Paeds · mental-behavioural-and-psychosomatic
Psychological impact of chronic illness and disability
Also known as Psychological adjustment to chronic illness in children · Psychosocial impact of chronic disease in childhood · Mental health of children with chronic physical illness · Adjustment to disability in children and adolescents · Biopsychosocial model of chronic illness in childhood · Resilience and coping in chronically ill children · Quality of life in children with chronic conditions
A fellowship approach to the psychological impact of chronic illness and disability in children and adolescents: a biopsychosocial, resilience-oriented model in which most children adapt well. Classify the response from healthy adjustment to diagnosable disorder, recognise the illness, child, family and social factors that raise risk, screen routinely for depression, anxiety and quality of life, and co-build a stepped, family-centred, school-inclusive plan across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 14-year-old with type 1 diabetes sits in your clinic. Her HbA1c has climbed, she has missed three months of school, and her mother describes her as "flat and withdrawn." The disease is the same one you have managed for years, but something else has happened: the chronic illness has begun to shape her inner life, her relationships, and her behaviour. This is the psychological impact of chronic illness and disability — not a psychiatric diagnosis in itself, but the lived psychological consequence of growing up with a long-term physical condition. [5] [4]
The right frame is the biopsychosocial model: the child sits at the centre of interacting biological, psychological, social and health-system domains, and no single domain explains the outcome. The biological domain is the illness itself — its type, severity, visibility and treatment burden. The psychological domain is the child's coping, mood, self-esteem and cognitive capacity. The social domain is the family, peers and resources around the child. The system domain is school, access to care and inclusion. Outcome emerges from the interaction of all four, which is why two children with identical diseases can have completely different trajectories. [2] [5]
The decisive idea — and the one examiners test — is that the outcome is mediated, not determined. A chronic illness is a sustained stressor, but whether it produces healthy adaptation or a psychiatric disorder depends on what happens in between: how the child appraises and copes, how the family functions, whether school is supportive, and whether the young person has access to care. That "in between" is your lever. Wallander and Varni formalised this as the disability-stress-coping model, in which risk factors and resistance factors (coping, social support, family function) jointly shape the crisis the stressor produces. [2]
Two implications follow. First, because risk is elevated but not universal, the rational strategy is routine screening of every child with a chronic condition, not reactive referral after a crisis. Second, because the mediators are modifiable, your intervention is curative: strengthening coping, supporting the family, restoring school engagement and optimising disease control are the active ingredients, whether or not a disorder has yet emerged. [3] [1]
Classification
Classify the psychological response on a single continuum — from healthy adjustment at one end to a diagnosable psychiatric disorder at the other — while remembering that most children sit somewhere on the healthy end. The continuum is not academic: the gate question at every contact is "where is this child on the line, and has the position shifted since I last saw them?" A child who drifts toward the disorder end, or who has stopped engaging with school and friends, needs more than reassurance. [5] [3]
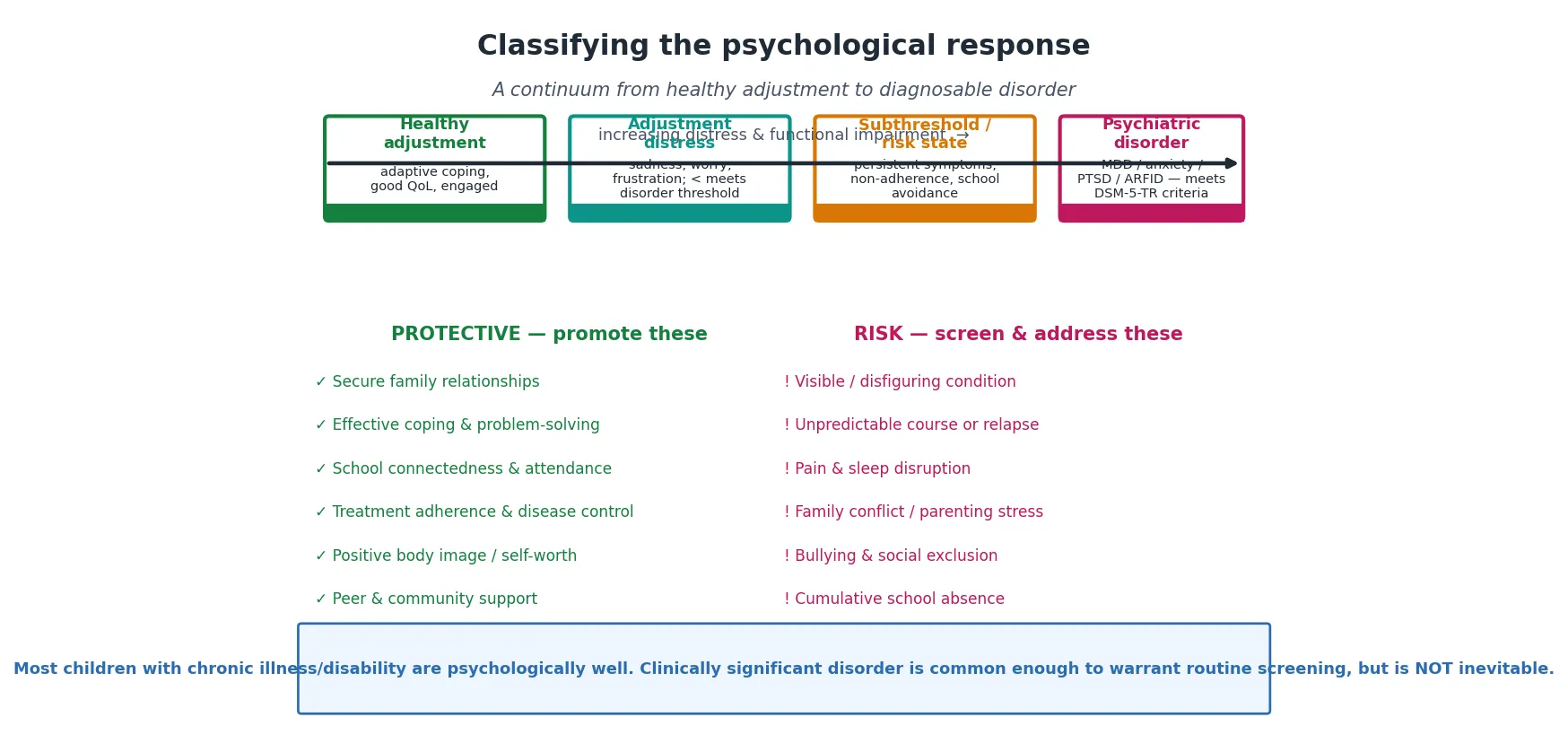
At the healthy end sits adjustment: the child acknowledges the condition, uses adaptive coping, maintains relationships and function, and reports a satisfactory quality of life. Next is an adjustment distress reaction — sadness, worry or frustration that is understandable and time-limited but does not meet disorder criteria; this is the commonest state and usually resolves with support. A subthreshold or risk state shows persistent symptoms, emerging non-adherence or school avoidance that is not yet a disorder but signals rising risk and warrants targeted intervention. Only at the far end does the presentation cross into a psychiatric disorder — a major depressive disorder, an anxiety disorder, post-traumatic stress, or an eating concern — that meets DSM-5-TR criteria and requires specialist treatment. [7] [3]
Healthy adjustment
The expected outcome
- Adaptive, engaged coping
- Maintains function, peers, school
- Satisfactory quality of life
- Most affected children sit here
Adjustment distress
A normal reaction
- Sadness, worry, frustration
- Understandable and time-limited
- Does NOT meet disorder criteria
- Resolves with support
Subthreshold / risk
Watch this zone
- Persistent, low-grade symptoms
- Emerging non-adherence
- School avoidance emerging
- Warrants targeted intervention
Psychiatric disorder
Meets DSM-5-TR
- Major depression / anxiety / PTSD
- Significant functional impairment
- Needs specialist mental-health care
- Treatable — do not miss it
The discriminating question between the last two zones is always the same: does this meet DSM-5-TR criteria for a disorder? A sad child who is still functioning, sleeping and socialising has an adjustment reaction. A child with persistent anhedonia, hopelessness, sleep and appetite disturbance, and functional decline — present most of the day, most days, for at least two weeks — has a major depressive disorder regardless of the underlying illness, and needs treatment for it. The chronic illness explains the stressor; it does not exempt the child from the diagnosis. [5] [7]
Epidemiology & Risk Factors
Chronic physical illness and disability are common in childhood, and they carry a real — but modest — elevation in psychological risk. The landmark Ontario Child Health Study (Cadman and colleagues) established the foundational finding: children with chronic illness and disability show higher rates of mental-health and social-adjustment problems than their healthy peers. Hysing and colleagues confirmed this in a large Norwegian population study, showing that chronic physical illness is associated with increased emotional and behavioural problems across the general child population. The signal is reliable; it is the size and the mediators that you must understand for the exam. [1] [4]
Pinquart's meta-analytic programme gives the most precise picture. Children and adolescents with chronic physical illness show small-to-moderately elevated internalising and externalising behaviour problems, higher depressive symptoms and anxiety, and modestly lower health-related quality of life and academic, physical and social functioning than their peers. The effect is real and consistent, but it is not large — which is precisely why resilience, not deficit, should frame the encounter. [6] [7] [9]
Pinquart — J Pediatr Psychol meta-analyses (2011–2020)
Population: Children & adolescents with chronic physical illness vs healthy/nondisabled peers
Key finding
Small-to-moderate elevation in behaviour problems, depressive symptoms and anxiety; modestly lower health-related quality of life and academic/social functioning.
Risk is not evenly distributed, and the risk factors cluster into four groups you can elicit in any history. Illness factors include a visible or disfiguring condition, an unpredictable or relapsing course, chronic pain, sleep disruption, cognitive involvement and a high treatment burden. Child factors are maladaptive or avoidant coping, low self-efficacy, and pre-existing anxiety or low mood. Family factors are conflict, parenting stress and parental mental illness. Social factors are bullying, socioeconomic disadvantage and school absence. Each is a screening question, not a footnote. [10] [11]
The protective factors are the mirror image, and they matter more for the plan than the risks do: secure family relationships, effective problem-focused coping, school connectedness and attendance, treatment adherence and disease control, a positive body image, and access to peer and community support. A child with a severe illness and strong protective factors will often adapt better than a child with a mild illness and weak ones — the clearest proof that outcome is mediated. [3] [2]
Pathophysiology
There is no single "lesion" of psychological distress in chronic illness. The mechanism is a stress-and-coping cascade in which a sustained stressor (the illness) is filtered through the child's appraisal and coping, moderated by family and social resources, and expressed as an outcome. Understanding the cascade is what lets you intervene at a point other than "give an antidepressant," and it is the heart of the disability-stress-coping model. [2] [3]
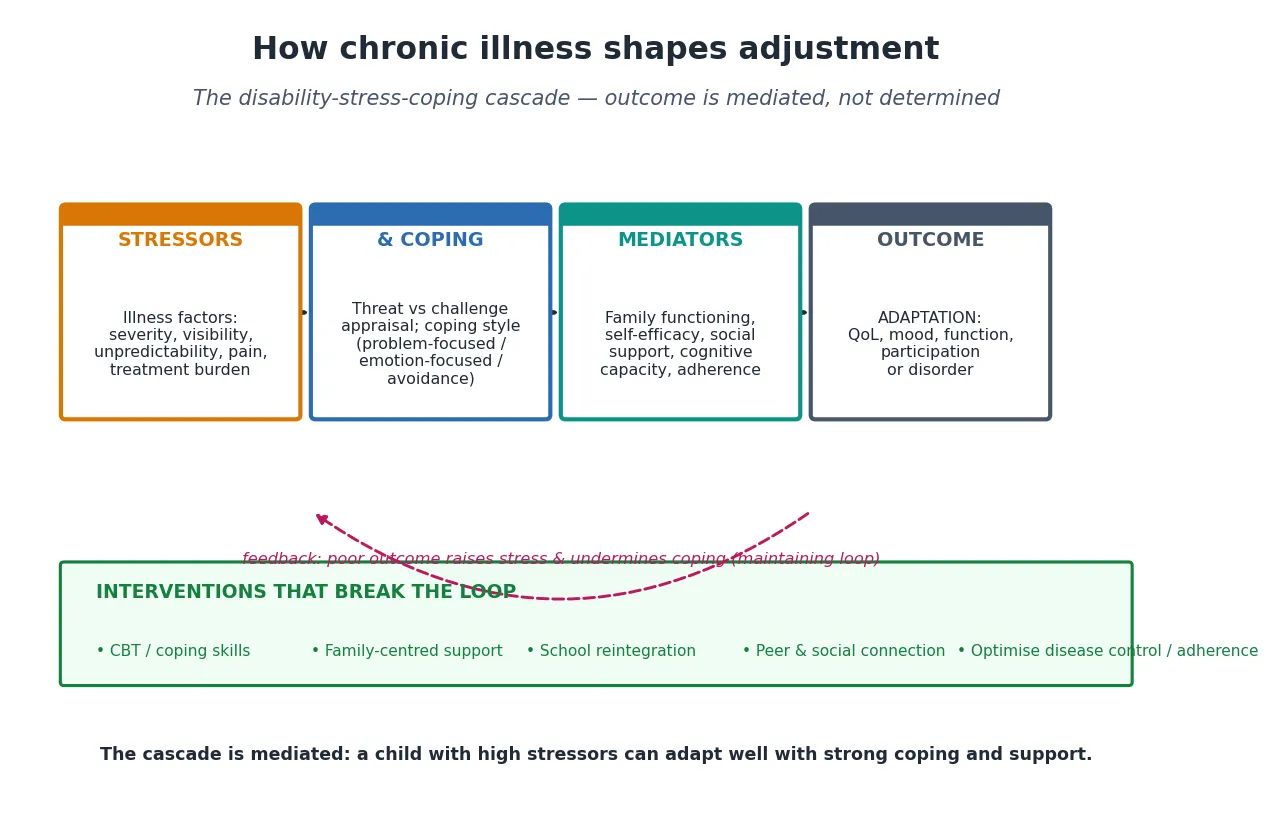
The cascade runs in four stages. The stressor is the illness and its treatment — pain, procedures, unpredictability, visibility and the daily burden of self-management. The appraisal and coping stage is where the child decides whether the illness is a threat to be endured or a challenge to be managed, and whether to engage with it (problem-focused coping) or withdraw from it (avoidance). The mediators — family functioning, self-efficacy, social support, cognitive capacity and adherence — amplify or buffer the coping response. The outcome is the child's adaptation: quality of life, mood, function and participation, or a disorder. [3]
Coping is the modifiable mediator that examiners reward, and Compas's review frames it cleanly. Problem-focused and engaged coping — actively managing the condition, seeking support, reframing the threat — predict better adaptation. Avoidance and disengagement coping — denial, withdrawal, substance use, emotional suppression — predict worse outcomes and are the early warning of a deteriorating trajectory. A child who has stopped checking blood glucose levels, or who avoids talking about the condition at all, is showing avoidant coping, not mere non-compliance. [3]
A maintaining feedback loop can lock in a poor outcome. Low mood reduces adherence; poor adherence worsens disease control; worse control increases symptoms and hospital admissions; more admissions disrupt school and friendships; lost school and friends deepen the low mood. The loop is self-reinforcing, and it explains why a child can slide from healthy adjustment to a disorder over months without any single dramatic event. Breaking the loop — at any node — is the point of intervention. [3] [5]
How the maintaining loop runs — and where you break it
Low mood / avoidance reduces engagement with the condition
Adherence slips → disease control worsens (e.g. rising HbA1c, more seizures)
Worse control → more symptoms, admissions and procedures
Disruption → school absence and social withdrawal
Lost school and peers deepen the low mood — and the loop restarts
Break it at ANY node: treat the mood, restore adherence, support school, reconnect peers
Pain, fatigue and sleep disruption add a biological-amplification layer. Chronic pain directly sensitises the nervous system and erodes mood; sleep disruption impairs emotional regulation and coping capacity; fatigue blunts engagement. These are not "just" disease symptoms — they are active drivers of psychological distress, and treating them is part of the mental-health plan. Finally, the social model of disability reframes the problem: the distress often comes less from the impairment itself than from the gap between the child's needs and an inaccessible, exclusionary environment. Removing barriers is treatment. [4] [5]
Clinical Presentation
Psychological distress in a chronically ill child rarely announces itself as "depression." It arrives disguised as the illness — a climbing HbA1c, missed clinic appointments, slipping school attendance, a flat affect the parent attributes to the disease. Your task is to recognise the disguise, because the presentation differs in each domain of response. [5] [4]
Depression presents with the core features of any adolescent depression — persistent low mood, anhedonia, hopelessness, sleep and appetite disturbance, and functional decline — but the picture is clouded by overlap with disease symptoms (fatigue, weight change) and treatment effects. The discriminator is anhedonia and hopelessness in a child whose disease is well controlled: a child whose gut is healing but who has stopped seeing friends is depressed until proven otherwise. Always ask directly about suicidal ideation. [7] [5]
Anxiety is even more varied in this group. Generalised worry, illness-specific anxiety (fear of the next seizure or relapse), medical or procedural trauma (needle phobia, scan-related distress), and health anxiety all occur. Post-traumatic stress can follow frightening medical events — a rough resuscitation, a painful procedure, a near-death episode — and presents as intrusion, avoidance, hyperarousal and negative mood. Ask specifically about frightening medical experiences, not just current symptoms. [3] [4]
The behavioural markers specific to chronic illness are the most easily missed because they masquerade as "the disease." Watch for emerging non-adherence (skipped medications, falsified readings), school refusal or escalating absence, social withdrawal, developmental regression, anger or irritability, and body-image concern (especially after surgery, disfigurement, or in conditions altering appearance or puberty). A change in any of these is a screening trigger, not a behavioural nuisance. [5] [11]
The family and siblings present too, and the family is part of the unit of care. Parenting stress is measurable and common in caregivers of children with chronic conditions; parental depression and post-traumatic stress occur after a frightening diagnosis or course; and siblings show their own adjustment difficulties that are routinely overlooked. A family that is burning out cannot sustain the child's care, so assess the family system as deliberately as you assess the child. [11] [2]
Differential Diagnosis
The central discrimination is between an expected adjustment reaction and a disorder meeting DSM-5-TR criteria. Both are legitimate; only one needs specialist mental-health treatment. The decision rests on duration, pervasiveness and functional impact — not on whether the child "has reason" to be sad. A child with every reason to be sad can still have a major depressive disorder that will respond to treatment. [5] [7]
The hardest overlap is between disease symptoms and mood symptoms. Fatigue, weight change, sleep disturbance, cognitive slowing and reduced appetite can all be caused by the active disease or its treatment (steroids, chemotherapy) as well as by depression. Resolve it by looking for the cognitive features of depression — hopelessness, worthlessness, guilt, suicidal ideation — which the disease alone does not produce, and by serial observation as the disease is optimised. [5] [7]
Non-adherence needs deconstruction. Psychological non-adherence — driven by avoidance, low mood or rebellion — is one cause, but so are practical barriers (cost, access, complexity), family disorganisation, neurodevelopmental difficulty, and genuine disagreement about the treatment. Treat each driver differently: an adolescent who omits insulin for weight loss has a different problem from one who cannot afford the strips. [5]
Distinguish school avoidance driven by mood or anxiety from avoidance driven by bullying, pain, learning difficulty, or family factors (a parent's illness, caregiving load). Each redirects to a different intervention, so do not accept "school refusal" as a terminal diagnosis — ask what is happening at school and at home. Finally, recognise somatic symptom overlap and post-traumatic stress: a child with persistent pain, fatigue or unexplained symptoms after the medical event is sorted may have a somatic or trauma process that a further test cascade will not solve. [5] [3]
Clinical & Bedside Assessment
Start the assessment with the child's and family's explanatory model — what they believe the illness means, what they fear, and what they hope for. This is not soft preamble; it tells you where the coping is stuck and what the family will accept as a plan. A family that believes the fatigue means "the disease is winning" will not engage with a graded-activity plan until you reframe it. [5]
Anchor the history in the biopsychosocial domains, working outward from the child. Take the illness history briefly (the disease team owns that), then spend your time on the psychological domain — mood, anxiety, sleep, coping, body image, self-esteem — the social domain — family functioning, parenting stress, siblings, peers, bullying — and the system domain — school attendance, connectedness, access to care. For the adolescent, run an adapted HEEADSSS, adding explicit items on the condition's place in their identity and on adherence. [5] [3]
HEEADSSS for the chronically ill adolescent
Ask directly and name each domain: "How has your mood been?" "Are you sleeping?" "What do you do when you feel overwhelmed?" "How is school going — are you going?" "Are people kind to you there?" "How is the family coping — mum, dad, your brother?" Direct, specific questions get honest answers where vague ones get "fine." Always ask about suicidal ideation explicitly; it does not plant the idea, and it is the single highest-yield question you can ask. [5] [7]
Observe the child–parent interaction and the young person's engagement in their own care. A child who is silenced, a parent who answers every question, a teenager who has never been seen alone — each is a diagnostic sign. Assess the young person's capacity for developmentally appropriate assent and participation in decisions, which is both an ethical and a clinical marker of healthy adjustment. Finally, screen the family: ask about parental mental health, sibling wellbeing, and the practical and financial strain of the condition. [11] [5]
Investigations
There is no blood test for "adjustment." The "investigation" of psychological impact is clinical, standardised, and repeated over time — screening instruments administered at intervals and at every developmental or disease transition. A single negative screen never closes the question; the child's circumstances change, and so must your surveillance. [5] [3]
The Strengths and Difficulties Questionnaire (SDQ) is the broad, free, well-validated screen for emotional and behavioural problems across childhood, usable from age four. For adolescent depression, the PHQ-A (or PHQ-9 modified for adolescents) is the standard; for anxiety, the GAD-7; for anxiety disorders more broadly in children, the SCARED. The Pediatric Quality of Life Inventory (PedsQL) — available in generic and condition-specific modules — tracks health-related quality of life and is the outcome measure of choice, because quality of life captures function and participation that a mood score alone misses. [9] [5]
Formal psychological assessment by a paediatric psychologist is indicated when screening is positive, when the presentation is complex or unclear, or when the family or school needs a structured formulation to access support. Referral to mental-health services is required when a disorder is suspected or confirmed, when there is any suicidality, or when the family system is failing. The trap to avoid is over-investigating the body to explain distress that is psychological — repeat scans and panels reassure no one and medicalise the presentation — while equally avoiding the opposite error of missing organic disease by assuming "it's psychological." Screen for the disorder; then trust the screen. [5] [3]
Interpreting overlapping somatic symptoms — fatigue that could be active disease, depression, or both — requires serial observation: optimise the disease control, treat the identifiable mood component, and re-assess. If the fatigue persists with a healed disease and a treated mood, look for a sleep disorder or a somatic/functional process. The principle is to avoid anchoring on either a pure-organic or a pure-psychological explanation. [5]
Management — Resuscitation
Before any plan, secure safety. The immediate priorities are three. First, assess suicide risk and self-harm directly, and if there is ideation, intent or a plan, build a safety plan and escalate to urgent mental-health assessment the same day — this overrides every other priority, including the disease. Second, recognise acute mental-health deterioration — a panic crisis, dissociation, or a frightening-medical-event flashback — and manage it with de-escalation, a safe environment and urgent referral. Third, identify severe non-adherence that risks acute medical harm, such as insulin omission risking diabetic ketoacidosis or abandoned immunosuppression, and respond with an urgent, structured, non-punitive plan. [5] [7]
The first conversation sets the tone for everything that follows. Validate the experience ("this is genuinely hard"), normalise the reaction ("many young people with this condition feel exactly this way"), and give hope ("there are things that help, and I will work through them with you"). Avoid the two destructive framings: "it's all in your head" (dismisses and shames) and "there's nothing we can do" (abandons). The paediatrician who gets the first conversation right has already begun the treatment. [5]
A crucial principle is that universal supportive care begins at the first diagnosis, not after a disorder develops. From the moment a chronic illness is confirmed, the family should receive validation, psychoeducation, a named point of contact, and an explicit invitation to raise emotional concerns. Waiting for a crisis to offer psychosocial support is a failure of prevention — and it is the model the evidence supports changing. [5] [3]
Management — Definitive & Stepwise
The definitive approach is a stepped, family-centred care pathway with three tiers, applied so that every child receives universal support, those with emerging distress receive targeted intervention, and the few with a disorder receive specialist care. The paediatrician is the coordinator who holds the plan together across medicine, psychology, school and family. [5] [3]
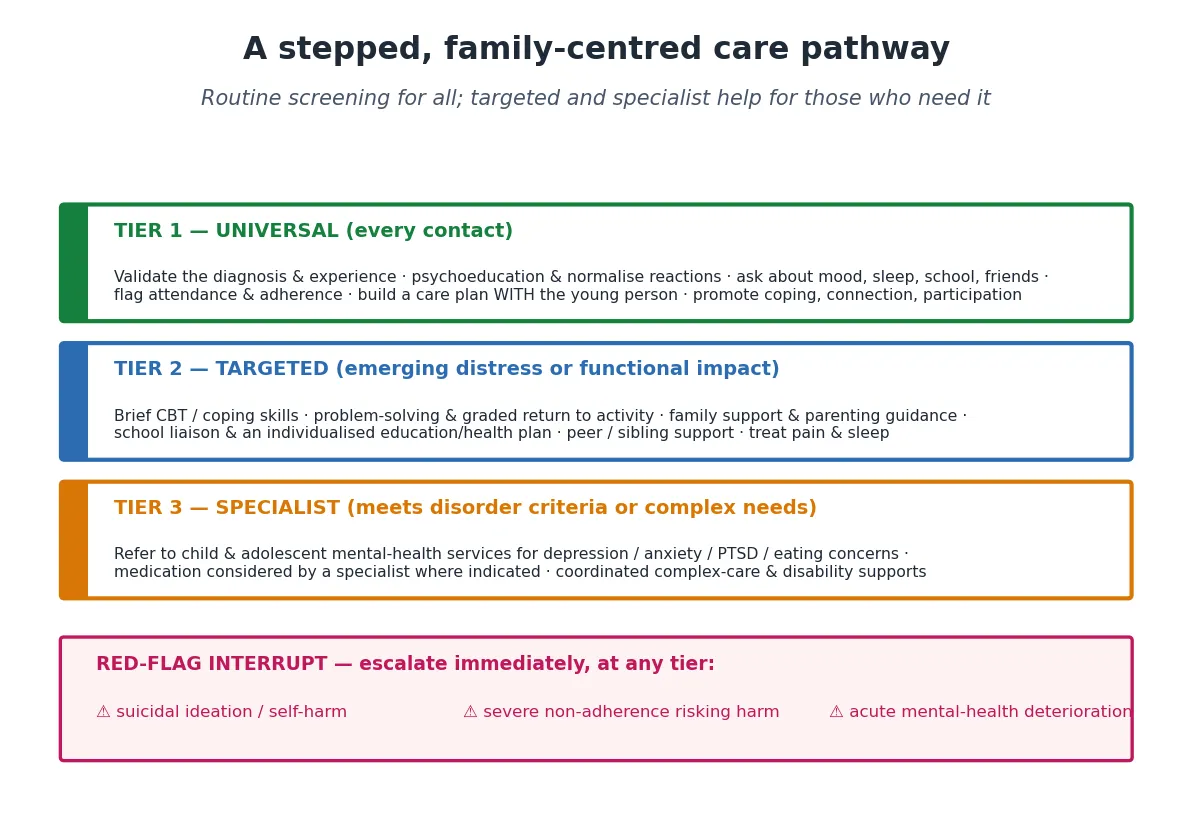
Tier 1 — universal, at every contact. Validate the experience, give honest psychoeducation that normalises the reaction, screen routinely for mood and function, and flag attendance and adherence early. Build the care plan with the young person, not for them, and actively promote coping, connection and participation. This is the treating team's job, not a referral — and it is where most of the benefit accrues. [5]
Tier 2 — targeted, for emerging distress or functional impact. Add brief cognitive-behavioural or coping-skills work, problem-solving and a graded return to activity, family support and parenting guidance, school liaison with an individualised education/health plan, and peer or sibling support. Treat pain and sleep, because they are drivers of distress. The paediatrician coordinates; a paediatric psychologist or counsellor usually delivers. [3] [5]
Tier 3 — specialist, for disorder or complex need. Refer to child and adolescent mental-health services for a depressive or anxiety disorder, PTSD, or eating concerns. Medication — an SSRI for a confirmed depressive or anxiety disorder — is considered by a specialist, started only where indicated, and monitored, never prescribed casually for "the stress of the illness." Coordinate complex-care and disability supports around the mental-health treatment. The gate into Tier 3 is the disorder diagnosis, not the severity of the underlying illness. [5] [7]
Building a school reintegration plan
Identify the barriers: is it mood, pain, bullying, fatigue, or learning difficulty?
Convene the school (nurse, welfare, year coordinator) with the family and the young person
Agree a graded, time-bound return with reduced load and built-in success
Put an individualised education/health plan in writing (e.g. health-condition plan)
Name a single school contact and a single clinical contact
Review at fixed intervals; celebrate progress; adjust the plan, not the goal
School reintegration is the single most powerful functional lever, and the paediatrician often has to drive it. The Cochrane review by Barnett and colleagues examined education support services for children and adolescents with a chronic health condition; while the evidence base is emerging and limited in certainty, the clinical principle is strong: structured, coordinated school support improves engagement, and a plan built jointly by clinic, school and family outperforms ad hoc arrangements. Your role is to convene the school, name the contacts, and put the plan in writing. [12]
The paediatrician as care coordinator is the thread running through all three tiers. You hold the relationship with the family, you see the child across disease and developmental transitions, and you are the one who notices the drift from healthy adjustment toward disorder. Coordinate with the disease team, the psychologist, the school and (where needed) mental-health services, and re-screen at every transition — diagnosis, adolescence, school change, and the move to adult care. [5] [3]
Specific Subtypes & Scenarios
Type 1 diabetes is the canonical high-risk model and a favourite long-case. The daily, unremitting burden of self-monitoring and dosing, the visibility of the regimen, the body-image and eating-disorder risk (insulin omission for weight), and "diabetes distress" — the specific emotional burden of the condition — combine to make psychological screening a core part of diabetes care, not an add-on. A rising HbA1c in an adolescent is as often a psychological signal as a metabolic one. [5] [3]
Cancer and oncology carry procedural trauma, body-image disruption (surgery, hair loss, fertility worry), and, for survivors, neurocognitive late effects that affect schooling and self-esteem. The re-entry to school after treatment is a recognised high-risk transition that needs a planned, supported return, and survivorship care must include cognitive and psychological surveillance, not just disease surveillance. [5]
Epilepsy and neurodisability (cerebral palsy, intellectual disability) compound the load through cognitive involvement, social stigma, unpredictable seizures, and — critically — communication impairment that makes psychological distress harder to express and easier to miss. This is the heartland of diagnostic overshadowing: a change in behaviour, mood or even a physical symptom in a disabled child is attributed to "the disability" and a treatable disorder is missed. Assume distress is real and has a cause; investigate both the body and the mind. [4] [2]
The visible-versus-invisible distinction changes the social burden. Visible conditions (amputation, skin disease, dysmorphism) attract staring, questions and bullying; invisible conditions (inflammatory bowel disease, chronic kidney disease, cystic fibrosis) carry the burden of concealment, disclosure decisions and the "but you look well" invalidation. Both are psychologically costly in different ways, and you should ask about the specific social cost the young person carries. [10] [5]
Adolescent transition to adult care is a psychological and logistical cliff. The young person must take on autonomy over a condition they may resent, the coordinated paediatric support falls away, and adherence and mental health often deteriorate in the gap. Build the transition early, transfer psychological support alongside medical care, and never hand over a young person whose mood and coping are unaddressed. [5]
Complications & Pitfalls
Diagnostic overshadowing is the single most tested pitfall in the mental health of disabled children. It is the error of attributing a new physical or psychological presentation to the underlying disability or illness, and thereby missing a treatable disorder — a painful limp blamed on "the cerebral palsy" rather than a fracture, or withdrawal attributed to "the intellectual disability" rather than depression. The safeguard is a discipline: every new symptom in a disabled child gets the same differential it would in an unaffected child. [4] [2]
The over-investigation trap is the mirror image. When distress is the driver, churning tests reassures no one, medicalises the presentation, and entrenches the illness identity. The opposite error — missing organic disease by assuming "it's psychological" — is equally dangerous. The resolution is the same discipline applied both ways: investigate the targeted differential, trust the result, and then treat the psychological component without re-investigating. [5]
Stigma, bullying and exclusion are iatrogenic-amplifiable harms. A pessimistic or stigmatising framing ("he will never be normal") becomes a self-fulfilling nocebo; social exclusion and bullying directly drive depression and school avoidance. Pinquart's meta-analysis shows children with chronic illness and disability are more involved in bullying than their peers — so ask about bullying and act on it, because it is a modifiable driver, not background noise. [10]
Family burnout, parental depression and sibling neglect are consequences of unaddressed child distress that then feed back to worsen the child's outcome. A family that has broken under the strain cannot sustain the care plan, and a sibling who has been invisible for years carries their own unmet need. Assess the family as part of the unit of care and refer parents and siblings for support in their own right. [11]
The transition cliff is a system complication: when a young person leaves coordinated paediatric care, the psychological and practical support that held the plan together often disappears, and outcomes deteriorate. Anticipate it, transfer the psychological plan early, and ensure an adult service is identified and engaged before the handover. [5]
Prognosis & Disposition
Outcome is determined less by the diagnosis than by the modifiable mediators: coping style and self-efficacy, family functioning, school engagement, adherence, and access to support. A child with a severe condition and strong mediators will usually adapt well; a child with a mild condition and broken mediators may not. This is the most hopeful and the most actionable fact in the whole topic — your assessment and intervention genuinely change the trajectory. [3] [2]
Most children adapt well over time, and the clinically significant minority who develop a disorder respond well to targeted and specialist intervention, particularly when caught early. Prognosis is better when coping is engaged rather than avoidant, when the family is supported, and when the child stays connected to school and peers — which is why those are the goals of the plan, not symptom elimination. [6] [7]
Disposition is outpatient, in the medical home, with shared care for those receiving targeted or specialist support. The paediatrician coordinates, the psychologist delivers Tier 2 intervention, mental-health services deliver Tier 3 treatment, and the school delivers the reintegration plan. The child stays under the treating team throughout, because the psychological and the medical care are one plan, not two. [5]
The safety-net and follow-up cadence is deliberate re-screening at intervals and at every transition — diagnosis, adolescence, school change, relapse, and transition to adult care. Use function, attendance, quality of life (PedsQL) and mood as the outcome measures, not the disease marker alone. A child whose HbA1c is perfect but who has stopped attending school is not doing well. [9] [5]
Special Populations
Neurodivergent children — those with autism, ADHD or intellectual disability — carry a higher baseline psychological load, present atypically, and have communication needs that make standard screening harder. Adapt your assessment: use observation, informant report and behaviour as well as self-report, and remember that diagnostic overshadowing is most dangerous in this group. A behaviour change is a signal, not a trait. [4]
Adolescents are the highest-stakes group. Identity formation, autonomy, risk-taking behaviour, confidentiality, and the drive for independence all collide with the demand to adhere to a resented regimen. Use HEEADSSS, see the young person alone, respect confidentiality within the bounds of safety, and build the plan around their goals, not the parent's. [5]
Aboriginal, Torres Strait Islander, Māori and other Indigenous children carry the additional weight of intergenerational trauma, racism and social determinants, and they benefit from culturally safe, strengths-based, family-and-community-centred care. Build the relationship before the plan, work with the local Aboriginal health service or cultural support, and recognise that resilience in this group is profound and is the foundation to build on. [2]
Migrant, refugee and asylum-seeking children, children in out-of-home care, and those in youth-justice settings often have compounding adversity, disrupted continuity of care, and barriers to disclosure. Children with complex or technology-dependent conditions, and those in rural and remote settings with limited access to psychology and mental-health services, need the paediatrician to be especially active in coordination and in bridging the access gap, including through telehealth. [5] [11]
Evidence, Guidelines & Regional Differences
The evidence base rests on three pillars. The Ontario Child Health Study (Cadman and colleagues) established the foundational association between chronic illness, disability and elevated mental-health morbidity. Pinquart's meta-analytic programme quantified the magnitude: small-to-moderate elevations in internalising and externalising problems, depressive symptoms and anxiety, and modestly lower quality of life and functioning — consistent, reliable, but modest. Compas's review established coping as the central, modifiable mediator of adjustment, giving the field its therapeutic target. [1] [6] [3]
[4] [2] [9] [12]The guideline posture is consistent across regions: routine psychosocial screening, family-centred and school-inclusive stepped care, and the medical home as the coordinating hub. Where regions differ is in the operational pathway — which screening tools are mandated, how mental-health services are accessed, and how school plans are formalised — so name your local pathway in any exam answer. [4] [9]
The principal controversy and limitation is that most of the evidence is cross-sectional and drawn from heterogeneous conditions, which limits causal inference and condition-specific precision. The counterbalance — and the framing examiners expect — is that resilience, not deficit, should lead: the group risk is modest, most children are well, and the treatable minority justify routine screening without justifying a deficit-based narrative. [6] [9]
Exam Pearls
Diagnostic overshadowing is the single most tested concept — never attribute a new symptom to the disability without running the full differential. Coping style is the modifiable mediator examiners reward: problem-focused and engaged coping predicts adaptation; avoidance predicts deterioration. The two screening instruments to name are the SDQ (broad) and the PedsQL (quality of life), plus the PHQ-A/GAD-7 for adolescent mood and anxiety. [9] [3]
Family and sibling impact is part of the assessment, not an aside — parenting stress is measurable and common, and an unsupported family cannot sustain the plan. Non-adherence is a psychological signal to be decoded, not a behavioural nuisance to be punished. School reintegration is the most powerful functional lever you have; convene the school and put the plan in writing. And remember the transition cliff: never hand over a young person whose mood and coping are unaddressed. [11] [12]
References
- [1]Cadman D; Boyle M; Szatmari P; Offord DR Chronic illness, disability, and mental and social well-being: findings of the Ontario Child Health Study. Pediatrics, 1987.PMID 2952939
- [2]Wallander JL; Varni JW Effects of pediatric chronic physical disorders on child and family adjustment. Journal of child psychology and psychiatry, and allied disciplines, 1998.PMID 9534085
- [3]Compas BE; Jaser SS; Dunn MJ; Rodriguez EM Coping with chronic illness in childhood and adolescence. Annual review of clinical psychology, 2012.PMID 22224836
- [4]Hysing M; Elgen I; Gillberg C; Lie SA; Lundervold AJ Chronic physical illness and mental health in children. Results from a large-scale population study. Journal of child psychology and psychiatry, and allied disciplines, 2007.PMID 17683450
- [5]Yeo M; Sawyer S Chronic illness and disability. BMJ (Clinical research ed.), 2005.PMID 15790645
- [6]Pinquart M; Shen Y Behavior problems in children and adolescents with chronic physical illness: a meta-analysis. Journal of pediatric psychology, 2011.PMID 21810623
- [7]Pinquart M; Shen Y Depressive symptoms in children and adolescents with chronic physical illness: an updated meta-analysis. Journal of pediatric psychology, 2011.PMID 21088072
- [8]Pinquart M; Teubert D Academic, physical, and social functioning of children and adolescents with chronic physical illness: a meta-analysis. Journal of pediatric psychology, 2012.PMID 22173882
- [9]Pinquart M Health-Related Quality of Life of Young People With and Without Chronic Conditions. Journal of pediatric psychology, 2020.PMID 32642762
- [10]Pinquart M Systematic Review: Bullying Involvement of Children With and Without Chronic Physical Illness and/or Physical/Sensory Disability-a Meta-Analytic Comparison With Healthy/Nondisabled Peers. Journal of pediatric psychology, 2017.PMID 27784727
- [11]Pinquart M Parenting stress in caregivers of children with chronic physical condition-A meta-analysis. Stress and health : journal of the International Society for the Investigation of Stress, 2018.PMID 28834111
- [12]Barnett T; Tollit M; Ratnapalan S; Sawyer SM; et al Education support services for improving school engagement and academic performance of children and adolescents with a chronic health condition. The Cochrane database of systematic reviews, 2023.PMID 36752365