Paeds · investigations-procedures-and-technology
Paediatric venepuncture and peripheral intravenous access
Also known as Paediatric cannulation · Paediatric IV access · Child venepuncture · Paediatric peripheral cannula insertion
A fellowship approach to paediatric venepuncture and peripheral intravenous access: choose a site by age (dorsal hand veins first, then antecubital fossa, forearm and great saphenous at the ankle), select a cannula gauge by age and indication (24G neonate and infant, 22G infant and small child, 20G older child, 18G adolescent or rapid bolus), apply a systematic comfort bundle (topical anaesthesia at the correct lead time, oral sucrose, distraction, comfort positioning and a single calm operator), use ultrasound-guided access for the difficult-access child, and escalate to intraosseous access when peripheral attempts fail in an emergency.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A dehydrated 18-month-old is brought to the emergency department dry-mouthed and listless, and you need a cannula in the next few minutes to give fluids. There is a small window to get this right, because a frightened, crying child collapses the very veins you are trying to find, a cold and vasoconstricted limb hides them, and each failed attempt destroys the next site and hardens the child's (and the family's) fear of needles for years to come. This page teaches the whole procedure — the sites, the gauges, the comfort bundle, the ultrasound-guided pathway, and what to do when access fails — so that the first attempt is calm, quick and successful. [1] [9]
The five questions before the needle
Overview & Definition
Imagine you are asked to "get access" on a child. The first thing to pin down is which of two different procedures is meant, because they share a needle and a vein but diverge in purpose, equipment and risk. Venepuncture is a one-off puncture of a vein, usually with a winged infusion butterfly needle, to take a blood sample; the needle comes out as soon as the tubes are filled. Peripheral intravenous cannulation is the placement of a short plastic cannula that stays in the vein so that you can give fluids, drugs or contrast over hours or days. Examiners test this distinction deliberately, so hold it precisely: venepuncture samples, cannulation treats. [7]
Both procedures live at the interface of technical skill and behavioural skill, and that is what makes children different from adults. A child's vein is small and mobile and often hidden under subcutaneous fat, the child is frightened and uncooperative, and the family is watching. The technical act of putting a needle in a vein is therefore inseparable from the act of keeping the child calm enough for that vein to fill. Treat comfort not as a kindness added at the end but as a procedural step as real as skin preparation. [9] [12]
The key idea a candidate must hold is the buffer. In an elective adult cannulation you can afford a slow, methodical search and a second or third attempt. In a child each attempt consumes the buffer of cooperation: the child cries, the veins constrict, the parents become distressed, and the next attempt becomes harder, not easier. Every choice you make before the needle — the topical anaesthesia applied an hour ago, the sucrose given, the distraction ready, the right operator, the right site — exists to preserve that buffer so the first attempt succeeds. [7]
Classification
Sort paediatric vascular access by how long the device stays in and what it is for, because that drives your choice of device and site. [6]
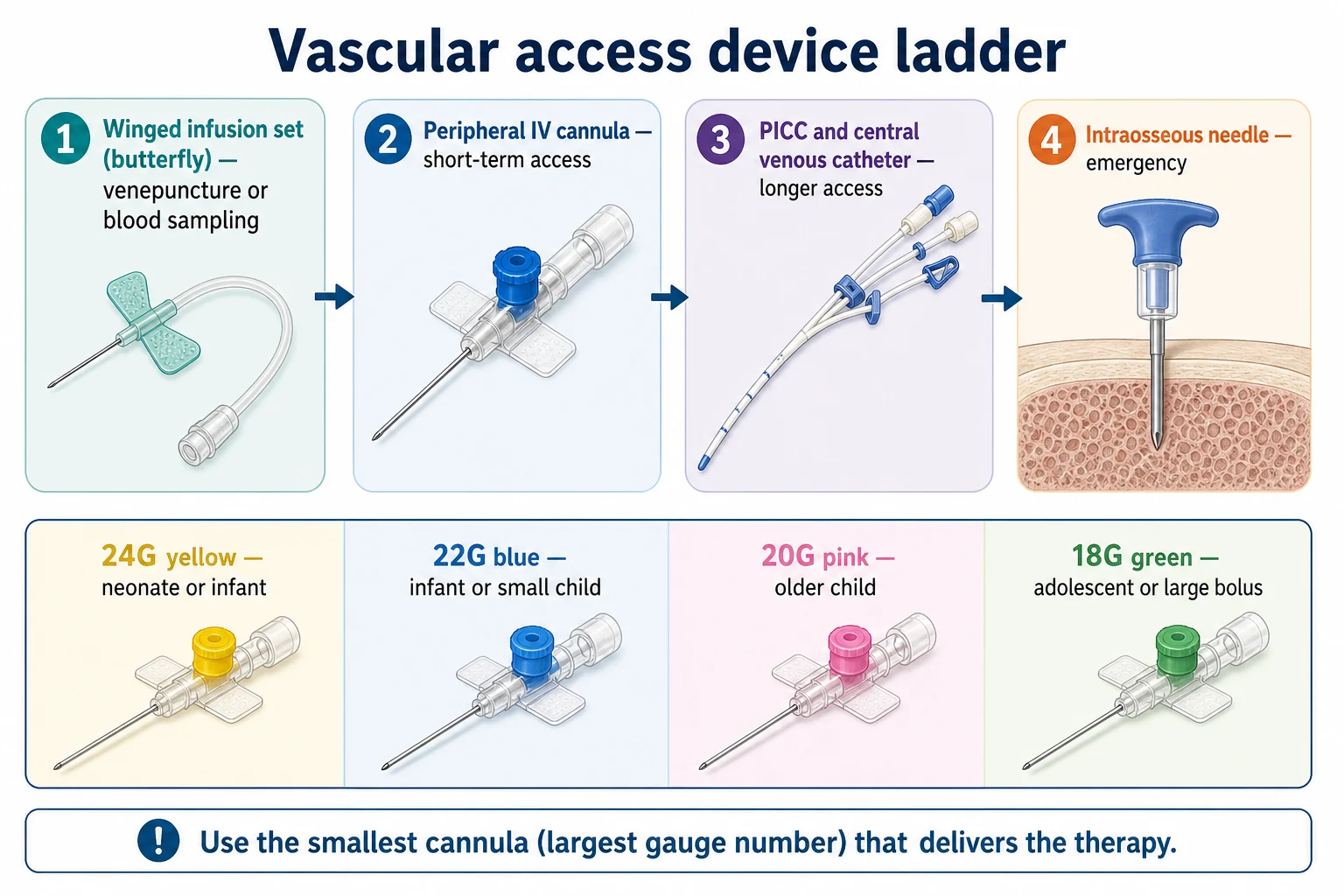
The first sort is by purpose. A winged infusion butterfly set is for venepuncture — a blood sample taken through a short needle with flexible wings and a length of tubing. A short peripheral cannula is for short-term therapy — fluids and drugs over hours to a few days. A peripherally inserted central catheter (PICC) or central venous catheter reaches the great vessels for longer or central access, and an intraosseous needle is the emergency device used when peripheral access has failed or is needed in arrest. This page owns the first two; the sister pages own the rest. [6]
The second sort is by gauge, and the gauge maps to the colour of the cannula hub. The examinable mapping is yellow 24G, blue 22G, pink 20G, green 18G, and grey 16G — and the higher the gauge number, the smaller the cannula. The principle is to use the smallest cannula (largest gauge number) that will deliver the therapy, because a smaller cannula is easier to place in a small vein and causes less trauma, while a larger cannula is needed only for a rapid bolus or a blood transfusion. [6]
The third sort is by predicted difficulty, and this is the one that changes your plan in the moment. A straightforward-access child has a visible, palpable vein and is calm. A difficult-access child has no visible vein, or is vasoconstricted, oedematous, dark-skinned, obese, an infant, oncology, or carries a known history of hard access. The difficult-access label is your trigger to go to ultrasound early rather than to persist blindly. [1] [4]
Epidemiology & Risk Factors
First-attempt failure is common in children and it is the single statistic that should shape how a candidate approaches the procedure. Roughly a third of paediatric cannulations need more than one attempt, and the youngest, the sickest and those with the fewest visible veins carry the highest failure rate. The practical reading is direct: do not be surprised by failure, but plan so that the first attempt is the best attempt and so that escalation is rehearsed rather than improvised. [1] [5]
The strongest predictors of a difficult cannulation are age and physiology working together. Infants and toddlers fail more often because their veins are small and hidden and because they cannot cooperate; dehydration and shock constrict the peripheral circulation and make a good vein disappear exactly when you need it most; obesity, oedema, dark skin tone and a history of repeated chemotherapy all hide the vessel. Operator experience is the most modifiable factor — the most experienced available operator should perform or directly supervise the difficult cannulation, and a learner should not persist after a failed attempt. [2] [5]
Procedural pain and needle fear are not side-effects of access — they are part of its epidemiology. A child who has a painful, repeated cannulation is more likely to develop needle phobia and to refuse or delay healthcare later. This is the evidence base for treating the comfort bundle as a standard of care rather than an optional extra, and it is why guidelines now expect topical anaesthesia, distraction and a calm single operator for every non-emergency needle in a child. [9] [12]
Pathophysiology
A child's peripheral vein is harder to cannulate than an adult's for mechanical reasons that you can see at the bedside. The vessel calibre is small, the vein sits under a relatively thicker layer of subcutaneous fat in the infant and toddler, the wall is thin and collapses easily under a tourniquet, and the child moves. Together these mean that a vein that looks generous on the surface can roll away, collapse, or prove deeper than it appeared. [7]
The second problem is physiological, not anatomical, and it works against you the moment the child becomes distressed. Pain and fear trigger a vasovagal reflex: heart rate and blood pressure fall, and the child may pale, yawn, sweat, or even faint. At the same time crying raises intrathoracic pressure and directly compresses the veins, while catecholamine release from fear constricts the peripheral vessels. A frightened child therefore has both fewer and smaller veins to find, which is why comfort is not merely kind — it is the manoeuvre that makes the vein appear. [9]
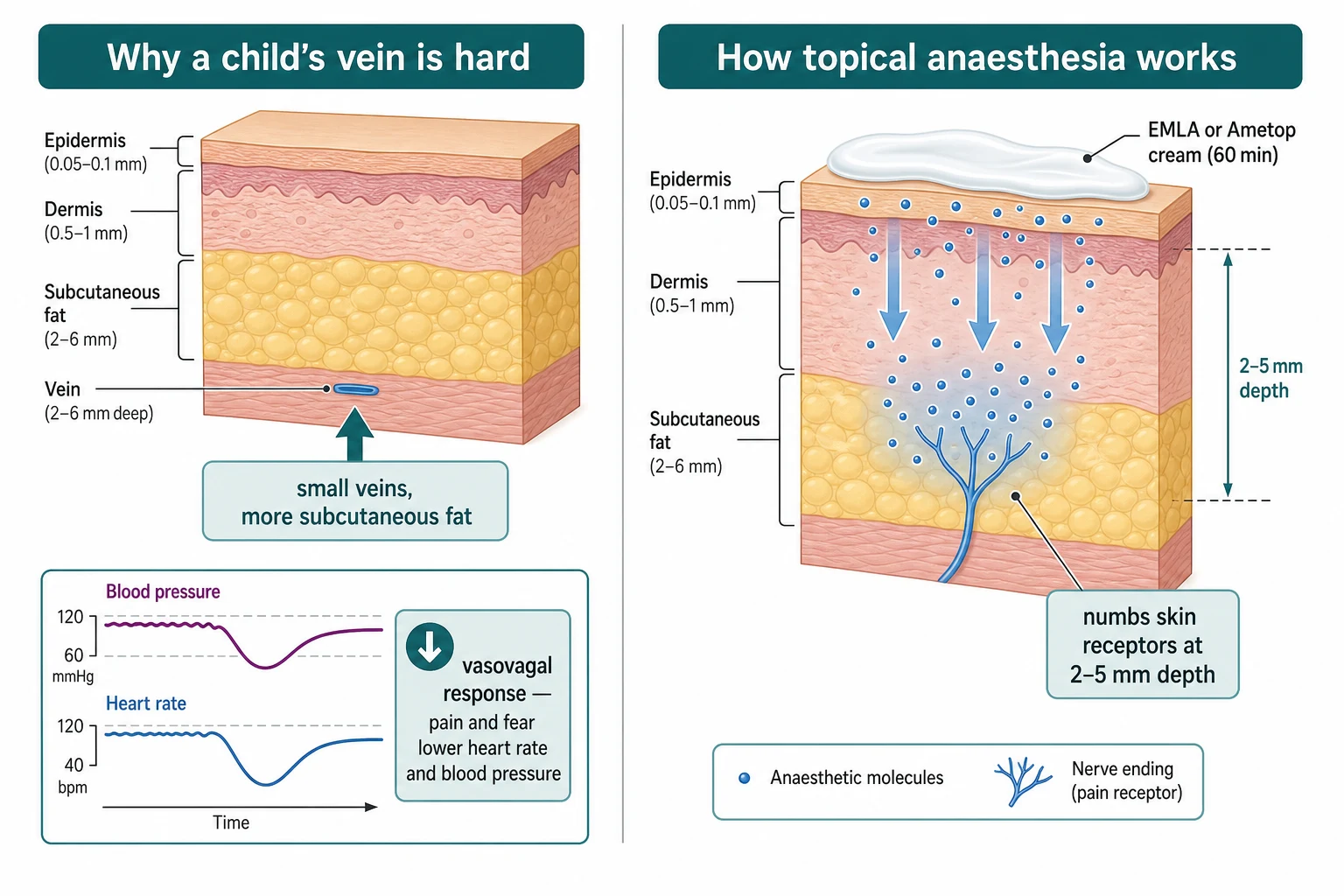
Topical anaesthesia works by diffusion. The active agent — lidocaine and prilocaine in EMLA, tetracaine in Ametop, or liposomal lidocaine in LMX4 — passes through the stratum corneum and epidermis to block sodium channels in the dermal nerve endings, and that diffusion takes time. The lead time is the whole point of the treatment: EMLA needs about 60 minutes, Ametop about 30 to 45 minutes, and LMX4 about 30 minutes. Apply it too late and the child feels the needle; the anaesthesia is a preparation step that must be built into the workflow, not added at the bedside. [7] [8]
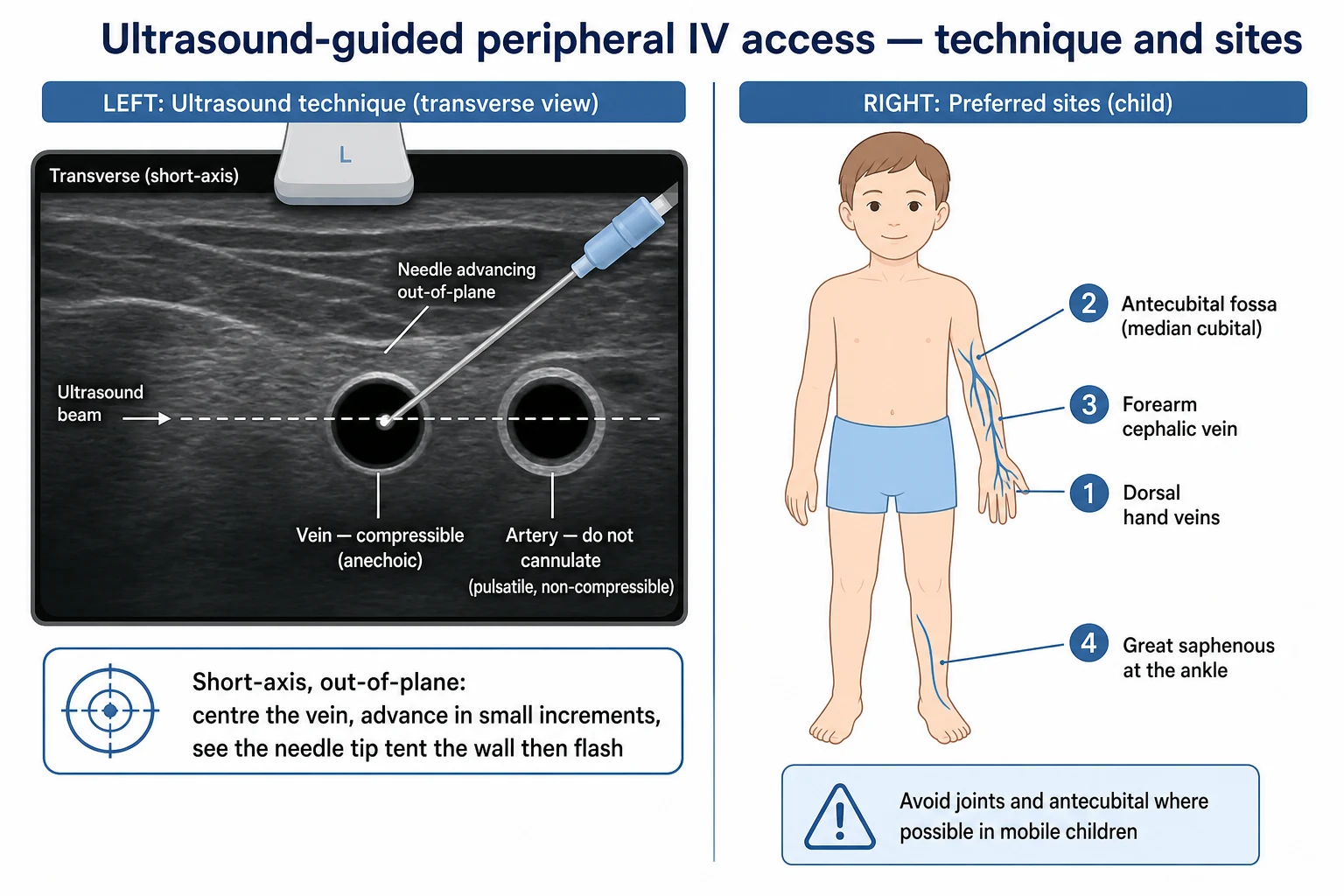
Ultrasound works because it separates a vein from an artery by behaviour rather than by appearance. On a high-frequency linear probe, both look like round dark structures, but the vein is compressible — gentle pressure with the probe flattens it — whereas the artery is non-compressible and pulsatile. Compressibility is the single most useful sign, and it is the manoeuvre that lets you confidently identify a target vein and avoid the artery beside it. [1] [6]
Clinical Presentation
The child who needs access presents in one of two ways, and the distinction changes everything about your speed and your tolerance for failure. The routine-access child needs a blood test or a cannula for non-urgent therapy: they are perfused, they have time, and you can apply topical anaesthesia and wait the full lead time. The emergency-access child is in shock, sepsis, or arrest: the peripheral circulation is shut down, the veins have disappeared, and every minute of delay is a minute of untreated hypoperfusion — here you go to ultrasound early and keep intraosseous access ready. [1]
Which features predict difficulty before you touch the child? Look for small or absent visible veins, a dehydrated or shocked child with cool peripheries and a prolonged capillary refill, oedema, obesity, dark skin tone, infancy, an oncology history, and any documented note of previous difficult access. These are not reasons to avoid the procedure — they are reasons to plan it: bring the most experienced operator, prepare ultrasound, and decide in advance how many blind attempts you will allow before escalating. [2] [5]
A frightened or needle-phobic child has a presentation of its own: a clenched fist, withdrawal, crying, pallor, and sometimes a frank vagal episode before the needle is even near. This is the child for whom the comfort bundle earns its place — distraction, a parent on the lap, topical anaesthesia, and a single calm operator — because the physiological stress response will actively hide the veins you need. [9]
After a cannula is in, the features that signal a complication are specific and must be asked for at every review: pain, swelling, redness or leakage at the site, sluggish flow, and a cool, pale limb distal to the cannula. Any of these demands that the cannula be removed and the limb assessed, and a vesicant drug that has extravasated demands immediate senior review. [6]
Differential Diagnosis
When is a peripheral approach the wrong first answer? The clearest case is the child in cardiac arrest or profound shock, where peripheral vasoconstriction makes success unlikely and where the time spent searching is time without therapy. In arrest the answer is intraosseous access, and it should not wait on repeated peripheral attempts. The examinable rule, drawn from APLS, is to move to intraosseous access within about 90 seconds of failed peripheral attempts, or immediately as the first route in a shocked child with no obvious vein. [2]
The reverse question — when is venepuncture enough and when must you cannulate? A single diagnostic blood test may need only a butterfly. But any child who is or may become unwell, who needs fluids or ongoing drugs, or who is being admitted, needs a cannula even if the immediate task was only a sample, because the deterioration you are trying to stay ahead of is exactly when access becomes hardest. [9]
Some conditions make peripheral access locally futile or dangerous, and they belong on the differential before you start. Severe local infection, burns or scarring at every site, a severe coagulopathy at a site you cannot compress, and superior vena cava obstruction (where you avoid the upper limb) all change the plan. The alternatives are ultrasound-guided peripheral access, the external jugular vein, the great saphenous vein, umbilical access in the newborn, or a central line. [6]
Keep one diagnosis always in mind at the moment of flashback: an intra-arterial or extravasation injury. Bright red, pulsatile blood, or pain on injection, means you may be in an artery — stop, withdraw, and do not flush. Swelling, blistering or discolouration around a running cannula means a vesicant has extravasated — stop, leave the cannula in to aspirate, elevate, and assess for compartment syndrome. [6]
Clinical & Bedside Assessment
The site is chosen by age and by what the limb will tolerate, and there is a preferred order you should be able to recite. Begin distally on the dorsum of the non-dominant hand, because hand veins are superficial and easy to secure and a distal site leaves proximal options open if you fail. If the hand fails, move to the antecubital fossa (the median cubital vein), the forearm cephalic vein, and finally the great saphenous vein at the ankle, which is remarkably consistent in position and a reliable site in the infant and toddler. Avoid joints where you can in a mobile child, because a cannula in the antecubital fossa kinks every time the child bends the arm. [6]
The gauge is chosen by age and by the therapy. The mapping to know is a 24G for the neonate and infant, a 22G for the infant and small child, a 20G for the older child, and an 18G for the adolescent or when a rapid bolus or blood transfusion is needed. The principle, stated again because examiners reward it, is to use the smallest cannula (largest gauge number) that will deliver the therapy. A neonate rarely needs anything larger than a 24G, while a shocked adolescent needing a fluid resuscitation may need an 18G or larger. [6]
Before the needle, assess the child's pain, fear and cooperation and decide which comfort measures to deploy. For the non-emergency needle this means topical anaesthesia applied at the correct lead time, oral sucrose for the infant, age-appropriate distraction, and a parent for comfort positioning. Gathering the equipment in advance is part of the assessment: gloves, skin preparation, tourniquet, the chosen cannula and a spare one of the next size, gauze, tape, a transparent dressing, labelled tubes in the correct order, a sharps bin within arm's reach, and the comfort measures ready. [7] [10]
When surface veins are absent, ultrasound is the bedside assessment that finds a target. Use a linear high-frequency probe, identify a compressible anechoic vein in the short axis, and mark its depth and position before you prep. The combination of palpation, warmth, a gentle tourniquet and gravity to distend a surface vein, with ultrasound held in reserve, is the complete bedside assessment. [1] [3]
Investigations
Most investigations are not needed before access, but a few bedside facts are mandatory. Confirm the child's identity and the indication, weigh the child (every drug and fluid dose depends on weight), check allergies and consent or assent, and judge the predicted difficulty. These take seconds and they prevent the errors — wrong child, wrong tube, wrong limb — that cause harm. [6]
Point-of-care testing is the investigation that access unlocks. A bedside glucose is essential in the febrile or unwell infant, in a metabolic presentation, and in the shocked child; a venous or capillary blood gas tells you the acid-base status and the lactate the moment the sample is drawn; and blood is taken into the correct tubes in an age-appropriate volume — never over-draw a small infant, in whom the volume taken is a clinically meaningful fraction of circulating blood. [9]
Ultrasound is itself the key investigation for the difficult-access child. A linear probe at a high frequency (around 8 to 15 megahertz) at a shallow depth identifies the target vein, its depth, and its relation to the artery, and it predicts whether a standard cannula will reach. Ray-Barruel and colleagues, in a 2024 scoping review of handheld ultrasound for cannulation, confirmed that point-of-care ultrasound improves first-attempt success in the difficult-access patient and is increasingly available as a handheld device. [6]
After placement, confirm patency by the feel of the flush: a free flashback, an easy saline flush with no resistance and no swelling, and a blood return. Imaging is not routine for a peripheral cannula — it is needed only to investigate a suspected complication such as a deep extravasation or an arterial injury. [4]
Management — Resuscitation
When access is needed in an emergency, the immediate response is to run preparation and comfort in parallel rather than in series, and to recognise failure fast. Call for help, gather the team, prepare the difficult-access pathway, and apply the comfort measures that the moment allows — while a second person opens the ultrasound and a third prepares the intraosseous driver. In true arrest you do not wait for any of this to be elegant: you go to intraosseous access immediately. [1]
The recognition that peripheral access is failing in resuscitation is itself a clinical skill. A shocked, vasoconstricted child with no visible vein after one or two careful attempts is not a child to keep stabbing — that child is a child for ultrasound, and if ultrasound is not immediately fruitful or the child is in arrest, for intraosseous access. The APLS rule of moving to intraosseous access within about 90 seconds of failed peripheral attempts, or as the first route in a shocked child with no obvious vein, exists to stop the dangerous habit of persisting blindly while resuscitation stalls. [2]
Never let access displace the airway and breathing priority in the deteriorating child. A hypoxaemic child needs oxygen and bag-mask ventilation first; the cannula for fluids or drugs comes next. Reversing the order — hunting for a vein while a child desaturates — is a classic and avoidable error. [1]
Management — Definitive & Stepwise
The definitive procedure is two sequences, one for venepuncture and one for cannulation, and both follow the same logic of prepare, comfort, puncture, confirm, and dispose of sharps. [7]
For venepuncture, confirm identity and indication, apply topical anaesthesia in advance, position the child on a parent's lap and deploy distraction, clean the skin, tether the skin distal to the vein to stop it rolling, and insert the winged infusion needle at about 15 to 30 degrees with the bevel up until you see flashback in the tubing. Collect blood into the labelled tubes in the correct order, withdraw the needle, apply firm pressure, and drop the whole device into a sharps bin without recapping. [7] [9]
For cannulation, prepare and comfort the child as above, apply a tourniquet proximal to the chosen site, clean the skin, and stabilise the vein by gentle traction distally. Insert the cannula at about 15 to 30 degrees bevel up until flashback appears in the chamber, then advance the whole assembly a millimetre or two further so both the needle tip and the cannula tip are in the lumen, withdraw the needle while sliding the cannula gently forward into the vein, release the tourniquet, attach the bung or giving set, secure with a transparent dressing and tape, flush with saline to confirm patency, and drop the stylet straight into a sharps bin. [6]
Peripheral cannulation sequence
Prepare: identity, indication, weight, consent, equipment and comfort measures ready
Comfort: topical anaesthesia at lead time, sucrose, distraction, comfort positioning
Site and gauge: dorsal hand first, smallest cannula that delivers the therapy
Clean and tourniquet: skin prep, tourniquet proximal, stabilise the vein distally
Puncture: insert bevel up at 15 to 30 degrees until flashback, advance slightly
Cannulate: withdraw needle while advancing the cannula, release tourniquet
Secure and flush: transparent dressing, flush with saline to confirm patency
Dispose and document: sharps bin, record site, gauge, date and operator
The comfort bundle is a procedural step, not an add-on, and it has specific components. Apply topical anaesthesia at the correct lead time — EMLA about 60 minutes before, Ametop about 30 to 45 minutes, LMX4 about 30 minutes — and occlude it with a dressing so it stays in contact. Give oral sucrose at a volume of 1 to 2 millilitres about two minutes before the procedure in infants. Deploy age-appropriate distraction, position the child for comfort on a parent's lap, and use a single calm operator. The rule on attempts is firm: no more than two per operator, then call a more senior clinician. [7] [10]
For ultrasound-guided cannulation, select a linear high-frequency probe, identify a compressible anechoic vein in the short axis, centre it under the probe marker, and insert the cannula out-of-plane, advancing in small increments and watching the needle tip tent the vessel wall and then drop into the lumen with a flash. Confirm with an easy saline flush and no swelling. Bair and colleagues, in a randomised trial of ultrasound-assisted access in young children, showed that ultrasound raises success in the difficult-access child, and the 2023 meta-analysis by Poulsen and colleagues and the 2024 review by Alvarez-Morales and colleagues confirmed a first-attempt success benefit for ultrasound-guided peripheral cannulation. [1] [2] [3]
Aftercare is mandatory and often neglected. Document the site, gauge, date and operator; date-label the dressing; flush with saline; set a review and a removal plan; monitor for infiltration and phlebitis; and use the cannula only while it is clinically needed. Routine replacement every few days is no longer recommended — remove the cannula when it is no longer needed or when a complication appears. [6]
Specific Subtypes & Scenarios
The neonate is the hardest routine access patient. The veins are tiny, a 24G cannula is usual, and the scalp veins and the dorsum of the hand are the preferred sites. Volume drawn must be guarded because a few millilitres is a meaningful fraction of circulating blood. EMLA is avoided in the preterm infant and in infants under about three months because prilocaine carries a risk of methaemoglobinaemia; umbilical venous access is available in the first week of life and is covered on the sister page. [7]
The infant and toddler is the uncooperative child, and the whole technique bends around cooperation. Comfort positioning on a parent's lap, oral sucrose, distraction, and a single calm operator are the package; a 24G or 22G cannula is usual; and the great saphenous vein at the ankle is a reliable site when the hand veins fail. The principle is that the technical act is easy once the child is still, and the behavioural act of keeping the child still is the real skill. [10]
The shocked or collapsed child is the scenario where peripheral access is both most urgent and least likely to succeed, because peripheral vasoconstriction has hidden the veins. Go to ultrasound early, keep intraosseous access ready, and never let a hunt for a peripheral line delay resuscitation. The cannula you place, if any, should be the largest the vein allows so that a bolus runs fast. [1] [2]
The oncology or chronically ill child often has veins already damaged by repeated chemotherapy. Preserve veins where possible, use an indwelling port or central line where one exists, apply topical anaesthesia and play therapy, and call the most experienced operator — a vascular access team if one is available — because a failed attempt closes a vein the child will need again. [5]
The adolescent has adult-like veins and gauges of 18G to 20G are usually feasible, but two things distinguish this group: consent and autonomy must be respected, and vasovagal syncope is common, so the adolescent should be lying or seated safely and never standing for a needle. [9]
Complications & Pitfalls
The early complications happen at the needle: a haematoma from poor pressure, pain, a vasovagal reaction, an accidental arterial puncture, a nerve injury, and a needlestick injury to staff. Most are prevented by good technique — a single calm attempt, firm pressure on withdrawal, and a sharps bin within reach so that no needle is ever recapped. A needlestick injury must be managed at once: let the wound bleed, wash with water, report immediately, and assess source and recipient for blood-borne viruses so that post-exposure prophylaxis can be started within hours if indicated. [6]
The later complications belong to the indwelling cannula. Infiltration is fluid running into the surrounding tissue; extravasation is the same but with a vesicant drug that can cause tissue necrosis; phlebitis is inflammation of the vein; thrombosis, local and bloodstream infection, and accidental dislodgement complete the list. The first sign of any of them — pain, swelling, redness, leakage, sluggish flow, or a cool pale limb — should trigger removal. [6]
The classic errors are the ones examiners probe. Repeated blind attempts that destroy the vein and traumatise the child; failing to use topical anaesthesia in a non-emergency needle; cannulating an artery because the pulsatile flashback was missed; flushing against resistance; forgetting to release the tourniquet; and leaving a cannula in longer than needed. Each is preventable by the discipline of preparing the five questions before the needle. [9]
Prognosis & Disposition
A peripheral cannula should stay in only as long as it is needed, and the modern evidence has retired the old practice of routine replacement every three to four days. Remove the cannula when therapy is complete or when a complication appears, and review the site at every shift for the signs of infiltration, phlebitis or infection. The child who was cannulated in shock or arrest goes to paediatric intensive care or retrieval, with the monitoring that resuscitation demands. [6]
The number of attempts is itself a prognostic marker. Each failed attempt raises the child's distress, the risk of a haematoma that closes the next vein, and the long-term risk of needle phobia, which is why first-attempt success is treated as a quality target and audited in many paediatric services. A cannulation that needed many attempts is a signal to ask why — was the operator inexperienced, the child difficult, or the pathway to ultrasound and intraosseous access too slow? [5]
The prognosis of an extravasation or arterial injury depends on the vesicant, the volume, the site, the speed of recognition, and early referral, and it can range from trivial to a limb-threatening injury. Communicate the procedure's risks and the aftercare to the family before you start, and give them the signs that should prompt return — redness, swelling, pain, fever, or a cold pale limb. [6]
Special Populations
The preterm and small neonate needs the most careful technique: very small veins, scalp and hand sites preferred, EMLA contraindicated due to methaemoglobinaemia, careful volume drawn, and umbilical venous access available in the first week. A 24G cannula is usual and sometimes a smaller device is needed. [7]
The child with autism or developmental disability needs a modified approach when time allows: preparation, social stories, a quiet environment, distraction, comfort positioning, and a low threshold for procedural sedation when the access is essential and cooperation is impossible. The comfort bundle here is scaled up, not abandoned. [9]
The immunocompromised or oncology child demands aseptic technique above all: preservation of veins, a port or central line where available, topical anaesthesia and play therapy, and the most experienced operator, because a bloodstream infection from a cannula is a serious event in this group. [5]
The child with a bleeding disorder or on anticoagulation changes the procedure in a predictable way: choose a compressible site, apply prolonged pressure, use the smallest gauge, and have a plan for haemostasis, such as factor cover in severe haemophilia, agreed with the haematology team before the needle. [6]
In remote and retrieval settings, the same principles apply with fewer hands. Retrieval teams are trained in ultrasound-guided peripheral access and intraosseous access, and the threshold to move the child to a centre that can manage access is lower than to persist with repeated attempts in a small unit. [2]
Evidence, Guidelines & Regional Differences
The guidelines converge on the same core: a planned comfort bundle, the right site and gauge, and a rehearsed escalation pathway. The Royal Children's Hospital Melbourne, APLS and ANZCOR agree on the gauge-by-age mapping, the site order, the comfort bundle, and the rule of moving to intraosseous access promptly in arrest. Where they differ is in the detail of topical agents and in the local ownership of ultrasound-guided access. [6]
The evidence for ultrasound-guided peripheral access in children has grown steadily. Bair and colleagues, in a 2008 randomised trial of ultrasound-assisted access in young children, showed improved success in the difficult-access child; the 2023 meta-analysis by Poulsen and colleagues confirmed a first-attempt success benefit for difficult cannulation; the 2024 review by Alvarez-Morales and colleagues and by Ray-Barruel extended this to nurse-led and handheld ultrasound practice; and the 2025 comparison by Refosco and colleagues showed favourable outcomes for ultrasound-guided deep-vein placement over blind superficial placement. The consistent message is that ultrasound raises success in the child whose surface veins have failed. [1] [2] [3] [4]
In ANZ practice (RCH Melbourne, APLS, ANZCOR), EMLA and Ametop are both used for non-emergency needles, ultrasound-guided peripheral access is increasingly nurse- and doctor-led, routine cannula replacement is not recommended, and intraosseous access is emphasised in the difficult-access and arrest pathway.
[6]The evidence on topical anaesthesia shows that all three agents work but differ in lead time and in cautions. Eichenfield and colleagues, in a 2002 study, found ELA-Max (LMX4) comparable to EMLA for venepuncture pain with a shorter application time, and Lal and colleagues showed that EMLA adds benefit even when distraction is used. EMLA carries the prilocaine-related methaemoglobinaemia caution in the youngest infants, which is why it is avoided under about three months. [8] [9]
The non-pharmacological comfort evidence is strong and grows with the age group: Cavicchiolo and colleagues confirmed that a single dose of oral sucrose controls venipuncture pain in infants, Haidar and colleagues compared the Buzzy device with EMLA for needle pain, and Balan and colleagues even showed that classical instrumental music reduces venepuncture pain in older children. The controversy in the field is less about whether comfort works and more about whether anaesthetist- or nurse-led ultrasound access should own the difficult-access pathway. [10] [11] [12]
Ultrasound-guided peripheral access — the cumulative evidence
Randomised trial plus systematic reviews and meta-analyses
Population: Children with difficult peripheral access in the emergency department
Key finding
Ultrasound guidance improves first-attempt success in the difficult-access child, with a consistent benefit shown across Bair 2008, the 2023 Poulsen meta-analysis, the 2024 Alvarez-Morales review, and the 2025 Refosco comparison.
Exam Pearls
The two facts most often misremembered are the topical anaesthesia lead times and the gauge-by-age mapping. EMLA needs the full 60 minutes — anything less and the child feels the needle. Ametop is faster at 30 to 45 minutes, and LMX4 at about 30 minutes. The gauge-by-age ladder starts at 24G in the neonate and climbs: 24, 22, 20, 18 from neonate to adolescent. State these as absolutes in the exam; they are the facts the topic exists to teach. [7] [6]
References
- [1]Bair AE, Rose JS, Vance CW, et al. Ultrasound-assisted peripheral venous access in young children: a randomized controlled trial and pilot feasibility study. West J Emerg Med, 2008.PMID 19561750
- [2]Poulsen E, Aagaard R, Lofgren B, et al. The effects of ultrasound guidance on first-attempt success for difficult peripheral intravenous cannulation: a systematic review and meta-analysis. Eur J Emerg Med, 2023.PMID 36727865
- [3]Alvarez-Morales L, Gomez-Urquiza JL, Romero-Beltran JL, et al. Ultrasound-guided peripheral intravenous cannulation by emergency nurses: a systematic review and meta-analysis. Int Emerg Nurs, 2024.PMID 38401479
- [4]Refosco M, Mazza A, Barco S, et al. Comparison of peripheral cannula outcomes, ultrasound-guided placement of deep veins versus blind placement of superficial veins. J Vasc Access, 2025.PMID 39305185
- [5]Jamal AN, Ruse N, Smith J, et al. Outcomes of a comprehensive ultrasound guided peripheral IV insertion (USGPIV) training program in the pediatric emergency department. J Emerg Nurs, 2023.PMID 37589623
- [6]Ray-Barruel G, Pather P, Marsh N, et al. Handheld ultrasound devices for peripheral intravenous cannulation: a scoping review. J Infus Nurs, 2024.PMID 38422403
- [7]Russell SC, Doyle E. A risk-benefit assessment of topical percutaneous local anaesthetics in children. Drug Saf, 1997.PMID 9113495
- [8]Eichenfield LF, Funk A, Fallon-Friedlander S, Cunningham BB. A clinical study to evaluate the efficacy of ELA-Max (4% liposomal lidocaine) as compared with eutectic mixture of local anesthetics cream for pain reduction of venipuncture in children. Pediatrics, 2002.PMID 12042548
- [9]Lal MK, McClelland J, Phillips J, et al. Comparison of EMLA cream versus placebo in children receiving distraction therapy for venepuncture. Acta Paediatr, 2001.PMID 11236044
- [10]Cavicchiolo ME, Daverio M, Battajon N, Frigo AC, Lago P. A single dose of oral sucrose is enough to control pain during venipuncture: a randomized clinical trial. Front Pain Res, 2022.PMID 35634454
- [11]Haidar NA, Al Amri MH, Al Otaibi AF, et al. Efficacy of Buzzy device versus EMLA cream for reducing pain during needle-related procedures in children: a randomized controlled trial. Pediatr Emerg Care, 2024.PMID 37163686
- [12]Balan R, Bavdekar SB, Karande B, et al. Can Indian classical instrumental music reduce pain felt during venepuncture? A randomized controlled trial. Indian J Pediatr, 2009.PMID 19390796