Paeds · mental-behavioural-and-psychosomatic
Pica and rumination disorder
Also known as Pica disorder · Rumination disorder · Rumination syndrome · Geophagia · Pagophagia · Childhood feeding and eating disorders
An age-aware fellowship approach to pica and rumination disorder: distinguish them from normal mouthing, culturally sanctioned practices and true vomiting; run a harm gate for lead, bezoar, helminth and malnutrition before assigning a label; treat reversible drivers such as iron and zinc deficiency; and replace the behaviour with supervision, response prevention and diaphragmatic breathing rather than punitive restraint.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A parent reports that their toddler eats paint chips, or an adolescent effortlessly brings food back up after meals and is losing weight. Both stories can be dismissed as a phase or as reflux, and both can hide serious medical complications. Your job is to sort the behaviour from its consequences, treat the harm first, and only then commit to a label and a behavioural plan. [1] [2]
H.A.R.M. G.A.T.E.
Overview & Definition
Picture three children in one clinic session. A fourteen-month-old mouths paper and fluff while teething. A six-year-old with sickle-cell disease chews foam and ice through the day. A fifteen-year-old brings lunch back up effortlessly, re-chews it, and has lost weight. The first is normal development. The second is pica driven by iron deficiency. The third is rumination disorder. Telling them apart is the whole task. [1] [13]
Pica is the persistent eating of non-nutritive, non-food substances for at least one month, in a way that is not developmentally or culturally appropriate and is not better explained by another disorder. Rumination disorder is the repeated, effortless regurgitation of recently swallowed food that is then re-chewed, re-swallowed or spat out, again not better explained by another condition. Both must cause clinically significant harm or impairment before the label sticks. [1] [2]
What makes these disorders easy to miss is that neither looks dangerous on the surface. Pica can hide inside ordinary toddler exploration, cultural practice, or the sensory world of an autistic child. Rumination can masquerade as reflux, vomiting or an eating disorder. The trap is reassurance before the complication screen is done. [2] [11]
Classification
Classify in two moves, not a long taxonomy. [1] [9]
First, run the harm gate. Ask whether an active complication is present: lead poisoning, bezoar with obstruction or perforation, helminth or Toxocara or Baylisascaris infection, iron or zinc deficiency, malnutrition, dental erosion, or weight loss. If any of these dominates, the label can wait and the complication drives the encounter. [2] [12] [15]
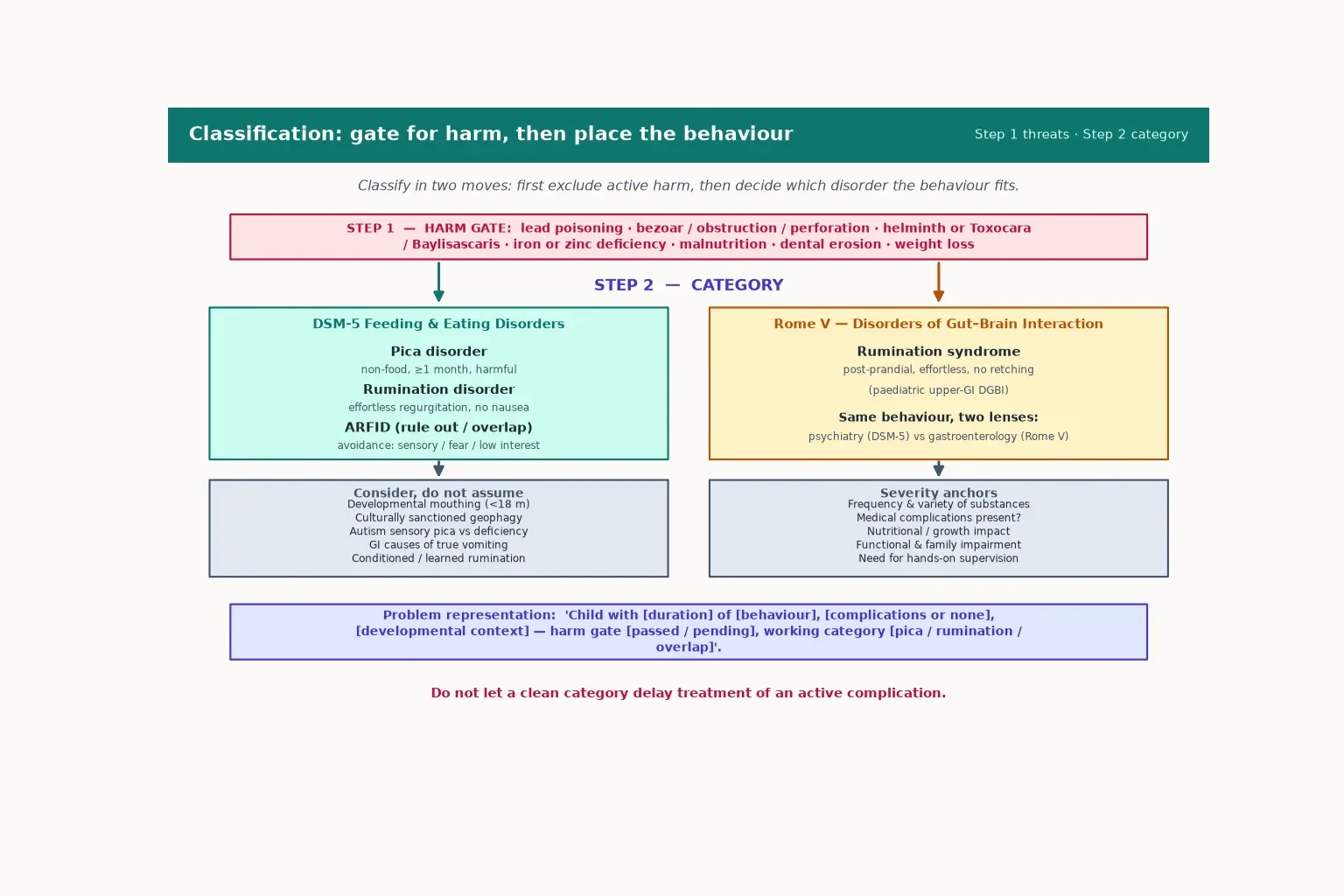
Second, place the behaviour. The DSM-5 lists pica, rumination disorder and avoidant/restrictive food intake disorder (ARFID) among the feeding and eating disorders. The Rome V framework calls rumination a disorder of gut–brain interaction (a paediatric upper-gastrointestinal DGBI). The same effortless regurgitation therefore wears two labels depending on whether a psychiatrist or a gastroenterologist is speaking, and you should be able to hold both in view. [9] [10]
Epidemiology & Risk Factors
Pica is common and commonly missed across childhood. It clusters where iron and zinc deficiency, sickle-cell disease, pregnancy, food insecurity, autism, intellectual disability and institutional care overlap. Toddlers explore with their mouths, but sustained, harmful non-food ingestion beyond the developmental window is the disorder. [1] [13]
Rumination is less common in general paediatrics but recognisable in adolescents, in children with cognitive impairment, and in young people under psychosocial stress. It is frequently mislabelled as treatment-resistant reflux for months before the effortless, post-prandial pattern is noticed. [7] [11]
Risk clustering
Poverty, older housing with lead paint, rural helminth exposure, and culturally sanctioned geophagy all shape who presents and how the behaviour should be interpreted. Migrant and refugee families may bring legitimate cultural practices that are not a disorder, and interpreters are essential when the history is subtle. [2] [12]
Pathophysiology
Pica and rumination are final-common-pathway behaviours with different, but interacting, drivers rather than a single proven mechanism in every child. [1] [4]
For pica, four drivers dominate. Nutrient deficiency — especially iron and zinc — may misdirect appetite cues toward non-food. Sensory and neurodevelopmental differences, particularly in autism and intellectual disability, make texture and ritual rewarding. Learning and reinforcement sustain the behaviour when anxiety falls or attention rises. Cultural and environmental factors, such as sanctioned geophagy or lead-paint housing, set the stage. [1] [4]
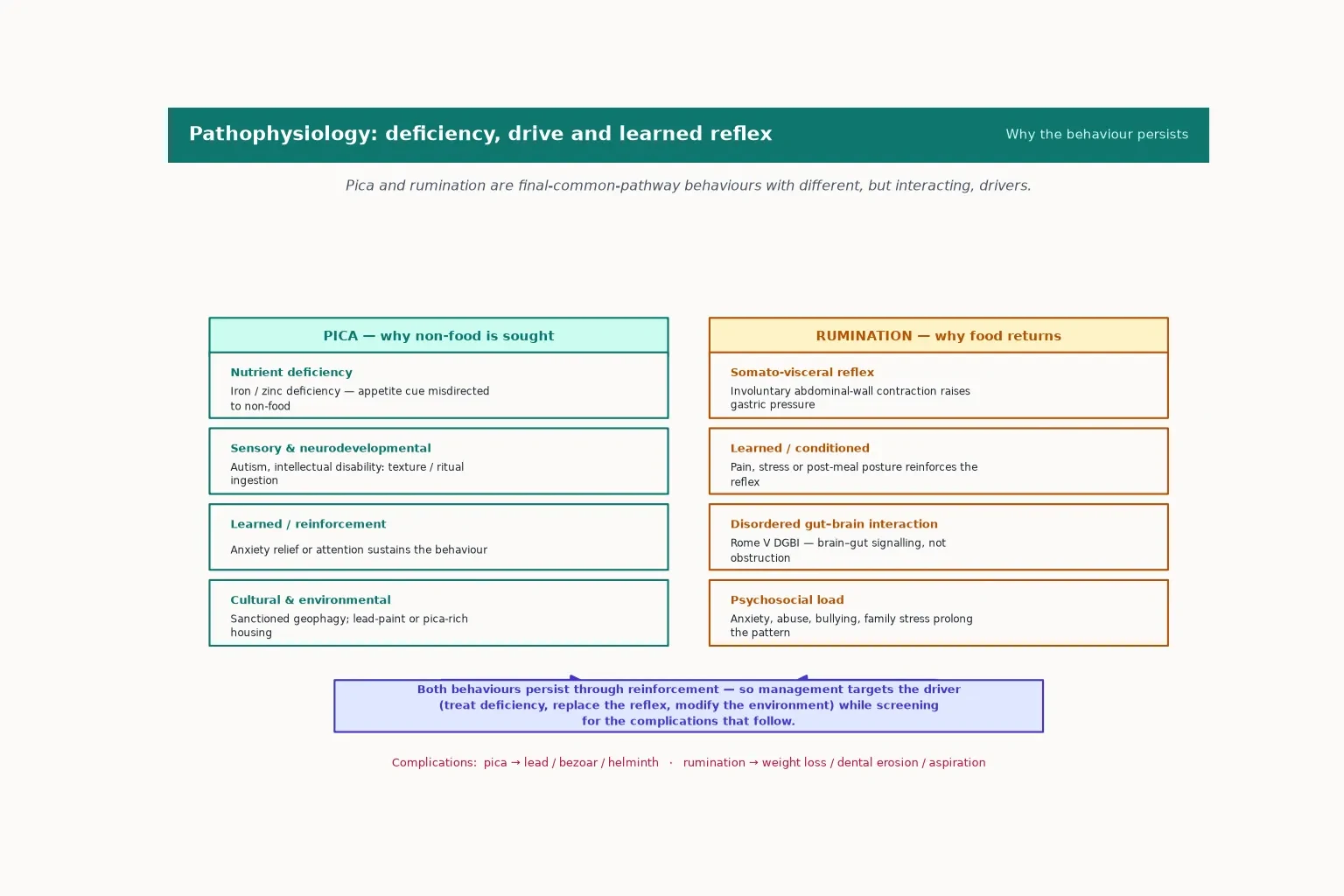
For rumination, the core mechanism is a somato-visceral reflex: an involuntary contraction of the abdominal wall raises intragastric pressure and pushes recently swallowed food back up, without nausea or retching. Rome V frames this as a disorder of gut–brain interaction rather than obstruction, and stress, pain or post-meal posture can condition the reflex until it runs automatically. [9] [10] [11]
The complications follow directly from the behaviour. Pica delivers lead, bezoars and helminths; rumination delivers weight loss, dental erosion and occasional aspiration. Understanding the mechanism is what makes the treatment logical: treat the driver, replace the reflex, modify the environment. [12] [15]
Clinical Presentation
Parents rarely open with the diagnosis. More often they report a complication — a child with abdominal pain, an odd eating habit, weight loss, or behavioural change — and the pica or rumination emerges only on direct questioning. [1] [2]
Pica may surface as the discovery of eaten objects, a craving for ice, starch, soap, soil or hair, or as a complication such as lead toxicity, constipation from a bezoar, or an unexplained anaemia. Rumination presents as effortless, post-prandial regurgitation: food returns to the mouth minutes after a meal, is re-chewed and re-swallowed or spat, and there is no nausea, no retching, and often weight loss or dental erosion over time. [6] [11]
Behaviour fingerprints
In autism and intellectual disability, the behaviour may be woven into sensory routines or limited communication, and caregivers are the key historians. In adolescents, pregnancy-related pagophagia, heavy menstrual iron loss, eating-disorder overlap and active concealment all change the history. Always ask directly, without judgement, and use a professional interpreter when needed. [2] [4]
Differential Diagnosis
Hold the common and the catastrophic together. The harm gate — lead poisoning, bezoar with obstruction or perforation, helminth infection including Baylisascaris, severe malnutrition, dental erosion and aspiration — must stay open before a label is assigned. [2] [12] [15]
Then separate the behaviour from its mimics. Developmental mouthing under eighteen months is normal, not pica. Culturally sanctioned geophagy is not a disorder in its context. Rumination must be distinguished from gastro-oesophageal reflux, cyclic vomiting syndrome, gastroparesis, eating-disorder purging, and true vomiting from obstruction or infection — the effortless, non-nauseated quality is the discriminator. ARFID overlaps when avoidance rather than ingestion or regurgitation is the core problem. [9] [10] [14]
Rumination versus its mimics
Keep safeguarding, neglect and abuse-related differentials open without premature labelling. New pica or rumination after family stress, a placement move, or disclosure of abuse changes both the assessment and the team you mobilise. [2]
Clinical & Bedside Assessment
Start with the body, not the label. Growth trajectory, hydration, dentition, abdominal signs, neurodevelopmental state and any suggestion of toxicity outrank a behavioural inventory, because a complication can be silent until it is severe. [1] [2]
The history should characterise the behaviour precisely: what is eaten or regurgitated, how often, in what setting, what triggers it, what reinforces it, and how much supervision is needed. Layer in deficiency clues (ice craving, fatigue, pallor, heavy menses), lead exposure (older housing, pica for paint or soil, behavioural change), helminth risk (rural or geophagy exposure), and the psychosocial context (school, family stress, trauma, safeguarding). [2] [12]
Examination is directed by the behaviour and its complications. Look for pallor and signs of iron deficiency, abdominal distension or a mass suggesting bezoar, dental erosion, neurological signs of lead toxicity, and growth faltering. For rumination, observing an effortless post-prandial episode — or asking the family to video one — can be diagnostic. [6] [8]
Assess function alongside symptoms: school attendance, play, self-care, and the impact on the family. Caregiver report and direct observation together matter most when the behaviour is concealed, which is common in adolescents and in children with limited communication. [4] [7]
Investigations
Tests should discriminate the active differential, not decorate the chart. After a clear, low-risk story with normal growth and examination, observation and early review may be enough — but the threshold for a targeted screen is low. [1] [2]
For pica, first-line testing targets the substance and context: blood lead level, full blood count, iron studies, zinc level where available, electrolytes, and a growth and developmental assessment. Add abdominal imaging when obstruction or a bezoar is suspected, dental review for erosion, helminth studies in relevant exposure, and a pregnancy test for adolescent girls with pagophagia. [2] [12]
For rumination, investigation supports the diagnosis and excludes mimics rather than proving the reflex. Check growth, exclude structural obstruction, and use high-resolution oesophageal impedance, pH monitoring or manometry where available to confirm the post-prandial, non-acidic pattern. Over-investigation is a pitfall: a normal endoscopy in an adolescent with effortless post-prandial regurgitation and weight loss should prompt rumination, not more tests. [8] [9]
A rising lead level, obstructive signs, severe malnutrition, or a result that does not fit the working label should force a rewritten problem representation and senior review. [12]
Management — Resuscitation
When a complication dominates, treat the complication first and keep the behavioural differential open. Lead poisoning with encephalopathy, bezoar with obstruction or perforation, severe malnutrition, and aspiration are the emergencies. [2] [12]
Remove the lead source and involve toxicology and public health for chelation decisions where indicated. Obtain urgent surgical review for a bezoar, obstruction or perforation. Treat helminth infection on the relevant protocol. Stabilise malnutrition with dietetic-led refeeding, and address aspiration risk with positioning and feeding review. [12] [15]
Senior, surgical, toxicology or mental-health activation should proceed early when local capability is exceeded, and a structured handover must preserve both the acute plan and the longer behavioural risk so the gain is not lost on transfer. [7]
Management — Definitive & Stepwise
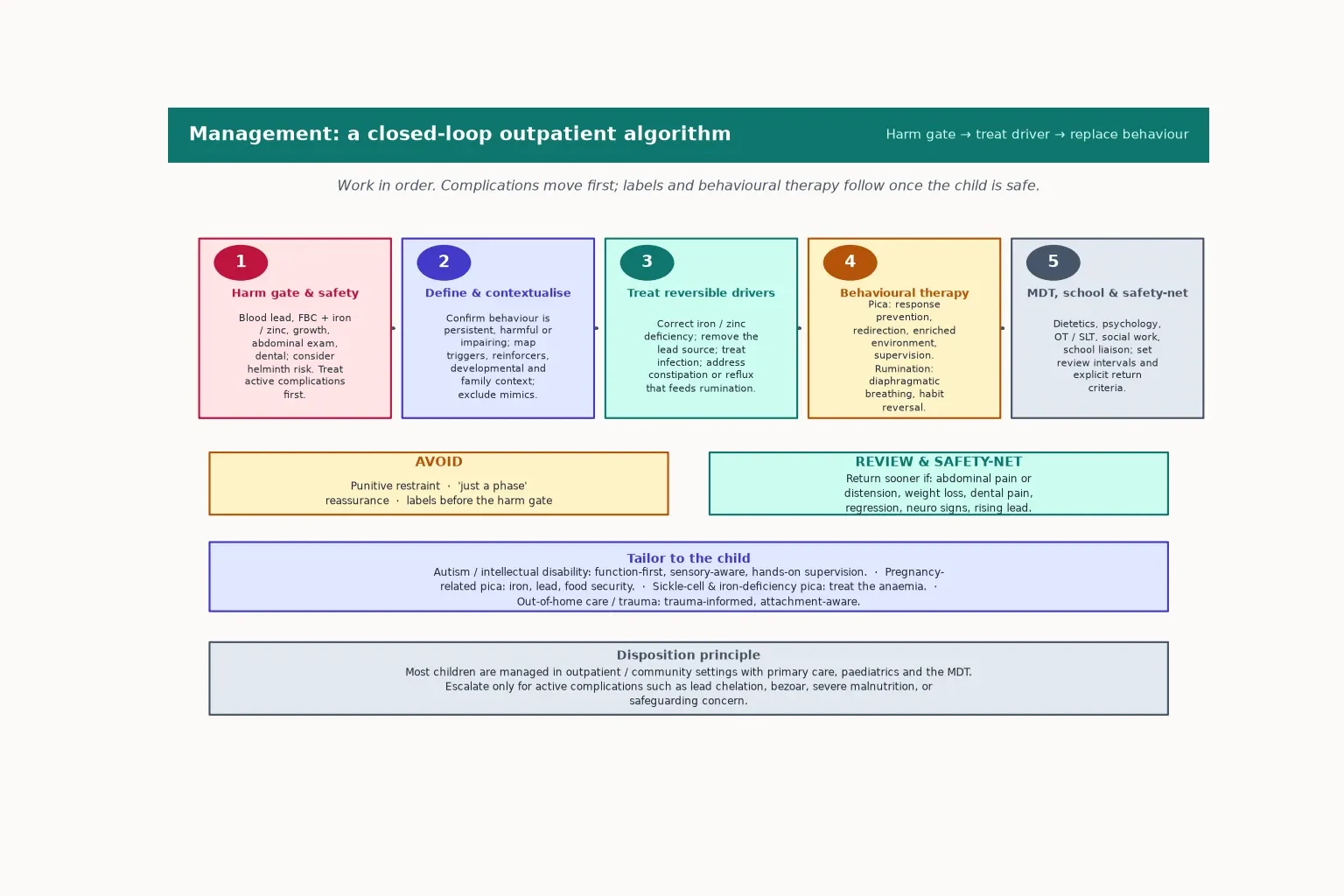
Once the harm gate is passed, care moves to a stepwise outpatient plan. The aim is to treat reversible drivers, replace the behaviour, support function, and safety-net explicitly. [1] [6]
Stepwise plan after the harm gate
Define and contextualise: confirm the behaviour is persistent, harmful or impairing; map triggers, reinforcers, developmental and family context; exclude mimics.
Treat reversible drivers: correct iron and zinc deficiency; remove the lead source; treat infection; address constipation and reflux that feed rumination.
Replace the behaviour: pica — response prevention, redirection, environmental enrichment, supervision and positive reinforcement; rumination — diaphragmatic breathing, habit reversal and post-meal strategy.
Coordinate the MDT: dietetics, psychology, occupational and speech-language therapy, social work and school liaison.
Safety-net: set review intervals and explicit return criteria — abdominal pain, weight loss, dental pain, regression, neuro signs or rising lead.
Correct iron and zinc deficiency and re-assess the behaviour — pica driven by deficiency often settles as the deficiency resolves. For pica that persists, behavioural therapy emphasises response prevention, redirection, an enriched environment, close supervision and positive reinforcement rather than punitive restraint, which does not work and can harm. [1] [4]
For rumination, diaphragmatic breathing is the first-line behavioural technique: it interrupts the abdominal-wall reflex by replacing it with a competing pattern, usually within weeks. Where breathing alone is insufficient, comprehensive cognitive-behavioural therapy and habit-reversal approaches augment it, and intensive outpatient protocols report good recovery in adolescents. [6] [7]
Diaphragmatic breathing (rumination)
Set review intervals, agree a school plan, and give the family explicit safety-net return criteria. Most children are managed in the community with a coordinated team; escalate only for an active complication or when safeguarding concerns emerge. [2] [7]
Specific Subtypes & Scenarios
Toddler with paint-chip eating in older housing. Run the lead gate. Check a blood lead level, examine neurodevelopment, identify the source, involve public health, and begin environmental and behavioural intervention. Do not reassure on age alone. [2] [12]
School-age child with sickle-cell disease and pica for foam or starch. Treat the anaemia and iron deficiency as the likely driver, monitor the behaviour over time, and coordinate with the haematology team — pica in sickle-cell disease is common and tracks with healthcare use. [13]
Adolescent girl with ice craving, heavy menses and fatigue. This is classic iron-deficiency pica. Check a full blood count and iron studies, treat the deficiency, address menstrual blood loss, and re-assess the craving as iron stores recover. [1]
Adolescent with effortless regurgitation and weight loss
This is rumination syndrome until proven otherwise, not treatment-resistant reflux. Confirm the effortless, post-prandial, non-nauseated pattern, exclude structural obstruction, and start diaphragmatic breathing with a therapist. Most adolescents recover with an intensive outpatient protocol; avoid endless repeat endoscopies. [6] [7] [8]
Child with autism and persistent pica for non-food items. Use a function-first, sensory-aware approach: hands-on supervision, environmental enrichment, response prevention, and positive reinforcement, with the multidisciplinary team around the family. Screen for Baylisascaris where there is pica and raccoon exposure, as devastating neurological infection has been described. [4] [15]
Child in out-of-home care with new rumination after family stress. Assess trauma and safeguarding alongside the gut. Treat the rumination behaviourally, and mobilise psychology and social work; the reflex often settles as the stressor is addressed. [2] [7]
Complications & Pitfalls
The complications are the harm gate by another name, and missing them is the cardinal error. Lead poisoning, bezoar with obstruction or perforation, helminth or Baylisascaris infection, severe malnutrition, dental erosion and aspiration all sit behind a behavioural label that looks benign. [2] [12] [15]
The common pitfalls are reassuring on "just a phase" when growth is faltering or dentition is eroding; missing iron or zinc deficiency that is both driver and treatment; using punitive restraint or forced re-feeding instead of behavioural replacement; and confusing rumination with reflux, cyclic vomiting or eating-disorder purging. [1] [11]
Premature psychiatric labelling before the complication and deficiency search is closed, and ignoring psychosocial stressors, abuse or safeguarding concerns, both distort the plan. A fragmented handover that drops the behavioural risk after an acute admission loses the gain. [2] [4]
Prognosis & Disposition
Most children do well once the driver is treated and the behaviour is replaced. Deficiency-driven pica often resolves as iron or zinc stores recover, and rumination responds well to diaphragmatic breathing and a coordinated outpatient protocol, with the majority of adolescents improving within weeks to months. [1] [6] [7]
Same-day admission is reserved for active complications — lead encephalopathy or chelation, bezoar with obstruction or perforation, severe malnutrition needing refeeding, or safeguarding concerns. Everything else is managed in the community with primary care, paediatrics and the multidisciplinary team. [2] [12]
School, supervision and activity plans support recovery without harm, and long-term supports matter most for autism- or intellectual-disability-associated pica and for severe or recurrent rumination. A clear response after first-line intervention reassures; deterioration or a rising lead level mandates escalation. [4] [13]
Special Populations
Infants and toddlers. Separate developmental mouthing from pathological pica, and run the complication search first. Rumination is rare in this group but possible, and must be distinguished from possetting and reflux. [1] [9]
Autism and intellectual disability. Use a function-first, sensory-aware approach with hands-on supervision, environmental enrichment and positive reinforcement. The behaviour often persists and demands long-term, individualised support rather than a short fix. [4] [15]
Pregnant adolescents. Screen for iron deficiency and lead exposure, address food security, and treat the anaemia as the driver of pagophagia. [1] [12]
Sickle-cell disease and chronic iron deficiency. Treat the anaemia as the driver, and track pica behaviour longitudinally with the haematology team. [13]
Migrant, refugee and Indigenous families. Interpret geophagy with cultural humility, use a professional interpreter, and weigh environmental lead and helminth exposure in the risk assessment. [2] [12]
Out-of-home care and trauma-exposed children. Assess trauma and safeguarding alongside the behaviour, avoid diagnostic overshadowing, and keep the family and care team in view. [2] [7]
Evidence, Guidelines & Regional Differences
The Pica, ARFID and Rumination Disorder Interview (PARDI) gives clinicians a structured, multi-informant way to assess these behaviours across the lifespan, and it is fair game in exams as the standardised assessment tool. [5]
Rome V reframes rumination as a paediatric disorder of gut–brain interaction, moving the conversation from "psychiatric" to "brain–gut" and aligning paediatric and gastroenterology practice. The Murray proof-of-concept trial showed that comprehensive cognitive-behavioural therapy augments diaphragmatic breathing, and the Lamparyk and Khoo paediatric studies describe realistic outpatient recovery for adolescents. [6] [7] [8] [9]
The psychiatric comorbidity literature around childhood pica (Rubino) and the neurology review (Schnitzler) remind candidates that pica is rarely an isolated behaviour — concurrent and sequential disorders are common and shape the plan. Lead-exposure public-health data (Dave) and the Baylisascaris case report (Lipton) anchor the complication discussion in real harm rather than theoretical risk. [3] [4] [12] [15]
Use local public-health lead and housing pathways for paint-chip and soil pica, and culturally safe conversations with Aboriginal and Torres Strait Islander families around geophagy and environmental health. Behavioural therapy access runs through primary care, paediatrics and allied health, coordinated with school liaison. [1] [12]
UKHSA lead-exposure investigations and NICE-aligned eating-disorder and ARFID pathways shape management. The PARDI tool and British Paediatric Surveillance Unit evidence inform service design, and rumination is increasingly recognised within paediatric gastroenterology. [2] [5]
AAP lead-screening and iron-deficiency guidance drive the pica work-up, and rumination is framed within paediatric gastroenterology and psychiatry practice. Behavioural therapy access varies by insurance and region, which affects realistic timelines. [1] [14]
Align lead, iron and behavioural-therapy access with provincial primary-care and paediatric pathways, and keep the harm gate universal across rural and remote settings. [2] [12]
Exam Pearls
- Harm gate before label: lead, bezoar, helminth and malnutrition come first. [2]
- Pica is non-food, non-nutritive, for at least one month, and harmful — developmental mouthing under eighteen months is normal. [1]
- Rumination is effortless, post-prandial, no nausea, no retching — not vomiting and not reflux. [9]
- Iron and zinc deficiency are common, treatable drivers of pica — correct them and re-assess. [1] [13]
- Diaphragmatic breathing replaces the rumination reflex; punitive restraint does not work for pica. [6]
- Rome V calls rumination a gut–brain interaction; DSM-5 calls rumination disorder a feeding and eating disorder — same behaviour, two lenses. [9] [10]
- Pica is rarely isolated: expect concurrent and sequential psychiatric comorbidity. [3]
- Most children are managed outpatient with the MDT; admit only for active complications. [2] [7]
High-yield anchors
References
- [1]Leung AKC Pica: A Common Condition that is Commonly Missed - An Update Review Current pediatric reviews, 2019.PMID 30868957
- [2]McNaughten B Fifteen-minute consultation: the child with pica Archives of disease in childhood. Education and practice edition, 2017.PMID 28487433
- [3]Rubino LG Pica in Childhood: Concurrent and Sequential Psychiatric Comorbidity The International journal of eating disorders, 2025.PMID 40574647
- [4]Schnitzler E The Neurology and Psychopathology of Pica Current neurology and neuroscience reports, 2022.PMID 35674869
- [5]Bryant-Waugh R Development of the Pica, ARFID, and Rumination Disorder Interview, a multi-informant, semi-structured interview of feeding disorders across the lifespan: A pilot study for ages 10-22 The International journal of eating disorders, 2019.PMID 30312485
- [6]Murray HB Comprehensive Cognitive-Behavioral Interventions Augment Diaphragmatic Breathing for Rumination Syndrome: A Proof-of-Concept Trial Digestive diseases and sciences, 2021.PMID 33175346
- [7]Lamparyk K Protocol and Outcome Evaluation of Comprehensive Outpatient Treatment of Adolescent Rumination Syndrome Journal of pediatric gastroenterology and nutrition, 2022.PMID 35687569
- [8]Khoo JS Impact of diagnostic testing on outcomes of children with rumination syndrome Journal of pediatric gastroenterology and nutrition, 2025.PMID 39803885
- [9]Rosen R Rome V Pediatric Upper Gastrointestinal Disorders of Gut-Brain Interaction Gastroenterology, 2026.PMID 41713704
- [10]Sawada A Belching Disorders and Rumination Syndrome: A Literature Review Digestion, 2024.PMID 37844547
- [11]Pomenti S Current state of rumination syndrome Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus, 2024.PMID 38741462
- [12]Dave M Lead exposure sources and public health investigations for children with elevated blood lead in England, 2014 to 2022 PloS one, 2024.PMID 39024259
- [13]Gresko S Longitudinal Trends of Pica Behaviors, Behavioral Support, and Healthcare Utilization in Pediatric Sickle Cell Disease Pediatric blood & cancer, 2026.PMID 41834333
- [14]Kambanis PE Prospective 2-Year Course and Predictors of Outcome in Avoidant/Restrictive Food Intake Disorder Journal of the American Academy of Child and Adolescent Psychiatry, 2025.PMID 38718975
- [15]Lipton BA Baylisascaris procyonis Roundworm Infection in Child with Autism Spectrum Disorder, Washington, USA, 2022 Emerging infectious diseases, 2023.PMID 37209678