Paeds · investigations-procedures-and-technology
Simple laceration repair and wound management
Also known as Wound closure · Skin laceration repair · Suturing in children · Tissue adhesive closure · Wound care
A fellowship approach to simple laceration repair and wound management in children covering wound assessment (mechanism, depth, contamination, neurovascular and tendon status, tetanus, and non-accidental injury), painless preparation with LET (lidocaine four percent, epinephrine one in two thousand, tetracaine half percent) applied for twenty to thirty minutes, the safe local anaesthetic maximum doses (lidocaine three milligrams per kilogram plain or seven milligrams per kilogram with adrenaline, bupivacaine two milligrams per kilogram), tap water irrigation equal to sterile saline, the four closure methods (tissue adhesive, sutures, adhesive strips, staples) with selection by tension and site, suture size by body region, suture removal timing, bite wound prophylaxis with amoxicillin-clavulanate, and the family-centred approach to a frightened child.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a four-year-old brought to the emergency department after falling against a table edge and splitting the skin over her chin. She is frightened, crying, and clutching a bloodstained towel. The task is not just to close a gap in the skin but to repair a wound in a child who will remember the experience for years. Good laceration repair is as much about painless technique, calm communication, and the right closure method as it is about the mechanics of a suture. [1] [3]
A laceration is a tear in the skin and underlying tissue caused by blunt or shearing force, distinct from a clean incision. Simple laceration repair means the assessment and bedside closure of a wound that is superficial enough, clean enough, and in a safe enough location to be managed without an operating theatre or a surgical specialist. The goal of repair is the same as it is for any wound: stop bleeding, remove contamination, approximate healthy tissue under minimal tension, and create the conditions for healing by primary intention while minimising infection, scarring, and the child's distress. [1]
The procedure looks small, but it carries real risks. Infection rates climb with contamination, bites, and delay. Local anaesthetic systemic toxicity is a genuine danger when doses are not calculated against weight. A cosmetic defect on the face lasts a lifetime. And a frightened child who is held down and sutured without adequate analgesia can develop lasting procedural anxiety. The fellowship candidate is expected to demonstrate a methodical, child-centred approach that gets all of this right. [3] [10]
Classification
Hold two classifications in mind at once: the closure method you choose and the wound itself, because the wound's characteristics dictate the method. The two decisions interact, and choosing the wrong method for the wrong wound is the commonest source of failure and harm. [1] [8]
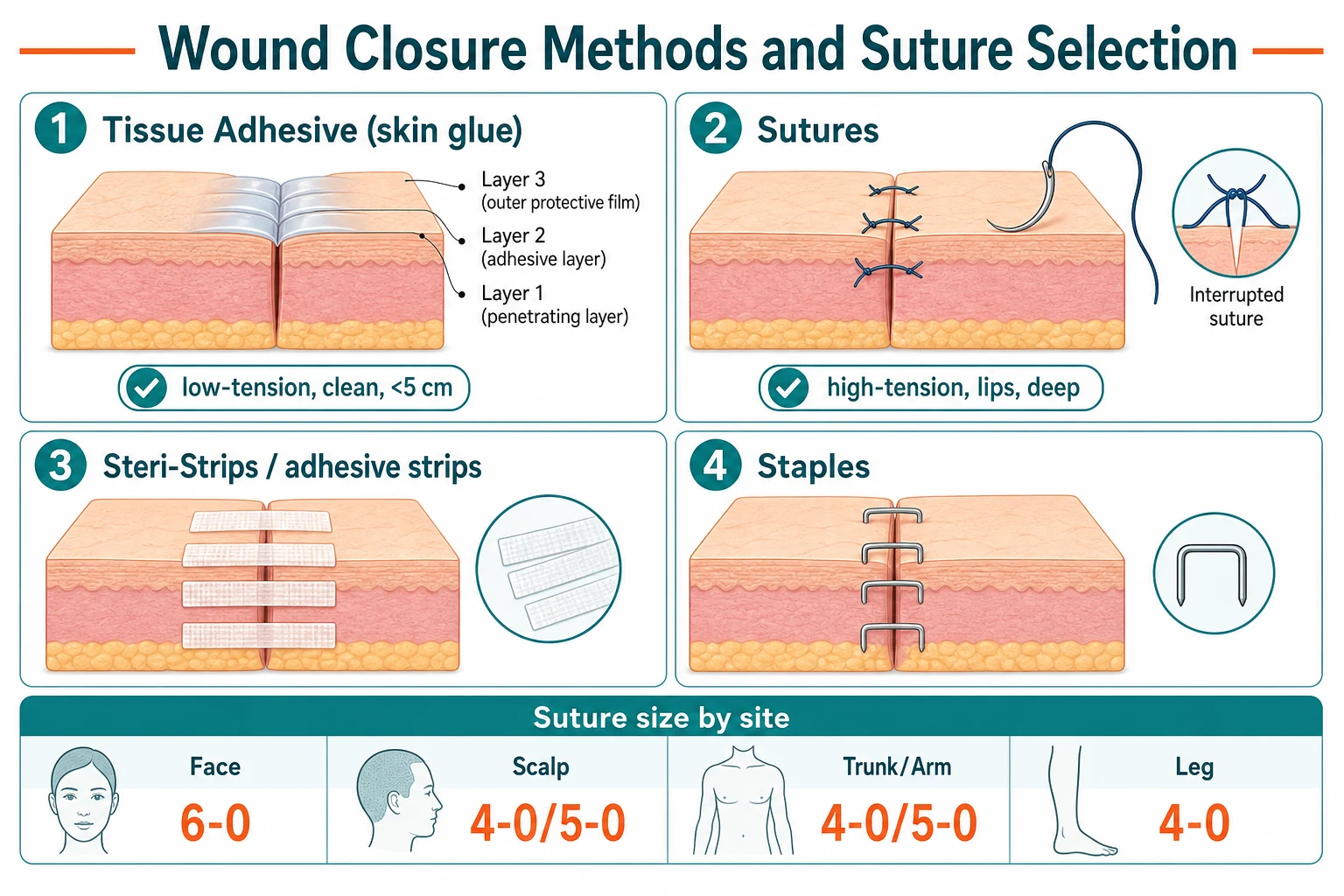
By closure method, four options exist for simple paediatric wounds. Tissue adhesive (two-octylcyanoacrylate, or skin glue) polymerises on contact with skin moisture to form a flexible bond and is first choice for clean, low-tension, simple lacerations under five centimetres with easily opposed edges. Sutures give the strongest, most precise closure and are needed for high-tension areas, deep or stellate wounds, wounds needing layered closure, and the face and lip where cosmetic precision matters. Adhesive skin closure strips (Steri-Strips) approximate low-tension wounds, support sutures, or close very superficial wounds. Staples are fast and strong but are reserved for the scalp, where cosmetic outcome matters least and cooperation is limited. [8] [1]
By wound type, classify along five axes that decide management. Depth: superficial (skin only), deep (involving subcutaneous tissue, tendon, or nerve). Contamination: clean, dirty, or a bite. Tension: low (edges fall together) versus high (edges spring apart, over joints). Age and location: a face wound tolerates later closure and demands fine sutures; a hand or foot wound threatens tendon and nerve. Mechanism: sharp incisions heal best; crush and bite injuries carry the highest infection risk. A clean, superficial, low-tension facial laceration is a tissue-adhesive wound; a contaminated bite over a finger joint is a suture-or-leave-open, antibiotic, and specialist wound. [1] [12]
Epidemiology & Risk Factors
Lacerations are among the commonest reasons a child presents to an emergency department. They account for a substantial fraction of paediatric presentations for minor trauma, peaking in the mobile preschool and school-age years when falls, collisions, and play dominate the day. Boys present more often than girls, and the head and face, the knees and shins, and the hands and fingers are the typical sites. [1] [3]
The wounds most likely to become infected, to scar badly, or to need specialist repair are predictable. Bite wounds carry a high infection rate because of oral and animal flora. Hand and foot wounds risk tendon, nerve, and joint involvement and have less forgiving blood supply. Contaminated wounds and those presenting after six to twelve hours on the hand or face have a higher infection risk. Crush injuries and wounds on darkly pigmented skin are more prone to poor scarring and keloid formation. Children with eczema or sensitive skin tolerate tissue adhesive and adhesive strips poorly. [12]
A single number carries the burden: laceration repair is the commonest single reason a child receives a painful procedure in the emergency department. The 2024 systematic review of pharmacologic distress management during paediatric laceration repair found that distress is near-universal without preparation, and that procedural anxiety in a young child predicts both worse immediate pain and future procedural avoidance. This is why child-centred preparation, topical anaesthesia, and distraction are not soft options but core parts of the technique. [2] [3]
Clean facial laceration
Low tension, 2 cm chin
- Tissue adhesive or 6-0 sutures
- Topical LET 20 to 30 minutes first
- Cosmesis excellent, low infection risk
- Review or removal at day 5
Scalp laceration
Bleeding, dirty
- Irrigate well, may staple or suture 4-0/5-0
- Hair apposition or tissue adhesive possible
- Tetanus status check
- Watch for hidden fracture or foreign body
Dog bite to hand
Contaminated, deep
- Irrigate copiously, do not close primarily
- Amoxicillin-clavulanate prophylaxis
- Assess tendon, nerve, joint, bone
- Specialist review; tetanus and rabies consideration
Knee laceration, over joint
High tension
- Suture 4-0 or 5-0, deep layer if needed
- Avoid tissue adhesive on high-tension skin
- Immobilise and limit flexion while healing
- Removal at 10 to 14 days
Pathophysiology
Two physiological facts govern laceration repair: how a wound heals, and how local anaesthesia blocks the pain of repairing it. Grasp both, and every decision about closure method and analgesia follows from them. [10]
Wound healing unfolds in four overlapping phases. Haemostasis begins within minutes, as platelets and clot seal the defect. Inflammation follows over hours to days, clearing bacteria and debris but also producing the redness and swelling that signal early infection if it persists. Proliferation brings fibroblasts and new capillaries over days to weeks, filling the defect with granulation tissue and laying down collagen. Remodelling over weeks to months reorganises collagen into a scar that reaches only a fraction of the original skin's strength. Primary intention closure works because clean, well-opposed edges need only bridge a tiny gap, so healing is fast and scarring is minimal. Contaminated or gaping wounds heal by secondary intention, which is slower and scars worse. [1]
Local anaesthetics block pain by reversibly binding voltage-gated sodium channels on nerve fibres, preventing the action potential that carries pain to the brain. Lidocaine and bupivacaine act on sensory fibres preferentially, which is why a well-infiltrated wound is numb while pressure is still felt. The dose limits exist because at toxic plasma concentrations the same sodium-channel blockade fires the brain (seizures) and the heart (conduction block and collapse). The weight-based maxima — lidocaine three milligrams per kilogram plain or seven milligrams per kilogram with adrenaline, bupivacaine two milligrams per kilogram — are the floor of safety, not a target. Adrenaline doubles the safe lidocaine dose because vasoconstriction slows systemic absorption, and it also helps a bleeding field. [10]
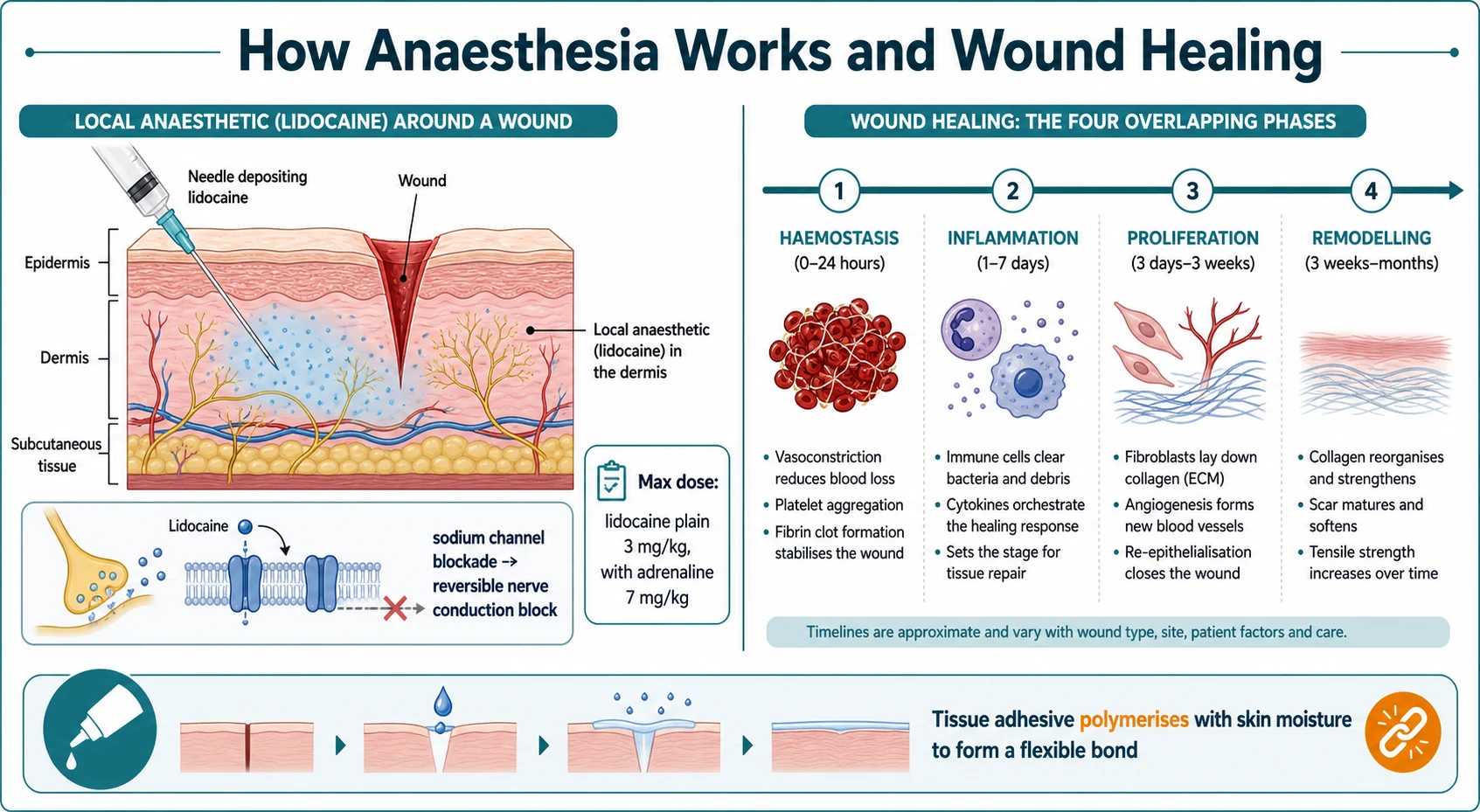
Topical LET works by the same sodium-channel mechanism, diffusing through intact broken skin to anaesthetise the dermis over twenty to thirty minutes. Tissue adhesive works by a different mechanism: the cyanoacrylate monomer polymerises on contact with moisture in the skin to form a strong, flexible bond that holds the edges together while healing proceeds beneath. It is a dressing and a closure in one, which is why it must not enter the wound itself or sit on mucosa. [4] [8]
Clinical Presentation
The child who needs laceration repair never arrives with a label on the wound. You build the picture from the history, the mechanism, and a careful, calm examination that the frightened child will allow. The presentations cluster around four scenarios. [1]
The first is the low-energy fall in a mobile child, producing a clean laceration to the chin, forehead, or knee — the bread and butter of paediatric emergency work. The second is the sharp or glass injury to a hand or foot, where the worry is a deeper structure: a tendon, a nerve, or a retained foreign body. The third is the bite, whether animal or human, where infection is the dominant risk and primary closure is usually wrong. The fourth is the unwitnessed or delayed-presentation injury, where the mechanism is unclear and safeguarding must be considered alongside repair. [1] [12]
The history that matters is short and targeted. Ask exactly how the injury happened, when it happened, what the child has eaten (relevant if sedation becomes necessary), and the child's immunisation and tetanus status. Ask about allergies, bleeding disorders, and any previous reaction to local anaesthetic or adhesive. Then examine the wound in good light, after letting the child settle and offering distraction: assess the depth, look for tendon, nerve, or vessel involvement, test distal sensation and function where relevant, and palpate for a foreign body. A wound on the hand should prompt active and passive movement testing of every involved tendon. [1]
Differential Diagnosis
There is no differential diagnosis of a laceration itself — the wound is visible. The differential that matters is whether a wound is truly simple and suitable for bedside closure, or whether a deeper or more complex problem hides beneath the skin and needs specialist repair, imaging, or theatre. [1]
The features that move a wound out of the simple category are worth listing because each redirects management. A tendon, nerve, or vessel injury needs surgical assessment and often an operating theatre. A retained foreign body — glass, wood, or gravel — needs location (radiograph or ultrasound for radio-opaque material) and removal before closure, or the wound will infect. A fracture beneath or communicating with the wound is an open fracture, an orthopaedic emergency. A contaminated or bite wound needs irrigation, debridement, and usually delayed closure or healing by secondary intention with antibiotics. A wound demanding precise cosmesis (lip vermillion border, eyelid margin, face) needs a clinician trained in that repair. [1] [12]
The second differential worth holding is the cause of a poor outcome after repair. Wound breakdown, infection, dehiscence, or a hypertrophic or keloid scar each have causes you can identify at the first encounter: excessive tension, inadequate irrigation, a missed foreign body, the wrong closure method (tissue adhesive on a high-tension or bite wound), or poor aftercare. Each is preventable by the methodical assessment described throughout this topic. [3]
Clinical & Bedside Assessment
The bedside assessment is about the wound and the child: choosing the right closure method, confirming the wound is safe to close at the bedside, and preparing the child so that the procedure is tolerable. Do this systematically, because a wound assessed badly is a wound repaired badly. [1]
First inspect the wound in good light after the child has settled. Note the length, depth, and shape, the state of the wound edges (clean and incised versus crushed and stellate), the presence of contamination or foreign material, and any signs of pre-existing infection. Test distal neurovascular and tendon function before you infiltrate, because local anaesthesia will mask a nerve injury afterwards. For hand and foot wounds, examine sensation with light touch, test two-point discrimination where relevant, and check active movement of each digit against resistance. [1]
Assess the need for imaging. Request a radiograph if glass or metal is suspected as a retained foreign body, if an underlying fracture or open fracture is possible, or if a penetrating wound may have reached bone or joint. Ultrasound can locate non-radio-opaque material. Do not close over a suspected foreign body. Then decide on closure method against tension and site, as set out in the classification and the management section, and check tetanus status against the child's immunisation history and the wound's cleanliness. [1]
Assessment in one pass
Investigations
No investigation is required before closing a straightforward clean laceration. The decision to repair is clinical and the procedure is immediate. Investigations have a limited but important role in selected wounds, and over-investigating a simple wound is a waste of the child's time. [1]
The investigation that matters most is imaging for a suspected foreign body or fracture. Glass and metal are radio-opaque and show on a plain radiograph; wood and some plastics are not, and ultrasound may locate them. Never close a wound over a suspected retained foreign body, because infection and breakdown will follow. Request a radiograph for any open fracture, any penetrating injury that may have reached bone or joint, and any wound with a suspicious mechanism or persistent pain despite repair. [1]
Swabs and wound cultures are not needed before closing a clean wound, because they do not predict infection and they do not change initial management. They are reserved for an established infection that is failing first-line treatment. The monitoring that matters after repair is the review appointment: check at forty-eight hours for an infected or contaminated wound, and at five to fourteen days (by site) for removal of non-absorbable sutures. Give the family written advice on signs of infection — increasing redness, spreading swelling, pain, discharge, or fever — and a clear route back. [1] [3]
Management — Resuscitation
Laceration repair is rarely a resuscitation procedure, but two resuscitation principles apply. Bleeding control comes first: almost all wound bleeding stops with firm direct pressure for five to ten minutes, applied while you take the history. Elevate the limb. Only rarely is a vessel tie or diathermy needed, and a wound that will not stop bleeding with pressure is a wound for theatre. [1]
The second principle is pain is an emergency to a frightened child. Do not begin cleaning, infiltrating, or suturing a child in pain. The default first move is to apply topical LET gel into the wound, cover it with an occlusive dressing, and give the child twenty to thirty minutes of calm distraction. LET provides effective anaesthesia for most simple lacerations and makes even subsequent infiltration painless. For the child who remains distressed, layer in non-pharmacological measures (comfort positioning, distraction, a child-life worker) and consider judicious procedural sedation for the long or complex repair. [4] [2]
Lidocaine 1% (local infiltration)
Dose
3 mg/kg plain (0.3 mL/kg of 1%), or 7 mg/kg with adrenaline (1:200,000)
The sedation decision is governed by safety and by the child. For the short, simple, well-anaesthetised wound, distraction and topical anaesthesia suffice. For a longer repair or an anxious child unable to cooperate, procedural sedation with a monitored regimen (for example intranasal or intravenous agents titrated to minimal or moderate sedation, with a trained team, monitoring, and rescue equipment) is appropriate and is increasingly used in paediatric emergency departments. The 2024 systematic review confirms that combined pharmacologic and non-pharmacologic strategies reduce distress during paediatric laceration repair. Never sedate a child without a fasting history, a full stomach caution, a monitored setting, and a clinician trained in paediatric airway rescue. [2] [7]
Management — Definitive & Stepwise
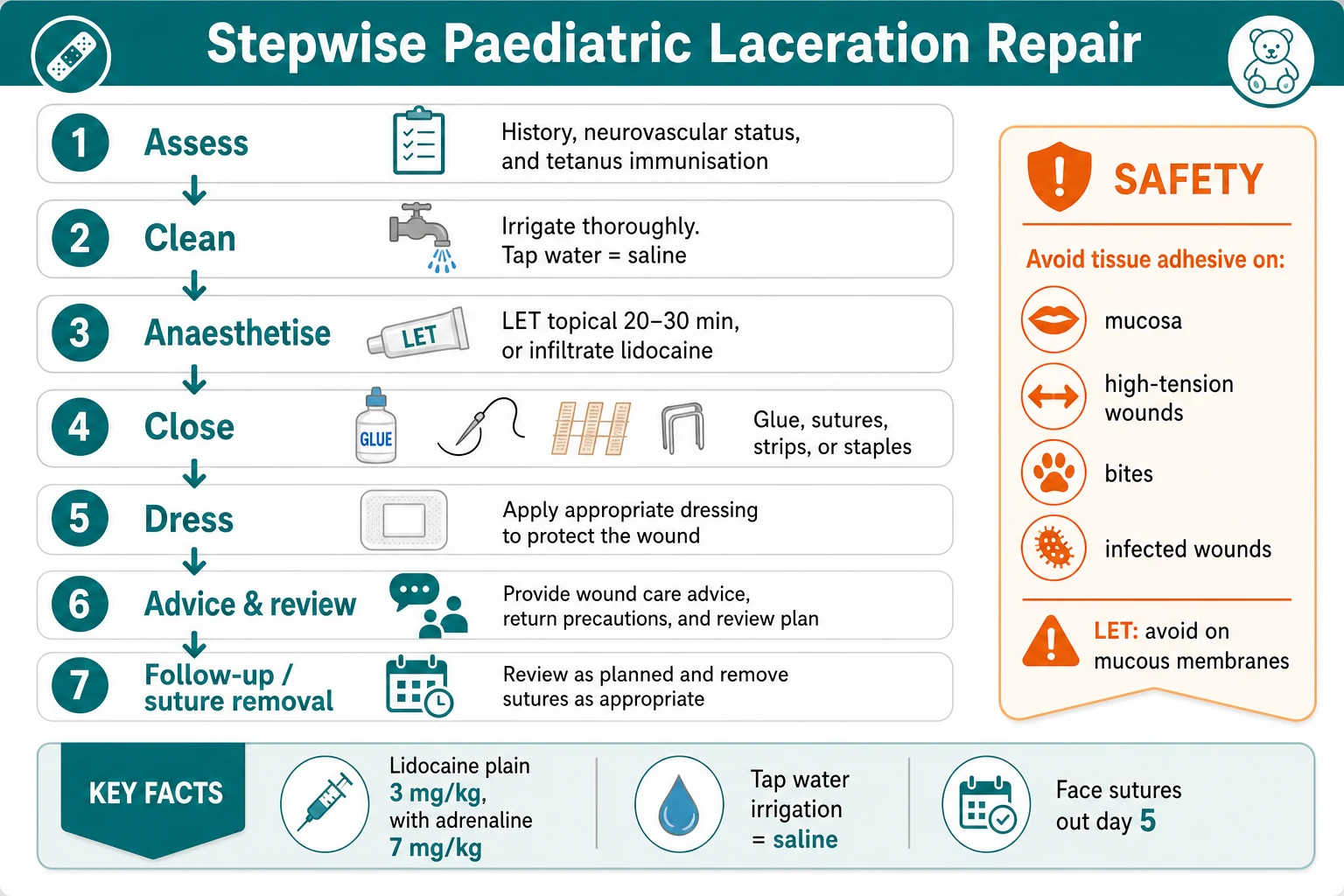
Once the child is settled and anaesthetised, the repair itself runs in seven ordered steps. Run through them the same way every time, and the quality of the result will follow. [1]
The laceration repair procedure, in order
1 · Assess
Confirm mechanism, depth, contamination, neurovascular and tendon status, tetanus status, and safeguarding. Decide the wound is simple enough for bedside closure.
2 · Prepare the child
Apply topical LET gel into the wound, cover with an occlusive dressing, and allow 20 to 30 minutes with distraction and comfort positioning. Offer oral sucrose to an infant.
3 · Clean and irrigate
Irrigate the wound with tap water or saline at moderate pressure (about 5 to 8 psi), volume roughly 50 to 100 mL per centimetre of laceration. Debride devitalised tissue; remove all visible foreign material.
4 · Anaesthetise
If topical is incomplete, infiltrate lidocaine 1% through the wound edge (max 3 mg/kg plain, 7 mg/kg with adrenaline). Buffer and warm it to cut stinging. Aspirate before injecting.
5 · Close
Choose the method by tension and site: tissue adhesive for clean low-tension wounds under 5 cm; sutures for high-tension, deep, or precise-cosmesis wounds; adhesive strips for very superficial wounds; staples for the scalp.
6 · Dress and advise
Apply an appropriate dressing, give written wound-care advice (keep clean and dry for 48 hours, no picking at glue), and state the infection warning signs and the review or removal date.
7 · Follow-up
Arrange review at 48 hours for contaminated or bite wounds, and suture removal at day 5 for the face, 7 days for the scalp and trunk, 10 to 14 days for the limbs and over joints.
A few technique points separate a clean closure from a poor one. Irrigate generously — the single biggest determinant of infection is wound cleanliness, and tap water is as effective as sterile saline in randomised paediatric trials. Evert the wound edges when suturing so the healed surface is flat, not indented; a simple interrupted technique with the needle driven perpendicular to the skin achieves this. Close in layers for deep wounds, approximating the dermis with an absorbable layer to remove tension from the surface. Use the finest suture the site allows, because finer sutures scar less. And never use tissue adhesive inside the wound — it bonds the surface only, traps subcutaneous dead space, and invites infection. [8] [9]
| Method | Best for | Avoid in | Removal |
|---|---|---|---|
| Tissue adhesive | Clean, low-tension, simple, <5 cm; many facial and limb lacerations | Mucosa, high-tension, bites, infected, contaminated, across joints | Peels off at 5 to 10 days |
| Sutures | High-tension, deep, stellate, lip and face, layered closure | Very superficial low-tension wounds where glue would do | Face 5 days; scalp/trunk 7; limbs 10 to 14 days |
| Adhesive strips | Very superficial, low-tension; support after suture removal | Bleeding, weeping, or high-moisture sites | Fall off or remove at 7 days |
| Staples | Scalp lacerations needing speed and strength | Face, cosmetic areas, hands and feet | Remove at 7 days |
[8] [1] Suture sizes follow site, not the operator's habit: 6-0 or 5-0 non-absorbable on the face for the finest cosmetic result, 5-0 or 4-0 on the scalp and trunk, 4-0 on the limbs where tension is greater.
Specific Subtypes & Scenarios
Four scenarios recur in fellowship vivas and OSCE stations, and each has its own twist. The first is the facial laceration in a young child. The face heals well and tolerates closure up to twenty-four hours after injury because of its rich blood supply, but it also demands the finest cosmetic result. Use tissue adhesive for clean, low-tension facial wounds, or a 6-0 or 5-0 non-absorbable suture removed at five days. The lip vermillion border is the one facial site where precision is non-negotiable: align the vermillion-cutaneous junction exactly with the first suture, or a step deformity will be visible for life. [8]
The second is the tongue or intra-oral laceration. Most tongue lacerations heal beautifully without repair; close only those that gape widely, bisect the tongue, bleed persistently, or impair function. Use an absorbable suture (4-0 or 5-0), because removing sutures from a child's tongue is harder than placing them. Do not use tissue adhesive in the mouth — it polymerises on the wet mucosa poorly and can be swallowed. [1]
The third is the animal or human bite. Bites are heavily contaminated and carry a high infection rate, particularly on the hand. Irrigate copiously, do not close primarily (especially hand bites), assess tendon, nerve, joint, and bone involvement, and give amoxicillin-clavulanate prophylaxis for high-risk bites (hand, face, deep, immunocompromised, or presenting late). Check tetanus status and consider rabies risk for overseas or unprovoked animal bites. [12]
| Bite type | Close primarily? | Antibiotic prophylaxis | Key pathogen |
|---|---|---|---|
| Dog or cat bite, low-risk site | Sometimes, after careful cleaning | Consider amoxicillin-clavulanate | Pasteurella, Capnocytophaga |
| Dog or cat bite to hand or face | Usually NO (delayed or open) | Amoxicillin-clavulanate | Pasteurella |
| Human bite (clenched-fist) | NO — leave open | Amoxicillin-clavulanate | Eikenella corrodens, streptococci |
| Puncture wound, minor | No | Consider amoxicillin-clavulanate | Staphylococci, anaerobes |
[12] Always check tetanus status and review the child at forty-eight hours for signs of infection.
The fourth is the frightened or uncooperative child, where the technical closure is the easy part and the challenge is delivering it without distress. The evidence is clear that combined strategies — child-centred preparation, comfort positioning, distraction (including virtual reality), topical anaesthesia, and, where needed, minimal or moderate sedation — markedly reduce procedural distress. A child held down and sutured in pain develops lasting procedural anxiety and behavioural change, documented even after straightforward repairs. Plan the approach before you start: get the team, the room, and the play therapy right, and the closure follows. [2] [3]
Complications & Pitfalls
Complications are uncommon when the wound is assessed and repaired well, but the candidate must be able to name and prevent each one, because several are directly under the operator's control. [1]
The commonest complication is infection, and it is almost always preventable by adequate irrigation, removal of foreign material, debridement of devitalised tissue, and the right closure method. The risk climbs with contamination, bites, delay, the hand as a site, and poor aftercare. Suspect infection at the forty-eight-hour review with increasing pain, spreading redness, swelling, discharge, or fever; treat by opening the wound, taking a culture, irrigating, and giving antibiotics. A wound abscess needs drainage. [1] [12]
Wound dehiscence (breakdown of the closure) follows excessive tension, premature suture or glue failure, or trauma to the site before healing. Prevent it by closing in layers for deep wounds, choosing sutures over tissue adhesive for high-tension areas, and giving clear activity advice. Scarring is universal but is minimised by clean primary closure, fine sutures, eversion of edges, and protection from sun in the healing months. Hypertrophic scars and keloids are more common in darker skin types and on the chest and shoulders; counsel families and refer for dermatological or plastic review if they develop. [3]
Local anaesthetic systemic toxicity is the feared pharmacological complication and is entirely preventable by calculating the maximum dose against the child's weight before drawing up the syringe. Early signs are perioral tingling, metallic taste, tinnitus, and agitation; progression brings seizures and then cardiovascular collapse. If it occurs, stop injecting, call for help, protect the airway, and treat with intravenous lipid emulsion according to the local protocol. The pitfall is the child who receives several incremental doses without a running total — keep a written dose tally for every infiltration. [10]
Prognosis & Disposition
Most simple paediatric lacerations heal well with primary intention closure and leave an acceptable scar that fades over twelve to eighteen months. The outcome is driven by the site, the mechanism, the child's skin type, and the quality of the repair and aftercare, rather than by the brand of adhesive or the suture material. The candidate should leave the family with a clear expectation: a visible scar that softens and lightens over time, with a small scar on the face of a child likely to be barely noticeable at maturity if the repair is clean. [3]
Disposition is usually home with written wound-care advice. Keep the wound clean and dry for forty-eight hours, avoid soaking, do not pick at glue or sutures, and protect the healing scar from sun. Return promptly with spreading redness, increasing pain, swelling, discharge, or fever. Give a concrete review or removal date: forty-eight hours for contaminated or bite wounds, five days for facial sutures, seven days for the scalp and trunk, and ten to fourteen days for the limbs and over joints. A child managed with tissue adhesive needs no removal appointment. [1]
The long shadow of a badly managed repair is behavioural, not just cosmetic. The 2024 post-discharge study found that a meaningful proportion of children develop maladaptive behavioural changes — sleep disturbance, new fears, procedural avoidance — after paediatric laceration repair, predicted by high in-procedure distress. Painless, child-centred repair is therefore not only kinder in the moment; it protects the child's relationship with healthcare for years. Frame the prognosis for the examiner in those terms. [3]
Special Populations
The frightened or neurodivergent child deserves a planned approach. Children with autism, intellectual disability, or anxiety, and very young children, need preparation, environmental modification, a child-life worker, and often procedural sedation to tolerate repair safely. Holding a child down without adequate analgesia is poor practice and predicts lasting procedural anxiety; plan and resource the encounter instead. [2]
The child with a bleeding disorder or on anticoagulation can still have a laceration repaired, but plan for haemostasis: use tissue adhesive where possible, apply prolonged firm pressure, and involve the haemophilia team for factor cover before and after repair. The child with eczema or sensitive skin tolerates tissue adhesive and adhesive strips poorly and may need sutures to avoid skin stripping. The child with a bite wound or a contaminated injury needs the antibiotic, irrigation, and review pathway, not simple primary closure. [1] [12]
For Aboriginal, Torres Strait Islander, Māori, and migrant and refugee children, and for children in remote communities or poverty, two equity points matter. Access to review and suture removal is harder when distance or cost is a barrier, so choose closure methods that minimise return visits (tissue adhesive or absorbable sutures where safe) and give clear, culturally appropriate, translated advice. And bites and contaminated wounds may present later in remote settings, raising infection risk — have a low threshold for irrigation, debridement, and antibiotic prophylaxis. A fellowship candidate should frame wound care in these children as an equity issue. [1]
Evidence, Guidelines & Regional Differences
The guidelines are strikingly concordant across regions. The Royal Children's Hospital Melbourne, the Advanced Paediatric Life Support course used across Australia and New Zealand, NICE in the United Kingdom, and the American and Canadian paediatric emergency bodies all agree on the same core method: assess thoroughly, provide adequate analgesia (topical first), irrigate well, close with the method that matches tension and site, and follow up appropriately. [1] [4]
The strongest recent evidence settles three practical questions. First, tap water is as effective as sterile saline for wound irrigation in children — a randomised trial and subsequent systematic reviews show no difference in infection rates, with the practical benefit of lower cost and unlimited volume. [9] Second, topical anaesthesia (LET) is effective and should be the default first step for paediatric laceration repair, reducing the pain of infiltration itself and of the whole procedure; quality-improvement work shows its routine use is achievable and improves the family experience. [4] [5] [11] Third, combined pharmacologic and non-pharmacologic distress management reduces procedural distress and its behavioural aftermath, supporting the child-centred approach. [2] [7]
The tissue-adhesive literature, opened by the 1993 randomised trial comparing adhesive with suturing for paediatric facial lacerations, has established glue as a safe and effective first choice for clean, low-tension wounds, with equivalent cosmetic outcomes, faster application, and no painful removal — provided it is reserved for the right wounds. [8]
[1] [9]The genuine controversies are narrow. Whether all bite wounds should be left open or selectively closed at low-risk sites is debated; current consensus is to avoid primary closure of hand bites and to irrigate and consider delayed closure or healing by secondary intention with antibiotics. Whether absorbable sutures should replace non-absorbable sutures in children to spare them removal is an active trend, with evidence supporting equivalent cosmetic outcome and much less distress. The exact LET dwell time (twenty versus thirty minutes) and whether three applications are better than one are settled in favour of adequate dwell time and repeat application if anaesthesia is incomplete. [5] [12]
Exam Pearls
A fellowship candidate should leave the examiner with a small set of sharp, sourced facts. Memorise these and you will answer any question on this topic. [1] [8]
The five-step sequence is the single highest-yield frame: assess, clean, anaesthetise, close, dress (with advice and follow-up). State it first. The default analgesic is topical LET gel applied for twenty to thirty minutes, which makes even infiltration painless. The local anaesthetic maximum doses are lidocaine three milligrams per kilogram plain and seven milligrams per kilogram with adrenaline, bupivacaine two milligrams per kilogram — calculate them against weight before drawing up. [4] [10]
Irrigate with tap water, which is as effective as sterile saline in children. Tissue adhesive is first choice for clean, low-tension, simple lacerations under five centimetres — never on mucosa, high-tension skin, bites, or infected wounds. Sutures are for high-tension, deep, or precise-cosmesis wounds; choose the size by site (6-0 face, 4-0 to 5-0 trunk and limbs) and remove at five days on the face, seven on the scalp and trunk, ten to fourteen on the limbs. [8] [9]
For bites, irrigate copiously, avoid primary closure of hand bites, give amoxicillin-clavulanate prophylaxis for high-risk wounds, and check tetanus status. Never close a wound over a suspected foreign body, an open fracture, or a tendon or nerve injury — those need imaging, debridement, or specialist repair. Remember that the frightened child deserves child-centred preparation, distraction, and adequate analgesia, because procedural distress has lasting behavioural consequences. [2] [12]
References
- [1]Duvidovich S, Finkelstein Y, Pecaric-Miklavcic S, et al Pediatric wound care in the emergency department Pediatric Emergency Medicine Practice, 2025.PMID 40193561
- [2]Siu A, Abou Assad N, Ali S, et al Pharmacologic Procedural Distress Management During Laceration Repair in Children: A Systematic Review Pediatric Emergency Care, 2024.PMID 37487548
- [3]Martin SR, Utukuri M, Woodland J, et al Paediatric laceration repair in the emergency department: post-discharge pain and maladaptive behavioural changes Emergency Medicine Journal, 2024.PMID 38724104
- [4]Jordan F, Maconochie I, Lyttle MD Topical Anesthetic for Laceration Repair in Children Pediatric Emergency Care, 2023.PMID 36715288
- [5]Siembieda J, Alletag M, Breyer M, et al Triple Versus Single Application of Lidocaine, Epinephrine, and Tetracaine for Laceration Repair in Children Pediatric Emergency Care, 2022.PMID 35100752
- [6]Resch K, Jacobi C, Cnossen W, et al Topical anesthesia for pediatric lacerations: a randomized trial of lidocaine-epinephrine-tetracaine solution versus gel Annals of Emergency Medicine, 1998.PMID 9832666
- [7]Mulcrone AE, Vitale M, Donoghue A, et al Minimal Sedation Use for Laceration Repair in the Pediatric Emergency Department Journal of Emergency Medicine, 2025.PMID 40561621
- [8]Quinn J, Wells G, Sutcliffe T, et al A randomized, controlled trial comparing a tissue adhesive with suturing in the repair of pediatric facial lacerations Annals of Emergency Medicine, 1993.PMID 8517562
- [9]Valente JH, Forti RJ, Freundlich LF, et al Wound irrigation in children: saline solution or tap water? Annals of Emergency Medicine, 2003.PMID 12712026
- [10]Saraghi M, Hersh EV Local anesthetic calculations: avoiding trouble with pediatric patients General Dentistry, 2015.PMID 25574719
- [11]Faris N, Gallentine A, Battaglia M, et al Applying Topical Anesthetic on Pediatric Lacerations in the Emergency Department: A Quality Improvement Project Pediatric Emergency Care, 2024.PMID 37616570
- [12]Jakeman M, Opilla R, Patel S, et al Pet dog bites in children: management and prevention BMJ Paediatrics Open, 2020.PMID 32821860