Paeds · investigations-procedures-and-technology
Lumbar puncture in infants and children
Also known as Lumbar puncture · LP · Spinal tap · Paediatric CSF sampling · Cerebrospinal fluid analysis · Intrathecal access
Fellowship guide to lumbar puncture in infants and children. Covers the indications, the absolute contraindications of raised intracranial pressure, coagulopathy, overlying skin infection and the unstable child, the indications for CT before LP, why the infant spinal cord ends at L3 and the safe interspaces this dictates, the lateral decubitus and sitting positions and why opening pressure is reliable only in a calm child in the lateral decubitus position, the atraumatic pencil-point needle and its reduction of post-dural puncture headache, the normal CSF values and the traumatic-tap correction, the topical, local and procedural-sedation analgesia options, the common and serious complications, and the ANZ, UK and North American guideline differences on antibiotics-first in suspected meningitis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the eight-month-old febrile, irritable infant with a bulging fontanelle, or the four-year-old who has had a brief generalised seizure with fever and now looks septic. In both, the question the team must answer is whether there is infection or inflammation in the subarachnoid space — and the only way to answer it reliably is to sample the cerebrospinal fluid by lumbar puncture. That is the territory this page owns. [1] [10]
A lumbar puncture (LP) is the percutaneous passage of a fine, hollow, styletted needle through the skin, supraspinous and interspinous ligaments, ligamentum flavum, dura mater and arachnoid into the lumbar subarachnoid space, below the level where the spinal cord ends, to sample cerebrospinal fluid, measure its pressure, or deliver a drug. The core diagnostic use is suspected meningitis or encephalitis; the other common indications include the septic workup of the young febrile infant, unexplained altered conscious state, suspected idiopathic intracranial hypertension, the staging and intrathecal treatment of leukaemia, and a small number of therapeutic indications such as the removal of CSF in normal-pressure or idiopathic intracranial hypertension. [1] [9]
What makes paediatric LP a distinct skill from adult LP is anatomy that changes with age and a child who cannot be reasoned into holding still. The infant's spinal cord ends lower than the adult's, the dural sac ends lower, the needle and the dose of local anaesthetic must be scaled to the child, and the procedure demands genuine analgesia and often procedural sedation. The fellowship skill being tested is reading the child, choosing the right indication, screening out the contraindications, and performing a calm single-pass procedure that yields diagnostic CSF and a reliable opening pressure without harm. [1] [12]
Classification
Sort the lumbar puncture by why it is being done, by how urgent it is, and by the needle that does the work, because each axis changes the team, the timing, and the harm profile. [1] [9]
By purpose, a diagnostic LP samples CSF for cells, protein, glucose, microscopy and culture, PCR and cytology; a therapeutic LP delivers an intrathecal drug such as methotrexate or cytarabine in oncology, or removes CSF in idiopathic intracranial hypertension. By urgency, an elective LP (leukaemia staging, possible IIH) is planned and consented; an urgent LP (the well-looking febrile infant, the cooperative child with suspected viral meningitis) is done promptly but in a controlled way; a time-critical LP (the child with suspected bacterial meningitis) is the one in which antibiotics come first and the LP follows when it is safe. [1] [10]
By needle, the modern teaching is to use an atraumatic pencil-point needle (Sprotte or Whitacre) wherever possible in preference to a cutting Quincke bevel needle, because systematic review evidence shows the atraumatic design substantially reduces post-dural puncture headache without reducing success. Whatever the type, the needle must be styletted: removing the stylet only after the dural puncture, and replacing it before withdrawal, prevents a core of skin being carried into the subarachnoid space and forming a delayed epidermoid tumour. [2] [3]
The numbers that anchor your viva
Epidemiology & Risk Factors
Lumbar puncture is among the commonest procedures a paediatrician performs: it is a routine part of the febrile-infant workup, of suspected meningitis, and of oncology staging and treatment. The risk of a difficult or failed LP rises with obesity, scoliosis, prior spinal surgery, an uncooperative child, and the very young infant in whom the landmarks are small and the subarachnoid space is narrow. [1] [9]
The risk of a serious complication is concentrated in three groups. The first is the child with raised intracranial pressure from a space-occupying lesion, hydrocephalus, or diffuse cerebral oedema, in whom LP can precipitate cerebral herniation. The second is the child with an unrecognised bleeding tendency — thrombocytopenia, a coagulopathy, or a child on anticoagulants — in whom the procedure can produce a spinal epidural haematoma that compresses the cord. The third is the child with overlying skin infection at the puncture site, in whom skin flora can be seeded into the CSF. [8] [9]
A paradox worth knowing is that post-dural puncture headache is less common in children under five than in adolescents and adults — the younger dura is more elastic and the elastic recoil tends to close the dural perforation — and rises through adolescence to the adult rate. The atraumatic needle and the smaller gauge reduce the risk at any age, which is the modern evidence-based choice. [4] [2]
Pathophysiology
The teaching model runs from the shape of the paediatric spine to the reason a small hole in the dura can cause a headache, and it rests on anatomy that changes with age and on CSF dynamics that are easily disturbed. [1] [9]
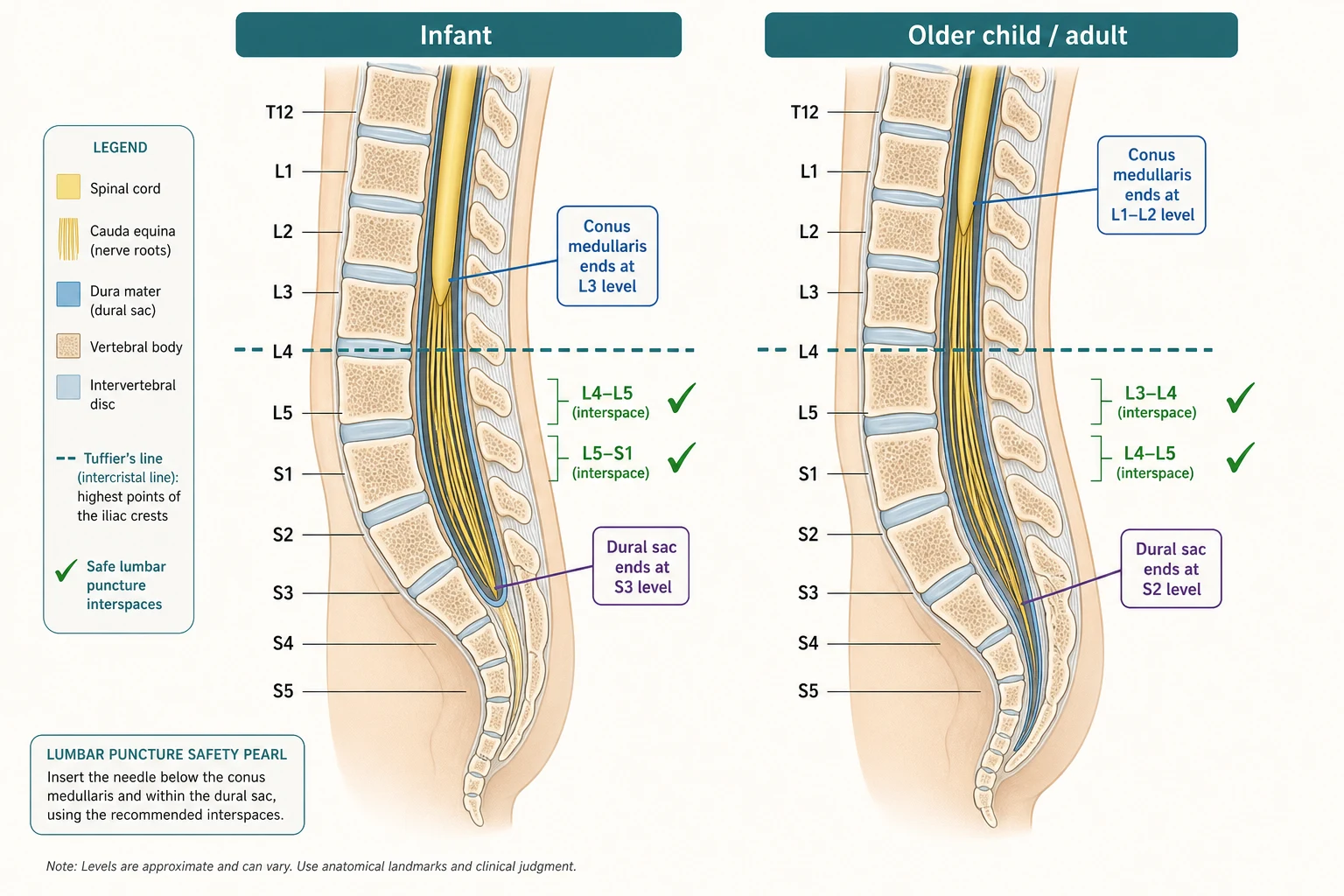
The single most testable anatomical fact is that the infant spinal cord ends lower than the adult's. At birth the conus medullaris sits at the L3 vertebral level; it ascends as the vertebral column grows faster than the cord, reaching its adult position at L1-L2 by adolescence. The dural sac ends correspondingly lower in the infant — at S3 or S4 — and at S2 in the adult. The practical consequence is that in the very young infant a needle placed at L3-L4 can still injure the cord, so the safe interspace is L4-L5 or L5-S1 in the infant and L3-L4 or L4-L5 in the older child and adult. The intercristal (Tuffier's) line drawn between the highest points of the iliac crests crosses the L4 spinous process or the L4-L5 interspace and is the external landmark that anchors the procedure. [1] [9]
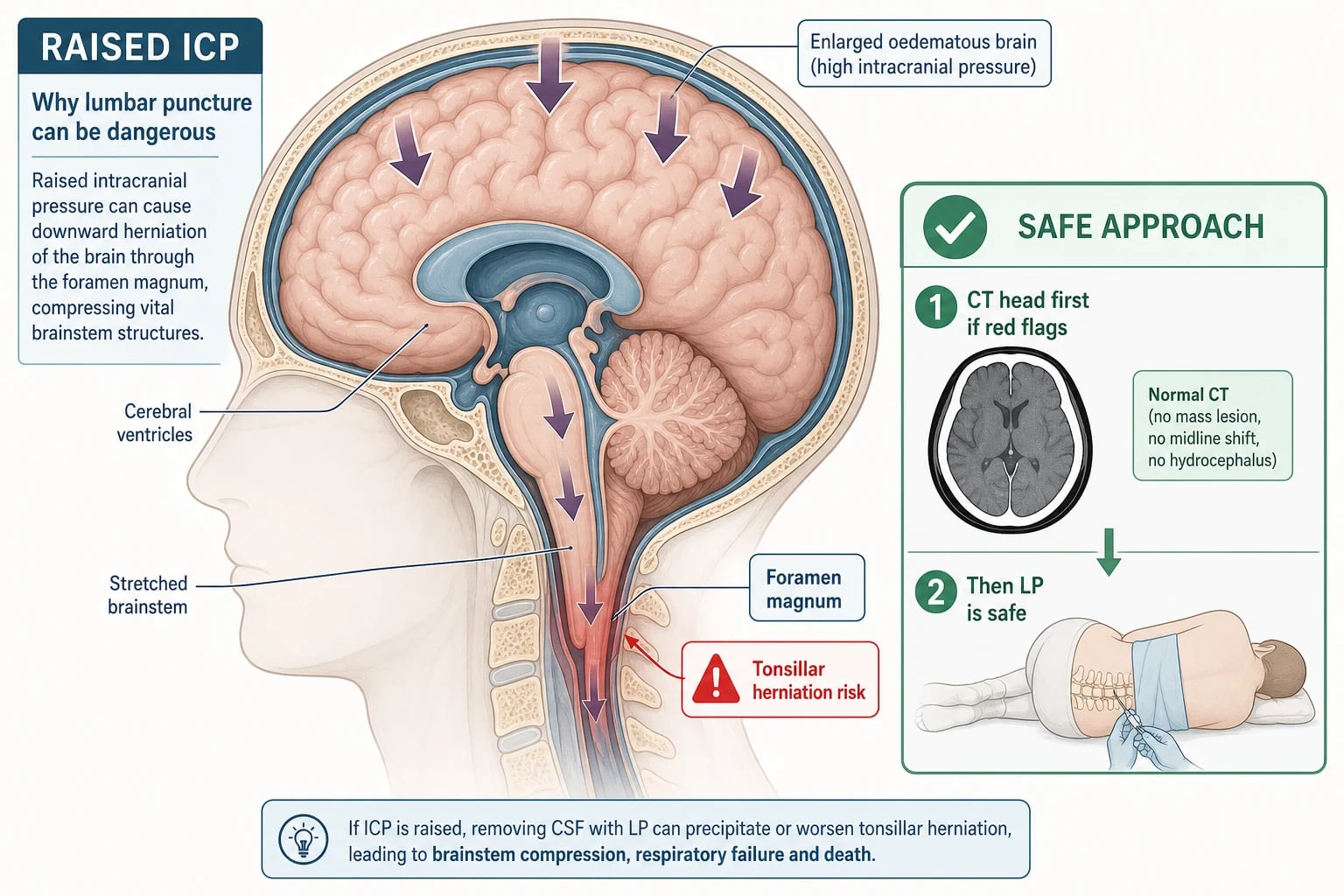
The mechanism of cerebral herniation after LP is a pressure gradient. In a child with raised intracranial pressure from a posterior fossa tumour, an obstructive hydrocephalus, or a large hemispheric lesion, the intracranial contents are under tension and partially wedged at the foramen magnum or the tentorial hiatus. When CSF is drained from the lumbar theca the pressure below the block falls, the gradient steepens, and the cerebellar tonsils or the medial temporal lobe are driven through the foramen magnum or the tentorial notch. The avoidance strategy is a CT head before LP whenever there is a red flag — focal neurology, papilloedema, a decreased conscious state, a prolonged postictal state, immunocompromise, or known CNS disease or a shunt — so that a space-occupying lesion or hydrocephalus is excluded first. [9] [10]
The mechanism of post-dural puncture headache is persistent CSF leak through the dural perforation, which lowers CSF pressure and tugs on pain-sensitive meninges and vessels when the child stands; the headache is characteristically postural, worse on sitting or standing and relieved by lying flat. A cutting Quincke needle slices longitudinal dural fibres apart and leaves a slit that gapes; an atraumatic pencil-point needle parts and spreads the fibres, and the elastic recoil closes the hole. This anatomical difference is why the atraumatic needle reduces post-dural puncture headache without compromising CSF yield, and is the modern default. [2] [4]
Clinical Presentation
The clinical scenarios that prompt LP are few and well defined, and the first task at the bedside is to decide which of them you are dealing with, because the urgency, the consent and the timing differ. [1] [10]
The commonest diagnostic scenario is suspected meningitis or encephalitis — the febrile child with irritability, neck stiffness, photophobia, altered conscious state, a non-blanching rash, or a seizure with fever — in whom CSF analysis is needed to confirm the diagnosis, to identify the organism, and to direct antimicrobial therapy. The second is the febrile infant in the septic workup, especially the neonate under 28 days and the young infant under three months, in whom LP is part of a complete septic screen because clinical examination alone cannot exclude meningitis. The third is the unexplained altered conscious state or unexplained seizure, in whom LP is performed once the brain has been imaged. The fourth is suspected idiopathic intracranial hypertension, where the opening pressure is itself the diagnostic anchor. The fifth is the oncology setting, where LP is performed under anaesthesia for leukaemia staging and intrathecal chemotherapy. [1] [11]
The urgency is graded by the clinical state. The septic-shocked or comatose child is the one in whom antibiotics and resuscitation come first and LP is deferred until the child is stable — CSF cell counts and biochemistry remain useful for 24 to 48 hours after a dose of antibiotics, and the polymerase chain reaction for bacteria and viruses is barely affected, so a deferred LP is still informative. The well-looking febrile infant can have an LP as part of a calm, planned septic workup. The cooperative older child can have an elective diagnostic LP with topical analgesia and explanation. [10] [11]
The presenting features that should prompt CT before LP rather than LP straight away are focal neurology, papilloedema where the fundus can be examined, a decreased or fluctuating conscious state, a prolonged postictal state, new-onset seizure with fever and slow recovery, immunocompromise, a known CNS lesion or a ventriculoperitoneal shunt, and any sign of raised intracranial pressure such as a bulging fontanelle, bradycardia with hypertension, or irregular respirations. [9] [10]
| Scenario | Urgency | What it dictates |
|---|---|---|
| Suspected bacterial meningitis, unwell | Antibiotics first, LP when safe | IV cefotaxime or ceftriaxone after blood culture; dexamethasone with or before the first dose in suspected pneumococcal disease; LP after stabilisation |
| Well-looking febrile infant under 3 months | Prompt LP as part of septic screen | Calm planned LP; defer and treat if the infant is unstable or LP cannot be performed promptly |
| Suspected viral meningitis, cooperative older child | Prompt LP | Topical anaesthesia, atraumatic needle, opening pressure in lateral decubitus |
| Suspected idiopathic intracranial hypertension | Elective LP after imaging and fundoscopy | Opening pressure is the diagnostic anchor; imaging first to exclude a venous sinus thrombosis or mass |
| Leukaemia staging or intrathecal chemotherapy | Elective LP under anaesthesia | Platelet support to above 50 × 10⁹/L; atraumatic needle; oncology protocol |
The trap is the child who is stable enough for LP at first glance but has an unrecognised red flag — a subtle focal sign, an early papilloedema, or a thrombocytopenia not yet resulted. The discipline is a structured pre-LP check that explicitly asks about raised pressure, neurology, coagulation and skin before the drape goes on. [9] [8]
Differential Diagnosis
The differential at the bedside is not "what is causing the headache" — it is whether LP is the right next step at all, in what order, and in whom. Frame the decision around four questions and the right answer follows. [1] [10]
LP now
default
- No red flags: normal conscious state, no focal neurology, no papilloedema
- Platelets and coagulation normal where relevant, no overlying skin infection
- Stable child; well-looking febrile infant or cooperative older child
- Diagnostic CSF and reliable opening pressure in lateral decubitus
LP after CT
- Any red flag: focal neurology, papilloedema, decreased or fluctuating GCS
- Prolonged postictal, new-onset seizure with slow recovery, immunocompromise
- Known CNS disease or a ventriculoperitoneal shunt
- CT excludes a mass, hydrocephalus or shift before LP is performed
LP deferred, antibiotics first
- Septic-shocked, comatose, or rapidly deteriorating child
- Antibiotics after blood culture; LP later when stable
- CSF cell count and biochemistry remain useful for 24–48 h
- PCR for bacteria and viruses is barely affected by prior antibiotics
LP not indicated
- Coagulopathy or thrombocytopenia not correctable
- Overlying skin infection until resolved or alternative interspace chosen
- Diagnosis made by another means, e.g. PCR on blood
- Risks outweigh the diagnostic yield
A second layer of differential is what the CSF result will mean once you have it. A high polymorph count with low glucose and high protein points to bacterial meningitis; a lymphocytic pleocytosis with normal or near-normal glucose points to viral meningitis or encephalitis; a very low glucose with a persistent lymphocytosis suggests tuberculous or fungal meningitis; a near-normal CSF after antibiotics is a "partially treated" picture that still requires clinical judgement; and a uniformly blood-stained CSF that does not clear through the four tubes is a traumatic tap or, much less commonly, a subarachnoid haemorrhage. [1] [9]
The traumatic tap deserves a specific question because it is common and often mismanaged. When the needle grazes a venous plexus on the way in, blood contaminates the CSF; the blood usually clears between the first and fourth collection tubes, which is itself the diagnostic clue. A reasonable correction is to subtract one white cell for every 500 to 700 red cells in the sample, comparing the ratio with the child's peripheral blood. A traumatic tap does not invalidate a low glucose, a high protein, or a positive Gram stain or culture — those findings stand on their own. [1] [9]
Clinical & Bedside Assessment
Assessment before LP is short, structured and explicit: it asks four questions, names the answer to each, and either proceeds, images, defers, or stops. The aim is never to be surprised once the drape is on. [1] [9]
Begin with a focused neurological examination: conscious level using a paediatric GCS, pupillary responses and symmetry, eye movements, limb power and tone, and any focal sign. Examine the fundus where the child will tolerate it, looking for papilloedema — difficult in the young infant, in whom a bulging or full fontanelle and the overall clinical picture are the practical substitutes. Look at the skin over the puncture site for cellulitis, a pilonidal anomaly, or a spinal dysraphism. Palpate the abdomen for organomegaly that might hint at an underlying malignancy. Confirm the observations: a child with shock, bradycardia with hypertension (Cushing's triad), or irregular respirations is not stable for an elective LP. [9] [10]
Check the laboratory results that are relevant to the child in front of you. A platelet count is needed if there is any suspicion of thrombocytopenia; an INR if there is liver disease, a bleeding history, or anticoagulant use. The procedural tradition is that LP is safe at a platelet count above 50 × 10⁹ per litre and an INR below 1.5, with a normal activated partial thromboplastin time. These are pragmatic thresholds rather than evidence from large trials, but they are the working rule. In the oncology setting the local protocol usually specifies a higher platelet target for intrathecal chemotherapy. [8] [9]
Assess the child's likely tolerance of the procedure and plan the analgesia accordingly. A neonate will need oral sucrose, a dummy, and containment; an infant and young child will need topical anaesthesia and often a parent holding them or sitting in next; a cooperative older child may manage with topical and subcutaneous lidocaine; an anxious or uncooperative child needs procedural sedation by a trained team with full monitoring. [12] [1]
The pre-LP checklist
Conscious state normal? Any focal neurology? Any papilloedema or bulging fontanelle? → if yes, CT head first
Stable observations? No shock, no Cushing's triad? → if no, resuscitate and antibiotics first, LP deferred
Platelets above 50 × 10⁹/L and INR under 1.5 where relevant? No overlying skin infection? → if no, correct or defer
Consent obtained and documented? Analgesia and sedation planned? → proceed when both are yes
Position chosen for the child and the indication: lateral decubitus if an opening pressure is needed
Atraumatic needle selected; stylet in; correct interspace palpated using Tuffier's line
Investigations
The CSF analysis is the laboratory extension of the procedure, and the candidate must know the normal values, the common abnormal patterns, and the corrections. The minimum analysis on a diagnostic LP is cell count and differential on the first and last tubes, protein and glucose (with a paired plasma glucose taken at the same time), Gram stain, and culture. In the relevant child, add a bacterial and viral multiplex polymerase chain reaction, a viral culture, acid-fast bacilli and tuberculosis studies, an Indian ink and cryptococcal antigen in the immunocompromised, and cytology where malignancy is suspected. [1] [9]
| Variable | Older child | Neonate / young infant |
|---|---|---|
| White blood cells | Less than 5 × 10⁶/L, predominantly lymphocytes | Up to 20–30 × 10⁶/L accepted in the neonate, more polymorphs tolerated |
| Red blood cells | Essentially zero (a few in a traumatic tap) | Variable; may be modestly raised without disease |
| Protein | 0.15 to 0.45 g/L | Higher in the neonate, up to about 1.0 g/L term and 1.5 g/L preterm accepted |
| Glucose (CSF) | Above 60% of a paired serum glucose, typically over 2.5 mmol/L | Same ratio; neonatal values follow the serum closely |
| Opening pressure (lateral decubitus, relaxed) | 10–20 cmH₂O | Lower in neonates, typically under 10 cmH₂O; reading easily falsely raised by crying |
The interpretation turns on a few named patterns. Bacterial meningitis typically shows a polymorphonuclear pleocytosis in the hundreds to thousands, a CSF glucose below 40% of the serum value or under 2.5 mmol/L, a protein over 1.0 g/L, and a Gram stain positive in the majority before antibiotics. Viral meningitis shows a lymphocytic pleocytosis, often modest, with a normal or near-normal glucose and mildly raised protein. Tuberculous meningitis shows a persistent lymphocytosis, a very low glucose, and a markedly raised protein, with a cobweb clot on standing. A traumatic tap is recognised by blood that clears between the first and fourth tubes; the corrected white-cell count uses the 1-to-500-to-700 rule, and a traumatic tap does not invalidate the glucose, protein, Gram stain or culture. [1] [9]
The opening pressure is the part of the CSF examination that examiners most often misuse. The reading is reliable only when the child is calm, in the lateral decubitus position, with the legs extended and relaxed at the moment the manometer is read. The normal range in a relaxed child over two years is 10 to 20 cm of water; values above 20 cm of water in a relaxed child, or above 25 cm of water, suggest raised intracranial pressure, but a single elevated reading in a crying or poorly positioned child is meaningless and must be repeated or set aside. In suspected idiopathic intracranial hypertension, an opening pressure above 25 cm of water in a relaxed child (above 28 cm of water in some criteria), with normal neuroimaging and normal CSF composition, is the diagnostic anchor. [6] [7]
Management — Resuscitation
When suspected bacterial meningitis coexists with shock or coma, the LP is not the priority — resuscitation and empirical antibiotics are. The ordered bundle is airway, breathing, circulatory access and a blood culture, followed by empirical intravenous antibiotics and, in suspected pneumococcal disease, dexamethasone, and the LP is performed when it is safe. [10] [11]
The single most important rule in suspected bacterial meningitis is that empirical intravenous antibiotics must never be delayed by the LP. If the LP cannot be performed promptly — within about an hour of presentation — give the antibiotics first, after a blood culture, and perform the LP when the child is stable. CSF cell counts, glucose, protein and Gram stain remain informative for 24 to 48 hours after a dose of antibiotic; bacterial culture is the test most affected, but bacterial and viral PCR are barely altered, so a deferred LP is still diagnostically useful. The fear that "antibiotics will make the LP useless" is a mistaken reason to delay treatment. [10] [1]
The role of dexamethasone in suspected bacterial meningitis is to reduce the inflammatory response to bacterial cell-wall products released by antibiotics, particularly in pneumococcal meningitis, in which it reduces hearing loss and other neurological sequelae. The evidence-based timing is that dexamethasone should be given with or just before the first antibiotic dose; giving it after the first dose is much less effective. In Haemophilus influenzae type b meningitis the benefit on hearing is also established; in meningococcal disease the evidence is weaker and the practice varies. [10]
Cefotaxime or ceftriaxone (empirical, suspected bacterial meningitis, ANZ / NICE)
If the child deteriorates during or immediately after the LP — a falling conscious state, a dilating pupil, an irregular respiratory pattern, or a bradycardia with hypertension — abandon the procedure, call for senior help, prepare for imaging and for the management of raised intracranial pressure (head-up positioning, controlled normocapnia, hypertonic saline or mannitol where indicated), and treat suspected herniation as an emergency. [9] [10]
Management — Definitive & Stepwise
Once the indications and contraindications have been settled, the procedure itself is an ordered sequence that should run the same way every time: consent, preparation, anaesthesia, positioning, sterile field, landmark identification, needle insertion, CSF collection and opening pressure, withdrawal with the stylet replaced, a dressing, and the labelling and transport of the samples. [1] [9]
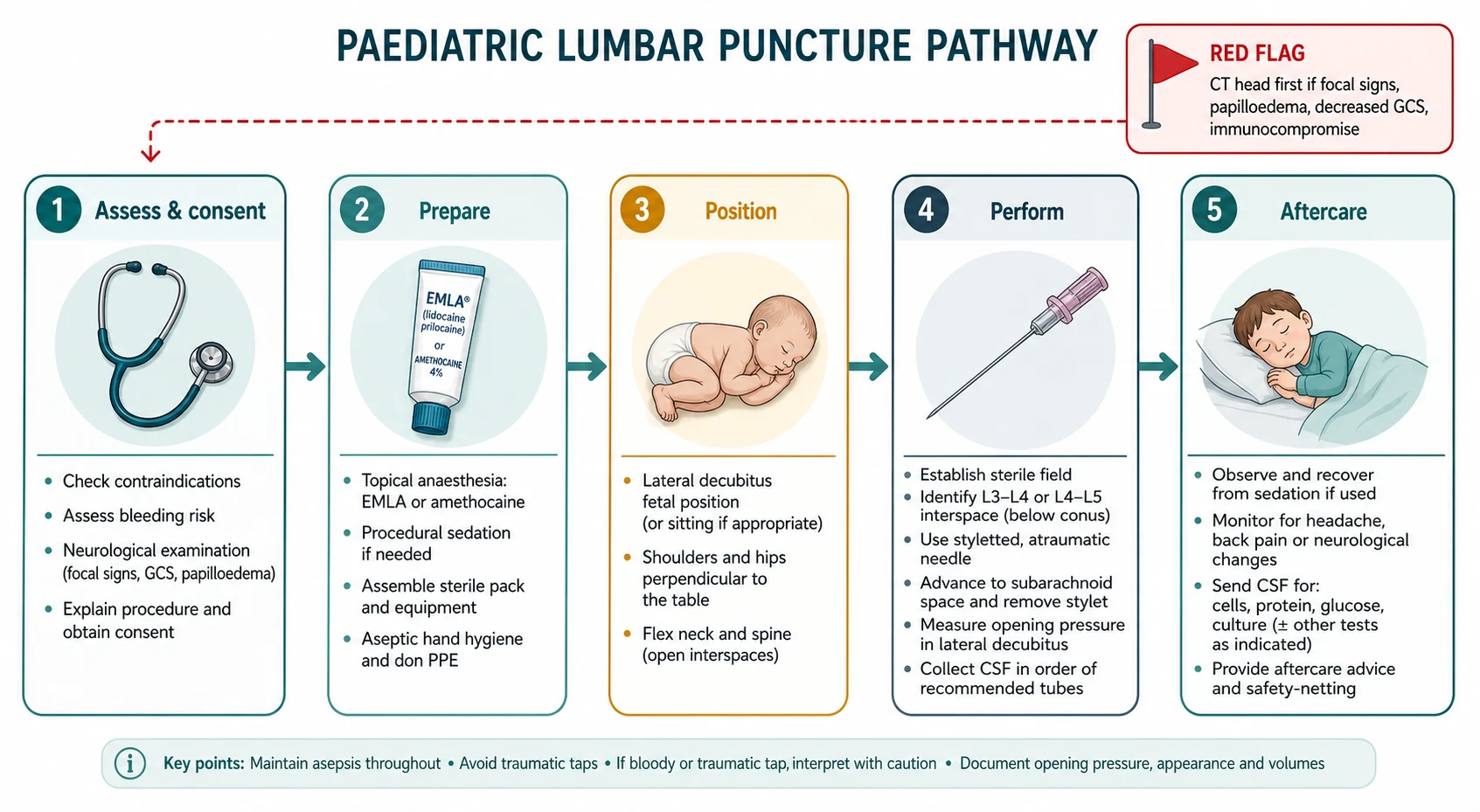
Begin with consent: explain to the parent and, where appropriate, the child, why the LP is needed, what it will feel like, the common discomforts (local pain, post-dural puncture headache), the serious but rare risks (bleeding, infection, neurological injury), and the alternatives. Document the consent. Apply the topical anaesthetic at the planned puncture site early — EMLA (eutectic lidocaine 2.5% and prilocaine 2.5%) under an occlusive dressing for at least 60 minutes, or amethocaine 4% (Ametop) for 30 to 45 minutes. Plan the procedural sedation if needed (nitrous 50/50 by trained staff, or ketamine by the local protocol) with full monitoring. [12] [1]
Position the child with care, because position determines success and the reliability of the opening pressure. The lateral decubitus position is the default whenever an opening pressure is needed: the child lies on their side curled into a fetal position, with hips and knees flexed and the neck slightly flexed in the older child — but avoiding over-flexion of the neck in the infant, who can obstruct their airway. The shoulders and hips must be perpendicular to the bed (not rolled forward or back), because rotation narrows the interspinous space and is a common cause of a failed LP. The sitting position is an alternative in the cooperative older child or in the obese infant in whom the lateral landmarks are hard to feel, and some operators find it easier, but the opening pressure cannot be reliably measured in the sitting position — if a pressure is needed, use lateral. [1] [9]
SLIPPED
Under sterile conditions, palpate the Tuffier's line between the iliac crests and identify the chosen interspace. Infiltrate the skin and subcutaneous tissues with 1% lidocaine up to a maximum of 3 mg/kg (4.5 mg/kg with adrenaline) if the topical alone is insufficient, using a small needle and injecting as you withdraw. Insert the styletted atraumatic spinal needle in the midline, angled slightly toward the umbilicus, and advance slowly. The classic feel is a distinct give as the needle passes through the ligamentum flavum and then the dura-arachnoid; remove the stylet to check for CSF flow. If using a cutting Quincke needle, orient the bevel parallel to the longitudinal dural fibres so that the bevel spreads rather than cuts the fibres. [1] [2]
Once CSF flows, attach the manometer and measure the opening pressure with the child calm and the legs extended. Collect four numbered tubes of CSF in the order cell count and differential, protein and glucose, Gram stain and culture, and any additional tests. Replace the stylet before withdrawing the needle to avoid arachnoid strand traction and a nerve root injury. Apply a small dressing. Label the tubes at the bedside and send them to the laboratory promptly. [9] [6]
Handle the dry tap, the traumatic tap, and the uncooperative child deliberately. A dry tap is most often a positional problem — re-palpate the landmarks, withdraw the needle into the subcutaneous tissue without exiting the skin, and re-advance in the midline; two or three passes in a cooperative child under good conditions is acceptable, but multiple passes in a struggling child warrant stopping and trying again later under sedation or with ultrasound guidance. A traumatic tap in which the CSF does not clear, or in which the child develops severe back or radicular pain, warrants stopping. Ultrasound before LP is increasingly used to map the interspinous space, the conus, and the optimal puncture site in the difficult child, and is the modern answer to the previously blind attempt. [1] [9]
Specific Subtypes & Scenarios
The approach to LP changes with the child and the clinical question, and the fellowship candidate must adjust the technique and the timing to the subtype in front of them. [1] [11]
In the neonate and young infant, LP is most often part of the septic workup of a febrile or unwell baby. The anatomy is smaller, the conus lower, the needle finer (typically a 22-gauge or a 25-gauge paediatric needle), and the position is the lateral decubitus with the head supported to avoid airway obstruction from over-flexion. The neonatal CSF accepts more white cells and more protein as normal, so the thresholds for abnormality are higher than in the older child. The opening pressure is technically possible but rarely reliable in a crying neonate, and is usually omitted. The JAMA 2026 prediction rule refined the risk stratification of febrile neonates under 28 days, but the safe default in the unwell neonate remains a full septic workup including LP and empirical antibiotics. [11] [12]
In the cooperative older child, the procedure is closer to an adult LP: the landmarks are easier, a 22-gauge atraumatic needle is appropriate, the lateral decubitus position allows an opening pressure, and topical anaesthesia with subcutaneous lidocaine is usually adequate. The focus is on genuine analgesia, an honest explanation appropriate to age, and a single atraumatic pass. [1] [2]
In suspected idiopathic intracranial hypertension, the opening pressure is the diagnostic anchor. The workup is neuroimaging first (to exclude a venous sinus thrombosis, a mass, or hydrocephalus), followed by an LP in the lateral decubitus position with the child calm and relaxed; an opening pressure above 25 cm of water (above 28 cm of water in some criteria) with normal CSF composition and normal imaging supports the diagnosis, and a therapeutic removal of CSF may both confirm the syndrome by relieving the headache and provide the first treatment. [6] [7]
In the immunocompromised or oncology child, LP is often performed under general anaesthesia for intrathecal chemotherapy or for staging, with platelet support to above 50 × 10⁹ per litre (or higher per the local oncology protocol), an atraumatic needle, and a strict "time-out" before any intrathecal drug is given to prevent a catastrophic wrong-route error. The immunocompromised child undergoing a diagnostic LP also needs an expanded CSF panel that includes cryptococcal antigen, an India-ink preparation, and mycological studies. [9] [8]
In the febrile neonate under 28 days, the modern risk-stratified approach (JAMA 2026) helps separate the very low-risk neonate from the rest, but the safe default in the unwell or borderline neonate remains a full septic workup including LP, and empirical antibiotics until the CSF and cultures are clear. [11]
In the remote or retrieval setting, where CT and skilled procedural sedation may be hours away, the priorities are empirical antibiotics after a blood culture, fluid resuscitation, and a calm LP if it can be performed safely; if not, the LP is deferred to the receiving unit, where it is performed once the child is stable. [10] [11]
Complications & Pitfalls
The complications of paediatric LP run from the common and self-limiting to the rare and catastrophic, and the discipline is to anticipate the serious ones and prevent them through the pre-LP check, while managing the common ones with honesty and evidence. [1] [9]
The common complications are local back pain at the puncture site, transient radicular pain during the procedure if a nerve root is brushed, and post-dural puncture headache (PDPH). PDPH is characteristically postural — worse on sitting or standing, relieved by lying flat — and usually begins within 24 to 72 hours of the LP. It is less common in children under five than in adolescents and adults. First-line management is rest, oral hydration or an intravenous fluid if nausea limits intake, and simple analgesia; caffeine has limited evidence in children. Most cases resolve within a few days. A severe or persistent PDPH that does not respond to conservative measures over several days, or that is disabling, warrants discussion with anaesthetics for an epidural blood patch, in which a small volume of the patient's own venous blood is injected into the epidural space to seal the dural perforation. [4] [5]
The serious complications are rare but worth knowing exactly. A spinal epidural haematoma can form if the needle injures an epidural vein in a coagulopathic child, presenting with severe back pain, progressive leg weakness, sensory loss, and sphincter disturbance; it is a surgical emergency and the threshold to image the spine urgently is low. A spinal epidural abscess is the rarest infectious complication, presenting days to weeks later with back pain, fever, and neurological deficit. Iatrogenic meningitis is the introduction of skin flora into the CSF through poor asepsis, an overlying skin infection, or a needle reused or contaminated; the protection is sterile technique, mask and gloves, and avoiding the infected skin. Cerebral herniation after LP in raised intracranial pressure is the catastrophic complication that the CT-first rule is designed to prevent. A persistent CSF fistula with chronic headache or a CSF leak is rare and may need neurosurgical repair. [8] [9]
A frequently tested misconception is that bed rest after LP reduces post-dural puncture headache. The systematic review evidence shows that routine bed rest, with or without a particular head position, does not reduce the rate or severity of PDPH, so a child who feels well may mobilise; the practical advice is to lie flat if a headache develops. [4] [2]
Prognosis & Disposition
The prognosis after an uncomplicated LP is excellent: the puncture site heals within days, and most children return to normal activity the same or the next day. The disposition is driven far more by the underlying diagnosis than by the procedure itself. [1] [9]
For an elective diagnostic LP in a well child — the suspected viral meningitis with a normal opening pressure, the resolved febrile seizure — the child can be observed for a short period after the procedure and discharged with advice to lie flat if a headache develops, to maintain fluids, and to return if there is severe headache, back pain, fever, weakness, numbness, or new symptoms. The CSF results should be chased and the family communicated with as soon as they are available. [1]
For post-dural puncture headache, the natural history is resolution within a few days in most children; a severe or persistent case that has not responded to conservative measures warrants referral for an epidural blood patch, which is highly effective. [4] [5]
For the child in whom bacterial meningitis is confirmed, the disposition is paediatric inpatient or intensive care for the duration of antibiotic therapy, with hearing assessment at recovery and follow-up for neurological sequelae; the LP is the diagnostic confirmation of a treatment that is already underway. [10]
For the serious procedural complications — epidural haematoma, epidural abscess, herniation, persistent CSF leak — the prognosis depends on the speed of recognition and definitive management, and the disposition is urgent imaging, neurosurgical and infectious-disease consultation, and a low threshold for transfer to a tertiary centre. [8] [9]
Special Populations
The approach to LP is adjusted for the child in front of you, and the fellowship candidate must show that they can match the technique and the timing to the population. [1] [11]
In the neonate and young infant, LP is technically harder, the cord ends lower, the needle is finer, the normal values are different, and the opening pressure is rarely reliable. The procedure is most often part of the septic workup, and the safe default is empirical antibiotics and a full septic screen in any unwell neonate. [11] [12]
In the immunocompromised child, including the oncology patient and the transplant recipient, the platelet threshold and the strict aseptic technique matter more, the CSF panel is expanded, and any fever or neurological symptom lowers the threshold for LP once imaging has cleared the brain. [9] [8]
In the child on anticoagulants or with a bleeding disorder, the procedure is coordinated with the haematology team: the anticoagulant is held for the appropriate interval, the INR and platelet count are checked and corrected into the safe range before the LP, and the anticoagulant is restarted after an interval that balances procedural bleeding against thrombosis. [8] [9]
In the child with a ventriculoperitoneal shunt, the LP is rarely the right first step in suspected shunt infection or obstruction; a shunt tap by the neurosurgical team is usually preferred, and the LP is reserved for specific indications after neurosurgical discussion. [9]
In the Indigenous, remote, or under-resourced setting, the indications are the same but access to CT, to atraumatic needles, and to skilled procedural sedation may not be. The equity intervention is to triage the well-looking child, to defer LP and treat empirically where imaging and stabilisation are distant, and to arrange retrieval. [10] [11]
In the technology-dependent or neurodivergent child, the procedure is planned with extra time, a communication strategy appropriate to the child, an assent process where possible, and a sedation plan that the child and family can support. [12]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric LP has matured in three areas: the choice of needle, the analgesia of the newborn, and the risk stratification of the febrile infant. The candidate should know each one and the regional deltas that follow from them. [1] [10]
The atraumatic-needle evidence is the strongest single change in modern practice. A systematic review and meta-analysis across children and adults showed that atraumatic pencil-point needles (Sprotte, Whitacre) reduce post-dural puncture headache compared with cutting Quincke needles without reducing the rate of successful LP, and that smaller gauges further reduce the headache rate. The teaching is now that atraumatic needles should be the default wherever they are available, and the historical preference for cutting needles is no longer evidence-based. [2] [3]
The Cochrane review on pharmacological interventions for LP in newborns (2023) concluded that breast milk or sucrose, topical anaesthesia, and where appropriate a small dose of an opioid all reduce procedural pain, and that combining non-pharmacological with pharmacological measures works better than either alone. The clear teaching is that an untreated neonatal LP is ethically and evidence-wise indefensible. [12]
The JAMA 2026 prediction rule for febrile neonates refined the stratification of bacteremia and bacterial meningitis in infants aged 28 days or younger, offering a structured tool to identify the very low-risk neonate in whom LP might be deferred. The rule complements but does not replace clinical judgement: in the unwell or borderline neonate, a full septic workup including LP and empirical antibiotics remains the safe default. [11]
Atraumatic vs cutting lumbar puncture needles (systematic review, Arch Dis Child Educ Pract Ed 2019)
PMID 30368456
Population: Children and adults undergoing diagnostic LP
Comparator: Conventional cutting (Quincke) spinal needle
Key finding
Atraumatic needles reduced post-dural puncture headache without reducing successful CSF collection. Smaller gauge further reduced headache. Recommendation: atraumatic needles should be the default.
Where the evidence is weak or contested: the routine use of ultrasound before LP, the threshold and indications for an epidural blood patch in young children, the exact platelet threshold for a safe LP (a pragmatic 50 × 10⁹ per litre rather than a trial-derived value), the value of routine bed rest after LP, and the optimal empirical antibiotic for the neonate under 28 days. Each is a defensible topic for the viva. [9] [4]
Exam Pearls
The fellowship examiner expects a candidate who knows the anatomy, the contraindications, the values, and the analgesia, and can defend the procedure at the bedside. [1] [9]
The single most testable anatomical fact is that the infant spinal cord ends at L3 and the adult cord at L1-L2, and the safe interspace is L4-L5 or L5-S1 in the infant and L3-L4 or L4-L5 in the older child. The dural sac ends correspondingly lower (S3 in the infant, S2 in the adult), and the intercristal (Tuffier's) line crosses the L4 spinous process or the L4-L5 interspace and is the external landmark. [1]
The named absolute contraindications are raised intracranial pressure without imaging, focal neurology, papilloedema or a decreased conscious state without a CT, uncorrected coagulopathy, an overlying skin infection, and an unstable child. The CT-first criteria are focal neurology, papilloedema, a decreased or fluctuating conscious state, a prolonged postictal state, immunocompromise, and a known CNS lesion or shunt. [9] [10]
The opening pressure is reliable only in the lateral decubitus position with the child calm and the legs relaxed, and the normal range is 10 to 20 cm of water in the relaxed child over two years (lower in the neonate). A reading from a sitting, crying, or straining child must not be used. The diagnostic anchor for idiopathic intracranial hypertension is an opening pressure above 25 cm of water (above 28 cm of water in some criteria) with normal imaging and CSF composition. [6] [7]
The classic distractors the exam rewards for naming: performing LP in the sitting position and quoting an opening pressure; relying on a single opening-pressure reading in a crying child; using a cutting Quincke needle where an atraumatic needle is available; performing LP through infected skin; performing LP without correcting coagulopathy; delaying antibiotics in suspected meningitis to obtain the LP; and prescribing routine bed rest after LP to prevent PDPH. Each is wrong for a specific evidence-based reason. [2] [4]
References
- [1]Cunningham S, Munro V, Harrower N How to use… lumbar puncture in children Arch Dis Child Educ Pract Ed, 2015.PMID 26104280
- [2]Haroon F, Munir K, Karunaratne TB Atraumatic lumbar puncture needles are associated with fewer complications than conventional needles Arch Dis Child Educ Pract Ed, 2019.PMID 30368456
- [3]Alcock A, Salter R Towards evidence-based emergency medicine: best BETs from the Manchester Royal Infirmary. BET 2: what gauge and type of lumbar puncture needle should we be using in the paediatric population to reduce the risk of postdural puncture headaches? Emerg Med J, 2013.PMID 23275464
- [4]Khleifat KM, Khasawneh AH, Alqdah MD, et al Factors Predisposing to Post Dural Puncture Headache in Children J Child Neurol, 2021.PMID 33882752
- [5]Benzel EC, Connolly MW Post-dural puncture headaches in children. A literature review Eur J Pediatr, 2003.PMID 12655411
- [6]Vinci M, Pirritano M, Veca A, et al Lumbar puncture opening pressure is not a reliable measure of intracranial pressure in children J Child Neurol, 2015.PMID 24799366
- [7]Kuo HC, Lin YJ, Chang CF, et al Opening Pressure and Post-Lumbar Puncture Headache in Children Undergoing Intrathecal Baclofen Trial J Child Neurol, 2024.PMID 38419482
- [8]Koch BL, Moosbrugger EA, Egelhoff JC Symptomatic spinal epidural collections after lumbar puncture in children. AJNR Am J Neuroradiol, 2007.PMID 17885251
- [9]Doherty CM, Forbes RB Diagnostic lumbar puncture: minimizing complications Intern Med J, 2008.PMID 18422562
- [10]Pelton SI, Harper MB, Bonsu BK, et al Management of bacterial meningitis and meningococcal septicaemia in children and young people: summary of NICE guidance BMJ, 2010.PMID 20584794
- [11]DeAngelis C, Lavelle A, Lopez MA, et al Prediction of Bacteremia and Bacterial Meningitis Among Febrile Infants Aged 28 Days or Younger JAMA, 2026.PMID 41359314
- [12]Urits I, Jones MR, Viswanath O, et al, on behalf of the Cochrane Pain, Palliative and Supportive Care Group Pharmacological interventions for the management of pain and discomfort during lumbar puncture in newborn infants Cochrane Database Syst Rev, 2023.PMID 37767875