Paeds · investigations-procedures-and-technology
Safe paediatric procedural sedation
Also known as Paediatric procedural sedation · Conscious sedation in children · Ketamine sedation · Nitrous oxide sedation · Dissociative sedation · Procedural sedation and analgesia
A fellowship approach to procedural sedation and analgesia in children, covering the continuum of sedation depth from minimal through moderate and deep sedation to general anaesthesia, the paediatric airway and ventilatory physiology that makes children vulnerable, the pre-sedation assessment (ASA physical status, airway, fasting and weight), the mandatory monitoring and rescue equipment, and the exact doses of ketamine (intravenous 1 to 1.5 milligrams per kilogram, intramuscular 4 to 5 milligrams per kilogram) and nitrous oxide 50 percent in oxygen. The page teaches the evidence that fasting status does not substitute for monitoring, the early detection of hypoventilation by capnography, the prevention and management of adverse events such as vomiting, emergence phenomena, laryngospasm and apnoea, the reversal agents naloxone and flumazenil, and the recovery and discharge criteria using the modified Aldrete score.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a five-year-old in the emergency department with a displaced forearm fracture, screaming in pain every time you touch the arm. To reduce and splint it safely you need the child still, calm and analgessed — but you do not want to take away their breathing. This is the everyday problem procedural sedation solves, and doing it safely is one of the most testable skills in paediatric fellowship examinations. [1]
Procedural sedation and analgesia is the deliberate, monitored depression of consciousness so that a diagnostic or therapeutic procedure can be performed, while the child's protective airway reflexes, spontaneous ventilation and cardiovascular function are preserved. The definition has two parts that sit in tension: you lower consciousness enough to make the procedure possible, but you do not lower it so far that the airway, breathing or circulation fail. The skill is choosing the depth and the agent that match the procedure and the child, and then guarding the child through it. [1] [4]
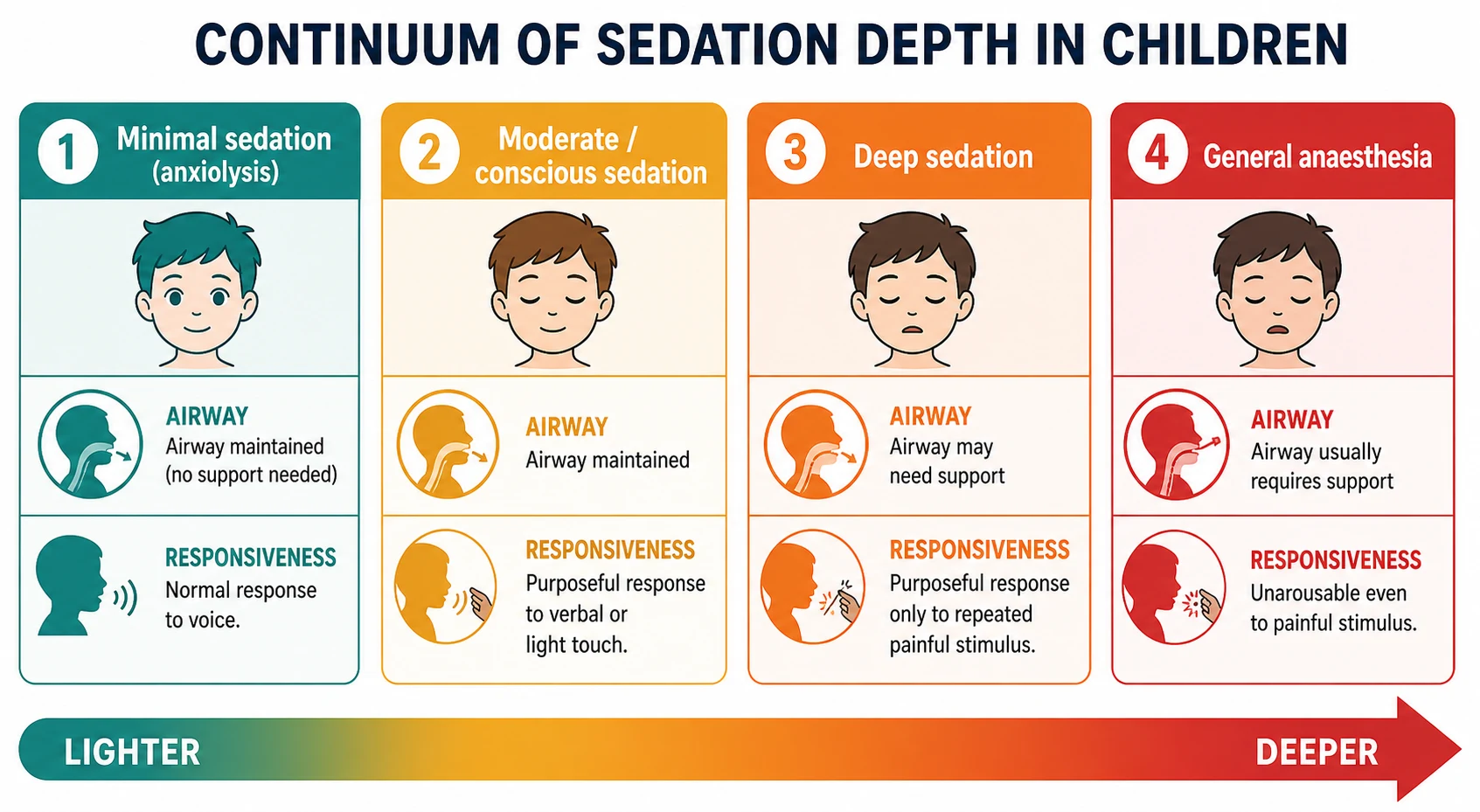
The crucial idea is that sedation is a continuum, not a switch. The American Society of Anesthesiologists and the joint American Academy of Pediatrics and American Academy of Pediatric Dentistry guidelines define four levels that shade into one another. In minimal sedation (anxiolysis) the child responds normally to voice and breathing and circulation are unaffected. In moderate or conscious sedation the child shows purposeful response to verbal command or light tactile stimulation, the airway stays open, and spontaneous ventilation is adequate. In deep sedation the child responds only purposefully to repeated or painful stimulation, the airway may need active support, and spontaneous ventilation may become inadequate. In general anaesthesia the child is unarousable even to painful stimulus, the airway usually cannot be maintained without intervention, and ventilation is frequently inadequate. The reason this matters at the bedside is that deep sedation and general anaesthesia carry the risk of airway loss and therefore require anaesthetic-level training — a proceduralist working alone must not go there. [4]
Classification
The candidate should classify sedation along two axes at once: the depth of central nervous system depression, and the pharmacological class of the agent. The two axes interact, because the agent partly determines how safely a given depth can be reached. [4]
By depth, the four ASA levels are the framework above, and the examiner rewards the candidate who can quote the responsiveness, airway and ventilation criterion for each rather than just the name. The dangerous boundary is the one between moderate and deep sedation, because moderate sedation can be supervised by a trained procedural team whereas deep sedation behaves pharmacologically like general anaesthesia and demands anaesthetic competence and the capacity to rescue an airway. A useful working rule is that if you would need to support the airway, you are in anaesthetic territory. [4]
By agent, paediatric procedural sedation falls into four practical families. Dissociative sedation with ketamine sits slightly apart: it produces a cataleptic state in which the eyes remain open, the airway reflexes and muscle tone are largely preserved, and profound analgesia coexists with apparent wakefulness, so it does not map neatly onto the moderate-to-deep continuum. Inhalational sedation with nitrous oxide 50 percent in oxygen gives light, rapidly reversible sedation and analgesia that sits at the minimal-to-moderate end. Benzodiazepines such as midazolam provide anxiolysis and amnesia with little analgesia, and propofol and other hypnotics produce deep sedation approaching anaesthesia and are generally reserved for anaesthetically trained providers in children. The combination of an opioid (fentanyl) with a sedative is particularly hazardous because each potentiates the other's respiratory depression. [1] [3]
Epidemiology & Risk Factors
Procedural sedation is among the commonest interventions performed on children outside the operating room — in emergency departments, oncology units, radiology suites and dental practices — and the central reassuring fact is that serious adverse events are rare when it is done by trained teams with proper monitoring. The Pediatric Sedation Research Consortium reported on tens of thousands of cases across North American centres and found that while minor events such as transient oxygen desaturation and vomiting occur in a few percent of cases, events serious enough to threaten the child — apnoea requiring intervention, laryngospasm, cardiac arrest — are uncommon. [2]
The child who is likely to come to harm is predictable, and the risk assessment is exactly what the examiner probes. The single most powerful predictor is ASA physical status: a child who is ASA I or II (healthy, or with mild systemic disease) tolerates sedation well, whereas a child who is ASA III or above (severe systemic disease) carries a several-fold higher risk of adverse events and generally needs anaesthetic input. [2] [4] Age matters: infants under one year are at higher risk of apnoea, hypoxia and airway obstruction, and sedation in this group usually requires anaesthetic involvement and a higher level of monitoring and recovery. A recent upper respiratory tract infection increases the risk of laryngospasm and airway reactivity, particularly with agents that irritate the airway. Other high-risk features include obesity and sleep-disordered breathing (airway obstruction), complex or uncorrected congenital heart disease, neuromuscular disease with weak respiratory muscles, and any known difficult airway. [1] [4]
Pathophysiology
The reason sedation can harm a child is that the same central nervous system depression that calms and immobilises the child also depresses the systems that keep them alive. Understanding the cascade lets you anticipate it, monitor for it, and rescue it before it becomes hypoxia. [1]
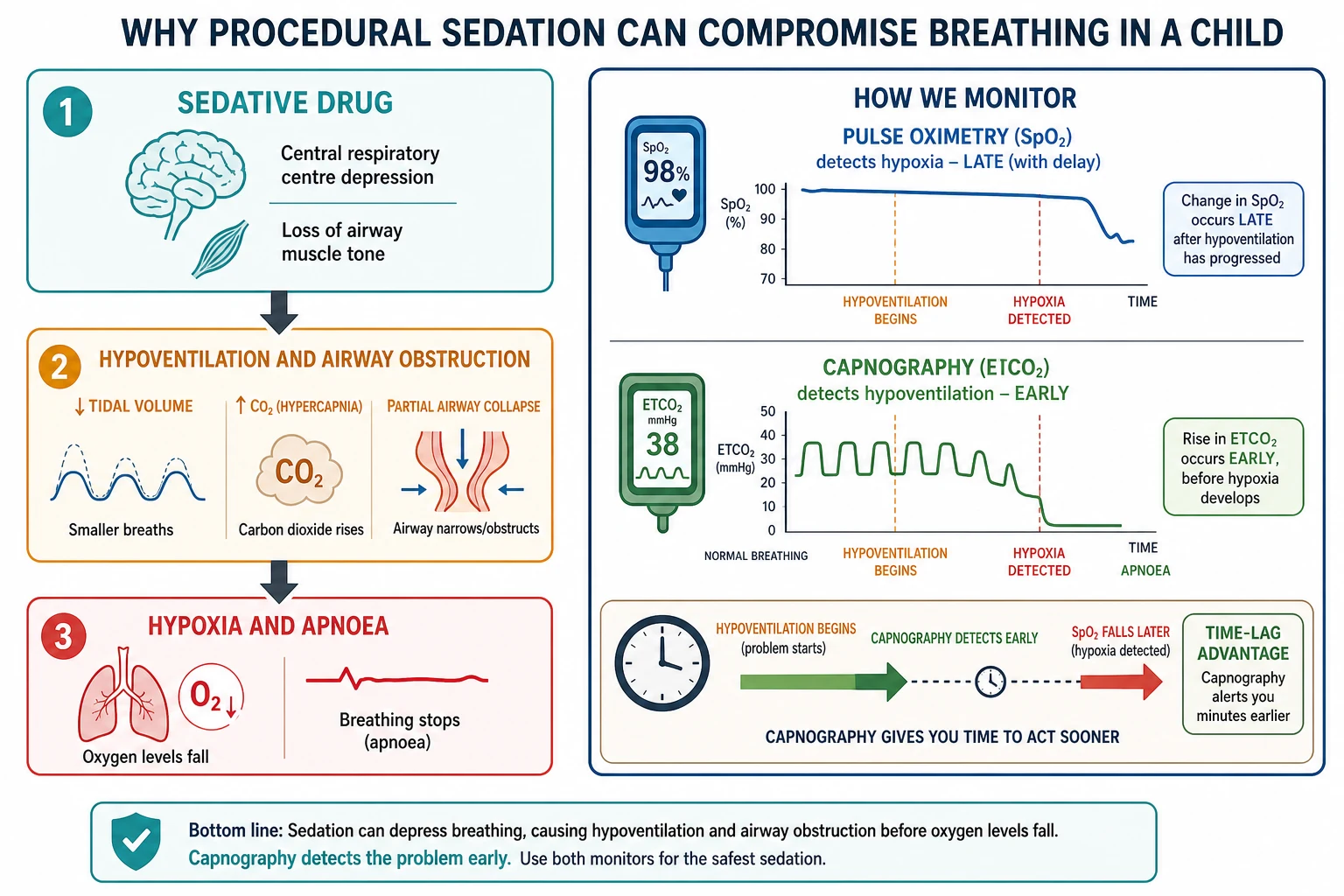
Every sedative agent depresses the central respiratory centre in the brainstem, reducing both the drive to breathe and the response to a rising carbon dioxide. At the same time, most agents reduce the tone of the pharyngeal and laryngeal muscles, so the upper airway narrows and can obstruct, especially in the small child whose airway is already narrow and who may be an obligate nose-breather. The first consequence is hypoventilation: the tidal volume falls and the carbon dioxide begins to rise, often for minutes before the oxygen saturation drops. Only later, as hypoventilation and airway obstruction progress, does hypoxia develop, and untreated hypoventilation proceeds to apnoea. This sequence — drive depression, airway obstruction, hypoventilation, hypoxia, apnoea — is the pathophysiology the monitoring is designed to catch early. [1] [4]
The child is more vulnerable than the adult for three physiological reasons. First, the functional residual capacity of the small lung is low relative to oxygen consumption, so the oxygen reserve is exhausted quickly once ventilation falls. Second, infants have a small tidal volume and a high respiratory rate, so even a small reduction in tidal volume produces a large proportional drop in alveolar ventilation. Third, the obligate nose-breathing infant with a short neck, large tongue and adenotonsillar tissue obstructs readily once pharyngeal tone is lost. These three facts explain why a child can desaturate within a minute or two of oversedation and why vigilance cannot be relaxed. [1]
This physiology also explains the central monitoring principle of the topic. Pulse oximetry measures arterial oxygen saturation, so it falls only after hypoventilation has progressed far enough to drop the alveolar oxygen — and supplemental oxygen masks the fall further by keeping the saturation normal even as the carbon dioxide climbs. Capnography, by measuring exhaled carbon dioxide, detects the rising carbon dioxide of hypoventilation directly and minutes earlier than the oximeter detects the hypoxia. A randomised trial of capnography during paediatric sedation showed it detects hypoventilation that oximetry misses. This is why capnography is the preferred ventilatory monitor and why relying on pulse oximetry alone is a recognised pitfall. [10] [4]
Clinical Presentation
The "presentation" in this topic is the clinical scenario that prompts a sedation decision, and the examiner constructs these deliberately because the right answer changes with the procedure and the child. The cardinal scenarios are the brief painful procedure — laceration repair, fracture or dislocation reduction, abscess drainage, burn dressing change, lumbar puncture or joint aspiration — and the immobility-dependent procedure such as magnetic resonance imaging or computed tomography, where analgesia is irrelevant and the goal is stillness. [1]
The history the operator must take before any drug is given is itself the clinical assessment, and it has a fixed shape. Ask about the procedure to be performed and the anticipated duration and pain, the child's age and weight in kilograms for dosing, the fasting history (last solid food, last clear fluid, last breastfeed), any recent upper airway infection or wheeze, snoring or sleep-disordered breathing, reflux or vomiting, previous sedation or anaesthetic problems, allergies, and the past medical history that feeds the ASA physical status. A focused airway assessment — mouth opening, neck movement, mandibular recession, visible tonsils, any stridor — flags the child in whom the airway may be difficult to rescue. [4]
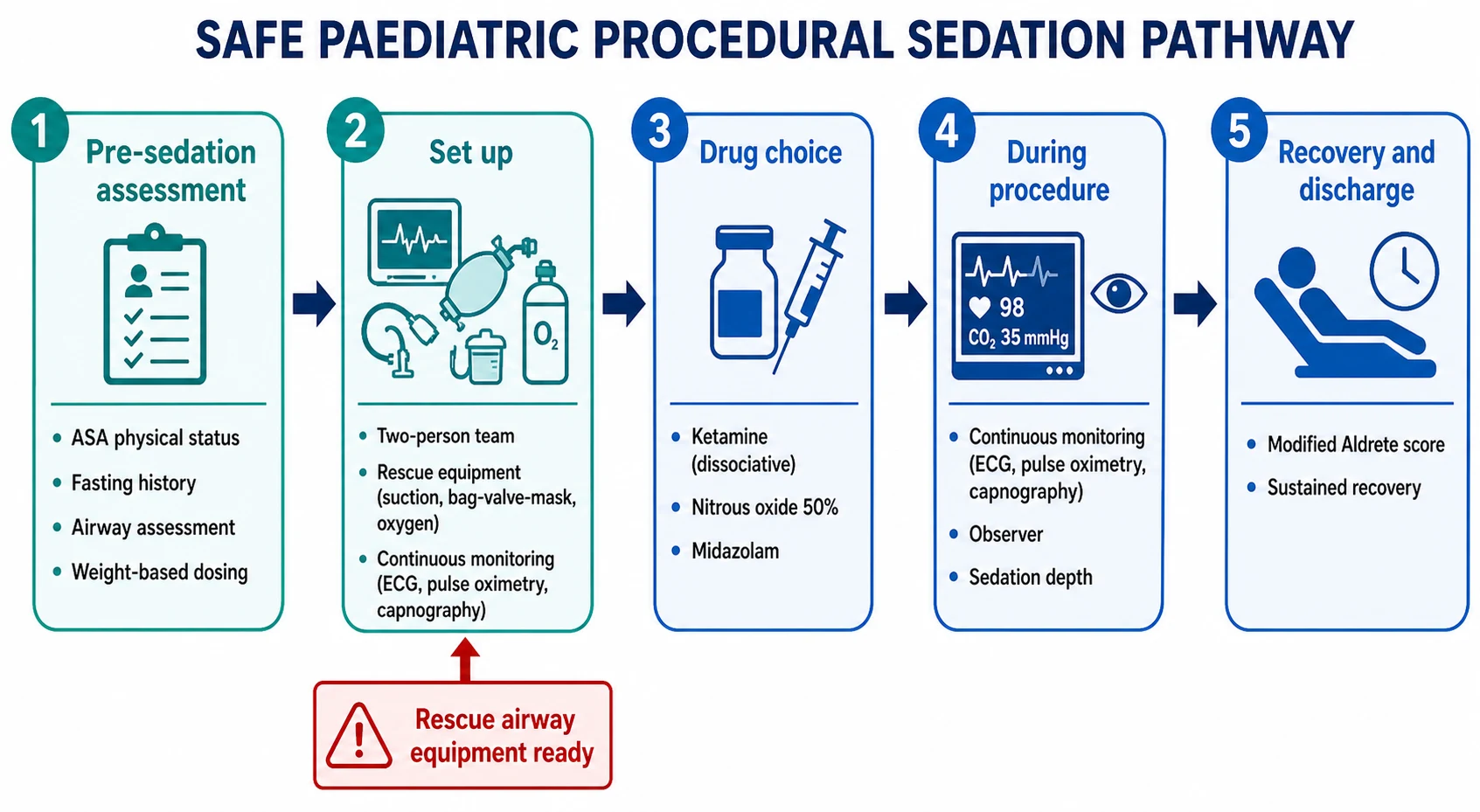
At the bedside, before any drug is drawn up, the operator deliberately confirms five things: the weight-based dose has been checked by two people, a two-person team is present (one to sedate and observe, one to perform the procedure), rescue airway equipment (suction, bag-valve-mask, age-appropriate oropharyngeal and nasopharyngeal airways, oxygen) is at the bedside, continuous monitoring is attached and a baseline is recorded, and vascular access is secured where the chosen agent or the child's status requires it. The approach for the technology-dependent or neurodivergent child who cannot cooperate is individualised, often with senior or anaesthetic input and a written plan. [4]
Differential Diagnosis
In a procedural-sedation stem, "differential diagnosis" means the decision between levels of intervention rather than a list of diseases, and the candidate who frames it as a ladder earns marks. At the bottom rung are non-pharmacological measures alone — distraction, play therapy, parental presence, comforting positioning (such as the seated parent's lap) — which suffice for many minor procedures in a cooperative child. The next rung adds topical or local anaesthesia (for example, a topical amethocaine or lidocaine preparation for venepuncture or laceration repair). Above that sits inhaled nitrous oxide for brief, moderately painful procedures, then dissociative ketamine for deeper or longer painful procedures, and at the top deep sedation or general anaesthesia, which belongs in theatre or with an anaesthetist. [1] [7]
The features that push a child up the ladder toward anaesthetic support are exactly the high-risk features named earlier. A child who is ASA III or above, who has an active upper airway infection with stridor, significant obesity or sleep-disordered breathing, complex cardiac disease, or neuromuscular respiratory weakness is not a candidate for sedation by a proceduralist alone. Likewise a child with active vomiting or a proven full stomach at high aspiration risk, or an infant under one year needing deep sedation, is better served by an anaesthetist. [4]
A different kind of "differential" sits in recovery: the team must distinguish acceptable emergence phenomena — vivid dreams, mild agitation or confusion on waking from ketamine, which settle with reassurance — from a true adverse event such as laryngospasm (stridor, paradoxical movement, falling saturation), apnoea, hypoglycaemia in the fasted infant, or anaphylaxis. The first is watched and comforted; the others demand immediate escalation. [3] [4]
Non-pharmacological + topical
Minor procedure, cooperative child
- Distraction, play therapy, parental presence
- Topical amethocaine or lidocaine
- No airway risk, no monitoring beyond observation
- Venepuncture, simple suturing, dressing change
Nitrous oxide 50%
Brief moderate procedure
- Light sedation and analgesia
- Onset minutes, recovery minutes after stopping
- Contraindicated in pneumothorax, bowel obstruction
- Often combined with intranasal fentanyl
Ketamine (dissociative)
Painful procedure needing stillness
- IV 1 to 1.5 mg/kg, IM 4 to 5 mg/kg
- Preserves airway reflexes and sympathetic tone
- Vomiting and emergence phenomena common
- Avoid in infancy, raised ICP, active URI
Deep sedation or GA
High-risk child or long immobile procedure
- Requires anaesthetic-level training
- Airway and ventilation likely need support
- Theatre or anaesthetist present
- ASA III or above, infant, difficult airway
Clinical & Bedside Assessment
The pre-sedation assessment is the most directly testable part of the topic because every guideline makes it the gate the child must pass before a drug is given. It has a fixed structure that the candidate should be able to recite. [4]
Begin with the ASA physical status classification, because it is the single best predictor of risk. ASA I is a healthy child, ASA II a child with mild systemic disease (for example, well-controlled asthma), ASA III a child with severe systemic disease, ASA IV a child with severe systemic disease that is a constant threat to life, ASA V a moribund child, and ASA VI an organ donor. The practical cut-off is that ASA I and II children are suitable for procedural sedation by a trained team, while ASA III and above need a higher level of care and anaesthetic input. Assigning the class forces a structured summary of the child's illnesses. [4]
Next, the focused airway assessment. Look for mouth opening, neck movement (flexion and extension), a receding mandible, large or visible tonsils, and any stridor. These features — collectively the predictors of difficult mask ventilation and intubation — flag the child in whom a lost airway would be hard to rescue, and that child should not be deeply sedated without anaesthetic backup. Then the fasting history, taken not to delay the procedure but to inform the risk. Then the weight in kilograms, confirmed and used for every dose. Finally the cardiorespiratory examination — baseline oxygen saturation, respiratory rate and effort, heart rate, and signs of shock or upper airway obstruction — and the consent, documented with the parent and, where appropriate, the child. [4]
The bedside assessment deliberately avoids three errors: sedating without rescue equipment, sedating alone (the proceduralist cannot both perform the procedure and watch the airway), and proceeding in a high-risk child without senior or anaesthetic input. The monitoring standard is continuous pulse oximetry and heart rate from the moment of drug administration, with capnography added wherever feasible, and intermittent blood pressure. A dedicated observer — a team member whose only job is to watch the child's airway, breathing and sedation depth — must be present throughout. [4] [10]
Investigations
There are no laboratory investigations routinely required before procedural sedation in the well child. The "investigations" in this topic are the bedside monitoring modalities, and the candidate must know what each one measures and when it fails. [4]
Pulse oximetry is mandatory and continuous, and it measures arterial oxygen saturation. Its limitation, explained in the pathophysiology section, is that it detects hypoxia late and is further delayed by supplemental oxygen, so it is a backstop rather than an early warning. Capnography (end-tidal carbon dioxide monitoring) measures exhaled carbon dioxide and detects the rising carbon dioxide of hypoventiation within seconds, before the oxygen saturation falls; a randomised trial confirmed it detects hypoventilation that oximetry misses, and current guidelines recommend it wherever available, particularly for deep sedation and for any sedation in a high-risk child. [10] [4] Electrocardiography is added for deeper sedation and for children with cardiac disease, and blood pressure is measured intermittently throughout.
Two point-of-care tests are worth naming in the relevant child. A point-of-care glucose is checked in the fasted infant or the child who has not eaten for many hours, because hypoglycaemia can mimic or compound sedation and is easily missed. A haemoglobin is relevant if the procedure carries a risk of significant blood loss. The sedation event itself is documented in real time — drug, dose, route, time of each dose, depth of sedation, observations, and the recovery score — because the record is part of the safety system. A two-person weight and dose check before the drug is drawn up closes the commonest source of drug error in paediatric sedation. [4]
Management — Resuscitation
The resuscitation phase in this topic is the management of acute deterioration during or immediately after sedation, and the candidate must be able to walk through each event in order. The unifying principle is that the response to every deterioration is airway, breathing, then circulation, supported by stopping or reversing the sedative, and that these manoeuvres must be initiated without waiting for the saturation to crash. [4]
The commonest deterioration is transient hypoxia or apnoea. The response is to stimulate the child verbally or by touch, open the airway with a jaw thrust and chin lift, give 100 percent oxygen by bag-valve-mask, and reduce the sedation depth by withholding further doses. Most episodes resolve with these airway manoeuvres alone. If an opioid has contributed, give naloxone 0.1 milligram per kilogram intravenously or intramuscularly (maximum 2 milligrams per dose), and if a benzodiazepine has contributed, give flumazenil 0.01 milligram per kilogram intravenously (maximum 0.2 milligrams for the first dose). The critical caveat is that the sedative outlasts the reversal agent, so the child can re-sedate after apparently recovering — reversal buys time, it does not replace monitoring and ventilatory support. [4]
Laryngospasm — the sudden closure of the vocal cords that can follow airway irritation, particularly in a child with a recent upper respiratory infection — presents with stridor or silent attempts at breathing, paradoxical chest wall movement and a falling saturation. The stepwise management is to clear secretions, apply sustained positive airway pressure with 100 percent oxygen via a tightly sealed bag-valve-mask using a jaw thrust, and if this does not break the spasm, give suxamethonium (for example 1 to 1.5 milligrams per kilogram intravenously, or 4 milligrams per kilogram intramuscularly if no intravenous access) to paralyse the cords and allow ventilation, with preparation for intubation. [4]
Vomiting during sedation risks aspiration; the response is to place the child in the lateral position, suction the oropharynx, pause the procedure, and ensure the airway is clear. Pulmonary aspiration itself is vanishingly rare during procedural sedation — large series report essentially no cases — and when it does occur it is managed as aspiration pneumonitis with supportive respiratory care. A sedation should be abandoned and the child escalated whenever the airway cannot be maintained, oxygenation cannot be restored, the procedure cannot be completed safely, or the child's status deteriorates unexpectedly; the team must know in advance where the child will go (theatre, intensive care, retrieval) if this happens. [6] [4]
Management — Definitive & Stepwise
The definitive management is the ordered conduct of a safe sedation, and it should be walked as a sequence. First, assess and consent: complete the pre-sedation assessment, assign the ASA class, weigh the child, take the fasting and airway history, and document consent. Second, prepare the team and equipment: assemble the two-person team, check the weight-based doses, place the rescue airway equipment and oxygen at the bedside, attach the monitoring, secure vascular access where needed, and record a baseline. Third, administer the agent in a titrated, weight-based fashion, observing the child's depth and airway throughout. Fourth, observe during the procedure with continuous monitoring and a dedicated observer. Fifth, recover in a monitored area until the child meets discharge criteria. [4]
The two agents whose exact doses a fellowship candidate must hold are ketamine and nitrous oxide. Ketamine produces dissociative sedation — a cataleptic state with preserved airway reflexes, maintained muscle tone and cardiovascular stability, and profound analgesia. The dose is 1 to 1.5 milligrams per kilogram intravenously, given slowly over 30 to 60 seconds, with onset within 30 to 60 seconds and a clinical duration of 10 to 20 minutes; when no intravenous access is available, 4 to 5 milligrams per kilogram intramuscularly works within 3 to 5 minutes and lasts 20 to 30 minutes. [3] Ketamine's advantages are that it preserves the airway and blood pressure and provides analgesia, which is why it is the workhorse for painful procedures in children; its disadvantages are vomiting in roughly 10 to 15 percent of children, emergence phenomena (vivid dreams, agitation or confusion on waking), hypersalivation, and a small risk of laryngospasm. It is relatively contraindicated in infants under three months, in raised intracranial or intraocular pressure, in active upper airway infection (laryngospasm risk), and used cautiously in significant cardiac disease. [3]
Nitrous oxide as a 50 percent mixture in oxygen (a premixed Entonox-type preparation) gives light sedation and analgesia for brief, moderately painful procedures. It takes effect within 2 to 5 minutes of inhalation, the depth is titratable to the procedure, and recovery occurs within minutes of stopping because the gas is excreted unchanged through the lungs. A decade of paediatric emergency department data confirms its safety and efficacy for the right procedures. [7] It is contraindicated where an enclosed gas space would expand — pneumothorax, middle-ear disease, bowel obstruction, and the first trimester of pregnancy — and in vitamin B12 deficiency. Vomiting and nausea are its commonest adverse effects, and these are reduced by giving oral ondansetron when nitrous is combined with an opioid such as intranasal fentanyl. [9] [11]
The two agents a fellowship candidate must hold
The other agents are named for completeness but generally fall to anaesthetically trained providers in children. Midazolam provides anxiolysis and amnesia with little analgesia and a longer recovery than ketamine. Propofol produces deep sedation approaching anaesthesia with rapid onset and recovery but marked respiratory depression and hypotension, and is usually restricted to anaesthetic or specially credentialed providers. Fentanyl (1 microgram per kilogram) is an opioid analgesic that is hazardous when combined with a sedative because of synergistic respiratory depression. Naloxone and flumazenil are the reversal agents for opioid and benzodiazepine overdose respectively, used as described above. [1] [4]
The under-sedated child — still distressed, moving, or in pain — receives supplemental titrated dosing of the same agent rather than switching agents mid-procedure. The over-sedated child — losing the airway, hypoventilating, or unresponsive — receives the resuscitation steps above: airway support, oxygen, withholding further sedation, and a reversal agent if an opioid or benzodiazepine is implicated. [4]
Specific Subtypes & Scenarios
Four scenarios recur in fellowship vivas and procedural assessments, and each carries a specific teaching point. The first is sedation for a brief painful procedure — laceration repair, fracture or dislocation reduction, abscess drainage. Here the goal is stillness and analgesia for a procedure lasting minutes, and dissociative ketamine is usually the right tool because it combines profound analgesia with a preserved airway. The second is sedation for imaging (magnetic resonance imaging, computed tomography), where analgesia is irrelevant and the goal is immobility, often for longer than a painful procedure; this usually needs deeper sedation or anaesthetic input, particularly in the young child who cannot cooperate with instructions to keep still. [1] [3]
The third is nitrous oxide with intranasal fentanyl for a minor-to-moderate procedure such as venepuncture, suturing, simple fracture splinting or dental work. This combination is effective and increasingly used, and its main adverse effect is vomiting, which a trial showed is reduced by prophylactic oral ondansetron. The fourth is the infant under one year, who is at higher risk of apnoea and airway obstruction, in whom ketamine is relatively contraindicated in the very young, and who usually requires anaesthetic input and a higher level of monitoring and recovery. [9] [4]
The oncology child having repeated procedures — bone marrow aspiration, lumbar puncture, Port-a-Cath access — needs a reliable, reproducible plan that provides amnesia and analgesia and is acceptable to the child over many encounters; these are often done with propofol or ketamine by an experienced team. The remote or retrieval setting, where anaesthetic backup may be hours away, demands a conservative threshold for sedation, a clear plan for deterioration, and familiarity with the agents and monitoring that are safely used without an anaesthetist present. The child with a difficult airway or complex cardiac disease is referred for anaesthetic input and often to theatre, because a lost airway in this child is hard to recover. [1] [4]
Complications & Pitfalls
The candidate must be able to name, prevent and manage each complication, because two — the unrecognised hypoventilation and the procedurally abandoned airway — are directly under the operator's control. The complications divide into common and minor, and rare and serious. [2] [4]
The common adverse events are transient oxygen desaturation, vomiting, and emergence phenomena with ketamine. Transient desaturation usually resolves with airway-opening manoeuvres and oxygen. Vomiting — commonest with ketamine and with nitrous-plus-opioid — is managed by positioning the child laterally, suctioning, and pausing the procedure; prophylactic ondansetron reduces it when nitrous is combined with intranasal fentanyl. Ketamine emergence phenomena (vivid dreams, agitation, confusion on waking) settle with reassurance and a quiet recovery environment, and they do not contraindicate future use; the older child and adolescent are more affected than the young child. [3] [9]
The serious adverse events are laryngospasm, apnoea requiring intervention, pulmonary aspiration, and cardiac arrest — all uncommon in trained hands, as the Pediatric Sedation Research Consortium data show. [2] Laryngospasm and apnoea are managed as described in the resuscitation section. The highest-yield preventable pitfalls are proceeding without rescue airway equipment at the bedside; sedating without a dedicated observer; giving a weight-based dose that has not been double-checked; relying on pulse oximetry alone without capnography; and relying on a reversal agent as a substitute for airway and ventilatory support. [4] [10]
Prognosis & Disposition
The outcome of procedural sedation, in the vast majority of cases, is a calm child, a completed procedure, and an uncomplicated recovery. Recovery time depends on the agent: nitrous oxide clears within minutes of stopping the gas, propofol within minutes, and ketamine over roughly 60 to 120 minutes, with the child returning to a normal conscious state and being observed until discharge criteria are met. [3] [7]
The discharge criteria are framed around the child returning safely to a less supervised setting. The structured tool is a modified Aldrete score (a paediatric recovery score assessing activity, respiration, circulation, consciousness and oxygen saturation), with a score of 9 or above, sustained over a period of observation, supporting discharge. The child should be alert or at their baseline conscious state, have a patent airway and adequate breathing, stable cardiovascular observations, and be able to tolerate oral intake. [4]
Admission is required after a sedation if recovery is prolonged, if any serious adverse event occurred, if the underlying condition needs observation, or if the child is an infant at higher risk of late apnoea. The aftercare advice given to families reflects the residual sedation: the child must be supervised by a responsible adult, must not drive, ride a bike, or operate anything dangerous for the remainder of the day, and the family is given return precautions (persistent drowsiness, breathing problems, vomiting). The disposition is driven by the underlying condition and the procedure performed, with the sedation event fully documented. [4]
Special Populations
The infant under one year deserves a separate line. The small functional residual capacity, the high oxygen consumption, the obligate nose-breathing, and the immature respiratory control make the infant unusually vulnerable to apnoea and rapid desaturation; ketamine is relatively contraindicated in the very young infant, and sedation in this age group usually needs anaesthetic input, continuous monitoring including capnography, and a period of recovery observation. [4]
The child with a difficult airway, obesity, or sleep-disordered breathing is at high risk of airway obstruction once sedated, because the pharyngeal tone that keeps the airway open is lost. The approach is anaesthetic involvement, a theatre or high-acuity setting, and a modified agent choice that minimises airway depression; deep sedation in this child is an anaesthetic event. The child with complex cardiac or neuromuscular disease — ASA III or above — carries a several-fold higher risk of adverse events and is referred for anaesthetic input. [2] [4]
The oncology or immunocompromised child having repeated procedures needs a consistent, individualised plan that is acceptable over many encounters, with Port-a-Cath access and a balance of amnesia, analgesia and rapid recovery. For Aboriginal, Torres Strait Islander, Māori, and migrant and refugee children, and for children in remote and under-resourced settings, the sedation may be delivered far from anaesthetic backup; the equity issue is that the team must be trained, the safe agents stocked, the monitoring available, and the retrieval pathway clear. The neurodivergent or technology-dependent child needs an individualised plan that accounts for communication, sensory needs, positioning and the capacity for assent, often developed with the family in advance. [1]
Evidence, Guidelines & Regional Differences
The guidelines are concordant on the core principles, and the candidate should be able to name them. The American Academy of Pediatrics and American Academy of Pediatric Dentistry guidelines (Coté and Wilson 2019) set the standard for the pre-sedation assessment, the personnel (a trained team with a dedicated observer), the monitoring (pulse oximetry mandatory, capnography recommended, heart rate and blood pressure), and the recovery and discharge criteria. The American Society of Anesthesiologists practice guidelines for moderate procedural sedation reinforce the same structure and define the depth continuum. The Green 2011 emergency department ketamine guideline codifies the ketamine dose, route, contraindications and recovery. [4] [3]
The area where the evidence has matured — and the examiner most likes to probe — is fasting before emergency procedural sedation. The traditional ASA fasting guideline (2 hours for clear fluids, 4 hours for breast milk, 6 hours for formula or a light meal, 8 hours for a fatty meal) was designed for elective anaesthesia in healthy patients, and applying it to a child in pain in the emergency department can delay needed care. [5] Green and Krauss examined the pulmonary aspiration risk during emergency procedural sedation and found it negligible and unrelated to fasting status, because aspiration is prevented by sedation depth and airway care rather than by the time since the last meal. [6] Subsequent work on fasting guideline impact for orthopaedic sedation reinforced that fasting status does not meaningfully predict safety. [8] The current position, reflected in updated ASA guidance, is that fasting is not a substitute for monitoring, that a child needing a time-critical sedation should not be denied it solely for fasting status, and that the fasting history informs the risk and the depth rather than gating the decision.
[4] [6]The evidence on capnography is clear: a randomised trial in a paediatric emergency setting showed capnography detects hypoventilation that pulse oximetry misses, supporting its recommendation as the preferred ventilatory monitor. [10] The genuine remaining controversies are narrow: whether propofol can be safely used by non-anaesthetist credentialed providers in children, the lower age limit and contraindications of ketamine, the role of routine pre-sedation fasting intervals in low-risk emergency cases, and the use of nitrous oxide in very young infants. On each, the conservative and defensible position is to match the agent and depth to the child's risk and the available expertise, and to involve an anaesthetist whenever the airway or the status is in doubt. [1]
Exam Pearls
A fellowship candidate should leave the examiner with a small set of sharp, sourced facts. Memorise these and you will answer any question on this topic. [1] [4]
The single framing idea is the continuum of sedation depth: moderate sedation preserves a purposeful response to voice and an independent airway; deep sedation preserves only a response to pain and may lose the airway; general anaesthesia loses both. State it first, name the four pillars (assessment, team and equipment, monitoring, recovery), and you have the spine of the topic. [4]
The drug doses the examiner rewards verbatim are ketamine 1 to 1.5 milligrams per kilogram intravenously over 30 to 60 seconds, or 4 to 5 milligrams per kilogram intramuscularly, and nitrous oxide 50 percent in oxygen. [3] The reversal doses are naloxone 0.1 milligram per kilogram (maximum 2 milligrams) for opioid overdose and flumazenil 0.01 milligram per kilogram (maximum 0.2 milligrams first dose) for benzodiazepine overdose — with the caveat that the sedative outlasts the reversal, so the child must be monitored for re-sedation. [4]
The safety maxim is that fasting is not a substitute for monitoring: aspiration during procedural sedation is negligible and is not predicted by fasting, so a fasting history informs risk but must never delay a time-critical sedation. The monitoring maxim is that capnography catches hypoventilation early where pulse oximetry catches hypoxia late, and supplemental oxygen masks the oximeter further. The risk maxim is that ASA III or above, infancy, a difficult airway, and complex cardiac or neuromuscular disease all shift the child toward anaesthetic input. Hold these four and you will defend any sedation question a fellowship examiner can pose. [6] [10] [2]
References
- [1]Krauss B, Green SM Procedural sedation and analgesia in children Lancet, 2006.PMID 16517277
- [2]Cravero JP, Blike GT, Surdyk M, et al Incidence and nature of adverse events during pediatric sedation/anesthesia for procedures outside the operating room: report from a Pediatric Sedation Research Consortium Pediatrics, 2006.PMID 16951002
- [3]Green SM, Roback MG, Kennedy RM, et al Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update Annals of Emergency Medicine, 2011.PMID 21256625
- [4]Coté CJ, Wilson S, American Academy of Pediatrics, American Academy of Pediatric Dentistry Guidelines for Monitoring and Management of Pediatric Patients Before, During, and After Sedation for Diagnostic and Therapeutic Procedures Pediatrics, 2019.PMID 31439084
- [5]American Society of Anesthesiologists Task Force on Preoperative Fasting Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures Anesthesiology, 1999.PMID 10078693
- [6]Green SM, Krauss B Pulmonary aspiration risk during emergency department procedural sedation--an examination of the role of fasting and sedation depth Academic Emergency Medicine, 2002.PMID 11772667
- [7]Croughan S, Barrett M, Sharwood R, et al Safety and efficacy of a nitrous oxide procedural sedation programme in a paediatric emergency department: a decade of outcomes Emergency Medicine Journal, 2024.PMID 38123983
- [8]Stewart RJ, Strickland CD Hunger Games: Impact of Fasting Guidelines for Orthopedic Procedural Sedation in the Pediatric Emergency Department Journal of Emergency Medicine, 2021.PMID 33323292
- [9]Fauteux-Lamarre E, McCarthy M, Zhang MM, et al Oral Ondansetron to Reduce Vomiting in Children Receiving Intranasal Fentanyl and Inhaled Nitrous Oxide for Procedural Sedation and Analgesia Annals of Emergency Medicine, 2020.PMID 31983494
- [10]Langhan ML, Shabanova V, Li FY, et al A randomized controlled trial of capnography during sedation in a pediatric emergency setting American Journal of Emergency Medicine, 2015.PMID 25445871
- [11]Fauteux-Lamarre E, Hearps S, McCarthy M, et al Associations with early vomiting when using intranasal fentanyl and nitrous oxide for procedural sedation in children: A secondary analysis Emergency Medicine Australasia, 2025.PMID 39268662