Paeds · investigations-procedures-and-technology
Intraosseous access
Also known as IO access · Intraosseous infusion · Bone marrow access · EZ-IO insertion · Proximal tibial IO needle
A fellowship approach to intraosseous access in children covering the indication (failed intravenous access within 60 to 90 seconds in shock, arrest or status epilepticus), why the marrow cavity is a non-collapsible vein, the proximal tibial landmark (flat anteromedial surface one to two centimetres below the tibial tuberosity), device and needle-set selection by weight (EZ-IO 15 mm pink for 3 to 39 kg, 25 mm blue for 40 kg and over, 45 mm yellow for the adolescent or oedematous child), the stepwise insertion technique, confirmation, drug and fluid administration at intravenous doses, the preservative-free lidocaine 0.5 milligram per kilogram dose for infusion pain in the conscious child, the complications of extravasation and compartment syndrome, removal within 24 hours, and the neonatal and pre-hospital scenarios.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a two-year-old brought to the emergency department cold, grey, and unresponsive with fulminating septic shock. The registrar cannot find a vein. Every second spent hunting for a peripheral cannula is a second the brain and heart go without perfusion. Intraosseous access is the answer to exactly this moment: a needle driven through the hard outer cortex of a bone into the soft, blood-filled marrow cavity inside, so that fluids and drugs can be delivered straight into the circulation. [1] [3]
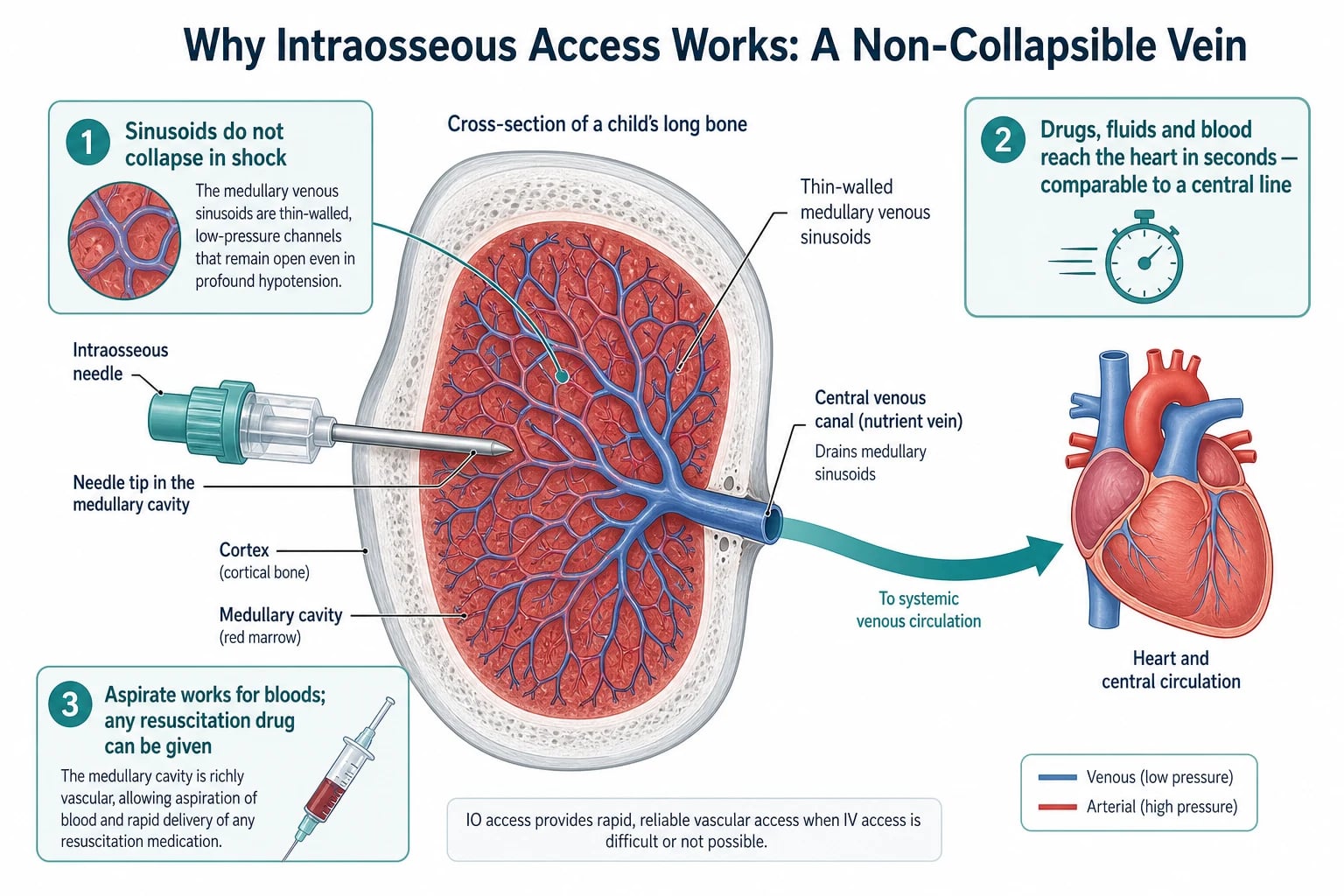
Intraosseous (IO) access means placing a rigid needle through the cortex into the medullary cavity of a long or flat bone. The marrow space is not a dead-end: it holds a dense network of thin-walled venous channels that drain through a central venous canal into the systemic circulation. Because the bone holds these channels open, they do not collapse when the child is in shock — and that is the whole reason IO works when peripheral veins do not. [9] [12]
The procedure is old — first described in the 1920s and a mainstay of military and paediatric resuscitation for decades — but it was the arrival of the battery-powered drill in the 2000s that made it fast and reliable enough for routine first-line use. Today the EZ-IO drill is the default device across Australian and New Zealand paediatric and retrieval services, and a fellowship candidate is expected to know not only how to place the line but when to stop trying for a vein and place one. [7] [10]
Classification
The candidate should hold two classifications in mind at once: the device you use and the site you choose. The two decisions interact, because needle length depends on both the size of the child and the thickness of the soft tissue over the chosen bone. [1] [9]
By device, three families exist. The manual trocar needle (Jamshidi-type) is twisted in by hand and is slow, fatiguing, and less often successful. The spring-loaded impact gun (Bone Injection Gun) fires a needle to a fixed depth and is hard to control in a small infant. The battery-powered drill (EZ-IO) drives a needle with a stylet through the cortex in under two seconds and is now first-line in nearly all paediatric services because it is fast, controllable, and highly successful. [7] [10]
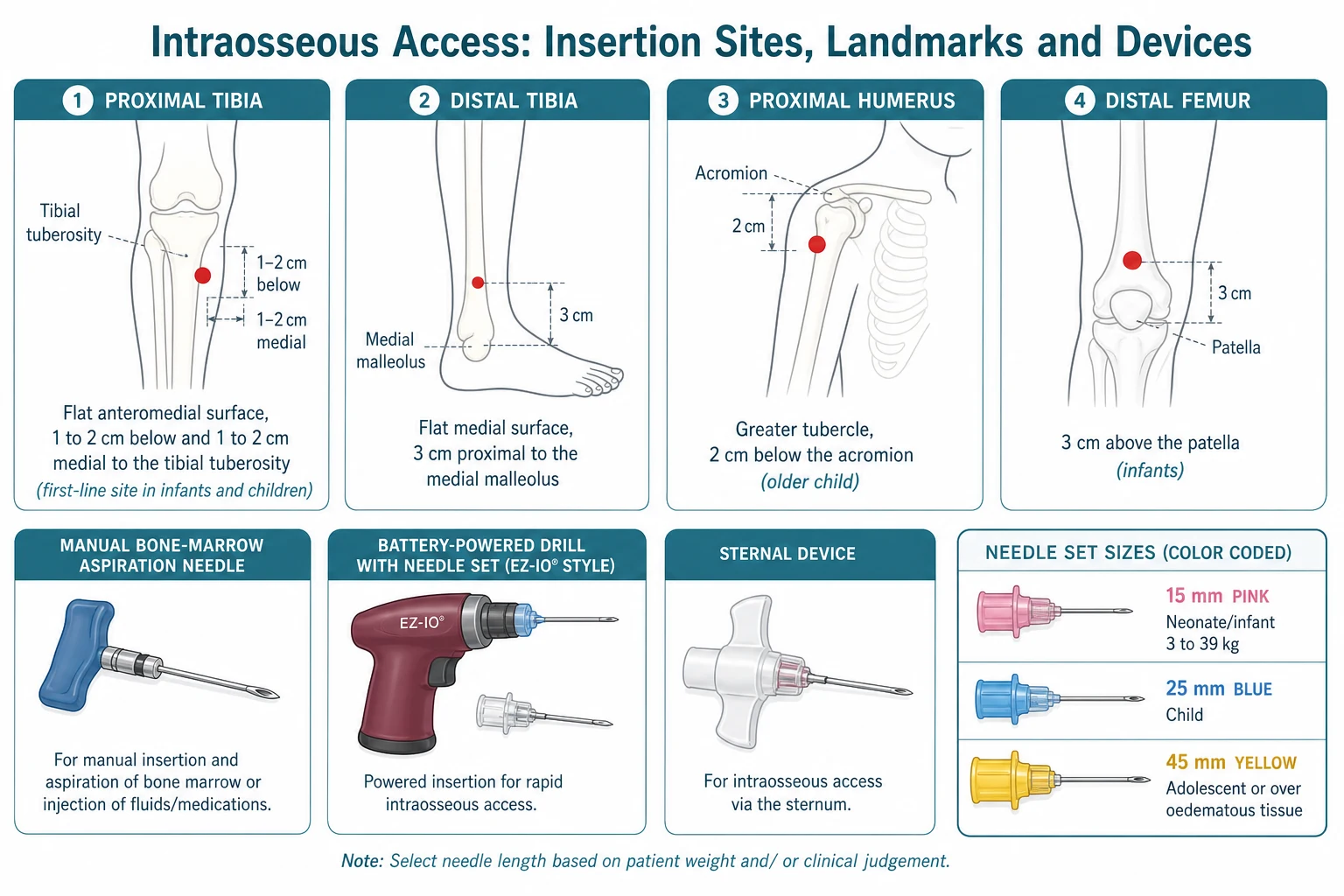
By site, four locations are used in children. The proximal tibia is the first-line site in infants and children because the landmark is easy and the bone is broad and flat. The distal tibia (flat medial surface, about three centimetres above the medial malleolus) is an alternative when the proximal tibia has already been used or is injured. The proximal humerus (the greater tubercle, about two centimetres below the acromion) is used in the older child and adolescent and gives the fastest return of drug to the central circulation. The distal femur (about three centimetres above the patella) is reserved for small infants. Sternal devices are restricted to older adolescents and adults and are not used in young children in any region. [1] [8]
Epidemiology & Risk Factors
Intraosseous access is used in roughly one in a hundred paediatric resuscitations, and far more often in the under-six age group, where peripheral cannulation fails most frequently. The children who need it are predictable: the infant or toddler with septic shock whose periphery has shut down, the child in cardiac arrest, the child in status epilepticus who cannot hold still, the burned child, the oedematous child, the obese child, and the technology-dependent child with sclerosed veins from repeated line access. [3] [5]
A single number carries the epidemiology: with a modern drill device, first-attempt success exceeds 80 to 90 per cent, and the access is secured in well under a minute. Manual needles are slower and succeed less often. This success rate is why pre-hospital and rural services now mandate IO as first-line after a failed intravenous attempt rather than a last resort. [5] [7]
Previously well infant
Septic shock, periphery shut down
- Peripheral veins invisible and collapsed
- Proximal tibial IO within 60 to 90 seconds
- Drill with 15 mm needle (under 3 kg use shortest available)
- Flush, give adrenaline and fluid at IV doses, then definitive access
Older child in arrest
In-hospital or pre-hospital
- Proximal humerus an option for faster central drug return
- 25 mm blue needle for 40 kg and over
- Adrenaline IO at the IV dose, flush after each drug
- Defibrillation drugs, glucose and fluid all given IO
Neonate in delivery room
Umbilical access failed
- IO is rescue when UVC cannot be placed
- Use a dedicated short neonatal needle
- Simulation data support semi-automatic devices
- Remove as soon as UVC or peripheral line is secured
Oedematous or obese child
Thick soft tissue over bone
- Use a 25 mm or 45 mm needle to reach cortex
- Palpate the tuberosity firmly before inserting
- Beware a shallow insertion that misses the marrow
- Confirm with a firm, stable needle and an easy flush
Pathophysiology
The reason intraosseous access works is a single physical fact: the marrow venous channels sit inside a rigid bony box, so they cannot collapse. In shock, the peripheral veins you cannot see have shut down, but the medullary sinusoids stay open. A needle placed in the marrow therefore delivers fluid and drugs into a functioning vascular space no matter how vasoconstricted the child. [9] [12]
Trace the path of a bolus given down an intraosseous line. The fluid enters the medullary cavity, passes into the thin-walled venous sinusoids, collects in a central venous canal, and leaves the bone through the nutrient vein into the systemic circulation. From there it reaches the heart in seconds, with drug-onset times comparable to a central line. This is why every intravenous drug — adrenaline, glucose, anticonvulsants, antibiotics, muscle relaxants, and anaesthetic agents — is given intraosseously at exactly the intravenous dose. [1] [12]
The marrow is also a window for laboratory testing. Marrow aspirate can be sent for blood gas, glucose, urea and electrolytes, blood group and cross-match, and culture, and the results are clinically valid even if some values differ slightly from a venous sample. Aspiration does more than confirm placement: it can save a second, harder cannulation when the child needs bloods taken urgently. [12]
Two consequences of this physiology govern practice. First, gravity flow through the marrow is slow, because the rigid cavity resists flow; rapid resuscitation needs a pressure bag or a syringe bolus. Second, the marrow and periosteum are richly innervated, so an infusion in a conscious child is genuinely painful — the basis for the specific lidocaine dose described later in this topic. [1] [9]
Clinical Presentation
The child who needs an intraosseous line never announces it with a labelled sign. You recognise the need by recognising the situation: a critically ill child plus failed intravenous access. The presentations cluster around four scenarios. [3] [5]
The first is the child in shock — septic, hypovolaemic, or anaphylactic — whose periphery is cold and shut and whose veins have disappeared. The second is the child in cardiac arrest, where intraosseous access does not interrupt chest compressions and delivers adrenaline to the heart in seconds. The third is the child in status epilepticus who cannot hold still for cannulation and who needs lorazepam, midazolam, and glucose without delay. The fourth is the peri-arrest child — the DKA with profound acidosis, the near-drowning, the severe trauma — where you can see deterioration coming and cannot afford to wait. [1] [2]
In the neonate, the presentation is the delivery-room or NICU resuscitation where umbilical venous access has failed or is taking too long. An intraosseous needle in the proximal tibia is a recognised rescue option and can be life-saving in the first minutes of life. [4] [6]
Differential Diagnosis
There is no differential diagnosis of intraosseous access itself — it is a procedure you either perform or you do not. The relevant question is which alternative route of access is realistic in the time you have, and that judgement turns on the child's age and stability. [9]
The realistic alternatives are a peripheral intravenous cannula, the umbilical venous catheter in the neonate, a central venous line, and a surgical cut-down. A peripheral line is preferred when it can be placed quickly; a central line and a cut-down take too long in cardiac arrest and are reserved for the stabilised child. In the neonate, the umbilical vein is first choice and intraosseous is rescue. The decision rule keeps the differential practical: try the quickest route first, and move to IO within 60 to 90 seconds if it fails. [1] [4]
The second differential worth holding is the cause of a failed insertion. If the line does not flush, consider through-and-through penetration of both cortices, a sub-periosteal position, a bent or blocked needle, the wrong site, or — in a child with a metabolic or dysplastic bone disease — an unexpectedly hard or brittle cortex. Each has a corrective action: remove, choose a shorter needle or shallower angle, re-palpate the landmark, or move to the other limb. [3] [8]
Clinical & Bedside Assessment
The bedside assessment is about the site: choosing it correctly and confirming it is safe before you drill. Do this by palpation, not by eye, because the tuberosity is felt more easily than it is seen in a chubby or oedematous leg. [1]
For the proximal tibia, run your thumb up the shin to the firm bump of the tibial tuberosity, then move one to two centimetres down and one to two centimetres medial onto the broad flat anteromedial surface. That flat patch is the insertion point. It is medial to avoid the growth plate, which sits in the epiphysis above the tuberosity, and it is below the tuberosity to reach the metaphysis, where the marrow cavity is widest and most vascular. [1] [9]
Before drilling, check the site is safe. Do not insert through a fractured bone, through infected or burned overlying skin, at a site used for an intraosseous needle in the previous 24 to 48 hours, or in a limb that carries a vascular graft or prosthesis. If any of these apply, choose the other limb or the proximal humerus. [3]
Confirmation after insertion turns on four signs. The needle should stand firmly upright without support, like a tent peg in firm ground. You may be able to aspirate marrow or blood into a syringe — and you can send that sample to the laboratory. A saline flush should run in easily with no resistance and no swelling of the calf. And the limb distal to the line should remain soft, warm, and well perfused. The common trap is reading a failed aspiration as a failed line: aspiration often fails even with perfect placement, so an easy flush with no swelling is the more reliable confirmation. [1] [12]
Landmark and confirmation
Investigations
No investigation is required before inserting an intraosseous line in an emergency. The decision is clinical and the procedure is immediate. Imaging has a limited role after insertion: request a plain radiograph only if you suspect a complication such as a fracture or unrecognised extravasation, or as part of a transport handover in some services. [3]
The marrow aspirate is itself an investigation worth taking. Send it for blood gas and glucose, urea and electrolytes, blood group and cross-match, and culture. Values are clinically usable; a few (notably potassium and some haematology indices) can differ from venous blood, so label the sample as marrow aspirate on the request form. Taking marrow for bloods can spare the child a separate, harder cannulation once the acute event has settled. [12]
The monitoring that matters after placement is distal limb observation: colour, warmth, capillary refill, and — above all — limb firmness and circumference. A limb that becomes swollen, firm, or painful while the infusion runs is extravasating, and the line must be stopped and removed at once. This single observation guards against the feared late complication of compartment syndrome. [3] [11]
Management — Resuscitation
Intraosseous access is a resuscitation tool, and the resuscitation rules are short. Drugs, fluids, and blood products are all given intraosseously at the intravenous dose. Adrenaline in cardiac arrest is 10 micrograms per kilogram, glucose for hypoglycaemia is 2 to 5 millilitres per kilogram of 10 percent dextrose, and fluid boluses in shock are 10 to 20 millilitres per kilogram of isotonic crystalloid — the same numbers you would use intravenously. After each drug, flush with saline to drive it into the central circulation. [1] [2]
Rapid fluid resuscitation needs help. Gravity flow through the marrow is too slow for shock, because the rigid cavity resists flow, so use a pressure bag inflated to 300 millimetres of mercury or a syringe-pump bolus to push each 10 to 20 millilitre per kilogram aliquot in efficiently. Without a pressure bag, you will under-resuscitate and mistakenly think the child is not responding. [1] [9]
Adrenaline (cardiac arrest)
Dose
10 micrograms per kilogram (0.1 mL/kg of 1:10,000)
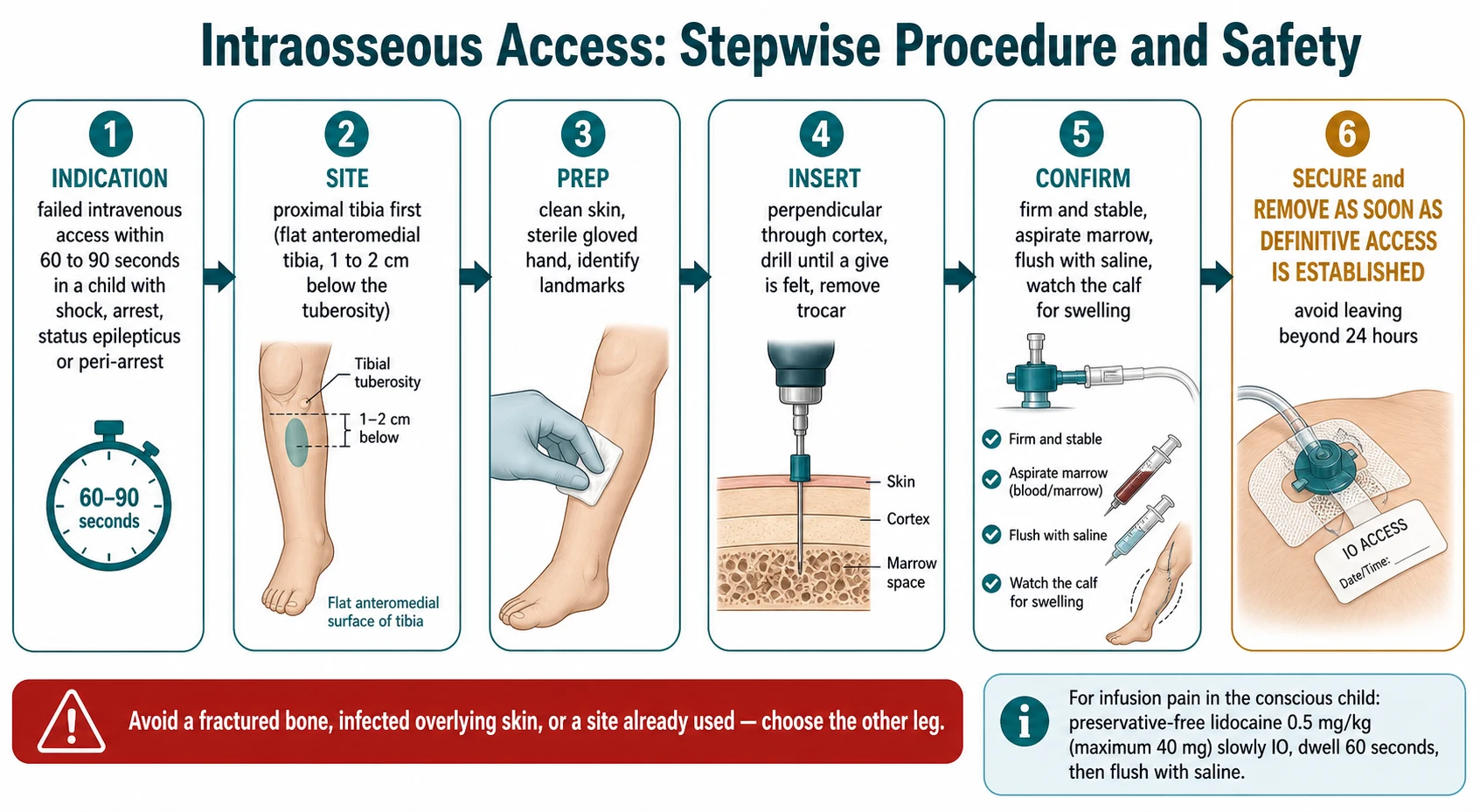
The conscious child deserves analgesia for the infusion. The marrow and periosteum are innervated, and a fluid running into the cavity is genuinely painful. The specific treatment is preservative-free lidocaine 0.5 milligram per kilogram (maximum 40 milligrams) injected slowly into the intraosseous line over about two minutes, allowed to dwell for 60 seconds, then flushed with saline. If pain returns, half the initial dose may be repeated. Use preservative-free, epinephrine-free lidocaine, because preservatives and epinephrine are harmful in the marrow. [1]
Management — Definitive & Stepwise
Once the resuscitation decision is made, the procedure itself is seven ordered steps. Run through them the same way every time, on a manikin until they are automatic, and they will stay automatic in a real arrest. [1]
The intraosseous procedure, in order
1 · Decide
Confirm the indication — shock, arrest, status epilepticus, or peri-arrest with no IV within 60 to 90 seconds. Name the operator and state the decision aloud.
2 · Choose site and needle
Proximal tibia first. EZ-IO 15 mm pink for 3 to 39 kg, 25 mm blue for 40 kg and over, 45 mm yellow for the adolescent or oedematous child.
3 · Prepare
Clean the skin, don sterile gloves, and palpate the flat anteromedial tibia one to two centimetres below and medial to the tuberosity.
4 · Insert
Hold the drill perpendicular to the skin. Apply gentle pressure and drill until you feel a distinct give as the cortex breaches. Stop, and remove the stylet.
5 · Confirm
The needle stands firm. Aspirate marrow if you can (failure to aspirate does not mean failure of the line). Flush with saline — it should run easily with no calf swelling.
6 · Secure and use
Attach the extension set, secure with a dressing, label the line, and begin fluids and drugs. Give IO lidocaine to the conscious child before the infusion.
7 · Remove early
Remove as soon as a reliable IV or central line is in place, and within 24 hours. Apply firm pressure, dress the site, and document and observe the limb.
A few technique points separate a clean insertion from a failed one. Angle the needle perpendicular to the skin, never angled down toward the ankle, because an oblique track risks the growth plate and a shallow position. Stop drilling the instant the cortex gives way — the drill is meant to penetrate bone, not marrow, and over-driving bends the needle and traumatises the cavity. Remove the stylet before connecting the line, or nothing will run. And do not reinsert a stylet into a needle that is already placed. [1] [8]
| Needle set | Length and colour | Patient weight or tissue | Typical site |
|---|---|---|---|
| 15 mm | Pink | 3 to 39 kg (infant and child) | Proximal tibia; distal tibia |
| 25 mm | Blue | 40 kg and over, or any age with thicker soft tissue | Proximal tibia; proximal humerus |
| 45 mm | Yellow | Adolescent or adult, or oedematous tissue over bone | Proximal humerus; proximal tibia |
[1] [9] Needle lengths follow the EZ-IO instruction for use; always confirm the set against the child's weight and tissue depth, and choose the next length up if the needle does not reach the cortex.
Specific Subtypes & Scenarios
Four scenarios recur in fellowship vivas and OSCE stations, and each has its own twist. The first is the neonate in the delivery room or NICU. When umbilical venous access fails or is delayed, an intraosseous needle in the proximal tibia is a recognised rescue. Use a dedicated short neonatal needle, because a standard needle is too long for the thin neonatal cortex. Simulation and systematic-review evidence show that semi-automatic devices are feasible and fast in term neonates, and neonatal life-support algorithms now list IO as a rescue route. [4] [6]
The second is the older child or adolescent, where the proximal humerus comes into its own. The humeral route delivers drug to the central circulation a little faster than the tibia, which matters in cardiac arrest, and the out-of-hospital data show first-attempt success comparable to the tibia. The trade-off is technical: the landmark (the greater tubercle, about two centimetres below the acromion, with the arm adducted and the hand resting on the abdomen to rotate the tubercle forward) is harder to teach and to feel. Most services teach the tibia first and the humerus second. [8]
The third is status epilepticus. The convulsing child cannot hold still for cannulation, and every minute of untreated seizure raises the risk of neuronal injury. An intraosseous line lets you give lorazepam or midazolam and check and correct glucose within a minute of the decision. The same logic applies to the child with severe diabetic ketoacidosis who is slipping toward coma and whose veins are depleted by dehydration. [1] [3]
The fourth is the rural and retrieval setting. Intraosseous competence is an equity issue as much as a clinical one. Aboriginal, Torres Strait Islander, and Māori children, and children in remote communities, present late with sepsis and gastroenteritis with shock, and the nearest doctor may be hours away. A rural clinician who can place an intraosseous line in 60 seconds converts a lethal access failure into a survivable retrieval, and paediatric retrieval services regard the skill as core. [5]
Complications & Pitfalls
Complications are uncommon when the procedure is done well, but the candidate must be able to name and prevent each one, because two of them — extravasation and infection — are directly under your control. [3] [11]
The commonest significant complication is extravasation: fluid leaks out of the marrow through a breach in the cortex and pools in the soft tissue of the calf. The first sign is swelling around the line or a firm limb while the infusion runs. The action is immediate: stop the infusion, remove the needle, apply firm pressure, and choose another site. Unrecognised extravasation is the pathway to compartment syndrome, the feared late complication, in which rising pressure in the calf compromises perfusion and threatens the limb. Watching the limb — colour, warmth, firmness, capillary refill — is the single act that prevents it. [3] [11]
Through-and-through penetration happens when the needle crosses both cortices, usually because too much force was used or the bone is small. Remove the needle, choose a shorter set or a shallower approach, and try the other limb. Fracture and growth-plate injury are prevented by the correct landmark and a perpendicular angle: stay below and medial to the tuberosity, never angle toward the joint. [3]
Infection rises with dwell time. Cellulitis, osteomyelitis, and septic arthritis are rare under 24 hours but become a real risk the longer the line stays in. The rule is unambiguous: remove the intraosseous needle as soon as a reliable intravenous or central line is in place, and certainly within 24 hours. Fat and bone-marrow micro-embolism to the lungs has been documented at autopsy and in animal models after intraosseous infusion; it is usually clinically silent, but it is a real reason to avoid repeated and prolonged use and to remove the line early. [11]
Prognosis & Disposition
Intraosseous access is a bridge, not a destination. Its job is to deliver resuscitation drugs and fluid for the minutes to hours it takes to place a reliable intravenous or central line, and then to come out. Once definitive access is secured, remove the needle, apply firm pressure, dress the site, and document. [1] [3]
After removal, observe the limb for 24 hours for swelling, pain, warmth, or any sign of infection or compartment syndrome, and review the site at handover. The vast majority of children need no follow-up beyond this observation, because the bone and skin heal quickly. A child who develops a swollen, firm, or painful limb in the hours after removal must be assessed urgently for compartment syndrome or osteomyelitis. [3] [11]
The outcome of the episode is driven by the underlying illness — sepsis, arrest, DKA — and not by the access route. What intraosseous access changes is the interval to treatment: it shortens the time from collapse to adrenaline, from seizure to anticonvulsant, and from shock to fluid. The most recent large paediatric out-of-hospital cardiac arrest study found that intraosseous access was achieved faster than intravenous access, but that faster access did not by itself improve survival to discharge — a reminder that IO is about speed of treatment, not a guarantee of outcome. [2]
Special Populations
The neonate deserves a separate line. The cortex is thin and the marrow cavity small, so a dedicated short neonatal needle and a gentle technique matter. Intraosseous access is a rescue in the delivery room and NICU when umbilical venous access fails, and neonatal resuscitation guidance now recognises it as such. Plan the site, keep the limb clear of monitoring leads, and remove as soon as umbilical or peripheral access is secured. [4] [6]
The complex, technology-dependent child often has sclerosed and hard-won veins from repeated access and long-term line use, and intraosseous access becomes a frequent necessity in an acute deterioration. Know which limb carries hardware, keep the limb clear of splints and monitors, and have the kit to hand on the ward and in the PICU rather than only in the emergency department. [3]
The obese or oedematous child defeats a needle that is too short. Choose a 25 or 45 millimetre set, palpate the tuberosity firmly before inserting, and beware the shallow insertion that seats the tip in soft tissue rather than marrow. The child with a bleeding disorder can still receive an intraosseous line in a life-threatening emergency; apply prolonged firm pressure on removal and give factor cover as soon as possible. [1] [9]
For Aboriginal, Torres Strait Islander, Māori, and migrant and refugee children, and for children living in poverty or in remote communities, sepsis and dehydration with shock present late and access is hardest exactly when it matters most. Intraosseous competence in the rural and retrieval workforce is therefore a matter of equity, and a fellowship candidate should frame it that way: this is a skill that closes a gap. [5]
Evidence, Guidelines & Regional Differences
The guidelines are strikingly concordant across regions. The American Heart Association Pediatric Advanced Life Support guidance, the European Resuscitation Council, and the Advanced Paediatric Life Support course used across Australia and New Zealand all place intraosseous access as first-line emergency vascular access when intravenous access cannot be promptly secured in a child. The Royal Children's Hospital Melbourne, NICE and RCPCH in the United Kingdom, and Canadian paediatric life support all align on the same point. [1] [3]
The strongest recent evidence is a 2025 JAMA Network Open study of paediatric out-of-hospital cardiac arrest in Japan, which compared intraosseous and intravenous access for adrenaline. Intraosseous access was achieved more quickly, but there was no difference in survival to discharge. The take-home for the candidate is precise: IO wins on speed of access, which is exactly what it is for, but the underlying arrest physiology determines outcome. [2]
The out-of-hospital literature has also settled the tibia-versus-humerus question. A landmark comparison of first-attempt success between tibial and humeral insertion during cardiac arrest found the two sites comparable; the tibia remains the taught first site because the landmark is easier and the limb is accessible during compressions. [8] Pre-hospital series from Australia confirm high success and a clear move to IO as first-line after a single failed intravenous attempt. [5]
[1] [4]The genuine controversies are narrow. Whether to attempt intravenous access first in cardiac arrest or go straight to intraosseous is unsettled; current consensus is to attempt intravenous first but to move to intraosseous within 60 to 90 seconds rather than prolong failed attempts. Whether routine intraosseous lidocaine should be given to every conscious child before any infusion is supported by the device manufacturer and resuscitation guidance but variably practised. Sternal devices remain restricted to older adolescents and adults and are not part of paediatric practice in any region. [9]
Exam Pearls
A fellowship candidate should leave the examiner with a small set of sharp, sourced facts. Memorise these and you will answer any question on this topic. [1] [3]
The decision rule is the single highest-yield fact: failed intravenous access within 60 to 90 seconds in a sick child equals an intraosseous needle. State it first. The landmark is two finger-breadths below the tibial tuberosity on the medial flat surface — perpendicular, never angled. The needle follows weight: 15 millimetre pink for 3 to 39 kilograms, 25 millimetre blue for 40 kilograms and over, 45 millimetre yellow for the adolescent or oedematous child. [1]
Every drug is given at the intravenous dose, and each is followed by a saline flush. Rapid fluid needs a pressure bag or syringe bolus, because gravity flow through the marrow is too slow. For the conscious child, preservative-free lidocaine 0.5 milligram per kilogram, maximum 40 milligrams, slow IO with a 60-second dwell, then flush relieves infusion pain. [1]
A failed marrow aspirate does not exclude a good line — an easy flush with no swelling is the better test. Remove within 24 hours because infection rises with dwell time. Watch the limb for the feared complication of compartment syndrome from unrecognised extravasation. Never insert through a fracture, infection, burn, or a site used in the last 24 to 48 hours. And remember that proximal humerus gives faster central drug return but the tibia is the taught first site. [1] [11]
References
- [1]Thim T, Løfgren B, Grove EL Intraosseous catheter placement in children New England Journal of Medicine, 2011.PMID 21631349
- [2]Okubo M, Komukai S, Izawa J, et al Intraosseous vs Intravenous Access for Epinephrine in Pediatric Out-of-Hospital Cardiac Arrest JAMA Network Open, 2025.PMID 40560587
- [3]Pifko EL, Price A, Busch C, et al Observational review of paediatric intraosseous needle placement in the paediatric emergency department Journal of Paediatrics and Child Health, 2018.PMID 29125229
- [4]Scrivens A, Reynolds PR, Emery FE, et al Use of Intraosseous Needles in Neonates: A Systematic Review Neonatology, 2019.PMID 31658465
- [5]Ting A, Smith K, Wilson CL, et al Pre-hospital intraosseous use in children: Indications and success rate Emergency Medicine Australasia, 2022.PMID 34704359
- [6]Keller A, Boukai A, Feldman O, et al Comparison of three intraosseous access devices for resuscitation of term neonates: a randomised simulation study Archives of Disease in Childhood Fetal and Neonatal Edition, 2022.PMID 34340986
- [7]Shavit I, Hoffmann Y, Galbraith R, et al Comparison of two mechanical intraosseous infusion devices: a pilot, randomized crossover trial Resuscitation, 2009.PMID 19586701
- [8]Reades R, Studnek JR, Garrett JS, et al Comparison of first-attempt success between tibial and humeral intraosseous insertions during out-of-hospital cardiac arrest Prehospital Emergency Care, 2011.PMID 21275573
- [9]Neuhaus D Intraosseous infusion in elective and emergency pediatric anesthesia: when should we use it? Current Opinion in Anaesthesiology, 2014.PMID 24651308
- [10]Feldman O, Nasrallah N, Bitterman Y, et al Pediatric Intraosseous Access Performed by Emergency Department Nurses Using Semiautomatic Devices: A Randomized Crossover Simulation Study Pediatric Emergency Care, 2021.PMID 30256319
- [11]Hasan MY, Kissoon N, Khan TM, et al Intraosseous infusion and pulmonary fat embolism Pediatric Critical Care Medicine, 2001.PMID 12797872
- [12]Orlowski JP, Porembka DT, Gallagher JM, et al The bone marrow as a source of laboratory studies Annals of Emergency Medicine, 1989.PMID 2589704