Paeds · investigations-procedures-and-technology
Paediatric ultrasound and point-of-care ultrasound
Also known as Point-of-care ultrasound · POCUS · Bedside ultrasound · Lung ultrasound · Focused assessment with sonography in trauma · FAST scan · Paediatric sonography · Focus-assessed echocardiography
A fellowship approach to paediatric ultrasound and point-of-care ultrasound covering probe selection and the frequency-to-depth trade-off, the lung ultrasound artefact repertoire (A-lines, B-lines, lung sliding, the lung point, pleural effusion and consolidation), the BLUE protocol decision tree for acute respiratory failure, an eight-zone lung scan, the focused assessment with sonography in trauma (FAST) and its limited sensitivity in children, abdominal applications (intussusception target sign and pyloric stenosis measurement), ultrasound-guided vascular access and the EPIC trial, focus-assessed cardiac ultrasound in shock, neonatal lung ultrasound patterns, the no-ionising-radiation and ALARA acoustic safety principle, and image acquisition principles of depth, gain, focus and probe choice.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture an eight-month-old brought to the emergency department with grunting, recession, and a high fever. The team needs to know, in the next two minutes, whether this is a bacterial pneumonia that needs antibiotics and admission or a viral bronchiolitis that needs supportive care. A chest radiograph means a portable machine, a trip or a wait, and a dose of ionising radiation in an infant whose lifetime cancer risk is shaped by every scan. A lung ultrasound, performed at the bedside in under two minutes by the clinician already caring for the child, shows the subpleural consolidation and the dynamic air bronchograms of pneumonia without any radiation at all. That single contrast — fast, bedside, radiation-free, and answering the question in front of you — is the whole point of paediatric POCUS. [3] [4]
Three terms travel together and the candidate must separate them. Diagnostic ultrasound is the formal, comprehensive scan performed and reported by a sonographer or radiologist, usually in a radiology department. Point-of-care ultrasound (POCUS) is a focused, binary-question scan performed by the treating clinician at the bedside, in real time, to answer a specific clinical question and then immediately integrated into the child's management. Lung ultrasound, FAST, focus-assessed echocardiography and ultrasound-guided vascular access are all POCUS applications, not formal scans. The difference is intent and scope: the radiologist's scan documents everything; the clinician's POCUS answers one question and is discarded. [1]
The paediatric context changes every one of these applications. The child's small body brings the structures of interest closer to the probe, so a high-frequency linear probe gives exquisite resolution in a neonate where it would be useless in an adult. The thin chest wall and incomplete ossification of the ribs mean ultrasound traverses the paediatric thorax far better than the adult's, which is why lung ultrasound works so well in children. The absence of ionising radiation matters more across a lifetime that has barely begun, and the Image Gently and ALARA principles take on their full force in the smallest patients. [1] [12]
Classification
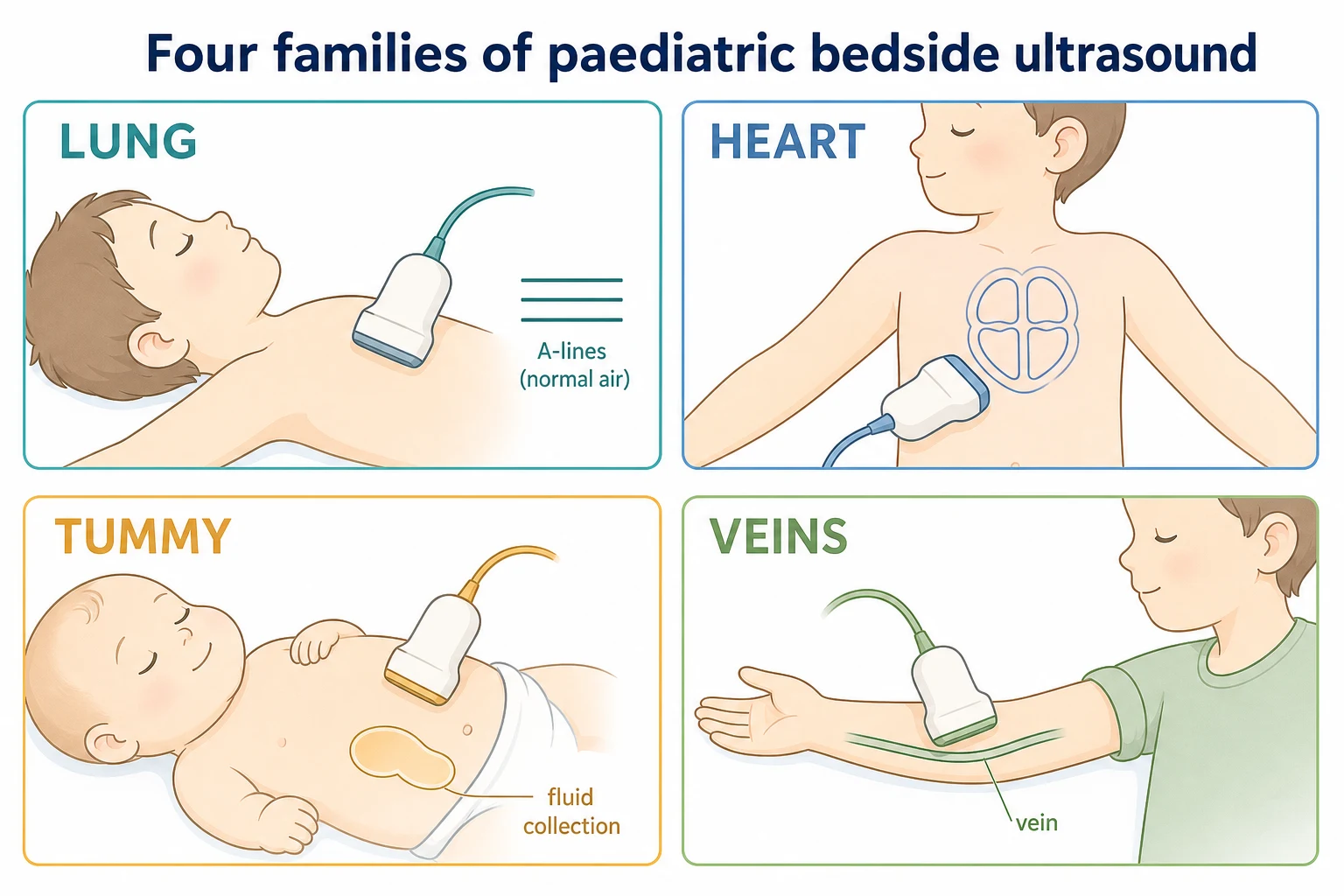
A clinician should classify paediatric POCUS by the body system scanned and by the question asked, because the probe, the protocol, and the artefact vocabulary all follow from those two choices. By system, four families cover almost all paediatric practice, and each carries its own probe, its own windows, and its own diagnostic signs. [1]
The thoracic or lung POCUS family scans the pleura and the lung through the intercostal spaces with a high-frequency linear probe in the small child and a curvilinear or phased array probe in the older child, reading A-lines, B-lines, lung sliding, the lung point, and consolidation. The abdominal and trauma POCUS family uses a curvilinear probe to scan the four FAST windows in trauma and the upper abdomen for the intussusception target sign, the pyloric muscle, and the appendicitis target. The cardiac POCUS family uses a phased array or small curvilinear probe in the subxiphoid, parasternal, and apical windows to answer four focused questions — left ventricular function, right ventricular size, pericardial effusion, and volume status from the inferior vena cava. The vascular and procedural POCUS family uses a high-frequency linear probe to guide peripheral and central cannulation, to confirm luminal aspiration, and to mark structures such as the longitudinal ligament before a lumbar puncture. [1] [11]
By question, every POCUS scan is either diagnostic (is there a pneumothorax, is there free fluid, is there a consolidation) or procedural (guide this needle into the vessel, mark this safe space). The diagnostic scan answers a binary question and is interpreted immediately; the procedural scan provides real-time visual guidance. A few applications are monitoring, such as serial lung ultrasound in a neonate evolving transient tachypnoea of the newborn into respiratory distress syndrome, or repeat FAST during observation of a stable traumatised child. The candidate who can name the family, the probe, and the question before picking up the transducer will read every scan correctly. [1] [12]
Epidemiology & Risk Factors
The adoption of paediatric POCUS is one of the fastest shifts in modern practice, driven by three forces that the candidate should be able to name. The first is the radiation-aware movement: children are ten times more radiosensitive than adults per unit dose, and every computed tomography scan of the chest carries a measurable lifetime excess cancer risk, so replacing ionising imaging with ultrasound wherever the evidence allows is a population-level duty. The second is the accuracy evidence: lung ultrasound now matches or exceeds the chest radiograph for community-acquired pneumonia in children, and ultrasound is the first-line test for intussusception, pyloric stenosis, and hip effusion. The third is workforce and technology: portable, laptop-sized machines have put a capable scanner into the hands of emergency, ward, neonatal, and retrieval clinicians. [1] [4]
The clinical epidemiology frames where POCUS changes outcome. Community-acquired pneumonia is among the commonest reasons a child is admitted to hospital, and a 2024 systematic review and meta-analysis found lung ultrasound as accurate as, or more accurate than, the chest radiograph for its diagnosis in children, with the added benefit of no radiation. Intussusception, most often ileocolic and peaking between three months and three years, is diagnosed by ultrasound with a sensitivity above 95 per cent, making ultrasound the definitive first-line test and contrast enema the therapeutic reduction. Hypertrophic pyloric stenosis presents at three to six weeks with projectile vomiting, and ultrasound measures the hypertrophied muscle directly, avoiding the upper gastrointestinal series in most infants. [4] [8] [9]
Trauma is the epidemiological setting where the FAST scan is most examined and most often misread. Blunt abdominal trauma in children injures solid organs — the liver and the spleen — that frequently bleed into their own parenchyma rather than into the peritoneal cavity, so the free intraperitoneal fluid that the FAST detects is often absent even in a significant injury. A systematic review and meta-analysis of the FAST in paediatric blunt abdominal trauma confirmed its high specificity but low and variable sensitivity, which is the single most important number a candidate must carry: a positive FAST in an unstable child drives laparotomy, but a negative FAST changes nothing and never clears the child. [7]
Lung — pneumonia or bronchiolitis
High-frequency linear probe
- Reads A-lines, B-lines, lung sliding, consolidation
- Matches or beats chest radiograph for paediatric pneumonia
- No ionising radiation — repeatable in an infant
- Dynamic air bronchograms distinguish consolidation from effusion
FAST — blunt abdominal trauma
Curvilinear probe, four windows
- High specificity, low sensitivity in children
- Solid organ bleeds into parenchyma, not the peritoneum
- Positive and unstable: to theatre; negative: observe or CT
- Never use a negative FAST to discharge a child
Abdominal — intussusception or pylorus
Curvilinear probe
- Target or donut sign of intussusception, sensitivity over 95 per cent
- Pyloric muscle thickness and channel length for stenosis
- Ultrasound is the first-line test for both
- Reduces the need for contrast studies and radiation
Vascular — difficult access
High-frequency linear probe
- Ultrasound guidance improves first-attempt success
- EPIC trial confirmed superiority for difficult PIVC
- Transverse and longitudinal views to confirm the lumen
- Sterile technique and securement still mandatory
Pathophysiology
To read a lung ultrasound image the candidate must understand that almost everything seen is an artefact, because ultrasound cannot penetrate air. The pleura is the only real structure the beam meets, and it is a bright horizontal line between two rib shadows. Everything below that line — the repeating horizontal A-lines, the vertical comet-tail B-lines, the swinging shimmer of lung sliding — is the lung's air and water content translated into recurring acoustic patterns. Master those patterns and the lung becomes the most transparent organ at the bedside. [3]
The physics generates two fundamental artefacts. A-lines are horizontal, equally spaced bright lines that repeat below the pleural line at the same interval as the skin-to-pleura distance; they are a reverberation artefact produced when a dry, air-filled lung reflects the beam back and forth. B-lines are vertical, well-defined comet-tail or ring-down streaks that arise from the pleural line, spread to the bottom of the screen without fading, and move with lung sliding; they are generated when the interlobular septa are thickened or fluid-filled, so each B-line marks a wet acoustic interface. A normal lung shows A-lines with sliding; a lung with three or more B-lines in a single intercostal space has alveolar-interstitial syndrome — pulmonary oedema, interstitial pneumonia, or bronchiolitis — and the candidate must read the pattern bilaterally and in context. [2] [3]
Lung sliding is the to-and-fro shimmering of the two pleural layers against each other during respiration, and its presence at a point rules out a pneumothorax at that point. Its absence is non-specific — apnoea, mainstem intubation, pleural adhesions, a consolidating pneumonia, and the supine neonate can all abolish sliding — so the discriminating sign is the lung point, the precise boundary on the chest wall where sliding lung meets the still, non-sliding air of a pneumothorax. The lung point is highly specific for pneumothorax but is only seen when the pneumothorax is partial and locatable; a complete or tension pneumothorax shows only absent sliding across the whole hemithorax, and tension remains a clinical diagnosis to be decompressed before any scan. [3]
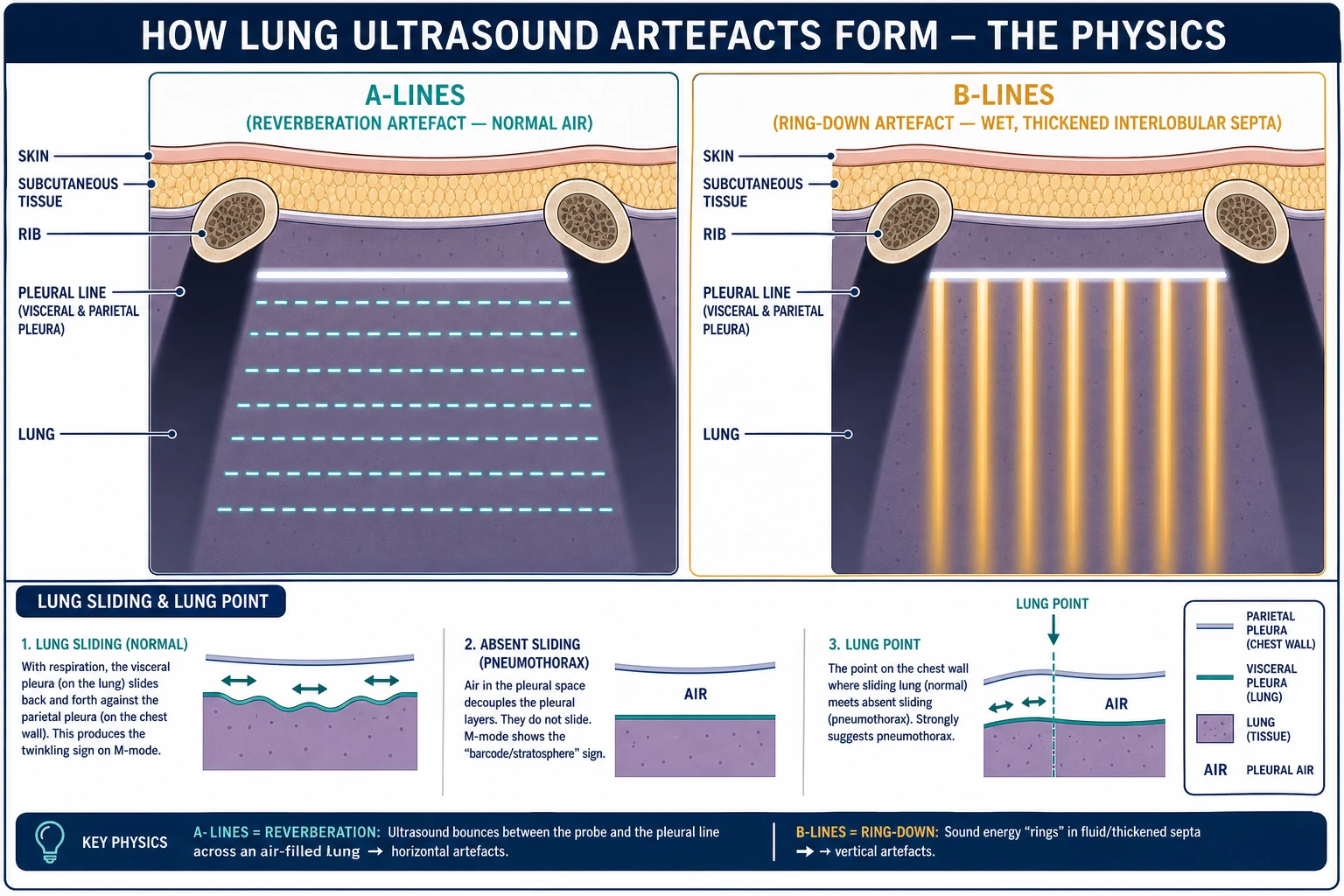
Two further signs complete the repertoire. A pleural effusion appears as an anechoic or echoic collection between the chest wall and the lung, bounded above by the lung line and showing the quad sign (four borders) and the sinusoid sign (the lung line swinging toward the probe on inspiration as the collapsing lung floats in the fluid). A consolidation appears as a tissue-like, hypoechoic wedge resembling liver (hepatisation) that reaches the pleura, often threaded with bright dynamic air bronchograms that move with respiration and distinguish live, ventilated consolidation from a static effusion or atelectasis. The BLUE protocol weaves all of these signs into a decision tree that points to pulmonary oedema, pneumonia, pneumothorax, asthma or chronic obstructive disease, pulmonary embolism, or pleural effusion as the cause of acute respiratory failure. [2] [3]
Clinical Presentation
The child who benefits from POCUS is recognised by the question the bedside scan can answer in real time, and four presentations recur in fellowship vivas. The candidate should be able to narrate each and to name the sign the scan is looking for. [1]
The first is the child in acute respiratory failure. The infant or child with grunting, recession, hypoxia, and respiratory distress needs the cause identified fast, and lung ultrasound at eight zones distinguishes a bilateral B-line pattern of pulmonary oedema from a focal consolidation of pneumonia from the absent sliding of a pneumothorax from the quad sign of a pleural effusion — all without moving the child or exposing the infant to radiation. The BLUE protocol was built for exactly this bedside moment. [2]
The second is the blunt-trauma victim. The child who has fallen from a height, been struck by a vehicle, or suffered an abdominal injury needs the primary survey completed and the FAST performed in parallel. A positive FAST with free fluid in Morison's pouch in a haemodynamically unstable child is the trigger for surgical or retrieval activation, not for more imaging. A negative FAST changes nothing, because the child's solid organs bleed into themselves. [7]
The third is the child with an acute surgical abdomen. The six-month-old with intermittent colicky screaming and red-currant-jelly stool needs the intussusception target sign; the four-week-old with projectile vomiting needs the pyloric muscle measured; the older child with right-lower-quadrant pain may have the non-compressible appendix or the target sign of appendicitis identified at the bedside, with ultrasound the first-line test for each. [8] [9]
The fourth is the child in shock or with difficult vascular access. A focus-assessed echocardiogram answers whether the left ventricle is hyperdynamic and empty, dilated and poor, or encircled by a pericardial effusion; the inferior vena cava is read for volume status; and when the peripheral veins are invisible in a dehydrated or pigmented child, ultrasound-guided cannulation converts a failed, traumatic attempt into a first-time success. [10] [11]
Differential Diagnosis
There is no differential diagnosis of the procedure itself, but there are three differential lists that an examiner will press, and each maps a POCUS sign to its pitfalls. [3]
The differential of absent lung sliding is the one most often mangled. Pneumothorax is the feared cause, but apnoea in the intubated or paralysed child, a mainstem bronchial intubation ventilating only one lung, prior pleurodesis or pleural adhesions, a large pleural effusion, an apical pneumonia, and the supine neonate with little diaphragmatic excursion can all abolish sliding. The lung point, when found, is highly specific; when it cannot be found in a child with a complete or tension pneumothorax, the absence of sliding alone must never override the clinical picture. [3]
The differential of B-lines is equally broad. Three or more B-lines in an intercostal space signal a wet lung, but the wetness may be cardiogenic pulmonary oedema, a non-cardiogenic acute respiratory distress syndrome, an interstitial viral pneumonia, bronchiolitis, or pulmonary fibrosis. The bilateral, symmetrical, dependent distribution points to oedema; a focal, asymmetrical distribution points to pneumonia. B-lines alone are never diagnostic; the candidate reads them with the history, the oxygenation, and the cardiac POCUS. [2] [3]
The differential of a negative FAST in abdominal trauma is the most clinically dangerous. Free intraperitoneal fluid may be absent because the solid organ is bleeding into its own capsule (a splenic or hepatic laceration contained or slowly leaking), because the injury is to a hollow viscus or the mesentery that bleeds little but perforates, or because the child is in the early phase before enough fluid has accumulated. A negative FAST in an unstable or high-mechanism child therefore mandates ongoing resuscitation, serial examination, and computed tomography or surgical review — never reassurance. [7]
Clinical & Bedside Assessment
The bedside assessment has two halves: machine set-up and probe selection, and a systematic scanning protocol run the same way every time. Both are procedural skills, and the candidate who can name the probe and the windows will read the signs correctly. [1]
Probe selection follows one rule — match the frequency to the depth of the target. A high-frequency linear probe (5 to 15 megahertz) gives superb resolution in the first few centimetres and is the probe of choice for lung ultrasound in the small child, for vascular access, for the testis, and for superficial soft tissue, at the cost of poor penetration into deep structures. A curvilinear probe (3 to 8 megahertz) penetrates more deeply at lower resolution and is the workhorse for the abdomen, the FAST, and the older child's chest. A phased array probe (1 to 5 megahertz) fits between the ribs and is preferred for cardiac POCUS. The frequency-to-depth trade-off is the single physics fact the examiner tests: higher frequency buys resolution but loses depth, and the child's small body is precisely where the highest frequencies become usable. [1]
Once the probe is chosen, four image-quality controls govern every scan and the candidate must name them. Depth is set so the target fills the screen — too shallow misses the deep collection, too deep wastes resolution on a tiny structure. Gain adjusts the brightness; too much gain creates false echoes, too little hides real fluid. Focus is placed at the depth of the target to sharpen it. And the probe orientation follows the convention that the marker on the probe corresponds to the upper-left of the screen, so the operator always knows left from right, head from foot. These four controls, set before the scan, separate a diagnostic image from an artefact. [1]
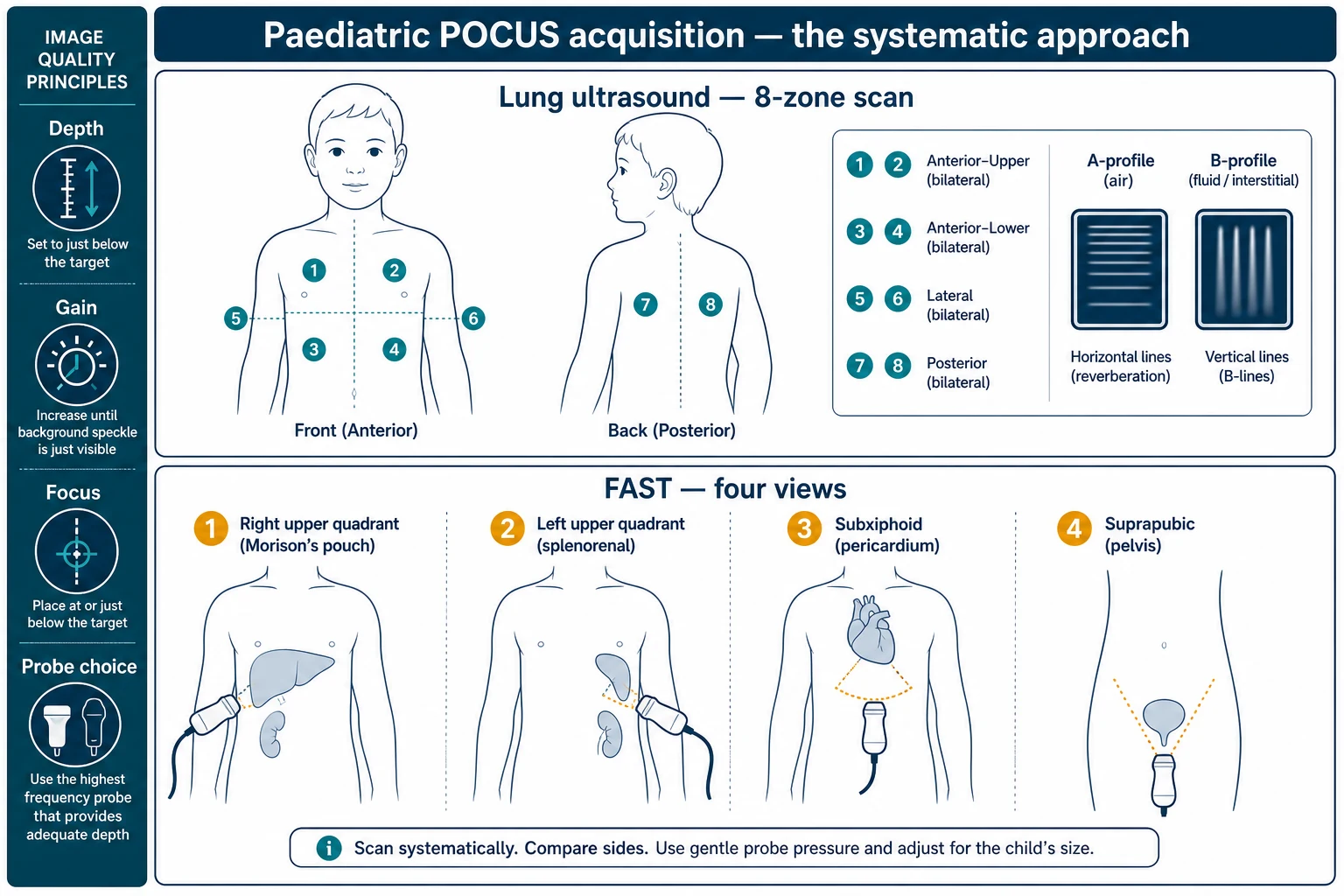
For lung ultrasound, the systematic protocol is the eight-zone scan. Each hemithorax is divided into four zones by the anterior and posterior axillary lines and by a horizontal line at the nipple — anterior-upper, anterior-lower, lateral and posterior — and both sides are scanned, giving eight zones in total. The probe sits perpendicular to the ribs in the intercostal space, the pleural line is identified between the rib shadows, and each zone is read for A-lines, B-lines, sliding, consolidation, and effusion. The BLUE protocol then interprets the pattern. For the FAST, the four windows are scanned in order — the right upper quadrant and Morison's pouch, the left upper quadrant and the splenorenal recess, the subxiphoid pericardial window, and the suprapubic pelvis — looking for anechoic free fluid that collects in the most dependent spaces. [2] [3] [7]
FAST windows and the lung artefact rule
Investigations
Point-of-care ultrasound is itself an investigation, and the candidate must understand how it relates to the formal imaging it sometimes replaces and sometimes augments. The principle is that POCUS answers a focused binary question at the bedside, while formal imaging documents anatomy comprehensively and is reported by a radiologist. [1]
For lung ultrasound, the evidence now supports it as equivalent or superior to the chest radiograph for community-acquired pneumonia in children. A 2024 systematic review and meta-analysis comparing lung ultrasound and chest radiography for paediatric community-acquired pneumonia found lung ultrasound highly accurate and free of ionising radiation, and a 2017 review and a 2019 meta-analysis of novice versus advanced sonographers showed that the accuracy is preserved even when the scan is performed by trained non-experts. Lung ultrasound is therefore increasingly the first-line chest imaging in the acutely wheezy or febrile child, with the chest radiograph reserved for equivocal cases, for suspected complications such as effusion or empyema, and for the child who is not responding as expected. [4] [5] [6]
For abdominal POCUS, ultrasound is the definitive first-line investigation for intussusception, with a sensitivity above 95 per cent for the target or donut sign, and ultrasound has replaced the diagnostic contrast enema, which is now reserved for therapeutic pneumatic or hydrostatic reduction. For hypertrophic pyloric stenosis, ultrasound measures the pyloric muscle thickness and channel length directly and avoids the upper gastrointestinal series in most infants, although the conventional cut-off values are under active revision. [8] [9]
For trauma, the FAST is an adjunctive triage investigation, not a definitive one. Its role is to detect free intraperitoneal fluid rapidly in the unstable child and to drive the decision for laparotomy or retrieval; in the stable child, computed tomography with intravenous contrast remains the reference standard for grading solid organ injury and excluding hollow viscus injury. The candidate must hold these roles apart: the FAST is for the unstable child in the resuscitation bay, and computed tomography is for the stable child who can be imaged safely. [7]
For cardiac and vascular POCUS, the focus-assessed echocardiogram is a screening investigation that flags a grossly abnormal left ventricle, an enlarged right ventricle, a pericardial effusion, or a collapsed or distended inferior vena cava; the formal echocardiogram remains the comprehensive study reported by cardiology. Ultrasound-guided peripheral and central cannulation is a procedural investigation that confirms vessel patency and luminal placement before the catheter is secured. [10] [11]
Management — Resuscitation
In resuscitation, POCUS is folded into the primary survey, never run ahead of it. The child who is airway-compromised, breathing inadequately, or in circulatory collapse is managed by the airway-breathing-circulation sequence first, and the probe is brought to the bedside to answer the focused question that remains. [1]
In the shocked child, the focus-assessed echocardiogram and the inferior vena cava read refine the physiology in real time. A hyperdynamic, empty-looking left ventricle with a small, collapsible inferior vena cava supports hypovolaemia and a fluid challenge; a dilated, poorly contracting ventricle with a full inferior vena cava supports cardiogenic shock and argues against further fluid; a pericardial effusion with right-heart compression identifies tamponade and the need for drainage; and an enlarged right ventricle raises pulmonary embolism or right-heart strain. The scan narrows a long differential into a working diagnosis within minutes. [11]
In the traumatised child, the FAST is performed during the circulation step of the primary survey. A positive FAST with free fluid in an unstable child is the indication for urgent surgical or retrieval intervention, and the scan is not repeated or refined; the child goes to theatre or to the retrieval team. A negative FAST in an unstable or high-mechanism child does not exclude injury and the resuscitation continues — two large-bore cannulae, fluid or blood boluses, and ongoing reassessment, with computed tomography or surgical review once the child is stabilised. The candidate must never allow a reassuring FAST to pause the resuscitation of an unstable child. [7]
In the child in respiratory failure, the lung ultrasound refines the cause while high-flow oxygen and respiratory support are established. A bilateral B-line pattern redirects the team toward pulmonary oedema; a focal consolidation confirms pneumonia and prompts antibiotics; absent sliding with a lung point confirms a partial pneumothorax, while a tension pneumothorax is decompressed on clinical grounds before the probe is applied. The eight-zone scan is quick enough to run during the first few minutes of resuscitation. [2] [3]
Ultrasound coupling gel (for bedside scanning)
Dose
A sufficient layer to eliminate air contact between the probe face and the skin; warmed gel is preferred in the neonate and infant to reduce cold stress
Management — Definitive & Stepwise
Once the resuscitation question is answered, the definitive POCUS examination is a sequence of focused scans run in a protocolised order. The candidate should be able to describe each protocol step by step, because the structure is what makes an operator-dependent scan reproducible. [1]
A systematic bedside POCUS examination, in order
1 · State the clinical question
Name the single binary question the scan will answer — is there a pneumothorax, is there free fluid, is the ventricle contracting, is the vessel patent. A scan without a stated question produces an image without an interpretation.
2 · Choose the probe and the preset
High-frequency linear for superficial lung and vessels, curvilinear for the abdomen and FAST, phased array for the heart. Select the machine preset so depth, gain and focus start appropriate to the target.
3 · Prepare the child and the gel
Position the child for the window, warm the gel for the neonate and infant, and apply enough gel to exclude air. Use distraction and a calm explanation; a settled child gives a better image.
4 · Optimise the image
Set depth so the target fills the screen, adjust gain so fluid is black and tissue is grey, and place the focus at the target depth. Confirm the probe marker orientation before interpreting.
5 · Run the protocol systematically
Eight zones for lung, four windows for FAST, the four cardiac questions for the focus-assessed echo, or the transverse and longitudinal views for the vessel. Scan every window every time, in the same order.
6 · Interpret the artefact or sign
Read A-lines, B-lines, sliding and the lung point for lung; anechoic fluid in a dependent space for FAST; ventricular size and function and pericardial fluid for the heart; the target sign or pyloric measurement for the abdomen.
7 · Integrate the answer into management
Place the finding into the clinical picture — a positive FAST in the unstable child drives surgery, a focal consolidation drives antibiotics, a target sign drives enema reduction. State the next step out loud.
8 · Document, save and escalate
Save representative stills and clips, document the finding and its limitation in the record, and escalate to formal imaging, radiology, or cardiology when the scan is equivocal or outwith the operator's credentialed scope.
The technique points that separate a diagnostic scan from a misleading one are few and worth memorising. Always exclude air with adequate gel, because even a thin air layer reflects the beam and creates a black, unreadable image. Always read the artefact, not the machine's guess — there is no automated pneumonia detector, and the operator's eye is the interpretive engine. Always scan the contralateral side as an internal control, because asymmetry (one lung sliding, the other still) is often more informative than any single image. Always treat a negative scan with humility in the high-stakes child, because the FAST misses contained solid-organ bleeding and a normal lung scan does not exclude a small central lesion. [3] [7]
| Application | Probe | Frequency | What it reads |
|---|---|---|---|
| Lung (small child) | Linear | 5 to 15 MHz | A-lines, B-lines, sliding, lung point, consolidation |
| Lung (older child) or FAST | Curvilinear | 3 to 8 MHz | Pleura and effusion at depth; free fluid in dependent spaces |
| Cardiac POCUS | Phased array | 1 to 5 MHz | Ventricular size and function, pericardial effusion, IVC |
| Vascular access | Linear (hockey-stick in neonate) | 5 to 15 MHz | Vessel in transverse and longitudinal, patency, needle tip |
| Abdominal (intussusception, pylorus) | Curvilinear | 3 to 8 MHz | Target sign, pyloric muscle thickness and channel length |
[1] [11] Probe frequencies are guides; select the highest frequency that still reaches the depth of the target, and confirm against the current ACEP, AIUM and ESPNIC guidance.
Specific Subtypes & Scenarios
Four scenarios recur in fellowship vivas and OSCE stations, and each carries a specific sign and a specific trap. The first is lung ultrasound for community-acquired pneumonia. The febrile, tachypnoeic child is scanned at eight zones; a subpleural hypoechoic consolidation with dynamic air bronchograms, often with adjacent B-lines, confirms pneumonia. The 2024 meta-analysis found lung ultrasound as accurate as the chest radiograph and free of radiation, and the 2019 novice-versus-advanced review showed trained non-experts retain that accuracy. The trap is over-calling B-lines from a poor gel layer or probe angle — re-scan with good contact before declaring alveolar-interstitial syndrome. [4] [5] [6]
The second is the FAST in paediatric blunt abdominal trauma. The four windows are scanned in the resuscitation bay during the primary survey. A positive FAST with free fluid in an unstable child drives laparotomy or urgent retrieval; a negative FAST changes nothing because the child's liver and spleen bleed into their own parenchyma, and the systematic review confirms a low, variable sensitivity in children. The candidate must state, unprompted, that a negative FAST never excludes injury and that the scan is for the unstable child, with computed tomography reserved for the stable child. [7]
The third is intussusception and hypertrophic pyloric stenosis. The infant with colicky screaming and red-currant-jelly stool shows the target or donut sign — concentric rings of oedematous bowel wall in the transverse view and the pseudokidney sign in the longitudinal view — with a sensitivity above 95 per cent, making ultrasound the definitive first-line test. The four-week-old with projectile vomiting shows a thickened pyloric muscle and a lengthened channel; the conventional cut-offs of a muscle wall thickness of 3 to 4 millimetres and a channel length of 15 to 17 millimetres sit at the boundary in small infants, and an Australasian consensus argues the criteria should be revised for contemporary infant size. [8] [9]
The fourth is ultrasound-guided vascular access and cardiac POCUS. In the child with difficult veins, a high-frequency linear probe identifies a patent vessel, confirms it is non-pulsatile and compressible, and guides the needle in real time in either an in-plane or out-of-plane approach; the EPIC superiority trial confirmed higher first-attempt success with ultrasound guidance for difficult peripheral cannulation, and the cardiac point-of-care scan in the shocked child distinguishes hypovolaemic, cardiogenic, and obstructive causes in minutes. [10] [11]
[1] [7]Complications & Pitfalls
Complications of paediatric POCUS fall into two families: the misinterpretation of the image and the misuse of the scan in the decision, and it is the second family that harms children. The candidate should be able to name the common pitfalls in each. [1]
The cardinal pitfall is over-reliance on a negative scan in a high-stakes child. A negative FAST in an unstable or high-mechanism traumatised child does not exclude solid organ injury; a lung scan with no B-lines does not exclude a small central pneumonia or an early effusion; a normal-looking cardiac scan does not exclude a low-output state. The remedy is to treat every POCUS answer as one piece of evidence, to integrate it with the clinical picture, and to escalate to formal imaging or senior review whenever the scan and the child disagree. [7]
The second pitfall is confusing artefact for pathology. B-lines generated by a poor gel layer or an oblique probe angle disappear with good contact; a reverberation artefact can masquerade as a lung point; a mirror-image artefact near the diaphragm can create a false impression of liver or spleen; and an anechoic bowel loop can be mistaken for free fluid on the FAST. The remedies are adequate gel, a perpendicular probe, scanning the contralateral side as a control, and rescanning the window in two planes before declaring a finding. [3]
The third pitfall is operator overconfidence. Point-of-care ultrasound is operator-dependent, and an untrained operator can both over-call artefact as disease and under-call real disease. The remedy is structured training, logged scans, image review with a mentor, and credentialing against a defined scope of practice; a survey of paediatric emergency departments found wide variability in POCUS credentialing, which is exactly why the scope of each operator matters. [1]
The procedural complications of ultrasound-guided vascular access — arterial cannulation, extravasation, haematoma, catheter dislodgement, and infection — are prevented by confirming the vessel is non-pulsatile and compressible in transverse, by visualising the needle tip throughout, and by maintaining sterile technique, secure fixation, and a post-procedure check. The acoustic-output considerations — thermal and mechanical index kept low and scan time minimised, especially in the neonate — are the ultrasound equivalent of the ALARA principle and complete the safety picture. [1] [10]
Prognosis & Disposition
The disposition of a child after a POCUS scan is driven by the clinical question the scan answered and by the limitations of that answer, and the candidate must always state both. A scan that answers the question confidently directs the child along a clear path; a scan that is equivocal or outwith the operator's scope escalates to formal imaging or specialist review. [1]
After a lung ultrasound for pneumonia, the child with a clear consolidation is treated with antibiotics and admitted or observed according to severity, and the radiation-free nature of the scan means it can be repeated to track resolution without cumulative dose. After a FAST in trauma, the disposition follows the physiology: the unstable child with a positive FAST goes to theatre or retrieval, the stable child with a negative FAST is observed with serial examination or proceeds to computed tomography, and the stable child with a positive FAST proceeds to computed tomography to grade the injury and guide non-operative management. [4] [7]
After an abdominal POCUS for intussusception, the finding of a target sign prompts urgent radiology-led pneumatic or hydrostatic reduction, with the surgical team standing by for failed reduction or perforation. After a pyloric measurement that confirms stenosis, the infant is resuscitated with fluids and electrolytes, the hypochloraemic hypokalaemic metabolic alkalosis is corrected, and surgery follows once stable — the operation is never an emergency, the resuscitation is. After ultrasound-guided vascular access, the catheter is secured, its function is confirmed, and the child is monitored for dislodgement, extravasation, and infection as for any line. [8] [9]
The prognosis of the underlying illness, not the scan, governs outcome, and the role of POCUS is to shorten the time to the right management. A child whose pneumonia is confirmed at the bedside receives antibiotics minutes earlier; a child whose intussusception is confirmed without a contrast study reaches reduction sooner; a child whose shock is deconstructed into a working diagnosis in minutes receives the right fluid or inotrope sooner. That time saved is the measurable benefit of bedside ultrasound. [1] [11]
Special Populations
The neonate is the population in whom lung ultrasound has advanced furthest, and the candidate should know the neonatal patterns. A point-of-care lung ultrasound in the neonate distinguishes transient tachypnoea of the newborn (a predominantly A-line pattern with rare B-lines and pleural effusion, the double lung point), respiratory distress syndrome (a diffuse, coalescent B-line or white-lung pattern with absent sliding in severe disease), meconium aspiration (coarse, patchy B-lines and consolidation), and pneumothorax (absent sliding and a lung point), all without moving the fragile infant to a radiograph. The neonatal lung ultrasound classification separates descriptive applications (naming the pattern) from functional applications (estimating lung aeration and monitoring response to surfactant or diuretics). [12]
The critically ill child in the paediatric intensive care unit benefits from cardiac POCUS that integrates into daily practice — assessing ventricular function and volume status, detecting pericardial effusion and tamponade, and guiding procedures such as central line placement and pericardiocentesis. The ESPNIC international guidelines define the scope, training, and quality assurance of POCUS in these settings, and a practical integration framework describes how the cardiac scan answers focused questions at the bedside without replacing the formal echocardiogram. [1] [11]
The child in the rural or retrieval setting is the population in whom POCUS is an equity tool as much as a clinical one. The rural clinician who can perform a lung ultrasound, a FAST, and a cardiac scan in a remote health centre or in a retrieval vehicle brings tertiary-level decision-making to the child hours from a computed tomography scanner. For Aboriginal, Torres Strait Islander, Māori, and migrant and refugee children, and children in remote communities, who often present late with advanced disease, the bedside scan that confirms a consolidation, a free-fluid collection, or a poor ventricle in minutes converts a delayed retrieval into a targeted one. [1]
The child with a complex chronic illness or a technology dependence, such as a home-ventilated child or a child with a cardiac lesion, benefits from serial POCUS that tracks familiar problems — a pleural effusion, a worsening ventricle, a dehydration-related vessel collapse — across encounters, and from procedural POCUS that preserves difficult veins and avoids repeated landmark cannulation. For these children, who accumulate radiation and procedure-related harm over a lifetime, the radiation-free, repeatable, guidance-capable nature of ultrasound is a cumulative benefit. [1] [11]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric POCUS has matured rapidly, and the candidate should know the landmark studies in each application. On lung ultrasound, Lichtenstein's BLUE protocol built the decision tree for acute respiratory failure from the artefact repertoire, and his synthesis of lung ultrasound in the critically ill codified the ten basic signs; the paediatric evidence now shows lung ultrasound matching or exceeding the chest radiograph for community-acquired pneumonia, with a 2024 meta-analysis confirming equivalence or superiority and a 2019 meta-analysis confirming that trained novices retain the accuracy. [2] [3] [4] [6]
On trauma, the systematic review and meta-analysis of the FAST in paediatric blunt abdominal trauma is the definitive evidence of its high specificity and low sensitivity in children, and it underpins the universal teaching that a positive FAST in an unstable child drives intervention while a negative FAST changes nothing. On abdominal emergencies, the meta-analysis of ultrasound for intussusception confirms a sensitivity above 95 per cent for the target sign, and the Australasian consensus on pyloric stenosis measurement argues that the conventional muscle-thickness and channel-length cut-offs should be revised for contemporary infant size. [7] [8] [9]
On procedures and critical care, the EPIC superiority randomised trial established higher first-attempt success for ultrasound-guided peripheral cannulation in difficult access, and the practical integration of cardiac point-of-care ultrasound in the paediatric and neonatal intensive care settings describes how the focused scan answers four questions at the bedside. The ESPNIC international evidence-based guidelines define the scope, training, quality assurance, and governance of POCUS for critically ill neonates and children and are the clearest statement of how a service should embed POCUS safely. [1] [10] [11]
The regional differences are narrow and the principles are concordant. The American College of Emergency Physicians and the American Institute of Ultrasound in Medicine define scope and credentialing in North America; the Royal Children's Hospital Melbourne clinical practice guidelines and the college curricula embed POCUS in Australasia; the Royal College of Paediatrics and Child Health and the Imaging Wisely programmes drive radiation-aware practice in the United Kingdom; and the Canadian Association of Emergency Physicians and the Royal College of Physicians and Surgeons of Canada include POCUS as a competency. The genuine debates are about training and credentialing — how many supervised scans define competence, how images are archived and reviewed, and how the scope of each operator is governed — rather than about the clinical value of the applications themselves. [1] [7]
Exam Pearls
A fellowship candidate should leave the examiner with a small set of sharp, sourced facts, and these will answer almost any question on this topic. [1] [3]
The single highest-yield fact is that paediatric POCUS is a focused, bedside, radiation-free scan that answers one clinical question, and its accuracy rests on choosing the right probe for the depth, reading a small set of artefacts, and never letting the scan delay a time-critical intervention. The probe rule is that higher frequency buys resolution but loses depth, so the small child's superficial lung and vessels take a high-frequency linear probe, the abdomen and the older child's chest take a curvilinear probe, and the heart takes a phased array probe. [1]
The lung artefact rule is the second pillar. A-lines are horizontal and dry; B-lines are vertical and wet, and three or more in an intercostal space is alveolar-interstitial syndrome; lung sliding, when present, rules out a pneumothorax at that point; the lung point, when found, is highly specific for a partial pneumothorax; and a tension pneumothorax is decompressed clinically before any probe. The BLUE protocol weaves these signs into a decision tree for acute respiratory failure. [2] [3]
The FAST rule is that the scan reads free fluid in four dependent windows — right upper quadrant and Morison's pouch, left upper quadrant and splenorenal recess, subxiphoid pericardium, suprapubic pelvis — and is highly specific but poorly sensitive in children because the solid organs bleed into their own parenchyma. A positive FAST in an unstable child drives surgery or retrieval; a negative FAST changes nothing and never excludes injury. The abdominal rule is that ultrasound is first-line for intussusception (the target sign, sensitivity above 95 per cent) and for pyloric stenosis (muscle thickness 3 to 4 millimetres, channel length 15 to 17 millimetres, with criteria under revision). [7] [8] [9]
For procedures, ultrasound guidance improves first-attempt success for difficult peripheral cannulation, as the EPIC superiority trial confirmed. For cardiac POCUS, the focused scan answers four questions — left ventricular function, right ventricular size, pericardial effusion, and volume status from the inferior vena cava — and never replaces the formal echocardiogram. And the safety rule is that ultrasound carries no ionising radiation, which is why it has displaced the radiograph for so many paediatric questions, but it remains operator-dependent, so training, logged scans, image review, and credentialing against a defined scope are what make a confident scan an accurate one. [1] [10] [11]
References
- [1]Singh Y, Tissot C, Fraga MV, et al International evidence-based guidelines on Point of Care Ultrasound (POCUS) for critically ill neonates and children issued by the POCUS Working Group of the European Society of Paediatric and Neonatal Intensive Care (ESPNIC) Critical Care, 2020.PMID 32093763
- [2]Lichtenstein DA, Mezière GA Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol Chest, 2008.PMID 18403664
- [3]Lichtenstein DA Lung ultrasound in the critically ill Annals of Intensive Care, 2014.PMID 24401163
- [4]Shi C, Xu X, Xu Y Systematic review and meta-analysis of the accuracy of lung ultrasound and chest radiography in diagnosing community acquired pneumonia in children Pediatric Pulmonology, 2024.PMID 39239917
- [5]Stadler JAM, Andronikou S, Zar HJ Lung ultrasound for the diagnosis of community-acquired pneumonia in children Pediatric Radiology, 2017.PMID 29043420
- [6]Tsou PY, Chen KP, Wang YH, et al Diagnostic Accuracy of Lung Ultrasound Performed by Novice Versus Advanced Sonographers for Pneumonia in Children: A Systematic Review and Meta-analysis Academic Emergency Medicine, 2019.PMID 31211896
- [7]Liang T, Roseman E, Gao M, et al The Utility of the Focused Assessment With Sonography in Trauma Examination in Pediatric Blunt Abdominal Trauma: A Systematic Review and Meta-Analysis Pediatric Emergency Care, 2021.PMID 30870341
- [8]Li XZ, Wang H, Song J, et al Ultrasonographic Diagnosis of Intussusception in Children: A Systematic Review and Meta-Analysis Journal of Ultrasound in Medicine, 2021.PMID 32936473
- [9]Piotto L, Gent R, Taranath A, et al Ultrasound diagnosis of hypertrophic pyloric stenosis - Time to change the criteria Australasian Journal of Ultrasound in Medicine, 2022.PMID 35978726
- [10]Kleidon TM, Schults JA, Royle RH, et al First-Attempt Success in Ultrasound-Guided vs Standard Peripheral Intravenous Catheter Insertion: The EPIC Superiority Randomized Clinical Trial JAMA Pediatrics, 2025.PMID 39869351
- [11]Conlon TW, Baker D, Bhombal S Cardiac point-of-care ultrasound: Practical integration in the pediatric and neonatal intensive care settings European Journal of Pediatrics, 2024.PMID 38236402
- [12]Raimondi F, Yousef N, Migliaro F, et al Point-of-care lung ultrasound in neonatology: classification into descriptive and functional applications Pediatric Research, 2021.PMID 30127522