Paeds · investigations-procedures-and-technology
Umbilical venous and arterial catheterisation
Also known as Umbilical venous catheter · Umbilical arterial catheter · UVC and UAC insertion · Umbilical line depth formula · Neonatal umbilical vessel cannulation
A fellowship approach to umbilical venous and arterial catheterisation in newborns covering the two vessel types and their courses, the high and low umbilical arterial catheter positions with high between T6 and T9 preferred over low at L3 to L4, the umbilical venous catheter target at T8 to T9 at the diaphragm, the Shukla birth-weight depth formula with umbilical arterial catheter length equal to three times birth weight in kilograms plus nine and umbilical venous catheter length equal to half that value plus one, catheter sizing of three point five French under 1500 grams and five French over 1500 grams, dwell limits of five days for the arterial line and fourteen days for the venous line, and the recognition and prevention of complications including malposition, portal vein and aortic thrombosis, lower-limb ischaemia, necrotising enterocolitis and line sepsis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a twenty-eight-week infant who needs arterial blood-gas monitoring and a reliable central line in the first hours of life, a term baby in shock who needs emergency venous access before a peripheral line is possible, and a neonate on the unit whose arterial line has been in for a week. Each of them turns on a different part of the same skill — choosing the right vessel, calculating the right depth, confirming the tip, and knowing when the line must come out. [1] [9]
The umbilical stump carries three vessels at birth: two umbilical arteries, which are thick-walled with a small round lumen, and one umbilical vein, which is thin-walled with a large oval lumen. The arteries return deoxygenated blood from the fetus to the placenta, while the vein carries oxygenated blood back, and after birth these channels stay open for only a short window — the arteries for a few days, the vein for up to a week — which is what makes them usable as a route to the central circulation. [9]
From the indication to a confirmed, safe line
1 · Confirm indication and exclude contraindications
Decide arterial versus venous access, and rule out omphalitis, omphalocele, gastroschisis, and necrotising enterocolitis.
2 · Calculate the depth and choose the catheter
Apply the Shukla formula, select 3.5 French under 1500 grams or 5 French over 1500 grams, and prepare full sterile precautions.
3 · Cannulate the correct vessel to the calculated depth
Identify the artery or vein, dilate gently, advance to depth, aspirate and flush, and secure with a suture bridge.
4 · Confirm the tip on radiograph
Take an AP and lateral film; the arterial line sits high at T6 to T9 or low at L3 to L4, the venous line at the diaphragm T8 to T9, and reposition any malposition.
5 · Monitor and remove on time
Watch for limb blanching and sepsis, add heparin to the arterial infusion, and remove at five days for arterial or fourteen days for venous, or sooner if needed.
Classification
The two umbilical lines serve opposite purposes and travel opposite routes, and the distinction between them is the first thing an examiner will test. The umbilical venous catheter drains into the systemic venous circulation for the delivery of fluid, drugs, nutrition, and blood products, and for emergency venous access. Its tip belongs at the junction of the inferior vena cava and the right atrium, projected on radiograph at the diaphragm around the eighth to ninth thoracic vertebra. [3] [9]
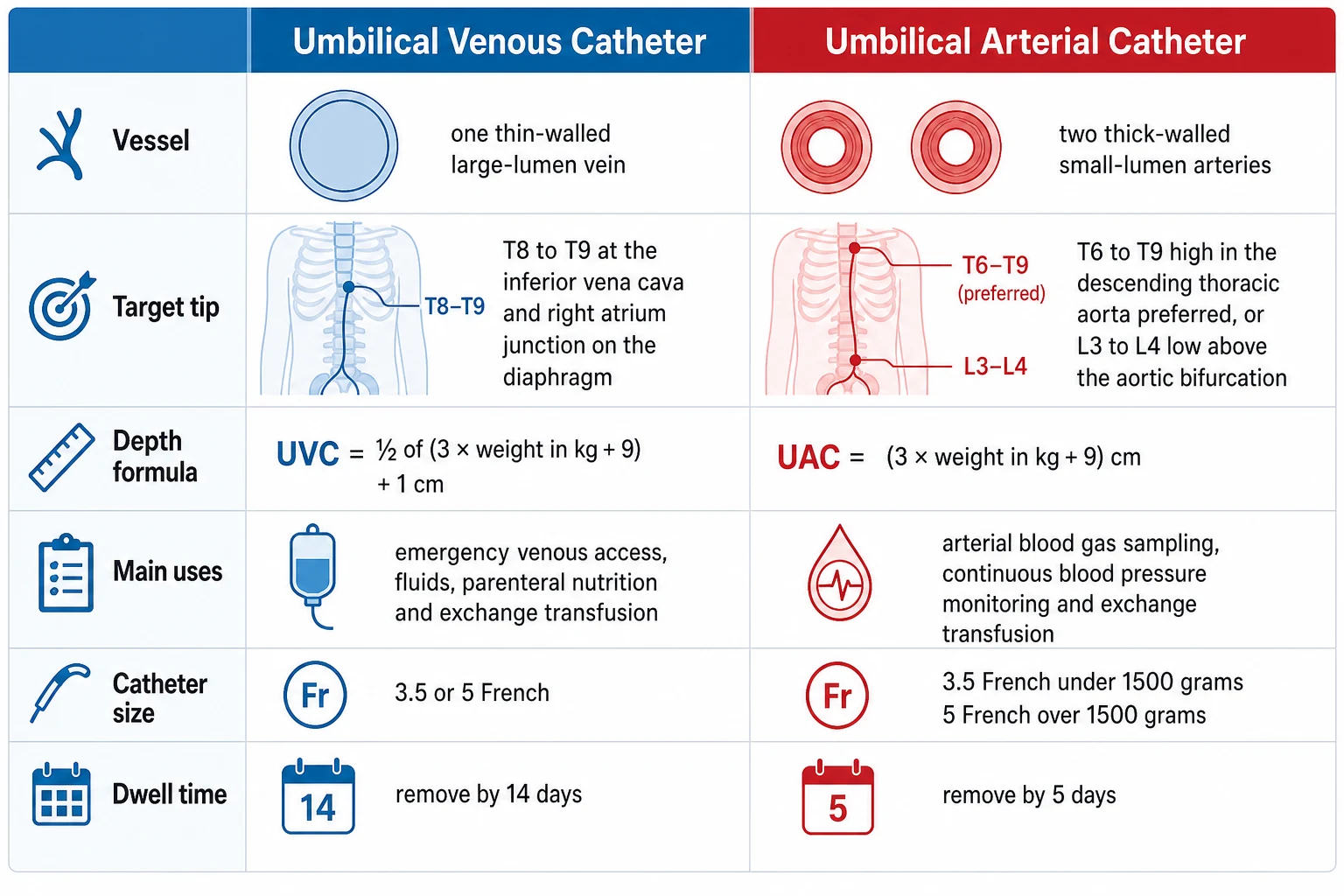
The umbilical arterial catheter reaches the systemic arterial circulation for the sampling of arterial blood gases, the continuous monitoring of blood pressure, and the conduct of an exchange transfusion. Its tip belongs in the descending aorta, where the high position between the sixth and ninth thoracic vertebrae is preferred because it sits above the origin of the celiac, superior mesenteric, and renal arteries, and the low position between the third and fourth lumbar vertebrae sits just above the aortic bifurcation at L4 and is used only when a high position is unattainable. [7] [9]
| Feature | Umbilical venous catheter | Umbilical arterial catheter |
|---|---|---|
| Vessel | One thin-walled large-lumen vein | Two thick-walled small-lumen arteries |
| Target tip | T8 to T9 at the diaphragm (IVC and right atrium junction) | T6 to T9 high (preferred) or L3 to L4 low |
| Shukla depth | Half of three times weight in kilograms plus nine, then plus one centimetre | Three times weight in kilograms plus nine centimetres |
| Main uses | Emergency venous access, fluids, parenteral nutrition, exchange transfusion | Arterial blood gases, continuous blood pressure, exchange transfusion |
| Catheter size | 3.5 or 5 French | 3.5 French under 1500 g, 5 French over 1500 g |
| Dwell limit | Remove by 14 days | Remove by 5 days |
Epidemiology & Risk Factors
Umbilical catheterisation is one of the commonest procedures in the neonatal intensive care unit, and its safety record is generally good when the lines are placed well and removed on time. A large level-four unit cohort found that around two and a half per cent of arterial catheters and thirteen per cent of venous catheters developed a complication, with malposition accounting for the great majority of venous-line events and line breakage or rupture for the majority of arterial-line events. [6]
The risk of a complication is driven above all by how long the line stays in. The cumulative incidence of trouble climbs most steeply after about ten days for an arterial catheter and sixteen days for a venous catheter, which is why dwell-time discipline — five days for arterial, fourteen days for venous — sits at the heart of safe practice. Smaller and sicker babies carry the extra risk of a thinner vessel wall and a harder course to negotiate, and any degree of sepsis, coagulopathy, or poor perfusion raises the stakes. [6] [10]
Well-placed high UAC
Low risk
- Tip T6 to T9, above visceral and renal arteries
- Lower vascular and thrombotic complication rate
- Accurate blood pressure and gas sampling
- Removed by day 5 once no longer needed
Low-sitting UAC
Higher ischaemic risk
- Tip L3 to L4, near the aortic bifurcation
- More lower-limb blanching and cyanosis
- Greater renal and mesenteric compromise
- Used only when high position unattainable
Malpositioned UVC
Commonest complication
- Tip in portal system, hepatic vein, or too far into the heart
- Risk of portal vein thrombosis and liver injury
- Arrhythmia or effusion if tip in the atrium
- Reposition before any use
Line left in too long
Dwell-time risk
- Complications rise after 10 days arterial, 16 days venous
- Thrombosis, malposition, and line sepsis
- Remove as soon as access no longer needed
- Plan definitive peripheral or central access early
Pathophysiology
The reason umbilical catheterisation works at all is that the fetal vessels stay open for a short window after birth, and the reason it can harm is that a foreign body sitting in a great vessel for days can obstruct, perforate, or seed infection. The umbilical venous catheter follows the path of fetal venous return: it enters the umbilical vein, passes through the left branch of the portal vein and the ductus venosus, and emerges in the inferior vena cava just beneath the right atrium. When the tip lands in the right place, infusate flows straight into the central venous circulation; when it lands too low in the portal system or the liver, infusate damages hepatic parenchyma and thrombosis of the portal vein may follow. [9]
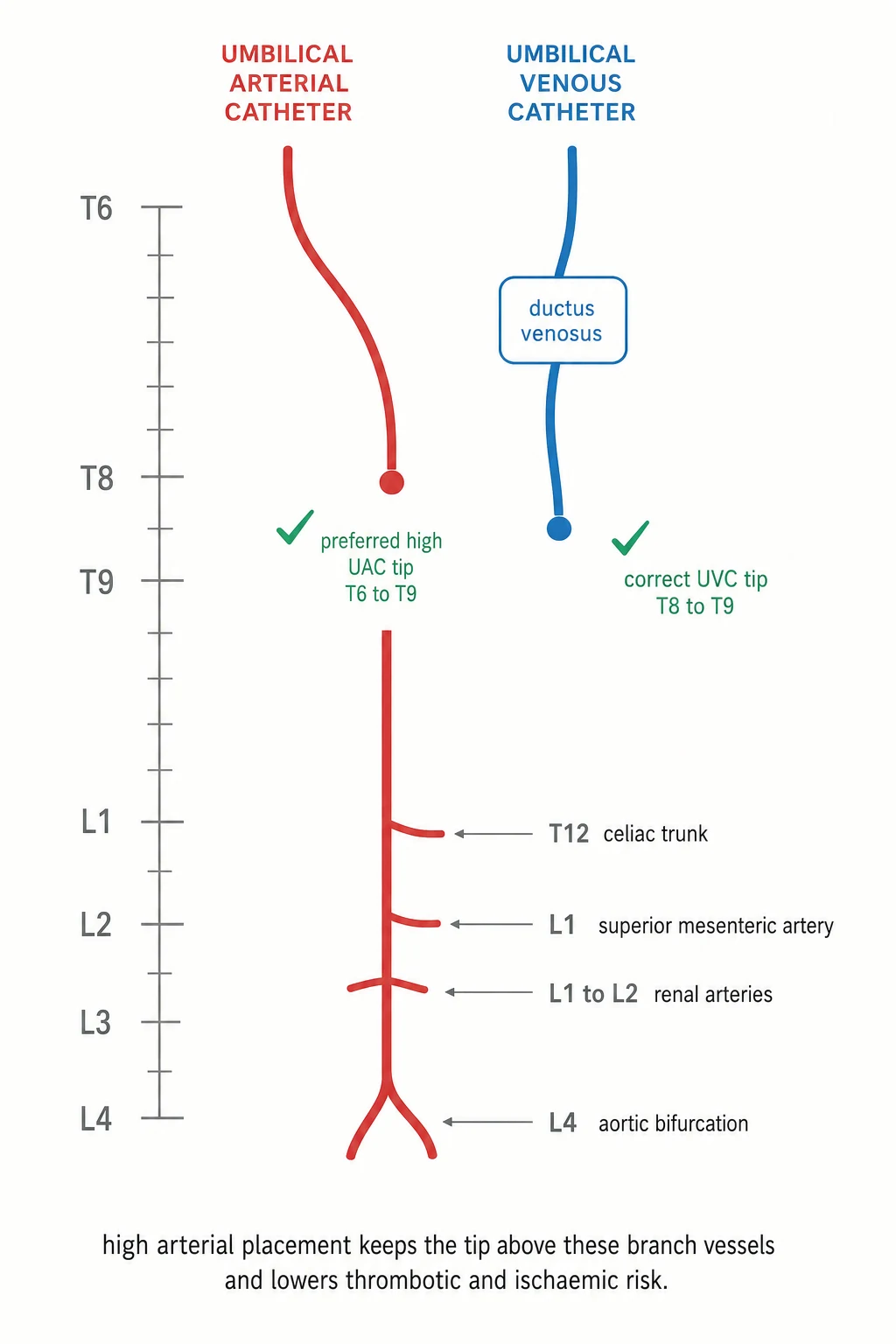
The umbilical arterial catheter retraces the fetal arterial route in reverse: it enters the umbilical artery, runs down the hypogastric and internal iliac arteries to the common iliac artery, and ascends the descending aorta to its tip. A high tip between the sixth and ninth thoracic vertebrae sits in a wide segment of aorta above the visceral and renal branches, where the catheter is bathed in fast flow and the risk of occluding a branch artery is low. A low tip between the third and fourth lumbar vertebrae sits in a narrower segment close to the aortic bifurcation, opposite the origins of the iliac arteries that feed the lower limbs and the kidneys, and it is here that vasospasm, thrombosis, and embolism do their damage. [7] [8]
Thrombosis is the unifying mechanism behind most of the serious harm. A clot that forms on the catheter or the vessel wall can occlude a branch artery — producing lower-limb ischaemia from iliac occlusion, hypertension from renal artery thrombosis, or necrotising enterocolitis from mesenteric compromise — or it can embolise distally. In the venous system, portal vein thrombosis may follow a malpositioned tip and lead in the longer term to portal hypertension, while a tip advanced into the right atrium or beyond can cause arrhythmia, perforation, or a pericardial effusion. Recognising that every complication traces back to position, dwell time, or sepsis is what keeps the lines safe. [6] [9]
Clinical Presentation
You meet umbilical catheterisation in three clinical moments. The first is the planned line in a sick neonate — a preterm infant on respiratory support who needs arterial blood-gas monitoring and a central line, where the umbilical route is the most reliable first access. The second is the emergency in the delivery room or resuscitation bay, where a collapsed newborn needs venous access now and the umbilical vein is the fastest central route available. The third is the line that has been in for days and is now causing trouble — a limb that has gone white, a baby that has become hypertensive, or a stump that has grown red — where the task is to recognise device-related harm and remove the line. [9] [10]
The signs that a line is harming the baby declare themselves along recognisable lines. A cold, white, or cyanosed lower limb points to arterial vasospasm or thromboembolism. Persistent hypertension points to renal artery thrombosis. Abdominal distension, bloody stools, or feed intolerance with a low arterial line point to mesenteric ischaemia and necrotising enterocolitis. A red, swollen, or discharging stump points to omphalitis or line sepsis. A sudden deterioration with a venous line that has migrated points to pericardial effusion or arrhythmia. Each sign carries its own time window and its own response, and the first response is almost always to stop using the line and reassess the position. [6] [9]
Differential Diagnosis
When a baby with an umbilical line deteriorates, the first task is to separate device-related harm from an unrelated deterioration, and then to name the specific mechanism. The differential turns on the line type, the tip position, and the dwell time, because each maps to a characteristic complication. [6] [9]
A lower limb that turns white after an arterial line is vasospasm or thromboembolism until proven otherwise, and the line comes out. Hypertension in a baby with an arterial line is renal artery thrombosis until proven otherwise, and the blood pressure is managed while the line is removed and the thrombosis is imaged. Abdominal signs with a low arterial line raise necrotising enterocolitis from mesenteric compromise, and a septic picture with any line raises catheter-related bloodstream infection. For a venous line that causes sudden collapse, pericardial effusion from a migrated tip is the emergency to exclude, because it is rare but rapidly fatal. Keeping this mapping in mind converts an undifferentiated deterioration into a directed response. [6] [10]
Clinical & Bedside Assessment
Bedside assessment begins before the line is inserted and continues every shift until it is removed. Before insertion, confirm the indication — venous access for fluids, nutrition, drugs, or resuscitation, or arterial access for monitoring and sampling — and exclude the absolute contraindications of omphalitis, an abdominal wall defect such as omphalocele or gastroschisis, necrotising enterocolitis, and peritonitis. Coagulopathy is a relative concern rather than an absolute bar, and a single umbilical artery, found in about one per cent of infants, is not itself a contraindication but prompts a check for associated renal and cardiac anomalies. [9] [10]
Then weigh the baby to calculate the insertion depth and choose the catheter size. The Shukla formula estimates the arterial catheter length as three times the birth weight in kilograms plus nine centimetres, and the venous catheter length as half of that value plus one centimetre. An infant under 1500 grams takes a 3.5 French arterial catheter and one over 1500 grams takes a 5 French catheter, while the venous catheter is usually 5 French, with a double-lumen line chosen when emergency resuscitation needs two lumens at once. Prepare a full sterile field, because the single biggest controllable driver of line sepsis is aseptic technique at insertion. [1] [5]
After insertion, assess the line at every encounter. Check the lower limbs for colour, warmth, and perfusion, because blanching or cyanosis is the earliest sign of arterial compromise and demands removal. Check the stump for redness, discharge, and breakdown. Review the radiograph for tip position against the landmarks, and review the indication daily, because the question of whether the line is still needed is the question that protects the baby from dwell-time harm. [6] [9]
Investigations
The only investigation that confirms catheter position is the radiograph, and it is mandatory before the line is used for anything but the briefest emergency access. A single anteroposterior film of the chest and abdomen maps the tip against the vertebral bodies, and a lateral film helps when the anteroposterior view leaves doubt. The arterial catheter tip should lie between the sixth and ninth thoracic vertebrae for a high line or the third and fourth lumbar vertebrae for a low line, and the venous catheter tip should lie at the diaphragm, projected at the eighth to ninth thoracic vertebra — above the ninth is too high and below the tenth is too low. [3] [9]
| Test | When it helps | What it tells you | Caveat |
|---|---|---|---|
| Chest and abdomen radiograph | After every insertion and after any migration | Tip position against the vertebral landmarks | Lateral view resolves doubt on an AP film |
| Point-of-care ultrasound or echocardiogram | When the venous tip is uncertain or suspected in the heart | Real-time tip location, and pericardial effusion if compromised | Reduces malposition and complications when used routinely |
| Blood pressure and limb perfusion | Every shift with an arterial line | Vasospasm, thrombosis, or renal compromise | A white limb means the line comes out now |
| Blood culture | With any septic picture or before elective removal | Catheter-related bloodstream infection | Paired peripheral and line cultures aid interpretation |
Bedside ultrasound and echocardiography have a growing role in confirming the venous catheter tip, and a randomised trial showed that echocardiographic determination of tip location lowered the rate of catheter-related complications. Ultrasound is especially useful when the radiograph leaves the venous tip uncertain or when a migrated line is suspected in the heart, and it can reveal a pericardial effusion at the bedside. The monitoring of the line itself — arterial waveform, blood-gas sampling, infusion patency — is part of nursing care, and the routine addition of low-dose heparin to the arterial infusion keeps the line patent and reduces clot formation. [10] [11]
UVC-UAC — the safe-line sequence
Management — Resuscitation
The resuscitation moment in this topic is the newborn who needs emergency vascular access in the delivery room or resuscitation bay. The umbilical venous catheter is the fastest central venous route in a newborn, and it is the line of choice for the administration of fluid, blood, resuscitation drugs, and adrenaline when peripheral access is impossible. The immediate actions are to prepare a sterile field, cut the cord, identify the thin-walled large-lumen vein, and advance a catheter far enough to enter the systemic circulation — often only four to five centimetres in a term baby for emergency use, with the definitive depth then calculated and confirmed once the baby is stabilised. [9] [10]
The second resuscitation moment is the line that has caused sudden harm. A baby who collapses with a venous line in situ may have a pericardial effusion from a tip migrated into the atrium, and the response is an immediate bedside ultrasound, pericardiocentesis if an effusion is confirmed, and removal of the line. A limb that turns white with an arterial line is vasospasm or thrombosis, and the response is to remove the line at once and arrange review of perfusion, with vasodilator or thrombolytic therapy guided by specialist input. In every resuscitation, the line is both the access that saves the baby and the device that may be harming it, so position and patency are checked before the line is trusted. [6] [11]
Management — Definitive & Stepwise
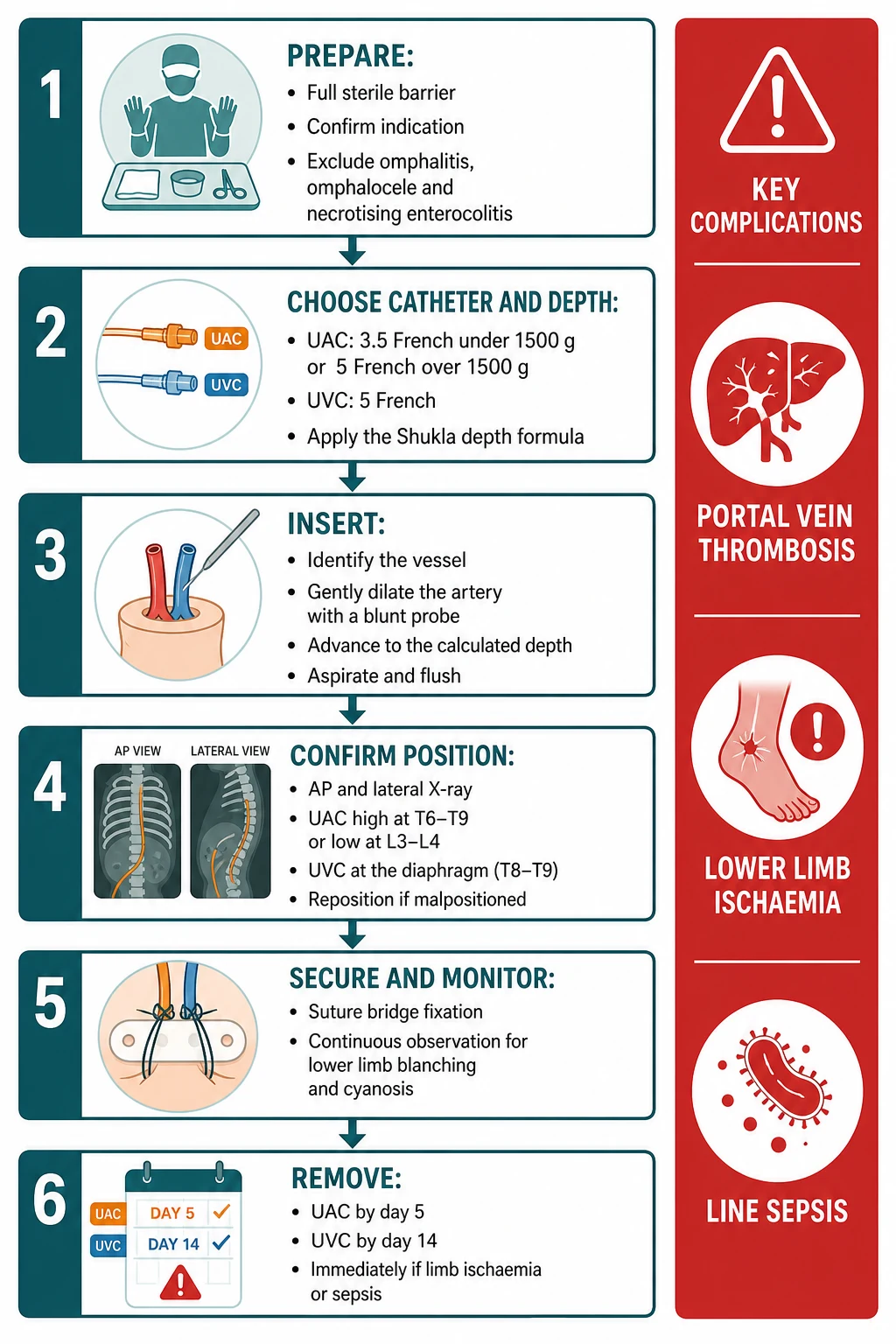
Preparation sets the safety of the whole procedure. A full sterile barrier is used — gown, gloves, mask, and a large drape — because catheter-related bloodstream infection is the complication that aseptic technique most directly prevents. The cord is cleaned with an aqueous or chlorhexidine-based antiseptic; tincture of iodine is avoided because of its effect on the neonatal thyroid, though povidone-iodine is acceptable and must be dried and removed afterwards. No topical antibiotic ointment is applied to the stump, because it promotes fungal colonisation and resistance. [10]
Choosing the catheter and the depth comes next. For an arterial line, a 3.5 French catheter is used under 1500 grams and a 5 French catheter over 1500 grams, with the insertion length calculated by the Shukla formula as three times the birth weight in kilograms plus nine centimetres. For a venous line, a 5 French single- or double-lumen catheter is usual, with the length calculated as half of the arterial value plus one centimetre. Body-measurement formulas and surface-anatomy methods — such as the umbilicus-to-nipple distance minus one centimetre for the venous line — can improve first-attempt accuracy, and the comparison of weight and body-measurement methods is the evidence base behind the choice. [1] [4]
Depth, sizing, and dwell values to verify against local neonatal guidelines
Insertion follows. The stump is cleaned and the vessels identified: the vein is the large, thin-walled oval opening, and the two arteries are the smaller, thick-walled round openings. The selected vessel is gently dilated — the artery often needs a blunt iris probe or fine forceps to overcome its natural spasm — and the catheter is advanced slowly to the calculated depth. Gentle aspiration confirms blood return, the line is flushed with saline, and it is secured with a suture bridge and a clear dressing. The arterial catheter is connected to a pressurised flush and a transducer for waveform monitoring, and the venous catheter is connected to the infusion. [9] [10]
Confirming the position is the step that cannot be skipped. An anteroposterior radiograph of the chest and abdomen is taken, and the tip is read against the vertebral landmarks: the arterial line at T6 to T9 for a high position or L3 to L4 for a low, the venous line at the diaphragm around T8 to T9. A line that is too high, too low, or coiled is repositioned before any use, because a malpositioned line is the commonest complication and the source of most of the serious harm. When the radiograph is uncertain, ultrasound or echocardiography resolves the tip. [3] [11]
Securing, monitoring, and removing close the pathway. The line is secured to prevent migration, the lower limbs and stump are checked every shift, and the indication is reviewed daily. Low-dose heparin is added to the arterial infusion to keep it patent. The line is removed the moment it is no longer needed, and no later than five days for an arterial catheter and fourteen days for a venous catheter, because dwell time is the biggest driver of thrombosis, malposition, and sepsis. When a line is removed, gentle pressure is held at the stump, and a definitive peripheral or central access has already been planned. [6] [10]
Specific Subtypes & Scenarios
The very preterm infant is the patient for whom the line matters most and in whom the calculation is hardest. A 700-gram baby has a short, fragile course and a vessel wall that tears easily, and the standard weight formulas carry a small but real error at the lowest weights. Body-measurement and surface-anatomy methods improve first-attempt placement in very low birth weight infants, and a planned, gentle technique with ultrasound backup reduces the number of manipulations. The arterial line in this baby is often the only reliable way to monitor blood pressure and gases in the first days, so getting the position right first time protects both the access and the baby. [4] [12]
A typical neonatal line journey
The term infant needing exchange transfusion uses both lines at once. Severe haemolytic disease of the newborn, or a dangerously high bilirubin unresponsive to phototherapy, is managed by an isovolumetric exchange through a venous and an arterial line — or two venous lines — so that blood is removed and replaced in equal volumes. The umbilical vessels are the standard route, the lines are placed under sterile conditions with confirmed positions, and the exchange is conducted with meticulous volume accounting. Once the exchange is complete, the lines are removed unless another indication persists. [9]
The infant with a complication already present is the patient where recognition drives the response. A white limb means the arterial line comes out now, and the limb is rewarmed and reviewed, with vasodilator or thrombolytic therapy guided by the specialist team. Persistent hypertension after an arterial line points to renal artery thrombosis, managed with antihypertensives and removal of the line, with imaging of the renal vasculature. A septic picture with a line in situ demands blood cultures, antibiotic therapy, and removal of the line, because a catheter-related bloodstream infection will not clear while the device remains. [6] [10]
Complications & Pitfalls
The complications of umbilical catheterisation fall into three families — malposition, thrombosis and ischaemia, and infection — and each has a signature. Malposition is the commonest, accounting for the great majority of venous-line complications in cohort studies: a venous tip in the portal system or the liver causes portal vein thrombosis and hepatic injury, a venous tip in the right atrium causes arrhythmia and effusion, and an arterial tip in a low or branch position causes ischaemia. Thrombosis and ischaemia show as a white limb, hypertension, or necrotising enterocolitis, and infection shows as catheter-related bloodstream infection, with the risk rising with dwell time. [6] [9]
Four pitfalls recur at the bedside. The first is the low arterial line left in place: a catheter at L3 to L4 carries more ischaemic risk than one high at T6 to T9, and it should not be accepted when a high position is achievable. The second is the unconfirmed or uncorrected venous malposition: a venous line used before the radiograph is checked, or left in the portal system, is the route to portal vein thrombosis and liver injury. The third is the ignored white limb: blanching or cyanosis after an arterial line is vasospasm or thrombosis, and waiting is the wrong response. The fourth is the line left in too long: dwell time beyond five days for arterial or fourteen days for venous lines is the single biggest preventable driver of complications. [6] [7]
Two lines
- UVC — umbilical vein to IVC; tip at T8 to T9 at the diaphragm
- UAC — umbilical artery to descending aorta; tip high T6 to T9 preferred, low L3 to L4
Depth formula (Shukla)
- UAC length = 3 × weight(kg) + 9 cm
- UVC length = half of UAC value + 1 cm
- Body-measurement and surface-anatomy methods improve first-attempt accuracy
Sizing and dwell
- UAC 3.5 Fr under 1500 g, 5 Fr over 1500 g; UVC usually 5 Fr
- Remove UAC by 5 days, UVC by 14 days, or sooner if not needed
- Low-dose heparin in the UAC infusion
Confirm before use
- AP chest and abdomen radiograph (lateral if unsure)
- Reposition any malposition; ultrasound or echo when uncertain
Contraindications
- Omphalitis, omphalocele or gastroschisis, necrotising enterocolitis, peritonitis
- Coagulopathy is relative; a single umbilical artery is not a bar
Complications
- UVC: malposition (commonest), portal vein thrombosis, line sepsis
- UAC: lower-limb ischaemia, renal artery thrombosis and hypertension, NEC
- A white limb — remove the line now
“Confirm indication and exclude contraindications → calculate depth with Shukla and choose the right French size → cannulate the correct vessel under full sterile precautions → confirm the tip on radiograph (UAC high T6–T9, UVC T8–T9) and reposition any malposition → secure, watch the limbs every shift, and remove by 5 days arterial or 14 days venous.”
Prognosis & Disposition
The prognosis for a newborn with a well-placed and well-managed umbilical line is excellent, because the lines deliver reliable access and monitoring through the most fragile days of life and are designed to come out. The complications that do occur are largely preventable through position confirmation, dwell-time discipline, and aseptic technique, and the great majority resolve without sequel once the line is removed and the underlying problem is addressed. The exceptions that leave lasting harm are a portal vein thrombosis that progresses to portal hypertension, a renal artery thrombosis that leaves chronic hypertension or renal injury, and a limb that was ischaemic for too long. [6] [9]
Disposition is shared between the proceduralist, the bedside nursing team, and the wider neonatal service. The proceduralist inserts and confirms the line, the nursing team monitors the limbs, the stump, and the waveform every shift, and the medical team reviews the indication daily and plans the next access. A line that is removed for a complication is followed by a focused workup of the complication — an ultrasound for a thrombosis, cultures for an infection, a surgical review for necrotising enterocolitis — and by early planning of definitive peripheral or central access so that the baby is never left without a reliable route. [10]
Special Populations
The very low birth weight infant is the patient in whom the lines are most needed and most fragile, and in whom the calculation of depth carries the greatest error. Body-measurement and surface-anatomy formulas improve first-attempt placement in these smallest babies, and a gentle, planned technique with ultrasound backup reduces the manipulations that injure the vessel wall. The single most important habit in this group is to plan definitive peripheral or central access early, so the umbilical line comes out on time rather than staying in by default. [4] [12]
The infant with an abdominal wall defect or NEC is the patient in whom umbilical access is contraindicated. Omphalocele and gastroschisis distort the umbilicus and the vessel course, active omphalitis seeds infection directly into the central circulation, and necrotising enterocolitis with mesenteric compromise is worsened by an arterial line. In these babies, alternative access — a peripheral cannula, a peripherally inserted central catheter, or an intraosseous needle in an emergency — is chosen from the outset. [9] [10]
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne clinical practice guideline and the local neonatal retrieval and tertiary-unit protocols set the insertion, confirmation, and dwell-time standards. The arterial line is placed high at T6 to T9 by default, the venous tip is confirmed at the diaphragm, and lines are removed at five days for arterial and fourteen days for venous access. Retrieval services rely on the umbilical route for the sick neonate in transit, with aseptic technique and radiographic confirmation at the receiving unit. [9] [10]
Global and low-resource settings: where imaging and specialist access are limited, the umbilical route remains a life-saving means of central access in the newborn, and the same principles hold — calculate the depth, cannulate the correct vessel under aseptic conditions, confirm the tip when any imaging is available, and remove the line on time. Discipline about dwell time, limb checks, and stump hygiene substitutes for technology when technology is unavailable, and early planning of definitive access protects the baby through the days ahead. [1] [9]
Evidence, Guidelines & Regional Differences
The evidence base for umbilical catheterisation rests on four pillars. The first is the depth-prediction literature, anchored by the Shukla and Ferrara birth-weight formula, whose arterial equation of three times weight in kilograms plus nine and venous equation of half that value plus one became the working standard worldwide. The subsequent comparison of weight and body-measurement methods, the revised venous formula that lowers the over-insertion rate, the surface-anatomy method that improves first-attempt accuracy, and the formula-tuning for very low birth weight infants have refined the original, but the Shukla formula remains the examination answer and the bedside starting point. [1] [3] [5]
The second pillar is the position evidence. The Cochrane review of high versus low arterial catheter position concluded that there is no evidence to support a low position and that high catheters should be used, because the high position carries a lower incidence of vascular complications without any rise in death, intraventricular haemorrhage, or necrotising enterocolitis — a conclusion reinforced by the randomised trial of high versus low position that found longer functional use and less lower-limb compromise with a high line. The radiographic landmark literature fixes the arterial tip at T6 to T9 high or L3 to L4 low and the venous tip at the diaphragm at T8 to T9. [7] [8] [9]
The third pillar is the complication and dwell-time evidence. The level-four cohort found complications in around two and a half per cent of arterial and thirteen per cent of venous catheters, with malposition dominating the venous events and the cumulative incidence climbing most steeply after ten days for arterial and sixteen days for venous lines, which underpins the dwell limits. The fourth pillar is the technology and guideline layer: the echocardiographic tip-localisation trial that lowered complications, the European position paper on neonatal vascular access that standardises aseptic technique, ultrasound use, securement, and surveillance, and the CDC infection-prevention recommendations that govern insertion and removal. [6] [10] [11]
The evidence is weaker where it rests on consensus rather than trials — the exact dwell-time thresholds, the choice between single and double-lumen venous catheters, and the role of routine ultrasound are handbook- and unit-defined. Where the evidence is consensus-derived, state the principle, cite the guideline, and communicate the value as one to verify against the current local neonatal protocol. [9] [10]
Board and assessment distinctions
RACP current PREP curriculum candidates must perform neonatal procedures safely, recognise device-related complications, and manage the acutely ill infant within the neonatal and patient-safety learning objectives. RCPCH Progress+ embeds procedural safety and device-related harm as a core patient-safety outcome. The ABP General Pediatrics Content Outline covers neonatal vascular access and procedural skills. Candidates are examined on the two lines, the two target positions, the Shukla formula, the dwell limits, and the recognition of complications.
[1] [9]| Board or format | What the candidate must demonstrate |
|---|---|
| RACP DWE | Identify the correct line, target position, and Shukla depth formula in a neonatal vignette |
| RACP DCE short case | Recognise a complication — a white limb, hypertension, or line sepsis — and state the immediate management |
| MRCPCH clinical | Explain the indications, contraindications, and dwell-time limits to a family and the team |
| ABP | Apply the formula, sizing, and radiographic landmarks under the neonatology domain |
| RCPSC structured oral | Defend the high arterial position and the dwell-time limits, and the management of portal vein thrombosis |
Exam Pearls
Viva: how do you calculate the insertion depth of an umbilical catheter, and where should each tip lie?
The Shukla and Ferrara birth-weight formula estimates both depths. The umbilical arterial catheter length is three times the birth weight in kilograms plus nine centimetres, which targets a high tip between the sixth and ninth thoracic vertebrae — the preferred position, because it sits above the visceral and renal arteries and carries fewer ischaemic and thrombotic complications. The umbilical venous catheter length is half of the arterial value plus one centimetre, which targets the tip at the inferior vena cava and right atrium junction at the diaphragm, around the eighth to ninth thoracic vertebra. A chest and abdomen radiograph confirms the tip before the line is used, and any malposition is repositioned. The low arterial position at the third to fourth lumbar vertebra is used only when a high position is unattainable. [1] [7]
Structured oral: a baby's leg goes white after an arterial line is inserted — what is happening and what do you do?
A white, cold, or cyanosed lower limb after umbilical arterial catheter insertion is arterial vasospasm or thromboembolism until proven otherwise, and the line is removed immediately. The mechanism is compromise of the iliac arterial supply by a low-sitting tip, a thrombus, or an embolus. The limb is rewarmed and the perfusion reassessed, and specialist input guides vasodilator or thrombolytic therapy if the ischaemia does not resolve. The catheter tip and any thrombus are imaged, the blood pressure is monitored for renal artery involvement, and a definitive plan for alternative access is made. The same principle governs every arterial-line assessment: check the limbs every shift, and act on blanching or cyanosis without delay. [6] [8]
References
- [1]Shukla H; Ferrara A Rapid estimation of insertional length of umbilical catheters in newborns American journal of diseases of children (1960), 1986.PMID 3728405
- [2]Lean WL; Dawson JA; Davis PG; Theda C; et al Accuracy of 11 formulae to guide umbilical arterial catheter tip placement in newborn infants Archives of disease in childhood. Fetal and neonatal edition, 2018.PMID 28818852
- [3]Verheij GH; te Pas AB; Smits-Wintjens VE; Sramek A; et al Revised formula to determine the insertion length of umbilical vein catheters European journal of pediatrics, 2013.PMID 23503982
- [4]Gupta AO; Peesay MR; Ramasethu J Simple measurements to place umbilical catheters using surface anatomy Journal of perinatology, 2015.PMID 25611793
- [5]Kieran EA; Laffan EE; O'Donnell CP Estimating umbilical catheter insertion depth in newborns using weight or body measurement: a randomised trial Archives of disease in childhood. Fetal and neonatal edition, 2016.PMID 26265678
- [6]Levit OL; Shabanova V; Bizzarro MJ Umbilical catheter-associated complications in a level IV neonatal intensive care unit Journal of perinatology, 2020.PMID 31911645
- [7]Barrington KJ Umbilical artery catheters in the newborn: effects of position of the catheter tip The Cochrane database of systematic reviews, 2000.PMID 10796375
- [8]Kempley ST; Bennett S; Loftus BG; Cooper D; et al Randomized trial of umbilical arterial catheter position: clinical outcome Acta paediatrica (Oslo, Norway : 1992), 1993.PMID 8477163
- [9]Marshall M Radiographic assessment of umbilical venous and arterial catheter tip location Neonatal network, 2014.PMID 24985114
- [10]Barone G; Piersigilli F; Pittiruti M Vascular access in the newborn: a position paper of Neonatal European Vascular Access Teams (NEVAT) European journal of pediatrics, 2026.PMID 41524806
- [11]Lin YJ; Liu YC; Huang HC; et al Echocardiographic determination of umbilical catheter tip location mitigates complications: a randomised controlled trial Children (Basel, Switzerland), 2025.PMID 41300627
- [12]Wright IM; Owers M; Wagner M The umbilical arterial catheter: a formula for improved positioning in the very low birth weight infant Pediatric critical care medicine, 2008.PMID 18679150