Paeds · mental-behavioural-and-psychosomatic
Attachment disorders and relational trauma
Also known as Reactive attachment disorder · Disinhibited social engagement disorder · RAD and DSED · Relational trauma · Developmental trauma from pathogenic care
Fellowship guide to reactive attachment disorder (RAD) and disinhibited social engagement disorder (DSED) and the wider relational-trauma picture in children: the two-disorder DSM-5-TR and ICD-11 structure built on grossly pathogenic early care, the developmental and caregiving-history assessment, the BEIP, ABC and Child-Parent Psychotherapy evidence, phased relationship-based care with no first-line medication and no coercive holding therapy, and a closed safeguarding and disposition plan across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A foster carer brings a four-year-old, placed six weeks ago after neglect, who will not look at her, pushes her away when hurt, yet wanders off with any adult in the waiting room. The question is not "is he attached?" but "has grossly pathogenic care produced a disorder of social relatedness, and which one?" Most children in substitute care settle as their carer becomes reliable; the minority who do not are the ones your assessment must find. [1] [13]
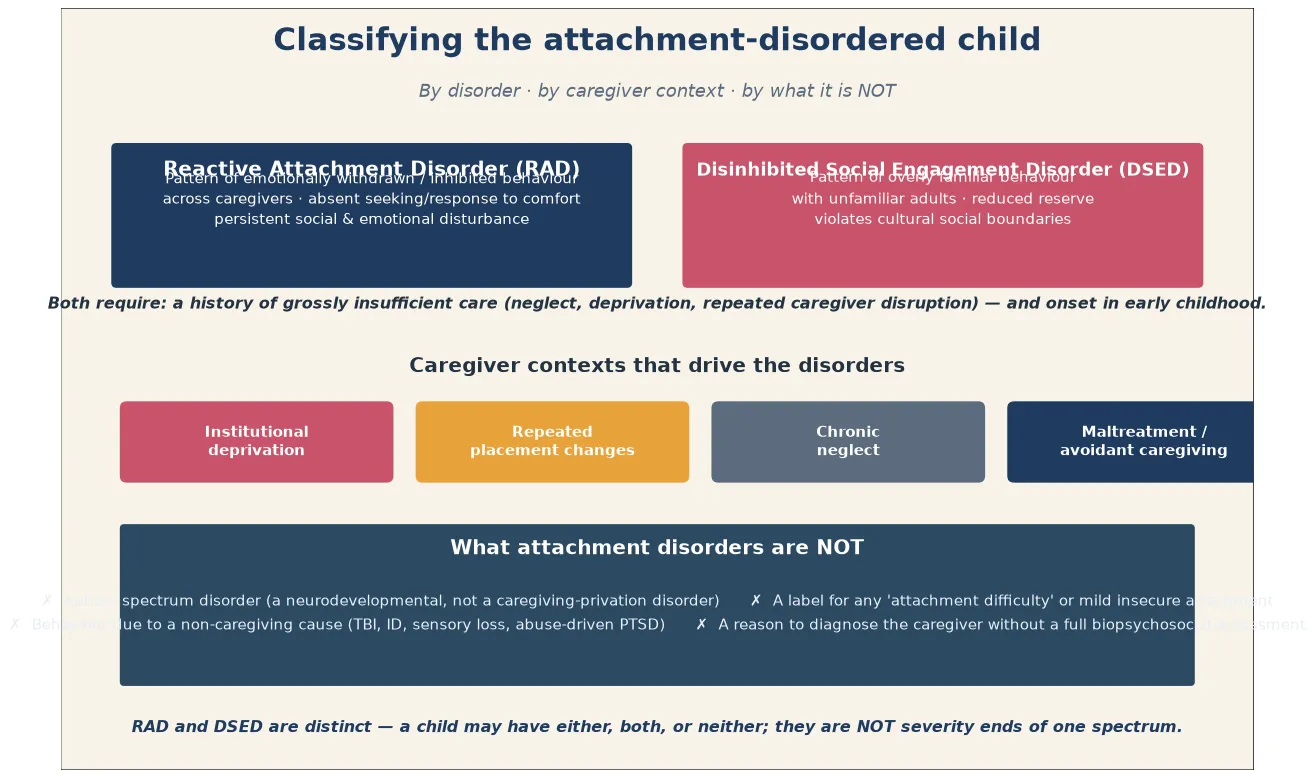
A reactive attachment disorder (RAD) is a pattern of emotionally withdrawn and inhibited behaviour toward adult caregivers: the child minimally seeks comfort when distressed and minimally responds to comfort when it is offered, with persistent social and emotional disturbance. A disinhibited social engagement disorder (DSED) is the mirror behavioural pattern — overly familiar, culturally inappropriate approach to unfamiliar adults, with reduced or absent social reserve. Both share one aetiological root: a history of grossly pathogenic care, through neglect, deprivation, or repeated disruption of the primary caregiver, that prevented a selective attachment from forming. [1] [2]
In children the picture is developmental and easy to misread. A preschooler with RAD looks withdrawn, vacant, or watchful rather than "shy." A child with DSED looks charmingly friendly, hugging strangers and wandering off with them, which families mistake for good adjustment. Because the behaviours overlap with autism, intellectual disability, and the wider relational-trauma picture, attachment disorders are over-diagnosed by those who skip the caregiving history and under-diagnosed by those who never ask about early care. [2] [3]
Deep technique for the single-incident trauma-response continuum lives on the PTSD leaf, autism recognition on the autism leaf, and acute self-harm risk on the suicide-and-self-harm leaf. This page owns the two attachment disorders and the relational-trauma spine that runs from recognition to closed-loop care. [13] [14]
Classification
Classify along three axes before you name a disorder: which behavioural pattern the child shows, what kind of caregiving drove it, and what it is not. The same odd social behaviour means something different with a healthy caregiving history than with a depriving one. [2] [13]
By disorder (DSM-5-TR and ICD-11)
| Pattern | Favours | Core behavioural features |
|---|---|---|
| Emotionally withdrawn / inhibited across caregivers | RAD | No comfort-seeking, no response to comfort, social & emotional disturbance |
| Indiscriminate / over-familiar with unfamiliar adults | DSED | Reduced reserve, verbal/physical familiarity, wanders off with strangers |
| Risk pattern, not a disorder | Insecure / disorganised attachment | Distress in the relationship, but no disorder threshold met |
| Neurodevelopmental, not caregiving-driven | Autism spectrum disorder | Social-communication impairment with restricted/repetitive behaviour |
By caregiver context
The caregiving contexts that produce these disorders cluster into four: institutional deprivation (the Romanian orphanage and modern equivalents), repeated placement changes that prevent any one carer from becoming a secure base, chronic neglect within a family, and overt maltreatment or avoidant caregiving. Severity, duration, and the number of caregiver disruptions predict which children cross the disorder threshold. [4] [5] [14]
Reactive attachment disorder versus disinhibited social engagement disorder
- Emotionally withdrawn / inhibited across caregivers
- Minimal comfort-seeking, minimal response to comfort
- Persistent social and emotional disturbance
- Often recovers faster when care becomes reliable
- Overly familiar with unfamiliar adults
- Reduced or absent social reserve
- Violates cultural social boundaries
- Indiscriminate behaviours may persist longer after corrective care
Epidemiology & Risk Factors
Attachment disorders are rare in the general population and concentrated where care has been grossly depriving. The Zeanah study of maltreated toddlers showed that the emotionally withdrawn and inhibited pattern of RAD is identifiable in severely neglected young children, and the Bucharest Early Intervention Project showed that institutionally-reared children have markedly higher rates of both disorders than community children. The teaching point for a viva is that deprivation, not temperament, carries the risk. [1] [5]
What predicts which deprived child develops a disorder? The Gleason work on indiscriminate behaviours showed that these persist in previously-institutionalised young children at rates far above community children, and that duration and timing of deprivation shape expression. Repeated changes of primary caregiver — each one resetting the chance to form a selective attachment — are as important as outright neglect. Protective forces point the other way: a stable, sensitive, committed carer; early corrective placement; and family support. [3] [12]
Cumulative adversity matters. A child in out-of-home care, exposed to family violence, or adopted after institutional rearing carries both higher baseline risk and a more complex presentation, which is why the out-of-home-care, refugee, and family-violence populations shift the whole plan. The carer is part of the risk equation: untreated carer trauma, mental illness, or substance use predicts poorer child outcomes and must be addressed as part of the child's plan. [13] [14]
Pathophysiology
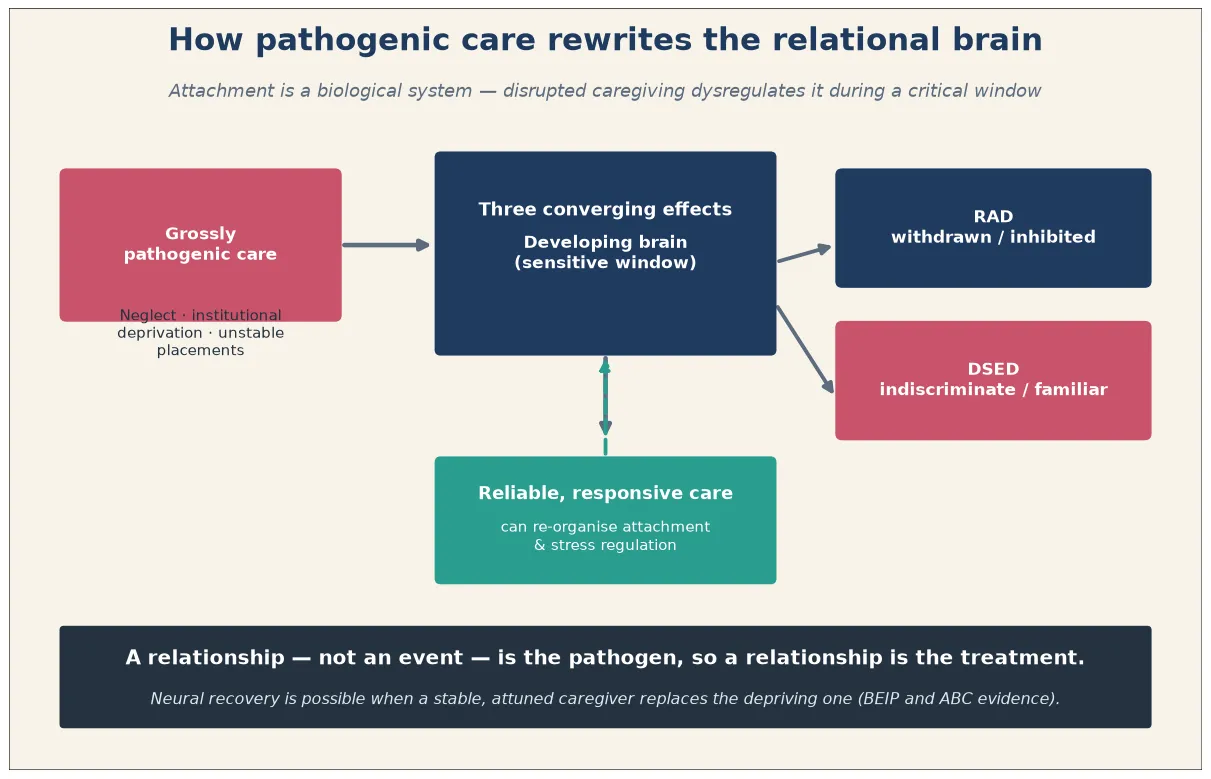
Picture the institutionally-reared four-year-old again. From infancy, distress met no responsive face, comfort came from rotating staff, and need taught the child nothing about a reliable other. Attachment is a biological system calibrated in that reciprocal loop, so when the loop is absent, the system miscalibrates. [6] [14]
The neuroscience is consistent with that experience. The HPA axis and cortisol pattern dysregulate, leaving the child physiologically primed or blunted in ways the Dozier group normalised with an attachment-based foster intervention. The amygdala and threat-salience circuitry over-tune to a world that was unpredictable, while prefrontal regulation lags behind. Sheridan's imaging work showed that institutional deprivation alters structural and functional neural connectivity, and that placement into family care partially normalises it. The net result is a relational brain shaped by unreliable care. [6] [7]
Development changes everything. Adversity encoded during the window when attachment, emotional regulation, and the stress response are being calibrated leaves deeper marks than the same adversity in an adult brain. That is why a relationship — not a single event — acts as the pathogen in relational trauma, and why the RAD and DSED phenotypes map onto different adaptive responses to unreliable care: one withdraws, the other approaches indiscriminately. The hopeful corollary is that a stable, attuned carer can re-organise attachment and stress regulation, which is exactly what the recovery evidence shows. [6] [12]
Clinical Presentation
Carers rarely lead with "attachment disorder." They bring a child who "won't let me comfort him," "goes to anyone," "doesn't seem to care," or who is withdrawn, watchful, or behaviourally dysregulated at home and at school. Your history converts that into the two patterns. [1] [13]
RAD appears as emotional withdrawal and inhibition across caregivers: minimal seeking of comfort when distressed, minimal response to comfort when offered, limited social responsiveness, and persistent emotional disturbance — unexplained fear, irritability, sadness, or a flat, watchful quality. DSED appears as indiscriminate sociability: approaching unfamiliar adults, reduced verbal and physical reserve, talking to or embracing strangers, wandering off with unfamiliar adults, and failing to check back with the carer. The two patterns can coexist, but they are not severity ends of one spectrum. [2] [3]
The developmental and contextual variants are where mistakes happen. Preschoolers show the raw behavioural patterns most clearly; school-age children layer on peer difficulty, dysregulation, and developmental delay; adolescents may present with risk-taking, substance use, and relational chaos layered on long-standing disorder. A child newly placed in out-of-home care may show a "honeymoon" of over-compliance followed by dysregulation as safety allows the old survival patterns to surface — this is not the carer's failure. Always gather the school's, the birth family's, and the social worker's view, because multi-informant data is how you separate a cross-caregiver pattern from a one-relationship problem. [4] [13]
Differential Diagnosis
Build the differential in layers: the other relational/developmental-trauma states, the neurodevelopmental disorders that mimic, the sensory and medical causes that must not be missed, and the risk patterns that are not disorders. [11] [13]
| Pattern | Favours | Against / distinguish |
|---|---|---|
| Social-communication impairment + restricted/repetitive behaviour, healthy care | Autism spectrum disorder | Pathogenic-care history present |
| Global delay, impaired cognition across domains | Intellectual disability | Social pattern tracks deprivation specifically |
| Does not respond to sound; speech delay | Hearing impairment | Audiometry and history clarify |
| Intrusion, avoidance, hyperarousal after a frightening event | PTSD / trauma response | Comfort-seeking intact outside triggers |
| Distress in one relationship, no disorder threshold | Insecure / disorganised attachment | Persistent cross-caregiver disorder pattern |
| Faltering growth, untreated illness, neglect signs | Neglect syndrome / medical mimic | Medical and safeguarding workup needed |
| History of prenatal alcohol exposure | FASD | Characteristic facies and growth, neuroprofile |
| Overlap with maltreatment injury | TBI from non-accidental injury | Symptoms predate placement; neuroimaging |
The two errors examiners love to probe are mirror-images: forcing an attachment-disorder label onto a socially odd child whose caregiving was healthy (usually autism), and missing the disorder in a withdrawn or over-friendly child because nobody asked about early care. When a neurodevelopmental label does not fit the natural history, or when the social pattern tracks deprivation, return to the caregiving history. [11] [13]
Clinical & Bedside Assessment
Lead with a caregiving history taken without blaming the current carer. A foster or kinship carer who feels accused will disengage, and the child loses the relationship you are trying to build. Pace the interview, gather the early-care story, and observe the child–carer relationship in a naturalistic moment rather than engineering one. [13] [14]
Attachment-informed assessment sequence
Safety and rapport
Calm setting, child-led pace, choice; confirm immediate safety; never force affection or 'attachment' demonstrations.
Caregiving history
Neglect, deprivation, institutional rearing, number and timing of caregiver disruptions, carer mental illness/substance use, maltreatment.
Behavioural pattern
Map RAD (withdrawn, no comfort-seeking/response) and DSED (indiscriminate familiarity) across multiple caregivers and settings.
Developmental track
Assess development in parallel; disorder and delay coexist and each needs its own assessment.
Risk and carer capacity
Ongoing neglect/abuse, placement safety, carer sensitivity, burnout, unrecognised carer trauma; self-harm in older children.
Formulate and plan
Diagnosis versus mimic and risk state, safeguarding status, step of care, named owner and safety-net.
Standardised observation tools and relationship measures sharpen the picture but do not replace clinical judgement, and many are proprietary or jurisdiction-specific — look them up rather than inventing cut-scores. Use what is matched to the child's age and language, and always gather the carer's, the teacher's, and the social worker's view alongside the child's, because discordance is itself data. Diagnosing on a single clinic observation is a classic error. [13] [14]
Examine the child too. Look for signs of neglect — faltering growth, untreated illness, dental disease, signs of abuse — that need their own medical and safeguarding pathway. Assess development directly, because attachment disorder and developmental delay coexist and each changes the plan. Ask the carer, kindly but directly, about their own history and capacity: an unsupported carer with their own unresolved trauma cannot run a relationship-based programme alone, and your plan must match real life. [1] [14]
Investigations
Attachment disorders are clinical diagnoses. There is no blood test, scan, or biomarker that confirms RAD or DSED, and the commonest investigation error is the shotgun panel ordered for "behaviour." Your core investigations are the structured caregiving history, the developmental assessment, the multi-informant observation, and the relationship assessment. [13] [14]
Investigate when the story points somewhere. Test hearing and vision when social unresponsiveness could be sensory; assess growth and nutrition when neglect may have caused faltering growth; consider FASD, genetic syndromes, or the effects of prenatal substance exposure when the phenotype fits. When maltreatment is disclosed, the safeguarding forensic examination is a separate, protocolised pathway — arrange it, do not improvise it. [13] [14]
Neuroimaging and EEG are not first-line for attachment-disorder behaviours without focal neurological signs or a head-injury history. Screen actively for the comorbidities that change the plan — autism, intellectual disability, ADHD, depression, anxiety, and abuse-driven PTSD — because treating the attachment picture while ignoring a comorbid disorder is a common cause of non-response. Where disorder and developmental delay coexist, run both tracks in parallel rather than forcing an either/or choice. [13] [14]
Management — Resuscitation
"Resuscitation" in an attachment-disorder presentation means immediate safety, medical stabilisation, and the end of ongoing pathogenic care — not a drug, and not a therapy session. [13] [14]
Make a same-day safety plan with the carer and the system: supervision, restriction of means where relevant, who to call, and where to go. Support the carer explicitly — carer burnout is common in this population, and an unsupported carer cannot be the secure base the child needs. Recognise that no medication "resuscitates" an attachment disorder; safety and stability are the resuscitation. [13] [14]
Management — Definitive & Stepwise
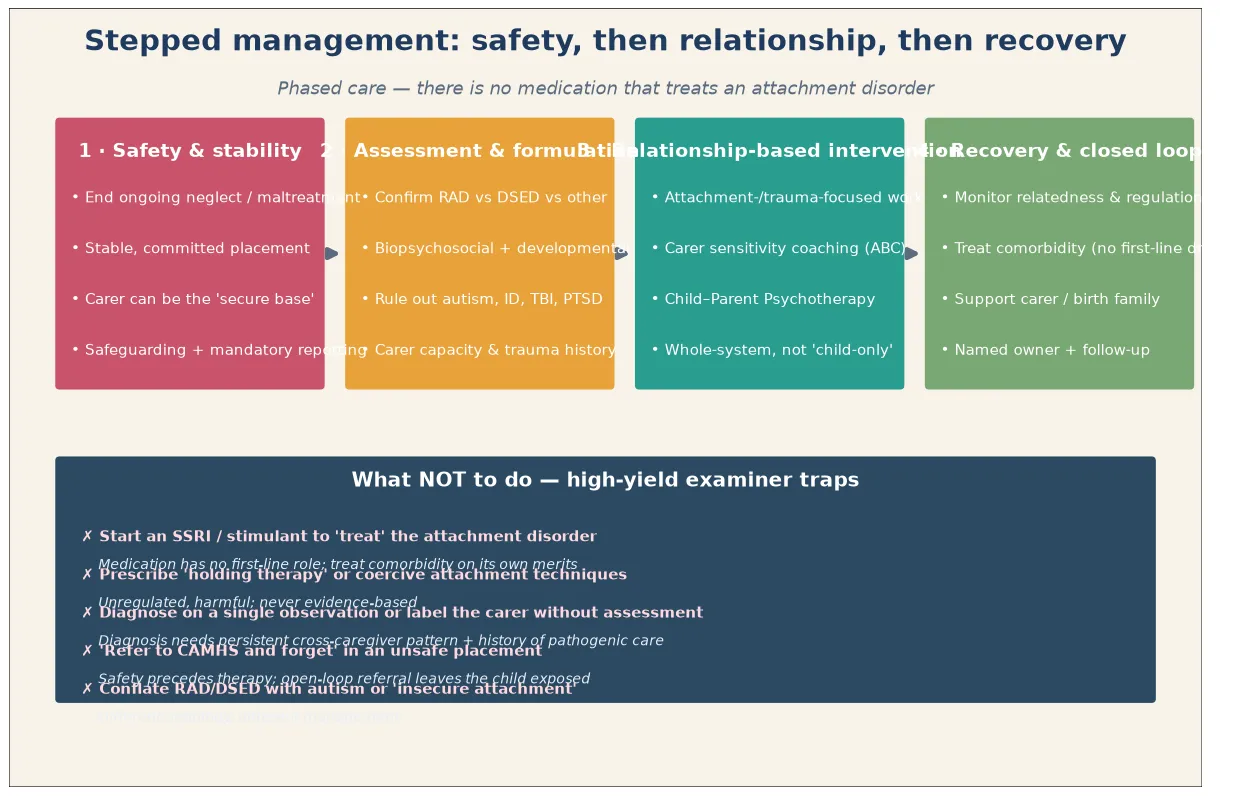
Phased, relationship-based care is the frame, and the order matters as much as the content. Safety and a stable committed placement come before any relationship work. [4] [13]
Step 1 — Safety and stability
End ongoing pathogenic care, secure a stable and committed placement, and ensure the carer can function as a "secure base." Without this foundation, no attachment- or trauma-focused intervention can take hold, because the child is still adapting to an unreliable world. [4] [13]
Step 2 — Assessment and formulation
Confirm RAD versus DSED versus other (autism, intellectual disability, sensory impairment, FASD, abuse-driven PTSD), run a biopsychosocial and developmental assessment, rule out medical mimics, and assess carer capacity and trauma history. A formulation that names both the disorder and the carer context is what guides the next step. [13] [14]
Step 3 — Relationship-based intervention (the evidence)
When safety and stability are in place, deliver an evidence-supported, relationship-based intervention to the carer-child dyad, not the child alone. The Bucharest Early Intervention Project randomised children to foster care versus continued institutional care and showed that placement reduces signs of RAD — placement is itself treatment, and recovery is mediated through attachment. Attachment and Biobehavioral Catch-up (ABC) is a carer-coaching programme: Dozier showed it normalises cortisol production in foster infants and improves young children's attachment behaviours. Child-Parent Psychotherapy (CPP), developed by Lieberman, improved outcomes for preschoolers exposed to violence with gains maintained at follow-up. [4] [7] [9]
Step 4 — Recovery and close the loop
Name the clinician who owns the plan, the date of follow-up, the interim carer strategy, and the return precautions: behavioural re-emergence, new disclosures, placement breakdown, or abuse recurrence. Monitor relatedness and regulation, treat any comorbid disorder on its own merits, support the carer and the birth family, and coordinate child protection, school, and the general practitioner. Do not "refer to CAMHS and forget" — an open-loop referral leaves a vulnerable child exposed. [13] [14]
Specific Subtypes & Scenarios
Reactive attachment disorder (withdrawn / inhibited). Relationship-based, sensitivity-focused intervention with a stable carer; expect slow recovery of comfort-seeking and social responsiveness as the carer becomes reliable. [1] [7]
Disinhibited social engagement disorder (indiscriminate / over-familiar). Add explicit safe-boundary and stranger-awareness work alongside the stable carer; indiscriminate behaviours can persist even after the RAD picture has resolved, so do not promise a quick fix. [3] [13]
Institutionally-reared / internationally-adopted child. Assess for both disorders and for developmental delay; recovery tracks the duration and timing of corrective placement, and the BEIP evidence shows placement into family care changes the trajectory. [4] [12]
Child newly placed in out-of-home care. Support the carer as the intervention; do not diagnose prematurely during the settling honeymoon, when inhibited or indiscriminate behaviours may briefly worsen before they improve. [13] [14]
Relational / developmental trauma (broader picture). After chronic interpersonal adversity, run phased care — safety, regulation, relationship, integration — over a longer course, with attention to attachment throughout. [10] [14]
Comorbid autism or intellectual disability. Run both tracks in parallel; do not let one diagnosis overshadow the other, and do not attribute all social oddness to attachment when a neurodevelopmental disorder is also present. [13]
Carer with their own unresolved trauma. Carer-focused support is part of the child's treatment plan; an unsupported, traumatised carer cannot sustain the relationship the child needs. [9] [14]
Adolescent with long-standing disorder plus risk-taking. Deliver integrated dual-focus care — never medication alone — and treat the self-harm and substance use that often accompany it. [13]
Refugee, asylum-seeking and culturally diverse child. Use culturally safe assessment, professional interpreters, and trauma-adapted care; beware of misreading culturally-shaped stranger norms as DSED. [13] [14]
Family-violence context. Safety and placement drive the plan; relational work cannot run in an unsafe home. [13] [14]
Complications & Pitfalls
- Diagnosing an attachment disorder on a single observation or without a caregiving history.
- Conflating "insecure" or "disorganised" attachment, or any "attachment difficulty," with a diagnosable disorder.
- Missing autism, intellectual disability, sensory impairment, or FASD by over-attributing to attachment.
- Blaming the current foster or kinship carer for behaviours that began before placement.
- Starting an SSRI or stimulant to "treat" the attachment disorder itself.
- Prescribing or tolerating coercive "holding therapy" or unregulated attachment techniques.
- Running relationship or exposure-based work while the placement is unsafe or unstable.
- Ignoring carer capacity, burnout, or unrecognised carer trauma.
- Missing ongoing neglect, maltreatment, or an unsafe placement.
- Open-loop referral to CAMHS with no interim plan, relapse signs, or safety-net.
Prognosis & Disposition
Recovery is possible and expected when care becomes reliable, stable, and responsive. The BEIP trial showed that randomised placement into family care reduced signs of RAD in institutionally-reared children, and McGoron showed that attachment mediates the effect of caregiving on psychopathology after deprivation — the mechanism of recovery is the relationship. DSED indiscriminate behaviours tend to be more persistent than RAD withdrawn behaviours even after corrective care, so set a realistic timeline with the carer. [4] [12]
Disposition after safety confirmed: phased relationship-based intervention via local CAMHS or early-intervention pathways, with medical-home interim support and developmental or comorbidity workup as indicated. [13]
Disposition when risk or a safeguarding concern surfaces: crisis and child-protection pathway, same-day supports, and stability before any therapy. [13]
Disposition for an older child with self-harm or suicidality: acute mental-health pathway layered onto the relational plan. [13]
Markers of response are emerging comfort-seeking and response to comfort, reduced indiscriminate behaviour, better regulation, developmental gains, and improved school function. Long CAMHS waitlists change the medical-home role: provide interim carer coaching, safety planning, and school liaison rather than passive waiting. [13] [14]
Special Populations
Institutionally-reared and internationally-adopted children carry the highest baseline risk; assess for both disorders and for developmental delay early, because recovery tracks the timing of corrective placement. Children in out-of-home care need the carer supported as the intervention, with the settling honeymoon handled gently and no premature diagnosis. [4] [14]
Children with autism, intellectual disability, or communication impairment may disclose less and present with overlapping social oddness — adapt assessment, run both tracks in parallel, and avoid diagnostic overshadowing. Refugee, asylum-seeking, and culturally and linguistically diverse families need culturally safe assessment, professional interpreters, and trauma-adapted care that does not misread cultural stranger norms. Indigenous families need non-stigmatising services that acknowledge intergenerational trauma and racism. Medically complex children and those with faltering growth from neglect need integrated medical and relational care. Rural and remote families should be offered telehealth-delivered relationship-based intervention rather than told to wait. [13] [14]
Evidence, Guidelines & Regional Differences
Key evidence anchors for exam defence: [1] [13]
- Zeanah 2004 Child Abuse Negl — RAD is identifiable in maltreated toddlers with a distinct withdrawn/inhibited pattern; the foundational epidemiology. [1]
- Gleason 2011 JAACAP — evidence-derived criteria discriminate RAD (withdrawn/inhibited) from DSED (indiscriminate/disinhibited); supports the two-disorder split. [2]
- Gleason 2014 Pediatrics — indiscriminate behaviours persist in previously-institutionalised young children at rates far above community children. [3]
- BEIP (Zeanah 2005 Child Dev; Smyke 2012 AJP) — attachment is disordered in institutionalised children, and randomised foster placement reduces signs of RAD; placement is treatment. [4] [5]
- Sheridan 2012 PNAS — institutional deprivation alters neural development, partially normalised by placement into family care. [6]
- Dozier 2008 Dev Psychopathol — the ABC attachment-based intervention normalises cortisol production in foster infants; biological mechanism of recovery. [7]
- Dozier 2009 Child Adolesc Social Work J — foster-parent training (ABC) improves young children's attachment behaviours; preliminary RCT. [8]
- Lieberman 2005 and 2006 JAACAP — Child-Parent Psychotherapy improves outcomes for preschoolers exposed to violence, with gains maintained at follow-up. [9] [10]
- McGoron 2012 JAACAP — attachment mediates the effect of caregiving on psychopathology after early deprivation; mechanism of recovery. [12]
- Rutter 2001 Br J Psychiatry — children's responses to profound institutional privation are specific and heterogeneous; deprivation can mimic but is not autism. [11]
- AACAP 2016 Practice Parameter (Zeanah, Chesher, Boris) — the assessment and treatment framework for RAD and DSED. [13]
- Bourne 2022 Clin Child Fam Psychol Rev — review of the consequences of inadequate caregiving for attachment, neurobiological development, and adaptive functioning. [14]
Attachment-focused, trauma-informed care is delivered through local CAMHS and early-intervention pathways, with carer-support programmes for foster, kinship, and adoptive families and telehealth options for rural and remote regions. Mandatory child-protection reporting thresholds are state and territory specific — name the principle and the local service, and do not invent statute numbers. Aboriginal Community Controlled Health Services and culturally safe pathways are central for Aboriginal and Torres Strait Islander and Māori children, acknowledging intergenerational trauma. [13] [14]
Controversies: over-diagnosis of "attachment disorder" in adoptive and foster populations where the full criteria are not met; the funding and fidelity of carer-coaching interventions; cultural adaptation of relationship-based programmes; and how to deliver evidence-based care when CAMHS waitlists are long and rural access is thin. [4] [13]
Exam Pearls
ATTACH
- RAD and DSED require grossly pathogenic care and onset in early childhood — the caregiving history opens the diagnosis. [1]
- RAD is withdrawn and inhibited with no comfort-seeking; DSED is indiscriminate and over-familiar with strangers. [2] [3]
- Attachment disorders are NOT insecure attachment, NOT autism, and NOT any "attachment difficulty." [11] [13]
- First-line treatment is a stable, responsive carer plus an evidence-based relationship intervention — there is no first-line medication. [7] [13]
- Coercive "holding therapy" is harmful and never indicated — a favourite examiner trap. [13]
- Placement into family care after institutional deprivation produces measurable recovery; ABC normalises cortisol. [4] [7]
- Safety and placement stability precede any relationship or exposure-based work. [13]
References
- [1]Zeanah CH, Scheeringa M, Boris NW, Heller SS, Smyke AT, Trapani J Reactive attachment disorder in maltreated toddlers. Child Abuse Negl, 2004.PMID 15350771
- [2]Gleason MM, Fox NA, Drury S, Smyke A, Egger HL, Nelson CA 3rd, et al Validity of evidence-derived criteria for reactive attachment disorder: indiscriminately social/disinhibited and emotionally withdrawn/inhibited types. J Am Acad Child Adolesc Psychiatry, 2011.PMID 21334562
- [3]Gleason MM, Fox NA, Drury SS, Smyke AT, Nelson CA 3rd, Zeanah CH Indiscriminate behaviors in previously institutionalized young children. Pediatrics, 2014.PMID 24488743
- [4]Smyke AT, Zeanah CH, Gleason MM, Drury SS, Fox NA, Nelson CA, et al A randomized controlled trial comparing foster care and institutional care for children with signs of reactive attachment disorder. Am J Psychiatry, 2012.PMID 22764361
- [5]Zeanah CH, Smyke AT, Koga SF, Carlson E, Bucharest Early Intervention Project Core Group Attachment in institutionalized and community children in Romania. Child Dev, 2005.PMID 16149999
- [6]Sheridan MA, Fox NA, Zeanah CH, McLaughlin KA, Nelson CA 3rd Variation in neural development as a result of exposure to institutionalization early in childhood. Proc Natl Acad Sci U S A, 2012.PMID 22826224
- [7]Dozier M, Peloso E, Lewis E, Laurenceau JP, Levine S Effects of an attachment-based intervention on the cortisol production of infants and toddlers in foster care. Dev Psychopathol, 2008.PMID 18606034
- [8]Dozier M, Lindhiem O, Lewis E, Bick J, Bernard K, Peloso E Effects of a Foster Parent Training Program on Young Children's Attachment Behaviors: Preliminary Evidence from a Randomized Clinical Trial. Child Adolesc Social Work J, 2009.PMID 22065891
- [9]Lieberman AF, Ghosh Ippen C, Van Horn P Child-parent psychotherapy: 6-month follow-up of a randomized controlled trial. J Am Acad Child Adolesc Psychiatry, 2006.PMID 16865033
- [10]Lieberman AF, Van Horn P, Ippen CG Toward evidence-based treatment: child-parent psychotherapy with preschoolers exposed to marital violence. J Am Acad Child Adolesc Psychiatry, 2005.PMID 16292115
- [11]Rutter ML, Kreppner JM, O'Connor TG, English and Romanian Adoptees (ERA) study team Specificity and heterogeneity in children's responses to profound institutional privation. Br J Psychiatry, 2001.PMID 11483469
- [12]McGoron L, Gleason MM, Smyke AT, Drury SS, Nelson CA 3rd, Gregas MC, et al Recovering from early deprivation: attachment mediates effects of caregiving on psychopathology. J Am Acad Child Adolesc Psychiatry, 2012.PMID 22721591
- [13]Zeanah CH, Chesher T, Boris NW, American Academy of Child and Adolescent Psychiatry (AACAP) Committee on Quality Issues (CQI) Practice Parameter for the Assessment and Treatment of Children and Adolescents With Reactive Attachment Disorder and Disinhibited Social Engagement Disorder. J Am Acad Child Adolesc Psychiatry, 2016.PMID 27806867
- [14]Bourne SV, Korom M, Dozier M Consequences of Inadequate Caregiving for Children's Attachment, Neurobiological Development, and Adaptive Functioning. Clin Child Fam Psychol Rev, 2022.PMID 35201540