Paeds · investigations-procedures-and-technology
Medical devices, digital health and remote monitoring
Also known as Paediatric medical devices and wearables · Continuous glucose monitoring and hybrid closed-loop systems in children · Home pulse oximetry and remote patient monitoring in infants and children · Telehealth and mHealth in paediatric chronic disease
A fellowship approach to selecting, deploying and remotely interpreting paediatric medical devices, wearables and digital-health tools. Sort devices into four classes — implantable or long-term, wearable or on-body, home monitoring and telehealth platforms — and distinguish a regulated medical-grade device from a consumer wellness product. Hold the two highest-yield sensor physiologies in working memory: the continuous glucose monitor (interstitial glucose with a five-to-fifteen-minute plasma lag) and the pulse oximeter (light absorption biased by dark skin pigmentation and poor perfusion). Run the ambulatory glucose profile targets from ISPAD 2024, recognise the equity and accuracy failures of pulse oximetry, and deploy a device only after the clinical question, the age validation, the thresholds and the escalation pathway are agreed with the family.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A family walks into clinic with a parent's smartwatch that has flagged an irregular rhythm on their eight-year-old, a continuous glucose monitor (CGM) reading for a four-year-old with type 1 diabetes, and a finger pulse oximeter they bought to monitor their baby's bronchiolitis at home. Each is a digital-health device, each generates a number, and each can either help or harm the child depending on whether the team can read it correctly. The candidate who treats every device reading as a fact will be caught; the candidate who knows the sensor physiology, the regulatory status and the equity pitfalls will counsel the family safely. This page teaches the four device classes, the two sensor physiologies that examiners reward, the ambulatory glucose profile (AGP) targets, the equity failures of pulse oximetry, and the shared-decision framework that turns a device into a clinical tool. [8] [9]
S.E.N.S.O.R. — what makes a paediatric device trustworthy
Overview & Definition
A medical device is any instrument, apparatus, implement, machine, implant, in-vitro reagent or related article — including the software that drives it — intended by the manufacturer to diagnose, prevent, monitor, treat or alleviate disease. In paediatrics the definition is sharpened by two features: the device must work across a wide range of body sizes, from the premature neonate to the young adult, and it must be tolerable to a developing child whose cooperation, skin, perfusion and cognition change with age. A pulse oximeter probe that fits an adult finger is not a paediatric device; a CGM adhesive that tolerates a toddler's skin is not the same as one designed for an adult arm. [8] [11]
Digital health is the umbrella term that covers the device, the data pipeline that carries its signal, the algorithm that interprets it and the platform that delivers the result to the family or clinician. Within digital health the candidate must distinguish three working concepts that examiners separate deliberately. Telehealth is the synchronous or asynchronous delivery of clinical care at a distance — most often a video consultation. Remote patient monitoring is the continuous or intermittent transmission of physiological data from a device in the home to a clinician who reviews it. A self-management app is a one-way behaviour-change tool that does not, by itself, send data to a clinician. The candidate who conflates the three loses the marks. [8] [9]
The defining principle of paediatric device use is that the device extends but never replaces the clinical assessment. A CGM extends the capillary glucose, a pulse oximeter extends the clinical observation of cyanosis, and a telehealth consult extends the bedside examination, but each can be wrong, biased or silent. The second principle is that the family — usually a parent, sometimes a young person — is the primary operator, and the device must be deployed with an education, a threshold set and a safety-net that the family can execute at three o'clock in the morning. The third principle is equity: a device that widens the gap between the family who has broadband and the family who does not has failed the child even if its signal is perfect. [7] [8]
Classification
Sort devices by where they sit on or in the child and by what they do, because the response to a device question is driven by both. The four classes below carry the canonical examples that examiners expect; the bottom bar of the figure separates the regulated medical-grade device from the consumer wellness product, the distinction that decides whether the family's number is a fact or a curiosity. [8]
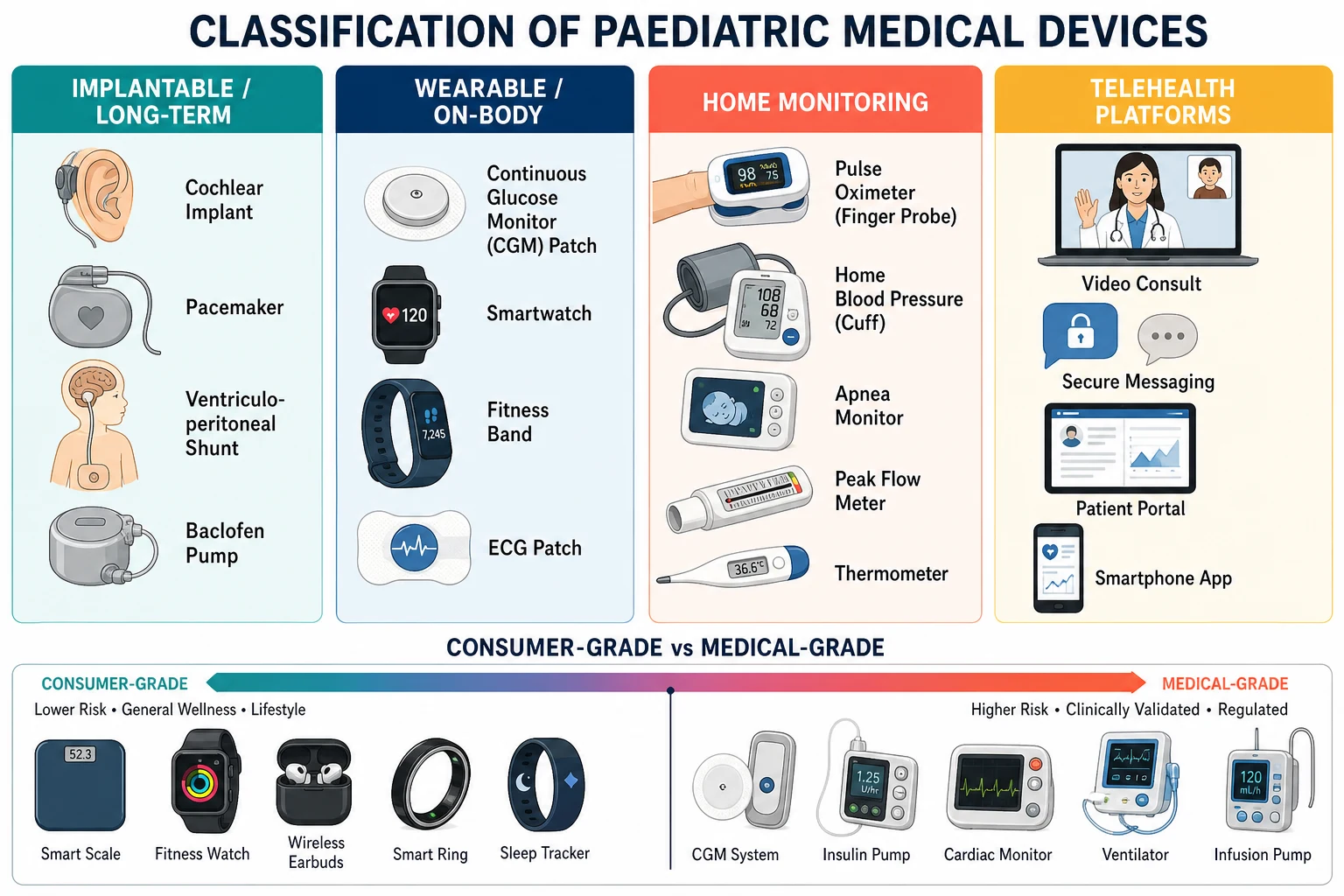
The implantable or long-term class is anchored by the cochlear implant, the cardiac pacemaker, the ventriculoperitoneal shunt and the intrathecal baclofen pump. These devices are placed surgically, are owned by the surgical or sub-specialty team, and present to the general paediatrician only when they fail; their troubleshooting belongs on the device-specific pages. The wearable or on-body class is where the candidate earns most marks: the CGM patch, the smartwatch, the fitness band and the ECG patch sit on the skin, generate a continuous signal, and are increasingly used by families without a clinician's intermediation. The home monitoring class includes the pulse oximeter finger probe, the home blood pressure cuff, the apnea monitor, the peak flow meter and the thermometer, each intermittent, each operator-dependent and each subject to the equity and accuracy problems below. The telehealth platforms class is the channel rather than the sensor — video consultation, secure messaging, the patient portal and the smartphone app — and it is examined as the access question rather than the device question. [8] [9]
Four device classes and the question each answers
Epidemiology & Risk Factors
Device use is now common across paediatrics because the technology has matured and the COVID-19 pandemic accelerated its uptake. Continuous glucose monitor use in children with type 1 diabetes has risen sharply; the Wadwa trial of hybrid closed-loop control in young children, the Laffel trial in adolescents and the SENCE trial in the very young have moved the CGM from an optional add-on to a near-standard of care in well-resourced settings, with ISPAD 2024 endorsing its use across the paediatric age range. [1] [2] [3] [4]
Home pulse oximetry is widespread after bronchiolitis, cardiac surgery and chronic neonatal lung disease, yet the Fierro survey of prescribers at a quaternary children's hospital showed wide variation in who was prescribed a device, for how long and with what thresholds — a finding that signals the absence of a single accepted standard. The Ferro study of parental insights added the family's perspective: many parents found home pulse oximetry reassuring, but a substantial minority described alarm-related sleep disruption and uncertainty about when to act. The Hoppenbrouwer study of night-to-night variability quantified the underlying problem: a single night of pulse oximetry under- or over-estimates the burden of desaturation, so clinical decisions must not rest on one recording. [10] [11] [12]
The equity burden is the third epidemiological fact the candidate must hold. The Sjoding analysis of over ten thousand paired pulse oximetry and arterial blood gas measurements showed occult hypoxaemia — a SpO2 reading in the normal range when the arterial saturation was low — was nearly three times more common in Black patients than in White patients. The Gudelunas prospective study extended the finding into low-perfusion states, where darkly pigmented skin was again associated with missed hypoxaemia. The Rathod collaborative recommendations framed the issue as a patient-safety rather than a tolerance problem and set equity-aware mitigations. [5] [6] [7]
The numbers the candidate must hold
Pathophysiology
Hold two sensor physiologies in working memory — the continuous glucose monitor and the pulse oximeter — because these are the two the fellowship examiner tests, and because they each carry a teachable failure mode that turns a number into a clinical decision. [4] [5]
The continuous glucose monitor measures interstitial fluid glucose, not plasma glucose. A tiny flexible sensor is placed subcutaneously — usually the upper arm or the abdomen in a child — and a glucose-oxidase enzyme electrode generates a current proportional to the interstitial glucose concentration. Because glucose must move from plasma to interstitial fluid before the sensor reads it, the interstitial value lags the plasma value by five to fifteen minutes, longer during rapid change. The clinical consequence is the lag: a falling glucose can be missed at the trough, and a post-meal rise can lag the capillary value. The sensor is either calibrated by the user against a fingerstick or factory-calibrated; the ambulatory glucose profile (AGP) summarises one to two weeks of data into a median trace with the time in range, time above range and time below range metrics. [4]
The pulse oximeter estimates arterial oxygen saturation by passing two wavelengths of light — 660 nanometres red and 940 nanometres infrared — through a pulsatile vascular bed and ratioing the absorbance of oxyhaemoglobin to deoxyhaemoglobin. The pulse is the discriminator: only the arterial bed pulsates, so the device subtracts the venous and tissue background. The failures arise where the assumptions break. Dark skin pigmentation increases the light absorbed at the red wavelength and biases the saturation upward, so a child with dark skin can have a normal SpO2 reading in the presence of true hypoxaemia. Low perfusion — cold extremity, shock, vasoconstriction — reduces the pulse signal and widens the error. Motion moves the probe and adds artefact. Nail polish, methaemoglobinaemia and carboxyhaemoglobinaemia each bias the reading in characteristic directions. These are not tolerances; they are patient-safety failures. [5] [6]
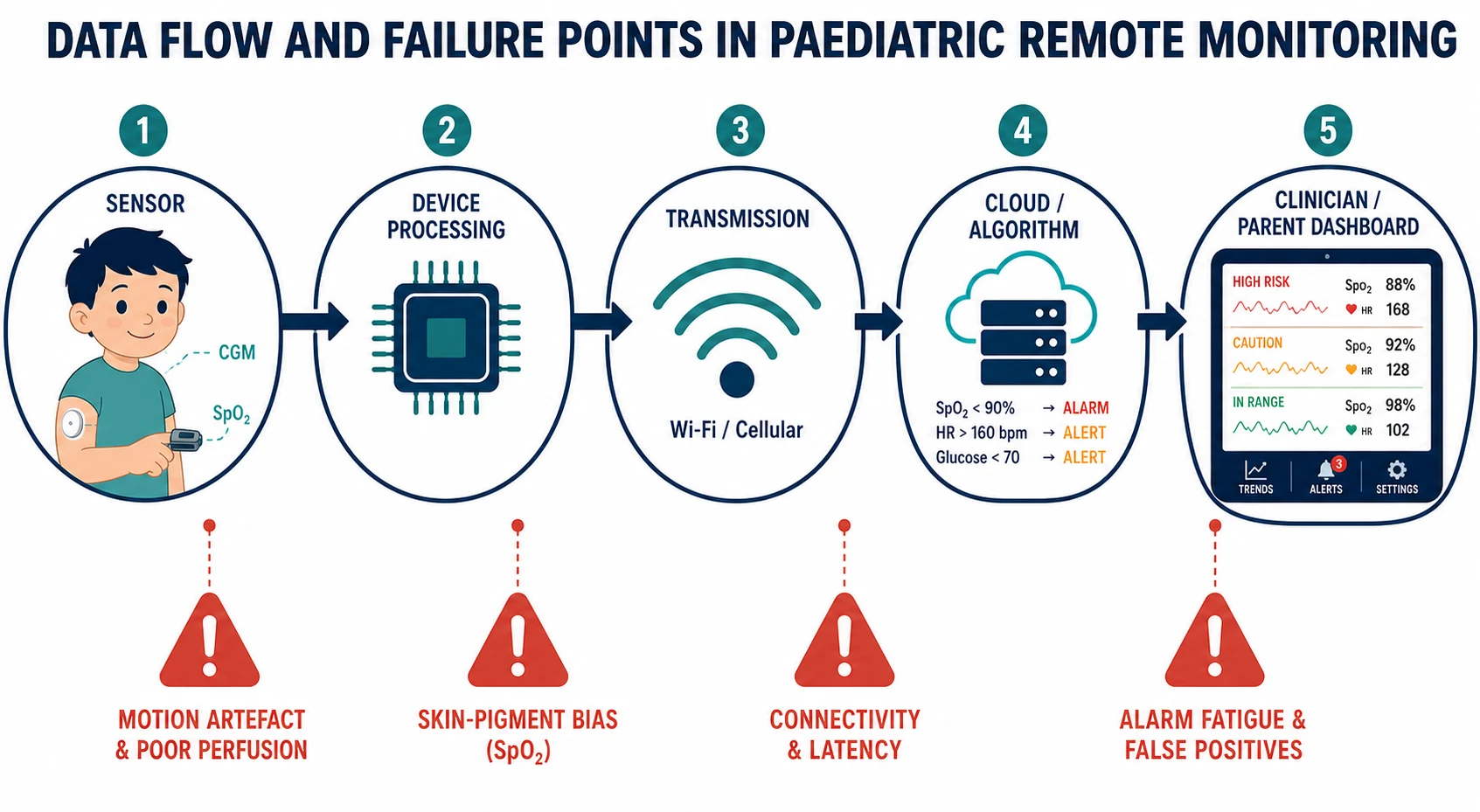
The data-flow pipeline that carries the sensor's signal from the home to the clinician fails at each node in a characteristic way. The sensor produces motion artefact and the perfusion error above. The device processing introduces calibration drift and skin-pigment bias. The transmission layer adds latency and dropout — a particular problem in rural and remote Australia, where the broadband that the device assumes may be absent. The cloud algorithm applies thresholds that, if poorly tuned, generate alarm fatigue. The clinician or parent dashboard demands interpretation: a missed alarm, a normalised abnormal or an over-reacted false alarm can each cause harm. The Hoppenbrouwer finding that a single night of pulse oximetry is unreliable extends the failure to the data-sampling node — too little data is as dangerous as the wrong data. [7] [10]
Clinical Presentation
The family brings the device to clinic in three characteristic ways. The first is the burden presentation: a parent of a child on a CGM describes night-time alarms, sleep disruption and anxiety about trend arrows, and asks whether the device is making the family's life worse rather than better. The second is the discrepancy presentation: a parent reports a CGM reading that does not match a fingerstick, or a pulse oximeter reading that does not match the child's appearance, and asks which to trust. The third is the screening-flag presentation: a parent's smartwatch has flagged an irregular rhythm or a low heart-rate variability score in the child, and the family seeks reassurance or action. [8] [11]
Each presentation demands a structured response. For the burden presentation the candidate assesses the family's experience, reviews the AGP or the pulse oximetry log, tunes the thresholds and decides with the family whether to continue, modify or stop. For the discrepancy presentation the candidate sorts the differential by sensor failure mode (the CGM lag, the pulse oximetry bias, the compressed sensor, the low perfusion) and confirms the true value with a device-independent measure — a capillary or laboratory glucose, an arterial blood gas with co-oximetry. For the screening-flag presentation the candidate treats the consumer device's output as a screening signal rather than a diagnosis, runs the clinical differential, and obtains the device-independent test — the 12-lead ECG, the Holter, the clinician overread. [6] [9]
Differential Diagnosis
The differential of a discrepant device reading runs in two columns — the differential of a discrepant CGM, and the differential of a discrepant pulse oximeter — and the candidate must hold both. [4] [5]
For the discrepant continuous glucose monitor, run the differential through (a) true hypoglycaemia or hyperglycaemia that the sensor has measured correctly but the user has misread; (b) sensor lag during rapid change, the five-to-fifteen-minute gap that produces a mismatch with the capillary value; (c) sensor compression, the classic sleep-on-arm flattening that drives the trace toward a false low for hours; (d) sensor failure at end of life, with drift, dropout or a no-calibration error; and (e) interference, the acetaminophen (paracetamol) interference with older glucose-oxidase sensors that produced a false high, and the hydroxyurea interference reported in some sensors. The first action for any critical CGM reading is a confirmatory fingerstick, because the differential is wide and the action — carbohydrate, glucagon, an emergency call — is costly to get wrong. [4]
For the discrepant pulse oximeter, run the differential through (a) true hypoxaemia that the sensor has under-read because of dark skin pigmentation; (b) true hypoxaemia that the sensor has under-read because of low perfusion or motion; (c) methaemoglobinaemia, where the pulse oximeter trends toward 85 per cent regardless of the true saturation; (d) carboxyhaemoglobinaemia from carbon monoxide poisoning, where the pulse oximeter over-reads because it cannot distinguish carboxyhaemoglobin from oxyhaemoglobin; and (e) nail polish or a poorly seated probe producing motion artefact. The first action for any pulse oximeter reading that does not fit the child is an arterial blood gas with co-oximetry, which measures the true saturation and the dyshaemoglobins in a single sample. [5] [6]
For the smartwatch arrhythmia flag, run the paediatric differential deliberately. Sinus arrhythmia — the variation of heart rate with respiration — is the normal physiological rhythm of childhood and a leading source of consumer-device flags. Premature atrial contractions are common and benign in the child with a structurally normal heart. Supraventricular tachycardia is the pathological fast rhythm that warrants action, and true atrial fibrillation is rare in children and should prompt a search for a structural or metabolic cause. A clinician-overread of the device tracing and a 12-lead ECG separate these before any action is taken. [9]
Two discrepant readings, two differentials
Discrepant CGM
Discrepant pulse oximeter
Clinical & Bedside Assessment
The bedside assessment of a family using a digital-health device is a structured interview, not a glance at the number. Begin with the device: its name, its manufacturer, its regulatory status — is it a TGA-registered or FDA-cleared medical device, or a consumer wellness product bought online? Then the deployment: who set it up, what thresholds were chosen, what education was given, what is the written action plan? Then the family's experience: the burden of alarms, the impact on sleep, school and work, the family's confidence, the decision to continue, modify or stop. Then the child's symptoms: is the number congruent with how the child looks, and what does the family do when they disagree? [8] [11]
For the continuous glucose monitor, assess the sensor age (most are ten to fifteen days, with paediatric-specific wear extensions), the calibration status, the most recent ambulatory glucose profile, and the family's hypoglycaemia symptoms. Read the AGP for the headline metrics — time in range, time below range, the glycemia risk index — and ask the family how they respond to a low alarm, a trend arrow down, a sensor compression alarm. Ask about the adhesive tolerance: skin reactions are common in children, and the family's choice of adhesive, barrier film and site rotation is a clinical decision. [1] [4]
For the pulse oximeter, assess the child's peripheral perfusion, skin pigmentation, the plethysmograph waveform if the device displays it, and the congruence between the number and the child's work of breathing, colour and conscious level. Repeat the reading with a different probe and a different site if the first does not fit. If the discrepancy persists in an unwell child, escalate to an arterial blood gas with co-oximetry — the device-independent measure that ends the differential. For the smartwatch flag, examine the child, obtain a 12-lead ECG, and arrange a clinician overread of the device tracing before accepting any algorithmic diagnosis. [5] [6]
Investigations
The investigations in paediatric digital health are the device-independent measures that confirm or refute the device's signal. For the continuous glucose monitor, the confirmatory test is the capillary glucose by fingerstick (point-of-care) and, where doubt persists, the laboratory glucose. The candidate must know the lag and the interference profile so the confirmatory test is interpreted in the light of the sensor's known failure modes — a sensor compression event, for example, is resolved by a fingerstick at a different site. [4]
For the pulse oximeter, the confirmatory test is the arterial blood gas with co-oximetry. Co-oximetry measures oxyhaemoglobin, deoxyhaemoglobin, carboxyhaemoglobin and methaemoglobin in a single sample, and it is the test that ends the differential of a discrepant pulse oximeter. The candidate must also know when a pulse oximeter reading should not be trusted at all: in shock, in severe anaemia, in methaemoglobinaemia and in carbon monoxide poisoning. [5] [6]
For the smartwatch arrhythmia flag, the confirmatory investigations are the 12-lead ECG, the ambulatory Holter monitor, and the clinician overread of the device tracing. The candidate must resist the algorithmic diagnosis: a consumer device's rhythm label is a screening signal, not a diagnosis, and the diagnosis is made on the device-independent tracing. [9]
The device-independent confirmatory tests
Management — Resuscitation
The deteriorating child comes before any device reading, and the structured ABCDE assessment overrides a falsely reassuring or falsely alarming number. A CGM low alarm does not delay the assessment of an unconscious child; a pulse oximeter high reading does not delay the oxygen therapy an unwell child needs; a smartwatch flag does not delay the resuscitation of a child in shock. The device extends the assessment; it does not restructure it. [8]
For the CGM reading below 54 mg/dL (3.0 mmol/L), the immediate management is the hypoglycaemia protocol: confirm with a fingerstick, give 10 to 15 grams of fast-acting oral carbohydrate if the child is conscious and able to swallow (glucose tablets, juice, glucose gel), give glucagon 0.5 milligrams intramuscularly for the child under twelve years or 1 milligram at twelve years and over if the child is unconscious or unable to swallow safely, and recheck the glucose in fifteen minutes. The family must have glucagon available at home and know how to use it; the device is not a substitute for the emergency kit. [4]
For the pulse oximeter reading that does not fit the unwell child, the immediate management is escalation to the arterial blood gas with co-oximetry and the treatment of the child — oxygen therapy, respiratory support, the management of the underlying cause — while the differential is resolved. Do not be falsely reassured by a normal number, and do not delay the respiratory support that the child's work of breathing already demands. For the lost device signal in a high-risk technology-dependent child, the immediate management is to call the family, assess the child clinically, and use the clinical pathway as the safety-net — silence does not mean the child is well. [5] [7]
Resuscitation sequence when a device reading does not fit the child
Assess airway, breathing, circulation, disability, exposure — the structured ABCDE overrides the device reading
If the CGM reads under 54 mg/dL (3.0 mmol/L), confirm with a fingerstick, give 10 to 15 g fast-acting oral carbohydrate if conscious, or glucagon 0.5 mg IM under 12 years or 1 mg at 12 years and over if unconscious; recheck in 15 minutes
If the pulse oximeter reading does not fit the unwell child, escalate to an arterial blood gas with co-oximetry and treat the child
If the device signal is lost in a high-risk child, call the family and assess the child clinically — silence is not safety
Document the device discrepancy and the device-independent confirmation, and review the thresholds with the family
Management — Definitive & Stepwise
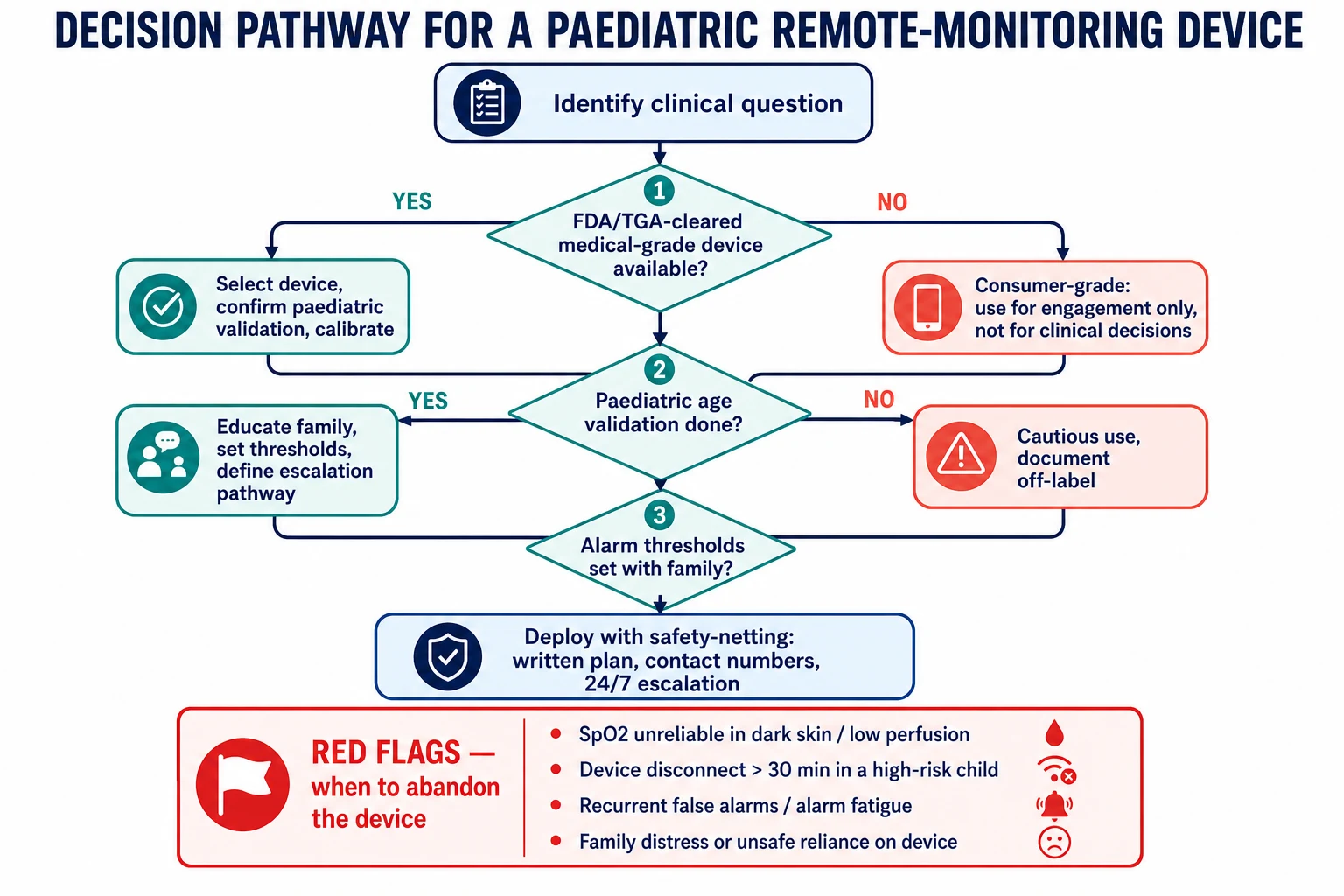
The definitive management of paediatric digital health is the deployment of a device on the S.E.N.S.O.R. principle, the tuning of the thresholds with the family, and the longitudinal review of the AGP, the pulse oximetry log or the wearable trend. The stepwise selection begins with the clinical question: what decision will the device's data inform? If the answer is "none", the device is not indicated. If the answer is "it will guide insulin dosing", a CGM is indicated; if "it will guide home oxygen titration in chronic lung disease", a pulse oximeter is indicated; if "it will reassure the parent", the device is treating the parent's anxiety and a different intervention is usually better. [8]
For continuous glucose monitoring, the ISPAD 2024 consensus and the Battelino international consensus set the operational targets. Time in range — glucose between 70 and 180 mg/dL (3.9 and 10.0 mmol/L) — should exceed 70 per cent of the day. Time below 70 mg/dL (3.9 mmol/L) should be under 4 per cent, and time below 54 mg/dL (3.0 mmol/L) under 1 per cent. The Wadwa trial of hybrid closed-loop control in young children showed closed-loop systems achieved a mean time in range of around 80 per cent versus around 55 per cent for sensor-augmented pump therapy, a near-doubling that moved the technology into the standard of care. The Laffel trial in adolescents and young adults showed CGM improved glycaemic control without increasing hypoglycaemia, and the SENCE trial in very young children showed CGM was feasible when paired with family behavioural support. [1] [2] [3] [4]
For home pulse oximetry, the deployment demands a chosen child (chronic lung disease, home oxygen, post-cardiac surgery), a calibrated medical-grade device, a trained family, a written action plan with explicit thresholds (when to increase oxygen, when to call, when to come in), and a review point at which the device is either continued, modified or stopped. The Hoppenbrouwer finding that a single night under-estimates the burden of desaturation means that a trend across several nights — not one recording — is the basis of the clinical decision. The Ferro parental insights and the Fierro prescriber survey together demand a shared-decision conversation at the start, an alarm-management conversation in the middle, and a stop-or-continue conversation at the review. [10] [11] [12]
For telehealth, the candidate must hold the access question alongside the safety limitations. Telehealth extends the reach of subspecialty care into rural and remote Australia, and the Li 2024 systematic review supports mHealth effectiveness in adolescents and young adults with chronic disease, particularly for self-management and transition. But telehealth cannot examine the abdomen, cannot palpate the abdomen, cannot auscultate the chest with the fidelity of the bedside, and cannot resuscitate. The decision to use telehealth turns on whether the clinical question can be answered without a bedside examination — and the safety-net is the rapid escalation to in-person care when it cannot. [9]
In ANZ the Therapeutic Goods Administration registers medical devices including software-based medical devices; the RACP and the Royal Children's Hospital Melbourne guide remote-monitoring programmes; the Australian Diabetes Society and the Australasian Paediatric Endocrine Group endorse the ISPAD-aligned CGM and hybrid closed-loop targets. The Closing the Gap framework and the National Aboriginal and Torres Strait Islander Health Plan place digital-health equity on the safety agenda, because the rural and remote family without broadband cannot benefit from a device that assumes it. [4] [7]
Specific Subtypes & Scenarios
The continuous glucose monitor in the very young child — under six years — is the highest-yield subtype. The SENCE trial established that CGM use is feasible in this age group when paired with family behavioural support, with the technical caveats of adhesive tolerance, alarm burden and the need for the family to confirm critical readings with a fingerstick. The Wadwa trial extended the evidence into hybrid closed-loop control, where the system achieved a substantially higher time in range than sensor-augmented pump therapy. The candidate must know that the very young child on a closed-loop system still requires meal announcement, still requires site changes, and still requires the family to respond to alarms — the system automates the basal insulin, not the whole of diabetes care. [1] [3]
The home pulse oximeter in the infant with bronchopulmonary dysplasia or chronic neonatal lung disease is the second subtype. The Fierro prescriber survey showed wide variation in practice, and the Hoppenbrouwer variability study demanded a multi-night trend rather than a single recording. The deployment demands a written action plan that the family can execute at three o'clock in the morning: what saturation triggers an increase in oxygen, what triggers a call to the team, what triggers an emergency department attendance. The apnea-of-prematurity home monitor is largely historical and is not recommended for routine home use, because it has not been shown to prevent sudden infant death and its false-alarm burden is high. [10] [11] [12]
The child with medical complexity or technology dependence is the third subtype. The Foster AAP policy on remote monitoring of patient- and family-generated health data frames this child: multiple devices, a care coordinator, a family that is both operator and interpreter, and a documented plan that integrates the device data into the clinical pathway. The candidate must hold the family burden as a clinical fact: the family of a technology-dependent child is the de facto intensive-care nurse at home, and the device must support rather than exhaust them. [8]
The rural or remote family is the fourth subtype. Telehealth extends the subspecialty reach, but the digital divide — broadband, device ownership, English-language and health-literacy — determines whether the extension reaches the family. The candidate must name the equity gap as a clinical risk and deploy the device with an access plan that addresses it. [9]
Complications & Pitfalls
The complications of paediatric digital health are the equity failure, the accuracy failure, the alarm-fatigue failure and the privacy failure, and each is examined. The pulse oximetry equity failure is the headline: Sjoding showed occult hypoxaemia in Black patients, Gudelunas extended it to darkly pigmented skin under low perfusion, and Rathod framed the mitigation as equity-aware thresholds, clinical correlation and an arterial blood gas when the reading does not fit. The candidate who quotes a pulse oximeter reading without naming its equity limitation in a child with dark skin has missed the question. [5] [6] [7]
The alarm-fatigue failure drives non-adherence and device abandonment. The CGM family who silences the low alarm because it sounds every night at three o'clock is the family whose child will have an unrecognised severe hypoglycaemia; the pulse oximetry family who stops using the device because of the false alarms is the family whose child will deteriorate unrecognised. The mitigation is the threshold review at every clinic visit, the silencing of non-critical alarms, the schedule of protected sleep, and the explicit conversation about whether to continue, modify or stop. Device abandonment without a safety-net is the pitfall. [8] [11]
The privacy failure is the unregulated data sharing of consumer paediatric wearables and apps. Many consumer products are not covered by the health-privacy frameworks that bind the clinician, and the data they collect — a child's heart rate, sleep, location, glucose — may be shared, sold or used for advertising in ways the family does not understand. The candidate must hold this as a child-safety issue: the paediatric data subject cannot consent, and the long-term stewardship of their data is unresolved. The mitigation is the preference for regulated medical-grade devices, the family's informed choice, and the policy advocacy for paediatric data protection. [9]
Prognosis & Disposition
The child who belongs in a remote-monitoring programme is the child with a chronic disease and a defined clinical question that the device's data can answer: the child with type 1 diabetes whose insulin dosing is guided by the AGP, the child with chronic lung disease whose home oxygen is titrated by the pulse oximetry trend, the technology-dependent child whose integrated data reaches a care coordinator. The child who does not belong is the well child for whom a device creates more anxiety than benefit, and the family for whom the device widens rather than narrows the equity gap. [8]
The disposition of a child who has had a true device alert — a severe hypoglycaemia, a sustained desaturation, a lost signal in a high-risk child — is the clinical review in person or by telehealth, the escalation to the emergency department if the child is unwell, and the documented plan to prevent recurrence. The plan reviews the thresholds, the family's response, the device's function and the underlying condition, and it sets the next review point. [4] [11]
The long-term prognosis of the technology-dependent child supported by a remote-monitoring programme depends on the team's preparation — a written plan, a trained family, a stocked bedside, an escalation pathway — and on the family's capacity to sustain the device over years. The decision to stop a device is balanced against the risk of the underlying condition and is made with the family as a shared decision with a documented safety-net. [8] [9]
Special Populations
The very young child — under six years — adapts the device to the small body surface, the adhesive tolerance, the family behavioural support and the SENCE-trial evidence. The CGM site is usually the upper arm or the buttock, the adhesive is reinforced with a barrier film, the alarms are tuned to limit the night-time burden, and the family is supported to confirm critical readings with a fingerstick. [3]
The Indigenous, rural or remote family adapts the device to the connectivity, the cultural safety, the integration with a local service and the avoidance of a digital tool that widens disparity. The candidate must name the Closing the Gap framework in ANZ, the cultural-safety obligation, and the family's right to a device that works in their context. Telehealth is not a substitute for the local service; it is a support to it. [7] [9]
The adolescent and young adult in transition adapts the device to the mHealth evidence for self-management, the developmentally appropriate choice, the shared care with adult services, and the privacy and consent issues that come to the fore as the young person takes ownership. The Li 2024 systematic review supports mHealth effectiveness in this group for chronic-disease self-management, but the digital divide persists into young adulthood and the transition planning must address it. [9]
The child with medical complexity or technology dependence integrates multiple devices, a care coordinator, the family's burden, and the documented plan. The child with a disability or neurodivergence adapts the device to the accessibility of the interface, the family's capacity, the sensory burden of alarms, and the avoidance of a one-size-fits-all deployment. [8]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric digital health is anchored by the CGM and hybrid closed-loop trials and by the pulse oximetry equity studies. The Wadwa NEJM 2023 trial randomised young children with type 1 diabetes to hybrid closed-loop control versus sensor-augmented pump therapy and showed a substantially higher time in range in the closed-loop arm, a finding that moved the technology into the standard of care for the very young. The Laffel JAMA 2020 trial extended the CGM evidence to adolescents and young adults, and the SENCE Diabetes Care 2021 trial established feasibility in the very young with family behavioural support. The Battelino Lancet Diabetes Endocrinol 2023 international consensus set the CGM metrics and targets that ISPAD 2024 operationalised for children. [1] [2] [3] [4]
The pulse oximetry equity evidence is anchored by the Sjoding NEJM 2020 cohort, which showed occult hypoxaemia was nearly three times more common in Black patients than in White patients across over ten thousand paired measurements, the Gudelunas Anesth Analg 2024 prospective study of missed hypoxaemia in darkly pigmented skin under low perfusion, and the Rathod JACC Adv 2022 collaborative recommendations on pulse oximeter accuracy and equity. The Foster Pediatrics 2022 AAP policy frames remote monitoring of patient- and family-generated health data in paediatrics, the Li J Med Internet Res 2024 systematic review supports mHealth in adolescents and young adults with chronic disease, and the home pulse oximetry evidence of Fierro, Ferro and Hoppenbrouwer anchors the home-monitoring practice. [5] [6] [7] [8] [9] [10] [11] [12]
Where thresholds, glucose targets or device-clearance ages differ across regions, the exam expects the candidate to name the regulator — the TGA in Australia, the MHRA in the United Kingdom, the FDA in the United States, Health Canada in Canada — and to state both values with the regional label rather than invent a compromise. [7]
Exam Pearls
A.G.P. — the CGM report a candidate must read
State the CGM lag verbatim: interstitial glucose lags plasma by five to fifteen minutes, so a rapid fall can be missed at the trough — confirm any critical reading with a fingerstick before acting. State the AGP targets verbatim: time in range of 70 to 180 mg/dL (3.9 to 10.0 mmol/L) above 70 per cent, time below 70 mg/dL (3.9 mmol/L) under 4 per cent, time below 54 mg/dL (3.0 mmol/L) under 1 per cent — ISPAD 2024 and the Battelino consensus. State the pulse oximetry equity red flag: SpO2 over-reads in dark skin pigmentation and under-reads in low perfusion, so a normal number in an unwell child does not exclude occult hypoxaemia — escalate to an arterial blood gas with co-oximetry. [4] [5] [6]
State the alarm-fatigue mitigation: tune the thresholds, silence the non-critical alarms, schedule protected sleep, and review at every clinic visit — do not abandon the device without a safety-net plan. State the device-selection rule: define the clinical question, choose a medical-grade device, confirm paediatric age validation, set the thresholds with the family, and define the escalation pathway before deployment. State the Wadwa result: hybrid closed-loop control in young children achieved a substantially higher time in range than sensor-augmented pump therapy, moving the technology into the standard of care. [1] [8]
References
- [1]Wadwa RP Trial of Hybrid Closed-Loop Control in Young Children with Type 1 Diabetes N Engl J Med, 2023.PMID 36920756
- [2]Laffel LM Effect of Continuous Glucose Monitoring on Glycemic Control in Adolescents and Young Adults With Type 1 Diabetes: A Randomized Clinical Trial JAMA, 2020.PMID 32543683
- [3]Strategies to Enhance New CGM Use in Early Childhood (SENCE) Study Group A Randomized Clinical Trial Assessing Continuous Glucose Monitoring (CGM) Use With Standardized Education With or Without a Family Behavioral Intervention Compared With Fingerstick Blood Glucose Monitoring in Very Young Children With Type 1 Diabetes Diabetes Care, 2021.PMID 33334807
- [4]Battelino T Continuous glucose monitoring and metrics for clinical trials: an international consensus statement Lancet Diabetes Endocrinol, 2023.PMID 36493795
- [5]Sjoding MW Racial Bias in Pulse Oximetry Measurement N Engl J Med, 2020.PMID 33326721
- [6]Gudelunas MK Low Perfusion and Missed Diagnosis of Hypoxemia by Pulse Oximetry in Darkly Pigmented Skin: A Prospective Study Anesth Analg, 2024.PMID 38109495
- [7]Rathod M Improving the Accuracy and Equity of Pulse Oximeters: Collaborative Recommendations JACC Adv, 2022.PMID 38939706
- [8]Foster C Remote Monitoring of Patient- and Family-Generated Health Data in Pediatrics Pediatrics, 2022.PMID 35102417
- [9]Li Z Usability and Effectiveness of eHealth and mHealth Interventions That Support Self-Management and Health Care Transition in Adolescents and Young Adults With Chronic Disease: Systematic Review J Med Internet Res, 2024.PMID 39589770
- [10]Hoppenbrouwer XLR Night to night variability of pulse oximetry features in children at home and at the hospital Physiol Meas, 2021.PMID 34713819
- [11]Ferro DF Parental Insights into Improving Home Pulse Oximetry Monitoring in Infants Pediatr Qual Saf, 2022.PMID 35369408
- [12]Fierro J Home pulse oximetry after discharge from a quaternary-care children's hospital: Prescriber patterns and perspectives Pediatr Pulmonol, 2022.PMID 34633759