Paeds · mental-behavioural-and-psychosomatic
Post-traumatic stress disorder and trauma responses
Also known as Paediatric PTSD · Childhood post-traumatic stress disorder · Acute stress disorder in children · Complex trauma and developmental trauma · Trauma-focused care
Fellowship guide to post-traumatic stress disorder and the wider trauma-response spectrum in children and adolescents: the reaction-to-disorder continuum, DSM-5-TR and ICD-11 structure, preschool subtype, trauma-informed assessment, risk factors that predict persistence, stepped care with trauma-focused CBT first-line, watchful waiting, no single-session debriefing, and a closed safeguarding and disposition plan across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent brings a seven-year-old who, three weeks after a serious car crash, will not get into a car, wakes screaming, and has stopped concentrating at school. The question is not "does he have PTSD?" but "is this an expected reaction still within the recovery window, or a disorder that has taken hold?" Most frightened children settle with time and support; the minority who do not are the ones your assessment must find. [7] [8]
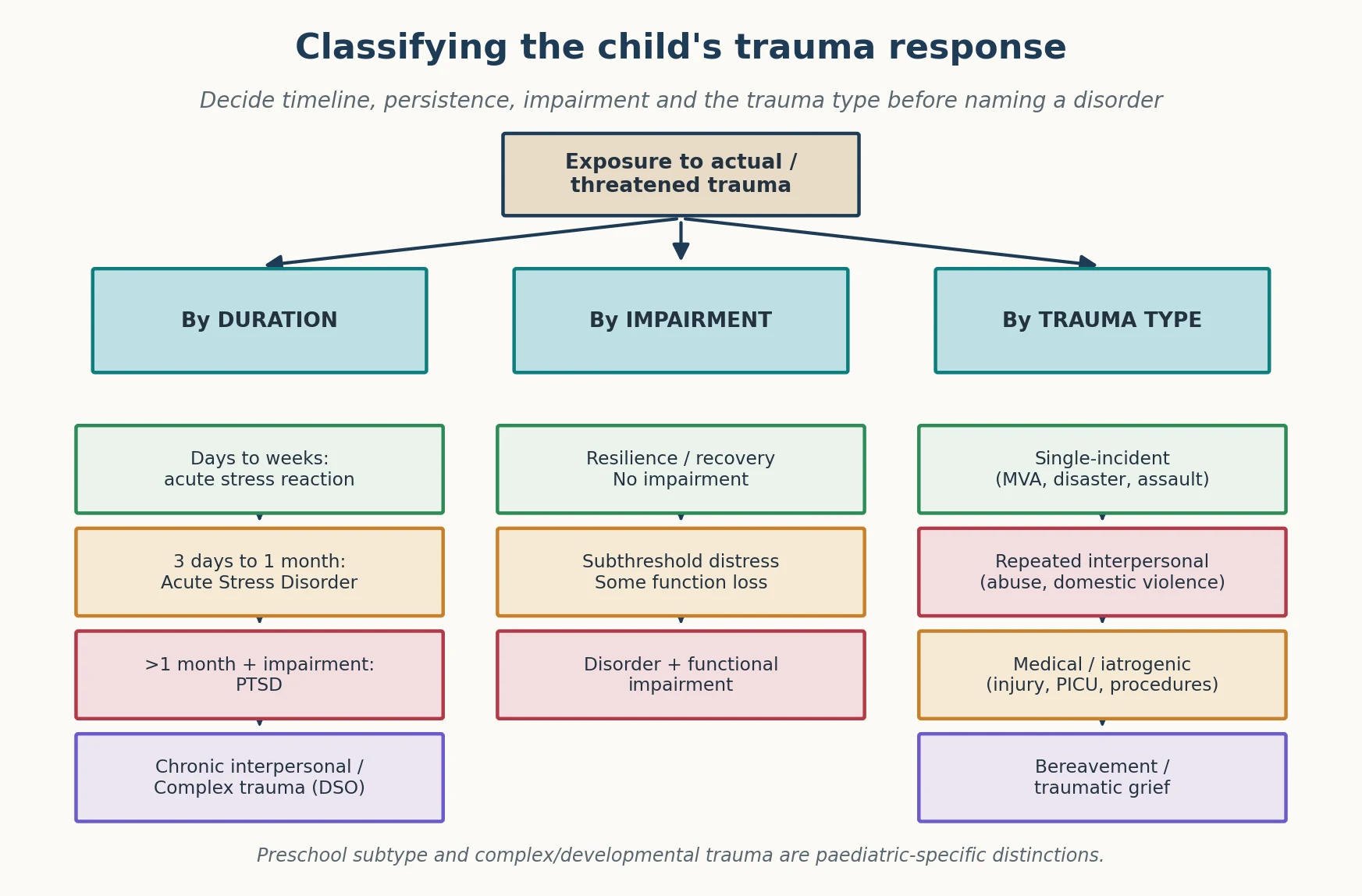
A trauma response is the full spectrum of psychological reactions to an event involving actual or threatened death, serious injury, or sexual violence — whether experienced directly, witnessed, learned about, or encountered repeatedly through aversive details. It runs from a brief, expected acute stress reaction in the first hours and days, through Acute Stress Disorder (three days to one month), to post-traumatic stress disorder (PTSD) when symptoms persist beyond one month and cause functional impairment. [12]
In children the picture is developmental. A preschooler does not narrate a "flashback"; they re-enact the event in repetitive play, develop new fears, regress, or cling. An adolescent may look sullen and irritable and self-medicate with alcohol rather than report intrusion. Because children express trauma through behaviour and the body far more than through verbal report, PTSD is easily missed — or wrongly labelled as ADHD, oppositional behaviour, or "just naughty". [2] [12]
Deep technique for suicide risk lives on the linked self-harm leaf, attachment-specific disorders on the attachment leaf, and acute crisis disposition on the emergency mental-health leaf. This page owns the trauma-response spine from recognition to closed-loop care. [1] [11]
Classification
Classify along three axes before you name a disorder: how long symptoms have lasted, how impairing they are, and what kind of trauma drove them. The same cluster of symptoms means something different at day 3, day 20, and month 4. [11] [12]
By duration
| Time since event | Label | Default move |
|---|---|---|
| Hours to days | Acute stress reaction | Psychological first aid, watchful waiting |
| 3 days to 1 month | Acute Stress Disorder | Consider early trauma-focused CBT if distressing |
| More than 1 month + impairment | PTSD | Trauma-focused CBT (first-line) |
| Months of chronic interpersonal adversity | Complex / developmental trauma | Phased, attachment-focused treatment |
By diagnostic system
DSM-5-TR frames PTSD around four symptom clusters — intrusion, avoidance, negative alterations in cognition and mood, and alterations in arousal and reactivity — following a Criterion-A exposure, lasting more than one month, and causing impairment. It carries a preschool subtype for children six years and younger, which requires fewer symptoms and weights observable behaviour over verbal report. ICD-11 is leaner: three core elements (re-experiencing, avoidance, a sense of current threat), with a separate Complex PTSD diagnosis that adds a disturbance in self-organisation — affect dysregulation, a negative self-concept, and disturbed relationships — seen after chronic interpersonal trauma. [2] [9]
Single-incident PTSD versus complex / developmental trauma
- One discrete event: crash, assault, disaster, medical event
- Defined intrusion-avoidance-arousal clusters
- Time-limited TF-CBT often resolves it
- Preschool and adolescent subtypes apply
- Chronic, interpersonal, often caregiver-mediated
- Adds self-organisation disturbance: affect, self, relationships
- Attachment and regulation disrupted early
- Needs phased, longer, attachment-focused care
Epidemiology & Risk Factors
Trauma exposure is common in childhood, but PTSD is not. The Alisic meta-analysis pooled rates of PTSD in trauma-exposed children and adolescents and found striking heterogeneity by trauma type: rates are far higher after interpersonal and sexual violence, refugee and war exposure, and disasters than after single-incident accidents. The teaching point for a viva is that the great majority of exposed children do not develop PTSD, so recovery is the expected baseline and persistence is what demands explanation. [7]
What predicts the minority who persist? The Trickey meta-analysis identified the risk factors that hold up across studies: perceived life threat and peri-traumatic fear or dissociation at the time of the event, lack of social support afterwards, prior psychopathology, severity and repetition of exposure, and female sex in adolescence. Protective forces point the other way — secure attachment, a calm and capable caregiver, a swift return to routine, and social support. [8]
Cumulative adversity matters. A child carrying multiple adverse experiences, poly-victimisation, or an unsafe placement has both higher baseline risk and a more complex presentation, which is why out-of-home care, family violence, refugee status and socioeconomic disadvantage shift the whole plan. The child's caregiver is part of the risk equation: untreated parental trauma or mental illness predicts worse child outcomes and must be addressed as part of the child's plan. [7] [8]
Pathophysiology
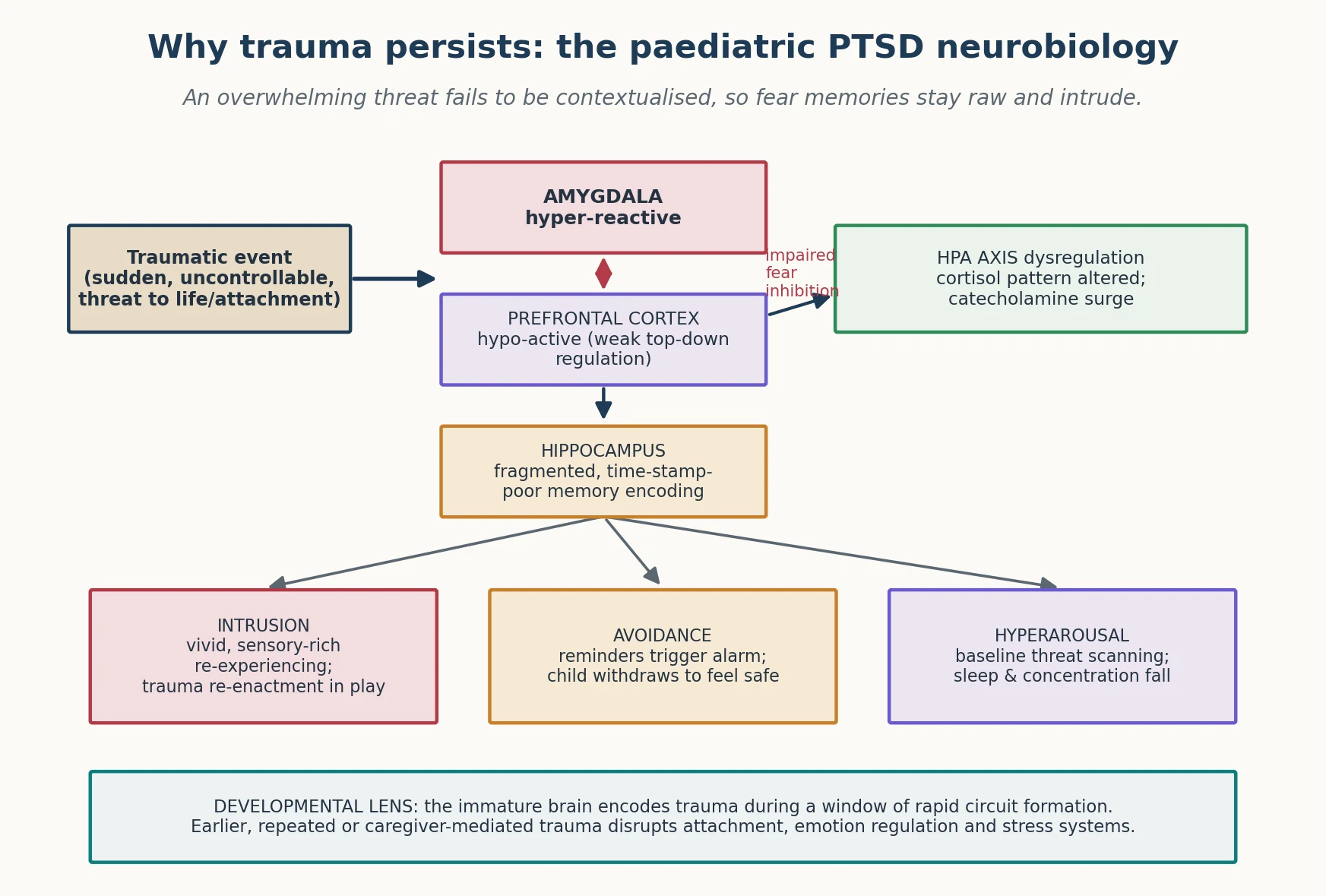
Picture the car-crash child again. In the moment, the threat is sudden, uncontrollable, and overwhelming. The brain encodes it as a vivid, sensory-rich fragment — the smell of petrol, the sound of metal — without a clean "time-stamp" placing it safely in the past. When something later echoes that fragment, the memory intrudes as if the crash is happening now. That sense of current threat is the engine of PTSD, and it is the frame Ehlers and Clark used to explain why trauma persists. [12]
The neuroscience is consistent with that experience. The amygdala — the threat detector — is hyper-reactive, firing fast and loud. The ventromedial prefrontal cortex, which normally tells the amygdala "this is a memory, not a danger," is under-active, so fear extinction fails. The hippocampus, which should contextualise the memory and pin it to time and place, encodes it in a fragmented way. The HPA axis and cortisol pattern are dysregulated, leaving the child primed. The net result is a brain that has learned the wrong lesson too well and cannot unlearn it without help. [12]
Development changes everything. Trauma encoded during a window of rapid circuit formation — when attachment, emotional regulation and the stress response are being calibrated — leaves deeper marks than the same event in an adult brain. That is why chronic, caregiver-mediated trauma disrupts not just memory but the architecture of self-regulation and relationship: the neurobiology of complex trauma. Medical events can condition the same circuits: a child who has been intubated, restrained, or repeatedly in pain in a PICU can develop a trauma response to the care that saved them. [2] [9]
Clinical Presentation
Parents rarely lead with "PTSD." They bring regression, nightmares, refusal, tummy aches, or a child who "isn't themselves." Your history converts that into the four clusters. [2] [12]
Intrusion appears as nightmares, intrusive memories, and flashbacks — but in young children, equally as repetitive traumatic play, drawings, or re-enactment, because children dramatise what they cannot narrate. Avoidance shows up as steering around the place, the person, the topic; emotional numbing; and withdrawal. Negative alterations in cognition and mood surface as guilt, shame, a foreshortened sense of the future, and detachment from people who used to matter. Arousal drives the sleep problems, irritability, concentration collapse, hypervigilance, and exaggerated startle that families actually notice first. [5] [12]
The developmental variants are where mistakes happen. Preschoolers regress — bedwetting, clinging, new fears, loss of recently won skills. School-age children show academic decline, somatic complaints, and behavioural change. Adolescents look closer to the adult picture but may express distress through irritability, risk-taking, and substance use, which hides the trauma rather than reveals it. Always ask what the school, the other parent, and the child separately tell you — multi-informant data is how you find the pattern. [2] [6]
Differential Diagnosis
Build the differential in layers: other trauma-response states, the anxiety and mood disorders that overlap, the disruptive-behaviour labels that mimic, and the medical and substance causes that must not be missed. [7] [13]
| Pattern | Favours | Against / distinguish |
|---|---|---|
| Symptoms clearing within days, no impairment | Expected acute stress reaction | Persistence beyond one month |
| Distress after a non-Criterion-A stressor | Adjustment disorder | True Criterion-A trauma present |
| Loss and yearning after a death, meeting grief criteria | Prolongued / traumatic grief | Intrusion-avoidance-arousal cluster dominates |
| Avoidance of reminders, no broader trauma cluster | Specific phobia / anxiety disorder | Full PTSD cluster after trauma |
| Low mood, anhedonia dominating | Major depressive disorder | Intrusion and hyperarousal prominent |
| New inattention, impulsivity, no trauma | ADHD | Onset after a frightening event; night-time intrusion |
| Irritability and aggression, no trauma history | ODD / conduct pathway | Hypervigilance, startle, re-enactment |
| Adolescent using substances to cope | Substance use disorder | Trauma driving the self-medication |
| Head injury then concentration and sleep problems | TBI / post-concussion syndrome | Symptoms predated the injury |
| Episodes with alteration of awareness | Dissociative / non-epileptic seizures | True PTSD intrusion between episodes |
The two errors examiners love to probe are mirror-images: forcing a PTSD label onto a normal reaction that will resolve, and missing PTSD entirely because the child "just looks oppositional" or "must have ADHD." When a behaviour label does not fit the natural history — new onset, trauma-linked triggers, night-time intrusion — return to the trauma history. [7] [12]
Clinical & Bedside Assessment
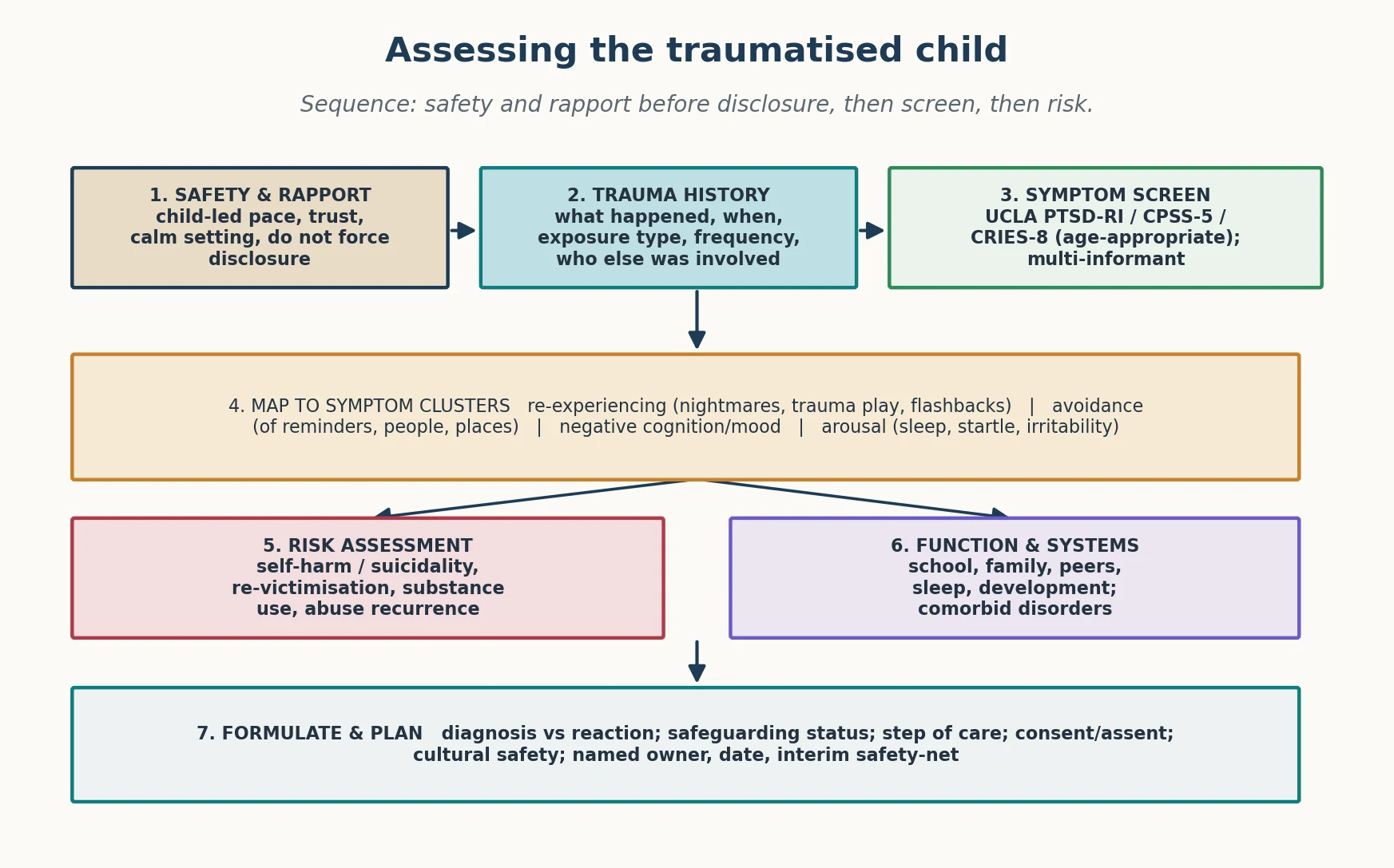
Lead with safety and rapport. A traumatised child who is pushed to disclose before trust is established can be re-traumatised in your consulting room. Pace the interview, give choice, and let the child lead how much detail they offer; your job is to assess, not to investigate. [12]
Trauma-informed assessment sequence
Safety and rapport
Calm setting, child-led pace, choice, do not force disclosure; confirm immediate safety.
Trauma history
What happened, when, exposure type, frequency, who was involved, perceived life threat, peri-traumatic dissociation.
Symptom clusters
Map intrusion, avoidance, negative cognition/mood, arousal with developmental framing.
Standardised screen
UCLA PTSD Reaction Index, Child PTSD Symptom Scale, or CRIES-8, age- and language-appropriate; multi-informant.
Risk and function
Self-harm, suicidality, re-victimisation, ongoing abuse; school, family, peers, sleep, development.
Formulate and plan
Diagnosis vs reaction, safeguarding status, step of care, consent/assent, named owner and safety-net.
Standardised measures sharpen the picture but do not replace clinical judgement. The UCLA PTSD Reaction Index and the Child PTSD Symptom Scale carry the strongest psychometric evidence for school-age children and adolescents; the CRIES-8 is a brief, widely used screen. Use the version matched to the child's age and language, and always gather the caregiver's and teacher's view alongside the child's — discordance is itself data. [5] [6]
Examine the child too. After abuse, look for signs that need a safeguarding pathway; after medical trauma, document the baseline. Ask directly and calmly about suicidality and self-harm, about whether the child is still safe at home, and about substance use in adolescents. Assess the caregiver — an untreated parent with their own trauma cannot run an exposure-based programme tonight, and your plan must match real life. [9] [13]
Investigations
PTSD is a clinical diagnosis. There is no blood test, scan, or electrophysiological marker that confirms it, and the commonest investigation error is the shotgun panel ordered for "behaviour." Your core investigations are the structured history, the standardised measure, and multi-informant reports. [5] [12]
Investigate when the story points somewhere. After a head injury with concentration and sleep problems, address traumatic brain injury and post-concussion syndrome rather than assuming pure PTSD. Consider thyroid disease, a primary sleep disorder, or non-epileptic / dissociative episodes when the picture is atypical. When sexual or physical abuse is disclosed, the safeguarding forensic examination is a separate, protocolised pathway — arrange it, do not improvise it. [7] [13]
Neuroimaging and EEG are not first-line for PTSD symptoms without focal neurological signs or seizures. Screen actively for the comorbidities that change the plan — depression, anxiety, ADHD, and adolescent substance use — because treating PTSD while ignoring a comorbid disorder is a common cause of non-response. Where trauma and a developmental disorder coexist, run developmental assessment in parallel rather than forcing an either/or choice. [7] [12]
Management — Resuscitation
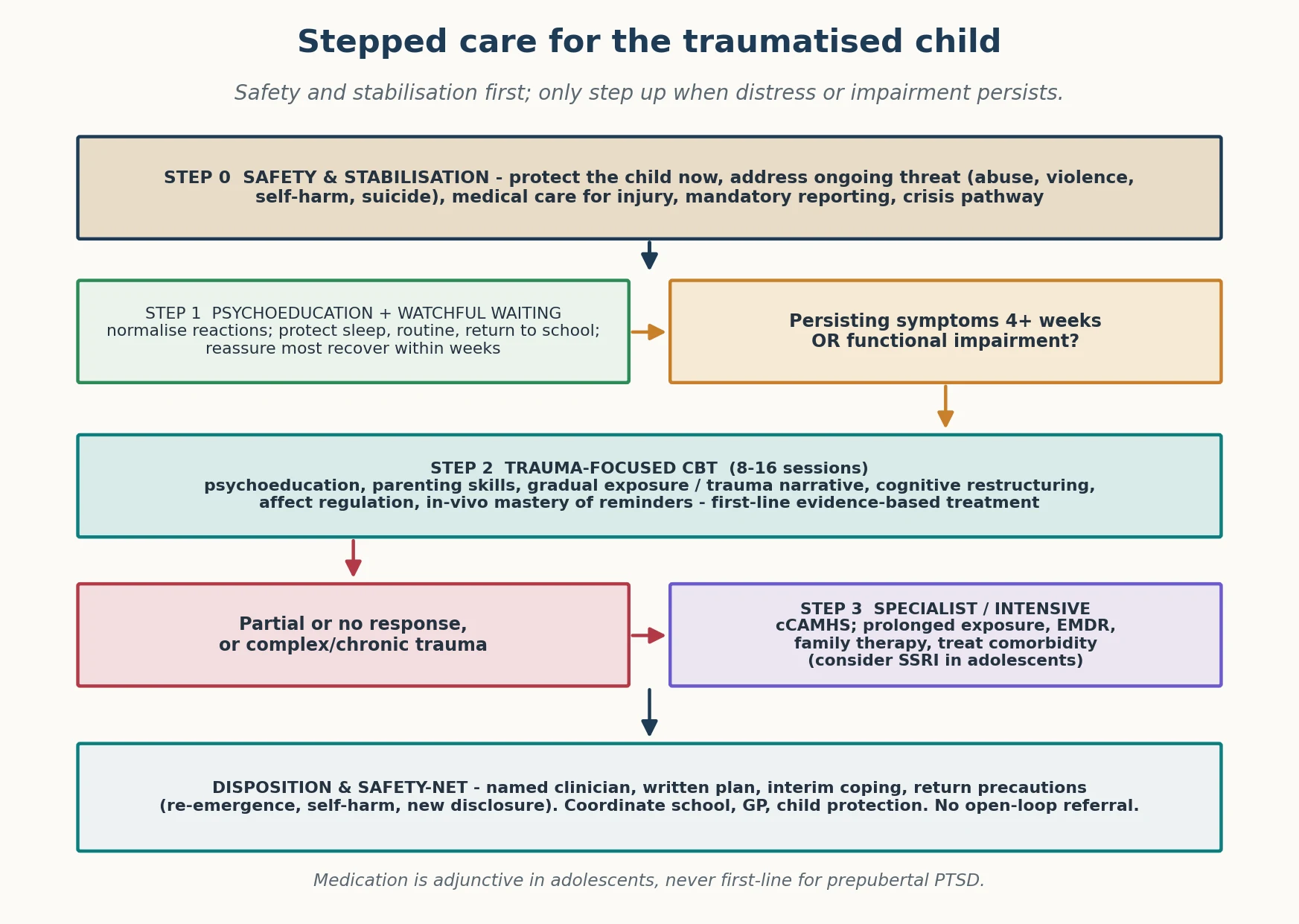
"Resuscitation" in a trauma-response presentation means immediate safety and the end of ongoing threat, not a drug or a debriefing session. [11] [13]
In the acute aftermath of a frightening event, deliver psychological first aid — comfort, safety, practical needs, and reconnection to supports — and deliberately avoid single-session debriefing. The evidence does not support routine debriefing as prevention, and some data suggest it can increase later symptoms; the safer default is watchful monitoring. Make a same-day safety plan with the family: supervision, restriction of means, who to call, and where to go. [10] [11]
Management — Definitive & Stepwise
Stepped care is the frame, and the order matters as much as the content. Safety and stabilisation come before any trauma work. [1] [11]
Step 1 — Psychoeducation and watchful waiting
For the first month after trauma, NICE recommends active monitoring rather than immediate treatment, because most children recover spontaneously. Educate the family that reactions are expected, protect sleep and routine, support return to school, and give a clear safety-net for what should bring them back sooner. [11]
Step 2 — Trauma-focused CBT (first-line)
When symptoms persist beyond four weeks or cause impairment, trauma-focused cognitive behavioural therapy (TF-CBT) is the first-line definitive treatment. The Cohen multisite randomised trial established TF-CBT's superiority over supportive therapy for sexual-abuse-related PTSD in children, and the evidence base has broadened across trauma types. A full course runs roughly eight to sixteen sessions and blends psychoeducation, parenting skills, gradual exposure and a trauma narrative, cognitive restructuring, affect regulation, and in-vivo mastery of avoided reminders. [1] [12]
Developmental adaptation is part of the treatment, not an add-on. TF-CBT works for preschool children — Scheeringa demonstrated it for three-to-six year-olds — and a stepped-care version is non-inferior to standard care in young children, which matters where specialist capacity is thin. For school delivery, the CBITS programme brings evidence-based group TF-CBT to children in the education setting, improving access for ethnically and socioeconomically diverse families. [2] [3] [4]
Step 3 — Specialist and intensive
For partial or non-response, or for complex and developmental trauma, step up to specialist child and adolescent mental-health services. Options include prolonged exposure, eye-movement desensitisation and reprocessing (EMDR), narrative exposure therapy, and attachment- and trauma-focused family therapy, with explicit treatment of comorbidity. An SSRI may be considered as an adjunct in adolescents with persistent symptoms or comorbid depression — but it is not first-line, and it is not appropriate as a stand-alone treatment for prepubertal PTSD. The adult Cochrane evidence underpinning trauma-focused therapies and EMDR extends to adolescents under specialist guidance. [10] [12]
Step 4 — Close the loop
Name the clinician who owns the plan, the date of follow-up, the interim coping strategy, and the return precautions: symptom re-emergence, new self-harm, new disclosures, or abuse recurrence. Coordinate child protection, school, and the general practitioner. Do not "refer to CAMHS and forget" — an open-loop referral leaves a vulnerable child exposed. [11] [13]
Specific Subtypes & Scenarios
Acute stress reaction (hours to days). Psychological first aid, safety, and watchful waiting; do not debrief routinely. [10] [11]
Acute Stress Disorder (three days to one month). Where distress is marked, offer early TF-CBT to reduce the chance of progression to PTSD. [1] [11]
Established PTSD (more than one month). First-line TF-CBT, with caregiver involvement integral to the paediatric model. [1] [12]
Preschool PTSD. Use developmentally-adapted TF-CBT; Scheeringa demonstrated efficacy for three-to-six year-olds, and stepped care is non-inferior in young children. [2] [3]
Complex / developmental trauma. After chronic interpersonal adversity, run phased treatment — stabilisation and safety, then regulation and relationship work, then integration — over a longer course, with attention to attachment. [9] [12]
Medical and iatrogenic trauma. After PICU, burns, or repeated painful procedures, combine trauma-informed medical care with early psychological support to prevent conditioned fear of treatment. [12]
Refugee, war-affected and disaster-exposed children. Use culturally-adapted, often group- or school-based interventions; Catani's work on family violence and war trauma shows the family context is central. [4] [9]
Traumatic or prolonged grief. After bereavement, distinguish normal grief from prolonged grief disorder; grief-informed TF-CBT addresses both the loss and any traumatic elements. [13]
Adolescent PTSD with substance use. Deliver integrated dual-focus care — never medication alone — and treat the suicidality that often accompanies it. [10] [13]
Out-of-home care and family violence. Safety and placement drive the plan; a trauma-focused programme cannot run in an unsafe environment. [9] [11]
Complications & Pitfalls
- Never asking about trauma, so PTSD is never on the differential.
- Over-diagnosing PTSD in a normal acute reaction that would resolve.
- Under-diagnosing the child who presents with behaviour, somatic complaints, or school refusal.
- Diagnostic overshadowing — attributing trauma symptoms to ADHD, ODD, or disability.
- Starting an SSRI first-line for prepubertal PTSD.
- Delivering single-session debriefing as "prevention."
- Forcing disclosure or running exposure work before the child is safe and stabilised.
- Missing ongoing abuse or an unsafe placement.
- Ignoring untreated caregiver trauma.
- Open-loop referral to CAMHS with no interim plan, relapse signs, or safety-net.
Prognosis & Disposition
Most trauma-exposed children recover within weeks with support; persistence is the exception that your assessment exists to detect, and the Trickey risk factors tell you whom to watch closely. Untreated PTSD risks chronicity, comorbidity (depression, substance use), impaired development, and adult PTSD — which is exactly why early, evidence-based treatment matters. [7] [8]
Disposition after a normal acute reaction: psychoeducation, watchful waiting, routine review. [11]
Disposition after persistent symptoms or impairment: stepped-care TF-CBT pathway with medical-home interim support and developmental or comorbidity workup as indicated. [1] [11]
Disposition after acute risk or active safeguarding concern: crisis and child-protection pathway, same-day supports. [9] [13]
Markers of response are fewer intrusive symptoms, better sleep and concentration, return to school, and improved mood and function. Long CAMHS waitlists change the medical-home role: provide interim coaching, safety planning, and school liaison rather than passive waiting. [11] [12]
Special Populations
Preschoolers need play-based assessment and developmentally-adapted TF-CBT; adolescents need privacy, direct risk assessment, and a different vocabulary than "trauma." Children with intellectual disability, autism, or communication impairment disclose trauma less readily — adapt measures, lean on behaviour and multi-informant data, and avoid diagnostic overshadowing. [2] [12]
Children in out-of-home care and family-violence contexts carry both higher risk and a safety-critical plan. Refugee, war-affected, migrant, and culturally and linguistically diverse families need culturally safe assessment, professional interpreters, and trauma-adapted care. Indigenous families need non-stigmatising services that acknowledge intergenerational trauma. Medically complex children and PICU survivors carry iatrogenic trauma risk that is easy to overlook. Rural and remote families should be offered telehealth TF-CBT rather than told to wait. [4] [9]
Evidence, Guidelines & Regional Differences
Key evidence anchors for exam defence: [1] [11]
- Cohen 2004 multisite RCT — TF-CBT superior to supportive therapy for sexual-abuse-related PTSD in children; the foundational paediatric evidence. [1]
- Scheeringa 2011 and Salloum 2016 — TF-CBT for preschool children, and stepped care as a non-inferior, access-friendly option for young children. [2] [3]
- Kataoka / Ngo 2008 CBITS — school-based, group TF-CBT delivery to ethnically diverse youths. [4]
- Alisic 2014 meta-analysis — PTSD rates in trauma-exposed children vary by trauma type; most exposed children do not develop PTSD. [7]
- Trickey 2012 meta-analysis — the risk factors (life threat, peri-traumatic fear/dissociation, low support, prior psychopathology, female sex in adolescence) that predict paediatric PTSD. [8]
- Mavranezouli 2020 — individual TF-CBT is cost-effective for children and young people with PTSD. [11]
- Bisson 2013 Cochrane — trauma-focused CBT and EMDR for chronic PTSD in adults, principle extending to adolescents under specialist care. [10]
- Screening measures — UCLA PTSD Reaction Index (Steinberg 2013) and Child PTSD Symptom Scale for DSM-5 (Foa 2018). [5] [6]
- Melhem 2013 — distinguishing prolonged grief from other post-bereavement presentations. [13]
Trauma-informed, stepped care is delivered through local CAMHS pathways, with watchful waiting for the first month and TF-CBT as first-line definitive treatment. School mental-health programmes (for example Be You and headspace-supported models) and telehealth TF-CBT extend access in rural and remote settings. Mandatory child-protection reporting thresholds are state and territory specific — name the principle and the local service, and do not invent statute numbers. [3] [11]
Controversies: how aggressively to intervene within the first month; the precise role and timing of pharmacotherapy in adolescents; fidelity of cultural adaptation; and how to deliver evidence-based TF-CBT when CAMHS waitlists are long and rural access is thin. [3] [10] [12]
Exam Pearls
TRAUMA
- Most exposed children recover; persistence, not exposure, is the diagnosis. [7]
- Watchful waiting for one month, then TF-CBT — TF-CBT is first-line, not an SSRI. [1] [11]
- Children re-experience through play, drawings, and behaviour more than verbal flashbacks. [2]
- The preschool subtype needs fewer symptoms and leans on observable behaviour. [2]
- Single-session debriefing is not recommended as routine prevention. [10]
- Complex PTSD (ICD-11) adds disturbance in self-organisation to the three core elements. [9]
References
- [1]Cohen JA, Deblinger E, Mannarino AP, Steer RA A multisite, randomized controlled trial for children with sexual abuse-related PTSD symptoms. J Am Acad Child Adolesc Psychiatry, 2004.PMID 15187799
- [2]Scheeringa MS, Weems CF, Cohen JA, Amaya-Jackson L, Guthrie D Trauma-focused cognitive-behavioral therapy for posttraumatic stress disorder in three-through six year-old children: a randomized clinical trial. J Child Psychol Psychiatry, 2011.PMID 21155776
- [3]Salloum A, Wang W, Robst J, et al Stepped care versus standard trauma-focused cognitive behavioral therapy for young children. J Child Psychol Psychiatry, 2016.PMID 26443493
- [4]Ngo V, Langley A, Kataoka SH, Nadeem E, Escudero P, Stein BD Providing evidence-based practice to ethnically diverse youths: examples from the Cognitive Behavioral Intervention for Trauma in Schools (CBITS) program. J Am Acad Child Adolesc Psychiatry, 2008.PMID 18645419
- [5]Steinberg AM, Brymer MJ, Kim S, et al Psychometric properties of the UCLA PTSD reaction index: part I. J Trauma Stress, 2013.PMID 23417873
- [6]Foa EB, Asnaani A, Zang Y, Caprioli J, Yadin E, Thompson KE Psychometrics of the Child PTSD Symptom Scale for DSM-5 for Trauma-Exposed Children and Adolescents. J Clin Child Adolesc Psychol, 2018.PMID 28820616
- [7]Alisic E, Zalta AK, van Wesel F, et al Rates of post-traumatic stress disorder in trauma-exposed children and adolescents: meta-analysis. Br J Psychiatry, 2014.PMID 24785767
- [8]Trickey D, Siddaway AP, Meiser-Stedman R, Serpell L, Field AP A meta-analysis of risk factors for post-traumatic stress disorder in children and adolescents. Clin Psychol Rev, 2012.PMID 22245560
- [9]Catani C, Schauer E, Neuner F Beyond individual war trauma: domestic violence against children in Afghanistan and Sri Lanka. J Marital Fam Ther, 2008.PMID 18412824
- [10]Bisson JI, Roberts NP, Andrew M, Cooper R, Lewis C Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults. Cochrane Database Syst Rev, 2013.PMID 24338345
- [11]Mavranezouli I, Megnin-Viggars O, Trickey D, et al Cost-effectiveness of psychological interventions for children and young people with post-traumatic stress disorder. J Child Psychol Psychiatry, 2020.PMID 31654414
- [12]Cohen JA, Deblinger E, Mannarino AP Trauma-Focused Cognitive Behavioral Therapy for Children and Parents. Child Adolesc Psychiatr Clin N Am, 2026.PMID 41934973
- [13]Melhem NM, Porta G, Walker Payne M, Brent DA Identifying prolonged grief reactions in children: dimensional and diagnostic approaches. J Am Acad Child Adolesc Psychiatry, 2013.PMID 23702449