Paeds · mental-behavioural-and-psychosomatic
Anxiety disorders in children and adolescents
Also known as Childhood anxiety · Paediatric anxiety disorder · Separation anxiety disorder · Social anxiety disorder in youth · Generalised anxiety disorder in children · Selective mutism · Paediatric panic disorder
Fellowship guide to anxiety disorders in children and adolescents: distinguish the seven DSM-5-TR disorders from normal developmental fear, assess multi-informant with SCARED/SCAS/RCADS, exclude medical mimics and comorbid depression, deliver stepped care from psychoeducation through exposure-based CBT (Coping Cat, FRIENDS) to SSRI (sertraline, fluoxetine), anchored by CAMS, Cochrane 2020 and AACAP Walter 2020 evidence, with activation and suicidality monitoring and adapted care for neurodiverse, Indigenous, refugee and rural youth.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
D.R.E.A.M. — what makes fear a disorder
Overview & Definition
A worried child is not, by itself, a diagnosis. Fear is a normal, healthy alarm: it keeps a toddler close to a caregiver, makes a teenager rehearse before an exam, and warns of real danger. Anxiety crosses into a disorder when that alarm fires too often, too loudly, for too long, and starts to shrink the child's world. The threshold examiners want is impairment plus persistence plus developmental excess. [2] [5]
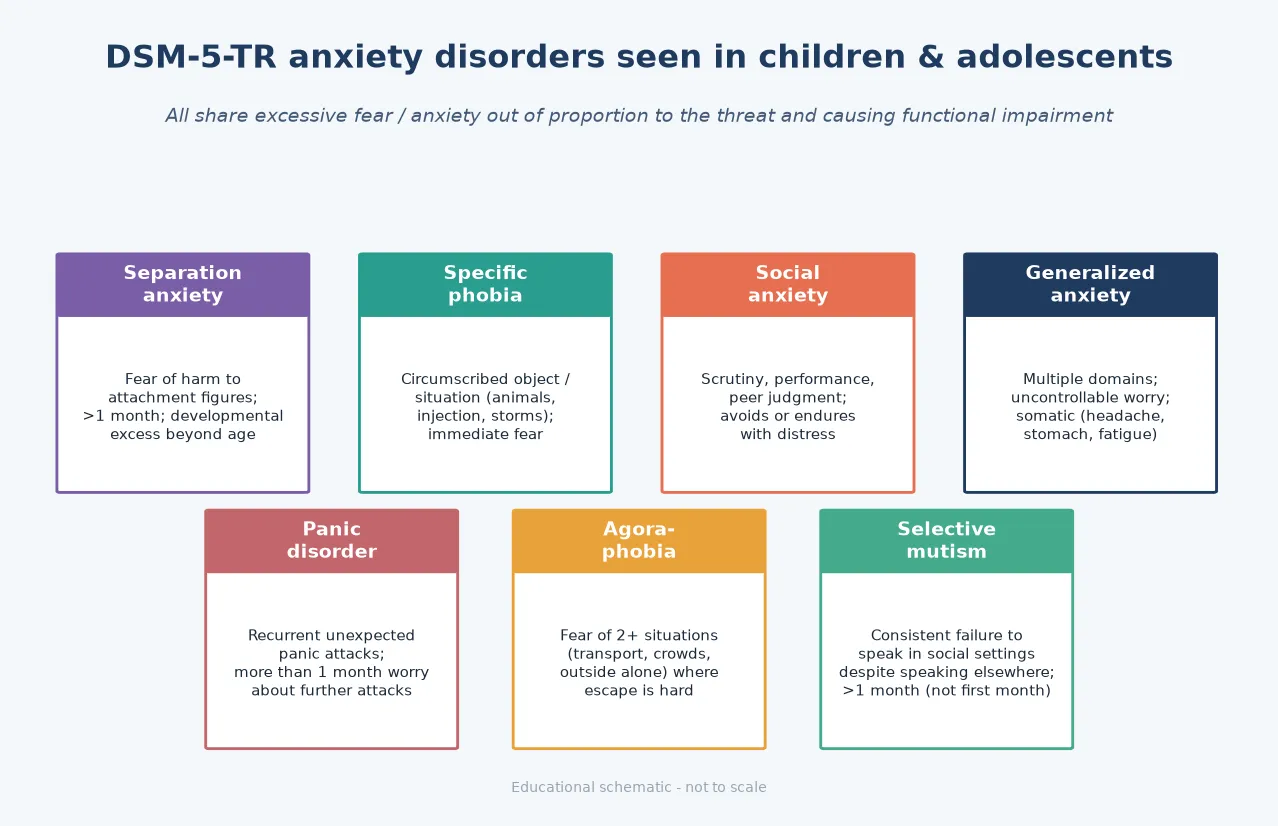
Across the DSM-5-TR anxiety disorders, the shared mechanism is a fear or anxiety response that is out of proportion to the actual danger, lasts beyond a normal developmental window, and causes clinically significant distress or functional impairment. The disorders differ mainly in what the threat is — separation from an attachment figure, a specific object, social scrutiny, the unpredictability of everyday life, or the body's own sensations. [2]
Your role as a general paediatrician is not to deliver a definitive psychiatric label on the first visit. It is to recognise the anxiety, quantify the impairment, exclude medical and safeguarding danger, stratify suicide risk, and start evidence-based stepped care — psychoeducation and CBT first, escalating to an SSRI when severity demands. [2] [10]
Classification
Seven DSM-5-TR anxiety disorders turn up regularly in paediatric practice. They share the same engine but differ in their trigger, their duration threshold, and the age at which they typically declare themselves. [2] [5]
The seven disorders, with the discriminator an examiner rewards
Separation anxiety
- Fear of harm to attachment figures; refusal to sleep or go to school alone
- Duration at least 4 weeks (DSM-5)
- No longer an early-childhood-only diagnosis — persists into adolescence
- Peak onset 7-9 years but can start later
Specific phobia
- Circumscribed object or situation (animals, blood-injection-injury, storms)
- Immediate, intense fear on exposure
- Duration at least 6 months
- Most prevalent single anxiety disorder in youth
Social anxiety
- Fear of scrutiny, performance, peer judgment
- In children must occur with peers, not only adults
- Duration at least 6 months
- Peak onset early adolescence
Generalised anxiety
- Uncontrollable worry across multiple domains
- Somatic: headache, stomach ache, fatigue, muscle tension
- Duration at least 6 months
- Children need only one associated symptom (adults need three)
Panic disorder
- Recurrent unexpected panic attacks
- At least 1 month of worry about further attacks
- Rare before puberty
- First exclude SVT, asthma, thyrotoxicosis
Agoraphobia
- Fear of two or more of five situations (transport, open, enclosed, crowds, outside alone)
- Duration at least 6 months
- Often follows panic disorder, can occur alone
Selective mutism
- Consistent failure to speak in social settings despite speaking elsewhere
- At least 1 month, not limited to first month of school
- Onset before 5 years, often missed until school entry
- Strongly associated with social anxiety
The most useful separation in a viva is disorder versus normal developmental fear. Stranger anxiety at 7 to 9 months, separation distress peaking at 12 to 18 months, fear of the dark and of animals in the preschool years, and performance nerves in adolescence are all expected. They become disorders only when they persist beyond the developmental window, cause real impairment, and exceed what is normal for the child's age. [2] [5]
Epidemiology & Risk Factors
Anxiety disorders are the most common class of mental disorder in young people. The U.S. National Comorbidity Survey Adolescent Supplement (NCS-A) found a lifetime prevalence of any anxiety disorder of about 31.9% by late adolescence — roughly one in three teenagers. [10]
Exam-order framing
Risk clusters into three streams. Temperament: behavioural inhibition — the tendency to withdraw from novelty — is the best-replicated early predictor, identified by Kagan's work. Family: parental anxiety, modelling of avoidance, overprotection, and family accommodation (the well-intended rearranging of family life to prevent the child's distress) all maintain symptoms. Environment: bullying (including online), adverse life events, trauma, chronic medical illness, and the load of unrecognised neurodevelopmental conditions such as ASD, ADHD and learning disorders. [2] [5]
The clinical consequence is severe when anxiety is missed. Untreated it is chronic and relapsing, tracks into adult anxiety and depression, and raises substance-use risk — yet most affected children receive no treatment. [10]
Pathophysiology
The engine that turns a moment of fear into a chronic disorder is short-term relief. When a child avoids the thing they fear, the alarm drops fast. That rapid fall in distress is negative reinforcement: the brain learns that avoidance is the only thing standing between it and catastrophe. Over weeks, the fear generalises, the child's world shrinks, and self-efficacy collapses. [2] [5]
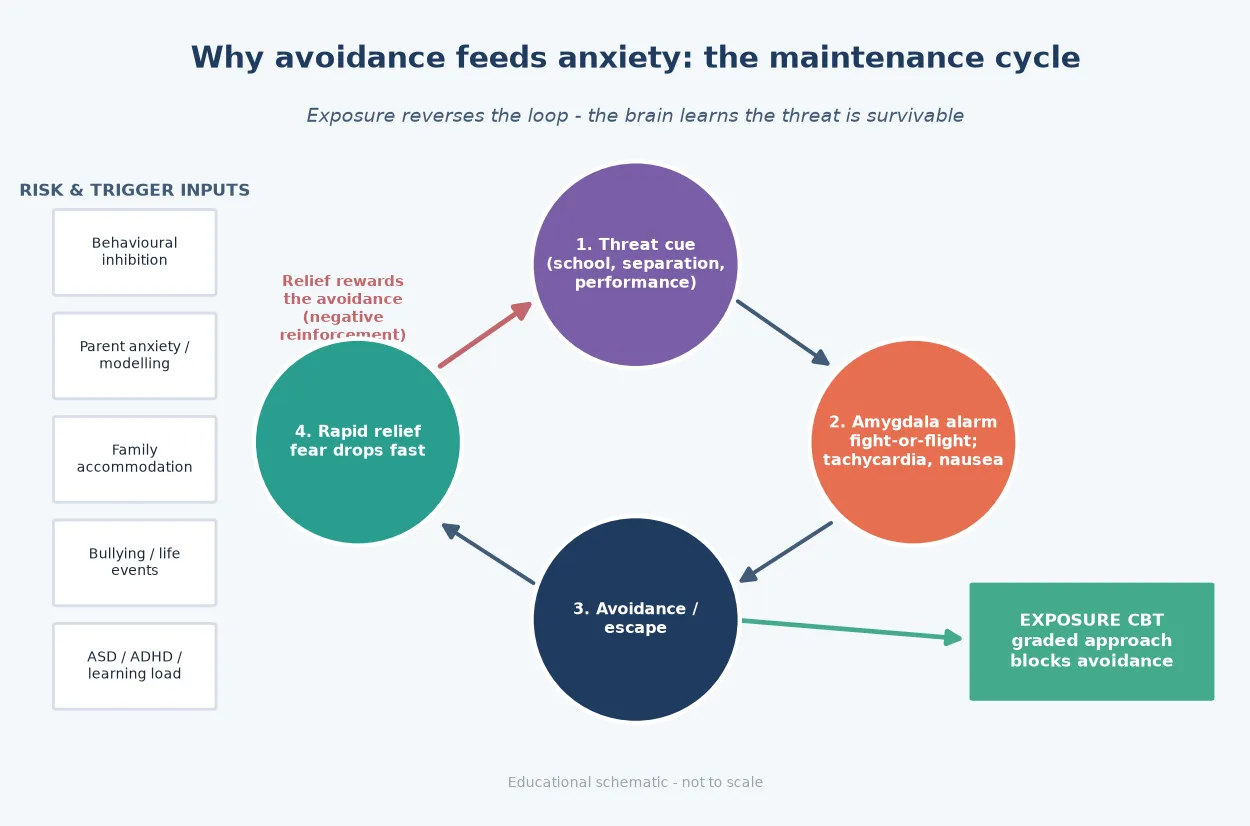
Avoidance is the problem because it blocks extinction learning. The brain never gets the chance to learn that the feared situation is survivable. Graded exposure works not by erasing the old fear memory but by building a new, competing safety memory — what clinicians call inhibitory learning. The fear circuit (amygdala, insula, anterior cingulate) calibrates to real threat, and the prefrontal cortex regains top-down control. [2]
Genetics and temperament load the gun. Heritability of anxiety is roughly 40 to 60%, and behavioural inhibition is a visible early marker. Parenting and environment pull the trigger: modelling, overprotection, accommodation, bullying and trauma all convert a vulnerability into a disorder. This is why treatment must address the maintaining factors, not just name the diagnosis. [2] [5]
Clinical Presentation
Anxiety in a child rarely walks in saying "I am anxious." More often it arrives as a stomach ache on a school morning, a meltdown at the school gate, a refusal to speak to the teacher, or a teenager who cannot get out of bed before an exam. Reading the somatic and behavioural signal correctly is the first clinical skill. [2] [5]
The preschool and early-primary child presents with separation distress, somatic complaints (abdominal pain, nausea, headache) that remit when separation is avoided, clinginess, sleep refusal, and — in selective mutism — consistent silence in one social setting while talking freely elsewhere. The school-age child shows school avoidance or refusal, specific and circumscribed fears, performance anxiety, reassurance-seeking, irritability, and sleep-onset delay. The adolescent may present with panic attacks, social and performance avoidance, pervasive worry and muscle tension (generalised anxiety), and functional impairment that parents attribute to "laziness" or "screens." [2]
Two atypical patterns trip clinicians. First, irritability and behavioural dysregulation can be the dominant presentation rather than verbalised fear — especially in younger children and in autistic youth, where alexithymia and communication differences mask the internal distress. Second, the somatic chief complaint (recurrent abdominal pain, recurrent headache, chest pain, palpitations) brings the child to a paediatric or emergency setting framed as physical illness. Both patterns demand the same multi-informant anxiety assessment. [2] [5]
Differential Diagnosis
The differential has three jobs: separate disorder from normal fear, separate anxiety from its psychiatric mimics, and exclude medical disease that masquerades as anxiety. Missing the medical column is the dangerous error. [2] [5]
| Differential | Discriminators | Why it matters |
|---|---|---|
| Normal developmental fear | Age-appropriate, transient, no impairment, resolves with reassurance | Over-diagnosis medicalises a healthy child |
| Major depression | Pervasive anhedonia, hopelessness, sleep/appetite change, suicide risk | Different treatment intensity and risk priority |
| ADHD | Inattention from worry vs primary attention deficit; lifelong cross-setting | Stimulant can worsen anxiety if misdiagnosed |
| ASD | Lifelong social-communication deficit, sensory load, routines | Adapt exposure; do not force "just try harder" |
| OCD | Obsessions and compulsions, not just worry | Different CBT (ERP) and SSRI dosing |
| PTSD | Trauma re-experiencing, avoidance, hyperarousal with clear trauma | Trauma-focused therapy first |
| Hyperthyroidism | Weight loss, heat intolerance, resting tachycardia, goitre | Check TSH before psychiatric framing |
| Arrhythmia / SVT mimicking panic | Exertional, sudden onset and offset, syncope, family sudden death | ECG; do not assume benign panic |
| Asthma / hypoglycaemia / substance | Episodic breathlessness, sweating, substance history | Targeted medical workup |
Clinical & Bedside Assessment
Assessment is multi-informant by design. Children under-report internalising symptoms because they lack the vocabulary and insight; parents and teachers see the avoidance and impairment the child minimises. Interview the young person alone and with caregivers, and gather school collateral. [2] [5]
Structure the history across five domains: the onset and course of the fear (when it started, what maintains it, the somatic pattern by day of week); the fear map (which situations trigger, which are avoided, the cost of the avoidance); impairment across school, peer and family function; risk (suicide, self-harm, abuse, bullying); and context (developmental and neurodevelopmental history, family psychiatric history, trauma, chronic illness). The developmental history is non-negotiable: ASD, ADHD, intellectual disability and learning disorders co-occur and reshape the plan. [2] [5]
Three validated scales anchor the assessment and track response. The SCARED (Screen for Child Anxiety Related Emotional Disorders, Birmaher 1997) is the most widely used multi-informant tool with child and parent versions and subscales mapping to the common disorders. The Spence Children's Anxiety Scale (Spence 1998) gives a dimensional profile across disorder domains. The RCADS (Revised Child Anxiety and Depression Scale, Chorpita 2000) screens anxiety and depression together — useful because the two are highly comorbid. Use them as adjuncts, not replacements for the clinical interview. [11] [12] [13]
A focused mental state examination looks at affect (often calm once the threat is "off the table," rising when it returns), thought content (catastrophic beliefs, intrusive thoughts, worry themes), perception, insight, and risk. Every anxious child or adolescent needs a structured suicide and self-harm risk assessment — anxiety carries its own suicide risk, and comorbid depression is common. Explain confidentiality limits and capacity principles, which are decision-specific and jurisdiction-specific. [2] [4]
Investigations
Anxiety disorders are clinical diagnoses. There is no blood test, scan, or biomarker that confirms one. The job of investigation is to exclude medical mimics selectively and to document comorbidity — not to reassure by exclusion. [2] [5]
Target a medical workup only when red flags are present: weight loss or growth failure, nocturnal or progressive symptoms, focal neurological signs, cardiovascular features (exertional chest pain, syncope, palpitations, family history of sudden death), or systemic features suggesting thyroid disease. In those cases, consider an ECG (to exclude arrhythmia and long QT before an SSRI), thyroid function, and other directed tests. No routine brain imaging for uncomplicated anxiety, and avoid serial investigations that delay treatment and medicalise avoidance. [2]
Document the comorbidities that change management: depression and suicidality, ADHD, ASD, learning disorder, OCD, and substance use. These determine whether CBT alone is enough or whether an SSRI, school liaison, or specialist referral is needed from the start. [2]
Management — Resuscitation
Stabilise risk first. An acute panic-like presentation needs medical exclusion of arrhythmia, asthma or hypoglycaemia when indicated, followed by rapid outpatient exposure-based care rather than chronic anxiolysis. Do not initiate chronic benzodiazepines for paediatric anxiety — dependence, cognitive effects and weak long-term evidence make them a poor fellowship answer. [2] [5]
Address safeguarding and medical red flags before a pure anxiety plan. If a short medical certificate is genuinely needed for acute unfitness, pair it with a written review date and a graded plan — indefinite certificates entrench avoidance and are a common iatrogenic pitfall. [2]
Management — Definitive & Stepwise
Core principles
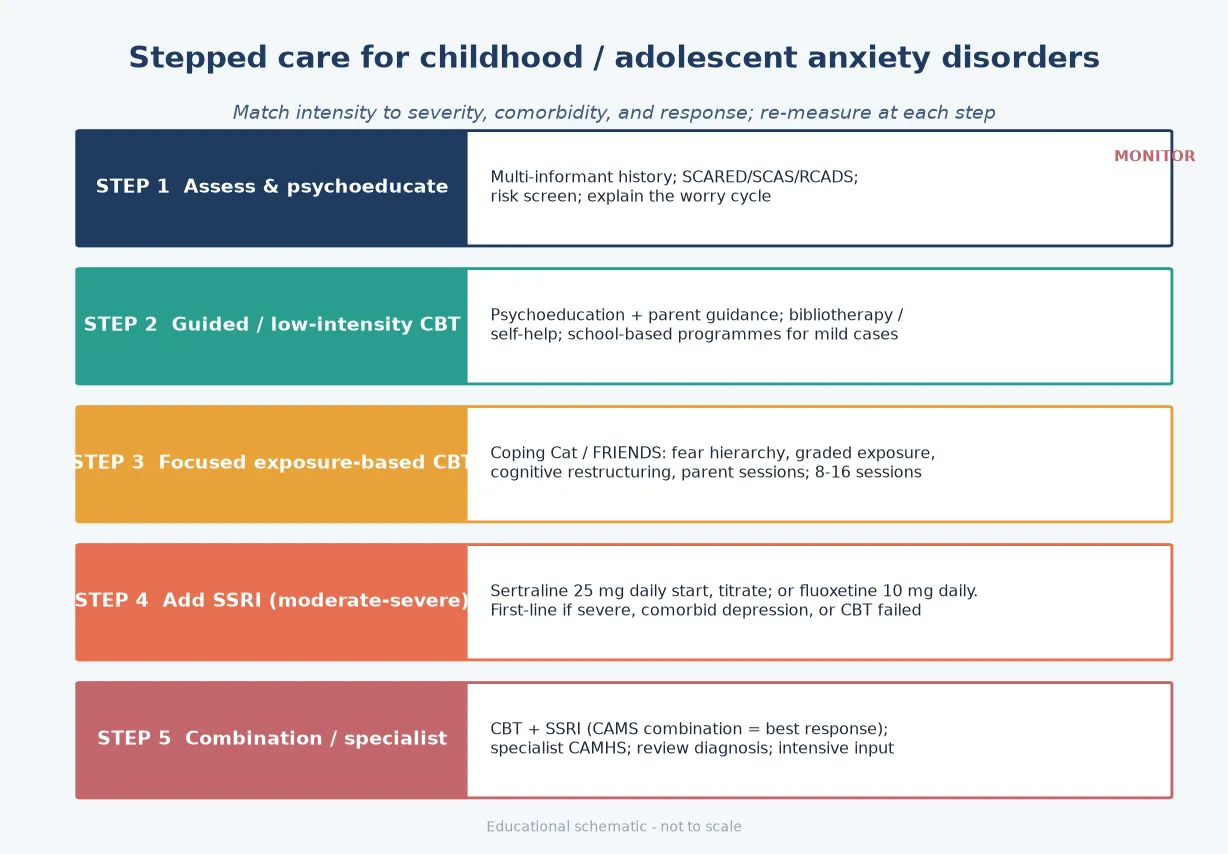
Treatment is stepped: start at the lowest intensity that fits the severity, escalate if response is inadequate, and re-measure with a validated scale at each step. The AACAP 2020 clinical practice guideline (Walter et al.) recommends CBT as first-line, with an SSRI added for inadequate response and combination therapy for severe or comorbid presentations. [2]
The five-step ladder
Step 1 — Assess and psychoeducate: multi-informant history, SCARED/SCAS/RCADS, risk screen; explain the worry cycle to family and young person
Step 2 — Guided or low-intensity CBT: psychoeducation plus parent guidance, bibliotherapy and self-help, school-based programmes for mild cases
Step 3 — Focused exposure-based CBT: Coping Cat or FRIENDS; fear hierarchy, graded exposure, cognitive restructuring, parent sessions; 8 to 16 sessions
Step 4 — Add an SSRI: sertraline 25 mg oral daily start, titrate; or fluoxetine 10 mg oral daily. First-line drug if severe, comorbid depression, or CBT failed
Step 5 — Combination and specialist: CBT plus SSRI (CAMS combination = best response); specialist CAMHS; review the diagnosis; intensive input for resistant cases
Psychological therapy
Exposure-based CBT is the first-line psychological treatment. The 2020 Cochrane review (James et al.) found CBT superior to no treatment or waitlist for childhood anxiety disorders, with a modest effect size; combination approaches and group formats add value. Manualised programs such as Coping Cat (Kendall) and FRIENDS (Barrett) structure the work around the core active ingredients. [3]
The active ingredients examiners want named are: psychoeducation; emotion identification; a fear hierarchy and graded in vivo exposure to the feared steps; cognitive restructuring of catastrophic beliefs; contingency management; parent sessions to reduce accommodation; and relapse prevention. Exposure is the ingredient that does the heavy lifting — it is what reverses the avoidance-reinforcement cycle. [2] [3]
The comparative-effectiveness meta-analysis by Wang et al. (JAMA Pediatrics 2017) found CBT and pharmacotherapy broadly comparable in effectiveness for childhood anxiety disorders, supporting either as a reasonable monotherapy with combination reserved for greater severity. [6]
Pharmacotherapy
An SSRI is indicated for moderate-severe anxiety, when CBT is inaccessible or has failed, when comorbid depression is present, or as combination therapy when impairment is high. It is not first-line for mild anxiety, and never a substitute for exposure. [1] [2]
| Evidence | Population / design | Exam takeaway |
|---|---|---|
| CAMS Walkup 2008 | Ages 7 to 17; separation, GAD, social anxiety; CBT vs sertraline vs combination vs placebo | Combination highest response (~80.7%); CBT (~60%) and sertraline (~55%) each beat placebo (~24%) |
| RUPP fluvoxamine 2001 | Children and adolescents with social, separation or generalised anxiety | Fluvoxamine superior to placebo; early SSRI class evidence |
| Birmaher fluoxetine 2003 | Childhood anxiety RCT | Fluoxetine efficacious versus placebo for separation, social and generalised anxiety |
| Strawn escitalopram 2020 | Adolescents with generalised anxiety disorder; double-blind placebo-controlled | Supports escitalopram for adolescent GAD |
Practical SSRI starts (when indicated). Start low, titrate slowly, and monitor. [1] [2]
Sertraline (first-line SSRI for paediatric anxiety)
Dose
Start 25 mg oral daily in children (some adolescents 25-50 mg); titrate gradually
Fluoxetine (alternative SSRI for paediatric anxiety)
Dose
Start 10 mg oral daily, often toward 20 mg as needed
Black-box / suicidality counselling. The Bridge et al. meta-analysis of paediatric antidepressant randomised trials (JAMA 2007) showed a small absolute increase in suicidal ideation and behaviour signals versus placebo alongside clinical response benefits. Discuss the risk-benefit, involve carers, and schedule early review. This applies to every youth antidepressant. [4]
Benzodiazepines are a poor answer for chronic paediatric anxiety maintenance because of dependence, cognitive effects and weak long-term evidence. Reserve them, if at all, for short-term acute crises under specialist guidance. [2] [5]
Family and multi-agency work
Train carers to limit excessive reassurance, support planned exposures, and hold consistent routines. Reduce family accommodation — the well-intended rearranging of family life around the child's avoidance — because it is a powerful maintaining factor. Coordinate GP, school and specialist mental health so messages do not conflict, and expand access through parent-led and school-based supports in stepped care for milder presentations. [2] [3]
Specific Subtypes & Scenarios
Separation anxiety. Parent coaching and graded separation exposure are central, with a school return plan. DSM-5 removed the age-of-onset cap, so the diagnosis is legitimate in adolescents — a common viva point. [2]
Social anxiety. Exposure to evaluative situations, role-play, and graded social tasks; consider an SSRI if impairment is severe. In children, the fear must occur with peers, not only with adults. [2]
Generalised anxiety. Worry-focused CBT, problem-solving training, and relaxation as an adjunct. Sertraline and escitalopram carry RCT support; the Strawn 2020 trial supports escitalopram in adolescent GAD. [2] [9]
Selective mutism. Behavioural treatment — stimulus fading, shaping and positive reinforcement — is first-line, with early intervention before the pattern consolidates. A 2018 systematic review found CBT, pharmacotherapy and combination all show benefit, but evidence quality is limited; an SSRI adjunct is reserved for resistant, impairing cases. [14]
Panic disorder (rare before puberty). Psychoeducation about the body's alarm system, interoceptive exposure to feared sensations, and CBT. Exclude SVT, thyrotoxicosis and substance causes first, and avoid chronic benzodiazepines. [2] [5]
Complications & Pitfalls
Failing viva answers: missing comorbid depression and suicide risk; medicalising somatic complaints with serial investigations and certificates; chronic benzodiazepines; starting an SSRI without an exposure plan or monitoring; leaving parental accommodation unaddressed; and under-treating on the assumption that anxiety is "just worry." Anxiety is chronic and relapsing if untreated — families often wait years before seeking help, and the cost is academic, social and developmental. [2] [4] [10]
Prognosis & Disposition
Anxiety disorders improve substantially with adequate treatment but are chronic and relapsing without it. The CAMS trial showed combination CBT plus sertraline achieved the best acute response, and substantial remission is achievable with adequate stepped care. Earlier, consistent intervention improves the long-term trajectory; untreated childhood anxiety tracks into adult anxiety, depression and substance use. [1] [2] [10]
Disposition follows stepped care: mild presentations in primary care with guided self-help; moderate in specialist CBT; severe, treatment-resistant or complexly comorbid in specialist CAMHS. Monitor for relapse at transitions and stressors, and safety-net for emerging depression or suicide risk at every review. [2]
Special Populations
Neurodiverse youth (ASD, ADHD, intellectual disability) need adapted exposure hierarchies, sensory and communication-load management, and visual supports — exposure is still needed for phobic avoidance, but the social-communication load must be respected. Aboriginal, Torres Strait Islander, Maori and Indigenous youth require cultural safety, community-based models, and awareness of intergenerational trauma. Refugee, asylum-seeker and migrant youth need trauma-informed care, interpreter use, and attention to acculturation stress. Rural and remote youth benefit from telehealth CBT and school-based programmes that close the access gap; gender and sexual minority youth carry minority stress that raises anxiety burden. Adapt the formulation and the delivery without abandoning the evidence-based principles. [2]
Evidence, Guidelines & Regional Differences
ANZ. General paediatric and CAMHS practice follows stepped care with exposure-based CBT, school liaison, and SSRI evidence (CAMS, fluoxetine) within public services, private specialists and education systems. Cite international trial evidence plus local consent, mandatory reporting and education-law frameworks. Do not invent foreign Mental Health Act section numbers — name the jurisdiction's own tools. [1] [2]
Named evidence stack for viva: CAMS (Walkup 2008); Cochrane CBT review (James 2020); AACAP guideline (Walter 2020); AACAP practice parameter (Connolly 2007); comparative-effectiveness meta-analysis (Wang 2017); fluoxetine (Birmaher 2003); fluvoxamine (RUPP 2001); escitalopram in adolescent GAD (Strawn 2020); suicidality meta-analysis (Bridge 2007); NCS-A prevalence (Merikangas 2010); SCARED (Birmaher 1997); SCAS (Spence 1998); RCADS (Chorpita 2000); selective mutism review (2018). [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14]
Exam Pearls
- Anxiety disorders are the most prevalent mental disorder class in youth — about one in three adolescents. [10]
- Separation anxiety duration is at least 4 weeks (DSM-5); it is no longer an early-childhood-only diagnosis. [2]
- CAMS combination response ~80% versus ~60% CBT and ~55% sertraline monotherapy — the landmark youth anxiety trial. [1]
- Sertraline 25 mg oral daily start; fluoxetine 10 mg oral daily start; counsel activation and suicidality with every youth SSRI. [1] [4]
- SCARED, SCAS and RCADS are the validated multi-informant scales; children under-report, so corroborate. [11] [12] [13]
- Avoid chronic benzodiazepines in paediatric anxiety; exposure-based CBT is first-line. [2] [3]
- Anxiety does not protect against suicide — assess risk every time. [2] [4]
References
- [1]Walkup JT, Albano AM, Piacentini J, Birmaher B, et al. Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. N Engl J Med, 2008.PMID 18974308
- [2]Walter HJ, Bukstein OG, Abright AR, Keable H, Ramtekkar U, et al. Clinical Practice Guideline for the Assessment and Treatment of Children and Adolescents With Anxiety Disorders. J Am Acad Child Adolesc Psychiatry, 2020.PMID 32439401
- [3]James AC, Reardon T, Soler A, James G, Creswell C. Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database Syst Rev, 2020.PMID 33196111
- [4]Bridge JA, Iyengar S, Salary CB, Barbe RP, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA, 2007.PMID 17440145
- [5]Connolly SD, Bernstein GA, Work Group on Quality Issues. Practice parameter for the assessment and treatment of children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry, 2007.PMID 17242630
- [6]Wang Z, Whiteside SPH, Sim L, Farah W, et al. Comparative Effectiveness and Safety of Cognitive Behavioral Therapy and Pharmacotherapy for Childhood Anxiety Disorders: A Systematic Review and Meta-analysis. JAMA Pediatr, 2017.PMID 28859190
- [7]Birmaher B, Axelson DA, Monk K, Kalas C, et al. Fluoxetine for the treatment of childhood anxiety disorders. J Am Acad Child Adolesc Psychiatry, 2003.PMID 12649628
- [8]The Research Unit on Pediatric Psychopharmacology Anxiety Study Group. Fluvoxamine for the treatment of anxiety disorders in children and adolescents. N Engl J Med, 2001.PMID 11323729
- [9]Strawn JR, Vinegar AP, Powell RA, Mills R, et al. Escitalopram in Adolescents With Generalized Anxiety Disorder: A Double-Blind, Randomized, Placebo-Controlled Study. J Clin Psychiatry, 2020.PMID 32857933
- [10]Merikangas KR, He JP, Burstein M, Swanson SA, et al. Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication--Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry, 2010.PMID 20855043
- [11]Birmaher B, Khetarpal S, Brent D, Cully M, et al. The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry, 1997.PMID 9100430
- [12]Spence SH. A measure of anxiety symptoms among children. Behav Res Ther, 1998.PMID 9648330
- [13]Chorpita BF, Yim L, Moffitt C, Umemoto LA, Francis SE. Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale. Behav Res Ther, 2000.PMID 10937431
- [14]Steinhausen HC, Juzi C, Jeker P, Seifert L, Winkler Metzke C. Treatment of selective mutism based on cognitive behavioural therapy, psychopharmacology and combination therapy - a systematic review. Nord J Psychiatry, 2018.PMID 29447060