Paeds · mental-behavioural-and-psychosomatic
Family assessment and family interventions
Also known as Family assessment · Family interventions · Family therapy and parent training · Family systems work in paediatrics · Evidence-based parenting and family programs
Fellowship guide to systematic family assessment and evidence-based family interventions in paediatrics: the three-generation genogram plus validated family-functioning measures and naturalistic dyad observation that build a shared, non-blaming formulation; the three named mechanisms (coercive cycle, expressed emotion, chronic stress/adversity load) that link the family system to child outcomes; and the stepped ladder of family-level care from universal parenting guidance and home visiting through behavioural parent training (PMT, Triple P, Incredible Years, PCIT) to structured family therapy (FFT, BSFT, FBT) and intensive multisystem care (MST) — always with safety and child-protection gating the plan, across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A seven-year-old whose aggressive behaviour did not settle with a stimulant for ADHD, an adolescent who relapsed after inpatient treatment for anorexia, a toddler who faltered despite a normal workup — these are the children whose family you need to understand. The question is never "is this family dysfunctional?" but "what is the family doing to this child, and what could it do for this child if we helped?" [6] [10]
A family assessment is the systematic appraisal of family structure, functioning, strengths, stressors and the caregiver-child relationship. It is not a single test or a label, and it never reduces a family to a score. Its product is a shared, non-blaming formulation that names the problem the family and clinician will work on together. [10]
A family intervention is any evidence-based treatment delivered to the parent, the caregiver-child dyad, or the whole family system — never the referred child alone. The strength of the field is that the interventions are no longer generic "family counselling" but manualised, tested models with named evidence: parent training, structured family therapy, and intensive multisystem care. [1] [4]
This page owns the assessment skill and the intervention-matching ladder. Dyadic attachment work lives on the attachment leaf, the child-level disorders on their own leaves, and the safeguarding pathway on the maltreatment leaf — but the spine of safe, evidence-based family care runs through here. [9] [10]
Classification
Classify family interventions along one axis before you choose one: how intense does this family's need make the intervention, and which named model fits? The same parenting difficulty means something different for a first-time parent who needs guidance than for a family with chronic adolescent offending. [4] [12]
The field sorts cleanly into four tiers of increasing intensity, cost and complexity. Universal and preventive work — anticipatory guidance, mass-media and primary-care parenting support, and home visiting such as the Nurse-Family Partnership — reaches whole populations and buffers risk before it crystallises. Targeted parent and dyadic training — behavioural parent training, the higher levels of Triple P, the Incredible Years, and Parent-Child Interaction Therapy — treats defined child behaviour problems by changing what the parent does. Structured family therapy treats the family as the patient through manualised models such as Functional Family Therapy, Brief Strategic Family Therapy, and Family-Based Treatment for anorexia. Intensive multisystem care, above all Multisystemic Therapy, wraps services around the family, school, peer group and community for severe and chronic presentations. [1] [4] [6]
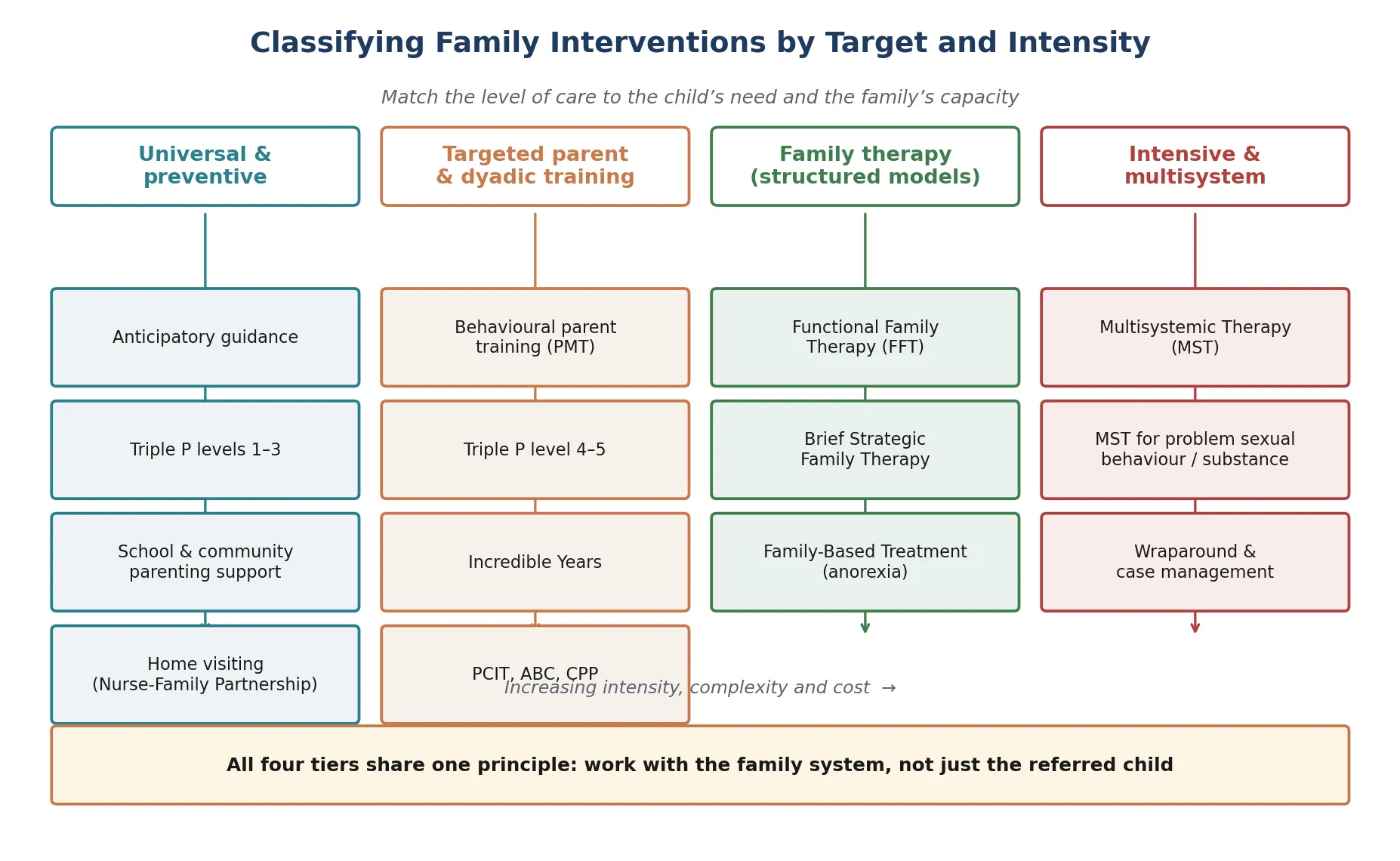
Parent training versus family therapy — the distinction examiners test
- Skills-based: the parent is the agent of change
- Targets the coercive cycle in disruptive behaviour
- Models: PMT, Triple P, Incredible Years, PCIT
- Usually first-line before family therapy
- Systemic: the family is the patient
- Targets interaction patterns and relationships
- Models: FFT, BSFT, FBT (Maudsley)
- Reserved for conduct/substance/anorexia and family-level problems
The trap is the opposite error at each end. Jumping a simple behaviour problem straight to family therapy overshoots, wastes resources, and drops out. But clinging to parent training when an adolescent's offending is entrenched and multisystem undershoots and fails. The classification exists to prevent both. [1] [12]
Epidemiology & Risk Factors
Family adversity is common in the paediatric clinic, and it is usually invisible until you ask. Parental mental illness, substance use, parental conflict, family violence and socioeconomic disadvantage each raise a child's risk across behaviour, mood, development and physical health — and they cluster, so the child who has one often has several. [6] [12]
What matters most is the cumulative load. A child carrying parental depression, recent separation and housing stress is not facing three small risks but a multiplied one, because chronic stress dysregulates the HPA axis, impairs coping, and erodes the caregiving capacity the child's recovery depends on. This is why the "what is happening at home?" question is clinical, not social nicety. [5] [6]
Protective forces point the other way, and they are just as powerful. Warmth, structure, consistent monitoring, family cohesion and a single trusted adult buffer adversity and predict recovery. The Nurse-Family Partnership, which delivers relationship-based home visiting from pregnancy through infancy, shows enduring maternal and child benefits at eighteen-year follow-up — proof that supporting a family early changes a trajectory, not just a score. [5]
Single-parent, blended and kinship structures are not themselves risk factors; they are markers for the adversity that sometimes accompanies them. The clinician's job is to find the active mechanisms, not to judge the family form. [6] [12]
Pathophysiology
Return to the seven-year-old with treatment-resistant aggression. What is the family doing to maintain it? Three named mechanisms carry most of the explanatory weight, and each maps to a different intervention. [6]
The coercive cycle, described by Patterson, is the engine of disruptive behaviour. The child behaves aversively — whining, demanding, hitting — and the parent, exhausted, reacts harshly or gives in. Either reaction ends the aversiveness in the short term, which negatively reinforces the behaviour, so it escalates over months and years. The parent is not failing; the interaction is being shaped by its consequences. Behavioural parent training and PCIT work because they break exactly this cycle. [6] [8]
Expressed emotion is a family tone — criticism, hostility and emotional over-involvement — that predicts relapse in adolescent anorexia, early psychosis and mood disorders. A family can love a child intensely and still carry a tone that undermines recovery. The intervention is psychoeducation plus structured family work that lowers the tone, which is precisely what Family-Based Treatment does for anorexia. [9]
The third mechanism is chronic stress and adversity load. Conflict, parental mental illness, violence and poverty sustain a stress response that impairs regulation, coping and recovery from any illness. Here the intervention is partly social — reduce the stressors, build the protective factors — and partly relational, because a supported parent regains the capacity to be the child's secure base. [5] [6]
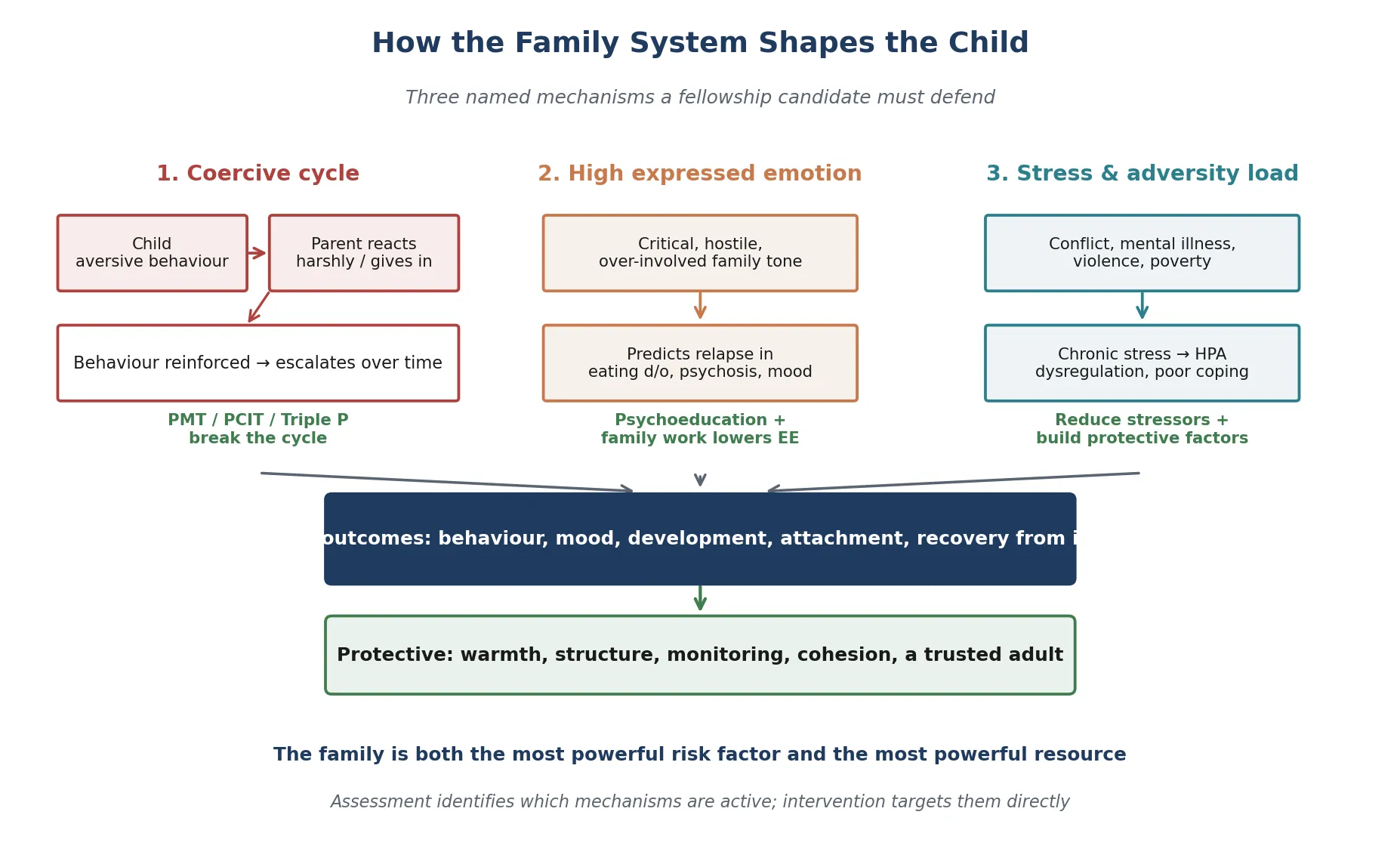
The hopeful corollary is that the same plasticity cuts both ways. If a relationship can wound a child, a relationship can heal one — which is why a stable, attuned carer and a well-matched family intervention re-organise behaviour and biology. The same adversity is never deterministic: resilience, a trusted adult, and corrective relational experience all modify the outcome. [5] [12]
Clinical Presentation
Families rarely present with "family dysfunction." They present with a child whose problem is not settling, who relapsed, who somatises, or whose behaviour the parent cannot manage — and the family dimension surfaces when you ask for it. [6] [12]
A coercive cycle shows itself as escalating aversive exchanges and inconsistent discipline: the parent tries one approach, abandons it, tries another, and the child's behaviour slowly worsens despite everyone's effort. High expressed emotion shows as a stream of critical or over-involved comments about a child with an eating disorder, mood disorder or emerging psychosis, often in a family that is clearly caring but whose tone undermines recovery. Chronic stress shows as parental overwhelm, chaos, missed appointments and treatment non-adherence. [6] [9]
The presentations that demand a safety conversion are the dangerous ones. A controlling partner who answers for the mother, a child whose anxiety or regression tracks contact visits, or injury patterns that do not fit the story — these are not family-therapy referrals, they are safeguarding. So is the parent whose acute mental illness, suicidality or intoxication has overwhelmed the caregiving capacity. [9]
Cultural and structural diversity must never be misread as dysfunction. A grandparent-led kinship household, an intergenerational home, or a discipline practice that is normative in the family's culture are not pathology, and treating them as such destroys trust. The same child can behave very differently across parents, carers and settings — which is exactly why multi-informant data is essential. [10]
Differential Diagnosis
Build the differential in layers: the child-level disorder that the family work is adjunctive to, the family-level states that change the plan, and the look-alikes that must not be mislabelled. [6] [9]
| Pattern | Favours | Against / distinguish |
|---|---|---|
| ADHD, ODD, anxiety, depression, anorexia | Child-level disorder; family work is adjunctive | Treat the child's diagnosis on its own merits; family work does not replace it |
| Primary attachment disorder or relational trauma | Grossly pathogenic early care, cross-caregiver pattern | Cross-link the attachment leaf; dyadic ABC/CPP, not generic parent training |
| Family / intimate-partner violence | Controlling partner, injury patterns, child fear | Safety pathway first; joint family therapy contraindicated while active |
| Parental mental illness or substance use | Parental overwhelm, disclosure, COPMI framing | Treat the parent as part of the child's plan; not parenting classes alone |
| Neurodevelopmental disorder | Autism, intellectual disability, developmental delay | Do not attribute to "poor parenting"; run both tracks in parallel |
| Socioeconomic / housing stress | Poverty, instability, unmet basic needs | The intervention is social and practical, not primarily therapeutic |
| Cultural / structural variation | Kinship, blended, intergenerational, cultural norms | Not pathology; do not pathologise cultural parenting |
| Normal developmental challenge | Toddler tantrums, adolescent boundary-testing | Guidance and reassurance, not a therapy referral |
The two classic errors are mirror-images: attributing a neurodevelopmental disorder to "poor parenting" (overshadowing the child's diagnosis), and treating a child's behaviour problem as the family's failure when the real driver is unrecognised parental mental illness, violence, or poverty that "parenting classes" will not touch. When the response is poor, return to the differential before changing the dose. [6]
Clinical & Bedside Assessment
Lead with the genogram, and lead it gently. A three-generation family map, drawn with the family, reveals structure, loss, conflict and repeating patterns in a few minutes — and it does so without anyone feeling accused. The act of drawing it together is itself the engagement. [10]
Family assessment sequence
Safety first
Screen for violence, maltreatment and acute parental crisis; convert to a safeguarding pathway if any is present before any family work proceeds.
Genogram
Draw three generations; record structure, significant events, losses, conflict and repeating patterns; let the family narrate it.
Functioning and the dyad
Add a validated family-functioning measure (FAD dimensions, Family APGAR) and observe the caregiver-child relationship in a naturalistic moment.
Strengths and stressors
Name the protective factors to build on and the stressors to address; assess parental mental health, substance use and conflict as part of the child's plan.
Shared formulation
Build the formulation WITH the family — non-blaming, naming the problem to work on together and which mechanism is active.
Match and close the loop
Match the intervention rung to the problem, name the owner and follow-up, and document return precautions.
Validated measures sharpen the picture but never replace clinical judgement. The McMaster Family Assessment Device structures functioning across problem-solving, communication, roles, affective responsiveness, affective involvement and behaviour control; the Family APGAR screens adaptation, partnership, growth, affection and resolve. Look up their cut-scores in the source manual rather than inventing them, and always gather the child's, each parent's and the school's view, because discordance is itself data. [10]
Observe the relationship in a naturalistic moment — how the parent responds when the child is bored, frustrated or asked to do something — rather than engineering a staged interaction. A coercive exchange, a missed opportunity for warmth, or a parent who cannot set a limit will show themselves. Diagnosing a family on a single clinic snapshot is a classic error. [6] [10]
Investigations
Family assessment is clinical. There is no blood test, scan or biomarker that confirms "family dysfunction," and the commonest investigation error is the shotgun panel ordered for "behaviour." Your core investigations are the genogram, the validated family-functioning measure, the developmental assessment, and the multi-informant observation. [6] [10]
Investigate when the story points somewhere. Screen for the comorbid child disorders — ADHD, ODD, anxiety, depression, anorexia — that the family intervention is adjunctive to, because treating the family while ignoring the child's own diagnosis is a common cause of non-response. Ask the COPMI question and screen for parental mental illness and substance use, which are drivers, not background. [9]
Screen safely for family violence. Ask the non-offending parent alone, never in front of a controlling partner, and have a safety plan before you ask, because a positive screen can endanger. When maltreatment is disclosed, the safeguarding forensic examination is a separate, protocolised pathway — arrange it, do not improvise it. [9]
Formal child mental-health or family-therapy assessment is indicated when the problem is complex, severe, or not responding to first-line parent guidance, and the urgency is set by the risk and the impairment. Where family difficulty and developmental delay coexist, run both tracks in parallel rather than forcing an either/or choice. [6] [10]
Management — Resuscitation
"Resuscitation" in a family presentation means immediate safety and the end of ongoing threat — not a therapy session and not a parenting handout. [9]
Make a same-day safety plan: supervision, restriction of means where relevant, who to call, and where to go. Support the non-offending parent explicitly. Recognise that acute parental mental illness, suicidality or intoxication has overwhelmed the caregiving capacity and needs its own urgent pathway — a parent in crisis cannot be the child's secure base today. No medication or single session "resuscitates" a family crisis; safety and stability are the resuscitation. [9] [10]
Management — Definitive & Stepwise
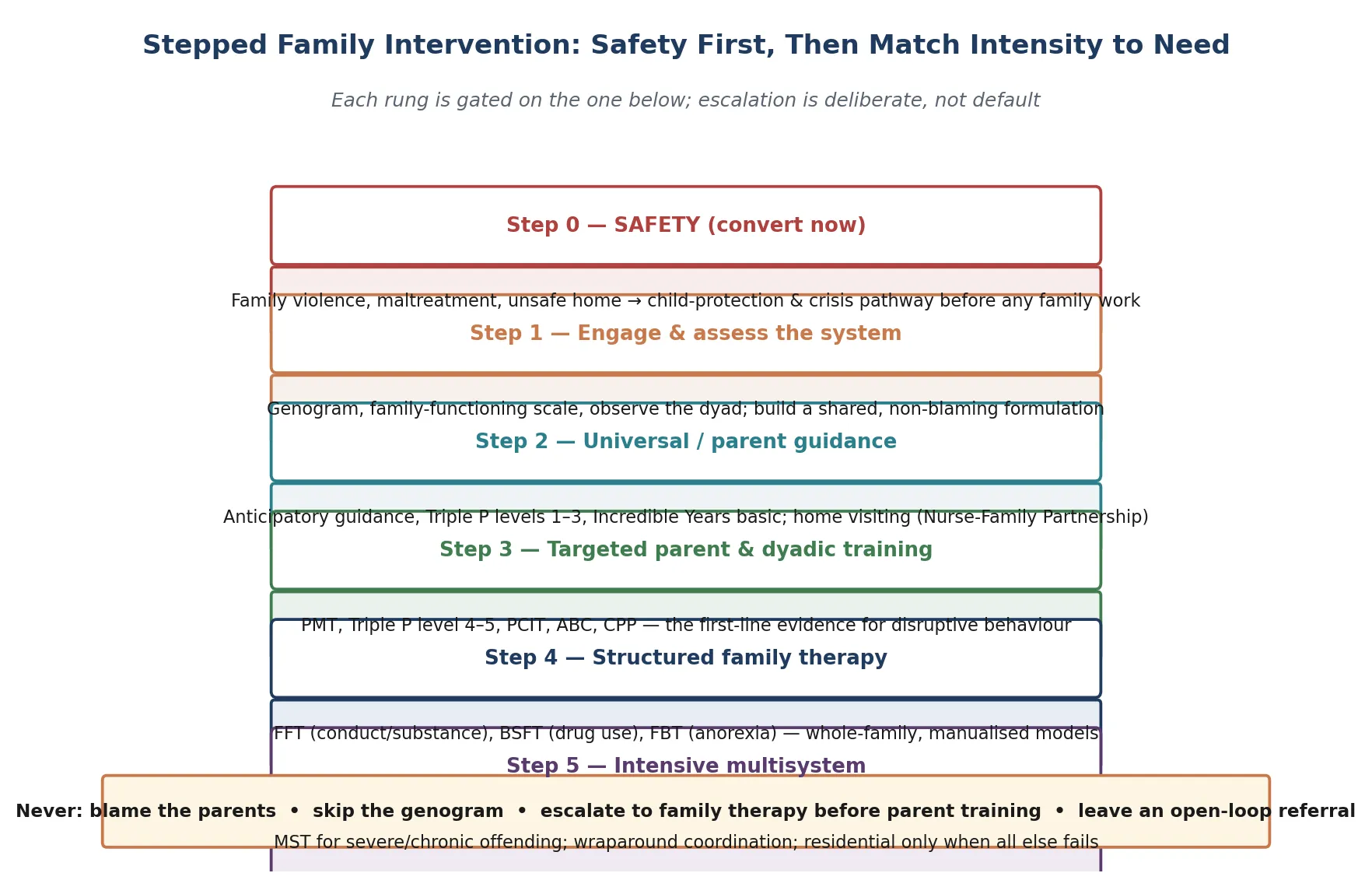
Stepped, intensity-matched family care is the frame, and the order matters as much as the content. Safety gates everything; the lowest effective rung is chosen first; escalation is deliberate, not default. [6] [12]
Step 0 — Safety
Convert to child-protection and crisis pathway if violence, maltreatment or an unsafe home is present. No family work proceeds until the environment is safe. [9]
Step 1 — Engage and assess the system
Draw the genogram, add a family-functioning measure, observe the dyad, and build a shared, non-blaming formulation that names the active mechanism and the problem to work on together. [10]
Step 2 — Universal and preventive
Anticipatory guidance, the lower levels of Triple P, Incredible Years basic, and home visiting such as the Nurse-Family Partnership reach whole populations and buffer risk before it crystallises. Olds' eighteen-year follow-up shows enduring maternal benefit — early support changes a trajectory. [4] [5]
Step 3 — Targeted parent and dyadic training (the first-line evidence)
For disruptive behaviour, behavioural parent training is first-line, not family therapy. Kazdin's work on parent management training, the Triple P systematic review, the Incredible Years, and the PCIT meta-analysis each show that changing what the parent does changes the child's behaviour — by breaking the coercive cycle. The Barlow Cochrane review and the Mingebach meta-meta-analysis confirm that parent-based interventions improve externalising outcomes broadly. [4] [6] [7]
Step 4 — Structured family therapy
When the problem is adolescent conduct or substance use, or anorexia, deliver a manualised, whole-family model. Functional Family Therapy is effective for youth with behavioural problems; Brief Strategic Family Therapy reduced adolescent drug use versus treatment as usual in a multisite trial; and Family-Based Treatment was superior to adolescent-focused individual therapy for anorexia. These are not generic counselling — they are named, tested models. [2] [3] [9]
Step 5 — Intensive multisystem care
For severe, chronic or entrenched presentations — violent and chronic juvenile offending — Multisystemic Therapy wraps services around the family, school, peer group and community and reduced re-arrest and out-of-home placement in Henggeler's landmark trial. Residential or out-of-home placement is reserved for when all else fails. [1]
Close the loop at every rung. Name the clinician who owns the plan, set the follow-up date, document the interim strategy and return precautions, and coordinate with school and general practitioner. The family intervention is adjunctive to treating the child's own disorder on its merits — medication for ADHD or depression is not a "family intervention," and treating the family does not excuse leaving the child's diagnosis undertreated. [9] [12]
Specific Subtypes & Scenarios
Disruptive behaviour / ODD / conduct. First-line behavioural parent training — PMT, Triple P level 4 to 5, Incredible Years, or PCIT — to break the coercive cycle. Escalate to FFT or MST only for persistent or severe cases. [6] [7]
Adolescent conduct or substance use. Structured family therapy: Functional Family Therapy for behavioural problems, or Brief Strategic Family Therapy for drug use, both with multisite RCT evidence. MST for severe or chronic offending. [1] [2] [3]
Adolescent anorexia nervosa. Family-Based Treatment (the Maudsley model) is first-line and was superior to adolescent-focused individual therapy. Family work is adjunctive to medical stabilisation and refeeding. [9]
Parental mental illness or substance use (COPMI). Treat the parent's illness as part of the child's plan. Family-focused, preventively oriented intervention reduces transmission; parenting classes alone do not treat a parental depression. [6]
Family violence / intimate-partner violence. Safety and child-protection pathway first. Joint family therapy is contraindicated while violence is active, because it can endanger the non-offending parent and the child. [9]
Child in out-of-home or kinship care. Support the carer as the intervention. Trauma-informed, attachment-aware family work — never blame the carer for behaviours that began before placement. [10]
Refugee, asylum-seeking and culturally diverse family. Culturally safe assessment, professional interpreters, and programs adapted to context. Do not pathologise cultural parenting norms or stranger behaviour. [10]
Indigenous family. Culturally safe, non-stigmatising services that acknowledge intergenerational trauma and racism; Aboriginal Community Controlled Health Services are central in ANZ. [10]
Developmental disability or autism. Run child-development and family-support tracks in parallel; psychoeducation, advocacy and respite are part of the family plan. [6]
Chronic illness or non-adherence. Family-based adherence and self-management support. Address family conflict and communication, not blame; a supported family sustains the regimen. [12]
Complications & Pitfalls
- Blaming the parents — especially the mother — for the child's problem. [6]
- Skipping the genogram and family-functioning assessment and jumping straight to therapy. [10]
- Escalating to family therapy before trying parent training where disruptive behaviour is the issue. [6]
- Conflating generic "family counselling" with evidence-based, manualised family models. [1]
- Running joint family sessions while family violence is active. [9]
- Missing parental mental illness or substance use as the real driver. [6]
- Misattributing a neurodevelopmental disorder to "family dysfunction" or "poor parenting." [6]
- Pathologising cultural or structural family variation. [10]
- Ignoring socioeconomic and housing stress when the real intervention is social, not therapeutic. [5]
- Leaving an open-loop referral to family therapy with no interim plan, relapse signs or safety-net. [12]
Prognosis & Disposition
Evidence-based family interventions produce measurable gains when they are matched to the problem and delivered with fidelity. Parent training improves disruptive behaviour broadly; FFT and BSFT improve adolescent conduct and substance outcomes; FBT improves anorexia; and MST reduces re-arrest in severe offending. Prognosis is better when the active mechanism is correctly identified and targeted. [1] [7] [9]
Parental mental illness, family violence and socioeconomic adversity worsen prognosis unless they are addressed as part of the plan. Early, lower-intensity intervention — parent training, home visiting — prevents escalation to intensive multisystem care, which is why matching the rung matters as much as choosing the model. [5] [6]
Disposition after safety confirmed: step the family into the matched rung via local CAMHS, early-intervention or parenting-program pathways, with medical-home interim support. Disposition when risk surfaces: crisis and child-protection pathway, same-day supports, stability before therapy. [9] [12]
Markers of response are reduced coercive exchange, improved warmth, structure and monitoring, reduced child symptoms, better adherence, and the family's own report of improved function. Engagement and retention — reducing dropout — are themselves determinants of outcome in family work, so an intervention the family will actually attend beats a "better" one they will not. Long waitlists shift the medical-home role to interim parent coaching, psychoeducation and school liaison rather than passive waiting. [6] [12]
Special Populations
Children of parents with mental illness or substance use (COPMI) carry disproportionate risk; treat the parent as part of the child's plan with preventive, family-focused intervention. Families experiencing violence need the safety and child-protection pathway first — family therapy is contraindicated while violence is active. [5] [9]
Out-of-home and kinship-care families need the carer supported as the intervention, with trauma-informed, attachment-aware care. Refugee, asylum-seeking and culturally and linguistically diverse families need culturally safe assessment, professional interpreters, and programs adapted to their context. Indigenous families need non-stigmatising services that acknowledge intergenerational trauma, with Aboriginal Community Controlled services central in ANZ. [10]
Families of children with developmental disability or autism run child-development and family-support tracks in parallel, with psychoeducation and respite. Adolescents need their confidentiality and voice respected, with family work adapted to their developmental stage and engagement. Rural and remote families should be offered telehealth-delivered parenting programs and family intervention rather than told to wait, and socioeconomically disadvantaged families need practical social support — housing, food, finance — paired with any therapeutic work, because poverty is not a parenting failure. [4] [6]
Evidence, Guidelines & Regional Differences
Key evidence anchors for exam defence: [1] [12]
Multisystemic Therapy
Key finding
MST with violent and chronic juvenile offenders and their families reduced re-arrest and out-of-home placement versus usual services — the multisystem evidence for intensive family-ecology intervention.
Functional Family Therapy
Key finding
FFT delivered in community settings is effective for youth with behavioural problems — structured family therapy that treats the family as the patient.
Family-Based Treatment for anorexia
Key finding
In the RCT comparing FBT with adolescent-focused individual therapy for adolescent anorexia, FBT was the superior approach — family therapy as first-line, not adjunctive.
The parent-training evidence is equally strong. Sanders' Triple P systematic review spans multiple levels and outcomes; Thomas' PCIT meta-analysis shows large effects on child behaviour and parenting; Kazdin's PMT work treats conduct problems and shows how to enhance outcomes; and the Barlow Cochrane review and Mingebach meta-meta-analysis confirm that parent-based interventions improve externalising outcomes broadly. The Nurse-Family Partnership shows that early, relationship-based home visiting produces enduring benefit. [4] [5] [7]
Family assessment and evidence-based parenting programs are delivered through the medical home, local CAMHS and early-intervention pathways, with universal home visiting (the Nurse-Family Partnership model) in many jurisdictions and telehealth delivery for rural and remote regions. Aboriginal Community Controlled Health Services and culturally safe pathways are central for Aboriginal and Torres Strait Islander and Māori children. Mandatory child-protection reporting thresholds are state and territory specific — name the principle and the local service. [4] [10]
Controversies: the fidelity and dissemination of manualised models as they scale; cultural adaptation without losing the active ingredient; whether family therapy adds benefit beyond individual treatment for some disorders; how to deliver evidence-based care when CAMHS waitlists are long and rural access is thin; and the persistent risk of parent-blaming language in family assessment. [1] [12]
Exam Pearls
FAMILY
- Disruptive behaviour is first-line for PARENT TRAINING (PMT, Triple P, Incredible Years, PCIT), not family therapy. [6] [7]
- FFT (Sexton), BSFT (Robbins) and MST (Henggeler) are the structured family-therapy and multisystem models for adolescent conduct and substance use. [1] [2] [3]
- FBT / Maudsley (Lock) is first-line family therapy for adolescent anorexia, superior to adolescent-focused individual therapy. [9]
- The three mechanisms: coercive cycle (Patterson), expressed emotion, and chronic stress / adversity load. [6]
- The Nurse-Family Partnership (Olds) is the preventive home-visiting rung with enduring benefit. [5]
- Safety and child-protection gate the whole plan — never run joint family sessions while violence is active. [9]
- The family is both the most powerful risk factor and the most powerful protective resource. [6] [12]
References
- [1]Henggeler SW, Melton GB, Brondino MJ, Scherer DG, Hanley JH Multisystemic therapy with violent and chronic juvenile offenders and their families: the role of treatment fidelity in successful dissemination. J Consult Clin Psychol, 1997.PMID 9337501
- [2]Sexton TL, Turner CW The effectiveness of functional family therapy for youth with behavioral problems in a community setting. J Fam Psychol, 2010.PMID 20545407
- [3]Robbins MS, Feaster DJ, Henderson C, Horigian V, Robbins M, Szapocznik J Brief strategic family therapy versus treatment as usual: results of a multisite randomized trial for substance using adolescents. J Consult Clin Psychol, 2011.PMID 21967492
- [4]Sanders MR, Kirby JN, Tellegen CL, Day JJ The Triple P-Positive Parenting Program: a systematic review and meta-analysis of a multi-level system of parenting support. Clin Psychol Rev, 2014.PMID 24842549
- [5]Olds DL, Kitzman H, Knudtson MD, Anson E, Smith JA, Cole R Prenatal and Infancy Nurse Home Visiting Effects on Mothers: 18-Year Follow-up of a Randomized Trial. Pediatrics, 2019.PMID 31748253
- [6]Kazdin AE Parent management training for conduct problems in children: Enhancing treatment effectiveness. Int J Clin Health Psychol, 2018.PMID 30487914
- [7]Thomas R, Abell B, Webb HJ, Avdagic E, Zimmer-Gembeck MJ Parent-Child Interaction Therapy: A Meta-analysis. Pediatrics, 2017.PMID 28860132
- [8]Thomas R, Zimmer-Gembeck MJ Behavioral outcomes of Parent-Child Interaction Therapy and Triple P-Positive Parenting Program: a review and meta-analysis. J Abnorm Child Psychol, 2007.PMID 17333363
- [9]Lock J, Le Grange D, Agras WS, Moye A, Bryson SW, Jo B Randomized clinical trial comparing family-based treatment with adolescent-focused individual therapy for adolescents with anorexia nervosa. Arch Gen Psychiatry, 2010.PMID 20921118
- [10]Miller IW, Kabacoff RI, Epstein NB, Bishop DS, Keitner GI, Baldwin LM, van der Spuy HI The development of a clinical rating scale for the McMaster model of family functioning. Fam Process, 1994.PMID 8039568
- [11]Barlow J, Bergman H, Kornør H, Wei Y, Bennett C Group-based parent training programmes for improving emotional and behavioural adjustment in young children. Cochrane Database Syst Rev, 2016.PMID 27478983
- [12]Mingebach T, Egberts MR, Kamp-Becker I, Poustka L, Lehmkuhl L, Christiansen H Meta-meta-analysis on the effectiveness of parent-based interventions for the treatment of child externalizing behavior problems. PLoS One, 2018.PMID 30256794