Paeds · mental-behavioural-and-psychosomatic
Child and adolescent suicide and self-harm assessment
Also known as Suicidal ideation assessment · Suicide risk assessment · Self-harm assessment · Non-suicidal self-injury assessment · Safety planning · Means restriction counselling
A fellowship approach to assessing suicide risk and self-harm in children and adolescents: distinguishing non-suicidal self-injury from suicidal self-harm; structured risk stratification using ideation, plan, intent, means access and prior attempts; co-building a Stanley-Brown safety plan; means restriction counselling with carers; and disposition matched to dynamic risk across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 14-year-old is brought to the emergency department after taking a handful of paracetamol tablets during an argument with a parent. A 16-year-old in your clinic quietly shows you fresh cuts on her forearm and asks you not to tell anyone. A 12-year-old, asked how he is feeling after a friendship breakdown, says, "Sometimes I wish I was dead." These are not rare presentations. They are the everyday work of paediatrics, and the skill they test is suicide and self-harm assessment. [3] [4]
Suicidal ideation means thoughts of ending one's own life. It ranges from passive ("I wish I could go to sleep and not wake up") to active ("I think about killing myself"). A suicide attempt is self-directed behaviour with at least some intent to die, regardless of medical lethality. Suicide is death caused by self-directed injurious behaviour with intent to die. Self-harm is intentional self-injury or self-poisoning regardless of motivation — and this umbrella term deliberately includes both suicidal and non-suicidal acts. [3] [4]
The single most important distinction in this topic is between non-suicidal self-injury (NSSI) and suicidal self-harm. NSSI is deliberate self-inflicted damage to the surface of the body — cutting, burning, hitting — undertaken to relieve an intolerable affect, without intent to die. Suicidal self-harm carries intent to die. The distinction matters because the function, the short-term risk and the management differ — and because mixing them up at the bedside leads either to dangerous under-reaction or to frightened over-hospitalisation. [7] [18]
The skill here is not predicting who will die by suicide — no tool can do that. It is running an encounter where a young person feels safe enough to tell you the truth, stratifying their acute risk honestly, and acting on it with a plan the young person and their carers can own. [15] [3]
Classification
Start with the patient in front of you, then classify what the behaviour is and how severe the current risk is. [1]
What kind of self-harm or suicidality is this?
Non-suicidal self-injury
NSSI
- Deliberate tissue damage without intent to die
- Function is affect regulation and distress relief
- Often repetitive (cutting, burning, hitting)
- Still assess for co-existing suicidal ideation
- Raises lifetime suicide risk - do not dismiss
Suicidal self-harm
Attempt
- Self-harm with intent to die
- Lethality is not the test - intent is
- Even ambivalent intent counts
- Higher acute risk, lower threshold for admission
- Always remove means and co-build a safety plan
Suicidal ideation only
No act yet
- Passive or active thoughts of death
- Stratify by plan, intent and means
- Most ideation never proceeds to action
- Still warrants a safety plan and follow-up
- Re-assess at every contact
Aborted / interrupted attempt
High-risk signal
- Started the act but stopped or was stopped
- Carries risk close to a completed attempt
- Treat as high risk regardless of outcome
- Detailed assessment of what stopped them
- Urgent mental-health involvement
The categories overlap and shift. A young person who self-harms without suicidal intent today may develop suicidal intent next week. Classify at the current contact and re-assess at the next. [7] [10]
Severity stratification: the C-SSRS dimensions
The Columbia Suicide Severity Rating Scale organises assessment around the dimensions that actually predict near-term risk: the severity of ideation, whether there is a plan, whether there is intent, access to means, and any history of prior attempts. You weigh these against protective factors to assign a working risk level — low, moderate, high or imminent — that drives disposition. [1] [2]
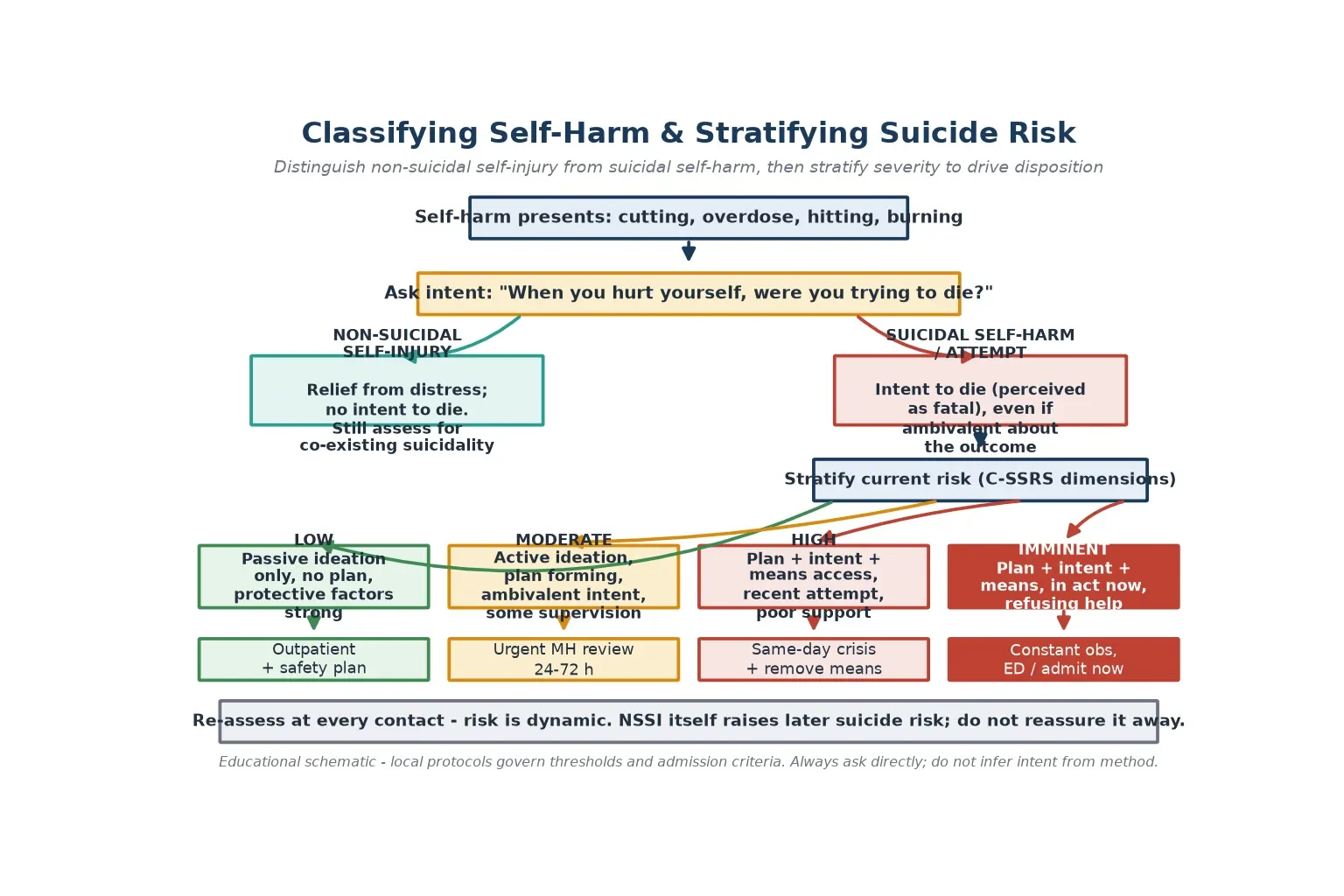
Read the figure like this: the branch point is intent, not lethality. A low-medical-lethality overdose taken with clear intent to die is suicidal and may be high risk; a deep wound inflicted purely to relieve distress, with no wish to die, is NSSI but still needs assessment. [7] [18]
Epidemiology & Risk Factors
Suicide is among the leading causes of death in adolescents worldwide. Community meta-analyses estimate that a substantial minority of adolescents report suicidal ideation, and that self-harm in adolescents is common across community-based studies. The epidemiology is sobering precisely because the acts cluster in a population that otherwise has few medical causes of death. [4] [5] [6]
A clear sex difference runs through the data: adolescent females report more ideation and make more non-fatal attempts, while males die by suicide more often, driven largely by choice of more lethal means. Younger children can and do die by suicide — Bridge's study of elementary school-age children documented a stable but real incidence — so age alone never excludes risk. [4] [21]
The single strongest predictor of future suicide is a previous attempt. Repetition is also common after a self-harm presentation: hospital-presenting adolescents carry a materially elevated risk of repeat self-harm and of subsequent suicide death, which is why every self-harm presentation demands a structured psychosocial assessment rather than a treat-and-discharge. [10] [4]
The modifiable risk factors cluster into mental illness (depression, anxiety, post-traumatic stress, early psychosis), substance use, sleep deprivation, bullying, abuse and family conflict, recent loss or humiliation, and access to lethal means. Cybulski's nested case-control studies in UK primary care quantified these associations, with mental illness and self-harm history dominating. [9] [3]
Protective factors matter as much as risk factors. Connected relationships with family, school and peers, engagement with care, future orientation, effective coping, reasons for living, and restricted access to lethal means all lower the probability that ideation becomes action. Your assessment weighs both sides. [4] [15]
Pathophysiology
There is no single "suicide gene" and no blood test for risk. The working model is the stress-diathesis framework: a pre-existing vulnerability (the diathesis) meets a proximal stressor, and the balance between risk and protective factors determines whether ideation progresses to a plan, intent and an act. [4]
Distal vulnerability is built from the risk factors above. A prior attempt rewires the psychological barrier to self-harm, making repetition more likely. Depression and other mental illnesses distort cognition toward hopelessness and entrapment. Abuse, bullying and family conflict load chronic stress. Sexual and gender minority youth, Indigenous youth and those in out-of-home care carry elevated exposure to these drivers. [4] [9]
Proximal triggers are the acute events that convert vulnerability into crisis: a relationship breakdown, a disciplinary or legal crisis, public humiliation, intoxication, or sudden access to lethal means. Intoxication is doubly dangerous because it both increases impulsivity and impairs the judgement that would otherwise restrain an act. [3] [4]
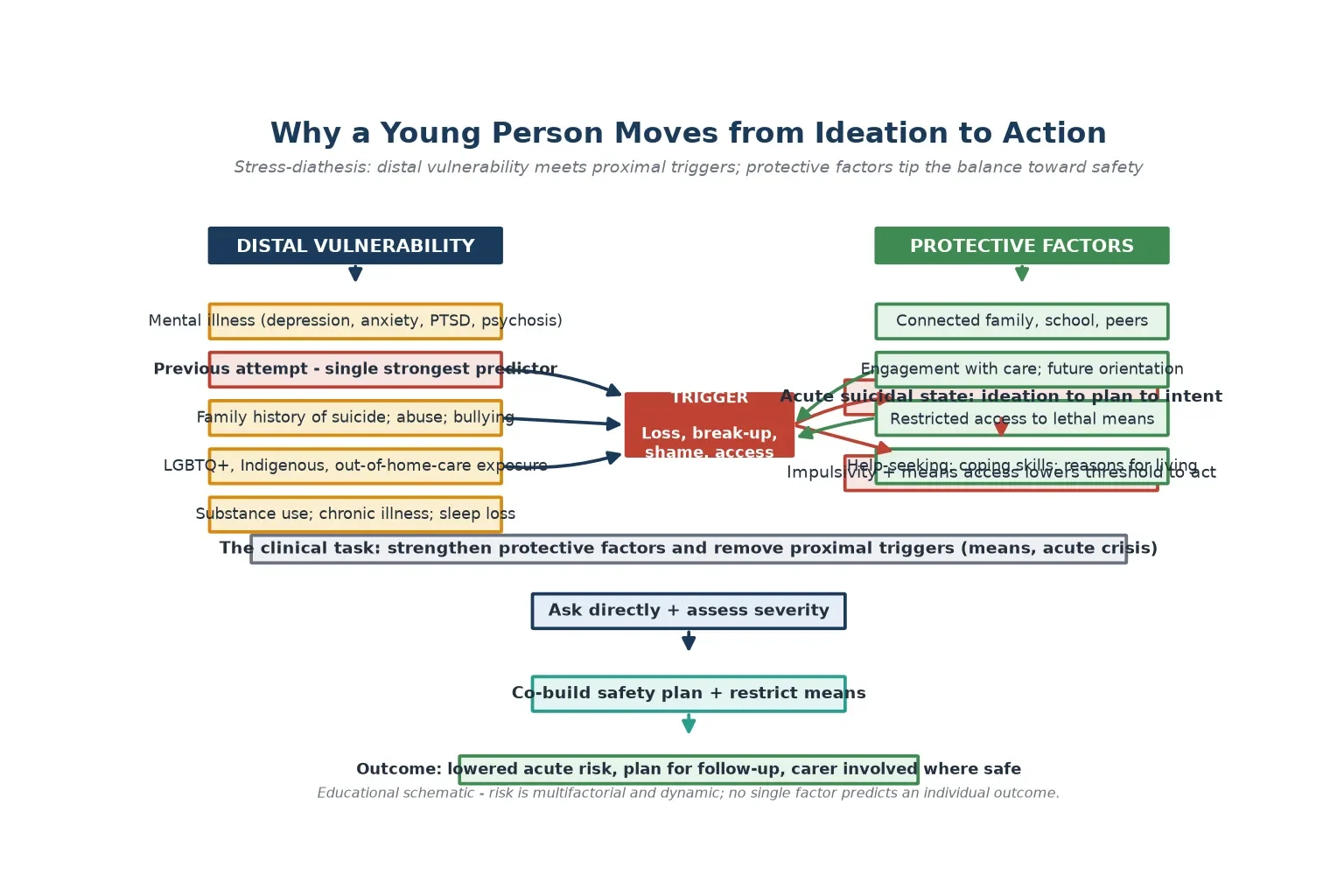
Read the figure like this: the lever you can pull fastest is means access. You cannot undo a history of abuse by tomorrow, but you can secure a firearm, lock away medications and remove ligature points tonight — and that single act can be life-saving during the narrow window of an acute crisis. [13] [14]
Why NSSI develops is partly understood through its function. Rasmussen and Hawton showed that adolescents most often self-harm to regulate an intolerable affect — to relieve tension, to feel something when numb, or to signal distress. Nock's review frames self-injury as a maladaptive coping strategy that is reinforcing because it works in the short term, which explains its repetition. Understanding the function guides which alternative coping skills you build into the safety plan. [8] [7]
Clinical Presentation
Suicidality rarely arrives labelled. It surfaces as small moments inside an ordinary consultation, an emergency presentation, or a school referral. [3]
The overt presentation is a self-harm act — an overdose, a laceration, a ligature mark — brought by family, school or ambulance. Here the task is to assess medical stability first, then assess intent and current risk. Never assume that a "minor" overdose reflects minor intent. [2] [3]
The disclosed presentation is a young person who tells you, often quietly, that they have been thinking about dying. This may come during screening, during a HEADSS or psychosocial history, or in response to a direct question. Treat every disclosure as credible until assessed. [11] [12]
The behavioural presentation is harder to see. Withdrawal from friends and activities, giving away possessions, a sudden calm after despair, researching methods online, increased substance use, or a sudden deterioration in chronic illness self-management can all signal rising risk. None is specific; together they warrant a direct conversation. [3] [4]
The screening-detected presentation is increasingly common as universal screening spreads into primary care and emergency settings. A positive ASQ or depression-and-suicide-risk screen flags a young person who needs a full structured assessment, not a reflexive referral and discharge. [2] [12] [11]
Differential Diagnosis
In this topic the differential is "what is driving this presentation, and what else must I exclude before I stratify risk." [4]
| What it looks like | The real question to answer | Do not miss |
|---|---|---|
| Self-harm "for attention" | NSSI with a real affect-regulation function | Co-existing suicidality, depression |
| "Minor" overdose | What was the intent, and is it still present? | Access to further means, repeat risk |
| Sudden calm after distress | Resolution, or deciding on a plan? | Impending attempt |
| Agitation and threats | Acute behavioural disturbance vs suicidal crisis | Intoxication, psychosis, means access |
| "Just anxious" adolescent | Is anxiety or depression driving suicidal ideation? | Untreated mood or trauma disorder |
| Refusal to engage | Fear, shame, or unmet safety need? | Abuse, coercion, ongoing risk |
Separate NSSI from suicidal self-harm by asking about intent directly. The method tells you about lethality and means access; it does not reliably tell you intent. A young person who took six paracetamol tablets to punish a parent may have had no intent to die, while one who took a non-lethal dose believing it was lethal may have had full intent. Ask. [7] [18]
Separate acute intoxication from baseline mental state. Alcohol and other substances both disinhibit behaviour and impair the capacity judgement that underpins discharge decisions. Re-assess once the young person is sober. [3] [4]
Clinical & Bedside Assessment
1. Build rapport and set the frame
See the young person in a private space. State conditional confidentiality honestly: what you discuss stays private unless you are worried they are not safe, and if that happens you will tell them what you must share and why. Direct, kind questioning does not increase risk. [2] [3]
2. Ask directly about suicidal ideation
Use a normalising, stepwise approach: "Sometimes when people feel overwhelmed, they have thoughts of hurting themselves or of not wanting to be alive. Has anything like that crossed your mind?" If yes, move to frequency, intensity, duration and recency. [1] [2]
3. Assess plan, intent and means access
If ideation is present, ask whether they have thought about how, whether they intend to act, and whether they have access to the means. The C-SSRS structures this precisely. A specific plan with intent and means access is high or imminent risk regardless of how the young person minimises it. [1] [3]
4. Take the precipitant and history
What happened in the hours and days before? What was the function of any self-harm? Is there a history of previous attempts — the strongest single risk factor? Screen for depression, anxiety, trauma, psychosis, substance use and sleep. [4] [9]
5. Assess protective factors
Ask about family, friends, school engagement, reasons for living, future plans and current help-seeking. Protective factors do not cancel acute risk, but they inform the safety plan and the disposition. [4] [15]
6. Involve carers and gather collateral
With the young person's agreement (or under a safety override where risk is high), involve a trusted carer. Collateral history from family and school often changes the risk picture. Carers are also the agents of means restriction and of overnight safety. [3] [13]
7. Stratify risk and co-build the safety plan
Weigh the C-SSRS dimensions against protective factors into low, moderate, high or imminent risk. Then co-build a written Stanley-Brown safety plan with the young person. Document the reasoning, the plan, and the disposition. [1] [15]
Investigations
There are no laboratory tests for suicide risk. The "investigations" here are structured assessment tools, collateral, and the medical work-up of any self-harm presentation. [1]
Medical assessment of the act. For an overdose, calculate the timing, agent and dose, check paracetamol and salicylate levels where indicated, and assess for medical instability. For lacerations, manage the wound and check for nerve or tendon injury. Medical stability comes before psychiatric disposition. [3]
Structured screening tools make direct questioning safe and reproducible. The C-SSRS assesses ideation severity, intensity and behaviour across the dimensions that predict near-term risk. The ASQ is a four-to-six-item tool validated for paediatric emergency departments and now adapted for inpatient and primary care settings. A positive screen triggers a full assessment, not a diagnosis. [1] [2] [11]
Universal screening is moving into primary care. Kemper's study of depression and suicide-risk screening in paediatric primary care found a meaningful yield of positive screens, and Horowitz documented the practical realities of implementing routine suicide-risk screening in a busy primary care setting. Screening is now a standard-of-care expectation in many systems. [12] [11]
Collateral information from parents, school and any mental-health services is an investigation in its own right. It frequently surfaces prior attempts, access to means, or recent precipitants the young person did not disclose. [4] [3]
C-SSRS dimensions to cover at every assessment
Management — Resuscitation
A self-harm presentation can be a medical emergency before it is a psychiatric one. [3]
- Stabilise the patient first. ABCDE; treat the overdose (N-acetylcysteine for paracetamol toxicity per local protocol), control any haemorrhage, manage intoxication and any airway or consciousness threat. [3]
- Keep the young person safe during the medical work-up. Do not leave a high-risk young person unattended. Remove access to means within the department, including sharps and medications. [2] [14]
- Re-assess mental state once medically stable and sober. Acute intoxication and medical instability both distort the risk assessment. The disposition decision is made on the settled picture, not the acutely intoxicated one. [3] [4]
In a psychiatric emergency where a young person is imminently at risk and cannot be kept safe, use your local mental-health and capacity law to provide care in their best interests, then return to collaborative planning as soon as they can engage. [3]
Management — Definitive & Stepwise
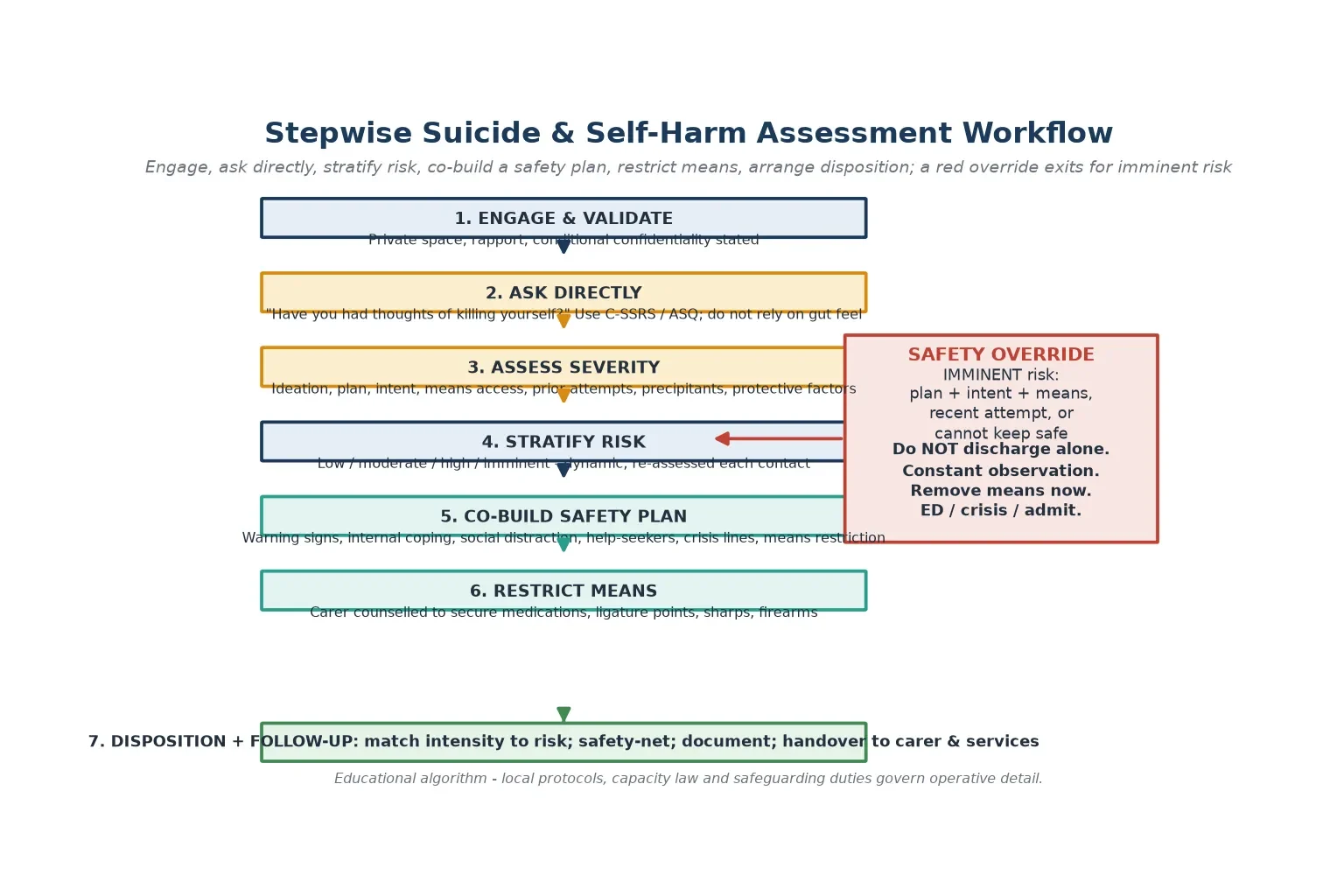
Read the figure like this: the override is a branch, not a failure of the assessment. Entering it is the correct response when plan, intent and means converge. [2] [3]
The routine assessment-to-disposition pathway
- Engage and validate in a private space with conditional confidentiality stated. [2]
- Ask directly about ideation, then plan, intent, means access and prior attempts using the C-SSRS dimensions. [1]
- Stratify risk as low, moderate, high or imminent, weighed against protective factors. [1] [4]
- Co-build a written safety plan with the young person (below). [15]
- Deliver means restriction counselling to the young person and their carer. [13] [14]
- Arrange disposition and follow-up matched to risk. [3]
The Stanley-Brown safety plan
The safety planning intervention is a brief, collaborative, written tool co-built with the young person. Albaum's 2025 systematic review and meta-analysis of safety planning in children and adolescents found evidence supporting its use in reducing suicide-related outcomes, making it one of the highest-value brief interventions available. A safety plan moves through these steps in the young person's own words. [15]
- Recognise warning signs — the thoughts, feelings, situations or times that signal a crisis is building. [15]
- Use internal coping strategies — things the young person can do alone to distract from suicidal thoughts. [15]
- Use social contacts and settings for distraction — places or people that pull attention away from the crisis. [15]
- Reach out to people for help — named family or friends the young person will contact. [15]
- Contact crisis and professional lines — the local mental-health crisis number and emergency services. [15]
- Make the environment safe — restrict access to lethal means, the bridge between the plan and an act. [13] [15]
Means restriction counselling
Restricting access to lethal means during a suicidal crisis saves lives because the impulse is often brief and method-specific. Bandealy documented that lethal means restriction counselling remains under-used in paediatric primary care despite its evidence base, and Siry mapped the barriers emergency clinicians face in delivering it. Your job is to counsel the carer concretely: secure or remove firearms, lock away medications (including over-the-counter paracetamol), secure sharps, and address ligature points. Name the carer as the agent of this safety step. [13] [14]
Follow-up intensity
- Low risk: safety plan, means restriction, routine mental-health or general-practitioner follow-up. [15]
- Moderate risk: safety plan, means restriction, urgent mental-health review within 24 to 72 hours, same-day carer involvement. [3]
- High or imminent risk: do not discharge alone; constant observation, crisis or emergency pathway, admit if the young person cannot be kept safe in the community. [2] [3]
Specific Subtypes & Scenarios
The young person who self-harms without suicidal intent (NSSI). Assess the function of the behaviour, screen for co-existing suicidal ideation, and build alternative coping skills into the safety plan. Do not reassure yourself or the family that NSSI is harmless — it raises lifetime suicide risk and predicts repetition. [7] [8]
The recent high-lethality attempt. Treat this as high or imminent risk regardless of how composed the young person now appears. Remove access to the method used, maintain observation, and involve mental-health services before any discharge decision. A perceived-calm state after a serious attempt is a red flag, not a reassurance. [3] [10]
The young person who cannot guarantee their safety. When asked, "Can you keep yourself safe until I see you next?" an honest "no" is the single most important piece of information in the encounter. It overrides moderate-risk features and pushes toward admission or intensive community crisis support. [2] [3]
Intoxicated or agitated young person. Assess capacity and risk once medically stable and sober. Acute intoxication both raises immediate risk and invalidates a capacity assessment made during it. Use de-escalation and, where necessary, local mental-health and sedation protocols for acute behavioural disturbance. [3] [4]
Younger child with suicidal ideation. Suicide does occur in pre-adolescent children. Adapt your language, involve parents directly, and recognise that family conflict, bullying and abuse are common drivers in this group. [4]
Chronic or repeated self-harm. Repetition is the rule rather than the exception after a self-harm presentation. Dialectical behaviour therapy for adolescents has randomised-trial evidence for repeated self-harm and suicidality, and a meta-analysis confirms its benefit. Ougrin's therapeutic assessment model also reduces repetition compared with routine psychosocial assessment. Plan for longer-term structured treatment, not serial crisis visits. [10] [16] [17] [18]
The young person in the emergency department after universal screening. A positive ASQ screen in a medical patient triggers a full risk assessment and disposition decision, even if the presenting complaint was unrelated. Brahmbhatt's clinical-pathway work frames how paediatric hospitals systematise this. Do not let a positive screen drift into discharge without assessment. [2] [11]
Complications & Pitfalls
- Discharging on a gut feeling of "low risk" without structured assessment of plan, intent and means. [1] [3]
- Treating a "minor" overdose as minor intent — lethality is not intent. [3] [18]
- Reassuring the family that NSSI is harmless when it predicts future suicide risk. [7] [10]
- Failing to remove means, or counselling means restriction in the abstract without naming the carer as the agent. [13] [14]
- Reassuring a suddenly calm, despairing young person instead of re-assessing for an impending attempt. [3] [4]
- Discharging before the young person is medically stable and sober. [3]
- Treating a single risk level as a fixed label rather than re-assessing at every contact. [1] [4]
- Sending a young person home with no written safety plan and no follow-up appointment. [15]
- Promising absolute secrecy when risk is high, then breaching it without explanation. [2] [3]
- Forgetting that carer mental illness, family violence or access to a firearm changes the whole risk picture. [4] [13]
Prognosis & Disposition
In this topic, prognosis means the trajectory of risk over the hours, days and weeks after the contact, not a disease stage. [3]
Routine disposition: passive or low-severity ideation, no plan or intent, strong protective factors, and a young person who can keep themselves safe. Provide a written safety plan, means restriction, and routine follow-up. [15]
Urgent disposition: active ideation with a forming plan, ambivalent intent, or incomplete assessment. Co-build a safety plan, deliver means restriction, involve the carer, and arrange mental-health review within 24 to 72 hours. [3] [15]
Emergency disposition: plan plus intent plus means access, a recent high-lethality attempt, inability to keep safe, or acute intoxication with suicidality. Use the crisis or emergency department pathway the same day, maintain observation, remove means, and admit if the young person cannot be kept safe in the community. [2] [3]
Safety-net explicitly: who to call tonight, when to come back sooner, and how confidentiality will work with carers after any override. Repeat self-harm and suicide death risk persists for months after a hospital presentation, so close the loop after any mental-health referral and confirm the follow-up happened. [10] [3]
Over the longer term, structured treatments change the prognosis. Dialectical behaviour therapy for adolescents reduces repetition in those with repeated self-harm, and therapeutic assessment reduces repetition after a self-harm presentation. The evidence base for self-harm interventions in young people continues to consolidate through Cochrane and individual-patient-data syntheses. [16] [18] [19] [20]
Special Populations
LGBTQ+ youth. Minority stress, family rejection and bullying drive elevated suicide risk. Offer an affirming, confidential space, use the young person's chosen name and pronouns, and assess carefully — this group is over-represented among suicidal adolescents for reasons that are largely environmental and modifiable. [3] [4]
Indigenous adolescents. Suicide rates are elevated in many Indigenous communities, reflecting intergenerational trauma, socioeconomic disadvantage and barriers to culturally safe care. Use local pathways and culturally safe services, and recognise cultural connection as a protective factor. [4]
Out-of-home care and youth justice. These young people carry high cumulative adversity, fragmented records and elevated mental-health and self-harm risk. Reconstruct the history actively, clarify consent authority, and assume higher baseline risk. [4] [3]
Migrant and refugee youth. Use trained interpreters, never family members, for sensitive content. Trauma, acculturation stress and interrupted care all raise risk. [4]
Disability and neurodiversity. Adapt communication to ability and watch for the diagnostic overshadowing that misses depression behind a disability. Autistic young people may express distress differently; ask concretely and patiently. [4]
Rural and remote. Distance to services, small-community dual relationships and firearm access all shape risk. Means restriction is especially high-yield here, and telehealth crisis follow-up can bridge distance. [4] [13]
Chronic illness. Chronic disease and its burden on identity, peer life and future plans raise suicide risk. Screen proactively and integrate mental-health care into the chronic-illness clinic rather than referring out and losing touch. [4]
Evidence, Guidelines & Regional Differences
The structured-assessment evidence base. Posner's C-SSRS validation established a common language for severity that is now used worldwide. Horowitz's ASQ gave paediatric emergency departments a brief, validated screening tool, and her implementation work showed how screening moves from research into routine primary care. Kemper documented the yield of depression and suicide-risk screening in paediatric primary care. [1] [2] [11] [12]
The epidemiology. Bridge and Brent's review frames adolescent suicide and suicidal behaviour; Liu's meta-analysis quantified the prevalence and correlates of suicide and NSSI in children; and Gillies's meta-analysis mapped self-harm prevalence in adolescents across community studies. Cybulski's nested case-control studies quantified the risk factors, and Qian documented repeat and suicide-death risk after hospital self-harm presentation. [4] [5] [6] [9] [10]
The treatment evidence. The Albaum meta-analysis supports safety planning in children and adolescents. Mehlum's randomised trial and Kothgassner's meta-analysis underpin dialectical behaviour therapy for repeated self-harm, while Ougrin's therapeutic-assessment work and the Witt Cochrane review and the Cottrell RISA individual-patient-data synthesis map the broader intervention evidence. [15] [16] [17] [18] [19] [20]
Means restriction. Bandealy and Siry document that lethal means counselling is evidence-based yet under-delivered in primary care and emergency settings — a clear quality-improvement target. [13] [14]
ANZ: headspace and state child and adolescent mental-health services (CAMHS) provide community and crisis pathways; the Royal Children's Hospital Melbourne clinical practice guidelines frame assessment. The mature-minor principle governs consent; mandatory-reporting duties for serious risk apply. Use trained interpreters for language needs. UK: NICE NG225 (2022) on self-harm assessment, management and preventing recurrence sets the standard for psychosocial assessment after every self-harm presentation; the Royal College of Psychiatrists CR204 frames child and adolescent practice. Gillick competence governs consent for under-16s. US: the AAP clinical report on suicide and suicide attempts in adolescents (Shain) frames practice; the ASQ toolkit is widely used for universal screening. Means restriction counselling focuses on firearms and medications; local mental-health and capacity law varies by state. Canada: provincial mental-health and crisis services vary; Greig Health Record and CPS guidance frame preventive care. Check the relevant province for crisis pathways and consent law.
State the principle — ask directly, stratify honestly, plan collaboratively, restrict means, follow up — and check local law and protocols. Do not invent universal thresholds or admission criteria, because they do not exist. [1] [3]
Exam Pearls
- Open every answer with ask directly, stratify, plan, restrict means, follow up. [1] [3]
- A previous attempt is the single strongest predictor of future suicide. Treat every self-harm presentation as serious until assessed. [10] [4]
- Lethality is not intent. A low-medical-lethality act can carry high intent. Ask about intent directly. [18] [3]
- NSSI is not harmless. It predicts future suicide risk and repetition; do not reassure it away. [7] [10]
- Stratify with ideation, plan, intent, means access, prior attempts, weighed against protective factors (the C-SSRS dimensions). [1]
- Means restriction saves lives because suicidal impulses are often brief and method-specific. Name the carer as the agent. [13] [14]
- A safety plan is co-built, written, and moves from warning signs through coping, social distraction, help-seekers, crisis lines, and means restriction. [15]
- Imminent risk = plan plus intent plus means, or inability to keep safe. Do not discharge alone. [3] [2]
- Re-assess at every contact; risk is dynamic, not a fixed label. [1] [4]
- Dialectical behaviour therapy for adolescents has trial evidence for repeated self-harm; therapeutic assessment reduces repetition. [16] [18]
IPIMH — the five C-SSRS dimensions
References
- [1]Posner K The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. The American journal of psychiatry, 2011.PMID 22193671
- [2]Horowitz LM Ask Suicide-Screening Questions (ASQ): a brief instrument for the pediatric emergency department. Archives of pediatrics & adolescent medicine, 2012.PMID 23027429
- [3]Shain B Suicide and Suicide Attempts in Adolescents. Pediatrics, 2016.PMID 27354459
- [4]Bridge JA Adolescent suicide and suicidal behavior. Journal of child psychology and psychiatry, and allied disciplines, 2006.PMID 16492264
- [5]Liu RT Prevalence and Correlates of Suicide and Nonsuicidal Self-injury in Children: A Systematic Review and Meta-analysis. JAMA psychiatry, 2022.PMID 35612875
- [6]Gillies D Prevalence and Characteristics of Self-Harm in Adolescents: Meta-Analyses of Community-Based Studies 1990-2015. Journal of the American Academy of Child and Adolescent Psychiatry, 2018.PMID 30274648
- [7]Nock MK Self-injury. Annual review of clinical psychology, 2010.PMID 20192787
- [8]Rasmussen S Why Do Adolescents Self-Harm? Crisis, 2016.PMID 26831210
- [9]Cybulski L Risk factors for nonfatal self-harm and suicide among adolescents: two nested case-control studies conducted in the UK Clinical Practice Research Datalink. Journal of child psychology and psychiatry, and allied disciplines, 2022.PMID 34862981
- [10]Qian J Risk of repeat self-harm and suicide death following an episode of hospital self-harm presentation among adolescents and young adults. Journal of affective disorders, 2023.PMID 36280199
- [11]Horowitz LM Implementing Suicide Risk Screening in a Pediatric Primary Care Setting: From Research to Practice. Academic pediatrics, 2022.PMID 35248306
- [12]Kemper AR Depression and Suicide-Risk Screening Results in Pediatric Primary Care. Pediatrics, 2021.PMID 34099503
- [13]Bandealy A Use of lethal means restriction counseling for suicide prevention in pediatric primary care. Preventive medicine, 2020.PMID 31644896
- [14]Siry BJ Lethal means counseling for suicide prevention: Views of emergency department clinicians. General hospital psychiatry, 2021.PMID 33971519
- [15]Albaum C Safety Planning Interventions for Suicide Prevention in Children and Adolescents: A Systematic Review and Meta-Analysis. JAMA pediatrics, 2025.PMID 40388177
- [16]Mehlum L Dialectical behavior therapy for adolescents with repeated suicidal and self-harming behavior: a randomized trial. Journal of the American Academy of Child and Adolescent Psychiatry, 2014.PMID 25245352
- [17]Kothgassner OD Efficacy of dialectical behavior therapy for adolescent self-harm and suicidal ideation: a systematic review and meta-analysis. Psychological medicine, 2021.PMID 33875025
- [18]Ougrin D Adolescents with suicidal and nonsuicidal self-harm: clinical characteristics and response to therapeutic assessment. Psychological assessment, 2012.PMID 21859219
- [19]Witt KG Interventions for self-harm in children and adolescents. The Cochrane database of systematic reviews, 2021.PMID 33677832
- [20]Cottrell D Reducing self-harm in adolescents: the RISA-IPD individual patient data meta-analysis and systematic review. Health technology assessment (Winchester, England), 2024.PMID 39024118
- [21]Bridge JA Suicide Trends Among Elementary School-Aged Children in the United States From 1993 to 2012. JAMA pediatrics, 2015.PMID 25984947