Paeds · investigations-procedures-and-technology
Nasogastric tube insertion and verification
Also known as Paediatric nasogastric tube placement · NG tube pH verification · NG tube never event · Nasogastric tube insertion in infants and children · Orogastric tube placement in neonates
Fellowship guide to inserting and verifying a nasogastric (NG) tube in a child of any age, from the preterm neonate to the adolescent. Covers selecting the tube size by age, measuring the insertion length, the gentle age-adapted insertion technique, and confirming gastric position by aspirate pH testing at a threshold of 5.5 or less, escalating to a radiograph when the pH is above 5.5 or no aspirate can be obtained. Names and rejects the deprecated methods (the whoosh test, the bubbling test, litmus paper and auscultation alone), defends why feeding or medicating through an unverified tube is a Never Event, and recognises the complications of misplacement (respiratory intubation, pneumothorax, pleural feed) and of traumatic insertion (pharyngo-oesophageal perforation in neonates, intracranial misplacement). Includes ANZ, UK, US and Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
VERIFY before every feed
Overview & Definition
A two-year-old is admitted overnight with a small-bowel obstruction and needs her stomach decompressed, or a preterm infant on the neonatal unit cannot yet coordinate suck and swallow and needs milk by tube. In both cases the device is a nasogastric tube: a flexible, hollow tube passed through a nostril, along the floor of the nose, through the pharynx and oesophagus, to rest with its tip in the stomach. Its job is to open a safe route into the gut for feed, fluid or medicine, or to let gas and gastric contents out when the bowel is obstructed. [1] [8]
The procedure looks simple, which is exactly why it is dangerous. The nose, the pharynx and the opening of the airway sit within a centimetre or two of each other, so a tube aimed at the oesophagus can instead turn into the larynx and travel down the trachea into a bronchus. A child who is intubated, sedated, very young, or who simply cannot cough, gives no signal that this has happened. If feed or medicine is then poured down the tube, it fills the lung or the pleural space, and the child aspirates or develops a pneumothorax. The safety of the procedure therefore rests not on the insertion but on what you do afterwards: you verify the position, and you do it every time before anything goes down the tube. [4] [9]
The discipline comes from a patient-safety history. In the United Kingdom, a series of deaths and serious harms from feeding misplaced tubes led the National Patient Safety Agency, and later NHS England and NHS Improvement, to retire the old bedside checks and to make pH testing of the aspirate the standard. Feeding or medicating through a tube whose position has not been confirmed, or has been confirmed by a method that is no longer allowed, is now classified in the NHS framework as a Never Event: a serious, largely preventable incident that should not occur if the known safety barriers are in place. The same logic shapes Australasian, North American and European paediatric guidance. [1] [4] [8]
Classification
Classify the tube first by what you want it to do, because the purpose decides the bore, the material, the size and the verification pathway. A fine-bore feeding tube is slim and soft, designed to deliver milk or liquid feed over hours with the least nasal discomfort; it is the tube you reach for when the gut works and the child simply cannot swallow safely or enough. A wide-bore decompression or lavage tube, the Ryles type, is stiffer and wider, designed to let gas, fluid and particulate gastric contents run out, or to allow gastric lavage after an ingestion; it is the tube you reach for in bowel obstruction or overdose. [8] [1]
Classify the route next: nasogastric, passed through the nose, against orogastric, passed through the mouth. The nasal route is usual for the older infant and child because it is comfortable and stays in place, but in the very preterm or small neonate, and in any child with a base-of-skull or significant mid-face injury, the nasal route is avoided and an orogastric tube is used instead. An orogastric tube is also the practical choice when the nares are blocked or when the neonate is an obligate nose-breather and a nasal tube would obstruct the airway. [1] [11]
Epidemiology & Risk Factors
Nasogastric tubes are among the commonest devices placed in a paediatric inpatient. They run through neonatal units, paediatric and cardiac intensive care, surgical and general wards, and emergency departments, and they are often placed and re-placed many times in a single admission. The risk is not that they are rare; it is that their familiarity hides how often a freshly placed tube lies outside the stomach. [1] [2]
When investigators have audited first-placed tubes with a radiograph, a meaningful proportion are found in the respiratory tract, coiled in the oesophagus or mouth, or short of the stomach. The risk concentrates where the child cannot signal the error: in the intensive care unit, in the intubated or sedated child who cannot cough or complain, in the infant and small neonate, and in the child with an altered level of consciousness. The child-level factors that raise misplacement are small size, reduced consciousness, an absent cough reflex, agitation, and an immature or distorted upper airway. [2] [5]
The procedure-level factors are the ones a team can actually control. The dominant one is the verification method: a tube checked with a deprecated method, or not checked at all before feeding, is the direct route to a Never Event. Close behind are the failures of the re-verification habit, feeding after the tube has been retaped, retched, transferred or extubated without re-checking, and the documentation failure of writing "tube in situ" without recording the method, the pH value and the length. [3] [9]
What shapes the risk of a misplaced tube
Pathophysiology
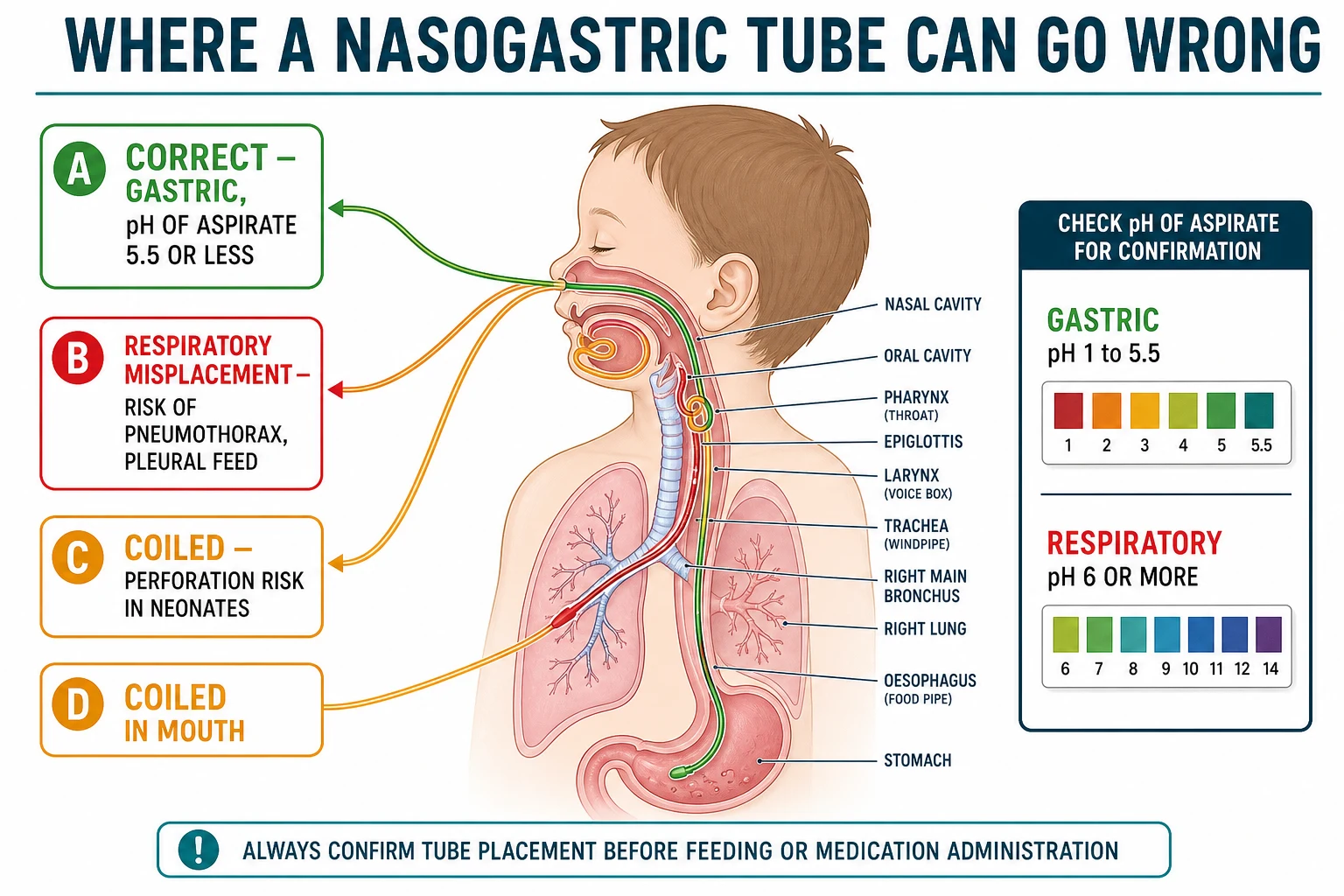
To understand why verification matters, picture where the tube can go. The intended path is short and direct: nostril, along the floor of the nose, into the nasopharynx, down past the laryngeal inlet, through the upper and then the lower oesophageal sphincter, to rest in the body or antrum of the stomach. The opening of the airway sits beside this path like a side road, and a tube that misses the oesophagus can drop into the larynx, pass between the vocal cords, and travel down the trachea into a main bronchus, most often the right. [4] [10]
A tube in the bronchial tree is the dangerous wrong path for two reasons. First, if feed or medicine is delivered it fills the airway and the alveoli or tracks into the pleural space, causing chemical pneumonitis, aspiration pneumonia, a pleural effusion or a pneumothorax; withdrawal of a tube that has already irritated or punctured the lung can itself trigger a tension pneumothorax. Second, the child who is intubated, sedated or very young often does not cough, so there is no clinical alarm until feed is running and the child deteriorates. That is why a single bedside check that is wrong, or absent, can be fatal. [9] [10]
The third wrong path is coiling. In the infant or the child who cannot cooperate with swallowing, the stiff tip meets the posterior pharyngeal wall and, instead of turning into the oesophagus, curls back on itself in the mouth or folds in the pharynx or upper oesophagus. The external length looks right, but the tip never reached the stomach; aspirate may be scant or absent, and a feed would pool or reflux. The fourth wrong path is traumatic: in the neonate the posterior pharyngeal wall and the cricopharyngeal region are fragile, and forceful or repeated insertion can create a false passage through the wall, sending the tube into the mediastinum or pleura and presenting as sudden deterioration with a pneumothorax or subcutaneous emphysema. [5] [11]
The science that makes pH testing work is the acidity of the stomach. Gastric contents are normally acidic, with a pH between roughly 1 and 5.5, because parietal cells secrete hydrochloric acid. Respiratory secretions and small-intestinal contents are not acidic, with a pH of 6 or more. So a strip of pH paper held to a drop of aspirate separates the two compartments: a value of 5.5 or less says the tip is almost certainly bathed in gastric acid, while a value of 6 or more says it is in the airway, has migrated into the duodenum, or that the acid has been diluted or suppressed. That single number is the basis of the whole bedside rule. [6] [7]
Clinical Presentation
The child who needs a nasogastric tube arrives with a problem the tube can solve, and the first clinical task is to be clear what that problem is. The common indications are unsafe or absent swallowing, as in the child with an altered conscious state or a severe neurodisability; inadequate intake or malnutrition that needs supplementing; bowel obstruction or ileus that needs decompression; the need to give a medicine that only has an enteral form; and, after some ingestions, gastric lavage. The indication sets the size and the bore of the tube and the urgency, and it should be written in the notes. [1] [8]
During insertion, the signs that the tube has entered the airway are worth knowing by heart. The cooperative, awake child coughs, splutters, becomes distressed, and may lose the ability to speak or develop a wet voice as the tube sits in the larynx. The oxygen saturation falls. In the child who cannot react, the intubated or sedated child and the small infant, these signals are muted or absent, and the only clue may be a drop in saturation or a change in breath sounds. This silence is exactly why the post-insertion check, and not the child's reaction, is the safety barrier. [4] [5]
The signs of a traumatic insertion are different and urgent. The operator meets unexpected resistance, or fresh blood appears at the nose or in the mouth. In the neonate the tube may pass but the child then deteriorates, with drooling, respiratory distress, subcutaneous emphysema at the neck, or a pneumothorax; these are the features of a pharyngo-oesophageal perforation and a false passage into the mediastinum or pleura, and they are a reason to stop and escalate, not to push harder or re-pass. [11]
The delayed presentation is the one that defines a Never Event: a tube that was misplaced but fed anyway, with the child developing new respiratory signs, pleuritic pain, a unilateral effusion or pneumonia, or sudden deterioration after a feed. The lesson written into the history of these events is that the deterioration often follows the first feed through a tube that was "checked" only by a whoosh or by habit, and that the feed itself is the injurious act. [9] [10]
Differential Diagnosis
When a tube is hard to pass, distinguish a resistant but normal child from a true anatomical cause before forcing it. A crying infant, a deviated nasal septum, or a child who simply clenches can all make passage difficult without anything being wrong. The true anatomical causes to consider are choanal atresia in the neonate, where the tube will not pass at all through one or both nares, a nasal polyp, a marked septal deviation, an oesophageal stricture or web, or a compressive vascular ring. If the tube repeatedly meets firm resistance, stop and reconsider the route and the diagnosis rather than push. [1] [11]
When the aspirate pH is above 5.5, distinguish the causes before assuming the tube is misplaced. The three benign reasons are acid suppression with a proton-pump inhibitor or an H2 blocker, which raises the gastric pH above its usual acidic range; a large recent feed or flush that has diluted the acid; and migration of the tip past the pylorus into the duodenum, where the contents are alkaline. Each of these can give a falsely high pH from a tube that is still safely in the gut, but none of them licences feeding on a pH above 5.5; the rule is to obtain a radiograph. [4] [6]
When the pH reading is plausible but the external length looks wrong, or the child retches during aspiration, consider a coiled oesophageal tube. A tip folded in the distal oesophagus can sometimes yield a small amount of acidic fluid that reads in the gastric range, while the bulk of the tube is curled and a feed would reflux. The length at the naris, compared with the measured insertion length, and the feel of the tube, are the clues that the pH number alone does not give. [8] [2]
The single most important differential judgement is the one that stops the procedure. In a child with a base-of-skull fracture or a significant mid-face injury, the nasal route is contraindicated because the tube can pass through a fractured cribriform plate into the cranium. The decision to switch to an orogastric route is made before insertion, on the history and the mechanism, not after the tube has been forced. [1] [4]
Clinical & Bedside Assessment
Begin with a focused pre-procedure assessment, because it decides whether to place the tube at all and by which route. Establish the indication and the urgency. Ask about and look for the contraindications to the nasal route: a suspected or confirmed base-of-skull fracture, a significant mid-face injury, a coagulopathy, suspected oesophageal varices, and recent nasal or oesophageal surgery. Assess the conscious level and whether the child can protect the airway and cooperate with swallowing. Decide who will hold the child and whether comfort measures or a sedative are needed. [1] [8]
Select the tube size by age. As a working guide, a neonate takes a 6 to 8 French tube, an infant an 8 French tube, a small child a 10 French tube, and an older child or adolescent a 12 to 14 French tube. Choose a fine-bore feeding tube for feeding and a wide-bore tube for decompression or lavage. These bands are starting points; the exact size for a given device and child should be checked against the current local paediatric procedure, and the choice is documented in the notes. [1] [8]
Measure the insertion length before you start. The standard bedside method is the nose-to-ear-to-xiphisternum measurement, called NEX: hold the tube tip at the nostril, lay it back to the earlobe, and then down to the xiphisternum, and note the mark. NEX is accurate enough in most children, but in infants it tends to underestimate the distance and leave the tip short of the stomach, so many units add an age-related correction or measure to a point a little beyond the xiphisternum; confirm the method your unit uses. Mark the tube, and record the length at the naris so the next clinician can detect migration. [1] [2]
Perform the insertion gently. Position the child upright or semi-recumbent, with a head tilt that opens the airway but is not overextended. Lubricate the tip with water-soluble gel. Advance slowly along the floor of the nose, aiming straight back, not upwards. In the cooperative child, encourage swallowing, offering small sips of water if permitted, and advance during the swallow. In the infant or non-cooperative child, advance steadily with a comfort hold and a pacifier. Stop at the measured length, wipe the nose, and secure the tube with tape to the cheek, leaving a loop to take the strain off the naris. [1] [8]
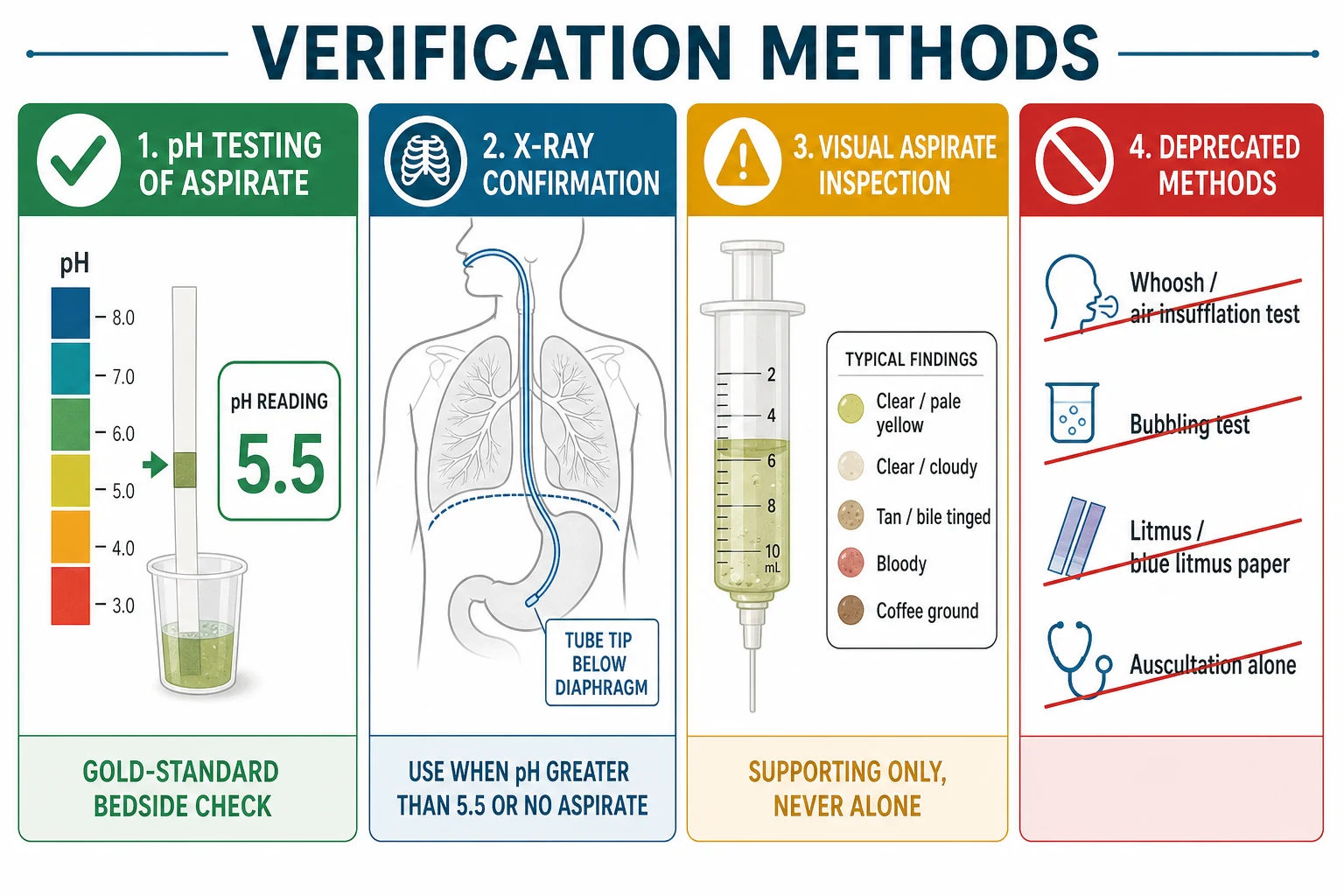
Now run the verification at the bedside. Attach a syringe and aspirate gently. Apply a drop of the aspirate to a CE-marked pH indicator strip and read the value at the time the manufacturer specifies. Record the exact number, not a symbol. If the reading is 5.5 or less, the tube is gastric and you may feed. If it is above 5.5, or no aspirate can be obtained, do not feed; reposition the tube, re-attempt aspiration once, and if the pH is still above 5.5 or aspirate is still absent, request a radiograph. Never proceed to feed on the external length, the aspirate volume, or the aspirate appearance alone. [1] [4]
Investigations
The first-line verification test is aspirate pH measured with a pH indicator strip. A reading of 5.5 or less is accepted as confirmation of gastric placement and is the bedside green light to feed. This threshold is the operational standard set by the United Kingdom patient-safety guidance and supported by the Metheny body of work and the paediatric NOVEL project, which found pH testing to be the most reliable bedside discriminator of gastric from respiratory placement. [1] [4] [7]
The second-line, confirmatory test is a radiograph. It is required when the pH is above 5.5, when no aspirate can be obtained, or whenever there is clinical doubt. The image must show the whole course of the tube, traced from the nose or mouth to the tip, with the tip below the diaphragm and lying over the stomach, and with no part of the tube in the airway or coiled in the oesophagus; a partial view that misses the tip is itself a common error. The radiograph is interpreted and the finding documented before any feed. [4] [8]
[1] [4] [2]The deprecated methods must be named and rejected. The whoosh or air-insufflation test, listening over the stomach with a stethoscope while pushing air in, was retired because it cannot reliably separate a gastric from a respiratory tube. The bubbling test, observing whether air bubbles appear when the tube end is held under water, is unsafe for the same reason and can expose staff to the child's secretions. Litmus and blue litmus paper are too coarse to read in the critical range around 5.5. Auscultation alone, palpation, and a reliance on the volume or appearance of the aspirate, are all unsupported. Using any of these as the sole confirmation is itself part of the Never Event. [3] [4] [9]
The limitation of pH testing matters on the ward. In a child on a proton-pump inhibitor or an H2 blocker, in the recently fed child, and when the tip has migrated into the duodenum, the gastric aspirate pH may read above 5.5 even though the tube is still in the gut. The correct response is not to abandon pH but to escalate: do not feed, and obtain a radiograph. Repeated high readings in a stable child on acid suppression should prompt a review of the verification strategy rather than a relaxation of the threshold. [4] [6]
Documentation closes the loop. Record the method used, the exact pH value, the radiograph and its interpretation if one was needed, the length of tube at the naris, and the date and time. This is what the next clinician inherits before the next feed, and it is the record that turns a safe system into an auditable one. [1] [2]
Management — Resuscitation
The first reaction when a tube is found in the respiratory tract is to stop and withdraw it. Stop any infusion, withdraw the tube, give oxygen, and assess and support the airway and breathing. Watch closely for a developing pneumothorax or pleural effusion, because the lung may have been injured by the tube or by feed already delivered; a child who becomes more breathless, more hypoxic, or who develops tracheal deviation and haemodynamic compromise after withdrawal may have a tension pneumothorax that needs immediate needle decompression. [9] [10]
When feed or medicine has already been given down a misplaced tube, recognise the event for what it is: a Never Event with the potential for serious harm. Stop the infusion. Escalate immediately to a senior clinician and to critical care. Image the chest with a radiograph, and treat the consequences, aspiration pneumonia, chemical pneumonitis, a pleural effusion or a pneumothorax, on their merits. The child is admitted, observed, and treated supportively or with respiratory support as needed, and the event is reported through the local incident system. [4] [9]
The response to a traumatic insertion in a neonate follows a different but equally urgent script. If the infant deteriorates during or just after a difficult insertion, with respiratory distress, drooling, subcutaneous emphysema or a pneumothorax, suspect a pharyngo-oesophageal perforation. Withdraw the tube. Do not re-pass it, because a second passage will enlarge the false passage. Escalate to neonatology and surgery, obtain a radiograph, start broad-spectrum antibiotics and supportive care, and arrange surgical review for a confirmed perforation. [11]
For every insertion in the high-risk child, the intubated, sedated or very young patient, airway and breathing protection runs alongside the procedure. Continuous pulse oximetry is the minimum, and a person trained to support the airway should be present. The reasoning is that the child most likely to suffer silent misplacement is the child least able to signal it, so the monitoring and the verifier are the only safety barriers that stand between the tube and the lung. [4] [5]
Management — Definitive and Stepwise
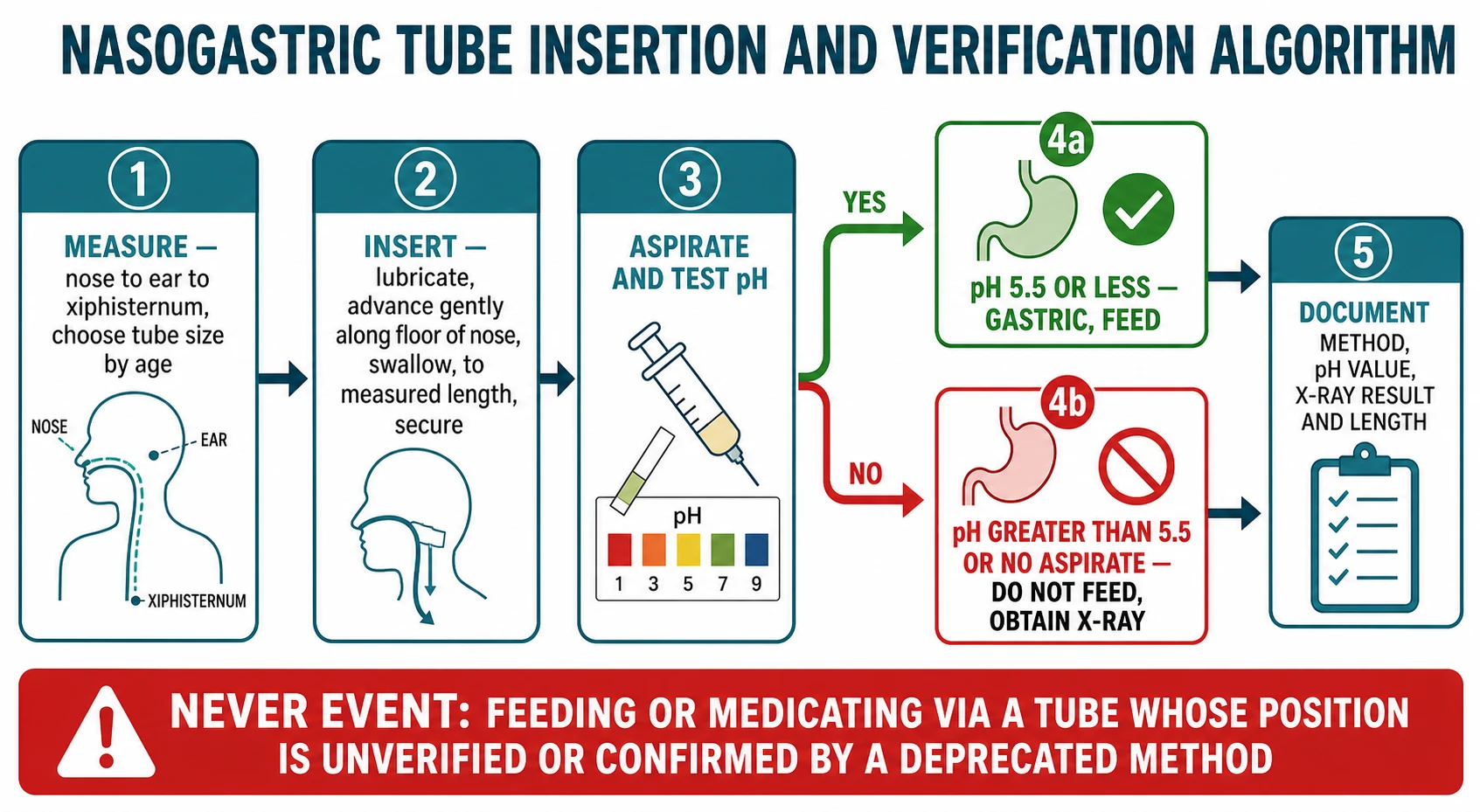
The definitive conduct of the procedure is a short, repeatable sequence that a candidate can say aloud at a viva. Prepare and explain the procedure to the child and family; confirm the indication and exclude the contraindications; position the child; measure the insertion length; choose the tube size; insert gently; secure; verify by pH; escalate to a radiograph if the pH is above 5.5 or no aspirate is obtained; document; and only then feed or medicate. The order is the point: verification always comes before the feed, never the other way around. [1] [8]
Adapt the technique to the age. In the neonate and young infant, consider the orogastric route, particularly in the very preterm or when the nares are blocked, because the nasal route can obstruct the obligate nose-breather and because the small pharynx is the site of perforation. Use a pacifier, a comfort hold, and non-nutritive sucking to settle the infant, and a trained assistant to hold the head and the hands. In the toddler and preschool child, explain in simple terms, use distraction, and accept that two people are usually needed. In the school-age child, the cooperative swallow makes passage smoother, and the child can be taught what to expect. [1] [2]
The re-verification rule is the single most important habit in long-term management. The position of the tube must be confirmed before every feed and before every medicine, and it must be re-checked after any event that could have moved it: retching, vomiting, a bout of coughing, retaping, transfer between wards or hospitals, and extubation. The reason is mechanical; a tube that has been vomited up and re-swallowed may now lie in the airway, and a tube that has been retaped may have migrated. A pH check takes seconds and is the barrier between a safe feed and a Never Event. [3] [9]
The insert-and-verify sequence
Prepare
Confirm indication and contraindications; explain; position; choose size and measure NEX length.
Insert
Lubricate; advance gently along the floor of the nose; encourage swallowing; stop at the measured length; secure.
Aspirate and test pH
Draw up aspirate; apply to a pH strip; read the exact value at the time the manufacturer states.
Decide
pH 5.5 or less means gastric and safe to feed; pH above 5.5 or no aspirate means do not feed and obtain a radiograph.
Document
Record the method, the pH value, the radiograph result if used, the length at the naris, and the date and time.
Ongoing tube care keeps the device safe and functional over days. Flush the tube with water before and after each feed and medicine to maintain patency, and use a larger flush to clear a blocked tube before resorting to replacement. Secure the tube with a loop that takes the strain off the naris, and inspect the nares and the skin daily for pressure injury, because a tight or malpositioned tube can erode the alar rim. Check the indication each day, so a tube that is no longer needed is removed rather than left in place to accumulate risk. [1] [2]
The criteria for removal are the mirror of the indications for insertion. Remove the tube when the child can swallow safely and is taking adequate oral intake, when the obstruction or ileus has resolved, when the lavage is complete, or when the medicine can be given another way. Plan the nutritional and medication transition with the dietitian and the pharmacist, and teach the family what to watch for after removal, particularly a return of poor intake or unsafe swallowing. [8] [1]
Specific Subtypes & Scenarios
The neonate and preterm infant deserve their own approach because the anatomy and the tissues are at their most fragile. In the very preterm or small neonate, an orogastric tube is often preferred over a nasogastric tube, both because the small nares can obstruct the obligate nose-breather and because the procedure is gentler by the oral route. A 5 to 8 French tube is typical. The specific danger at this age is traumatic perforation of the posterior pharynx or cricopharyngeal region, which can present as a pharyngeal perforation mistaken at first for oesophageal atresia, with sudden deterioration and a pneumothorax; the safe response is to withdraw, not to re-pass. [11] [5]
The intubated and sedated child in paediatric intensive care is the patient in whom misplacement is both commonest and hardest to detect, because the child cannot cough, splutter or complain. Here the verifier is the only safety barrier, and many units move more readily to radiographic confirmation, especially after repositioning or transfer. The lesson is that the more helpless the patient, the stricter the verification must be. [4] [2]
The child with a base-of-skull or significant mid-face injury is the scenario in which the route, not the verification, is the decision that matters. The nasal route is contraindicated, because a tube can pass through a fractured cribriform plate or sinus wall into the cranium. Use an orogastric tube, or another route to enteral access, and document the reason the nasal route was avoided. [1] [4]
The child on an acid-suppressing medicine is the scenario that tests the pH rule. A proton-pump inhibitor or an H2 blocker raises the gastric pH and increases the proportion of readings above 5.5, even when the tube is correctly placed. The correct response is to escalate to radiography rather than to feed on a high pH or to abandon pH testing; the rule bends toward more imaging, never toward a looser threshold. [4] [6]
The child needing gastric decompression for bowel obstruction uses a wide-bore tube and produces larger aspirate volumes, which can give false reassurance. The verification pathway is unchanged: confirm gastric position before draining, because a wide-bore tube misplaced in the pleural space and used to drain would cause the same catastrophe as a feeding tube. The bilious or obstructed child still needs a verified tube. [9] [1]
Complications & Pitfalls
The complications of misplacement are the severe end of the topic and the reason the safety system exists. Feed or medicine delivered into the bronchial tree causes aspiration pneumonia and chemical pneumonitis; delivery into the pleural space causes an effusion and pleuritic inflammation; and a tube that has punctured or irritated the lung can trigger a pneumothorax, occasionally a tension pneumothorax on withdrawal. These injuries have killed children, and each is preventable by a correct verification. [9] [10]
The complications of traumatic insertion cluster in the neonate and small infant. Pharyngo-oesophageal perforation can progress to mediastinitis; intracranial misplacement, in the child with a base-of-skull injury, can cause brain injury; and epistaxis and nasal trauma accompany forceful insertion. The unifying thread is force: a tube that meets resistance should be reconsidered, not pushed. [11] [1]
The complications of a correctly placed tube over time are the slower, quieter harms. Nasal pressure injury and alar erosion come from a tube secured under tension; sinusitis and otitis come from a tube that blocks sinus and eustachian drainage over days; a tube can block, migrate, or be pulled out; reflux and aspiration can still occur even with a gastric tube; and prolonged gastric drainage depletes electrolytes and fluid. Each is a reason to review daily whether the tube still needs to be there. [2] [8]
The recurring pitfalls are the human errors the safety system is built to catch. The first is treating an absent aspirate as proof of safety and feeding anyway. The second is accepting a single deprecated-method check, a whoosh, a bubble or an auscultation, and moving on. The third is failing to re-verify after the tube has moved, especially after retaping or transfer. The fourth is the documentation pitfall of recording "tube in situ" without the method, the pH value and the length, so the next clinician inherits a habit rather than a decision. [3] [9]
Prognosis & Disposition
A correctly inserted and verified tube does its job for the duration of the indication and is removed when that indication resolves. The expected outcome is safe enteral access for feeding, medicine or decompression, with the tube in place only as long as it is needed. The candidate should be able to state this plainly: the device is a temporary means to an end, and the end is the child swallowing safely again or the obstruction resolving. [1] [8]
After a Never Event, the disposition is senior and systems-level. The child is reviewed by a senior clinician, imaged, and admitted or escalated to critical care as the injury demands. The event is reported through the local incident-reporting system, disclosed to the family honestly and early, and used as the trigger for a review of the unit's verification process, the documentation, and the training. The clinical prognosis depends on the volume and the nature of what was infused and the speed of recognition. [9] [4]
For safe discharge or ward transfer with a tube in place, three conditions must be met: a verified position recorded in the notes, a clear plan for re-verification before each use, and, where the tube goes home, a carer who is trained and competent. A child sent home with a feeding tube needs written instructions, a contact for problems, and a planned review, because the safety system that protects the inpatient must be recreated in the home. [2] [1]
When nasogastric feeding is needed beyond the medium term, plan the transition to more definitive enteral access. A child with a severe neurodisability, a safe but long-term swallowing failure, or a gut that works but a mouth that cannot, is often better served by a gastrostomy, which removes the nasal trauma and the daily re-insertion risk; a child with aspiration despite gastric feeding may need a post-pyloric or jejunostomy route. The decision is made with the family, the dietitian and the surgeon. [1] [8]
Special Populations
The preterm and term neonate sits at the highest procedural risk and gets the most conservative approach. Prefer the orogastric route in the very small or nasal-obstructed infant, use a 5 to 8 French tube, and treat any resistance or deterioration during insertion as a possible perforation. The neonatal unit is also the setting in which the documentation and the re-verification habit must be most disciplined, because the patient cannot signal the error. [11] [5]
The child with cerebral palsy or a severe neurodisability often needs a feeding tube for the long term. The altered tone, the reflux, and the sometimes-poor cough raise both the aspiration and the misplacement risk, and the family lives with the device. This is the population for whom the eventual transition to a gastrostomy is most often the right answer, and the candidate should be able to discuss the timing and the trade-offs with the family. [1] [8]
The child with a developmental disability or autism may find repeated insertions distressing, and the procedure itself can become a source of trauma. Preparation, visual supports, distraction, comfort holding, and, where appropriate, the involvement of a sedation or child-life service, reduce the distress and the risk of a traumatic insertion. The plan should be individualised and agreed with the family and the child. [1] [2]
The child with a facial or skull injury has the nasal route contraindicated, and the orogastric route is the default until the injury is excluded or resolved. The decision is made on the mechanism and the examination, and it is documented so that every clinician who follows knows why the nasal route was avoided. [1] [4]
The child in out-of-home care or in a remote setting brings the safety system home or far from hospital. The carer, whether a foster carer, a parent or a remote-area nurse, must be trained in re-verification, in the warning signs of misplacement, and in when to seek help. The documentation and the safety-netting are the bridge between the inpatient system and the community setting. [2] [8]
Evidence, Guidelines & Regional Differences
The paediatric evidence base crystallised in the NOVEL project, a multi-professional effort that produced best-practice recommendations specifically for paediatric nasogastric tube placement and verification, and that underpins much of current North American and international practice. Its central message, that aspirate pH testing is the bedside standard and that the whoosh test and its cousins must be abandoned, is the spine of the modern rule. [1] [2]
The pH threshold itself rests on a body of work led by Metheny and colleagues over more than two decades. Their studies of feeding-tube aspirates established that pH is the most reliable bedside discriminator of gastric from respiratory placement, and that a cut-off around 5.5 best separates the two compartments while remaining usable in the real ward environment. Subsequent guideline reviews have consolidated pH testing at 5.5 or less as the accepted standard, with radiography as the confirmatory test when pH fails or is unobtainable. [6] [7] [4]
The patient-safety origin of the rule is British. A series of deaths and serious harms from feeding misplaced tubes led the National Patient Safety Agency, and later NHS England and NHS Improvement, to issue alerts and a resource set that retired the whoosh test, fixed aspirate pH at 5.5 or less as the bedside standard, and classified the misplacement of a naso- or orogastric tube as a Never Event when feed or medicine is given through an unverified tube or one verified by a deprecated method. This framework is the most operationally explicit in the world and is widely cited. [9] [4]
The Australasian practice guidance, from the Royal Children's Hospital Melbourne clinical practice guideline and equivalent state documents, sets the tube-size-by-age bands, the insertion-length measurement, and the verification pathway for children. These sit comfortably alongside the British standard on the pH cut-off and the deprecated-method list, with minor local differences in organisation and in consumables. The administration of medicines down enteral tubes follows the same verification discipline, with the choice of formulation guided by the local paediatric formulary. [1] [8]
The controversy, such as it is, concerns the accuracy of pH alone in the child on acid suppression, where the rate of readings above 5.5 rises and the reliance on radiography grows, and the residual error rate of any single bedside method. The response across regions is consistent: pH at 5.5 or less remains the bedside standard, radiography is the confirmatory test, and the two together, with disciplined documentation and re-verification, form the system that has driven down the harm. The current national guidance for each region should be checked for the exact wording of the cut-off and the deprecated-method list. [4] [9]
Exam Pearls
Aspirate pH of 5.5 or less is the accepted bedside confirmation of gastric position; a reading above 5.5, or no aspirate, means do not feed and obtain a radiograph. The whoosh test, the bubbling test, litmus and blue litmus paper, and auscultation used alone are deprecated, and using any of them as the sole check is part of the Never Event. Feeding or medicating through an unverified tube is itself a Never Event under the NHS framework. [1] [4] [9]
Tube size by age: a neonate takes 6 to 8 French, an infant 8 French, a small child 10 French, and an older child or adolescent 12 to 14 French, with fine-bore for feeding and wide-bore for decompression or lavage. Measure with the nose-to-ear-to-xiphisternum method, noting that NEX can underestimate in the infant. In a base-of-skull or significant mid-face injury, the nasal route is contraindicated and an orogastric tube is used. [1] [8]
Re-verify before every feed and every medicine, and after any event that could move the tube: retching, vomiting, coughing, retaping, transfer or extubation. In the neonate, prefer an orogastric tube and treat resistance or sudden deterioration as a possible pharyngo-oesophageal perforation, withdrawing rather than re-passing. Document the method, the exact pH value, the radiograph result if used, the length at the naris, and the date and time, so the next clinician inherits a decision and not a habit. [3] [11]
References
- [1]Irving SY, Rempel G, Lyman B Pediatric Nasogastric Tube Placement and Verification: Best Practice Recommendations From the NOVEL Project. Nutr Clin Pract, 2018.PMID 30187517
- [2]Northington L, Kemper C, Rempel G Evaluation of methods used to verify nasogastric feeding tube placement in hospitalized infants and children - A follow-up study. J Pediatr Nurs, 2022.PMID 34763985
- [3]Kisting MA, Korcal L, Schutte DL Lose the Whoosh: An Evidence-Based Project to Improve NG Tube Placement Verification in Infants and Children in the Hospital Setting. J Pediatr Nurs, 2019.PMID 30798144
- [4]Metheny NA, Krieger MM, Healey F A review of guidelines to distinguish between gastric and pulmonary placement of nasogastric tubes. Heart Lung, 2019.PMID 30665700
- [5]Metheny NA, Pawluszka A, Lulic M Testing Placement of Gastric Feeding Tubes in Infants. Am J Crit Care, 2017.PMID 29092869
- [6]Metheny NA, Stewart BJ, Smith L pH and concentration of bilirubin in feeding tube aspirates as predictors of tube placement. Nurs Res, 1999.PMID 10414681
- [7]Metheny N, Reed L, Wiersema L Effectiveness of pH measurements in predicting feeding tube placement: an update. Nurs Res, 1993.PMID 8247814
- [8]Society of Pediatric Nurses (SPN) Clinical Practice Committee, SPN Research Committee, Longo MA Best evidence: nasogastric tube placement verification. J Pediatr Nurs, 2011.PMID 21726788
- [9]Taylor SJ Feeding tube safety: National guidance ignores the 'elephant in the room'. Int J Risk Saf Med, 2025.PMID 39973429
- [10]Andresen EN, Frydland M, Usinger L Deadly pressure pneumothorax after withdrawal of misplaced feeding tube: a case report. J Med Case Rep, 2016.PMID 26846268
- [11]Knight RB, Webb DE, Coppola CP Pharyngeal perforation masquerading as esophageal atresia. J Pediatr Surg, 2009.PMID 19944236