Paeds · investigations-procedures-and-technology
Suprapubic aspiration and urinary catheterisation
Also known as Suprapubic aspiration · SPA · Urethral catheterisation · In-out catheterisation · Bladder tap · Urine collection for culture · Paediatric urinary catheter · Catheter-associated urinary tract infection
Fellowship guide to suprapubic aspiration and urethral catheterisation in infants and children. Covers the four urine collection methods and their contamination rates, the anatomical landmark of one to two centimetres above the pubic symphysis in the midline for the suprapubic aspiration, the role of the point-of-care bladder ultrasound in raising the success rate, the paediatric catheter sizing of a 6 to 8 French feeding tube for an infant and an 8 to 10 French catheter for an older child, the aseptic no-touch technique, the management of the failed tap, and the catheter-associated urinary tract infection prevention bundle in which the dwell time is the single strongest modifiable risk factor.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Suprapubic aspiration and urethral catheterisation are the two procedures that obtain an uncontaminated urine sample from the bladder of the infant or the young child who cannot produce a clean catch specimen. The suprapubic aspiration passes a fine needle through the lower abdominal wall into the distended bladder, and the urethral catheterisation passes a sterile catheter through the urethra into the bladder. The shared purpose is to collect urine for the culture that confirms or excludes the urinary tract infection, which is the most common serious bacterial infection in the febrile infant. The choice between the two methods is a practical trade-off between the lowest contamination and the lowest invasiveness, and both are recommended over the bag and the pad method for any sample used to diagnose an infection. [1]
The clinical question that drives the procedure is the source of the fever in the young child. The American Academy of Pediatrics clinical practice guideline states that a urine specimen must be obtained by the catheterisation or the suprapubic aspiration, and the result known, before any antimicrobial is started in the febrile infant two to twenty-four months in whom a urinary tract infection is suspected. The reason is operational and not academic. A contaminated bag specimen produces a false positive culture, the unnecessary antibiotic treatment, and the missed true source of the fever, and any antibiotic given before a clean sample makes the culture uninterpretable. [1]
The urethral catheterisation has a second and distinct role beyond the diagnosis. The indwelling catheter monitors the urine output in the acutely unwell child, decompresses the bladder in the obstruction, and delivers the bladder medications. The same procedure therefore serves the diagnostic and the therapeutic pathways, and the catheter-associated urinary tract infection is the complication that links the two roles and the prevention bundle to the daily ward and the intensive care practice. [2]
Classification
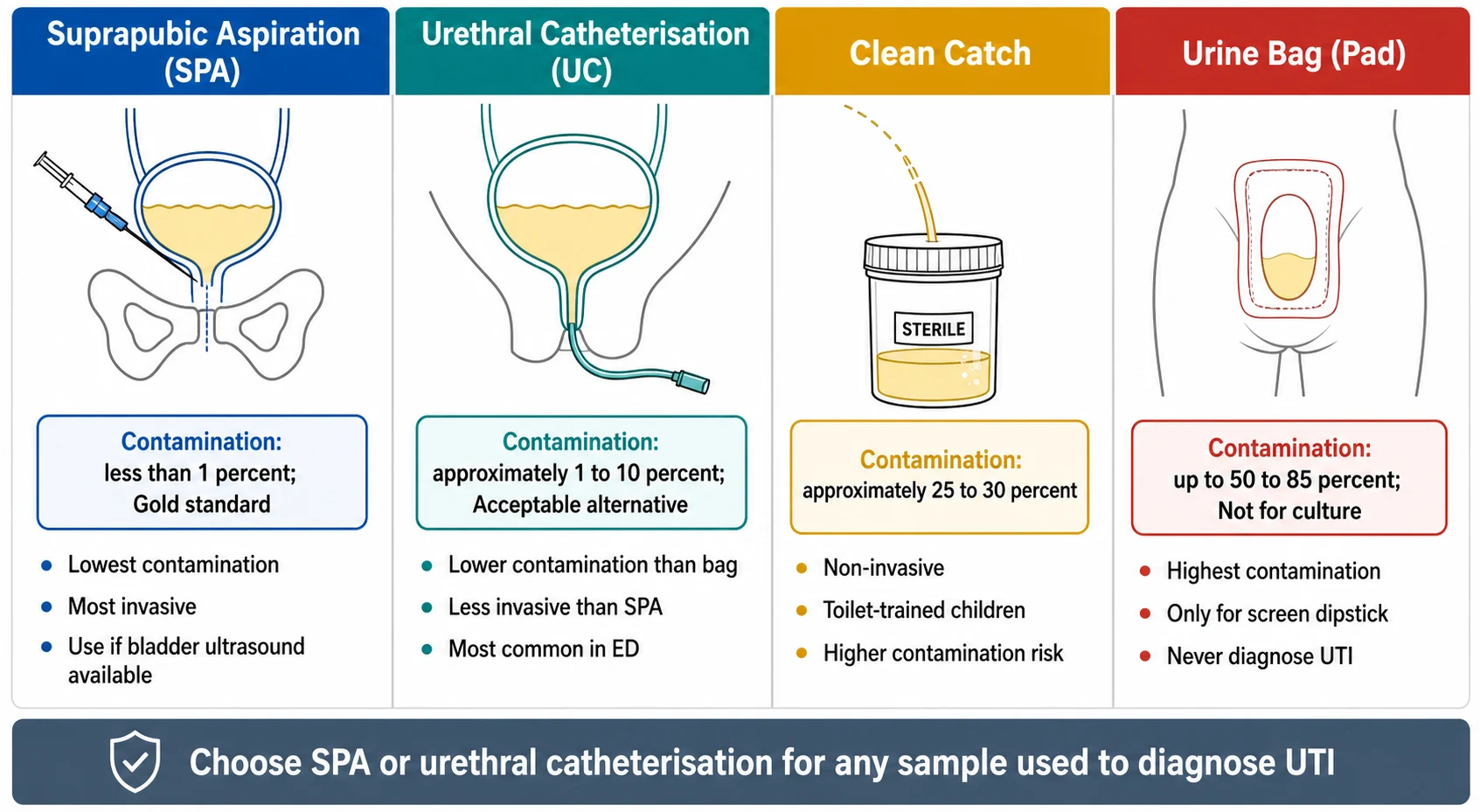
The classification of the urine collection methods rests on the contamination rate, because the contamination is the property that determines whether the culture result is interpretable. The suprapubic aspiration is the historical gold standard because it samples the bladder urine directly through a sterile needle, bypassing the urethra and the perineal flora. The contamination rate is under 1 percent, and any organism that grows from a suprapubic aspirate is a true pathogen because the bladder urine is normally sterile. The urethral catheterisation is the acceptable alternative because it samples the bladder urine through a sterile catheter that passes the urethra, with a small but real contamination from the urethral flora, at a rate of approximately 1 to 10 percent. [5]
The clean catch is the first-line method for the toilet-trained child who can cooperate, but it has a contamination rate of approximately 25 to 30 percent because the stream passes the perineum. The bag and the pad method, in which the collection bag is stuck to the perineum or the pad absorbs the urine, has a contamination rate of up to 50 to 85 percent because the periurethral and the perineal flora multiply in the bag and the pad. The bag specimen is therefore suitable only for a screen dipstick that, if negative, excludes the infection without the need for the invasive collection, and a positive screen must always be confirmed by the suprapubic aspiration or the catheterisation before the antibiotic is started. [5]
The clinical consequence of the contamination is the false positive culture. A bag specimen that grows a mixed flora or a low count of the common organism is uninterpretable, and the temptation to start the antibiotic on the basis of the result is the source of the unnecessary treatment, the antibiotic resistance, and the missed alternative diagnosis. The corollary is that a negative dipstick on a bag specimen is useful because it lowers the probability of the infection enough to defer the invasive collection, but a positive dipstick on a bag specimen mandates the confirmatory catheterisation or the aspiration before the antibiotic. [6]
Epidemiology & Risk Factors
The suprapubic aspiration and the urethral catheterisation are performed whenever a sterile urine sample is needed in the child who cannot produce a clean catch. The commonest indication is the febrile illness in the infant or the young child, because the urinary tract infection is the most common serious bacterial infection in this age group, with a prevalence of approximately 5 to 7 percent in the febrile infant under two years and a higher prevalence of approximately 7 to 9 percent in the febrile infant under three months. The high background prevalence is the reason the invasive collection is the default rather than the exception in the well-appearing but febrile young infant. [1]
The risk factors for the failed suprapubic aspiration are the empty or the under-filled bladder, the wrong landmark or the wrong angle, the absence of the ultrasound guidance, and the operator inexperience. The failed tap is the most common adverse outcome of the aspiration, reported in approximately 25 to 50 percent of the blind attempts, and the single most effective intervention is the confirmation of the bladder volume before the procedure. The risk factors for the catheter-associated urinary tract infection are the longer dwell time as the strongest modifiable factor, the young age, the female sex in some series, the underlying urinary tract abnormality such as the reflux or the posterior urethral valves, the absence of the closed drainage system, and the breach of the aseptic technique. [11]
The epidemiological shift in the procedural practice is the move from the blind to the ultrasound-guided suprapubic aspiration and from the reusable to the single-use catheterisation sets. The point-of-care bladder ultrasound has moved from the radiology department to the bedside, and the systematic review of the randomised and the observational evidence shows that the ultrasound guidance raises the success rate of the aspiration from approximately 50 to 70 percent in the blind technique to over 90 percent in the guided technique. The trend reflects the wider principle that the confirmation of the anatomical target before the procedure improves the yield and the safety. [8]
Pathophysiology
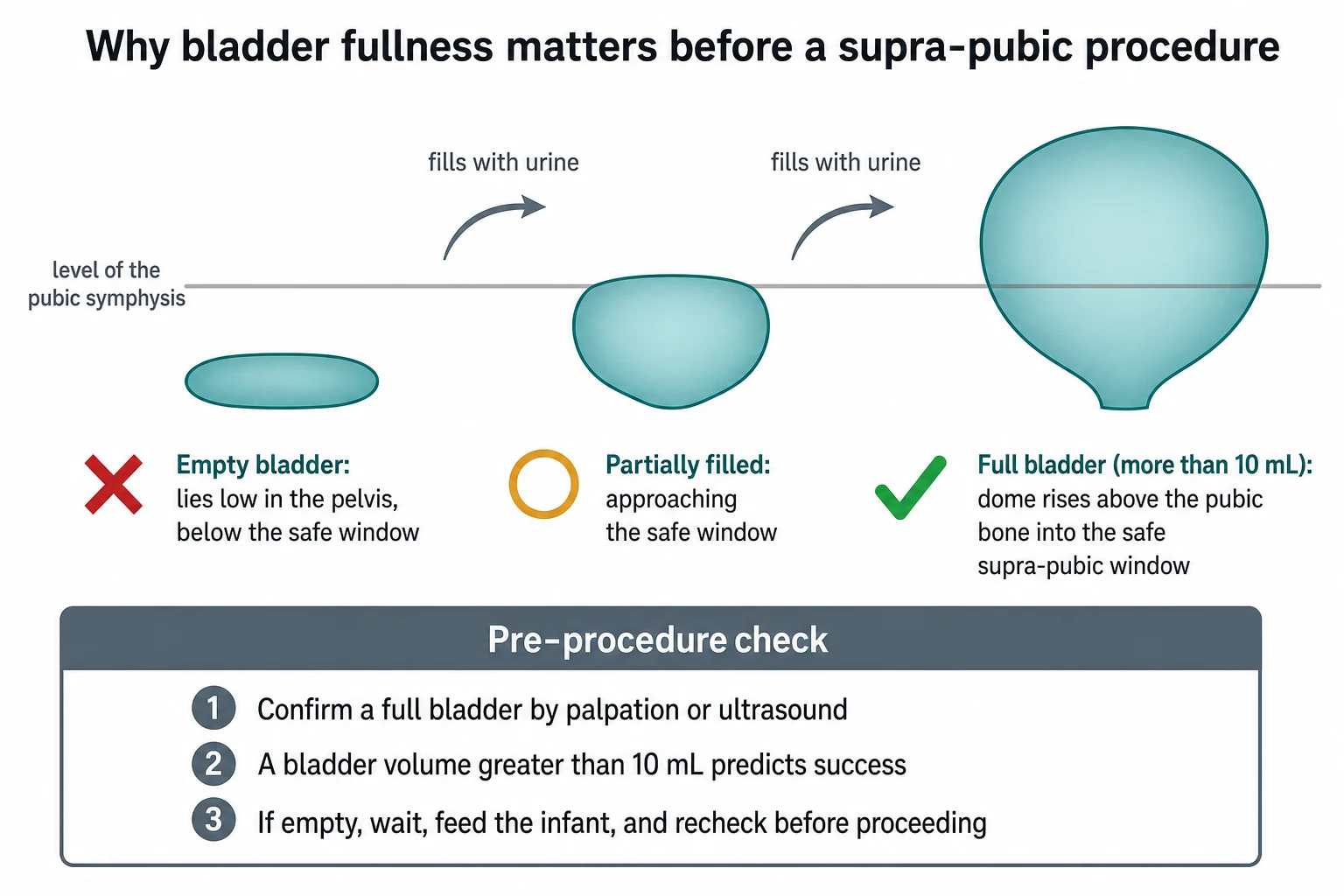
The anatomical basis of the suprapubic aspiration is the position of the full bladder in the infant. The full bladder rises out of the pelvis as a dome that sits above the pubic symphysis and lifts the bowel out of the anterior abdominal wall, which is why the midline needle one to two centimetres above the pubic symphysis reaches the bladder lumen without encountering the bowel. The empty bladder, in contrast, collapses below the pubic symphysis into the true pelvis, and the bowel falls into the space the full bladder occupied, so a needle aimed at the expected position of the bladder may pass through the bowel instead. The fullness of the bladder is therefore the single most important determinant of the safety and the success of the aspiration. [6]
The urethral anatomy determines the catheter size and the technique. The female urethra is short and straight, and the meatus lies anterior to the vaginal opening, so the catheter passes directly with the gentle advancement. The male urethra is longer and curves through the prostatic and the membranous urethra, so the catheter must be advanced with the penis held on gentle upward traction to straighten the curve, and the resistance in the male may signal a stricture, a posterior urethral valve, or a meatal stenosis. The wrong technique in either sex causes the trauma, the false passage, and the later stricture. [6]
The catheter-associated infection arises from the periurethral flora that ascends along the outside or the inside of the catheter and forms a biofilm on the surface. The biofilm protects the bacteria from the antibiotic and the immune clearance, and the risk of the symptomatic infection rises with every day the catheter remains in place. The pathophysiology is the basis for the prevention bundle: the avoidance of the unnecessary catheter removes the biofilm substrate, the aseptic insertion reduces the inoculum, the closed drainage system limits the ascending migration, and the prompt removal ends the biofilm accumulation. [11]
Clinical Presentation
The clinical presentation that triggers the urine collection is the febrile infant, the ill child with the suspected sepsis, and the child who needs the accurate urine output monitoring or the bladder decompression. The non-toilet-trained child cannot produce a clean catch specimen on command, which is the practical reason the invasive collection is required. The typical patient is the febrile infant under two years, often with no localising signs, in whom the urinary tract infection is the leading serious bacterial diagnosis. The very young infant under three months, the ill-appearing child, and the child with the documented bacteraemia are the highest-priority groups. [1]
The contraindications and the cautions to the suprapubic aspiration must be recognised before the procedure. The empty bladder is the most common and the most important, because the aspiration on the empty bladder risks the failed tap and the bowel injury. The coagulopathy and the anticoagulant are the relative contraindications, managed by the correction or the timing. The abdominal wall infection at the site, the distended abdomen from the organomegaly or the pelvic mass, and the abnormal lower urinary tract anatomy such as the cloacal anomaly or the bladder exstrophy are the contraindications that favour the catheterisation or the specialist referral. [6]
The modes of presentation that trigger the procedure
The febrile infant under two years with no localising source, the default indication for the sterile urine sample
The ill-appearing infant or child with the suspected sepsis, where the urine is one of the cultures obtained before the antibiotic
The febrile neonate under one month, who needs the full septic work-up including the urine by catheterisation or aspiration
The acutely unwell child who needs the indwelling catheter for the urine output monitoring
The child with the urinary retention or the bladder outlet obstruction who needs the decompression
The child with the neurogenic bladder who needs the long-term clean intermittent catheterisation
The presentation of the child who needs the indwelling catheter is shaped by the acute illness. The child in the shock, the severe dehydration, the burns, or the postoperative state needs the accurate hourly urine output, and the indwelling catheter is the most reliable method. The child with the spinal cord lesion, the sacral agenesis, or the postoperative bladder surgery may need the catheter for the bladder emptying. The child with the posterior urethral valves or the urethral trauma may need the catheter for the decompression. Each indication carries the catheter-associated infection risk, and the daily review of the ongoing need is the prevention practice that links the insertion to the removal. [11]
Differential Diagnosis
The differential at the procedural level is the choice of the urine collection method for the clinical question. For the diagnosis of the urinary tract infection in the non-toilet-trained child, the suprapubic aspiration and the urethral catheterisation are the indicated methods, and the choice between them rests on the local practice, the operator skill, and the availability of the ultrasound. The aspiration gives the lowest contamination but is the more invasive and the more technically demanding, and the catheterisation gives the slightly higher contamination but is the easier to learn and the more commonly used in the emergency department. The systematic review by Phillips concluded that the two methods are broadly comparable for the contamination, with the aspiration favoured where the catheterisation is difficult or refused. [7]
The second distinction is between the diagnostic and the therapeutic catheterisation. The in-out catheterisation collects the specimen and removes the catheter, with the minimal infection risk. The indwelling catheterisation leaves the catheter in the bladder for the output monitoring or the decompression, with the rising infection risk. The choice is dictated by the indication, and the indwelling catheter must not be placed for the diagnostic collection alone. The suprapubic catheter, placed by the urologist for the long-term bladder management in the neurogenic bladder or the urethral trauma, is a separate procedure from the bedside suprapubic aspiration. [11]
Suprapubic aspiration
- Gold standard, contamination under 1 percent
- Needle through the lower abdominal wall in the midline
- Any growth from the aspirate is significant
- Failed tap in 25 to 50 percent of blind attempts, reduced to under 10 percent with ultrasound
Urethral catheterisation
- Acceptable alternative, contamination 1 to 10 percent
- Catheter through the urethra into the bladder
- Commonest method in the emergency department
- Lower risk of the failed sample when the bladder is small or empty
Indwelling catheter
- Therapeutic role for the output monitoring and the decompression
- Closed drainage system connected
- Catheter-associated infection risk rises with the dwell time
- Daily review and prompt removal are the prevention practice
Bag or pad
- Contamination up to 50 to 85 percent
- For the screen dipstick only, never for the culture
- A negative screen excludes the infection and avoids the invasive collection
- A positive screen must be confirmed by the catheterisation or the aspiration
The third distinction is between the methods when the bladder is empty or the child is constipated. The suprapubic aspiration on the empty bladder is contraindicated, and the catheterisation may recover the small residual volume. The constipated child with the stool-loaded rectum may distort the bladder and the urethra, and the gentle technique and the patience are required. The child with the labial adhesions, the phimosis, or the meatal stenosis may make the catheterisation difficult, and the specialist help is sought rather than the forceful attempts. [6]
Clinical & Bedside Assessment
The bedside assessment before the procedure confirms the indication, the urgency, and the absence of the contraindications. Confirm the indication for the sterile urine sample, the suspected sepsis, or the output monitoring. Examine the abdomen for the distension, the organomegaly, the palpable bladder, and the abdominal wall lesions that would contraindicate the aspiration. Check the coagulation status and the anticoagulant medication, the platelet count, and the recent surgery. Assess the hydration, the time since the last void, and the time since the last feed. [6]
The positioning of the infant is the foundation of the safe procedure. Place the infant supine in the frog-leg position with the hips slightly flexed and abducted, and have an assistant stabilise the pelvis and the limbs, because the movement of the child at the moment of the needle or the catheter insertion is the cause of the injury and the failed sample. For the suprapubic aspiration, palpate the pubic symphysis and confirm the bladder is full by the palpable bladder dome or the point-of-care ultrasound; if uncertain, wait thirty to sixty minutes, feed the infant, or use the ultrasound to confirm the bladder volume greater than 10 millilitres before the attempt. [6]
The consent is obtained appropriate to the urgency. In the planned setting, the family is told that the urine sample is needed to confirm or exclude the infection, that the bag specimen cannot be relied upon for the culture, and that the catheterisation or the aspiration is the standard method. The common and the important risks are explained: the failed tap and the need for the second attempt in the aspiration, the transient haematuria in both procedures, the urethral trauma in the catheterisation, and the catheter-associated infection in the indwelling catheter. In the emergency, the consent is implied, and the explanation is given alongside the procedure. [6]
Investigations
The investigation here is the urine sample itself. The suprapubic aspirate is sent for the microscopy, the culture, and the sensitivity. The defining rule is that any organism grown from a suprapubic aspirate, at any colony count, is a true pathogen, because the bladder urine is normally sterile and the needle bypasses the urethral flora. The catheter specimen has the threshold of the single organism at greater than 10 000 to 50 000 colony forming units per millilitre, and the mixed growth or the low count suggests the contamination and the repeat collection. The culture result is the definitive test, and it takes twenty-four to forty-eight hours. [1]
The urinalysis by the dipstick or the microscopy gives the immediate preliminary result. The positive leukocyte esterase and the nitrite raise the probability of the infection, but the nitrite is unreliable in the young infant who voids frequently and does not allow the bladder dwell time for the nitrate conversion. The microscopy of greater than 5 to 10 white cells per high power field supports the infection. The negative dipstick in the well-appearing child lowers the probability enough to defer the antibiotic while the culture is awaited, but the positive dipstick is not sufficient to start the antibiotic without the supporting culture from the low-contamination sample. [1]
The point-of-care bladder ultrasound before the suprapubic aspiration measures the bladder volume and predicts the success. The systematic review by Abosamak and colleagues showed that the point-of-care ultrasound guidance raised the success rate of the suprapubic aspiration from approximately 50 to 70 percent in the blind technique to over 90 percent in the guided technique, and the randomised trial by Mahdipour and colleagues confirmed the benefit. The volume greater than 10 millilitres is the commonly used threshold for the attempt, and the volume below 10 millilitres warrants the wait, the feed, or the deferral. The ultrasound is therefore the standard preparation wherever it is available. [8]
Management — Resuscitation
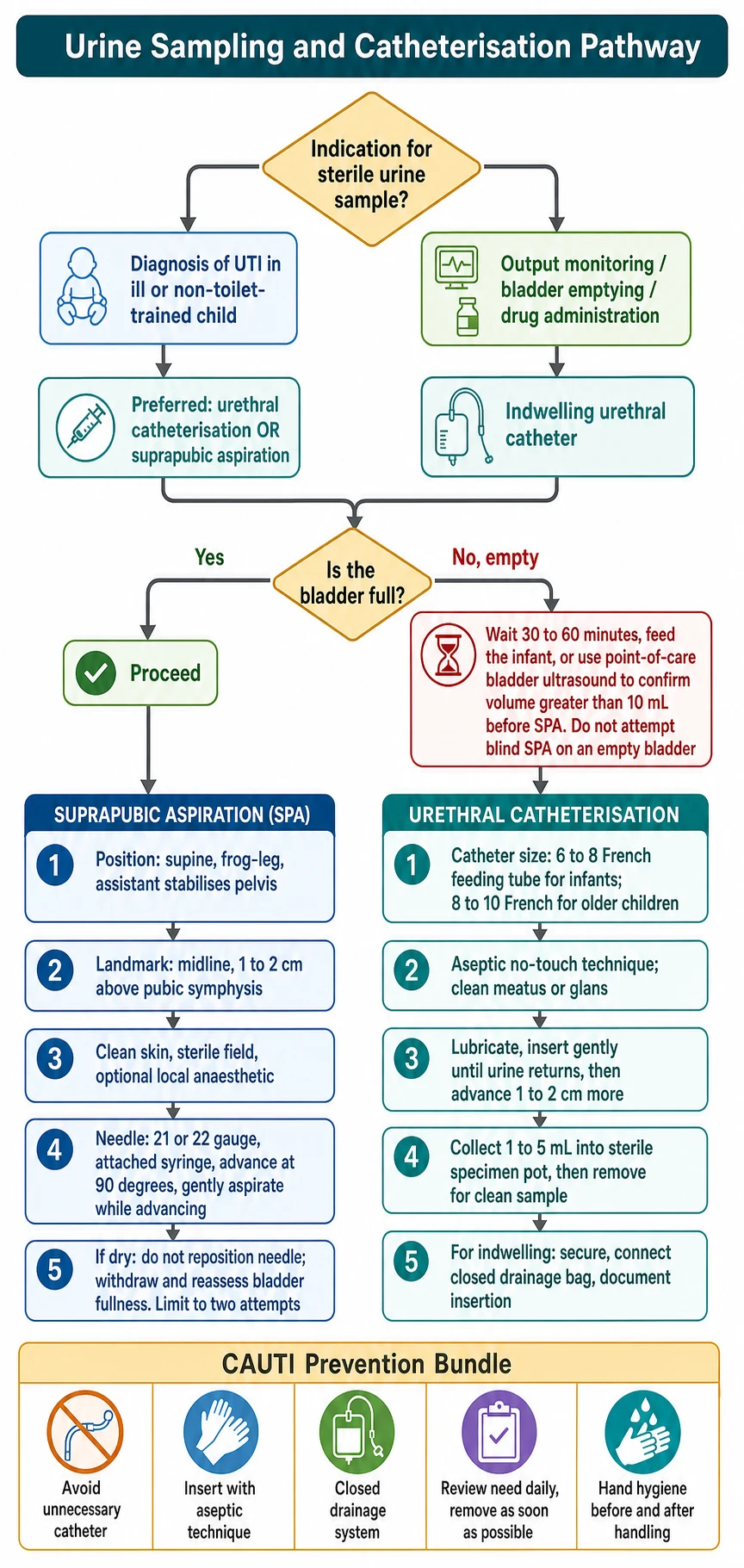
The procedural management begins with the preparation, the analgesia, and the aseptic technique. Gather the equipment: the sterile field, the 21 or 22 gauge needle with the attached syringe for the aspiration, the 6 to 8 French feeding tube for the infant catheter and the 8 to 10 French for the older child, the water-soluble lubricant, the chlorhexidine, the sterile gloves, and the specimen pots. Use the non-pharmacological analgesia of the oral sucrose and the pacifier in the infant, and consider the topical local anaesthetic at the suprapubic aspiration site. [6]
The suprapubic aspiration is performed at the midline one to two centimetres above the pubic symphysis. After the skin preparation and the sterile field, the needle attached to the syringe is advanced at 90 degrees to the skin with the gentle aspiration, and the urine appears in the syringe as the bladder lumen is entered. The angle is directed slightly toward the bladder, and the depth in the infant is typically 2 to 3 centimetres. If no urine is aspirated, the needle is withdrawn slowly with the continuous aspiration, because the bladder may be entered on the way out. The procedure is limited to two attempts, and the failed second attempt warrants the wait, the ultrasound, or the catheterisation. [6]
Non-pharmacological analgesia for the suprapubic aspiration or the catheterisation in the infant
Dose
Oral sucrose 1 to 2 mL of a 24 percent solution two minutes before the procedure
The urethral catheterisation is performed with the aseptic no-touch technique. After the meatal cleaning, the lubricated catheter is inserted gently until the urine returns, then advanced one to two centimetres more to ensure the intravesical position. In the male, the penis is held on the gentle upward traction to straighten the urethra, and the resistance is met with the pause and the gentle advancement rather than the force. In the female, the meatus is visualised anterior to the vaginal opening, and the catheter is directed upward and inward. The specimen is collected into the sterile pot before the removal for the clean sample, and the closed drainage bag is connected for the indwelling catheter. [6]
Management — Definitive & Stepwise
[6]The definitive stepwise management is the avoidance of the failed tap, the trauma, and the infection through the correct technique and the preparation. The point-of-care ultrasound guidance is the single most effective step for the suprapubic aspiration. The systematic review by Abosamak and colleagues pooled the randomised and the observational studies and found that the ultrasound guidance raised the success rate to over 90 percent, compared with the 50 to 70 percent of the blind technique. The earlier study by Buntsma and colleagues showed the same benefit with the BladderScan device, and the randomised trial by Mahdipour and colleagues confirmed the advantage in the infants. The practical implication is that the ultrasound is the standard preparation wherever the device is available, and the blind attempt is reserved for the situation where the ultrasound is unavailable and the clinical urgency is high. [8]
The definitive technique of the urethral catheterisation prevents the trauma and the meatal injury through the correct catheter size, the generous lubrication, the gentle advancement, and the aseptic no-touch practice. The 6 to 8 French feeding tube is the standard for the infant, and the 8 to 10 French catheter for the older child. The forceful insertion against the resistance is the source of the urethral trauma, the false passage, and the later stricture, and the response to the resistance is the pause, the repositioning, and the urology referral rather than the force. [6]
The definitive management of the indwelling catheter is the catheter-associated urinary tract infection prevention bundle. The bundle has five elements: the avoidance of the unnecessary catheter, the aseptic insertion, the closed drainage system, the daily review of the ongoing need, and the prompt removal. The systematic review by Araujo da Silva and colleagues of the interventions to prevent the catheter-associated infections in the children and the neonates concluded that the multifaceted bundle approach and the daily review of the indication are the best-supported interventions, and the single most important determinant is the dwell time. The study by Lee and colleagues of the risk factors for the catheter-associated infections in the paediatric institution confirmed that the longer dwell time and the underlying urinary tract abnormality are the strongest predictors. [12]
Specific Subtypes & Scenarios
The suprapubic aspiration in the neonate and the young infant is favoured by the high position of the full bladder, the low morbidity, and the very young age group in whom the urinary tract infection is the leading serious bacterial diagnosis. The point-of-care ultrasound guidance is especially valuable in this age group, because the small bladder is difficult to assess by the palpation alone. The neonate with the fever under one month needs the full septic work-up including the urine by the catheterisation or the aspiration, and the specimen is obtained before the empirical antibiotic. [6]
The urethral catheterisation in the male infant requires the straightening of the urethra by the gentle upward traction on the penis, and the recognition of the urethral resistance that may indicate the stricture, the posterior urethral valve, or the meatal stenosis. The resistance is met with the pause and the gentle advancement, never the force, and the persistent resistance warrants the urology referral. The urethral catheterisation in the female requires the clear visualisation of the meatus, which lies anterior to the vaginal opening and may be hidden by the labia, and the avoidance of the insertion into the vagina, which is the common technical error. [6]
FULL for the prevention of the failed suprapubic aspiration
The child with the neurogenic bladder from the spina bifida or the spinal cord lesion needs the long-term bladder management that may include the clean intermittent catheterisation, the anticholinergic medication, and the suprapubic catheter placed by the urologist. The clean intermittent catheterisation is the technique the family and the older child are taught to perform at home, and it is the standard of care for the neurogenic bladder because it preserves the upper tracts and reduces the infection risk compared with the indwelling catheter. The child with the complex chronic and the technology-dependent condition has the higher exposure to the catheterisation and the higher risk of the catheter-associated infection with the multi-resistant organism, which raises the threshold for the catheter and the vigilance for the removal. [11]
[4]Complications & Pitfalls
The complications of the suprapubic aspiration are the failed tap from the empty bladder, reported in approximately 25 to 50 percent of the blind attempts and reduced to under 10 percent with the ultrasound, the transient microscopic haematuria in approximately 1 to 8 percent, the macroscopic haematuria, the bladder wall injury, and the rare bowel perforation or the intraperitoneal injury that occurs when the bladder is empty and the bowel is in the needle path. The complications of the urethral catheterisation are the urethral trauma and the meatal injury from the forceful insertion, the urethral stricture from the repeated trauma, the bladder spasm, the bypassing of the urine around the catheter, and the catheter-associated urinary tract infection that rises with every day of the dwell time. [6]
The systematic review by Araujo da Silva and colleagues of the interventions to prevent the catheter-associated infections in the children and the neonates found that the bundle approach and the daily review of the indication are the best-supported interventions, and the single most important risk factor is the dwell time. The study by Lee and colleagues of the risk factors in the paediatric institution confirmed the longer dwell time and the underlying urinary tract abnormality as the strongest predictors. The practical implication is that the avoidance of the unnecessary catheter and the prompt removal are the two interventions that prevent the most infections. [12]
The classic pitfalls are the procedural and the diagnostic errors. The first pitfall is the failure to confirm the bladder is full before the suprapubic aspiration, which produces the failed tap and the risk of the bowel injury. The second pitfall is the wrong landmark below or at the pubic symphysis, which misses the bladder and enters the bowel or the pelvic structures. The third pitfall is the failure to use the ultrasound where available, which forgoes the single most effective step for the success. The fourth pitfall is the forceful urethral catheterisation against the resistance, which causes the urethral trauma and the later stricture. The fifth pitfall is the open drainage system or the breach of the aseptic technique, which raises the catheter-associated infection risk. The sixth pitfall is the failure to remove the indwelling catheter promptly, which allows the biofilm to accumulate and the infection to develop. [6]
Prognosis & Disposition
The prognosis after the urine collection is the prognosis of the underlying condition and the diagnostic yield of the sample. The well-collected suprapubic aspirate or the catheter specimen gives the confident diagnosis and the targeted antimicrobial treatment, and the poorly collected specimen delays the diagnosis and leads to the unnecessary or the prolonged antibiotics. The child who undergoes the uncomplicated suprapubic aspiration or the urethral catheterisation recovers immediately, and the transient haematuria resolves within twenty-four to forty-eight hours without the intervention. [6]
The child with the catheter-associated infection has the prognosis of the urinary tract infection modified by the underlying abnormality. The systematic review by Araujo da Silva and colleagues supports the bundle approach and the daily review as the interventions that reduce the incidence in the intensive care and the ward settings. The prevention bundle is the disposition practice: the catheter is placed only for the clear indication, the closed drainage is maintained, the ongoing need is reviewed daily, and the removal is documented as soon as the indication ends. [12]
The disposition after the procedure is the return to the clinical pathway of the underlying illness, the result of the culture in twenty-four to forty-eight hours, and the follow-up for the confirmed infection. The child with the confirmed urinary tract infection is treated with the antibiotic course, the imaging is considered for the recurrent or the atypical infection, and the follow-up addresses the renal function and the blood pressure. The child with the negative culture is reassessed for the alternative source of the fever, and the antibiotic is withheld or stopped. The catheter-associated infection is managed with the catheter removal, the culture-guided antibiotic, and the review of the indication for the re-catheterisation. [1]
Special Populations
The neonate and the young infant under two months are the highest-yield group for the invasive urine collection because the urinary tract infection is the most common serious bacterial infection and the clean catch is rarely possible. The febrile neonate under one month needs the full septic work-up including the urine by the catheterisation or the aspiration, and the specimen is obtained before the empirical antibiotic. The suprapubic aspiration with the ultrasound guidance is especially suitable in this age group because of the high position of the full bladder and the low morbidity, and the catheterisation is the alternative where the aspiration is declined or unavailable. [1]
The child with the neurogenic bladder from the spina bifida, the spinal cord lesion, or the sacral agenesis needs the long-term bladder management that may include the clean intermittent catheterisation and the suprapubic catheter placed by the urologist. The clean intermittent catheterisation is the technique the family and the older child are taught to perform at home, and it is the standard of care for the neurogenic bladder because it preserves the upper tracts and reduces the infection risk compared with the indwelling catheter. [11]
The child with the complex chronic and the technology-dependent condition has the higher exposure to the catheterisation and the higher risk of the catheter-associated infection with the multi-resistant organism. The threshold for the catheter is higher in this group, the vigilance for the removal is greater, and the microbiology of the infection is more likely to require the broad-spectrum antibiotic. Aboriginal and Torres Strait Islander children and the children from the remote settings have the higher risk of the delayed presentation and the complications, and the culturally appropriate communication, the consent, and the follow-up are essential to the equitable care. [4]
The child with the suspected abuse or the unexplained urethral injury may need the forensic consideration before the catheterisation, and the documentation and the specialist involvement are the safeguards. The young person with the transition to the adult care and the long-term catheter need the coordinated plan that addresses the bladder management, the renal surveillance, and the reproductive and the sexual health. [11]
Evidence, Guidelines & Regional Differences
The evidence base spans the guidelines, the systematic reviews of the collection methods, and the prevention studies. The American Academy of Pediatrics 2011 clinical practice guideline and its 2016 reaffirmation established the principle that the urine specimen must be obtained by the catheterisation or the suprapubic aspiration before any antimicrobial in the febrile infant two to twenty-four months with the suspected urinary tract infection. The European Association of Urology and the European Society for Paediatric Urology guidelines, updated by 't Hoen and colleagues, and the Swiss consensus recommendations by Buettcher and colleagues provide the European guidance with the same principle. [2]
The systematic review by Abosamak and colleagues of the point-of-care ultrasonography for the suprapubic bladder aspiration pooled the randomised and the observational studies and found that the ultrasound guidance raised the success rate to over 90 percent, compared with the 50 to 70 percent of the blind technique. The earlier study by Buntsma and colleagues showed the benefit with the BladderScan device, and the randomised trial by Mahdipour and colleagues confirmed the advantage in the infants. The systematic review by Araujo da Silva and colleagues of the interventions to prevent the catheter-associated infections in the children and the neonates concluded that the multifaceted bundle approach and the daily review are the best-supported interventions. [8]
AAP 2011
- Pediatrics clinical practice guideline
- Urine by catheterisation or SPA before any antibiotic in the febrile infant two to twenty-four months
- Reaffirmed in 2016
EAU/ESPU 2015
- European urology guidelines on the urinary tract infections in children
- Updated by 't Hoen in 2021
- SPA or catheterisation as the low-contamination methods
Swiss consensus 2021
- European journal of pediatrics recommendations
- Buettcher and colleagues
- Practical thresholds for the collection and the imaging
Abosamak 2026
- Arab journal of urology systematic review and meta-analysis
- Point-of-care ultrasound raises the SPA success to over 90 percent
- Supports the ultrasound as the standard preparation
The Diviney review of the urine collection methods and the dipstick testing in the non-toilet-trained children summarised the contamination rates and the practical considerations, and the Kaufman paper in the Archives of Disease in Childhood Education and Practice provided the practical how-to guide for the collection. The systematic review by Phillips compared the catheter and the aspiration for the contamination and found the two methods broadly comparable. [5]
The regional differences centre on the access to the point-of-care ultrasound, the local preference for the aspiration or the catheterisation, and the catheter-associated infection surveillance. In the well-resourced settings, the ultrasound guidance is the standard for the aspiration, and the prevention bundle is the standard for the indwelling catheter. In the lower-resource settings, the blind aspiration is more common, and the prevention bundle is applied with the available resources. The international guidelines, including the AAP, the EAU and ESPU, and the Swiss consensus, are applicable across the settings, with the intensity of the preparation and the surveillance tailored to the local resources. [4]
Exam Pearls
BUNDLE for the catheter-associated urinary tract infection prevention
References
- [1]Subcommittee on Urinary Tract Infection, Roberts KB Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months Pediatrics, 2011.PMID 21873693
- [2]Stein R, Dogan HS, Hoebeke P, et al Urinary tract infections in children: EAU/ESPU guidelines European Urology, 2015.PMID 25477258
- [3]'t Hoen LA, Bogaert G, Radmayr C, et al Update of the EAU/ESPU guidelines on urinary tract infections in children Journal of Pediatric Urology, 2021.PMID 33589366
- [4]Buettcher M, Trueck J, van der Heijden M, et al Swiss consensus recommendations on urinary tract infections in children European Journal of Pediatrics, 2021.PMID 32621135
- [5]Diviney J, Puar T, Ladhani S, et al Urine collection methods and dipstick testing in non-toilet-trained children Pediatric Nephrology, 2021.PMID 32918601
- [6]Kaufman J, Fitzpatrick P, Tosif S, et al How to... collect urine samples from young children Archives of Disease in Childhood Education and Practice Edition, 2020.PMID 31444213
- [7]Phillips B Towards evidence based medicine for paediatricians. Urethral catheter or suprapubic aspiration to reduce contamination of urine samples in young children? Archives of Disease in Childhood, 2009.PMID 19700430
- [8]Abosamak MF, Elbalty AE, George S, et al Point-of-care ultrasonography for suprapubic bladder aspiration in pediatric patients: A systematic review and meta-analysis Arab Journal of Urology, 2026.PMID 41940116
- [9]Buntsma D, Stock A, Bevan C, et al Success rate of BladderScan-assisted suprapubic aspiration Emergency Medicine Australasia, 2012.PMID 23216726
- [10]Mahdipour S, Zehtabchi S, Soltani S, et al Strengthening the success rate of suprapubic aspiration in infants by integrating point-of-care ultrasonography guidance: A parallel-randomized clinical trial PloS One, 2021.PMID 34265015
- [11]Lee NG, Marchalik D, Lipsky A, et al Risk Factors for Catheter Associated Urinary Tract Infections in a Pediatric Institution Journal of Urology, 2016.PMID 25858421
- [12]Araujo da Silva AR, Mota DM, de Oliveira A, et al Interventions to prevent urinary catheter-associated infections in children and neonates: a systematic review Journal of Pediatric Urology, 2018.PMID 30126746