Paeds · investigations-procedures-and-technology
Joint aspiration
Also known as Arthrocentesis · Synovial fluid aspiration · Joint tap · Paediatric joint aspiration · Hip aspiration · Synovial fluid analysis
Fellowship guide to joint aspiration (arthrocentesis) in infants and children. Covers the indications, the single biggest question of septic arthritis versus transient synovitis, the Kocher and Caird predictors (fever above 38.5°C, refusal to bear weight, ESR above 40, white cell count above 12,000 and CRP above 20), the relative contraindications of overlying cellulitis and uncorrected coagulopathy, why the deep paediatric hip is aspirated under ultrasound guidance, the synovial fluid cell-count categories that separate septic from inflammatory from non-inflammatory effusions, the sterile technique and landmarks for the knee, hip, ankle and shoulder, the local anaesthetic infiltration and its safe dose, and the common and serious complications including infection seeding and bleeding.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the three-year-old who will not walk, carried into the emergency department with a flexed hip and a face that says pain, or the eight-year-old with a knee swollen tight and hot after a fever. In both, the question the team must answer quickly is whether there is infection in the joint, because septic arthritis dissolves articular cartilage within hours and the only way to answer the question with certainty is to aspirate the synovial fluid and analyse it. That is the territory this page owns. [5] [10]
A joint aspiration (arthrocentesis) is the percutaneous passage of a hollow needle through skin, subcutaneous tissue and the joint capsule into the synovial cavity, to withdraw synovial fluid for diagnostic analysis, to decompress a tense effusion or haemarthrosis, or to instil a drug such as a corticosteroid. The core diagnostic use is the child with a possible septic joint, where the cell count, Gram stain and culture of the fluid settle the diagnosis that no blood test or imaging can settle alone. The therapeutic uses are drainage of a painful effusion, washout of a septic joint in concert with the orthopaedic team, and the intra-articular corticosteroid injection that is a mainstay of juvenile idiopathic arthritis care. [12] [11]
What makes paediatric arthrocentesis a distinct skill from the adult procedure is the child who cannot hold still, the joints that are small and superficial or deep and inaccessible, and the clinical decision that dominates everything else — separating septic arthritis from the common and benign transient synovitis of the hip. The fellowship skill being tested is reading the limping child, applying the prediction rules to decide who crosses the threshold to aspiration, choosing the right joint and the right guidance, and performing a calm single-pass sterile procedure that yields diagnostic fluid without harm. [1] [10]
Classification
Sort the joint aspiration by why it is being done, by which joint is being entered, and by the clinical question that sent you to the needle, because each axis changes the guidance, the needle and the timing. [12] [5]
By purpose, a diagnostic aspiration withdraws fluid for cell count, Gram stain and culture and, rarely, crystal analysis; a therapeutic aspiration decompresses a painful effusion or haemarthrosis, or delivers an intra-articular corticosteroid in juvenile idiopathic arthritis. By joint, a superficial joint (knee, ankle, elbow, wrist, shoulder) is aspirated on surface landmarks in most cases, whereas the deep hip is aspirated under ultrasound guidance because the landmarks are hard to feel and the femoral neurovascular bundle lies close. By clinical question, the procedure that rules out septic arthritis is time-critical and often orthopaedic, the procedure that samples an unexplained effusion is planned and rheumatological, and the procedure that injects a corticosteroid is elective and consented. [12] [7]
By needle, the gauge is chosen to the joint and the likely fluid: a larger-bore needle (18 to 20 gauge) for the knee when pus is expected, because thick pus will not pass through a fine needle, and a finer needle (21 to 23 gauge) for small joints or when a clear effusion is expected; the deep hip may need a longer spinal-type needle to reach the capsule. [12]
The numbers that anchor your viva
Epidemiology & Risk Factors
Joint aspiration is a common procedure in any service that sees children with limp, swelling or fever: the acute limp is one of the commonest paediatric presentations, and a small fraction of those children turn out to have septic arthritis. The incidence of septic arthritis in children is roughly 1 to 40 per 100,000 depending on age and region, highest in the under-fives, and the hip and knee account for the majority of cases. [5] [10]
The risk of a difficult or failed aspiration rises with the small joints of the very young, with obesity, with an uncooperative child, and with any joint in which the effusion is small or loculated. The hip is the classic difficult joint in the infant and toddler precisely because it is deep and the effusion is hard to feel, which is why ultrasound guidance has become the standard. [7] [8]
The risk of a serious complication is concentrated in three groups. The first is the child with overlying cellulitis or a skin infection at the puncture site, in whom the needle can seed skin flora into the sterile joint and cause iatrogenic septic arthritis. The second is the child with an unrecognised bleeding tendency — haemophilia, a coagulopathy, thrombocytopenia or an anticoagulant — in whom the procedure can produce a tense haemarthrosis. The third is the child with a prosthetic joint, in whom aspiration is generally deferred to the orthopaedic team because of the high stakes of prosthetic infection. [12]
A point worth carrying into the viva is that Kingella kingae has become the dominant cause of septic arthritis in young children in the vaccine era, especially between six months and four years, and that Kingella joint infections tend to run a milder, lower-count course than staphylococcal disease. This is why the Kocher and Caird criteria, built in the staphylococcal era, are now re-examined, and why a modest synovial white cell count does not exclude infection in a young child with the right clinical picture. [4] [5]
Pathophysiology
The teaching model runs from the anatomy of a child's joint to the reason a septic effusion looks and counts the way it does, and it rests on a synovial joint that is easy to enter when it is superficial and hard to enter safely when it is deep. [5] [12]
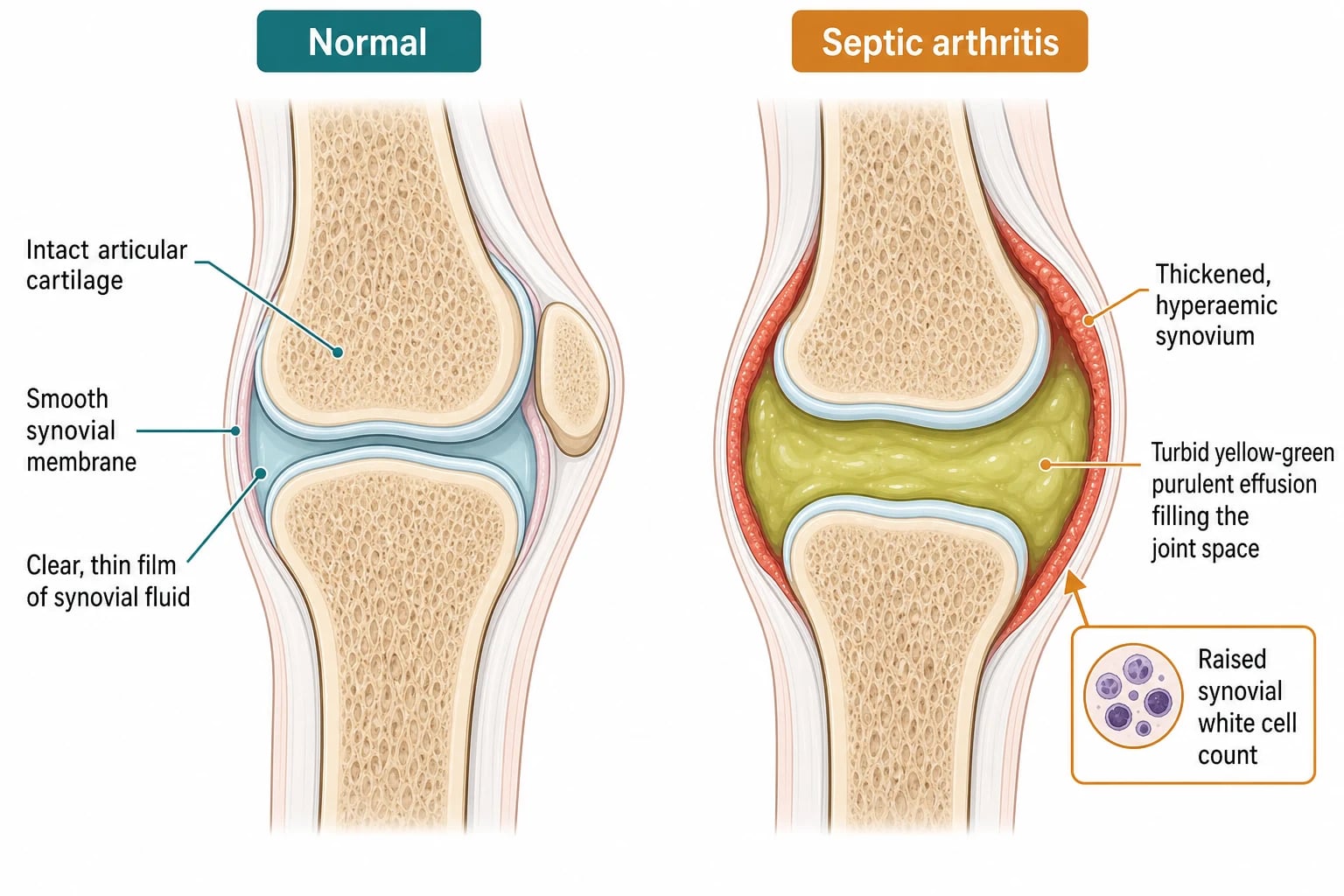
A synovial joint is a low-friction space bounded by articular cartilage and a synovial membrane, lubricated by a thin film of synovial fluid produced by the synovium. In health the fluid is clear, viscous and nearly acellular, holding fewer than 200 white cells per microlitre. When the synovium is inflamed by infection, autoimmunity or crystal deposition it produces more fluid and recruits white cells into the space, so the effusion becomes larger, thinner and progressively more cellular. The synovial white cell count is therefore a direct read-out of how inflamed the joint is, which is why the cell count is the single most useful bedside result from an aspiration. [12]
The mechanism by which untreated septic arthritis destroys cartilage is a combination of pressure and enzymes. The purulent effusion raises intra-articular pressure, which both causes severe pain and compromises the blood supply to the cartilage and the epiphysis, while bacterial and neutrophil proteases digest the proteoglycan matrix of the articular cartilage. Because cartilage has limited capacity to regenerate, the damage becomes irreversible within a day or two, which is the biological reason septic arthritis is a time-critical emergency and aspiration is not deferred. [5]
The reason the deep paediatric hip is aspirated under ultrasound is anatomical. The hip joint lies deep to a thick soft-tissue envelope in the infant and toddler, the effusion cannot be felt, the bony landmarks are cartilaginous and hard to palpate, and the femoral neurovascular bundle lies medial to the joint. A blind pass is as likely to miss the effusion or strike cartilage or vessel as to hit the joint, which is why ultrasound, which shows the effusion and the needle in real time, has become the standard for the hip and is increasingly used for other deep or difficult joints. [7] [8]
Clinical Presentation
The clinical scenarios that prompt aspiration are few and well defined, and the first task at the bedside is to decide which of them you are dealing with, because the urgency, the consent and the team differ. [5] [10]
The commonest diagnostic scenario is the febrile child with an acute hot swollen joint who refuses to use the limb — the toddler who will not walk and holds the hip flexed, abducted and externally rotated, or the older child with a red, hot, exquisitely tender knee. This is septic arthritis until proven otherwise, and the aspiration is the test that settles it. The second is the limping child without a clearly septic joint, in whom the prediction rules and the blood markers are used to decide who crosses the threshold to aspiration and imaging, and who can be observed as presumed transient synovitis. The third is the unexplained chronic or relapsing effusion, often in the rheumatology setting, in whom aspiration confirms an inflammatory picture and supports a diagnosis such as juvenile idiopathic arthritis. [1] [9]
The urgency is graded by the clinical state. The septic, shocked or toxic child is the one in whom resuscitation, blood culture and empirical antibiotics come first, with aspiration and orthopaedic washout as soon as it is safe — but the synovial fluid is obtained before the first antibiotic dose whenever it can be, because culture is the test most affected by prior antibiotics. The well-looking limping child with a low-risk prediction score can be managed conservatively with close observation and repeat assessment. The child with a clear, non-septic effusion can have a planned, consented aspiration. [5] [10]
The presenting features that should move a limping child straight to imaging and aspiration rather than observation are the predictors themselves — a fever above 38.5°C, an inability or refusal to bear weight, severe pain on passive movement, a markedly raised C-reactive protein or erythrocyte sedimentation rate, and an effusion on ultrasound — together with the unwell, toxic or shocked appearance. [1] [6]
| Scenario | Urgency | What it dictates |
|---|---|---|
| Febrile child, hot swollen joint, raised CRP — probable septic arthritis | Emergency | Blood culture, ultrasound-guided aspiration of synovial fluid before antibiotics if feasible, empirical antibiotics, urgent orthopaedic washout |
| Limping child, low-risk prediction score, well-looking | Urgent but observed | Ultrasound to confirm or exclude an effusion; observe and reassess if transient synovitis is the working diagnosis |
| Chronic or relapsing effusion, suspected juvenile idiopathic arthritis | Elective | Planned diagnostic aspiration and rheumatology review; intra-articular corticosteroid injection on the same list |
| Painful haemarthrosis in a boy with haemophilia | Urgent | Factor replacement first; aspiration only if there is diagnostic doubt about sepsis, after haematology cover |
| Prosthetic joint, suspected infection | Urgent | Defer aspiration to the orthopaedic team; do not aspirate in the emergency setting without consultation |
The trap is the child who is well enough to observe at first glance but has an unrecognised high-risk feature — a borderline fever, a CRP that has not yet resulted, or a small hip effusion that is in fact early septic arthritis. The discipline is a structured pre-aspiration assessment that explicitly scores the prediction rule and confirms an effusion before deciding to observe. [3] [6]
Differential Diagnosis
The differential at the bedside is not "what is the swelling" — it is whether to aspirate now, to image first, or to observe, and then what the fluid will mean once you have it. Frame the decision around the prediction rule and the answer follows. [1] [9]
Aspirate now
high risk
- Fever above 38.5°C with refusal to bear weight
- Raised CRP above 20 mg/L or ESR above 40 mm/h, or peripheral WBC above 12,000/µL
- Hot, swollen, tender joint with severe pain on passive movement
- Ultrasound effusion in a deep hip with raised inflammatory markers
Image then decide
- Limp with a possible effusion but a low or intermediate prediction score
- Uncertain whether an effusion is present, especially at the hip
- Child well enough to observe but with one borderline predictor
- Ultrasound separates transient synovitis from a septic-appearing joint
Observe
low risk
- Afebrile, weight-bearing, normal inflammatory markers
- Classical transient synovitis picture after sepsis excluded
- Close observation with a clear safety net and planned reassessment
- Return immediately if fever, worsening pain or refusal to walk
Not a joint tap
- Cellulitis over the joint — aspirate from an uninfected approach or defer
- Uncorrected coagulopathy until corrected
- Prosthetic joint — refer to orthopaedics
- Diagnosis clear and aspiration adds risk without benefit
A second layer of differential is what the synovial fluid result will mean once you have it. A turbid fluid with a white cell count above 50,000 per microlitre and a neutrophil predominance, particularly with a positive Gram stain, points to septic arthritis. A clear or slightly cloudy fluid with a moderate cell count in a well child points to transient synovitis. A persistent inflammatory effusion with a cell count in the inflammatory range points to juvenile idiopathic arthritis or reactive arthritis. A uniformly bloody effusion points to haemarthrosis from trauma or a bleeding disorder, and a bloody aspirate that does not clot raises haemophilic or, rarely, neoplastic disease. [12] [9]
The transient synovitis versus septic arthritis distinction deserves its own sentence because it is the single most tested decision. Transient synovitis is the common, benign, self-limiting cause of the irritable hip in children, usually following a viral illness; septic arthritis is the rare, destructive, time-critical bacterial infection. They overlap clinically, which is exactly why the prediction rules and the synovial fluid analysis exist, and why a child who does not clearly fall into the low-risk transient-synovitis group crosses the threshold to imaging and aspiration. [1] [9]
Clinical & Bedside Assessment
Assessment before aspiration is short, structured and explicit: it scores the prediction rule, examines the joint, checks the overlying skin and the bleeding risk, and decides between aspirate now, image first, or observe. The aim is never to be surprised once the drape is on. [1] [10]
Begin with a focused examination of the joint and the child. Look at the joint for swelling, erythema and warmth, and compare it with the other side. Feel for an effusion and for the temperature difference. Move the joint gently through its range and note the pain at the limit of passive movement — the septic joint is held still and hurts at the slightest movement. Palpate the overlying skin for cellulitis or a wound. Examine the child as a whole for fever, toxicity and signs of shock, and assess the distal neurovascular status of the limb. [5] [10]
Score the prediction rule at the bedside. The Kocher predictors are a fever above 38.5°C, refusal to bear weight, an erythrocyte sedimentation rate above 40 mm per hour and a peripheral white cell count above 12,000 per microlitre; the Caird refinement adds a C-reactive protein above 20 mg per litre. The more predictors present, the higher the probability of septic arthritis and the lower the threshold to aspirate. Remember that external validation found the original high probabilities fall substantially in other cohorts, so the rule is a guide to the threshold for aspiration, not a replacement for clinical judgement. [1] [3]
Check the laboratory results and the bleeding risk that are relevant to the child in front of you. A full blood count, C-reactive protein and erythrocyte sedimentation rate are part of the prediction rule; a blood culture is taken before antibiotics in the unwell child. Ask explicitly about a bleeding history, haemophilia, recent anticoagulants or a known thrombocytopenia, because the coagulopathic or haemophilic child is not aspirated until the bleeding risk is corrected. Confirm the overlying skin is clean. [12] [5]
The pre-aspiration checklist
Score the prediction rule: fever above 38.5°C, refusal to bear weight, ESR above 40, WBC above 12,000, CRP above 20 — how many are present?
Examine the joint: effusion, warmth, erythema, pain on passive movement, and the distal neurovascular status
Is the overlying skin clean? If cellulitis overlies the joint, choose an uninfected approach or defer
Bleeding risk excluded? Platelets, coagulation and haemophilia factor cover confirmed where relevant
Is this a deep hip or a difficult joint? If so, arrange ultrasound guidance before the pass
Consent obtained and documented; analgesia and sedation planned; samples and lab arranged before draping
Investigations
The synovial fluid analysis is the laboratory extension of the procedure, and the candidate must know the cell-count categories, the Gram stain and culture yield, and the blood markers that frame the result. The minimum analysis on a diagnostic aspirate is a white cell count and differential, a Gram stain, and culture; in the relevant child add a crystal analysis, a viral or mycobacterial study, and cytology. [12] [5]
| Category | Synovial white cells per microlitre | Typical paediatric cause |
|---|---|---|
| Normal | Fewer than 200 | No effusion; the joint is not the problem |
| Non-inflammatory | 200 to 2,000 | Transient synovitis, osteoarthritis, trauma without haemarthrosis |
| Inflammatory | 2,000 to 75,000 | Juvenile idiopathic arthritis, reactive arthritis, transient synovitis at the upper end |
| Septic | Above 50,000, often above 100,000 | Bacterial septic arthritis, predominantly neutrophils |
| Haemorrhagic | Bloody throughout | Trauma, haemophilia, rarely neoplasm |
The interpretation turns on a few named patterns. Septic arthritis typically shows a turbid, yellow-green fluid with a white cell count above 50,000 per microlitre and a neutrophil predominance, a Gram stain positive in roughly half to three-quarters before antibiotics, and a positive culture that grows the organism. Transient synovitis shows a clear or slightly cloudy fluid with a moderate, predominantly mononuclear cell count and a negative Gram stain and culture. Juvenile idiopathic arthritis shows an inflammatory fluid in the same child over weeks and months, with a negative culture. Kingella kingae disease can be deceptively mild, with a modest cell count, and requires specific culture or polymerase chain reaction to detect. [4] [12]
The blood markers frame the result and are part of the prediction rule. A C-reactive protein above 20 mg per litre combined with a hip effusion of at least 7 mm on ultrasound carries a high specificity and sensitivity for paediatric hip septic arthritis, and a rising C-reactive protein over serial measurements is a useful marker of response to treatment. The erythrocyte sedimentation rate above 40 mm per hour and the peripheral white cell count above 12,000 per microlitre complete the rule, and a blood culture is positive in a minority but is taken before antibiotics in the unwell child. [1] [6]
Management — Resuscitation
When the child with a septic joint is also septic or shocked, the aspiration is not the first priority — resuscitation is. The ordered bundle is airway, breathing and circulation, a blood culture, empirical intravenous antibiotics, analgesia, and then aspiration and orthopaedic washout as soon as it is safe. [5] [10]
The single most important timing rule in suspected septic arthritis is that the synovial fluid is obtained before the first antibiotic dose whenever it can be, because bacterial culture is the test most affected by prior antibiotics. If the fluid cannot be obtained promptly, give empirical antibiotics after a blood culture and aspirate as soon as the team and the ultrasound are available — the cell count and Gram stain remain useful after a dose, and the polymerase chain reaction for organisms such as Kingella is barely affected. The fear that one antibiotic dose renders the joint uninformative is mistaken, but it is still the reason the fluid is chased early. [5] [4]
Analgesia is part of resuscitation in the child with a painful joint. Position the limb in the position of comfort — the septic hip is often happiest flexed and abducted — give intravenous opiate analgesia titrated to the child, and apply a topical anaesthetic at the aspiration site early so it has time to work by the time the procedure begins. [10] [12]
If the child deteriorates during the assessment — rising fever, falling perfusion, increasing pain or a spreading cellulitis — escalate to senior paediatric and orthopaedic help, broaden the empirical antibiotics, and move the aspiration and washout forward. The septic joint is an orthopaedic emergency: aspiration confirms the diagnosis, but definitive treatment is a surgical washout in most cases, and the paediatric team's job is to diagnose, resuscitate and start antibiotics while mobilising the surgeon. [5] [10]
Management — Definitive & Stepwise
Once the decision to aspirate has been made, the procedure is an ordered sequence that should run the same way every time: consent, preparation, anaesthesia, positioning, sterile field, landmark or ultrasound identification, needle insertion, fluid withdrawal, sample handling, withdrawal and a dressing. [12] [7]
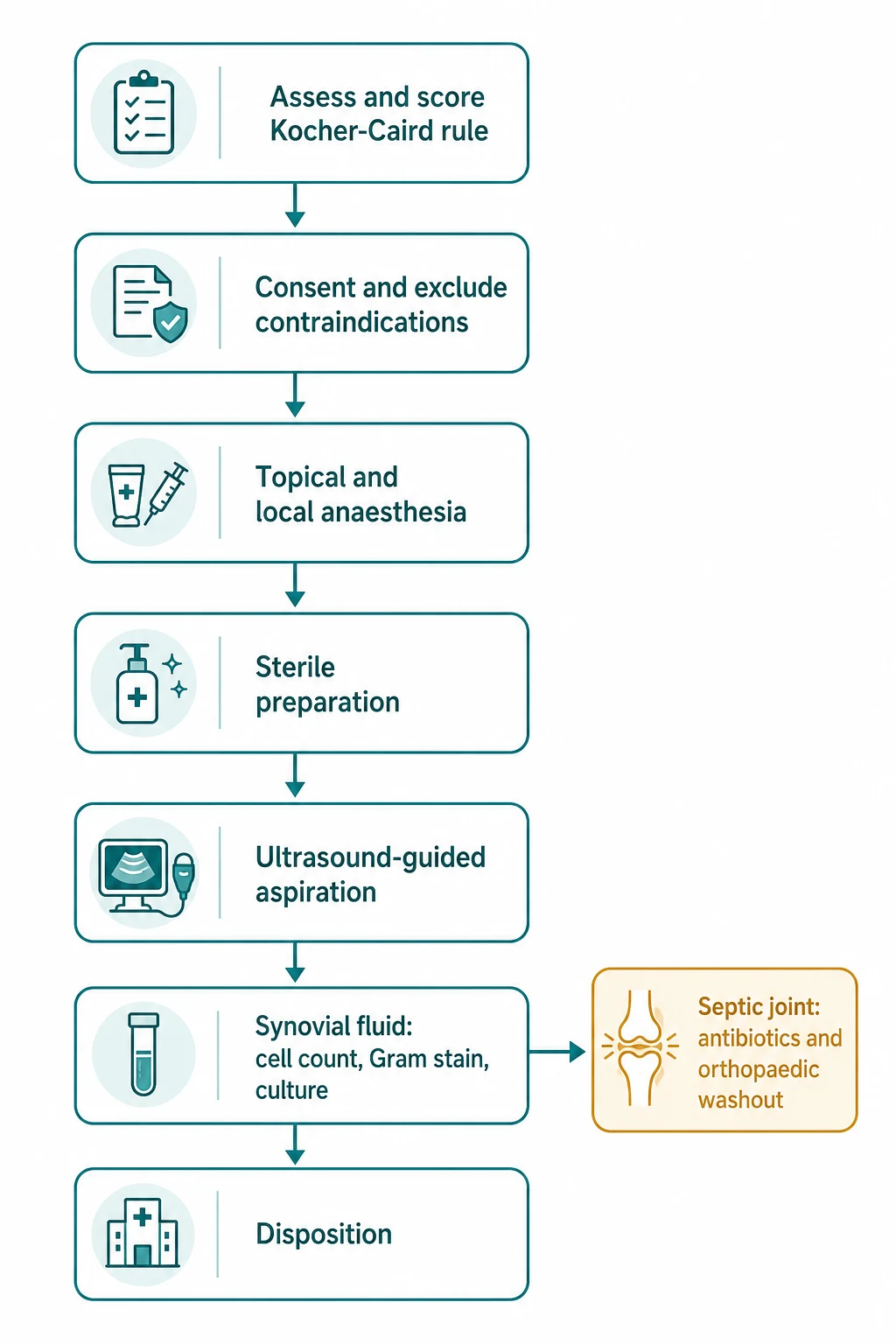
Begin with consent and preparation: explain to the parent and, where appropriate, the child, why the aspiration is needed, what it will feel like, the common discomforts (local pain, transient bleeding) and the serious but rare risks (infection, bleeding, cartilage injury). Document the consent. Apply the topical anaesthetic early — EMLA (lidocaine 2.5% and prilocaine 2.5%) under an occlusive dressing for at least 45 to 60 minutes, or amethocaine 4% for 30 to 45 minutes. Plan procedural sedation if the child cannot hold still, with full monitoring and a trained team. [12] [10]
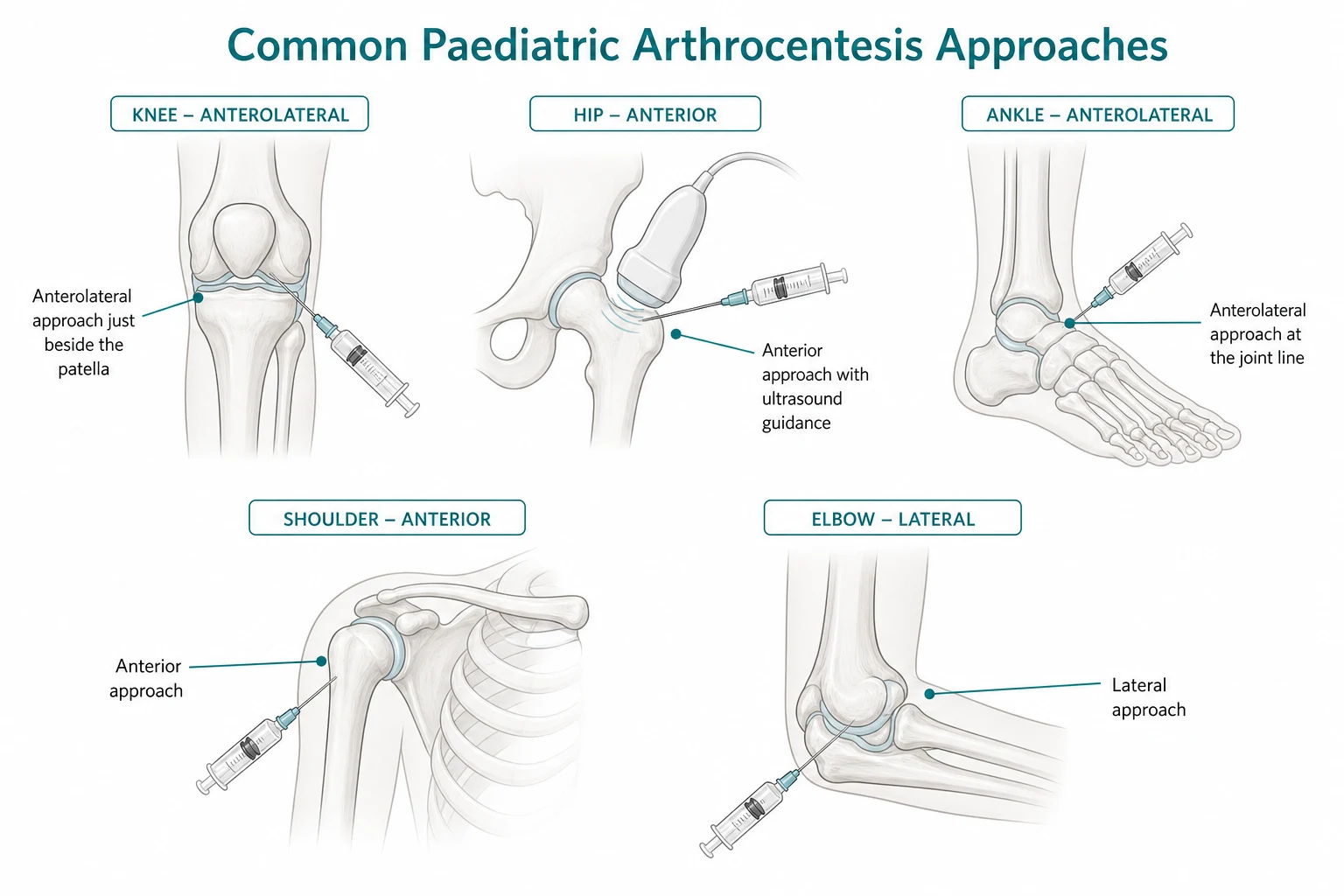
Position the child for the chosen joint and approach. The knee is aspirated supine with the knee slightly flexed, approaching from the anterolateral or anteromedial side just at the margin of the patella, directing the needle under the patella toward the intercondylar notch. The hip is aspirated supine with the leg neutral, under ultrasound guidance, by an anterior approach that enters lateral to the femoral artery pulse and below the inguinal ligament, or a lateral approach over the greater trochanter. The ankle is approached anterolaterally at the joint line, avoiding the dorsalis pedis and extensor tendons, and the shoulder anteriorly just lateral to the coracoid. The exact depth is determined by ultrasound or by the feel of the capsule, not by a fixed measurement. [7] [12]
TAP-JOINT
Under sterile conditions, prepare the skin and drape. Infiltrate the skin and subcutaneous tissues with 1% lidocaine at a maximum of 3 mg/kg without adrenaline, using a small needle and injecting as you withdraw, taking care to stay below the safe dose for the child's weight. Insert the aspiration needle slowly, aspirating gently as you advance; a give is felt as the capsule is breached and fluid enters the syringe. For the hip and any difficult joint, perform the pass under real-time ultrasound guidance. Withdraw as much fluid as is reasonable to relieve pressure and to send for analysis, then withdraw the needle and apply a dressing. [12] [7]
Lidocaine 1% infiltration for arthrocentesis
Handle the dry tap, the bloody tap and the uncooperative child deliberately. A dry tap is most often a positional or guidance problem — reposition, confirm the effusion on ultrasound, and re-advance; multiple blind passes in a struggling child warrant stopping and trying again under sedation and ultrasound. A uniformly bloody aspirate suggests trauma or a bleeding disorder rather than sepsis; a truly septic fluid is turbid rather than frankly bloody. If the child will not tolerate the position, stop, sedate and return, because a moving child turns a safe procedure into a dangerous one. [7] [8]
Specific Subtypes & Scenarios
The approach to aspiration changes with the joint, the child and the clinical question, and the fellowship candidate must adjust the technique to the subtype in front of them. [5] [10]
In the deep paediatric hip, aspiration is performed under ultrasound guidance by an operator trained in the technique, by an anterior approach that enters the joint lateral to the femoral vessels. The hip is the joint in which a blind pass is most likely to miss the effusion or injure cartilage or vessel, and the modern evidence confirms that ultrasound-guided aspiration is feasible and safe in children and is the standard of care for the hip and for any joint in which the effusion is hard to define. [7] [8]
In the superficial knee, the procedure is closer to an adult arthrocentesis: the landmarks are easy, the effusion is palpable, an anterolateral or anteromedial approach under the patella works well, and a larger-bore needle is chosen if pus is expected because thick pus will not pass a fine needle. The focus is on sterile technique, genuine analgesia and a single pass. [12]
In the child with juvenile idiopathic arthritis, the aspiration is often paired with a therapeutic intra-articular corticosteroid injection on the same elective list, performed under anaesthesia or sedation, with the fluid sent to confirm the inflammatory picture and exclude infection before any steroid is instilled. Intra-articular corticosteroid is a mainstay of local JIA therapy and is highly effective, with the procedural detail — the choice of steroid preparation, the volume, the post-injection rest — owned by the rheumatology team. [11]
In the boy with haemophilia and a painful swollen joint, the working diagnosis is a haemarthrosis, not sepsis, and the first step is factor replacement with the haematology team, not aspiration. Aspiration is reserved for the case in which there is genuine diagnostic doubt about sepsis, and it is performed only after adequate factor cover, because passing a needle into an uncorrected haemophilic joint worsens the bleed and can compromise the limb. [12]
In the febrile young child between six months and four years, remember that Kingella kingae is now the dominant organism in many settings and runs a milder, lower-count course; the synovial fluid should be sent for the specific culture or polymerase chain reaction that detects it, and a modest cell count should not reassure against the clinical picture. [4]
In the remote or retrieval setting, where ultrasound and a trained proceduralist may be hours away, the priorities are empirical antibiotics after a blood culture, analgesia and positioning, and aspiration of any accessible superficial effusion; a deep hip aspiration is deferred to the receiving centre, where it is performed under ultrasound once the child is stable. [5] [10]
Complications & Pitfalls
The complications of paediatric arthrocentesis run from the common and self-limiting to the rare and serious, and the discipline is to anticipate the serious ones and prevent them through the pre-aspiration check, while managing the common ones with honesty and evidence. [12] [5]
The common complications are local pain at the puncture site, a small transient haemarthrosis if a synovial vessel is grazed, and a vasovagal response in the anxious older child. Most settle with simple analgesia, rest and observation. After a corticosteroid injection, a post-injection flare of inflammation and local skin or fat atrophy at the injection site are recognised effects that are usually self-limiting. [11] [12]
The serious complications are rare but worth knowing exactly. Iatrogenic septic arthritis is the introduction of skin flora into the sterile joint through poor asepsis, an overlying cellulitis, or a needle passed through infected skin; the protection is sterile technique, a mask and gloves, and choosing an uninfected approach. A tense haemarthrosis can complicate aspiration in the coagulopathic or haemophilic child who has not been corrected, raising intra-articular pressure and compromising the limb; the protection is the bleeding-risk check and factor cover. Cartilage or neurovascular injury is the rare mechanical harm of a misplaced needle, prevented by ultrasound for the deep hip and by a careful single pass for the superficial joint. [12] [8]
A frequently tested misconception is that a synovial white cell count below 50,000 per microlitre excludes septic arthritis. It does not: the cell count is a continuous variable, partially treated and Kingella disease run lower, and the threshold is a guide to probability rather than a rule. The other misconception is that antibiotics should be withheld until the aspiration is done — true when the aspiration is imminent, but in the unwell child the fluid is chased after empirical antibiotics rather than allowing the child to deteriorate untreated. [4] [5]
Prognosis & Disposition
The prognosis after an uncomplicated diagnostic aspiration is excellent: the puncture site heals within days, and most children return to normal activity the same or the next day. The disposition is driven far more by the underlying diagnosis than by the procedure itself. [12] [5]
For confirmed septic arthritis, the disposition is paediatric inpatient or intensive care for intravenous antibiotics, analgesia and monitoring, with an urgent orthopaedic washout in most cases, serial C-reactive protein to track the response, and follow-up for joint function and any growth disturbance. The aspiration is the diagnostic confirmation of a treatment that is already underway. [5] [10]
For transient synovitis, once sepsis is excluded by a low-risk prediction score and a benign aspirate or a confident ultrasound, the disposition is rest, simple analgesia and close observation, usually at home with a clear safety net — return immediately if fever, worsening pain or refusal to walk develops. Most children recover within a week or two. [9] [1]
For juvenile idiopathic arthritis, the disposition is rheumatology follow-up after an intra-articular corticosteroid injection, with local advice on rest and on the expected post-injection course. [11]
For the serious procedural complications — iatrogenic septic arthritis, a tense haemarthrosis, cartilage or neurovascular injury — the prognosis depends on the speed of recognition and definitive management, and the disposition is urgent orthopaedic and infectious-disease consultation and a low threshold for imaging and washout. [12]
Special Populations
The approach to aspiration is adjusted for the child in front of you, and the fellowship candidate must show that they can match the technique to the population. [5] [10]
In the neonate and young infant, a septic joint can present subtly as irritability, reluctance to move a limb or pseudoparalysis rather than the classic hot swollen joint, and the threshold to image and aspirate is lower. The hip is always imaged and aspirated under ultrasound, the needle is finer, and the procedure is coordinated with the orthopaedic and infectious-disease teams. [5]
In the immunocompromised child, including the oncology patient and the transplant recipient, the threshold to aspirate is lower, the organism list is broader, the sterile technique matters more, and any joint pain or fever prompts imaging and aspiration once the bleeding risk is checked. [12]
In the child with haemophilia or a bleeding disorder, the procedure is coordinated with the haematology team: the factor level is corrected before any aspiration, the procedure is reserved for genuine diagnostic doubt about sepsis, and the joint is observed for a re-bleed afterwards. [12]
In the child with juvenile idiopathic arthritis, the aspiration is paired with a therapeutic corticosteroid injection under the rheumatology protocol, with attention to the steroid preparation, the volume, the post-injection rest and the recognition of a post-injection flare. [11]
In the Indigenous, remote or under-resourced setting, the indications are the same but access to ultrasound, to a trained proceduralist and to same-day washout may not be. The equity intervention is to recognise the septic joint on clinical and blood markers, to start empirical antibiotics early, to aspirate what is accessible and to arrange retrieval to a centre that can image and wash out a deep joint. [5]
In the technology-dependent or neurodivergent child, the procedure is planned with extra time, a communication strategy appropriate to the child, an assent process where possible, and a sedation plan that the child and family can support. [10]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric joint aspiration has matured in three areas: the prediction rule for the septic hip, the role of ultrasound guidance, and the changing microbiology of the Kingella era. The candidate should know each one and the regional deltas that follow from them. [1] [5]
The Kocher prediction rule and its validation are the strongest single change in modern practice. The original 1999 algorithm gave a probability of septic arthritis rising from under 1% with no predictors to over 99% with all four; the 2004 validation confirmed a high probability with three or four predictors. Subsequent external validation found that the original high probabilities fall substantially in other cohorts, so the rule is best used as a guide to the threshold for imaging and aspiration rather than as a certainty. The Caird refinement added C-reactive protein to the predictors, and modern evidence combining a C-reactive protein above 20 mg per litre with a hip effusion of at least 7 mm on ultrasound carries a high specificity and sensitivity for paediatric hip septic arthritis. [1] [6]
The ultrasound-guidance evidence has made the deep paediatric hip a guided procedure. Ultrasound shows the effusion, the synovial thickening and the needle in real time, and modern series confirm that ultrasound-guided aspiration of the hip and other joints in children is feasible and safe, with a low rate of re-aspiration and complications. The teaching is now that the hip and any difficult joint are aspirated under ultrasound, while the superficial joints remain a landmark procedure in trained hands. [7] [8]
The Kingella kingae era has prompted a re-examination of the prediction rules built in the staphylococcal age. Kingella is now the dominant cause of septic arthritis in young children in many settings, runs a milder and lower-count course, and requires specific culture or polymerase chain reaction to detect — which is why a modest synovial cell count never excludes infection in the right child, and why the Kocher and Caird criteria are tested and refined rather than applied uncritically. [4]
Kocher prediction algorithm and validation (J Bone Joint Surg Am 1999 and 2004)
PMID 15292409
Population: Children with an irritable hip in whom septic arthritis and transient synovitis must be distinguished
Comparator: The probability of septic arthritis across the range of predictor counts
Key finding
The original algorithm gave a probability rising from under 1% with no predictors to over 99% with four. External validation found the high probabilities fall in other cohorts, so the rule guides the threshold for imaging and aspiration rather than giving certainty. The Caird refinement adds CRP above 20 mg/L.
Where the evidence is weak or contested: the exact cell-count threshold that defines septic arthritis as a single number, the reliability of the Kocher probabilities in the Kingella era, the role of serial aspiration versus immediate washout for the septic hip in some settings, and the optimal steroid preparation and regimen for the intra-articular injection in juvenile idiopathic arthritis. Each is a defensible topic for the viva. [4] [8]
Exam Pearls
The fellowship examiner expects a candidate who knows the prediction rule, the relative contraindications, the synovial fluid categories and the technique, and can defend the procedure at the bedside. [1] [12]
The single most testable decision is septic arthritis versus transient synovitis, scored by the Kocher and Caird predictors: a fever above 38.5°C, refusal to bear weight, an erythrocyte sedimentation rate above 40 mm per hour, a peripheral white cell count above 12,000 per microlitre, and a C-reactive protein above 20 mg per litre. The more predictors present, the lower the threshold to image and aspirate. [1] [3]
The named relative contraindications are overlying cellulitis (aspirate from an uninfected approach or defer), uncorrected coagulopathy or thrombocytopenia and the haemophilic child without factor cover (correct first), and the prosthetic joint (defer to orthopaedics). The imaging-first rule for the deep paediatric hip is that the hip is aspirated under ultrasound guidance, not blind. [12] [7]
The synovial fluid categories must be quoted exactly: normal fewer than 200 white cells per microlitre, non-inflammatory 200 to 2,000, inflammatory 2,000 to 75,000, and septic above 50,000 with a neutrophil predominance. Remember that a count below 50,000 does not exclude sepsis in the partially treated child or in Kingella kingae disease. [12] [4]
The classic distractors the exam rewards for naming: reassuring on a low synovial cell count in a febrile non-weight-bearing child; aspirating a deep hip blind; passing the needle through overlying cellulitis; aspirating a haemophilic child without factor cover; withholding antibiotics in the unwell child while waiting for an aspiration that is not imminent; and treating a hot joint with antibiotics before sending the synovial fluid. Each is wrong for a specific evidence-based reason. [5] [4]
References
- [1]Kocher MS, Zurakowski D, Kasser JR Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction algorithm J Bone Joint Surg Am, 1999.PMID 10608376
- [2]Kocher MS, Mandiga R, Zurakowski D, et al Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children J Bone Joint Surg Am, 2004.PMID 15292409
- [3]Luhmann SJ, Jones A, Schootman M, et al Differentiation between septic arthritis and transient synovitis of the hip in children with clinical prediction algorithms J Bone Joint Surg Am, 2004.PMID 15118038
- [4]Valisena S, De Marco G, Vazquez O, et al The Kocher-Caird Criteria for Pediatric Septic Arthritis of the Hip: Time for a Change in the Kingella Era? Microorganisms, 2024.PMID 38543601
- [5]Nannini A, Giorgino R, Bianco Prevot L, et al Septic arthritis in the pediatric hip joint: a systematic review of diagnosis, management, and outcomes Front Pediatr, 2023.PMID 38188916
- [6]Olandres RA, Seng DWR, Seneviratna A, et al C-reactive protein of at least 20 mg per litre and ultrasound finding of an effusion of at least 7 mm has a high specificity and sensitivity in diagnosing paediatric hip septic arthritis Arch Orthop Trauma Surg, 2023.PMID 37530844
- [7]Cavalier R, Herman MJ, Pizzutilo PD, et al Ultrasound-guided aspiration of the hip in children: a new technique Clin Orthop Relat Res, 2003.PMID 14612652
- [8]Michaud J, Dutron S, Pico J, et al The feasibility and safety of ultrasound-guided puncture for treatment of septic arthritis in children Ital J Pediatr, 2024.PMID 39334397
- [9]Nouri A, Walmsley D, Pruszczynski B, et al Transient synovitis of the hip: a comprehensive review J Pediatr Orthop B, 2014.PMID 23812087
- [10]Naranje S, Kelly DM, Sawyer JR A Systematic Approach to the Evaluation of a Limping Child Am Fam Physician, 2015.PMID 26554284
- [11]Li S, Zhang W, Lin Y Application of Intra-articular Corticosteroid Injection in Juvenile Idiopathic Arthritis Front Pediatr, 2022.PMID 35425732
- [12]Tantillo TJ, Boudreaux S, Katsigiorgis G Arthrocentesis StatPearls, 2026.PMID 32491737