Paeds · mental-behavioural-and-psychosomatic
Somatic symptom and related disorders
Also known as Somatic symptom disorder in children · Illness anxiety disorder in children · Conversion disorder (functional neurological symptom disorder) in children · Paediatric psychosomatic disorder · Medically unexplained symptoms in children · Somatisation in childhood and adolescence · Psychological factors affecting medical condition
A fellowship approach to somatic symptom and related disorders (DSM-5) in children and adolescents: a validating, biopsychosocial, function-first model. Recognise the disorder on positive grounds (distressing symptoms plus disproportionate thoughts, feelings and behaviours — not 'medically unexplained'), screen once for organic disease, stop the test cascade, and co-build an interdisciplinary plan across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 13-year-old has had daily abdominal pain, headaches and tiredness for eight months. She has seen four specialists, had three normal scans and a long list of normal bloods. She now attends school only two days a week, her mother is convinced something is being missed, and the folder of results is thicker than your textbook. The temptation is to order one more test, or to tell the family "the tests are normal, so there's nothing wrong." Both are harmful. The clinician who understands this presentation does a third thing: recognises a real nervous-system and coping problem, completes the targeted exclusion honestly, and starts a recovery plan. [1] [2]
The modern name for this cluster is the somatic symptom and related disorders (SSRD), a DSM-5 family that replaces the older, stigmatising "somatoform disorders" and "somatisation" labels. The defining idea is not the symptom itself but the relationship the child and family have with it: a distressing bodily symptom is paired with excessive, disproportionate thoughts, feelings or behaviours, and persists in a way that disrupts life. The symptom is genuine; the problem is the amplifying pattern around it. [2] [1]
The single most important sentence for the exam — and for the family — is that the symptoms need not be "medically unexplained". Under DSM-5-TR, a child with a genuine medical illness (coeliac disease, asthma, epilepsy) can still meet criteria for an SSRD if they also have the disproportionate cognitive and behavioural response. You diagnose the positive pattern of thoughts and behaviours, never the absence of disease. This shift is why the older "medically unexplained symptoms" framing is now a trap, and why the examiner expects DSM-5 language. [2]
Two facts anchor everything that follows. First, symptoms commonly shift between body systems in the same child — abdominal pain this year, fatigue and dizziness next — and the SSRD family shares a common biology and a common management approach, so a rigid single-organ diagnostic hunt is the wrong frame. Second, outcomes are far more modifiable than frightened families believe, and the lever that matters most is restoration of function: getting the child back to school, sleep, movement and friends. [1] [7]
Classification
Classify on one axis — which disorder — while holding the shared core that runs underneath all of them. The core is what makes management converge regardless of the label: genuine distress, anxiety and catastrophising about symptoms, functional impairment and school absence, high healthcare use and poor reassurance, and frequent comorbid anxiety and depression. [1] [2]
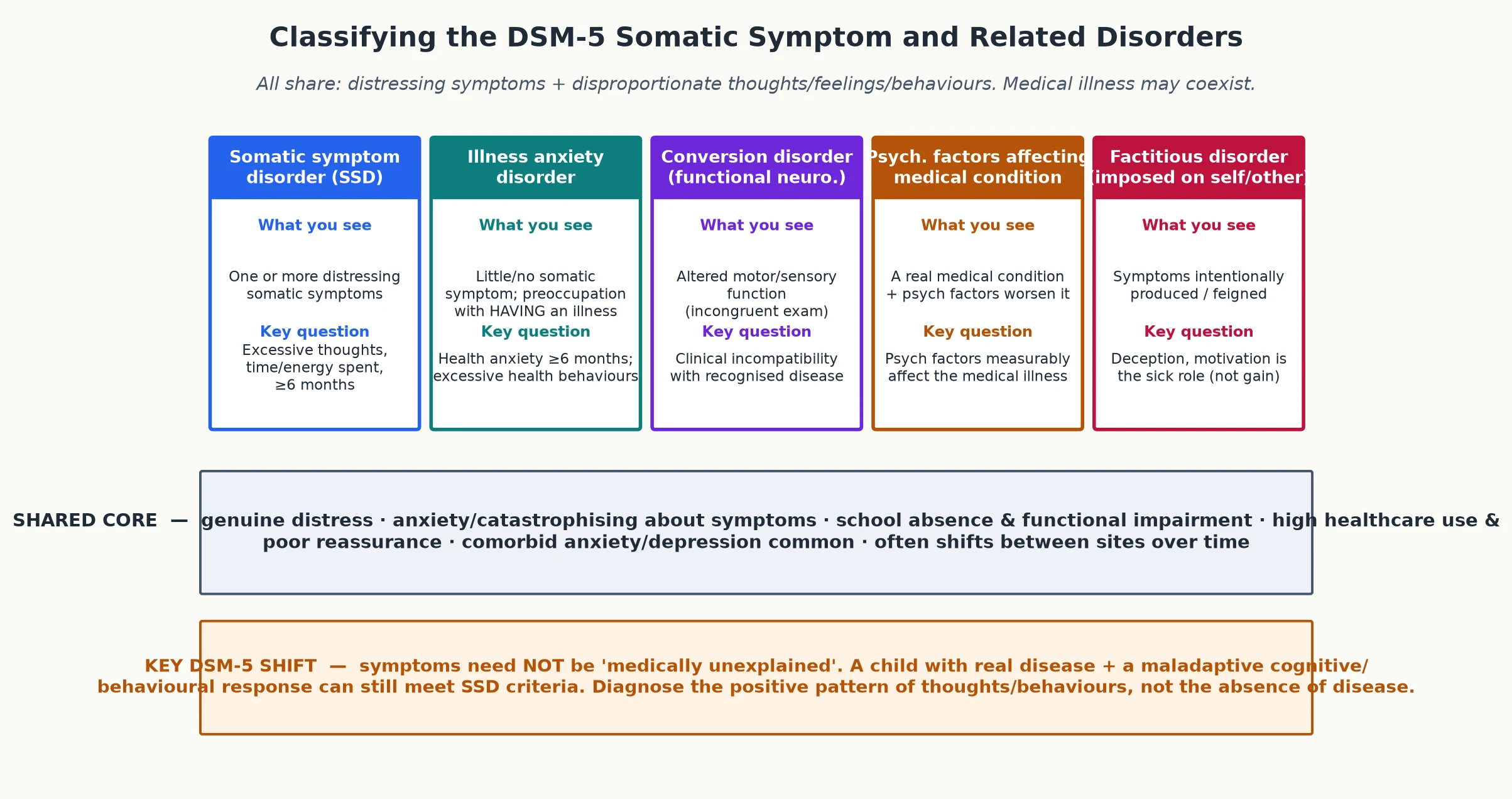
Read the figure like this: do not force the child into one box on first contact, and never use "medically unexplained" as the test for any of them. The discriminating question for each is printed on the card — learn that single sentence per disorder. [2]
Somatic symptom disorder
Symptom-predominant
- One or more distressing somatic symptoms
- Excessive thoughts/feelings/behaviours about them
- Persistent, typically ≥6 months
- Symptoms need NOT be unexplained
Illness anxiety disorder
Worry-predominant
- Minimal or no somatic symptom
- Preoccupation with HAVING an illness
- Excessive health behaviours/checking
- Health anxiety ≥6 months
Conversion disorder (functional neurological)
Neuro-predominant
- Altered motor/sensory function
- Incongruent/incompatible exam signs
- Diagnosed on positive grounds after exclusion
- Hoover sign, non-epileptic events
Psychological factors affecting medical condition
Disease-plus-stress
- A real medical condition is present
- Psych factors measurably worsen it
- e.g. stress-driven asthma, diabetes, epilepsy
- Treat disease and the stressor both
Factitious disorder (incl. fabricated/induced illness)
Safeguarding-predominant
- Symptoms intentionally produced/feigned
- Deception; motive is the sick role
- Fabricated/induced illness by carer = safeguarding
- Do NOT confront the carer alone
The one distinction the examiner presses is factitious disorder versus the rest. Somatic symptom disorder, illness anxiety disorder and conversion disorder are unconscious processes — the child is not feigning, and the family is not deceiving. Factitious disorder (and fabricated or induced illness imposed on a child by a carer) involves intentional production of symptoms and deception, with the sick role as the motive. That single word — intentionality — turns the management pathway into a safeguarding pathway. [2] [8]
Epidemiology & Risk Factors
Persistent somatic complaints are among the commonest reasons children and adolescents present to primary and secondary paediatric care — recurrent abdominal pain, headache, fatigue and limb pain predominate — but only a minority cross the threshold into a full somatic symptom and related disorder, where the disproportionate thoughts and behaviours drive persistent disability. Garralda's reviews establish that unexplained physical complaints are high-volume, often recurrent, and frequently associated with anxiety, depression and functional impairment rather than being rare curiosities. [1] [2]
Risk is not evenly distributed. The classic profile is an older child or adolescent, with a female predominance emerging after puberty, who carries pre-existing anxiety or depression, disturbed sleep, a family pattern of illness or pain modelling, and exposure to adverse childhood experiences. Smakowski and colleagues' meta-analysis confirms that anxiety, depression and catastrophising are reliably associated with somatic symptom disorder across cross-sectional and longitudinal studies — these are the psychological risk factors to actively screen for, not background noise. [11] [1]
Two precipitant profiles matter in paediatrics. First, life events and stressors — family conflict, loss, school transitions and abuse — are over-represented in young people with SSRD; Bedard-Thomas and colleagues showed that medically hospitalised children with SSRD report a high burden of negative life events. Second, bullying and peer victimisation cluster with these presentations; Ibeziako and colleagues found bullying victimisation was common among hospitalised paediatric SSRD patients and associated with greater complexity. Ask directly about both. [5] [6]
The functional and economic cost is large. Children with SSRD accumulate school absence, repeated healthcare contacts, normal investigations and procedures — and poor reassurance is itself a driver, as Puri and Dimsdale argue: the very pattern of high healthcare utilisation and failure to be reassured is a predictor of the somatoform trajectory rather than evidence that "more tests" will solve it. [10] [4]
Pathophysiology
You need a usable model of why a real symptom persists, because the model is the explanation you give the family and the rationale for every intervention. [1]
The keystone is the symptom-amplification loop. A genuine bodily signal — ordinary gut sensation, a muscle ache, a normal heartbeat — is met with selective attention and catastrophising threat appraisal ("this means something is wrong with me"). That appraisal drives anxiety and autonomic arousal, which sensitise the nervous system so the signal is amplified and felt more intensely — which confirms the fear and tightens attention on the body. The loop is self-sustaining, and it runs on a real signal. This is the cognitive-behavioural substrate that Garralda frames as the engine of somatisation in childhood. [1] [11]
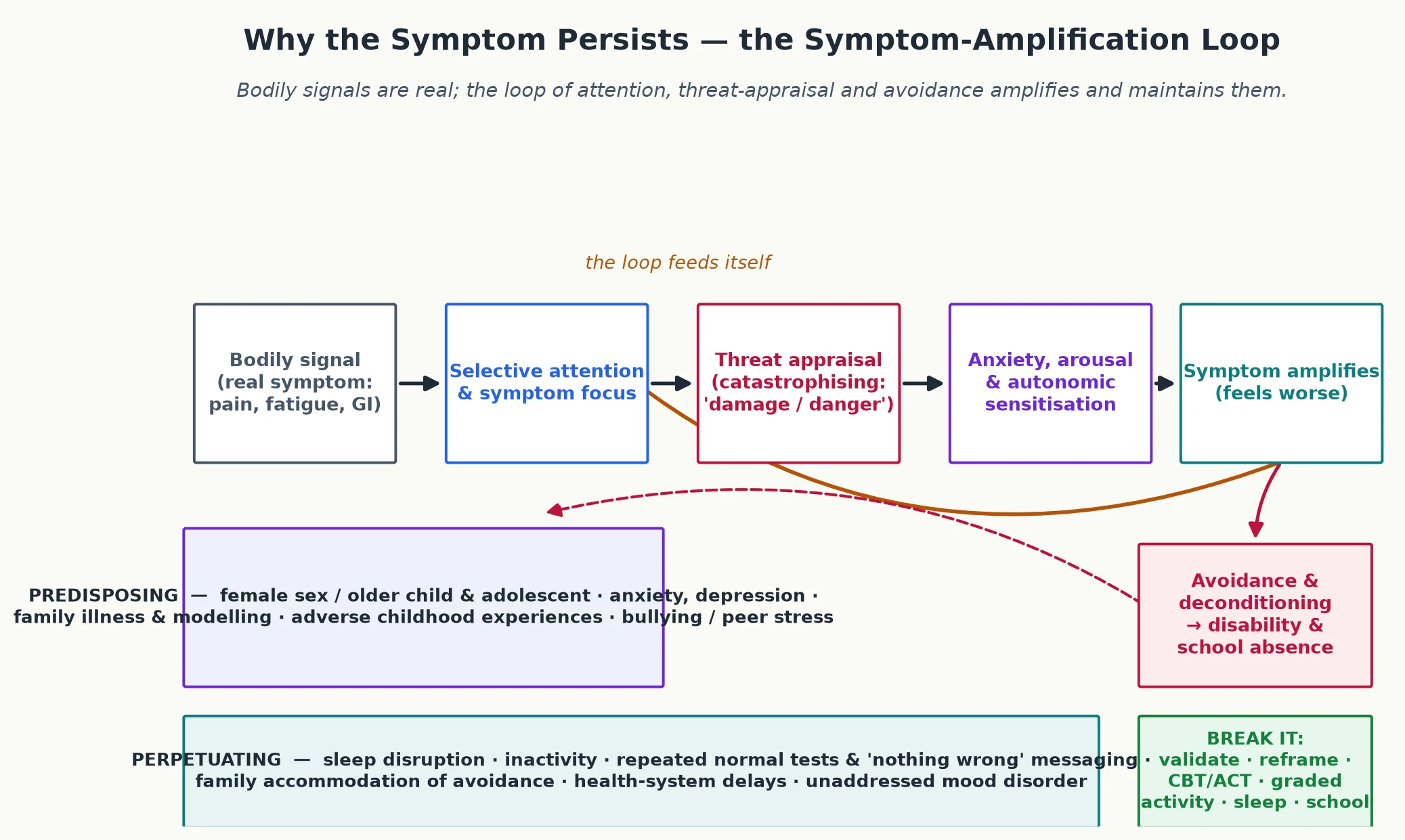
Read the figure like this: the arrows run in a circle, which is exactly why a single-modality fix fails — the clinician must interrupt the loop at attention, appraisal, arousal and avoidance at once. That is what an interdisciplinary team is for. [1]
Three modifiers run through the loop. Avoidance and deconditioning turn a worrying symptom into disability: the child stops moving, loses fitness and confidence, and a weaker body generates more symptoms, not fewer. Sleep disruption lowers the symptom threshold and creates a symptom-sleep cycle. And conversion/functional neurological symptoms share the same substrate understood through a predictive-coding lens — the brain's motor and sensory programs run an altered, internally generated pattern that produces real, often dramatic neurological symptoms without damaged tissue. [8] [1]
The biopsychosocial model holds that no single factor is sufficient: biological predisposition (family loading, puberty, sensitisation), psychological processes (anxiety, catastrophising) and social context (stress, family beliefs, school) interact. The practical corollary is that a management plan attacking only one level will fail. [1] [11]
Clinical Presentation
A child with an SSRD rarely arrives labelled. More often they present with recurrent abdominal pain or headache that has defeated repeated normal investigations, persistent fatigue and school refusal, a parade of shifting symptoms (dizziness, chest pain, limb pain, non-epileptic events), or — in the illness-anxiety pattern — a relentless, symptom-light conviction that a serious disease is being missed. A high index of suspicion for the SSRD frame is what surfaces the right plan. [1] [2]
The presentation is rarely just about the symptom. The child shows school refusal or prolonged absence, withdrawal from friends, broken sleep, low mood, family conflict and a shrinking identity — they describe themselves as "a sick person." The symptom and the disability are entangled, and you assess both. [7] [4]
Conversion disorder has a recognisable shape: non-epileptic events, functional weakness or sensory change, or a functional movement, with incongruent examination findings — for example a positive Hoover sign in functional leg weakness, or events that do not injure despite dramatic collapse. Pehlivantürk and Unal's clinical series describes the presentation and the high rate of comorbid anxiety and depression in children and adolescents with conversion disorder. [9] [8]
[1] [2]Differential Diagnosis
In this topic the differential is "what else could this be, and what must I rule out once — then stop." [1]
| Presentation | Consider alongside | Do not miss |
|---|---|---|
| Recurrent abdominal pain | Coeliac disease, IBD; functional abdominal pain disorders | Weight loss, growth failure, peri-anal disease, raised inflammatory markers |
| Persistent fatigue | Anaemia, thyroid disease, sleep disorder; chronic fatigue syndrome | Malignancy, autoimmune disease, post-infective organic complications |
| Headache | Migraine, tension-type; medication-overuse | Raised intracranial pressure, nocturnal/waking headache, neurological deficit |
| Functional weakness / events | Functional neurological symptom disorder | Epilepsy, demyelination, neuromuscular disease, spinal cord lesion |
| Non-specific multisystem symptoms | Somatic symptom disorder; anxiety/depression | Systemic autoimmune/malignant disease; fabricated/induced illness |
Two traps recur, and the examiner tests both. The first is over-investigating and medicalising — each extra normal scan can reinforce a disease model, cause nocebo harm, and delay recovery. The second, opposite trap is dismissing genuine organic disease by attributing everything to "functional" — the classic route by which children with evolving inflammatory, neurological or malignant illness get missed. The discipline is to screen for red flags once with targeted tests, then commit to the SSRD frame and hold it unless a new red flag appears. [1] [10]
A third, distinct trap is diagnostic overshadowing: once a child carries a "functional" or developmental label, new organic symptoms are attributed to the label rather than assessed on their merits. Disabled and neurodivergent children are at particular risk. Guard against it by reassessing any genuinely new symptom with a fresh differential. [1]
Clinical & Bedside Assessment
1. Open and validate
Greet the young person first, secure time alone (age-appropriate), and state conditional confidentiality with its lawful limits. Then do the single most therapeutic early act: validate the symptom as real. A sentence like "I can see these symptoms are genuinely distressing, and I believe you — this is not your fault and it's not 'in your head'" sets the foundation for everything that follows. Kozlowska's "first interview" framework is built entirely around this validating, family-engaged opening. [3]
2. Focused symptom history
Take the symptom history — site, onset, course, shifting sites, triggers, previous investigations and treatments, and functional impact — and explicitly elicit the family's explanatory model: what do they currently believe is wrong? The explanatory model drives adherence, and a family convinced a disease is being missed will not engage with a functional plan until they feel heard. [1] [3]
3. Biopsychosocial / HEEADSSS assessment
Run a HEEADSSS-tailored assessment emphasising mood, sleep, school attendance, peers, family function, adversity and bullying. Screen actively for anxiety and depression, and — because SSRD and self-harm cluster — assess suicidality at every meaningful contact. Ask about sleep onset, night waking and refreshment, about family illness modelling and parental distress, and about bullying and recent life events (Bedard-Thomas; Ibeziako). [5] [6]
4. Focused examination
Examine generally, then the affected system, and complete a full neurological screen. In suspected conversion, look for incongruence — findings that do not map to a single anatomical pathway (Hoover sign, non-epileptic event features, tubular field defects) — which supports, but never alone proves, a functional origin. Examine respectfully and with consent. [8] [9]
5. Functional and goal assessment
Quantify functional disability directly — current school attendance, activity level, sleep and participation — using the Functional Disability Inventory validated by Claar and Walker, where higher scores indicate greater disability. Frame goals around function, not symptom scores: what does the young person want to get back to? [7]
Investigations
Investigations in an SSRD serve one purpose: to exclude organic disease once, with a focused, rationale-led panel, and then stop. An open-ended cascade is a cause of harm, not diligence. [1]
Targeted exclusion. A focused baseline set — full blood count, inflammatory markers (CRP, ESR), basic biochemistry, thyroid function, and coeliac serology where indicated — excludes common organic mimics. Imaging is reserved for genuine red flags or focal neurological findings; routine extensive imaging of a stable somatic presentation is low-value and reinforces a disease model. [1] [2]
Positive diagnosis for conversion. Conversion disorder (functional neurological symptom disorder) is diagnosed on positive grounds — symptoms clinically incompatible with recognised neurological disease — after targeted exclusion, not by adding more scans after the first normal set. This is a diagnosis made on the ward or in clinic with neurology input, not one of exhaustion. [8] [9]
Functional assessment is investigation. Validated instruments — the Functional Disability Inventory, plus mood, anxiety and somatic-symptom scales — are part of the investigation set, not optional extras, because they quantify the very disability the plan targets. [7]
Low-value patterns. Routine extensive autoimmune panels, repeated MRI of the same region without a new red flag, and escalating symptomatic drug trials without a function plan are markers of a stalled, iatrogenic trajectory. Document the reasoning that supports stopping, so the next clinician does not restart the cascade. [10] [1]
Management — Resuscitation
Most SSRD care is planned and rehabilitative, but a "routine" visit can tip into crisis in one disclosure. There is no pharmacological "rescue" for the core disorder, and the resuscitation skill is to recognise the emergencies that surface around it. [1]
- Acute suicidality or self-harm: never leave the young person alone; perform a same-visit suicide and safety assessment (ideation, plan, intent, means, prior attempts, protective factors), remove means, and arrange urgent mental-health or crisis pathway care. SSRD and self-harm cluster, so this is a recognised emergency in this population. [1]
- Suspected fabricated or induced illness: treat as a safeguarding presentation. Document carefully and objectively, refer to the local child-protection/multi-agency pathway, do not confront the carer alone, and do not withold clinically necessary treatment while the process runs. [2]
- A newly disclosed red flag: re-enter the diagnostic pathway with targeted bloods and directed imaging for the specific concern; reassess for organic disease. Do not abandon the functional plan if organic disease is again excluded, but never let a functional label stop you from thinking. [1]
Document decisions, the safety plan, and who was informed. Where confidentiality is overridden for safety, tell the young person what you must do and why. [1]
Management — Definitive & Stepwise
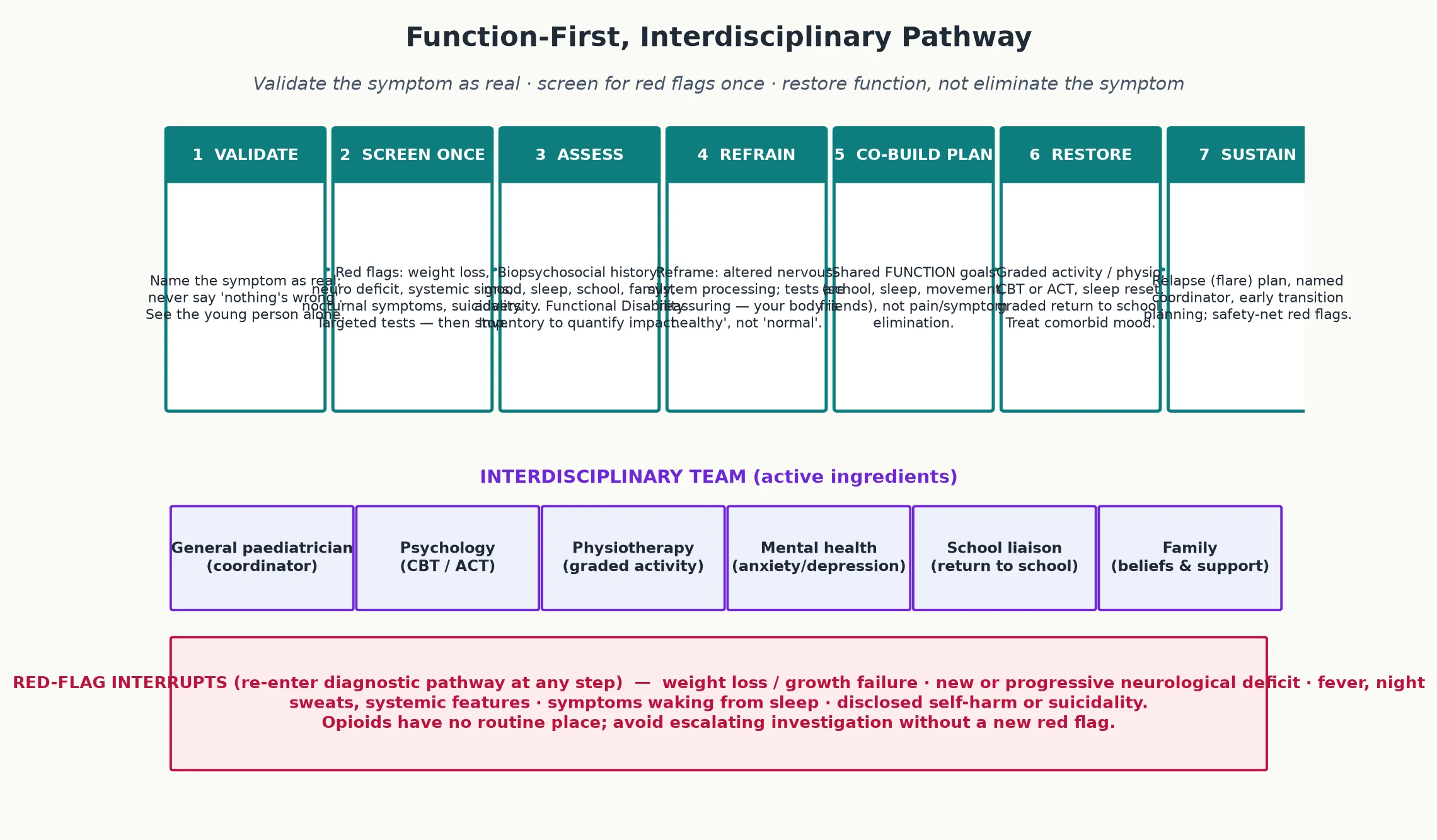
Read the figure like this: school reintegration and restored function sit at the centre of the algorithm, not at the end. The interdisciplinary team is the active ingredient, not optional ornamentation. [7]
Stepwise pathway
- Validate. Name the symptom as real; never say "nothing's wrong." See the young person alone and secure the alliance. [3]
- Screen once. Red flags and suicidality, targeted tests to exclude organic disease — then stop the cascade. [1]
- Assess. Biopsychosocial history, mood, sleep, school, family, adversity and bullying; quantify disability with the Functional Disability Inventory. [7]
- Reframe. Explain altered nervous-system processing and the symptom-amplification loop in validating language; communicate normal results as "reassuring — your body is healthy." [1] [10]
- Co-build the plan. Set shared function goals (school, sleep, movement, friends), explicitly not a symptom-elimination goal. [3]
- Restore. Graded activity / physiotherapy, CBT or ACT, a sleep reset, a graded return to school; treat comorbid mood. [1]
- Sustain. Relapse (flare) plan, named coordinator, family work, early transition planning. [1]
The seven steps in one line
Validate
Symptom is real — never dismiss.
Screen once
Red flags + targeted tests — then stop.
Assess
Biopsychosocial + Functional Disability Inventory.
Reframe
Nervous-system processing; 'body is healthy'.
Co-build
Function goals, not symptom elimination.
Restore
Physio + CBT/ACT + sleep + return to school.
Sustain
Flare plan, coordinator, transition.
Psychology and rehabilitation
Cognitive behavioural therapy and acceptance and commitment therapy are the evidence-based psychological backbone, and the broader paediatric chronic-pain literature shows that psychological therapies reduce pain and disability in children and adolescents — the same principles apply to SSRD. For severe disability, prolonged school absence or refractory presentations, intensive interdisciplinary rehabilitation (day-program or inpatient) is the evidence-based escalation, because it interrupts the amplification loop on every front at once. [1] [3]
Treating comorbid mood and medication
Treat comorbid anxiety and depression — untreated mood is a modifiable driver of poor outcome. Where an SSRI is indicated for a comorbid anxiety or depressive disorder, this is initiated and monitored under child psychiatry / specialist guidance per local formulary with the standard attention to onset, monitoring and safety; there is no pharmacological treatment for the core SSRD itself. Opioids and benzodiazepines have no routine place in a paediatric somatic presentation. [1] [11]
Follow-up intensity
- Low disability, engaged young person and family: coordinated outpatient review with clear safety-netting. [1]
- Moderate disability or partial school return: structured multidisciplinary input and active school liaison. [7]
- Severe disability, complete school absence or refractory symptoms: intensive interdisciplinary rehabilitation; consider specialist psychosomatic/liaison service involvement. [3]
Specific Subtypes & Scenarios
Somatic symptom disorder with predominant abdominal pain or headache. The commonest paediatric SSRD phenotype. Validate, exclude organic disease once (including coeliac serology for abdominal presentations), reframe the amplification loop, and coordinate CBT, graded activity and a school plan. Avoid escalating analgesia. [1] [2]
Illness anxiety disorder. Minimal somatic symptoms but relentless preoccupation with having a serious illness and excessive health-checking behaviour. Management is a reassurance strategy with explicit limits on reassurance and testing, plus CBT; an open-door "come back for more tests" stance fuels the disorder. [10] [1]
Conversion disorder (functional neurological symptom disorder). Neurology confirms the diagnosis on positive grounds and excludes mimics; functional physiotherapy (a specific graded motor/sensory retraining approach) and psychology are the treatment, built on validation that the symptoms are real. Pehlivantürk and Unal's follow-up work shows good outcomes for childhood conversion with timely treatment and high rates of comorbid anxiety/depression that must be addressed. [8] [9]
Psychological factors affecting a medical condition. A real disease — asthma, diabetes, epilepsy — measurably worsened by psychosocial stress. The clinician treats both: optimise the disease management and address the stressor, often with liaison psychiatry and psychology. [1]
Fabricated or induced illness (carer-fabricated). A safeguarding emergency, not a psychiatric referral. Features include inexplicable or recurrent symptoms that occur only in the carer's presence, discordant histories between carers, eagerness for investigation and procedures, and symptoms that resolve when the child is separated from the carer. Document objectively, refer to the multi-agency child-protection pathway, and do not confront the carer alone. [2]
The school-absent adolescent. Treat school absence as a clinical marker of severity and a primary treatment target; build a graded, school-led return with education liaison. [7]
Neurodivergent child (autism, ADHD, intellectual disability). Adapt assessment and explanation to communication style and sensory profile; somatic presentations and the amplification loop may look different, and avoid diagnostic overshadowing of genuine symptoms. [1]
Trauma, out-of-home care, or housing insecurity. Assume trauma exposure and fragmented records; adopt trauma-informed pacing, clarify consent, and rebuild trust before expecting adherence. Bedard-Thomas and colleagues' life-events data underline how often adversity underlies these presentations. [5]
Complications & Pitfalls
- Over-investigation and medicalisation — each unnecessary test can reinforce a disease model and cause nocebo harm; repeated normal results erode trust rather than build it. [10] [1]
- Dismissal and stigmatising language — "it's all in your head" destroys the alliance, drives disengagement, and misses comorbidity. [1]
- Diagnostic overshadowing — a "functional" or developmental label that causes new organic symptoms to be misattributed; disabled and neurodivergent children are at highest risk. [1]
- Missed comorbidity — untreated anxiety, depression, self-harm and suicidality are the dangerous omissions in an SSRD presentation. [11]
- Prolonged school absence — social isolation, mood deterioration, identity loss and persistence into adulthood. [7]
- Fabricated/induced illness missed or mishandled — premature confrontation that endangers the child, or safeguarding failure by missing it altogether. [2]
- Iatrogenic opioid or benzodiazepine use — dependence and adverse effects for no long-term benefit in a somatic presentation. [1]
- Poor coordination and "new-doctor restarts" — each new clinician restarting the diagnostic cascade resets recovery to zero. [3]
Prognosis & Disposition
Prognosis here means the functional trajectory of the child, and it is striking how modifiable it is — a fact families often disbelieve at first contact. [1]
Better outcomes are predicted by restoration of function (school, sleep, movement, friends), treated anxiety and depression, an engaged family and an interdisciplinary plan. Where these are present, children recover meaningfully — not always to zero symptoms, but to a life no longer organised around the symptom. Where they are absent — ongoing school absence, untreated mood, family conflict, high healthcare utilisation and repeated ineffective interventions — outcomes worsen and the presentation is more likely to persist into adulthood. [7] [10]
The disposition plan spans assessment, rehabilitation and maintenance phases and names who owns each: the general paediatrician as coordinator, psychology for thoughts and mood, physiotherapy for movement, mental health for comorbid illness, and school liaison for reintegration. Specialist psychosomatic/liaison services and intensive interdisciplinary rehabilitation are indicated for severe disability or refractory presentations. Conversion disorder specifically often has a good prognosis with early functional treatment, whereas fabricated/induced illness follows a safeguarding trajectory rather than a purely clinical one. [8] [3]
Special Populations
Neurodivergent children (autism, ADHD, intellectual disability). Adapt assessment and explanation to communication and sensory profile; sensory differences alter the bodily-signal experience, and avoid diagnostic overshadowing — neurodivergence does not explain away a genuine symptom. [1]
Indigenous children (Aboriginal, Torres Strait Islander, Māori). Cultural safety, recognition of racism as a health exposure, and holistic framing matter as much as the guideline; centre the young person's community and integrate cultural and family supports. [1]
Migrant and refugee children. A professional interpreter is required for sensitive content; family members are not equivalent. Apply trauma-informed care and respect cultural framings of bodily illness. [5]
Out-of-home care and youth justice. Assume trauma exposure, fragmented records and interrupted schooling; clarify legal consent carefully and rebuild the history actively. [5]
Gender- and sexually-diverse young people. Use correct name and pronouns, recognise minority stress as a contributor to arousal and symptom amplification, and tailor assessment without making the patient a curiosity. [1]
Children with coexisting chronic physical illness or disability. Separate disease-related symptoms from the superimposed amplification component and treat both; a real disease does not make a somatic-symptom component untreatable. [2]
Housing or food insecurity. Ask before labelling a plan "non-adherent"; instability derails every rehabilitation plan you write. [5]
Evidence, Guidelines & Regional Differences
Assessment and management framework. Garralda's practitioner review (1999) and unexplained-physical-complaints review (2010) remain the reference frameworks for the assessment and management of childhood somatisation, establishing the validating, biopsychosocial, function-first approach this topic is built on. [1] [2]
Family-engaged assessment. Kozlowska's "first interview" framework (2013) describes how to conduct the opening, validating, family-engaged interview with somatising children and their families — a practical resource for the communication station. [3]
The hospitalised burden and precipitants. The Boston Children's Hospital (Ibeziako, Bujoreanu, Bedard-Thomas) body of work establishes the inpatient burden of paediatric SSRD: high rates of comorbid pain, a heavy load of negative life events, and frequent bullying victimisation among hospitalised children with SSRD. These papers anchor the biopsychosocial precipitant profile. [4] [5] [6]
Conversion disorder outcomes and comorbidity. Pehlivantürk and Unal's clinical and follow-up studies establish that childhood conversion disorder carries high psychiatric comorbidity (anxiety and depression) and that outcomes are generally favourable with timely treatment — the evidence base for early functional intervention. [9] [8]
Functional measurement. Claar and Walker's psychometric validation of the Functional Disability Inventory gives the field a reliable, validated tool to quantify the very disability the plan targets. [7]
Risk factors and healthcare use. Smakowski and colleagues' meta-analysis (2024) confirms anxiety, depression and catastrophising as psychological risk factors for somatic symptom disorder, and Puri and Dimsdale (2011) frame poor reassurance and high healthcare utilisation as predictors of the somatoform trajectory rather than indications for more testing. [11] [10]
Where the evidence is weak. High-quality randomised trials specifically of interventions for the full DSM-5 SSRD category in children remain scarce; much practice is extrapolated from the paediatric chronic pain, recurrent abdominal pain and functional neurological symptom literature. State this honestly in a long-case answer. [1]
ANZ: RCH Melbourne clinical guidance and state-based paediatric psychosomatic/liaison services deliver interdisciplinary and intensive rehabilitation; RACP training frames SSRD under general and developmental/behavioural paediatrics. School-health integration varies by state. UK: RCPCH Progress+ (mental health and behavioural presentations) and NICE principles for medically unexplained symptoms (applied with developmental adaptation in children) emphasise early psychosocial intervention, avoidance of opioids, and liaison with child and adolescent mental health services. US: AAP guidance and the move away from opioids for chronic non-cancer symptoms in young people; access to intensive interdisciplinary programs is uneven; the Boston Children's model of paediatric consultation-liaison for SSRD is influential. Canada: Canadian Paediatric Society guidance and provincial psychosomatic/liaison networks; rural-remote access is a recognised equity gap.
Exam Pearls
- Open every answer by validating the symptom as real and screening once for red flags — never dismiss as "all in the head." [1]
- State the pivotal DSM-5 principle: symptoms need not be medically unexplained — diagnose the positive pattern of disproportionate thoughts, feelings and behaviours. [2]
- Name the five DSM-5 categories and the one discriminating feature of each — especially intentionality as the line between factitious disorder and the rest. [2]
- Investigations exclude organic disease once with a targeted panel — then stop; over-investigation is a cause of harm, not diligence. [10]
- Function (school, sleep, movement, friends) is the goal and the outcome metric — never symptom elimination. [7]
- Opioids have no routine place; treat comorbid mood with appropriate therapy and specialist input. [1]
- Fabricated or induced illness = safeguarding: document objectively, refer to the multi-agency pathway, do not confront the carer alone. [2]
- Communicate normal results as "reassuring — your body is healthy," never "nothing is wrong." [10]
- Conversion disorder is diagnosed on positive grounds (incompatibility with disease) after targeted exclusion — not as a diagnosis of exhaustion. [8]
- Guard against diagnostic overshadowing, especially in disabled and neurodivergent children. [1]
VALIDATE-SSRD care anchors
References
- [1]Garralda ME Practitioner review: Assessment and management of somatisation in childhood and adolescence: a practical perspective. Journal of child psychology and psychiatry, and allied disciplines, 1999.PMID 10604395
- [2]Garralda ME Unexplained physical complaints. Child and adolescent psychiatric clinics of North America, 2010.PMID 20478496
- [3]Kozlowska K; English M; Savage B Connecting body and mind: the first interview with somatising patients and their families. Clinical child psychology and psychiatry, 2013.PMID 22969165
- [4]Ibeziako P; Randall E; Vassilopoulos A; Choi C; Thomson K Prevalence, Patterns, and Correlates of Pain in Medically Hospitalized Pediatric Patients With Somatic Symptom and Related Disorders. Journal of the Academy of Consultation and Liaison Psychiatry, 2021.PMID 32641234
- [5]Bedard-Thomas KK; Bujoreanu S; Choi CH; Ibeziako PI Perception and Impact of Life Events in Medically Hospitalized Patients With Somatic Symptom and Related Disorders. Hospital pediatrics, 2018.PMID 30327327
- [6]Ibeziako P; Choi C; Randall E; Bujoreanu S Bullying Victimization in Medically Hospitalized Patients With Somatic Symptom and Related Disorders: Prevalence and Associated Factors. Hospital pediatrics, 2016.PMID 27073256
- [7]Claar RL; Walker LS Functional assessment of pediatric pain patients: psychometric properties of the functional disability inventory. Pain, 2006.PMID 16480823
- [8]Pehlivantürk B; Unal F Conversion disorder in children and adolescents: a 4-year follow-up study. Journal of psychosomatic research, 2002.PMID 11943237
- [9]Pehlivantürk B; Unal F Conversion disorder in children and adolescents: clinical features and comorbidity with depressive and anxiety disorders. Turkish journal of pediatrics, 2000.PMID 10936979
- [10]Puri PR; Dimsdale JE Health care utilization and poor reassurance: potential predictors of somatoform disorders. Psychiatric clinics of North America, 2011.PMID 21889677
- [11]Smakowski A; Hüsing P; Völcker S; Löwe B; Rosmalen JGM Psychological risk factors of somatic symptom disorder: A systematic review and meta-analysis of cross-sectional and longitudinal studies. Journal of psychosomatic research, 2024.PMID 38365462