Paeds · investigations-procedures-and-technology
Point-of-care glucose, ketone and urinalysis testing
Also known as Bedside blood glucose meter · Capillary glucose testing · Beta-hydroxybutyrate testing · Blood ketone monitoring · Urine dipstick · Urinalysis · Reagent strip testing · Point-of-care testing
Fellowship guide to the three core paediatric point-of-care tests. Covers the capillary blood glucose meter and its known inaccuracy in the neonate from the high haematocrit and the galactose or maltose interference with the glucose dehydrogenase strips, the rule to confirm any critical value with a laboratory plasma glucose, the blood beta-hydroxybutyrate ketone meter as the preferred measure over the urine acetoacetate in diabetic ketoacidosis with the ISPAD thresholds of greater than three millimoles per litre for the diagnosis and the fall that tracks the resolution, and the urine dipstick with the leukocyte esterase and the nitrite performance, the lower sensitivity of the nitrite in the young infant, and the rule that the dipstick screens while the culture confirms the urinary tract infection.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
The three point-of-care tests in this topic give a rapid bedside answer to three different clinical questions. The capillary blood glucose meter answers whether the child is hypo- or hyperglycaemic at this moment. The blood beta-hydroxybutyrate ketone meter answers whether the child has accumulated ketones and how severe the ketosis is. The urine dipstick answers whether the urine contains the cells, the chemicals, and the metabolites that point to the infection, the glycosuria, or the dehydration. Each test takes seconds to minutes, runs on a small device or a reagent strip at the bedside, and changes the immediate management. [1]
The unifying principle is that these are screening and monitoring tools, not definitive laboratory measurements. The glucose meter, the ketone meter, and the dipstick guide the first decision, but the laboratory plasma glucose, the formal blood gas, and the urine culture carry the definitive answer. The clinician who trusts a single bedside value over the clinical picture, or who forgets the known interference and the timing errors, makes the error that this topic is built to prevent. The ISPAD 2022 diabetic ketoacidosis guideline is the central reference for the glucose and the ketone thresholds, and the American Academy of Pediatrics urinary tract infection guideline is the central reference for the urinalysis. [1]
The clinical settings span the emergency department, the ward, the neonatal and the paediatric intensive care, the diabetes outpatient clinic, and the rural and the remote service. The febrile infant, the vomiting child, the breathless and acidotic child, the neonate with the poor feeding, and the child with the known diabetes all trigger one or more of these tests. The same three devices sit in every paediatric resuscitation bay, and the skill of performing and interpreting them correctly is a core competency for the general paediatric trainee and the fellow. [2]
Classification
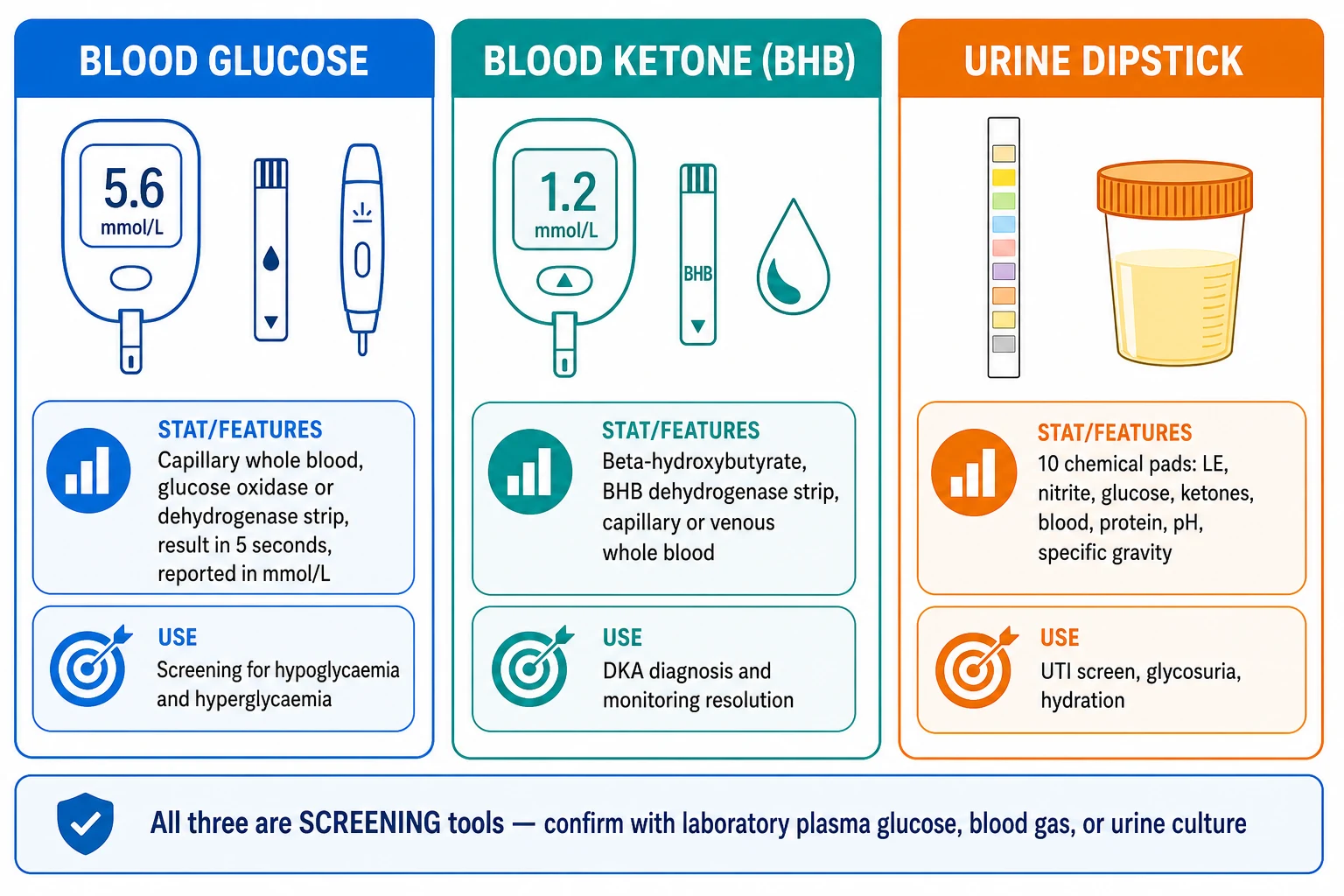
The classification rests on the specimen and the analyte. The glucose meter and the ketone meter share the whole-blood specimen from the capillary finger-prick or the heel-prick, and they share the electrochemical strip chemistry, but they measure two different analytes. The glucose strip uses the glucose oxidase or the glucose dehydrogenase enzyme to generate a current that is proportional to the glucose concentration, read in five seconds and reported in the millimoles per litre. The ketone strip uses the beta-hydroxybutyrate dehydrogenase enzyme to measure the beta-hydroxybutyrate, the predominant circulating ketone in the diabetic ketoacidosis. [1]
The urine dipstick is a third class because it runs on the urine rather than the blood, and it answers several questions at once on a single plastic strip. The standard ten-pad strip measures the specific gravity, the pH, the leukocyte esterase, the nitrite, the protein, the glucose, the ketones, the blood or the haemoglobin, the urobilinogen, and the bilirubin. The strip is read against the colour chart at the timed interval, usually sixty seconds for most pads, and the result is the semiquantitative colour change. The dipstick therefore covers the infection screen, the glycosuria and the ketonuria, the haematuria and the proteinuria, and the hydration in the one test. [2]
The clinical use separates the three tests further. The glucose meter is the first test in the unwell neonate, the child with the altered consciousness, and the child with the known or the suspected diabetes. The ketone meter is the first test in the child with the type one diabetes during the illness, the vomiting, or the high glucose, and it is the monitoring tool throughout the diabetic ketoacidosis treatment. The urine dipstick is the first test in the febrile child, the abdominal pain, and the dehydration, and it is the screen that decides whether the culture is needed. [1]
Epidemiology & Risk Factors
The three tests are among the commonest bedside investigations in paediatrics because the conditions they detect are common. The urinary tract infection is the most common serious bacterial infection in the febrile infant, with the prevalence of approximately seven percent in the febrile infant under two years and a higher prevalence in the febrile infant under three months, which makes the dipstick and the culture the daily practice in the emergency department. The type one diabetes affects approximately one in three hundred children by the age of eighteen, and the diabetic ketoacidosis is the presentation in fifteen to seventy percent of the new diagnoses, which makes the glucose and the ketone measurement the daily practice in the diabetes service. [3]
The risk factors for the glucose meter inaccuracy are concentrated in the neonate and the critically ill child. The high haematocrit of the neonate biases the reading, the low blood oxygen affects the glucose oxidase chemistry, and the galactose, the maltose, or the xylose in the blood cross-reacts with the glucose dehydrogenase pyrroloquinoline-quinone strips to give a falsely high reading. The neonate on the parenteral nutrition, the neonate with the galactosaemia, and the child receiving the maltose-containing immunoglobulin are the high-risk groups. The child in the shock, the severe dehydration, or the peripheral vasoconstriction gives a capillary reading that diverges from the venous or the arterial value. [6]
The risk factors for the misleading urine ketones are the recovery phase of the diabetic ketoacidosis and any state where the beta-hydroxybutyrate is converting to the acetoacetate. The urine pad measures the acetoacetate, and the conversion during the insulin therapy can keep the urine ketones high or even raise them while the blood beta-hydroxybutyrate falls, which is the source of the false reassurance or the false alarm. The dilute urine and the very frequent voiding in the young infant lower the nitrite sensitivity and are the risk factors for the false-negative dipstick. [8]
The epidemiology of the error matters because the falsely reassuring result changes the management in the wrong direction. The normal or the high glucose meter reading in the galactosaemic neonate, the negative nitrite in the infant with the Escherichia coli urinary tract infection, and the falling urine ketones that belie a persisting acidosis are the errors that the confirmatory laboratory test must catch. The general principle is that the bedside test is the first filter and the laboratory test is the arbiter, and the clinical condition of the child overrides both when they disagree. [6]
Pathophysiology
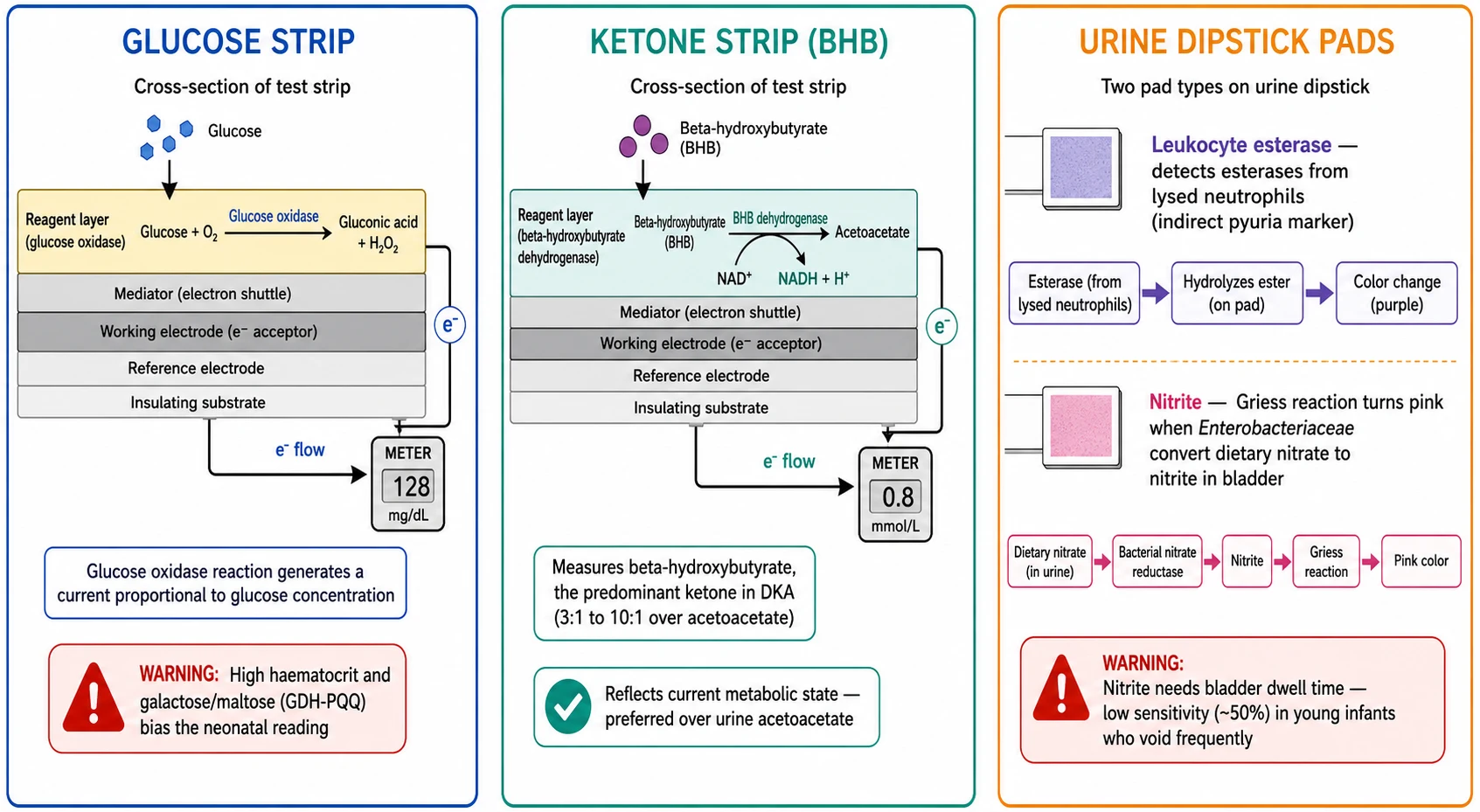
The glucose strip chemistry is the glucose oxidase or the glucose dehydrogenase reaction on the red-cell-rich whole blood. The glucose oxidase reaction converts the glucose to the gluconic acid and the hydrogen peroxide, and the electrons flow to the electrode to generate the current that the meter reads. The chemistry depends on the oxygen in some systems, which is the source of the oxygen interference in the high or the low oxygen states. The glucose dehydrogenase reaction does not depend on the oxygen, but the pyrroloquinoline-quinone variant cross-reacts with the galactose, the maltose, and the xylose, which is the source of the falsely high reading in the neonate on the parenteral nutrition or the maltose-containing product. [6]
The ketone strip chemistry is the beta-hydroxybutyrate dehydrogenase reaction that converts the beta-hydroxybutyrate to the acetoacetate and generates the measured current. The beta-hydroxybutyrate is the predominant ketone in the diabetic ketoacidosis because the hepatic ketogenesis in the insulin deficiency produces it at a three-to-one to ten-to-one ratio over the acetoacetate. The blood ketone meter therefore measures the analyte that reflects the current metabolic state and the severity of the ketosis, in contrast to the urine pad that measures the acetoacetate after it has been filtered and concentrated in the bladder over time. [1]
The dipstick pad chemistry is the colour-changing reaction that each pad performs on the urine. The leukocyte esterase pad detects the esterases released from the lysed neutrophils, which is the indirect marker of the pyuria. The nitrite pad uses the Griess reaction that turns pink when the Enterobacteriaceae have converted the dietary nitrate to the nitrite in the bladder. The glucose pad uses the glucose oxidase double-pad reaction that turns green in the glycosuria. The blood pad detects the haemoglobin and the myoglobin, and the protein pad detects the albumin at the trace level. Each reaction needs the timed read against the colour chart, and the delay or the early read biases the result. [5]
Clinical Presentation
The clinical presentations that trigger these tests are the everyday paediatric problems. The febrile infant, the child with the vomiting and the dehydration, the breathless and the acidotic child, the lethargic neonate, and the child with the polyuria and the polydipsia all prompt the bedside measurement. The first question is often answered at the triage or the bedside before the formal laboratory results return, and the speed is the value of the point-of-care test. The corollary is that the wrong bedside answer sends the management in the wrong direction, which is why the interpretation skill matters as much as the test itself. [2]
The glucose is triggered by the altered consciousness, the seizure, the poor feeding in the neonate, the insulin overdose, the known or the suspected diabetes, and the severe illness. The ketone is triggered by the high glucose reading, the vomiting, the abdominal pain, the rapid breathing, and the illness in the child with the type one diabetes. The urinalysis is triggered by the unexplained fever, the dysuria, the abdominal pain, the haematuria, and the dehydration assessment. Each trigger has its own threshold for the confirmatory test, and the trainee who learns the triggers learns when to reach for the device. [1]
The presentations that trigger the three point-of-care tests
The febrile infant under two years with no localising source, the default trigger for the urine dipstick and the culture
The breathless, vomiting, or abdominal pain in the child with the type one diabetes, the trigger for the glucose and the blood ketone
The lethargic or the poorly feeding neonate, the trigger for the capillary glucose with the laboratory confirmation
The child with the altered consciousness or the seizure, the trigger for the immediate capillary glucose
The dehydrated child, the trigger for the urine specific gravity and the ketones alongside the weight and the perfusion
The child in the resuscitation, the trigger for the bedside glucose and the blood gas as the first-line tests
The clinical context overrides the number. The well-appearing child with a borderline glucose is managed differently from the comatose child with the same number, and the child with the high glucose and the high ketones but the normal pH is the mild ketosis and not the ketoacidosis. The test is the input to the clinical judgement, and the trainee who treats the number and ignores the child makes the error that the structured assessment prevents. [1]
Differential Diagnosis
The differential at the point-of-care level is the choice of the test for the clinical question, and the choice of the confirmatory test when the bedside result is ambiguous. For the low glucose, the differential includes the true hypoglycaemia, the meter error from the haematocrit or the oxygen, and the interference from the galactose or the maltose. For the high glucose, the differential includes the true hyperglycaemia, the stress hyperglycaemia of the acute illness, and the diabetes. The confirmatory laboratory plasma glucose resolves each, and the clinical state of the child determines the urgency of the treatment while the result is awaited. [7]
For the ketones, the differential is the source and the timing. The physiological ketosis of the fasting or the vomiting gives a beta-hydroxybutyrate up to approximately three millimoles per litre, and the diabetic ketoacidosis gives a value greater than three with the acidosis. The urine ketones that stay high during the recovery are not a relapse but the conversion of the beta-hydroxybutyrate to the acetoacetate. The clinician who reads the urine ketone without the blood beta-hydroxybutyrate or the blood gas mistakes the lagging marker for the active ketosis. [8]
Blood beta-hydroxybutyrate
- The predominant ketone in the diabetic ketoacidosis
- Reflects the current metabolic state
- Falls with the insulin therapy and tracks the resolution
- Preferred over the urine ketone for the diagnosis and the monitoring
Urine acetoacetate
- The filtered ketone concentrated in the bladder
- Lags behind the blood beta-hydroxybutyrate
- Can rise during the recovery as the BHB converts to the acetoacetate
- Useful when the blood ketone meter is unavailable
Blood glucose meter
- The first test in the suspected hyperglycaemia or hypoglycaemia
- Confirms the hyperglycaemia of the diabetes
- Biased by the haematocrit and the galactose or maltose interference in the neonate
- Confirm the critical value with the laboratory plasma glucose
Urine dipstick
- The first screen for the urinary tract infection and the glycosuria
- The leukocyte esterase and the nitrite as the infection markers
- A screen and not a culture
- The both-negative result lowers the probability of the infection
The third distinction is the screen versus the confirmatory test. The dipstick screens for the infection but the culture confirms it. The glucose meter screens for the dysglycaemia but the laboratory plasma glucose confirms it. The ketone meter monitors the trend but the blood gas confirms the acidosis. The trainee who stops at the screen and treats on the bedside result alone forgoes the definitive test, and the trainee who waits for the laboratory result when the child is collapsing forgoes the speed. The balance is the bedside test for the immediate decision and the laboratory test for the definitive answer, run in parallel. [2]
Clinical & Bedside Assessment
The bedside assessment before the test confirms the indication, the right specimen, and the device check. Confirm the indication for the glucose, the ketone, or the urinalysis. Check the device is in date, the strips are in date and from the same container, and the quality control has been run on the schedule. For the glucose, warm the periphery, clean the finger or the heel, and use the first or the second drop of the free-flowing blood, not the squeezed or the milking attempt that dilutes the sample with the tissue fluid. [7]
The specimen handling for the urine dipstick is the foundation of the correct result. Collect the fresh urine, ideally within the one to two hours, because the leukocyte esterase and the nitrite degrade with the time and the bacterial overgrowth. The clean catch is the first-line for the toilet-trained child, the catheterisation or the suprapubic aspiration for the non-toilet-trained child, and the bag only for the screen. Dip the strip fully, tap off the excess, and read the pads at the timed interval against the colour chart, because the early or the late read biases the colour. [10]
The interpretation is always in the clinical context. Read the number alongside the heart rate, the perfusion, the consciousness, and the hydration. The low glucose in the well neonate who is feeding is managed differently from the low glucose in the convulsing neonate. The high ketone in the child with the normal pH is the mild ketosis, and the high ketone with the acidosis is the ketoacidosis. The positive leukocyte esterase with the fever and the abdominal pain is the probable infection, and the isolated trace in the well child is the contamination or the false positive. The clinical picture assigns the weight to the number. [1]
Investigations
The investigation hierarchy for each bedside test is the screen followed by the confirmatory measurement. The glucose meter is confirmed by the laboratory plasma glucose, which is the gold standard because the plasma separation removes the haematocrit bias and the laboratory analyser has the tighter precision. The capillary whole-blood glucose reads approximately ten to twelve percent lower than the plasma glucose because the red cells contain less glucose than the plasma, and the clinician must know whether the device reports the whole-blood or the plasma-calibrated value. [6]
The blood beta-hydroxybutyrate is confirmed by the venous blood gas and the formal biochemistry, and the blood gas adds the pH and the bicarbonate that define the acidosis. The ISPAD 2022 diabetic ketoacidosis definition combines the glucose greater than eleven millimoles per litre, the venous pH under 7.3 and the bicarbonate under fifteen millimoles per litre, and the beta-hydroxybutyrate greater than three millimoles per litre or the moderate-to-large ketonuria. The severity is graded by the pH, with the mild at 7.2 to 7.3, the moderate at 7.1 to 7.2, and the severe under 7.1. [1]
The urinalysis by the dipstick and the microscopy gives the immediate preliminary result, and the culture gives the definitive result. The positive leukocyte esterase raises the probability of the infection, and the positive nitrite raises it further, but the febrile non-toilet-trained child needs the culture from the catheterisation or the suprapubic aspiration regardless of the dipstick, because the dipstick is a screen. The microscopy of greater than five to ten white cells per high-power field supports the infection, and the bacteria on the unspun Gram stain supports it further. The culture threshold for the catheter specimen is the single organism at greater than ten thousand to fifty thousand colony-forming units per millilitre. [2]
Management — Resuscitation
The procedural management begins with the preparation, the specimen, and the device check. Gather the equipment: the glucose meter and the strips, the ketone meter and the strips, the lancet and the sterile lancet device, the alcohol swab, the urine dipstick and the colour chart, the specimen pot, and the gloves. Warm the periphery of the cold child before the capillary sample, because the peripheral vasoconstriction gives the poor flow and the biased reading. Use the non-pharmacological comfort for the infant, and the explanation and the distraction for the older child. [7]
The capillary sample is taken from the side of the fingertip in the older child and the heel in the neonate and the young infant. Clean the site, allow it to dry, lance, wipe the first drop, and apply the second drop of the free-flowing blood to the strip. The milking or the squeezing dilutes the sample with the tissue fluid and biases the reading low. The neonatal heel-prick uses the warmed heel and the lateral plantar surface, and the puncture depth is limited to avoid the calcaneal osteomyelitis. The capillary glucose is read in five seconds, and the capillary ketone is read in ten to thirty seconds. [6]
Capillary sampling for the glucose and the ketone meter in the child
Dose
One drop of the free-flowing capillary whole blood applied to the reagent strip, volume approximately 1 microlitre for the glucose and approximately 1 to 5 microlitres for the ketone
The urine dipstick is dipped into the fresh urine immediately after the collection. The fully immersed strip is tapped to remove the excess, and the pads are read at the timed interval against the colour chart, usually the leukocyte esterase and the nitrite at sixty seconds. The delayed read overestimates the colour, and the early read underestimates it. The result is recorded with the time and the specimen type, and the culture is sent from the same specimen when the dipstick is positive or the clinical suspicion is high. [10]
Management — Definitive & Stepwise
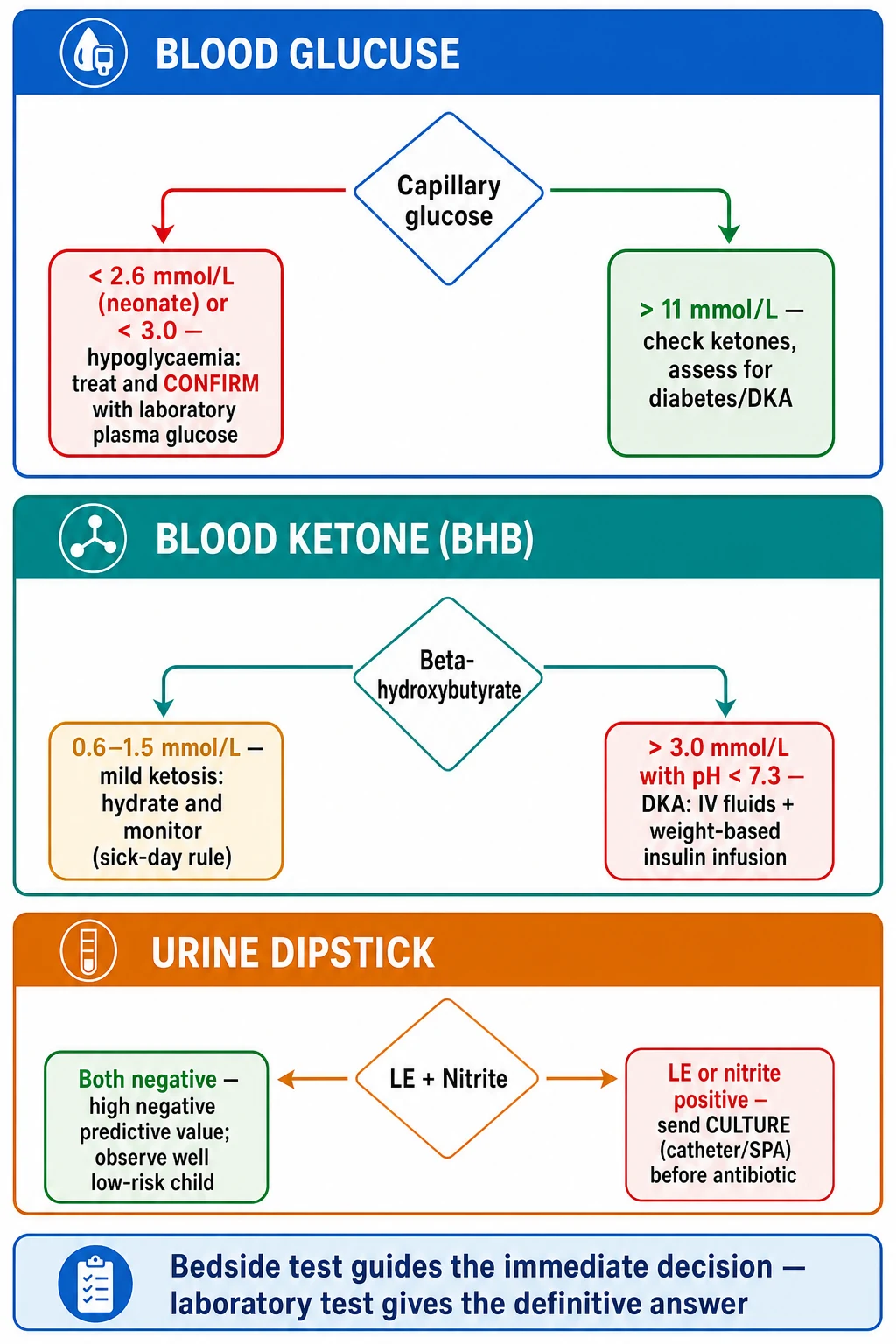
[1]The definitive stepwise management for the glucose is the confirmation of the critical value and the treatment of the symptomatic child. The operational treatment threshold for the neonatal hypoglycaemia is the commonly used value of under 2.6 millimoles per litre, confirmed by the laboratory plasma glucose, and the symptomatic neonate is treated while the result is awaited. The high glucose is interpreted alongside the ketones and the clinical state, and the child with the glucose over eleven and the ketones over three millimoles per litre is assessed for the diabetic ketoacidosis with the venous blood gas. The stress hyperglycaemia of the acute illness resolves with the treatment of the underlying condition and does not need the insulin. [1]
The definitive stepwise management for the ketone is the ISPAD sick-day rule and the diabetic ketoacidosis protocol. The child with the type one diabetes checks the ketones when the glucose is over fourteen millimoles per litre or during the illness, the fever, or the vomiting. The beta-hydroxybutyrate under 0.6 millimoles per litre needs no action, the 0.6 to 1.5 needs the hydration and the monitoring, and the over 3.0 with the acidosis needs the intravenous fluids and the weight-based insulin infusion per the local diabetic ketoacidosis protocol. The blood ketone is preferred over the urine ketone for the monitoring, and the fall of the beta-hydroxybutyrate is the marker of the resolution. [8]
The definitive stepwise management for the urinalysis is the culture and the antibiotic stewardship. The febrile non-toilet-trained child with the positive leukocyte esterase or the nitrite obtains the culture from the catheterisation or the suprapubic aspiration before the antibiotic, and the antibiotic is started on the clinical probability while the culture is awaited. The well-appearing toilet-trained child with the both-negative dipstick and the low clinical probability may be observed without the antibiotic, because the negative predictive value of the combined leukocyte esterase and nitrite is high. The symptomatic child with the dipstick and the microscopy supporting the infection is treated as the probable urinary tract infection pending the culture. [2]
Specific Subtypes & Scenarios
The neonate is the highest-risk group for the glucose meter error. The high haematocrit, the low haematocrit, the variable oxygen, and the galactose or maltose interference all bias the reading, and the symptomatic neonate needs the laboratory plasma glucose to confirm. The improved point-of-care glucose monitoring in the neonatal intensive care using the interference-corrected meter such as the Nova StatStrip gives the better accuracy, the better sensitivity, and the reduced test utilisation compared with the uncorrected meter. The capillary ketone in the early neonate is also a useful marker of the inadequate breast-milk intake, with the rising ketone signalling the underfeeding before the hypoglycaemia. [11]
KETONE for the blood ketone over the urine ketone in the diabetic ketoacidosis
The child with the type one diabetes uses the blood ketone meter at home during the illness and the high glucose, and the home measurement of the beta-hydroxybutyrate guides the sick-day management in the child under five as well as the older child. The clinical utility of the home beta-hydroxybutyrate in the physiological ketosis of the child under five has been demonstrated, and the meter empowers the family to act early and to avoid the progression to the ketoacidosis. The blood-versus-urine ketone comparison in the adolescent and the child with the diabetic ketoacidosis shows the blood ketone tracks the therapeutic response more closely than the urine ketone. [9]
[2]Complications & Pitfalls
The complications of the bedside testing are the procedural and the interpretive. The procedural complications of the capillary sample are the pain, the bruising, and the rare infection at the puncture site, and the neonatal heel-prick carries the small risk of the calcaneal osteomyelitis when the puncture is too deep. The procedural complications of the urine dipstick are minimal. The interpretive complications are the false reassurance and the false alarm, and these are the commoner and the more dangerous errors. [7]
The classic interpretive pitfalls are the five that this topic is built to prevent. The first is the trust in a single neonatal glucose meter reading without the laboratory confirmation, which sends the management in the wrong direction in the galactosaemic or the parenteral-nutrition neonate. The second is the reassurance from the falling urine ketones during the recovery from the diabetic ketoacidosis, when the acetoacetate can rise as the beta-hydroxybutyrate converts. The third is the exclusion of the urinary tract infection from a negative nitrite in the young infant, when the frequent voiding lowers the nitrite sensitivity to approximately fifty percent. The fourth is the diagnosis of the urinary tract infection from the dipstick alone, when the febrile non-toilet-trained child needs the culture. The fifth is the miss of the euglycaemic diabetic ketoacidosis, when the glucose is under eleven and the ketone and the blood gas make the diagnosis. [8]
The systematic review by St John and colleagues of the urinary dipstick tests to exclude the urinary tract infection confirmed that the combined leukocyte esterase and nitrite result carries the high negative predictive value that supports the rule-out in the low-risk child, and the meta-analysis by Gorelick and Shaw of the screening tests for the urinary tract infection in children established the performance of the individual pads. The clinical application is that the both-negative dipstick in the well, low-risk child supports the observation, but the positive dipstick or the high-risk child needs the culture. [5]
Prognosis & Disposition
The prognosis after the bedside testing is the prognosis of the condition the test detects, modified by the speed and the accuracy of the interpretation. The rapid bedside glucose in the hypoglycaemic seizure that leads to the immediate treatment improves the outcome, and the delayed or the wrong reading worsens it. The rapid bedside ketone that triggers the early rehydration in the sick child with the type one diabetes prevents the progression to the severe ketoacidosis. The accurate dipstick that leads to the well-collected culture gives the correct diagnosis and the targeted antibiotic. [1]
The disposition is set by the clinical condition and the trend. The child with the mild ketosis and the falling beta-hydroxybutyrate is managed at home with the sick-day plan and the close contact. The child with the moderate-to-severe diabetic ketoacidosis is admitted to the high-dependency or the intensive care for the protocolised fluids and the insulin. The febrile infant with the positive dipstick is managed with the culture and the empirical antibiotic pending the result, and the well child with the negative dipstick is observed with the safety-net advice. The bedside test sets the first disposition, and the confirmatory test and the clinical trend refine it. [8]
The follow-up for the child with the diabetes addresses the sick-day education, the ketone meter technique, and the prevention of the recurrence. The follow-up for the child with the urinary tract infection addresses the imaging for the recurrent or the atypical infection, the renal function, and the blood pressure. The follow-up for the neonate with the hypoglycaemia addresses the feeding, the glucose trend, and the underlying cause. Each bedside test opens a clinical pathway, and the accurate interpretation at the start sets the direction of the whole pathway. [2]
Special Populations
The neonate is the special population for the glucose meter, because the haematocrit, the oxygen, and the galactose or maltose interference are all greatest in this age group, and the symptomatic hypoglycaemia carries the neurodevelopmental risk. The laboratory plasma glucose is the confirmatory test for any critical or unexpected capillary value, and the interference-corrected meter is the preferred device where it is available. The capillary ketone in the early neonate signals the inadequate breast-milk intake before the hypoglycaemia, and the early feeding support prevents the progression. [6]
The child with the type one diabetes is the special population for the ketone meter, and the home beta-hydroxybutyrate measurement empowers the family to manage the sick days and to prevent the ketoacidosis. The child under five and the adolescent both benefit from the home ketone monitoring, and the diabetes service provides the meter, the strips, and the education. The child with the recurrent diabetic ketoacidosis needs the structured education and the psychosocial support, because the recurrence is often the marker of the adherence or the psychosocial difficulty. [9]
The child with the complex chronic and the technology-dependent condition has the repeated exposure to the bedside testing and the higher risk of the meter and the dipstick error from the altered perfusion, the altered haematocrit, and the repeated courses of the antibiotic that change the urine flora. The threshold for the confirmatory laboratory test is lower in this group. Aboriginal and Torres Strait Islander children and the children from the remote settings have the higher burden of the serious bacterial infection and the lower access to the laboratory, and the accurate bedside testing combined with the clear threshold for the retrieval is the standard of care. [3]
Evidence, Guidelines & Regional Differences
The evidence base spans the international guidelines, the device-accuracy studies, and the diagnostic-accuracy reviews. The ISPAD 2022 clinical practice consensus guidelines on the diabetic ketoacidosis and the hyperglycaemic hyperosmolar state define the diagnostic thresholds and recommend the blood beta-hydroxybutyrate over the urine ketone for the diagnosis and the monitoring. The glucose greater than eleven millimoles per litre, the venous pH under 7.3, the bicarbonate under fifteen, and the beta-hydroxybutyrate greater than three are the combined criteria, and the severity is graded by the pH. [1]
The device-accuracy studies in the neonate established the inaccuracy of the uncorrected glucose meter and the benefit of the interference-corrected meter. The study by Raizman and colleagues of the Nova StatStrip in the neonatal intensive care showed the improved accuracy, the better sensitivity, and the reduced test utilisation, and the study by Wada and colleagues of the two glucose meters and the interference corrections for the screening of the neonatal hypoglycaemia quantified the bias that the interference correction reduces. The meta-analysis by Gorelick and Shaw and the systematic review by St John and colleagues established the performance of the urine dipstick for the rule-out of the urinary tract infection. [6]
ISPAD 2022
- Pediatric diabetes consensus guideline
- DKA defined by the glucose over 11, the pH under 7.3, and the BHB over 3 mmol per litre
- Blood beta-hydroxybutyrate over the urine ketone for the diagnosis and the monitoring
- Severity graded by the pH
AAP 2011
- Pediatrics clinical practice guideline
- Dipstick is a screen and the culture confirms the infection
- Urine by the catheterisation or the suprapubic aspiration before any antibiotic in the febrile infant
- Reaffirmed in 2016
Gorelick 1999
- Pediatrics meta-analysis of the screening tests
- Established the performance of the LE and the nitrite pads
- The combined result carries the high negative predictive value
Raizman 2016
- Clinical biochemistry device study
- The interference-corrected meter improves the neonatal accuracy
- Better sensitivity and reduced test utilisation in the NICU
The diagnostic-accuracy evidence for the urinalysis includes the meta-analysis by Shaikh and colleagues of the prevalence of the urinary tract infection in childhood and the review by Diviney and colleagues of the urine collection methods and the dipstick testing in the non-toilet-trained children. The blood-versus-urine ketone comparison by Pulungan and colleagues and the home beta-hydroxybutyrate study by Vanelli and colleagues established the clinical utility of the blood ketone in the management of the ketosis. The capillary ketone study by Futatani and colleagues in the early neonate extended the use to the marker of the inadequate breast-milk intake. [8]
The regional differences centre on the device availability, the local protocol for the diabetic ketoacidosis, and the access to the laboratory confirmation. In the well-resourced settings, the interference-corrected glucose meter and the blood ketone meter are the standard, and the laboratory plasma glucose and the venous blood gas are readily available for the confirmation. In the lower-resource and the remote settings, the uncorrected glucose meter and the urine dipstick are more common, and the threshold for the retrieval to the higher-level care is lower. The international guidelines, including the ISPAD and the AAP, are applicable across the settings, with the intensity of the confirmation and the monitoring tailored to the local resources. [3]
Exam Pearls
GLUCOSE for the neonatal glucose meter limitations
References
- [1]Glaser N, Kuppermann N, Yuen M, et al ISPAD clinical practice consensus guidelines 2022: Diabetic ketoacidosis and hyperglycemic hyperosmolar state Pediatric Diabetes, 2022.PMID 36250645
- [2]Subcommittee on Urinary Tract Infection, Roberts KB Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months Pediatrics, 2011.PMID 21873693
- [3]Shaikh N, Morone NE, Lopez J, et al Prevalence of urinary tract infection in childhood: a meta-analysis Pediatric Infectious Disease Journal, 2008.PMID 18316994
- [4]Gorelick MH, Shaw KN Screening tests for urinary tract infection in children: a meta-analysis Pediatrics, 1999.PMID 10545580
- [5]St John A, Boyd JC, Lowes AJ, Price CP The use of urinary dipstick tests to exclude urinary tract infection: a systematic review of the literature American Journal of Clinical Pathology, 2006.PMID 16880133
- [6]Raizman JE, Dearras L, Sikaria K, et al Clinical impact of improved point-of-care glucose monitoring in neonatal intensive care using Nova StatStrip: evidence for improved accuracy, better sensitivity, and reduced test utilization Clinical Biochemistry, 2016.PMID 27157715
- [7]Wada Y, Nakamura M, Mitsui M, et al Evaluation of two glucose meters and interference corrections for screening neonatal hypoglycemia Pediatrics International, 2015.PMID 25441549
- [8]Pulungan AB, Tridjaja B, Pulungan L, et al Diabetic ketoacidosis in adolescents and children: a prospective study of blood versus urine ketones in monitoring therapeutic response Acta Medica Indonesiana, 2018.PMID 29686175
- [9]Vanelli M, Gualandi S, Scipione M, et al Clinical utility of beta-hydroxybutyrate measurement in the management of physiological ketosis at home in children under 5 Acta Bio-Medica, 2019.PMID 31124998
- [10]Diviney J, Puar T, Ladhani S, et al Urine collection methods and dipstick testing in non-toilet-trained children Pediatric Nephrology, 2021.PMID 32918601
- [11]Futatani T, Shimizu Y, Yorifuji T, et al Capillary blood ketone levels as an indicator of inadequate breast milk intake in the early neonatal period Journal of Pediatrics, 2017.PMID 29173326