tract is confirmed by pH or contrast before feeding. Finally, in every device emergency, resuscitate the child before the hardware. [1] [9]
References
- [1]Novak I Gastrostomy Tubes: Indications, Types, and Care. Pediatr Rev, 2024.PMID 38556513
- [2]Sutherland C Pediatric gastrostomy tubes and techniques: making safer and cleaner choices. J Surg Res, 2017.PMID 29180216
- [3]Wynings EM Accidental Tracheostomy Decannulations in Children: A Prospective Cohort Study of Inpatients. Laryngoscope, 2023.PMID 35712851
- [4]Willis LD Pediatric Tracheostomy Year in Review. Respir Care, 2024.PMID 38626953
- [5]Chauhan JC Tracheoinnominate Artery Fistula Formation in a Child with Long-Term Tracheostomy Dependence. J Pediatr Intensive Care, 2019.PMID 31093462
- [6]Chiaravalli J Management of an Obstructed Tracheostomy in a Limited-Resource Setting. Cureus, 2017.PMID 28616369
- [7]Espinel AG Tracheostomy manipulations: Impact on tracheostomy safety. Pediatr Investig, 2019.PMID 32851308
- [8]Giordano P Recommendations for the use of long-term central venous catheter (CVC) in children with hemato-oncological disorders: management of CVC-related occlusion and CVC-related thrombosis. Ann Hematol, 2015.PMID 26300457
- [9]Anderson DM Alteplase for the treatment of catheter occlusion in pediatric patients. Ann Pharmacother, 2013.PMID 23463740
- [10]Baskin JL Thrombolytic therapy for central venous catheter occlusion. Haematologica, 2012.PMID 22180420
- [11]Park CK Neonatal central venous catheter thrombosis: diagnosis, management and outcome. Blood Coagul Fibrinolysis, 2014.PMID 24477225
- [12]Buetti N Strategies to prevent central line-associated bloodstream infections in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol, 2022.PMID 35437133