Paeds · mental-behavioural-and-psychosomatic
Avoidant restrictive food intake disorder
Also known as ARFID · Avoidant/restrictive food intake disorder · Selective eating disorder · Food avoidance emotional disorder · Sensory food aversion · Food phobia
Fellowship approach to avoidant/restrictive food intake disorder (ARFID): a DSM-5-TR/ICD-11 eating disorder of restriction that harms nutrition, growth or function without weight/shape overvaluation. Three driver patterns — sensory, fear/aversive, low appetite/interest. Stepwise care: medical safety, stop coercion, protect nutrition, evidence-based CBT-AR or FBT, escalate with exit plan.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A ten-year-old will eat only beige crackers from one brand, drinks no milk, and has fallen two weight centiles in a year. He is not trying to lose weight. He panics if the packet changes. This is the face of avoidant/restrictive food intake disorder — and it was invisible in older classifications that recognised only anorexia and bulimia. ARFID was added to the DSM-5 in 2013 precisely to capture the large group of children whose restriction harms them but is not motivated by weight or shape, and ICD-11 followed. [14] [3]
ARFID is defined by four features taken together. The eating or feeding disturbance leads to a failure to meet nutritional or energy needs, shown by one or more of: significant weight loss or failure to gain expected growth; significant nutritional deficiency; dependence on oral nutritional supplements or enteral feeding; or marked interference with psychosocial function. The disturbance is not better explained by lack of available food or a cultural practice. Critically, there is no persistent disturbance in the way body weight or shape is experienced — the defining feature of anorexia nervosa is absent. The behaviour is also not better explained by another mental disorder or medical condition. [14] [2]
What makes ARFID a fellowship topic rather than a footnote is that it sits at the junction of four services that do not always talk to each other: general paediatrics, gastroenterology and nutrition, mental health, and developmental-behavioural paediatrics. The general paediatrician is usually the first port of call, owns the medical safety question, and must get the boundary with anorexia nervosa and the relationship to pediatric feeding disorder right — because wrong triage sends the child to the wrong team. [5] [3]
This page owns the ARFID diagnosis itself. Cross-link the feeding-problems page for the broader spectrum of selective eating and pediatric feeding disorder, the faltering-growth page for full growth-algorithm detail, and the autism page for the developmental context that so often surrounds ARFID. [23] [25]
Classification
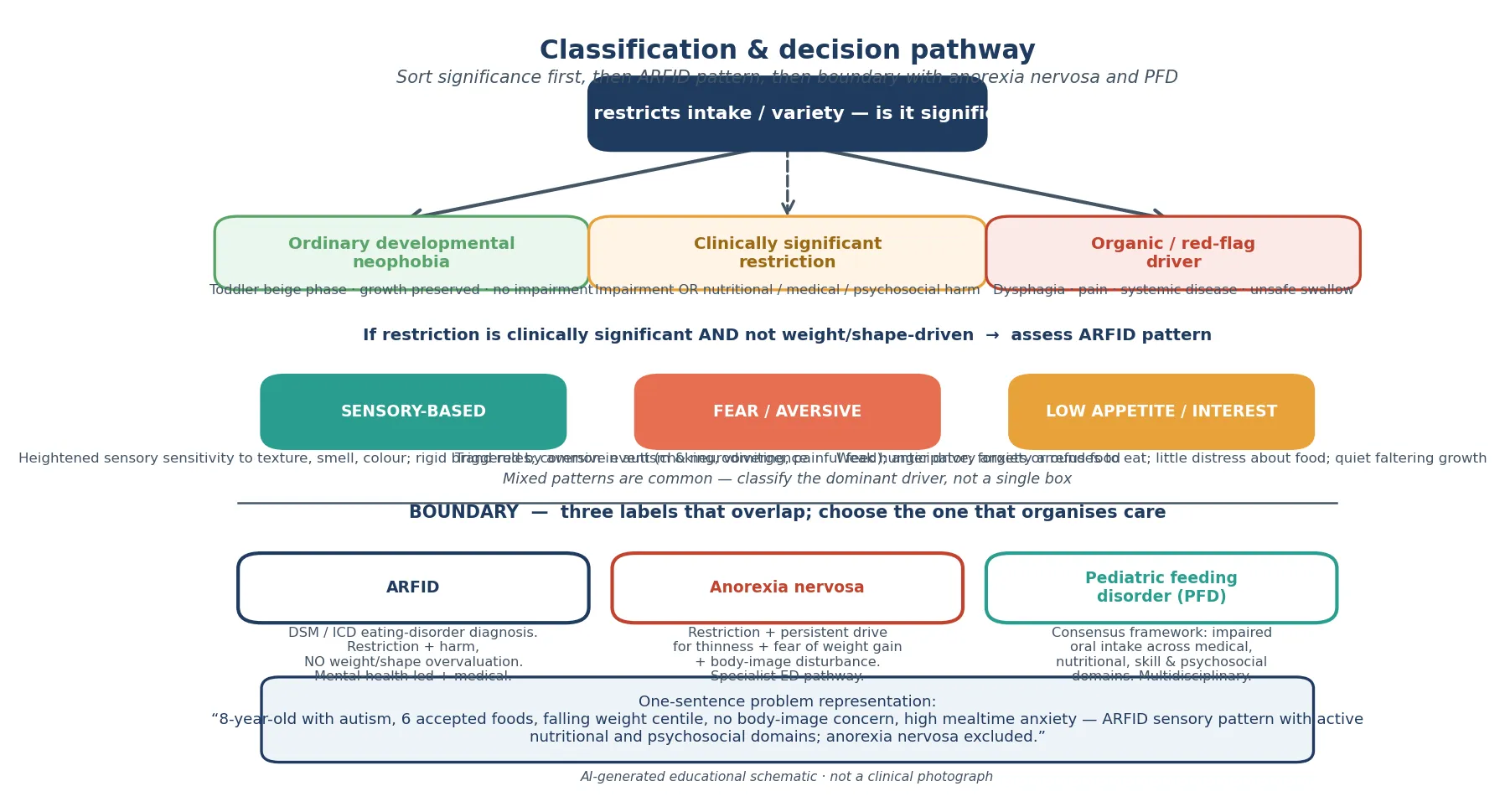
Classify in three moves: how significant, which pattern, and where is the boundary with anorexia nervosa. [2] [3]
- Driven by heightened sensory sensitivity — texture, smell, colour, even brand or packaging
- Often rigid: same food, same plate, same brand, meltdowns if rules violated
- Common in autism and neurodivergence; not a choice or naughtiness
- Variety is tiny but some children maintain weight by over-consuming accepted calorie-dense foods
- Triggered by a specific aversive event — choking, violent vomiting, a painful feed, or an invasive procedure
- Rapid onset; child avoids whole food groups or all solids
- Marked anxiety, panic, food phobia at the table
- May accept only purees or liquids; weight can drop quickly
- Weak hunger drive; child forgets to eat, is uninterested, rarely asks for food
- Little distress about eating — restriction is quiet, not anxious
- Growth can falter silently without dramatic food wars
- Overlaps with Chatoor's infant/toddler 'lack of interest' phenotype
These patterns are descriptive, not mutually exclusive. Many children show mixed features — a sensory-sensitive autistic child who develops food phobia after a choking scare is common. The point of classifying is to pick the dominant driver, because therapy is pattern-matched: CBT-AR is built around all three, but exposure technique differs for a sensory aversion versus a conditioned fear. [3] [9]
The harder and more examinable classification is the boundary with the two neighbours. ARFID, anorexia nervosa, and pediatric feeding disorder (PFD) overlap in clinical reality, and the Estrem consensus work exists precisely because teams were double-counting or arguing labels instead of treating. The rule: ARFID is the DSM/ICD eating-disorder label when restriction causes harm and there is no weight/shape overvaluation; anorexia nervosa adds that overvaluation; PFD is the consensus medical framework spanning medical, nutritional, feeding-skill and psychosocial domains. A child can meet both ARFID and PFD criteria. Use the label that organises care in your service, state the active problems clearly, and never let taxonomy delay safety or dietetics. [5] [14]
Epidemiology & Risk Factors
ARFID is far commoner than the older textbooks implied, but exact population figures depend on how strictly the criteria are applied. Katzman's Canadian surveillance and administrative data showed ARFID is a meaningful share of paediatric eating-disorder presentations, with age- and sex-specific patterns: younger children and boys are over-represented compared with anorexia nervosa, and many present to medical rather than mental-health services first. [1] [21]
The broad ARFID phenotype — children with significant restriction meeting the spirit of the criteria even if not captured by a registry — carries high rates of co-occurring mental and somatic conditions. Wronski's work shows that comorbid anxiety, neurodevelopmental conditions, and medical illness are the rule, not the exception, so comorbidity hunting is part of assessment, not optional colour. [4] [12]
Risk clusters in three groups. First, autism and neurodivergence: sensory-based selectivity is strikingly common in autism, can be severe and brand-specific, and is a top reason ARFID presents in developmental clinics. Second, a clear aversive trigger — a choking or vomiting episode, or repeated painful medical experiences such as nasogastric tubes, procedures, or severe reflux — primes the fear pattern. Third, anxious temperament, family anxiety, and high-pressure or coercive feeding amplify all three patterns. [17] [3] [23]
Do not forget the social determinants. Food insecurity, out-of-home care, family conflict, and migrant or Indigenous contexts where food culture is poorly understood all change both true risk and the help-seeking pathway. Ask about these openly and without judgement. [23]
Pathophysiology
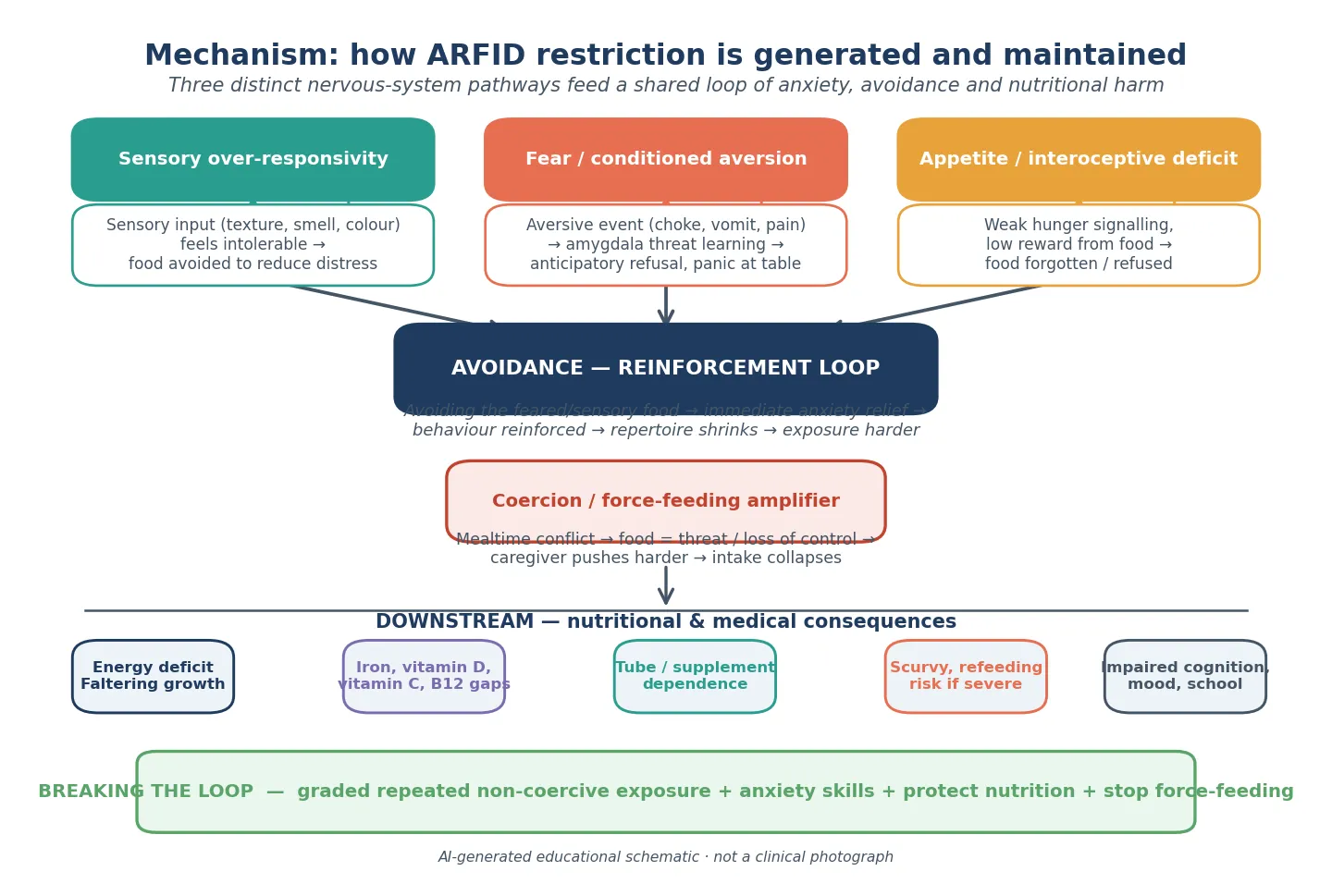
There is no single ARFID lesion. Three nervous-system pathways generate restriction, and they share a reinforcing loop that keeps restriction alive once it starts. Understanding the pathway tells you why exposure, not willpower, is the treatment. [3] [9]
Sensory over-responsivity is the engine of the sensory pattern. In some children — especially autistic children — the nervous system amplifies sensory input so that a crunch, a mixed texture, or a strong smell is genuinely intolerable, not fussy. Avoiding the food removes the distress, and the avoidance is rewarded. The repertoire shrinks because each new food feels like an assault, and the nervous system is never given the repeated calm exposure that would habituate it. [17]
Fear or conditioned aversion is fast threat learning. One choking episode, one violent vomit, or a painful feed links food to danger in the amygdala. From then on, the mere sight or smell of the food triggers anticipatory anxiety, panic, or refusal — even purees or liquids may be refused. This is a phobic mechanism, and like other phobias it responds to graded exposure, not to reassurance or force. [3] [14]
Low appetite or interoceptive deficit looks different and is the quietest. The child's hunger signalling is weak or the reward from eating is blunted, so food simply does not command attention. The child grazes, forgets meals, and fails to grow without the dramatic food wars of the other two patterns. Chatoor's work on toddlers with lack of interest in eating maps onto this pathway. [27] [3]
The three pathways converge on a shared avoidance-reinforcement loop: avoiding the food brings immediate relief, which strengthens avoidance, which narrows the repertoire further, which makes the next exposure harder. Coercion and force-feeding close the trap — when every meal is a battle, the child learns that food equals threat and loss of control, caregivers push harder, and intake collapses. Stopping the coercive cycle is treatment, not permissiveness. [23] [3]
Downstream, restricted diets risk energy shortfall and faltering growth, iron deficiency, vitamin D and other micronutrient gaps. In extreme restriction the consequences can be dramatic — scurvy from vitamin C deficiency has been reported in autistic children with ARFID, and refeeding risk appears in the severely malnourished. Swallow-safety problems can hide under a behaviour label if nobody asks about cough, wet voice, or chest infections. [18] [19] [13]
Clinical Presentation
Listen for the exact script, because the pattern often declares itself in the first minute. [1] [2]
Sensory pattern (any age, commonest in younger and autistic children). A parent says, "He only eats beige food," "She gags on lumps," or "He screams if the brand changes." Accepted foods may be as few as five to ten. The child is often calm when allowed the safe foods and distressed only when pushed. Weight may be preserved if accepted foods are calorie-dense, or may be falling. [17] [2]
Fear pattern (often sudden onset). "Since he choked last month he won't eat solids." Onset is dated to an event. The child is anxious around food, may panic at the table, and may accept only liquids or purees. Weight can drop quickly. Ask specifically about the trigger — choking, vomiting, a painful swallow, an invasive procedure. [3] [14]
Low-interest pattern (insidious). "She just never seems hungry." Meals are skipped or forgotten, grazing is poor, and growth has slipped quietly. There is little anxiety and little conflict — the absence of food wars is itself a clue. This is the pattern most easily missed because nobody is alarmed until the growth chart is checked. [27] [3]
Adolescent presentation. ARFID can present for the first time in adolescence, and the boundary with anorexia nervosa matters here as much as anywhere. An adolescent who restricts without body-image concern, drive for thinness, or compensatory behaviour may have ARFID. An adolescent who restricts and expresses fear of weight gain, body dissatisfaction, or engages in purging or compulsive exercise is on the anorexia nervosa pathway. Get this boundary right because the service route differs. Some patients begin in an ARFID pattern and later develop overvaluation of weight and shape — the boundary is not always static, so reassess over time. [7] [15]
Atypical and severe presentations. ARFID may first present through a medical crisis — scurvy, severe malnutrition with refeeding risk, or dehydration. A child may present through a mental-health crisis if family conflict or comorbid anxiety has become overwhelming. Always ask about weight loss tempo, dehydration signs, and systemic symptoms that suggest an organic driver hiding under a behaviour label. [18] [19] [25]
Differential Diagnosis
Build the differential around three questions: is there an organic driver, is this anorexia nervosa, and is this ordinary picky eating? [5] [14]
- Restriction PLUS persistent drive for thinness, fear of weight gain, body-image disturbance
- Purging, compulsive exercise, or hidden restriction support it
- Older child or adolescent predominates; often more weight loss
- Route to specialist eating-disorder service, not ARFID pathway
- Dysphagia (anatomical, neuromuscular, eosinophilic oesophagitis) — ask about cough, wet voice, chest infections
- Pain-driven refusal: severe reflux disease when truly present, food allergy, GI inflammation, constipation
- Coeliac disease, inflammatory bowel disease, malignancy can masquerade as 'behaviour'
- Red flags: dysphagia, odynophagia, systemic features, nocturnal symptoms, progressive course
- Common toddler phase; growth preserved; no nutritional or psychosocial harm
- No impairment — the child still meets needs and functions
- Improves with time and calm exposure; the family is not in crisis
- The line is HARM: once nutrition, growth, or function suffer, it is no longer 'just picky'
Cannot-miss traps: silent aspiration labelled as picky eating; coeliac disease or inflammatory disease presenting as restriction; eosinophilic oesophagitis in the vomiting or food-impaction child; severe malnutrition hidden by "he has always been small"; and an adolescent anorexia nervosa mislabelled as ARFID because nobody asked about body image. The single question that catches most — "Does it bother you what you weigh or what your body looks like?" — is worth asking at every ARFID contact. [7] [15] [25]
Clinical & Bedside Assessment
Assessment has two jobs: make the child medically safe, and build the problem representation that drives therapy. [3] [1]
History. Take a structured eating history, not a free-form chat. List accepted foods, textures, brands, and rules. Ask meal duration, where and with whom the child eats, what happens after refusal, and whether there is bribery, threats, or force. Ask specifically about choking, coughing, wet voice, vomiting, swallow pain, stool pattern, energy, sleep, and previous advice. For adolescents, see the young person alone and screen explicitly for drive for thinness, fear of weight gain, body-image concern, purging, and exercise — this is the anorexia-nervosa screen and must not be skipped. Screen development, autism traits, anxiety, mood, and suicidality. [3] [21]
Growth. Plot weight, length or height, and BMI or weight-for-length on appropriate charts using serial points. WHO standards anchor early-childhood interpretation. Tempo matters more than any single number — a child crossing two centiles down needs action regardless of where they sit. [26] [25]
Observe a meal. If safe, watch a snack or meal. Look for approach, gagging, packing, expulsion, pocketing, caregiver hovering, force, and child shutdown. Observation data often explain more than any laboratory panel. [23]
Examine. Check oromotor structure, dentition, thrush, abdomen, tone, hydration, skin (look for micronutrient signs — perifollicular keratosis and bruising in scurvy), and any signs of systemic disease. Assess work of breathing if intake fatigue is part of the story in younger children. [18] [28]
Team. Involve dietetics early when variety is tiny or growth is threatened. Add psychology or eating-disorder services for CBT-AR or FBT and for comorbid anxiety. Add speech-language pathology or occupational therapy for oromotor skill and sensory texture work. Add gastroenterology, ENT, or other medical teams when red flags appear. The general paediatrician usually coordinates. [3] [11]
Investigations
Most thriving children with short-lived mild selectivity need no shotgun panel. In ARFID, investigation follows the harm and the hypothesis. [3] [25]
Order bloods when growth is faltering, the diet is extremely narrow, energy is poor, or symptoms suggest deficiency or organic disease. Common targets guided by history include full blood count and iron studies, vitamin D, and other micronutrients selected by diet pattern. In extreme restriction add vitamin C, vitamin A, and B12 where the history suggests risk. Coeliac serology belongs when growth, stool, family history, or other clues raise it — not as automatic decoration. [18] [25]
Pursue swallow assessment when cough, wet voice, recurrent chest infection, or neurological concern suggests an unsafe swallow. Clinical feeding evaluation comes first; instrumental tests (videofluoroscopic swallow study, fibre-endoscopic evaluation) are for selected children who are stable enough and in whom results will change management. [28]
An electrocardiogram is indicated when restriction is severe or the child is bradycardic, because malnutrition and electrolyte disturbance carry refeeding and cardiac risk. In the severely malnourished child, refeeding bloods — phosphate, magnesium, potassium — are part of safety, not investigation. [13] [11]
Avoid low-value cascades: routine abdominal imaging for every restricted eater, automatic long-term acid suppression without a clear indication, endless allergy panels driven by parental fear alone, and repeated normal imaging that reinforces a disease model without changing management. NASPGHAN and ESPGHAN reflux guidance argues for stewardship, not reflexive proton-pump inhibitor use. [28]
Management — Resuscitation
Most children with ARFID are ambulatory. A minority are not, and recognising them is the first management act. [13] [11]
Treat as urgent or emergency when there is dehydration, inability to maintain fluids orally, suspected hypoglycaemia risk from near-zero intake, severe malnutrition with refeeding risk, progressive aspiration, or an acute medical illness wearing a food-refusal mask. ABCDE, point-of-care or laboratory glucose when indicated, cautious fluids, and senior review come before behavioural coaching. Admit when home safety is uncertain. [13] [25]
For the severely malnourished child, refeeding syndrome is the killer. Restore nutrition gradually under monitoring — phosphate, magnesium, and potassium surveillance, with supplementation guided by local refeeding protocol — because the shift from catabolism to anabolism drives electrolytes intracellularly. This is a medical emergency managed on a paediatric ward or eating-disorder unit, not at home. [13] [11]
If the child is medically unstable, pause graded exposure work. You cannot desensitise a child who needs intravenous rehydration, airway protection, or refeeding surveillance. [13]
Management — Definitive & Stepwise
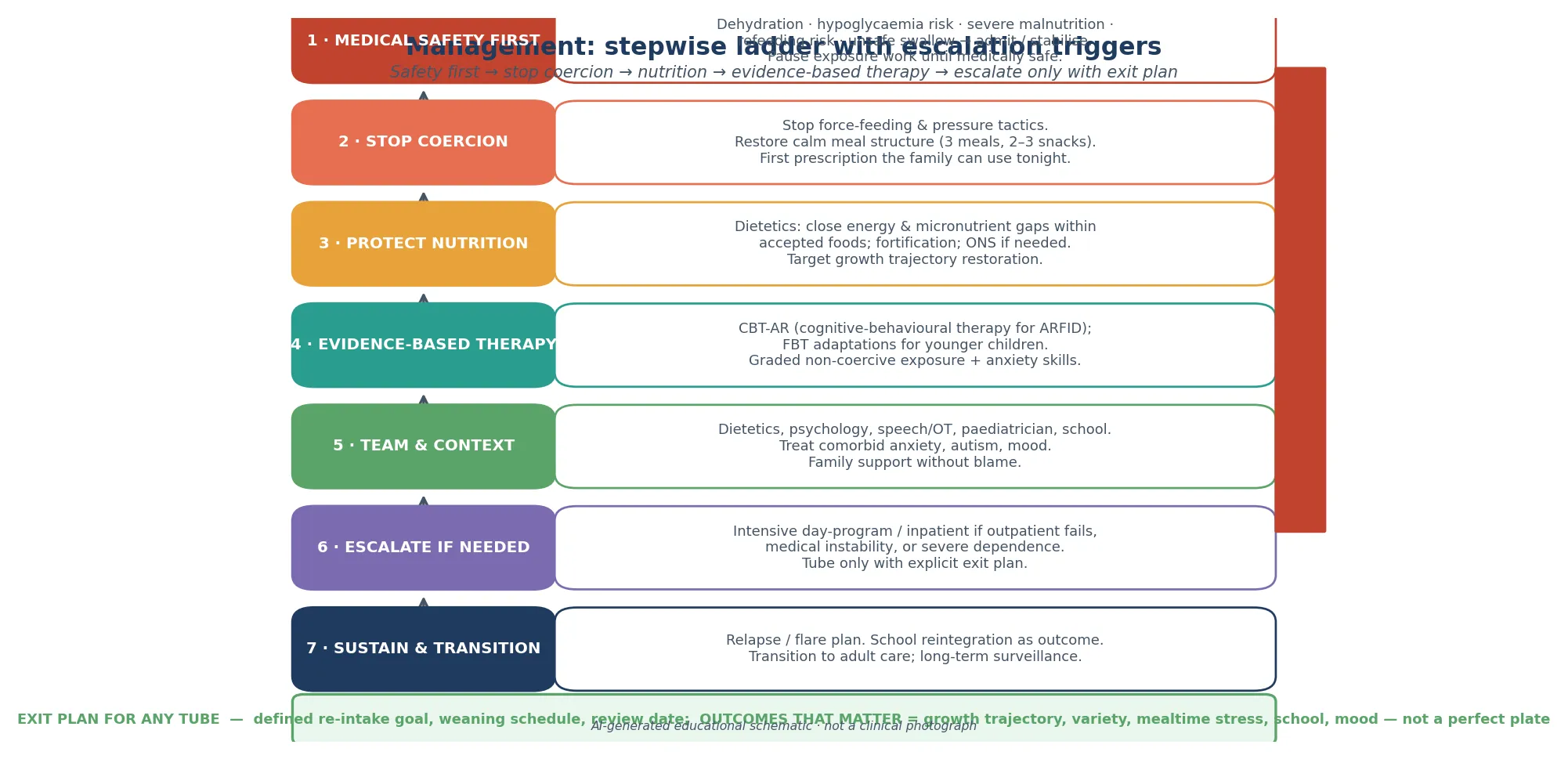
Once safety is clear, climb a ladder — and climb only as far as the child needs. [3] [8]
ARFID management ladder
Medical safety first — stabilise dehydration, hypoglycaemia, refeeding risk, unsafe swallow before any therapy
Stop coercion — end force-feeding and pressure tactics; restore calm meal structure of three meals and two to three snacks
Protect nutrition — dietetics closes energy and micronutrient gaps within accepted foods, with fortification and oral nutritional supplements where needed, targeting growth restoration
Deliver evidence-based therapy — CBT-AR for adolescents and adults with strong feasibility and preliminary-outcome evidence, or FBT adaptations for younger children; graded non-coercive exposure matched to the driver pattern
Treat comorbidity and context — manage anxiety, autism, mood; coordinate school and family support without blame
Escalate if needed — intensive day-program or inpatient care if outpatient fails, medical instability recurs, or severe supplement or tube dependence develops
Sustain and transition — relapse or flare plan, school reintegration as an outcome, and structured transition to adult care with long-term surveillance
Cognitive-behavioural therapy for ARFID (CBT-AR). Thomas and colleagues developed and piloted CBT-AR, a manualised treatment that targets all three driver patterns through psychoeducation, regular eating, and graded exposure matched to the mechanism — interoceptive exposure for low-interest, systematic desensitisation for fear, and sensory-based exposure for selectivity. Feasibility and preliminary outcome data are encouraging, and a proof-of-concept study has supported its mechanisms of change. The Winten meta-analysis of psychological therapies for ARFID supports the direction of benefit, though the evidence base is still maturing. [8] [9] [20]
Family-based treatment (FBT) adaptations. For younger children, FBT-style adaptations — empowering parents to restore nutrition and lead exposure at home — have shown feasibility in case series. The Canadian practice guidelines for child and adolescent eating disorders endorse a family-involved, evidence-informed approach. [10] [11] [22]
Nutrition and medical adjuncts. Dietetics is central, not peripheral: closing gaps within accepted foods, fortifying, and using oral nutritional supplements or, when truly necessary, enteral feeding — always with an explicit exit plan and review date. Simple measures are adjunctive only; there is no pharmacotherapy licensed for ARFID itself. [3] [25]
Specific Subtypes & Scenarios
Autism and sensory ARFID. Expect rigid, brand-specific rules and sensory-driven selectivity. Change one variable at a time, protect calories while expanding flexibility, and do not demand a neurotypical plate as the first goal. Sensory-informed goals beat generic try-everything advice, but still check growth and swallow. [17] [18]
Post-choking or post-vomit fear. Medical clearance of swallow if indicated, then graded fear-based treatment with psychology and feeding therapy. Do not force solids to prove they are safe — that is how phobias are strengthened, not broken. [3] [8]
Low-interest with quiet faltering growth. Schedule meals, reduce endless grazing, assess medical contributors, and involve dietetics and mental-health supports early. This is the pattern most easily missed because there is no drama. [27] [3]
Severely malnourished or low-weight ARFID. Bryson and Lange report the outcomes of low-weight ARFID after medical hospitalisation and at long-term follow-up — these children need inpatient medical stabilisation with refeeding surveillance, then a structured psychological pathway, and they carry meaningful persistent morbidity. Treat refeeding risk seriously. [13] [16]
Adolescent new-onset restriction. Explicitly assess weight and shape overvaluation, drive for thinness, purging, and compulsive exercise. Some adolescent ARFID presentations cross over to anorexia nervosa over time, so screen at every contact and reroute when overvaluation emerges. [7] [15]
Comorbid anxiety, depression, or neurodevelopmental disorder. Comorbidity is the rule. Treating ARFID without treating the comorbid anxiety is a common reason for failure. Build mental-health care into the plan from the start. [4] [12]
Rural or telehealth review. Use video of a meal where possible, local growth measurements, clear escalation criteria, and early dietetic and psychology telehealth. Do not pretend observation is complete when it is not. [3]
Complications & Pitfalls
The errors are predictable and examinable. [3] [5] [23]
- Calling every selective eater ARFID, or dismissing every ARFID presentation as "just picky" — the line is harm, not parental annoyance. [23]
- Missing anorexia nervosa because nobody asked about body image — the single highest-yield screening question in adolescent ARFID. [7] [15]
- Missing an organic driver (eosinophilic oesophagitis, coeliac disease, unsafe swallow, severe reflux) hidden under a behaviour label. [28] [25]
- Missing refeeding syndrome in the severely malnourished child — a preventable killer. [13]
- Missing a micronutrient emergency such as scurvy, or vitamin A or B12 deficiency, in extreme restriction. [18] [19]
- Using force-feeding or high-pressure tactics, which amplify the avoidance loop and worsen outcome. [23]
- Fragmented care: multiple specialists giving contradictory messages that leave the family confused and the child stuck. [3] [22]
- Placing a feeding tube without an exit plan, creating iatrogenic dependence. [3]
- Letting the ARFID label stop you thinking — a functional or psychiatric frame must not block reassessment when a new red flag appears. [25]
Prognosis & Disposition
ARFID is more treatable than families often believe, but it is not always quick, and the long-term course is still being mapped. The Kambanis prospective two-year study of ARFID course and predictors of outcome gives the clearest modern picture: outcomes vary, a subset persists or crosses into other eating disorders, and predictors of poorer outcome include longer duration, low weight, and comorbidity. The Lange long-term follow-up of low-weight ARFID confirms meaningful persistent morbidity in the most severely affected. [6] [16]
What predicts better outcomes? Early recognition, medical stabilisation, structured evidence-based therapy, protected nutrition, treated comorbidity, and family engagement without blame. What predicts worse? Prolonged school absence, untreated anxiety or depression, coercion, fragmented care, and tubes placed without exit plans. [6] [12]
Primary care and medical home fits mild presentations with preserved growth and a workable plan. Secondary paediatric and mental-health teams fit multi-domain impairment, micronutrient risk, or failed first-line coaching. Tertiary eating-disorder or intensive pathways fit severe ARFID, medical instability, refeeding risk, or failed outpatient care. Safety-net every discharge: red flags, the next weight-check date, and who to call. [3] [11]
Outcomes that matter are growth trajectory, dietary variety, mealtime stress, micronutrient status, school participation, mood, and caregiver confidence — not a perfect food pyramid photograph. [6]
Special Populations
Autism and neurodivergence. Sensory ARFID is common and can be severe. Neurodiversity-affirming, sensory-informed goals outperform generic advice, but growth, swallow, and micronutrients still need active surveillance. [17] [18]
Intellectual disability. Restriction and caregiver accommodation can be long-standing; diet quality, constipation, and micronutrients often need active surveillance. [4]
Complex chronic and technology-dependent children. Tube history, oromotor limits, and repeated medical procedures all raise ARFID risk; plan feeding support and family mental-health attention together. [22]
Out-of-home care and safeguarding. Mealtime control, force, and food restriction can signal broader harm. Document carefully and follow local safeguarding pathways. [23]
Indigenous, migrant, and language-discordant families. Use interpreters, respect food culture, and avoid judging traditional foods as the problem. Ask about access, racism in prior care, and food insecurity. [23]
Adolescents and transition. Screen for anorexia-nervosa crossover at every contact, and plan structured transition to adult eating-disorder or mental-health services, carrying the recovery and relapse plan across. [7] [15]
Evidence, Guidelines & Regional Differences
The evidence base for ARFID is young and growing fast. The diagnosis itself was operationalised for research by the Radcliffe ARFID Workgroup, which laid out criteria and directions for study. Katzman's incidence and classification work defined the clinical phenotype and its age- and sex-specific patterns, while Wronski's broad-phenotype study mapped the comorbidity landscape. [14] [1] [2] [4]
On treatment, Thomas and colleagues established CBT-AR feasibility and preliminary outcomes; Burton-Murray provided proof-of-concept evidence for its mechanisms of change; Spettigue showed family therapy and adjunctive-treatment feasibility; and the Winten meta-analysis synthesised psychological-therapy evidence for adolescents and adults — supportive but still maturing. The Canadian practice guidelines give the most concrete current service-level recommendations for children and adolescents with eating disorders including ARFID. [8] [9] [10] [20] [11]
On outcomes, Kambanis's two-year prospective study and the Lange long-term follow-up of low-weight ARFID are the current anchors, joined by Bryson's hospitalisation-outcomes work and Norris's comorbidity and treatment-needs data. [6] [16] [13] [12]
ANZ. RACP training expects growth, nutrition, behavioural, and mental-health synthesis in long and short cases. Use RCH-style growth resources and multidisciplinary community and mental-health feeding supports where available; eating-disorder services (such as the CADS model in some regions) take moderate-to-severe ARFID. [25]
UK. NICE NG69 (eating disorders: recognition and treatment) applies to ARFID and routes children and young people to specialist community eating-disorder services for treatment. NICE NG75-era faltering-growth thinking informs thresholds for investigation and support. Community dietetics and CAMHS or eating-disorder interfaces vary by region. [25]
US. DSM-5-TR criteria are native. AAP-aligned primary care plus NASPGHAN pathways are common; intensive multidisciplinary day programmes and academic ARFID services are more visible in the literature but access is uneven. [28] [5]
Canada. Canadian practice guidelines for child and adolescent eating disorders give concrete service-level recommendations; Katzman and Norris contributions make Canadian paediatrics a strong voice in ARFID classification and treatment. [11] [1]
Controversies worth naming in viva: how to operationalise ARFID versus pediatric feeding disorder in service design; whether ARFID and anorexia nervosa are better understood as points on a single restrictive-eating spectrum with migration between them; how early and how intensively to use psychological therapy; how far to push enteral feeding and for how long; and how to ensure equitable access to evidence-based care for autistic, Indigenous, rural, and socioeconomically disadvantaged children. [5] [15] [20]
Exam Pearls
- The defining exclusion is weight or shape overvaluation — name it first, every time. [14]
- Three driver patterns: sensory, fear or aversion, low appetite or interest; mixed is common. [2] [3]
- Harm — nutritional, medical, or psychosocial — is what separates ARFID from ordinary picky eating, not parental annoyance. [23]
- Comorbidity is the rule: screen for anxiety, autism, ADHD, mood, and organic disease. [4] [12]
- CBT-AR is the leading evidence-based therapy; FBT adaptations work for younger children. [8] [10]
- Refeeding syndrome kills the severely malnourished ARFID child — restore gradually under electrolyte surveillance. [13]
- Scurvy and other micronutrient emergencies can be the first presentation of extreme restriction, especially in autism. [18] [19]
- A feeding tube is a bridge with an exit plan, never an endpoint. [3]
SAFE-ARFID assessment hooks
Long-case ready synthesis
In a long case, open with growth trajectory and medical safety, explicitly exclude anorexia nervosa, then name the dominant ARFID pattern, then give a staged plan with who does what this month. Examiners reward the boundary question held cleanly, comorbidity treated in parallel, and communication with exhausted caregivers that refuses to moralise the child. [3] [6]
References
- [1]Katzman, DK Incidence and Age- and Sex-Specific Differences in the Clinical Presentation of Children and Adolescents With Avoidant Restrictive Food Intake Disorder. JAMA pediatrics, 2021.PMID 34633419
- [2]Katzman, DK Classification of Children and Adolescents With Avoidant/Restrictive Food Intake Disorder. Pediatrics, 2022.PMID 35945342
- [3]Kambanis, PE Assessment and Treatment of Avoidant/Restrictive Food Intake Disorder. Current psychiatry reports, 2023.PMID 36640211
- [4]Wronski, ML Mental and Somatic Conditions in Children With the Broad Avoidant Restrictive Food Intake Disorder Phenotype. JAMA pediatrics, 2025.PMID 39960738
- [5]Estrem, HH A US-Based Consensus on Diagnostic Overlap and Distinction for Pediatric Feeding Disorder and Avoidant/Restrictive Food Intake Disorder. The International journal of eating disorders, 2025.PMID 39679744
- [6]Kambanis, PE Prospective 2-Year Course and Predictors of Outcome in Avoidant/Restrictive Food Intake Disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 2025.PMID 38718975
- [7]Kambanis, PE Course of avoidant/restrictive food intake disorder: Emergence of overvaluation of shape/weight. Journal of eating disorders, 2024.PMID 38702736
- [8]Thomas, JJ Cognitive-behavioral therapy for avoidant/restrictive food intake disorder: Feasibility, acceptability, and proof-of-concept for children and adolescents. The International journal of eating disorders, 2020.PMID 32776570
- [9]Burton-Murray, H Cognitive-behavioral therapy for avoidant/restrictive food intake disorder: A proof-of-concept for mechanisms of change and target engagement. The International journal of eating disorders, 2024.PMID 38213085
- [10]Spettigue, W Treatment of children and adolescents with avoidant/restrictive food intake disorder: a case series examining the feasibility of family therapy and adjunctive treatments. Journal of eating disorders, 2018.PMID 30123505
- [11]Couturier, J Canadian practice guidelines for the treatment of children and adolescents with eating disorders. Journal of eating disorders, 2020.PMID 32021688
- [12]Norris, ML Treatment Needs and Rates of Mental Health Comorbidity in Adolescent Patients With ARFID. Frontiers in psychiatry, 2021.PMID 34349680
- [13]Bryson, AE Outcomes of low-weight patients with avoidant/restrictive food intake disorder and anorexia nervosa at long-term follow-up after treatment in a partial hospitalization program for eating disorders. The International journal of eating disorders, 2018.PMID 29493804
- [14]Eddy, KT Radcliffe ARFID Workgroup: Toward operationalization of research diagnostic criteria and directions for the field. The International journal of eating disorders, 2019.PMID 30758864
- [15]Eddy, KT Avoidant/Restrictive Food Intake Disorder Plus Eating Disorder Comorbidity: Are Two Diagnoses Better Than One? The International journal of eating disorders, 2025.PMID 40099862
- [16]Lange, CRA Long-term follow-up study of low-weight avoidant/restrictive food intake disorder and childhood-onset anorexia nervosa: comparison of autistic eating behaviours. Journal of eating disorders, 2026.PMID 42421087
- [17]Bourne, L Avoidant/restrictive food intake disorder and severe food selectivity in children and young people with autism: A scoping review. Developmental medicine and child neurology, 2022.PMID 35112345
- [18]Sharp, WG Scurvy as a Sequela of Avoidant-Restrictive Food Intake Disorder in Autism: A Systematic Review. Journal of developmental and behavioral pediatrics : JDBP, 2020.PMID 32044868
- [19]Benezech, S Is it leukemia, doctor? No, it's scurvy induced by an ARFID! European journal of clinical nutrition, 2020.PMID 32313189
- [20]Winten, CG A Systematic Review and Meta-Analysis of Psychological Therapies for Avoidant/Restrictive Food Intake Disorder (ARFID) in Adolescents and Adults. The International journal of eating disorders, 2026.PMID 41913341
- [21]Matherne, CE Avoidant/Restrictive Food Intake Disorder (ARFID) Symptoms in Adolescent Patients With Disorders of Gut-Brain Interaction. The International journal of eating disorders, 2025.PMID 39912431
- [22]Rienecke, RD Adapting treatment in an eating disorder program to meet the needs of patients with ARFID: Three case reports. Clinical child psychology and psychiatry, 2020.PMID 31315462
- [23]Kerzner, B A practical approach to classifying and managing feeding difficulties. Pediatrics, 2015.PMID 25560449
- [24]Goday, PS Pediatric Feeding Disorder: Consensus Definition and Conceptual Framework. Journal of pediatric gastroenterology and nutrition, 2019.PMID 30358739
- [25]Gonzalez-Viana, E Faltering growth in children: summary of NICE guidance. BMJ (Clinical research ed.), 2017.PMID 28963099
- [26]WHO Multicentre Growth Reference Study Group WHO Child Growth Standards based on length/height, weight and age. Acta paediatrica (Oslo, Norway : 1992). Supplement, 2006.PMID 16817681
- [27]Chatoor, I Failure to thrive in toddlers with lack of interest in eating and food and their cognitive development during later childhood. Frontiers in pediatrics, 2023.PMID 37705600
- [28]Rosen, R Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. Journal of pediatric gastroenterology and nutrition, 2018.PMID 29470322
- [29]Kovacic, K Pediatric Feeding Disorder: A Nationwide Prevalence Study. The Journal of pediatrics, 2021.PMID 32702429
- [30]Cardona Cano, S Trajectories of picky eating during childhood: A general population study. The International journal of eating disorders, 2015.PMID 25644130