Paeds · mental-behavioural-and-psychosomatic
Children of parents with mental illness or substance use
Also known as COPMI — children of parents with a mental illness · Parental mental illness and offspring risk · Parental substance use and child outcomes · Intergenerational transmission of mental disorder · Young carers of mentally ill parents
Fellowship guide to the child of a parent with mental illness or substance use: a heightened but probabilistic — never deterministic — risk-and-need picture driven by gene-environment interplay, the Rutter / Reiss / Gotlib transmission evidence, the offspring-risk data by parental disorder (Weissman STAR*D-child; Rasic), and stepped two-generational, family-focused care whose non-negotiables are treating the parent, assessing the child in their own right, safeguarding when thresholds are met, and a closed loop — across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A mother with treatment-resistant depression brings her eight-year-old, who has started missing school, complains of tummy aches, and has begun "looking after Mum." The question for the paediatrician is not whether to diagnose the child — he may be perfectly well — but whether this family carries risk that early, two-generational support can redirect. That is the framing this topic demands: risk and need, searched for early, not a label applied automatically. [1] [6]
Children of parents with mental illness or substance use are the population whose parent or primary caregiver has a mental disorder — depressive, bipolar, schizophrenia-spectrum, anxiety, trauma-related, or a substance use disorder — and who therefore stand a measurably higher chance of developing an emotional or behavioural disorder themselves. Michael Rutter's 1984 work established the foundational point that parental psychiatric disorder has real effects on children, and forty years of evidence since has refined that blunt truth into something a fellowship candidate must hold precisely: the risk is real, it is heightened, it runs through gene-environment interplay, and it is absolutely not destiny. [1] [5]
Two reframes are essential. First, this is a risk-and-need picture, not a diagnosis of the child. Most children of affected parents do not develop disorder; a resilient majority thrive with adequate support, and labelling a well child from parental history alone is a serious error. Second, the parent's illness is never blame. A mental illness or substance use disorder is a health condition that impairs, at times profoundly, the caregiving environment — and the clinician who approaches the family with stigma or accusation drives them away from exactly the help that changes the trajectory. [1] [14]
The deep diagnosis and treatment of the child's own depressive or anxiety disorder lives on those leaves; the adolescent's own substance use on its leaf; acute self-harm risk on the suicide-and-self-harm leaf; and the forensic child-protection pathway on the safeguarding leaf. This page owns the recognition, risk-assessment, and two-generational, family-focused spine that runs from "is there a child at risk here?" to closed-loop care. [14]
Classification
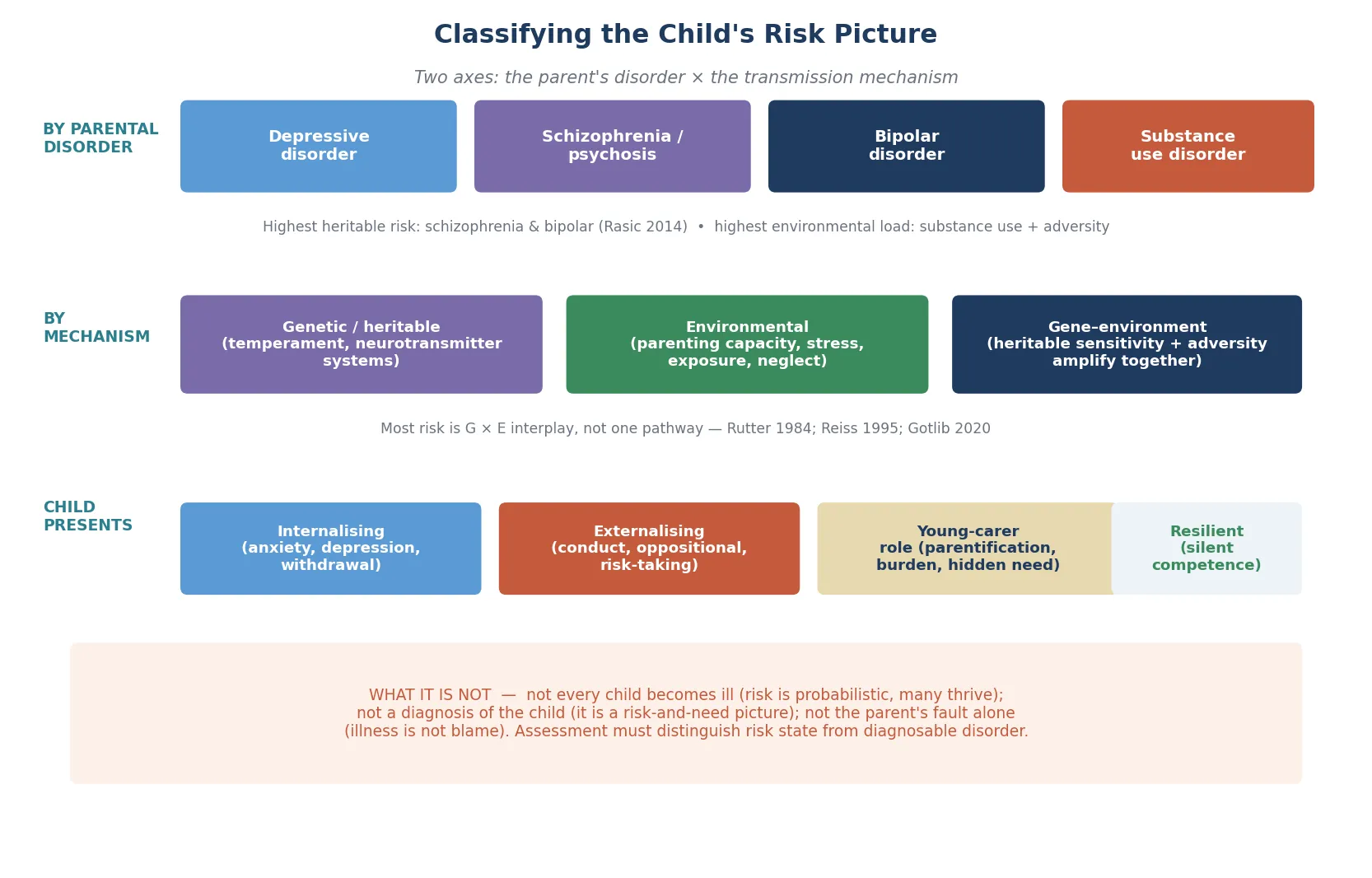
Classify along three axes before you decide what to do: which parental disorder is in the home, what mechanism carries the risk to the child, and what the child is showing you right now. The same parental illness means something different paired with a stable second carer and a supportive school than it does in isolation and chaos. [1] [5]
By parental disorder
| Parental disorder | Risk character | Dominant load |
|---|---|---|
| Depressive disorder | Commonest affected parent in practice; strong family-focused-prevention evidence | Mixed — heritable + caregiving |
| Schizophrenia / psychosis | Highest heritable offspring risk | Strongly heritable + stigma/secrecy |
| Bipolar disorder | High heritable risk; episodic caregiving disruption | Heritable + episodic chaos |
| Substance use disorder | High environmental-adversity burden | Strongly environmental + possible prenatal exposure |
The Rasic systematic review showed that offspring of parents with schizophrenia, bipolar disorder, and major depressive disorder all carry a markedly higher risk of mental illness than the general population — but the flavour of risk and the environmental load differ by disorder, which matters when you plan. [4]
By transmission mechanism
Risk travels to the child through three intertwined pathways that you should never try to separate into "nature or nurture." Heritable vulnerability (temperament, stress-response set-points, neurotransmitter systems) sets a probabilistic baseline; the caregiving environment (parenting capacity, responsiveness, consistency, the effect of symptoms like withdrawal or irritability) mediates how that vulnerability is expressed; and gene-environment interplay means the two amplify or buffer each other. Reiss's work on the non-shared environment showed that even siblings in the same family differ — differential parenting and differential experience shape who crosses the threshold into disorder. [3] [5]
Heritable vulnerability versus caregiving environment
- Temperament, stress-response set-points
- Probabilistic, not deterministic
- Amplified by adversity, buffered by support
- Cannot be changed directly — but its expression can
- Parenting capacity, responsiveness, consistency
- Impaired by untreated illness, substance use, chaos
- Restored by parental treatment and remission
- This is where the clinician intervenes
Epidemiology & Risk Factors
The overlap between adult and child mental-health need is large and bidirectional. Campbell and colleagues found that a high proportion of parents of children receiving treatment within child and adolescent mental-health services have a mental illness themselves — which means the paediatrician seeing a child in CAMHS is, very often, also seeing a family with an affected parent who has their own unmet need. [13]
The offspring-risk data are striking but must be held with the resilience qualifier. The Rasic systematic review showed that offspring of parents with schizophrenia, bipolar disorder, and major depression carry a markedly higher risk of mental illness than the general population, with the highest heritable load in schizophrenia and bipolar. Yet the foundational Rutter message holds: this is heightened probability, and many — most — exposed children do not develop disorder. The candidate who quotes only the risk and omits the resilience half has mis-stated the epidemiology. [1] [4]
What amplifies risk from "heightened" toward "disorder"? Severity and chronicity of the parent's illness, untreated illness, comorbid substance use, frequent relapse and hospitalisation, family violence, socioeconomic disadvantage, and isolation all compound the genetic baseline. Parental substance use carries a particularly heavy environmental-adversity burden — household chaos, inconsistency, neglect features, possible prenatal exposure, and elevated maltreatment risk — which is why a substance-using parent shifts the whole assessment toward safeguarding. [1] [8]
The protective forces point the other way and are the entire basis for intervention: parental treatment and remission, a stable and warm second parent or carer, responsiveness and consistency, a connection to school, one trusted adult outside the home, and social support. A transdiagnostic meta-analysis confirms that offspring risk is real and persists across disorders, yet remains modifiable — which is the whole argument for not waiting. [6] [14]
Pathophysiology
Picture the eight-year-old again. For years, Mum's face has, at times, gone flat and unreachable; her responses have been slow or absent; the house has swung between stillness and crisis. The child has learned that need does not reliably produce comfort, and that his job is sometimes to hold the household together. Risk encoded in that kind of early environment is not "psychological" in any dismissive sense — it is calibrated into the developing stress-response and emotional-regulation systems. [1] [5]
The mechanism is best understood as gene-environment interplay rather than a nature-or-nurture contest. Heritable vulnerability supplies a probabilistic baseline; the caregiving environment mediates how, and how severely, that vulnerability is expressed; and the two amplify or buffer one another across development. Gotlib's programme of work argues that intergenerational transmission can only be understood prospectively and mechanistically — following mother-child pairs over time and measuring the biological and relational mediators — because the static, retrospective study cannot disentangle them. [5]
Three downstream channels carry the calibrated risk to the child. The stress-response system (the HPA axis and cortisol pattern) develops atypically when early distress meets inconsistent care; emotional-regulation and attachment learning is shaped by the quality of the caregiving loop; and a cognitive model forms around the illness — self-blame, guilt, the conviction that "Mum being ill is my fault," and hopelessness about change. These are precisely the mediators that family-focused prevention targets. [5] [11]
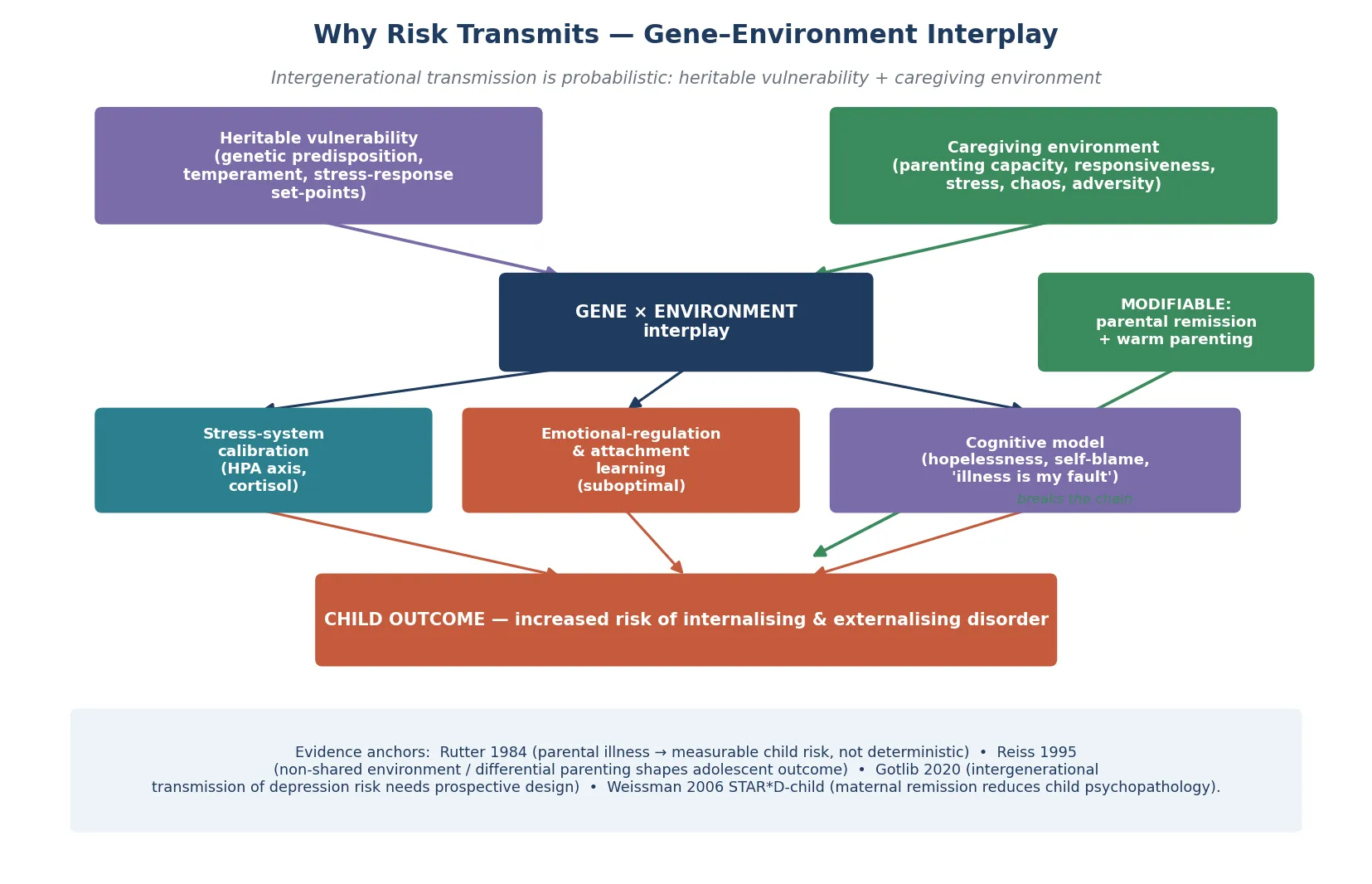
The hopeful corollary, and the reason this whole topic is an intervention topic rather than a fatalism topic, is that the caregiving environment is the modifiable mediator. Weissman's STAR*D-child data showed that when a mother's depression remitted, her child's psychopathology fell — treating the parent measurably treats the child. That single finding is the mechanistic and ethical basis for two-generational care. [7]
Clinical Presentation
Children rarely present with "I am the child of a depressed parent." They present with the downstream signal, and your history converts it. A young child may show clinginess, regression, withdrawal, irritability, behavioural dysregulation, or somatic complaints. A school-age child may show anxiety, school refusal or underachievement, low self-esteem, peer difficulty — or the quiet, over-mature competence of a young carer who has learned to manage the household. An adolescent may show depression, anxiety, risk-taking, emerging substance use, or self-harm, often layered with parentification and role-reversal that the family conceals as "being helpful." [1] [6]
The parental disorder shapes the flavour. Parental depression tends to produce the withdrawn, inconsistent-caregiving picture; parental substance use produces chaos, inconsistency, neglect features, and possible prenatal exposure effects; parental psychosis produces fear, confusion, secrecy, and bizarre-content exposure that can frighten a child; and a parent who is hospitalised produces a discontinuity that the child experiences as abandonment unless it is explained. [1] [8]
A "silent competence" presentation is the one most easily missed: the child who copes, who is praised for being mature, who is in fact absorbing a load that is eroding their development. Always gather the school's and the other carer's view, because the family system tends to under-report and the school tends to see the cost first. And always ask about safeguarding — neglect, family violence, parental suicidality, and exposure to intoxication or psychosis-driven harm are embedded in the presentation, not volunteered. [1] [13]
Differential Diagnosis
Build the differential in layers: the child's own emergent disorders, the relational and trauma states, the safeguarding categories, and — crucially — wellness. [1] [6]
| Pattern | Favours | Against / distinguish |
|---|---|---|
| Child's own depressive / anxiety / adjustment disorder | Persisting internalising symptoms meeting criteria | Treat the disorder on its own merits, alongside the family work |
| Conduct / oppositional disorder or risk-taking | Externalising behaviour, often in a substance-use home | Assess directly; do not write it off as "the family" |
| Attachment / relational-trauma state | Pathogenic care present | Cross-link the attachment leaf; relationship-based care |
| Child maltreatment / neglect / family violence | Impaired capacity causing harm | A safeguarding pathway, not a mental-health differential |
| Effects of prenatal substance exposure (FASD spectrum) | Characteristic phenotype, history | Dedicated FASD assessment |
| Bereavement / grief | Parent has died (suicide, overdose) | Bereavement pathway layered onto risk work |
| Normal variation — a well, resilient child | No disorder despite the risk | Support and watchful waiting, not over-medicalisation |
The two errors examiners love to probe are mirror-images: labelling a well child from parental history (over-medicalisation, stigma), and missing an emergent child disorder by attributing its symptoms to "the family" (diagnostic overshadowing). When the child meets criteria for a disorder, treat that disorder on its own merits; when the child is well, support and watch — but never assume. [1] [6]
Clinical & Bedside Assessment
The assessment begins with a question that should be routine in every paediatric and adult mental-health encounter: does an affected adult have dependent children, and does a child in difficulty have an affected parent? This COPMI identification step is the gate through which everything else flows, and it is missed more often than it is asked. [14]
Two-generational assessment sequence
Identify and ask
Routinely ask whether an affected parent has dependent children, and whether a struggling child has an affected parent. Ask the child directly: 'Who cares for you when your parent is unwell?'
Family and parental-illness history
Parental diagnosis, treatment status, relapse pattern, substance use, hospitalisations, household composition, the protective second carer.
Assess the child in their own right
Emotional and behavioural functioning (internalising and externalising) with age-appropriate, multi-informant tools; developmental status; the young-carer role.
Assess caregiving capacity
Warmth, responsiveness, consistency, the effect of parental symptoms, and the presence of a protective adult — without blame.
Assess risk to the child
Neglect, family violence, parental suicidality, exposure to intoxication or psychosis-driven harm, maltreatment.
Formulate and plan
Risk-and-need picture versus diagnosable child disorder; safeguarding status; step of care; named owner and safety-net.
Standardised screens support, but never replace, clinical judgement. The Strengths and Difficulties Questionnaire (SDQ) and a brief parental-depression screen are the practical, multi-informant tools to detect emergent child disorder and unrecognised parental illness — use what is matched to the child's age and gather the parent's, the teacher's, and where possible the child's own view, because discordance is itself data. Always examine the child too: look for signs of neglect, faltering growth, untreated illness, or abuse that need their own medical and safeguarding pathway. [13] [14]
Investigations
This is a clinical risk-and-need assessment, not a test-positive diagnosis. There is no blood test, scan, or biomarker that confirms "risk" from a parental history, and the commonest investigation error is the shotgun panel ordered for "behaviour" in a child whose real need is a family assessment. Your core investigations are the structured family and parental-illness history, the standardised child emotional/behavioural screen, the developmental assessment, and the multi-informant view. [13] [14]
Investigate when the story points somewhere. Assess development directly when concern coexists, because parental illness and developmental delay can co-occur and each changes the plan. Where the parent's treatment status is unclear, clarifying it (with consent) matters because treatment optimisation is itself the child's intervention — coordinating with the adult team is an investigation in the service of the child. Screen actively for the comorbidities that change the plan — the child's own depression, anxiety, conduct disorder, and, in adolescents, substance use — because treating the family risk while ignoring an emergent child disorder is a common cause of non-response. [1] [14]
When maltreatment is disclosed or suspected, the safeguarding forensic assessment is a separate, protocolised pathway — arrange it through the local child-protection service, do not improvise it, and do not let a mental-health framing delay it. [1]
Management — Resuscitation
"Resuscitation" here means immediate child safety, confirmed caregiving arrangement, and an end to acute threat — not a drug, and not a therapy session. [1] [14]
Support the protective second parent, carer, or extended family explicitly — they are the immediate stabiliser and, often, the relationship that makes everything else possible. Recognise that no medication "resuscitates" a risk state; safety and stability are the resuscitation, and the rest of the plan follows once the child is safe tonight. [1] [14]
Management — Definitive & Stepwise
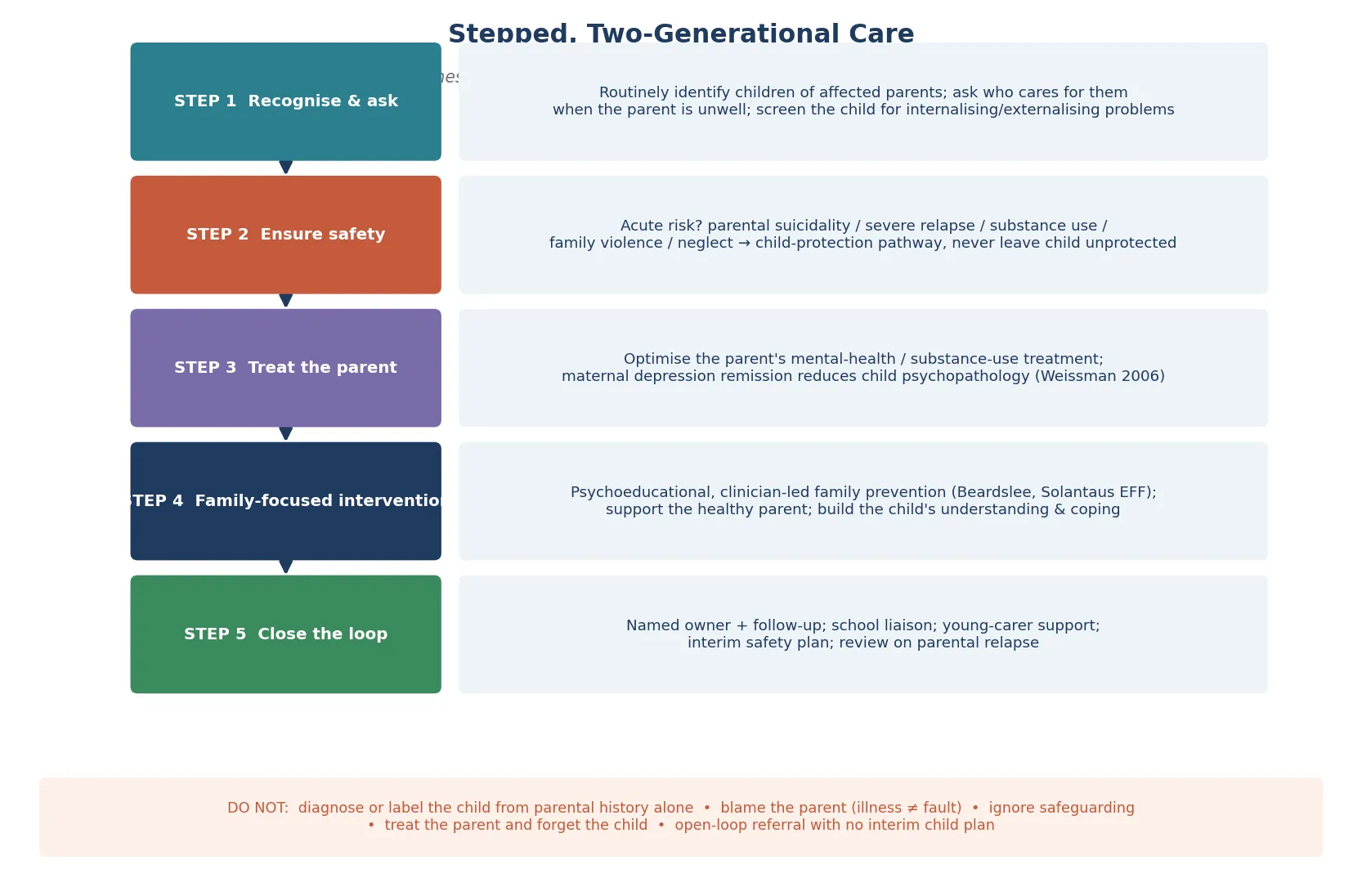
Two-generational, family-focused care is the frame, and the order matters as much as the content: recognise the child, ensure safety, treat the parent, deliver a family-focused intervention, and close the loop. [7] [14]
Step 1 — Recognise and ask
Routinely identify children of affected parents and screen the child for need. The single highest-yield question is "who cares for you when your parent is unwell?" — it surfaces the young carer, the hidden need, and the caregiving network in one breath. [13] [14]
Step 2 — Ensure safety
Address the immediate caregiving arrangement, run the safeguarding or crisis pathway where thresholds are met, and confirm that the child is safe tonight before any family work proceeds. [1]
Step 3 — Treat the parent
Optimise the parent's mental-health or substance-use treatment through the adult service. This is not a side-task for someone else — it is the child's intervention. The Weissman STAR*D-child finding is the evidence: when a mother's depression remitted, her child's psychopathology fell. Treating the parent measurably treats the child, which is the mechanistic and ethical core of two-generational care. [7]
Step 4 — Family-focused intervention
When safety and parental treatment are in train, deliver an evidence-supported family-prevention programme to the family, not the child alone. Beardslee's clinician-facilitated approach produced sustained change in parents and children in families with parental depression; Solantaus's Effective Family (EFF) intervention reduced children's psychosocial symptoms; and Punamäki's work showed that preventive family intervention improves children's cognitive attributions — directly attacking the self-blame and hopelessness that mediate risk. The active ingredient is the family, working together, with a clinician — not the child extracted for individual therapy. [9] [10] [11]
Step 5 — Support the protective carer and the child's understanding
Bolster the healthy second parent or carer, help the child build an age-appropriate understanding of the illness (so it stops being "my fault"), and secure at least one trusted-adult relationship outside the ill parent. The bidirectional evidence — Nestor showed that an adolescent depression-prevention programme reduced maternal criticism — underscores that intervening on either side of the dyad helps both. [12]
Step 6 — Close the loop
Name the clinician who owns the plan, fix a follow-up date, document an interim safety plan with return precautions (parental relapse, new disclosures, escalation of child symptoms), coordinate with school and the general practitioner, and arrange young-carer support. Do not "refer to CAMHS and forget" — an open-loop referral leaves a vulnerable child exposed. [13] [14]
When the child meets criteria for their OWN disorder — depression, anxiety, conduct — treat that disorder on its own merits, alongside the family work, and never let the family framing delay or substitute for the child's evidence-based treatment. [1] [6]
Specific Subtypes & Scenarios
Child of a parent with depression. The commonest scenario in practice and the one with the strongest family-focused-prevention evidence. Maternal remission reduces child psychopathology, and the Beardslee, Solantaus and Punamäki programmes are built for this family. Deliver family-focused prevention early; do not wait for the child to "develop something." [7] [9]
Child of a parent with schizophrenia or bipolar disorder. The highest heritable offspring risk; address the secrecy, stigma, and the fear-based cognitive model that forms when a child witnesses psychotic symptoms without explanation. Honest, age-appropriate explanation is itself protective. [4]
Child of a substance-using parent. The highest environmental-adversity burden. Assess for neglect, prenatal exposure (the FASD spectrum), household chaos, and maltreatment; coordinate actively with child-protection services where indicated; and recognise that substance use disorders carry episodic risk that demands a different, more safeguarding-weighted plan. [1]
The young carer. Identify parentification and hidden burden early; provide dedicated young-carer support; and protect the child's development and education, which the role quietly erodes. [14]
Child of a hospitalised parent. Ensure continuity of care, clarify and stabilise the caregiving arrangement, and support the child's understanding so that hospitalisation is experienced as treatment rather than abandonment. [1]
Adolescent of an affected parent. Screen for emerging depression, anxiety, substance use, and self-harm; deliver integrated dual-focus care that treats the adolescent's own risk alongside the family work. [6]
Child where the parent has died (suicide, overdose). Run a bereavement and grief pathway layered onto the risk work; these children carry both bereavement and the inherited risk picture. [1]
Infant of a mother with perinatal mental illness. Prioritise parent-infant relationship work and early intervention; the perinatal window is a high-leverage, time-sensitive opportunity. [5]
Resilient, well child of an affected parent. The presentation that must not be over-medicalised. Offer support and watchful waiting, protect the child from being labelled, and keep the door open — resilience is real, but it is not a reason to discharge and forget. [1] [6]
Complications & Pitfalls
- Labelling a well child from parental history alone — over-medicalisation and stigma. [1]
- Missing an emergent child disorder by attributing its symptoms to "the family" — diagnostic overshadowing. [6]
- Treating the parent and forgetting the child — never close the child's loop. [14]
- Failing to safeguard when parental illness, substance use, or family violence places the child at acute risk. [1]
- Blaming the parent — illness is never fault; stigma drives families away from help. [14]
- Open-loop referral to CAMHS with no interim child plan, no safety-net, no named owner. [13]
- Ignoring the young-carer role and hidden parentification. [14]
- Over-interpreting risk as deterministic and removing a child when capacity and safety are intact. [1]
- Failing to optimise the parent's treatment, which is itself the child's intervention. [7]
- Confidentiality errors: disclosing without consent, or failing to share when a child is at risk. [1]
Prognosis & Disposition
The prognosis is, by design, optimistic — because the modifiable lever is real. Most children of affected parents do not develop disorder; resilience is common with adequate support; and parental remission measurably reduces child psychopathology, which is the single clearest evidence that intervening on the family changes the child's trajectory. [1] [7]
Severity, chronicity, comorbidity, substance use, and the adversity load predict worse child outcomes; protective relationships and early family-focused prevention predict better ones. A transdiagnostic meta-analysis confirms the offspring risk persists across disorders yet remains modifiable — the argument against "wait and see" and for active, two-generational support. [6]
Disposition after safety confirmed: family-focused prevention via local CAMHS, early-intervention, or COPMI pathways, with medical-home interim support and developmental or comorbidity workup as indicated. [14] Disposition when a safeguarding concern surfaces: child-protection pathway, same-day supports, and stability before any family therapy. [1] Disposition for a child with an emergent disorder: treat that disorder on its own merits alongside the family work. [6]
Markers of response are improved child functioning, reduced internalising and externalising symptoms, parental stability, and restored caregiving capacity. Long CAMHS waitlists change the medical-home role: provide interim family support, safety planning, and school liaison rather than passive waiting. [13] [14]
Special Populations
Young carers carry a hidden burden that erodes development and education; identify them early, provide dedicated young-carer support, and protect schooling. Children in out-of-home care of an affected parent need the carer supported as the intervention, with attachment and developmental impact assessed in parallel. Infants of mothers with perinatal mental illness are a high-leverage, time-sensitive window for parent-infant relationship work. [5] [14]
Adolescents need screening for substance use, self-harm, and emergent disorder, with integrated dual-focus care. Aboriginal and Torres Strait Islander and Māori children need culturally safe services that acknowledge intergenerational trauma and the legacy of racism — never a stigmatising pathway that re-traumatises. Refugee, asylum-seeking, and culturally and linguistically diverse families need culturally safe assessment, professional interpreters, and trauma-adapted care. [14]
Rural and remote families should be offered telehealth-delivered family-focused care rather than told to wait. Families with comorbid parental substance use carry the highest environmental-adversity burden and need active coordination with addiction and child-protection services. Children bereaved by parental suicide or overdose need a bereavement pathway layered onto the inherited-risk work. [1] [14]
Evidence, Guidelines & Regional Differences
Key evidence anchors for exam defence: [1] [7]
- Rutter 1984 Psychol Med — parental psychiatric disorder has measurable effects on children; the foundational risk-and-resilience evidence. [1]
- Quinton 1995 Br J Psychiatry — long-term follow-up of adult psychiatric patients shows intergenerational continuities in disorder and social functioning. [2]
- Reiss 1995 Arch Gen Psychiatry — non-shared environment and differential parenting shape adolescent adjustment; siblings in the same family differ. [3]
- Rasic 2014 Schizophr Bull — offspring of parents with schizophrenia, bipolar, and major depression carry markedly higher risk of mental illness. [4]
- Gotlib 2020 Curr Dir Psychol Sci — intergenerational transmission of depression risk needs prospective, mechanistic study. [5]
- Weissman 2006 JAMA (STAR*D-child) — maternal depression remission is associated with reduction in child psychopathology; treating the parent treats the child. [7]
- Pilowsky 2006 J Clin Psychiatry — children of currently depressed mothers have high rates of psychopathology. [8]
- Beardslee 1997 Am J Psychiatry — clinician-facilitated preventive intervention for families with parental depression produces sustained change. [9]
- Solantaus 2010 Eur Child Adolesc Psychiatry — the Effective Family (EFF) intervention reduces children's psychosocial symptoms. [10]
- Punamäki 2013 J Fam Psychol — preventive family intervention improves children's cognitive attributions, attacking self-blame and hopelessness. [11]
- Nestor 2020 J Fam Psychol — an adolescent depression-prevention programme reduced maternal criticism; the benefit is bidirectional. [12]
- Campbell 2021 Eur Child Adolesc Psychiatry — a high proportion of parents of children in CAMHS have a mental illness themselves. [13]
- Nicholson 2025 Front Psychiatry (ParentingWell) — family-focused practice adapts to support parents with mental illness and their children. [14]
The Children of Parents with a Mental Illness (COPMI) national initiative, now delivered through Emerging Minds, provides the Australian framework for family-focused, two-generational practice, with resources for clinicians, parents, and young carers, and telehealth options for rural and remote regions. Family-inclusive practice is embedded in RANZCP guidance, and mandatory child-protection reporting thresholds are state, territory, and jurisdiction-specific — name the principle and the local service, and do not invent statute numbers. Aboriginal Community Controlled Health Services and culturally safe pathways are central for Aboriginal and Torres Strait Islander and Māori children, acknowledging intergenerational trauma. [14]
Controversies: how to deliver two-generational care when adult and child services are siloed; how to balance early identification against stigma and over-medicalisation; CAMHS waitlists and rural access; and the cultural adaptation of family-prevention programmes so they serve, rather than pathologise, diverse and Indigenous families. [1] [14]
Exam Pearls
FAMILY
- Risk is HEIGHTENED but PROBABILISTIC — most children of affected parents do not develop disorder; never label a well child. [1]
- Treating the parent treats the child: maternal depression remission reduces child psychopathology (Weissman 2006). [7]
- Offspring risk is highest for schizophrenia and bipolar (Rasic 2014), but depression is the commonest affected parent in practice. [4]
- The mechanism is GENE × ENVIRONMENT interplay — Rutter 1984, Reiss 1995 non-shared environment, Gotlib 2020. [3] [5]
- Always ASK "who cares for you when your parent is unwell?" — identify the young carer and hidden need. [14]
- Family-focused prevention (Beardslee, Solantaus EFF, Punamäki) is the evidence base — delivered to the family, not the child alone. [9] [10]
- Parental illness is NEVER blame; safeguarding is threshold-based (capacity, harm, risk), never stigma-driven. [1]
References
- [1]Rutter M Parental psychiatric disorder: effects on children. Psychol Med, 1984.PMID 6545419
- [2]Quinton D, Rutter M, Liddle C A 15-20 year follow-up of adult psychiatric patients. Psychiatric disorder and social functioning. Br J Psychiatry, 1995.PMID 7496639
- [3]Reiss D, Plomin R, Hetherington EM, Howe GW, Rovine MJ, Tryon A, Stanley Hagan M Genetic questions for environmental studies. Differential parenting and psychopathology in adolescence. Arch Gen Psychiatry, 1995.PMID 7487341
- [4]Rasic D, Hajek T, Alda M, Uher R Risk of mental illness in offspring of parents with schizophrenia, bipolar disorder, and major depressive disorder: a systematic review and meta-analysis. Schizophr Bull, 2014.PMID 23960245
- [5]Gotlib IH, Choi E, LeMoult J Studying the Intergenerational Transmission of Risk for Depression: Current Status and Future Directions. Curr Dir Psychol Sci, 2020.PMID 33758474
- [6]Uher R, Pavlova B, Radua J, Provenzani U, Najafi S, Fortea L, Ortuño M, Nazarova A, Perroud N, Palaniyappan L, Domschke K, Cortese S, Arnold PD, Austin JC, Vanyukov MM, Weissman MM, Young AH, Hillegers MHJ, Danese A, Nordentoft M, Murray RM, Fusar-Poli P Transdiagnostic risk of mental disorders in offspring of affected parents: a meta-analysis of family high-risk and registry studies. World Psychiatry, 2023.PMID 37713573
- [7]Weissman MM, Pilowsky DJ, Wickramaratne PJ, Talati A, Wisniewski SR, Fava M, Hughes CW, Garber J, Malloy E, King C, Cerda G, Sood MW, Trivedi MH, Rush AJ, STAR*D-Child Team Remissions in maternal depression and child psychopathology: a STAR*D-child report. JAMA, 2006.PMID 16551710
- [8]Pilowsky DJ, Wickramaratne P, Talati A, Tang M, Hughes CW, Garber J, Malloy E, King C, Cerda G, Sood MW, Trivedi MH, Fava M, Wisniewski SR, Aaronson L, Trivedi MH, Rush AJ, Weissman MM Children of currently depressed mothers: a STAR*D ancillary study. J Clin Psychiatry, 2006.PMID 16426099
- [9]Beardslee WR, Wright E, Rothberg PC, Salt P, Versage M Sustained change in parents receiving preventive interventions for families with depression. Am J Psychiatry, 1997.PMID 9090338
- [10]Solantaus T, Toikka S, Alasuutari M, Sarkka H, Leinonen R Preventive interventions in families with parental depression: children's psychosocial symptoms and prosocial behaviour. Eur Child Adolesc Psychiatry, 2010.PMID 20890622
- [11]Punamäki RL, Qouta S, Isosävi S, Diab SY Effectiveness of preventive family intervention in improving cognitive attributions among children of depressed parents. J Fam Psychol, 2013.PMID 23978323
- [12]Nestor B, Sacks E, Diamond GS, Shirk S, Fein JA Effects of an adolescent depression prevention program on maternal criticisms and positive remarks. J Fam Psychol, 2020.PMID 32658515
- [13]Campbell TCH, Dave S, Rimes KA, Taggart S, Allgar V, Braeken M, Todd J, Smith P, Atchison R, Ford T Prevalence of mental illness among parents of children receiving treatment within child and adolescent mental health services (CAMHS). Eur Child Adolesc Psychiatry, 2021.PMID 32133563
- [14]Nicholson J, Albert K, Biebel K, Williams V, Katz-Leavy J ParentingWell: adapting a family-focused practice for parents with mental illness. Front Psychiatry, 2025.PMID 41048916