Paeds · mental-behavioural-and-psychosomatic
Grief, bereavement and adjustment disorder in children
Also known as Prolonged grief disorder · Complicated grief in children · Persistent complex bereavement disorder · Adjustment disorder in children and adolescents · Childhood bereavement
Fellowship guide to grief, bereavement and adjustment disorder in children: separating normal grief from prolonged grief disorder (PGD) and from adjustment disorder using the DSM-5-TR and ICD-11 structure (the bereavement gateway and duration threshold that set PGD apart from any-stressor, three-month adjustment disorder), the grief-versus-MDD-versus-PTSD distinction, suicide and safeguarding assessment in every case, watchful waiting and caregiver-supported care as first-line, the Boelen CBT-for-PGD and Cohen/Mannarino TF-CBT evidence with no first-line medication, and a closed-loop disposition across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
An eight-year-old whose grandfather died six weeks ago cries at bedtime, talks about him, and has stopped enjoying football — but plays with friends at school and is eating again. Next door, a thirteen-year-old whose parents separated two months ago is refusing school, snapping at everyone, and wrote in a diary that she "can't see the point." Both are distressed. One is grieving normally; the other may have an adjustment disorder. The skill is telling them apart, and the first principle is that grief is a process, not a disease — most bereaved children adapt without ever needing a diagnosis or a referral. [1] [3]
Bereavement is the objective situation of having lost someone significant. Grief is the natural, multifaceted response — emotional, cognitive, behavioural and physical — to that loss. Normal (uncomplicated) grief in a child shows as waves of sadness and yearning, disturbed sleep and appetite, longing for the deceased, and a gradual return to play, peers and engagement, with overall function preserved. This is the expected trajectory, and the reassurance it offers the family is therapeutic in itself. [1] [3]
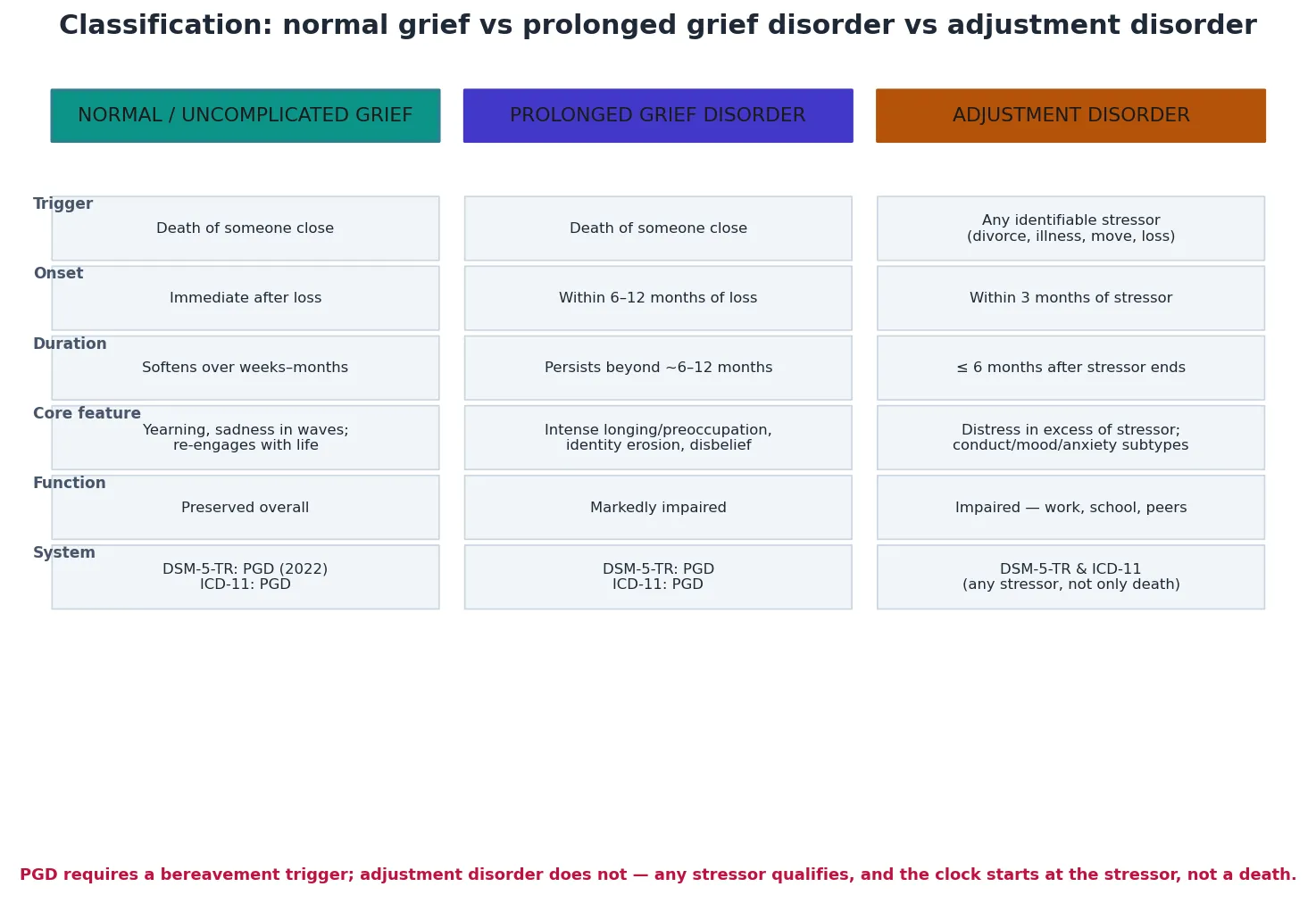
Two states cross a disorder threshold and need active treatment. Prolonged grief disorder (PGD) is grief that persists beyond the expected cultural and developmental window — intense yearning or preoccupation with the deceased, with identity disruption, disbelief, avoidance of reminders, and a sense that life has lost meaning — causing marked impairment. Adjustment disorder is a maladaptive reaction to an identifiable psychosocial stressor, developing within about three months, with distress in excess of the stressor or functional impairment, that resolves within about six months of the stressor ending. The gateway that separates them is the trigger: PGD follows a bereavement, whereas adjustment disorder follows any stressor — a parental separation, a serious illness, displacement, or school upheaval. [4] [12]
[4] [6]Depth on the depressive-syndrome spine lives on the depression leaf, the trauma-response continuum on the PTSD leaf, and acute self-harm risk on the suicide-and-self-harm leaf. This page owns the grief–bereavement–adjustment spine that runs from recognition through stepped care to a closed loop. [2] [12]
Classification
Classify along three questions before you name a disorder: what happened (the trigger), how long it has lasted (the clock), and what it is not (MDD, PTSD, or normal variation). A tearful child six weeks after a grandfather's death means something different from the same child at fifteen months with persistent impairment. [1] [4]
By trigger and clock (DSM-5-TR and ICD-11)
| Pattern | Trigger | Onset & duration | Core feature |
|---|---|---|---|
| Normal grief | A death | Immediate; softens over weeks–months | Wavelike sadness, yearning, function preserved |
| Prolonged grief disorder | A death (bereavement) | Beyond the threshold (~6–12 months) | Intense longing/preoccupation, identity erosion, impairment |
| Adjustment disorder | Any identifiable stressor | Within ~3 months; resolves within ~6 months | Distress in excess of stressor; depressed/anxious/mixed/conduct subtypes |
By subtype — especially adjustment disorder in children
Adjustment disorder splits by the dominant mood, and the split matters for risk and for management. The depressed-mood and anxious subtypes are the ones most families recognise. The mixed anxiety-and-depressed subtype combines low mood with worry. The disturbance of conduct subtype — defiance, rule-breaking, recklessness — is the one that gets misread as "just bad behaviour" and that hides suicidality in adolescents, which is why it must never be dismissed. [12] [13]
Prolonged grief disorder versus adjustment disorder
- Triggered by a bereavement — a death
- Declares itself after a duration threshold (~6–12 months)
- Core is intense yearning/preoccupation plus identity erosion
- Treated with CBT for PGD or TF-CBT for traumatic grief
- Triggered by any identifiable stressor, not only death
- Onset within ~3 months; resolves within ~6 months
- Core is distress in excess of the stressor with impairment
- Depressed, anxious, mixed or conduct subtypes; assess suicidality
Epidemiology & Risk Factors
Most children will experience the death of someone close before adulthood, and the single most important epidemiological fact for this topic is that the majority of them adapt without developing a disorder. The children you are looking for are the minority whose grief crosses the PGD threshold, and the larger group whose reaction to a non-death stressor crosses into adjustment disorder. [1] [3]
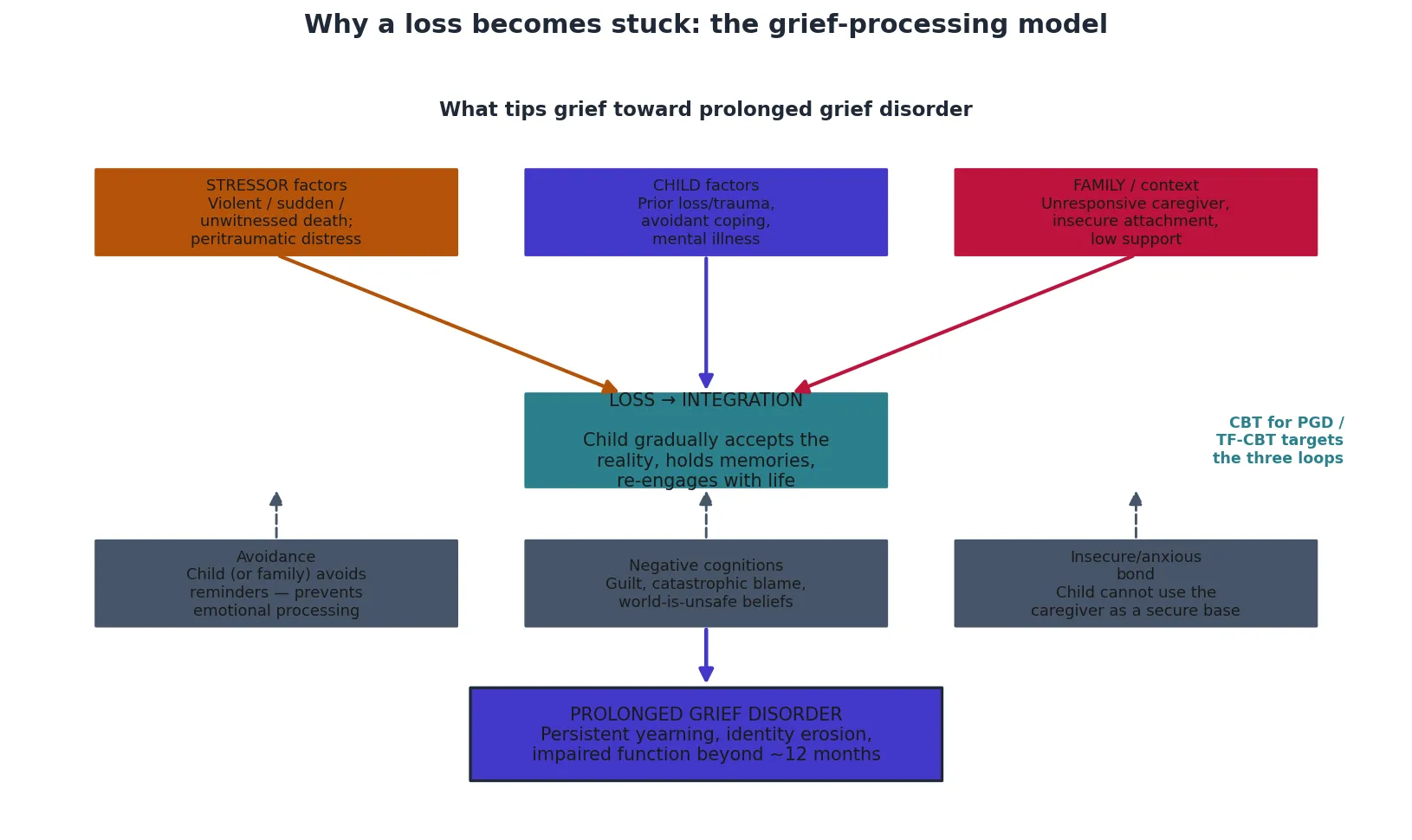
What tips a bereaved child toward PGD? The Melhem group showed that complicated grief in children and adolescents has a distinct phenomenology and set of correlates, and Revet showed that peritraumatic distress — the distress the child felt at the moment of learning of the death — predicts later PGD severity after the death of a parent. The nature of the death matters: a sudden, violent, suicide or witnessed death, or one the child feels they should have prevented, raises risk. So do child-level factors — prior bereavement or trauma, pre-existing anxiety or depression, and an avoidant coping style — and family factors, especially an unresponsive caregiver whose own grief is unresolved and who cannot be the secure base the child needs. [1] [5]
Adjustment disorders are among the most common psychiatric diagnoses in children and adolescents presenting to services, precisely because the trigger is any stressor and the bar is functional impairment. The warning the Pelkonen study lands is that adolescent adjustment disorder outpatients carry substantial suicidality — distress in excess of a stressor is not, in a teenager, a benign time-limited state, and the conduct subtype hides risk. [12] [13]
Pathophysiology
Think of grief not as a sequence of fixed "stages" but as the work of updating a child's internal world. A child has built an attachment figure into their sense of safety and self; when that figure dies, the model has to be rewritten — the reality of the loss accepted, the memories held, and a future re-imagined without the person. Most children do this work, fitfully and with waves of pain, and come through it. PGD is what happens when the work stalls. [3] [6]
The cognitive-behavioural model that frames PGD, developed in the Boelen group's work on children and adults, names three keeping the grief stuck. First, experiential avoidance — the child, or the whole family, dodges the reminders and the feelings, so the loss is never emotionally processed. Second, negative cognitions — guilt ("it was my fault"), catastrophic blame, or a belief that the world is wholly unsafe. Third, an insecure or anxious bond that leaves the child unable to use the surviving caregiver for co-regulation at exactly the moment they need one. These are not abstract ideas; they are the targets the therapy aims at. [6]
Development shapes everything. A preschooler does not yet hold the concrete idea that death is irreversible, and may believe the dead person will return, which is why magical thinking and guilt appear so often in this age group. A school-age child grasps irreversibility and can feel acute, specific guilt about things they did or did not do. An adolescent faces the existential weight of it — the first real encounter with mortality and with the fragility of the future. Adjustment disorder, by contrast, is best understood not as a discrete neurobiological disease but as the moment a stressor overwhelms the child's existing coping resources. [3] [13]
Clinical Presentation
Families rarely arrive saying "grief" or "adjustment disorder." They bring a child who is "not coping," "won't go to school," "is angry all the time," or who has stopped sleeping and eating. Your history converts that into one of the three pictures, and the conversion hinges on the trigger, the clock and the quality of the distress. [1] [12]
Normal grief shows as sadness in waves, yearning for the deceased, disturbed sleep and appetite, transient regression, talking about the person, and a gradual return to play and peers. Crucially, the positive affect returns between the waves — the child laughs, plays, and re-engages. Prolonged grief disorder shows as intense and persistent longing or preoccupation that does not soften, disbelief that the person is gone, avoidance of reminders, a feeling that a part of oneself has died, emotional numbness, and a sense that life is meaningless — running past the duration threshold and eroding function at school, at home and with friends. Adjustment disorder shows as distress that is clearly in excess of the stressor or function that has clearly broken down, within about three months of an identifiable trigger, with a depressed, anxious, mixed, or conduct flavour. [4] [12]
The age variants are where mistakes happen. A preschooler may regress, complain of tummy aches, or state confidently that the dead person is "coming back on Tuesday." A school-age child may show concentration and school decline, specific guilt, or concrete fears that they or another loved one will die next. An adolescent may present with existential despair, irritability, withdrawal, risk-taking, or substance use layered onto the grief. A quiet, "well-behaved," compliant child is not necessarily coping — withdrawal, numbness and over-compliance can mask PGD. [1] [13]
[1] [12]Differential Diagnosis
Build the differential in layers: the other normal-state end of the spectrum, the disorders that mimic symptomatically, and the medical mimics that must not be missed. [2] [12]
| Pattern | Favours | Against / distinguish |
|---|---|---|
| Pervasive anhedonia, worthlessness, psychomotor change | Major depressive disorder | Grief is wavelike; positive affect returns between waves |
| Cue-driven intrusion, avoidance, hyperarousal | PTSD | Linked to trauma cues; can coexist with grief after violent death |
| Wavelike grief, function preserved | Normal (uncomplicated) grief | Below the PGD duration and impairment threshold |
| Distress in excess of a stressor within ~3 months | Adjustment disorder | Trigger is any stressor; resolves within ~6 months |
| Persistent worry or separation fear after a loss | Anxiety disorder | Anxiety is the dominant feature, not grief |
| Somatic complaints dominating the presentation | Somatic symptom disorder | Physical symptoms are the focus; loss is secondary |
| Fatigue, weight change coinciding with a stressor | Medical mimic (thyroid, anaemia, infection) | Targeted screens clarify |
The discriminating question for grief-versus-MDD is the texture of the mood. Grief comes in waves tied to thoughts of the deceased, with the capacity for pleasure intact between waves; major depression is pervasive and anhedonic, with worthlessness and self-loathing. The Geronazzo-Alman study of children bereaved after 9/11 showed that grief, depression and post-traumatic stress are empirically distinct constructs in bereaved children — which is why treating them as one bucket leads to the wrong therapy. [2]
Clinical & Bedside Assessment
Lead with the loss or stressor history, taken at the child's pace. You need to know what happened, when, how the child learned of it, whether it was sudden, violent or witnessed, and what the child understood — because the developmental understanding of death shapes both the presentation and the assessment. Map the grief pattern: the waves, the yearning, sleep, appetite, play, peer re-engagement, and whether function is preserved or impaired. [1] [5]
Grief- and adjustment-informed assessment sequence
Stressor or loss history
What happened, when, how the child learned of it, sudden/violent/witnessed, what the child understood developmentally.
Pattern mapping
Map the grief waves and yearning vs adjustment-distress; assess sleep, appetite, play, peers and function over time.
Threshold check
Screen PGD (persistent longing, identity erosion, avoidance, meaninglessness beyond the duration threshold) and adjustment disorder (stressor, onset within ~3 months, in excess, subtypes).
Suicide & safeguarding
Ideation, intent, plan, means, hopelessness, prior self-harm; abuse, family violence, unsafe placement — every case.
Caregiver & comorbidity
Caregiver's own grief and capacity to be the secure base; screen depression, anxiety, PTSD, substance use.
Formulate and plan
Name the state and the subtype, the safety status, the step of care, the named owner and the safety-net.
Standardised grief and adjustment rating scales sharpen the picture and track response over time, but they do not replace clinical judgement, and several are proprietary or jurisdiction-specific — look up the manual rather than inventing a cut-score. Gather the caregiver's and the school's view alongside the child's, because function across settings is part of the diagnosis, and discordance is itself data. [4] [13]
Examine the child too. Significant weight loss, severe sleep deprivation, or signs of self-harm need their own pathway. Do not let a behavioural label obscure a medical mimic when fatigue or somatic symptoms dominate — targeted thyroid, blood-count and sleep screens clarify when the story points there. And assess the caregiver directly, kindly: a caregiver drowning in their own unprocessed grief cannot be the secure base this child needs, and your plan must match real life. [1] [13]
Investigations
Grief, PGD and adjustment disorder are clinical diagnoses. There is no blood test, scan, or biomarker that confirms any of them, and the commonest investigation error is the shotgun panel ordered for "low mood." Your core assessment is the structured loss-and-stressor history, the mental state and functional assessment, the multi-informant picture, and the suicide and safeguarding screen. [1] [12]
Investigate when the story points somewhere. Run targeted screens when fatigue, weight change or somatic symptoms suggest a medical mimic — thyroid function, full blood count, and inflammatory markers when infection is plausible. Consider a sleep evaluation when persistent insomnia is driving the impairment. None of these confirms a grief or adjustment diagnosis; they exclude the mimics that masquerade as one. [4] [13]
Screen actively for the comorbidities that change the plan — depression, anxiety, PTSD and adolescent substance use — because treating the grief while ignoring a comorbid disorder is a common cause of non-response. Where a child's developmental understanding of death is unclear, run a developmental assessment in parallel, since it shapes both the formulation and the approach. Refer to child psychology or psychiatry when PGD is suspected, when there is treatment non-response, when comorbidity is complex, or when the diagnosis is genuinely uncertain. [2] [6]
Management — Resuscitation
"Resuscitation" here means immediate safety, the restoration of daily scaffolding, and the end of any ongoing threat — not a drug, and not a therapy session. [12] [13]
[12] [13]Make a same-day safety plan with the caregiver and the system: who supervises, where the means are restricted, who to call, and where to go. Support the caregiver explicitly, because an emotionally available, supported caregiver is the most powerful acute intervention a grieving child has. Restore the scaffolding of daily life — sleep, meals, routine, and a gentle return to school and peers — because these are the foundation on which any later therapy will stand. Recognise that no medication "resuscitates" grief or an adjustment disorder; safety, psychoeducation and caregiver support are the resuscitation. [1] [12]
Management — Definitive & Stepwise
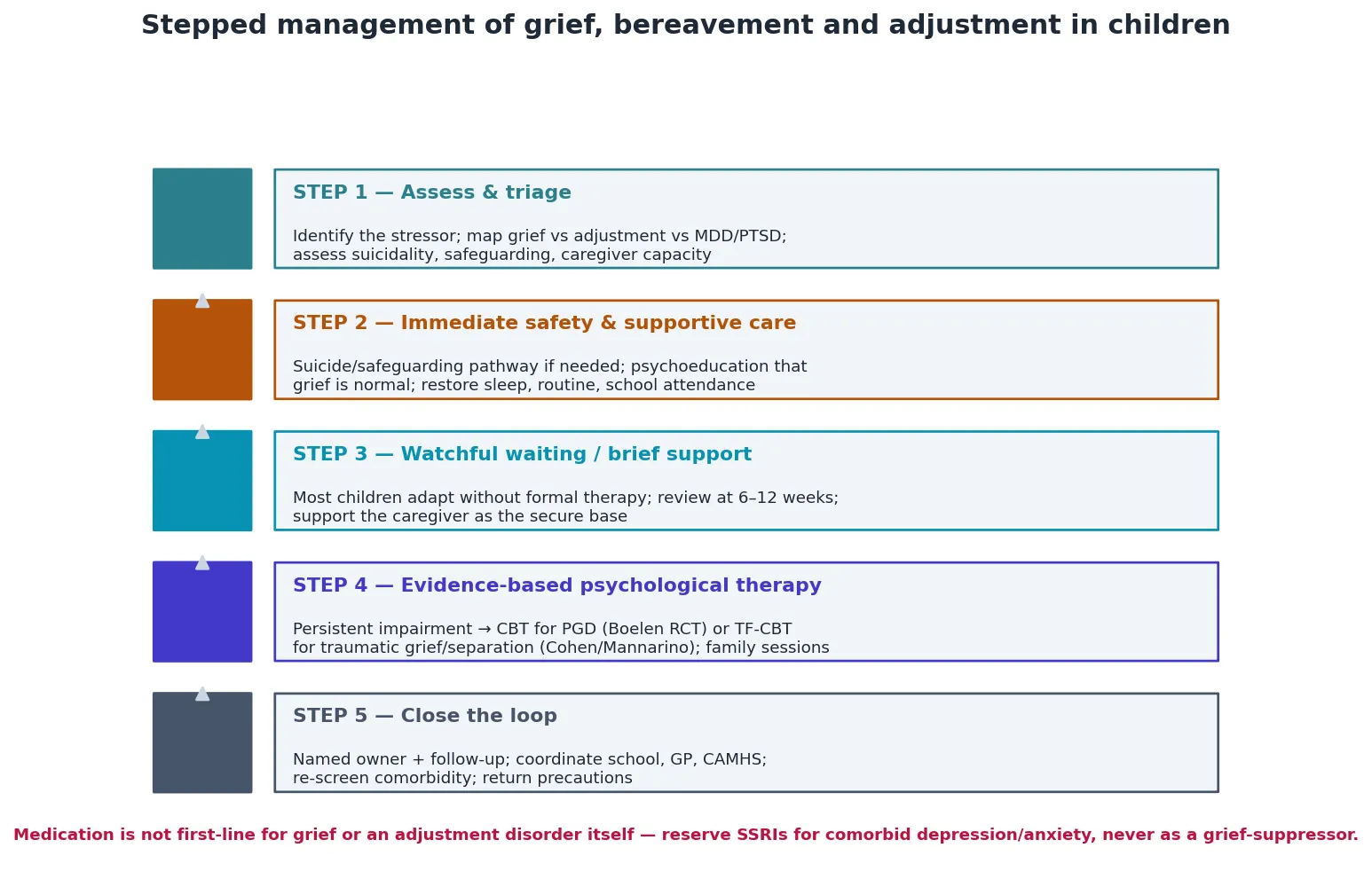
Stepped care is the frame, and the order matters as much as the content. The first step is not therapy — it is assessment and reassurance, because most children will never need the later steps at all. [1] [6]
Step 1 — Assess and triage
Identify the stressor, classify the picture as normal grief, PGD, adjustment disorder, MDD or PTSD, and assess suicidality, safeguarding and caregiver capacity. The classification determines everything downstream, so spend the time to get it right. [4] [12]
Step 2 — Immediate safety and supportive care
Give the family psychoeducation that grief is a normal process, not a disease, and that adaptation is the expected outcome. Restore sleep, routine and school attendance. Support the caregiver as the secure base. Run the safety pathway wherever risk has surfaced. [1] [11]
Step 3 — Watchful waiting and brief support
Most children adapt without formal therapy. Review at six to twelve weeks, keep the door explicitly open, and support the caregiver through the interval. This is active management, not neglect — the reassurance and the scheduled review are the treatment. [1] [10]
Step 4 — Evidence-based psychological therapy
When impairment persists past the threshold, deliver an evidence-based psychological therapy. CBT for PGD — the Boelen randomised clinical trial — is the pivotal paediatric evidence that grief-focused cognitive-behavioural therapy works for prolonged grief in children and adolescents, by targeting the three maintaining loops of avoidance, negative cognitions and the insecure bond. TF-CBT for childhood traumatic grief and traumatic separation, developed by Cohen and Mannarino from pilot work onward, addresses the trauma memory and the grief in parallel when the loss was traumatic. Family sessions amplify any child-focused work, because the active ingredient is often the supported caregiver, not the child's sessions alone. [6] [7] [8] [9]
Step 5 — Close the loop
Name the clinician who owns the plan, the follow-up date, the interim strategy, and the return precautions: re-emergent suicidality, new disclosures, functional decline, or placement breakdown. Treat any comorbid disorder on its own merits, coordinate school, the general practitioner and CAMHS, and do not "refer to CAMHS and forget." An open-loop referral leaves a vulnerable child exposed. [1] [13]
Specific Subtypes & Scenarios
Normal uncomplicated grief. Psychoeducation, caregiver support, watchful waiting, and the reassurance that adaptation is the expected outcome. Do not pathologise, and do not refer every bereaved child for counselling regardless of distress — the evidence does not support universal grief counselling. [1] [10]
Prolonged grief disorder. CBT for PGD is the evidence-based treatment; grief-focused cognitive-behavioural work targets avoidance and the negative cognitions, with family involvement. The Boelen trial showed clinically meaningful improvement, so a persistent grief that crosses the threshold is treatable, not a life sentence. [6]
Adjustment disorder with depressed mood. Brief supportive therapy, problem-solving and coping-skills work, and watchful resolution within about six months. Assess suicidality explicitly — this is the subtype and the age group where risk hides. [12]
Adjustment disorder with disturbance of conduct. The common-in-children subtype that gets misread as "just bad behaviour." Address the underlying stressor, use behavioural work, liaise with family and school, and assess safety actively. [12] [13]
Childhood traumatic grief and traumatic separation. When the death was violent, witnessed, or the loss a traumatic separation, deliver TF-CBT — the Cohen and Mannarino framework — addressing the trauma memory and the grief in parallel rather than forcing the child to choose one track. [7] [8] [9]
Parentally-bereaved child. Support the surviving caregiver as the intervention, offer grief-focused support, and monitor for PGD over the months that follow. The Bergman systematic review of support programs for parentally bereaved children and their caregivers found benefit in targeted programs, reinforcing the family-centred approach. [11]
Preschool-age child. Give simple, concrete, repeated explanations, address the magical thinking that the person will return, and support the caregiver to tolerate the regression that often accompanies early grief. [1] [3]
Adolescent. Respect the identity and existential dimensions of grief, assess suicidality and substance use explicitly, and offer a combination of individual and family work that lets the young person hold both autonomy and support. [12] [13]
Refugee, displaced or culturally diverse child. Deliver trauma- and bereavement-informed care with professional interpreters, and respect culturally appropriate grief rituals rather than imposing a Western "stages" frame. [1] [11]
Complications & Pitfalls
- Diagnosing prolonged grief disorder within the first months of a loss, before the duration threshold — pathologising normal grief.
- Missing adjustment disorder because the stressor was never elicited, or dismissing the conduct subtype as "just behaviour."
- Failing to assess suicidality in every case — adjustment disorder in adolescence carries elevated suicidality.
- Confusing PGD with MDD or PTSD and applying the wrong treatment.
- Starting an antidepressant to "treat" grief or an uncomplicated adjustment disorder itself.
- Universally referring all bereaved children to grief counselling regardless of distress — this medicalises normal grief and is not evidence-based.
- Ignoring the caregiver's own grief and capacity — an unsupported caregiver cannot be the secure base.
- Running grief-focused exposure work while the child is unsafe, actively suicidal, or the placement is unstable.
- Assuming a quiet, compliant child is coping — withdrawal and numbness can mask PGD.
- Open-loop referral to CAMHS with no interim plan, no safety-net, and no follow-up date.
Prognosis & Disposition
The prognosis of normal grief is excellent — the vast majority of bereaved children adapt without a disorder, which is the single most useful thing you can tell a frightened family. PGD is treatable: the Boelen randomised trial showed that CBT for PGD produces clinically meaningful improvement in children and adolescents, so a grief that has crossed the threshold is not permanent. Adjustment disorder is by definition time-limited, generally resolving within about six months of the stressor ending, although comorbidity and suicidality extend the course and must be actively managed. [1] [6]
Disposition after safety confirmed: supportive care and watchful waiting in the medical home, with escalation to evidence-based therapy if impairment persists past the threshold. Disposition when suicidality or a safeguarding concern surfaces: crisis and child-protection pathway, same-day supports, and stability before any grief-focused therapy. Disposition for an adolescent with active suicidality: acute mental-health pathway layered onto the grief or adjustment plan. [12] [13]
Markers of response are re-engagement with peers and play, improved sleep and appetite, reduced preoccupation and avoidance, and a return toward baseline function. Long CAMHS waitlists change the medical-home role: provide interim psychoeducation, caregiver support, school liaison, and safety planning rather than passive waiting. Comorbidity — depression, anxiety, PTSD — worsens prognosis and must be identified and treated on its own merits. A named owner and a closed loop matter, because an open referral leaves a suicidal or unsupported child exposed. [1] [6]
Special Populations
Parentally bereaved children need the surviving caregiver supported as the intervention, with monitoring for PGD and grief-focused support if impairment persists. Children bereaved by suicide, homicide or a violent or witnessed death need layered PTSD and trauma-informed care alongside the grief work — TF-CBT is the framework when the loss was traumatic. [7] [11]
Children with a pre-existing mental illness or prior trauma carry higher risk and a more complex recovery, and both tracks must run. Out-of-home-care and displaced or refugee children often carry multiple and cumulative losses, and need trauma- and bereavement-informed care with professional interpreters. Children with developmental disability or communication impairment may disclose less and present with overlapping behavioural change — adapt the grief assessment and explanation to their developmental level and avoid diagnostic overshadowing. [1] [13]
Adolescents need explicit suicidality and substance-use assessment and respect for the identity dimensions of grief. Culturally and linguistically diverse families need culturally appropriate grief rituals and non-stigmatising framing. Indigenous families need services that acknowledge intergenerational loss and trauma and are delivered in culturally safe ways. Rural and remote families should be offered telehealth-delivered psychological therapy rather than being told to wait. [11] [13]
Evidence, Guidelines & Regional Differences
Key evidence anchors for exam defence: [1] [6]
- Melhem 2007 J Am Acad Child Adolesc Psychiatry — phenomenology and correlates of complicated grief in children and adolescents; the foundational phenomenology. [1]
- Geronazzo-Alman 2019 JAACAP — grief, depression and PTSD are distinct constructs in bereaved children; supports separating the diagnoses. [2]
- Melhem and Brent 2019 (editorial, JAACAP) — grief in children: phenomenology and beyond; frames the field. [3]
- Boelen, Spuij and Lenferink 2019 J Affect Disord — comparison of DSM-5 persistent complex bereavement disorder and ICD-11 PGD criteria in help-seeking bereaved children. [4]
- Revet 2021 Eur J Psychotraumatol — peritraumatic distress predicts PGD severity after the death of a parent in children and adolescents. [5]
- Boelen, Lenferink and Spuij 2021 Am J Psychiatry — CBT for PGD in children and adolescents; the pivotal paediatric treatment RCT. [6]
- Cohen, Mannarino and Knudsen 2004 JAACAP — TF-CBT for childhood traumatic grief; pilot study. [8]
- Cohen, Mannarino and Staron 2006 JAACAP — modified CBT-CTG for childhood traumatic grief. [9]
- Cohen and Mannarino 2019 Child Abuse Negl — TF-CBT for childhood traumatic separation. [7]
- Rosner, Kruse and Hagl 2010 Death Stud — meta-analysis of interventions for bereaved children and adolescents. [10]
- Bergman, Axberg and Hanson 2017 BMC Palliat Care — systematic review of support programs for parentally bereaved children and caregivers. [11]
- Pelkonen 2005 Eur Child Adolesc Psychiatry — suicidality in adjustment disorder; clinical characteristics of adolescent outpatients. [12]
- Chung 2014 Asia Pac Psychiatry — adjustment disorder, sleep disturbance and suicidal ideation in adolescents. [13]
Grief- and adjustment-focused care is delivered through local CAMHS and primary-care stepped pathways, with school counsellors and grief-support organisations (for example Kenzie's Gift and Feel the Magic in Australia, and Skylight in New Zealand) providing non-clinical bereavement support alongside the medical home. Mandatory child-protection reporting thresholds are state, territory and nation specific — name the principle and the local service, and do not invent statute numbers. Aboriginal Community Controlled Health Services and culturally safe pathways are central for Aboriginal and Torres Strait Islander and Māori children, acknowledging intergenerational loss. [1] [11]
Controversies: the exact duration threshold for PGD in children (DSM-5-TR's 12 months for adults versus ICD-11's 6 months versus a developmental conceptualisation); whether universal grief counselling for non-distressed bereaved children is warranted (the evidence says no, and it risks medicalising normal grief); the role of pharmacotherapy (none first-line for grief or an uncomplicated adjustment disorder); and how to deliver evidence-based care when CAMHS waitlists are long and rural access is thin. [4] [10]
Exam Pearls
GRIEF
- Grief is wavelike with preserved positive affect between waves; MDD is pervasive anhedonia and worthlessness; PTSD is cue-driven intrusion and hyperarousal. [2]
- PGD requires a bereavement and a duration threshold; adjustment disorder follows any stressor within ~3 months and resolves within ~6 months — do not mix the two clocks. [4] [12]
- First-line treatment is psychoeducation, caregiver support and watchful waiting; there is no first-line medication for grief or an uncomplicated adjustment disorder. [1] [6]
- CBT for PGD works in children (Boelen 2021 RCT); TF-CBT treats childhood traumatic grief and traumatic separation (Cohen/Mannarino). [6] [7]
- Universal grief counselling for all bereaved children regardless of distress is not evidence-based — target the distressed and impaired. [10]
- Assess suicidality in every case — adolescent adjustment disorder carries elevated suicidality (Pelkonen). [12]
References
- [1]Melhem NM, Moritz G, Walker M, Shear MK, Brent D Phenomenology and correlates of complicated grief in children and adolescents. J Am Acad Child Adolesc Psychiatry, 2007.PMID 17420684
- [2]Geronazzo-Alman L, Fan B, Duarte CS, Layne CM, Wicks J, Guffanti G, Musa GJ, Hoven CW The Distinctiveness of Grief, Depression, and Posttraumatic Stress: Lessons From Children After 9/11. J Am Acad Child Adolesc Psychiatry, 2019.PMID 30877043
- [3]Melhem NM, Brent D Editorial: Grief in Children: Phenomenology and Beyond. J Am Acad Child Adolesc Psychiatry, 2019.PMID 30877044
- [4]Boelen PA, Spuij M, Lenferink LIM Comparison of DSM-5 criteria for persistent complex bereavement disorder and ICD-11 criteria for prolonged grief disorder in help-seeking bereaved children. J Affect Disord, 2019.PMID 30836282
- [5]Revet A, Suc A, Auriol F, Djelantik AAAMJ, Raynaud JP, Bui E Peritraumatic distress predicts prolonged grief disorder symptom severity after the death of a parent in children and adolescents. Eur J Psychotraumatol, 2021.PMID 34249245
- [6]Boelen PA, Lenferink LIM, Spuij M CBT for Prolonged Grief in Children and Adolescents: A Randomized Clinical Trial. Am J Psychiatry, 2021.PMID 33472391
- [7]Cohen JA, Mannarino AP Trauma-Focused Cognitive Behavioral Therapy for Childhood Traumatic Separation. Child Abuse Negl, 2019.PMID 30999167
- [8]Cohen JA, Mannarino AP, Knudsen K Treating childhood traumatic grief: a pilot study. J Am Acad Child Adolesc Psychiatry, 2004.PMID 15381889
- [9]Cohen JA, Mannarino AP, Staron VR A pilot study of modified cognitive-behavioral therapy for childhood traumatic grief (CBT-CTG). J Am Acad Child Adolesc Psychiatry, 2006.PMID 17135992
- [10]Rosner R, Kruse J, Hagl M A meta-analysis of interventions for bereaved children and adolescents. Death Stud, 2010.PMID 24479177
- [11]Bergman AS, Axberg U, Hanson E When a parent dies - a systematic review of the effects of support programs for parentally bereaved children and their caregivers. BMC Palliat Care, 2017.PMID 28797262
- [12]Pelkonen M, Marttunen M, Henriksson M, Lönnqvist J Suicidality in adjustment disorder--clinical characteristics of adolescent outpatients. Eur Child Adolesc Psychiatry, 2005.PMID 15959663
- [13]Chung MS, Chiu HJ, Sun WJ, Lin CN, Kuo CC, Huang WC, Chen YS, Cheng HP, Chou P Association among depressive disorder, adjustment disorder, sleep disturbance, and suicidal ideation in Taiwanese adolescent. Asia Pac Psychiatry, 2014.PMID 24357621