Paeds · nephrology-urology-fluids-and-electrolytes
Acid-base disorders in children
Also known as Acid-base disorders in children · Acid-base disturbances · Metabolic acidosis · Metabolic alkalosis · Respiratory acidosis · Respiratory alkalosis · Anion gap · Winters formula · Mixed acid-base disorder · Delta gap
Fellowship guide to acid-base disorders in children: a systematic six-step approach to any blood gas, the anion gap and its albumin correction, Winters formula for the expected pCO2 in metabolic acidosis, the delta gap for mixed disorders, and the compensation rules for each of the four primary disorders, anchored in diabetic ketoacidosis as the commonest high anion gap metabolic acidosis, diarrhoea and renal tubular acidosis as the normal anion gap acidoses, chloride-responsive metabolic alkalosis, and the respiratory acidoses and alkaloses of bronchiolitis, asthma and hyperventilation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
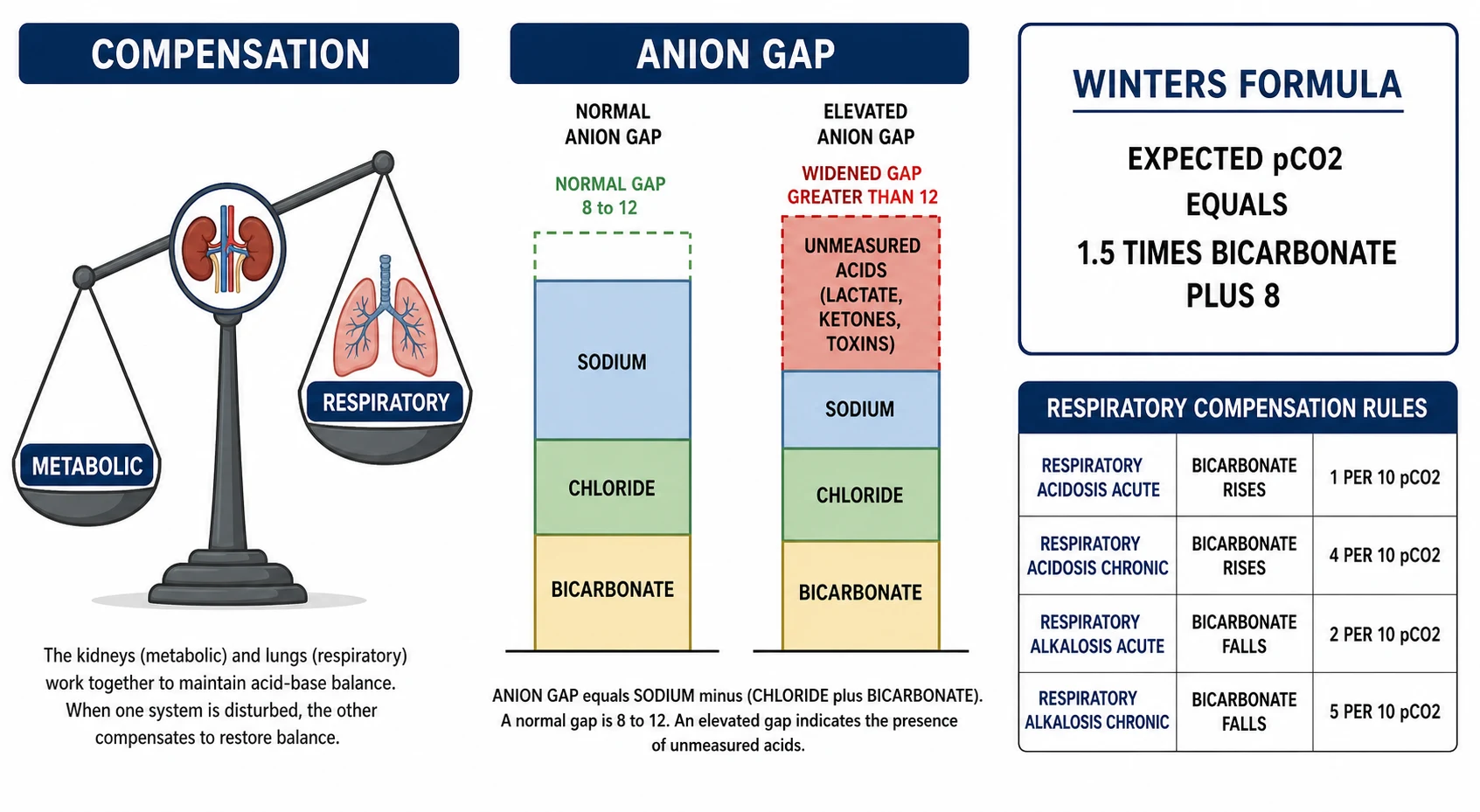
Every blood gas is a story about two variables working in opposition. The Henderson-Hasselbalch equation sets the pH from the ratio of bicarbonate to dissolved carbon dioxide, and the body defends that ratio with two organs: the kidney controls bicarbonate over hours to days, and the lung controls carbon dioxide over seconds to minutes. When one variable moves abnormally, the other shifts in the same direction to pull the pH back toward normal, and that is called compensation. A disorder is "simple" when the compensation is appropriate and "mixed" when a second process is also at work, and the whole skill of acid-base interpretation is telling those two apart with a small set of calculations rather than guesswork. [1] [11]
In children, three things make the gas harder to read than in adults. Normal values shift with age, so a neonate runs a lower bicarbonate and carbon dioxide tension than a teenager. The common disorders differ, with diabetic ketoacidosis, bronchiolitis, asthma and inherited metabolic disease dominating rather than the chronic renal and respiratory disease of adults. And the child decompensates faster, because the smaller body buffers less acid and the airway gives way more quickly, so the gas is both a diagnostic and an emergency tool. This page builds the model around the systematic approach, then applies it to the four primary disorders and their paediatric causes. [2] [7]
Overview & Definition
Acid-base homeostasis keeps the arterial pH between 7.35 and 7.45 by balancing acid generation against excretion. The body produces acid constantly from protein metabolism and carbon dioxide load, and it disposes of it through the lung (as carbon dioxide) and the kidney (as titratable acid and ammonium). A disorder arises when generation overwhelms excretion, or when excretion fails, and the result is a pH that drifts outside the normal range. The venous or arterial blood gas measures the three numbers that define the disturbance: pH, the carbon dioxide tension, and the bicarbonate concentration. [1] [11]
The first decision on any gas is the pH itself. Acidemia is a pH below 7.35 and alkalemia is a pH above 7.45; a pH within the normal range with abnormal carbon dioxide and bicarbonate means a mixed disorder or a fully compensated single disorder. The pH names the dominant process and sets the direction of the analysis, because the body never over-compensates. If the pH is acidemic, the primary process is an acidosis; if it is alkalemic, the primary process is an alkalosis, and only then do the carbon dioxide and bicarbonate reveal whether that process is metabolic or respiratory. [1] [2]
Four primary disorders cover almost everything a clinician meets. Metabolic acidosis is a fall in bicarbonate from acid gain or bicarbonate loss. Metabolic alkalosis is a rise in bicarbonate from acid loss or bicarbonate gain. Respiratory acidosis is a rise in carbon dioxide tension from hypoventilation. Respiratory alkalosis is a fall in carbon dioxide tension from hyperventilation. Each has a characteristic compensation, and the task of the systematic approach is to confirm that the compensation is appropriate, because an inappropriate compensation unmasks a second disorder. [1] [3]
Classification
The classification of acid-base disorders is built around two questions: which variable moved first, and is the compensation appropriate. The figure below lays the four primary disorders onto a single decision tree that begins with the pH and branches into metabolic and respiratory arms, with the anion gap and the compensation rules as the second-tier discriminators. [1] [2]
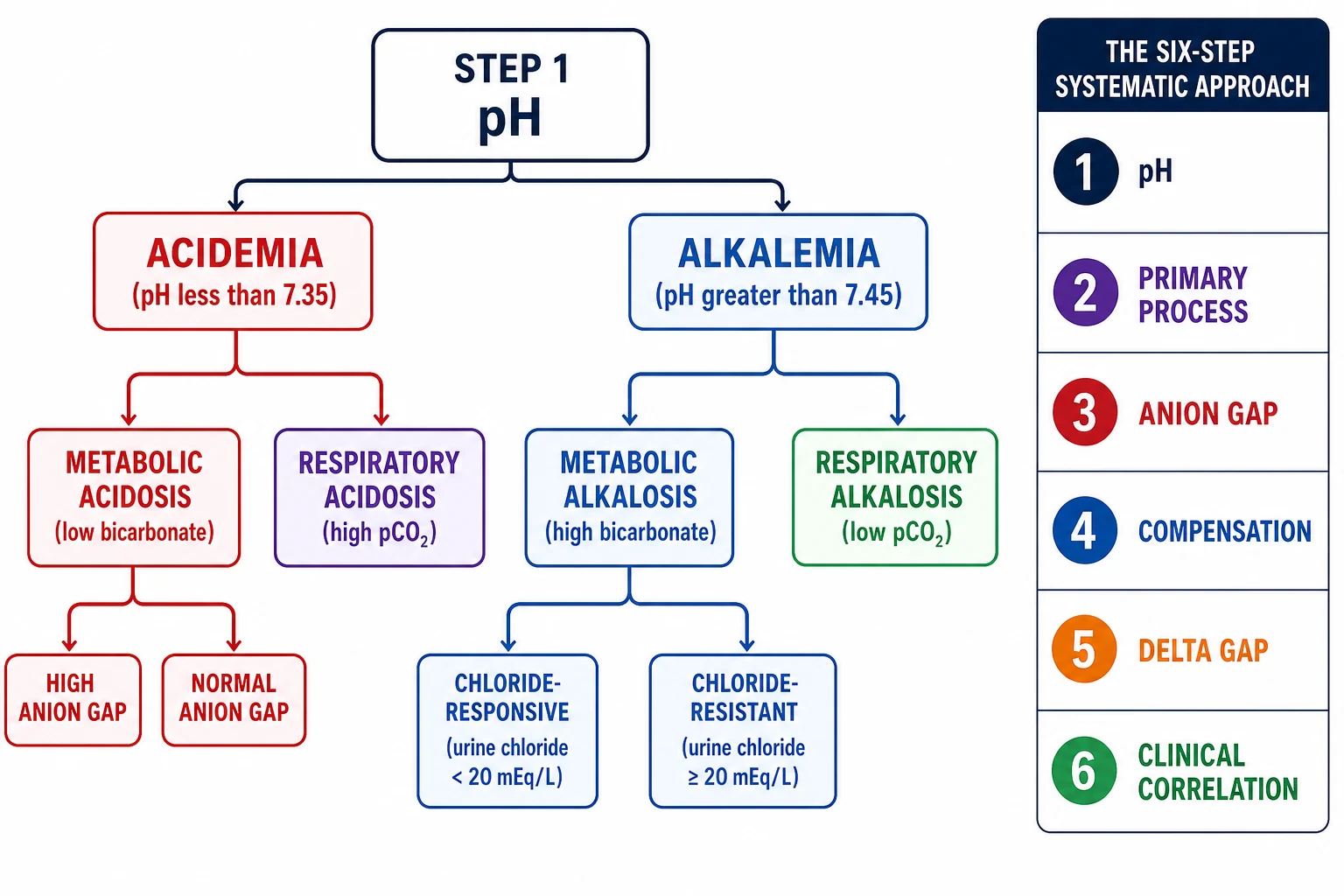
Metabolic acidosis divides most usefully by the anion gap, because the gap separates acid gain from bicarbonate loss and redirects the whole differential. A high anion gap metabolic acidosis means unmeasured acid has accumulated, and in children the causes are diabetic ketoacidosis, lactic acidosis from shock or sepsis, renal failure, and the toxins and inborn errors of metabolism. A normal anion gap (hyperchloraemic) metabolic acidosis means bicarbonate has been lost or diluted, and in children the causes are diarrhoea, renal tubular acidosis, acetazolamide, and aggressive normal saline resuscitation. The anion gap is the gate through which every metabolic acidosis must pass. [3] [4]
Metabolic alkalosis divides by the urinary chloride, which separates chloride-responsive from chloride-resistant causes. The chloride-responsive alkaloses are driven by volume and chloride depletion, with vomiting, nasogastric drainage and diuretic use as the paediatric mainstays, and they correct with saline and potassium. The chloride-resistant alkaloses are driven by mineralocorticoid excess, with hyperaldosteronism, Cushing syndrome and exogenous steroid as the examples, and they do not correct with saline because the kidney keeps generating bicarbonate. The respiratory disorders track the drive to breathe: respiratory acidosis from hypoventilation in bronchiolitis, asthma, neuromuscular weakness and opiate overdose, and respiratory alkalosis from hyperventilation in anxiety, pain, fever, hypoxia and early salicylate toxicity. [12] [2]
Metabolic acidosis
- Low bicarbonate with acidemia as the primary process
- Split by the anion gap: high gap (acid gain) versus normal gap (bicarbonate loss)
- High gap: DKA, lactic acidosis, renal failure, toxins, inborn errors
- Normal gap: diarrhoea, renal tubular acidosis, acetazolamide, saline
- Compensation: pCO2 falls by Winters (1.5 x HCO3 + 8)
Metabolic alkalosis
- High bicarbonate with alkalemia as the primary process
- Split by urine chloride: responsive (low) versus resistant (high)
- Responsive: vomiting, nasogastric losses, diuretics
- Resistant: mineralocorticoid excess, steroid, Bartter and Gitelman
- Compensation: pCO2 rises 0.6 mmHg per 1 mmol rise in bicarbonate
Respiratory acidosis
- High pCO2 with acidemia from alveolar hypoventilation
- Acute: HCO3 rises 1 mmol per 10 mmHg rise in pCO2
- Chronic (3 to 5 days): HCO3 rises 3.5 to 4 mmol per 10 mmHg
- Causes: bronchiolitis, severe asthma, neuromuscular weakness, opiates
- Treat the cause and support ventilation, do not lower pCO2 fast
Respiratory alkalosis
- Low pCO2 with alkalemia from alveolar hyperventilation
- Acute: HCO3 falls 2 mmol per 10 mmHg fall in pCO2
- Chronic: HCO3 falls 4 to 5 mmol per 10 mmHg fall
- Causes: anxiety, pain, fever, hypoxia, early salicylate, CNS lesion
- Treat the cause; correct hypoxia with oxygen rather than sedation
Epidemiology & Risk Factors
Diabetic ketoacidosis is the single commonest cause of a high anion gap metabolic acidosis in children, and it is the disorder around which paediatric acid-base teaching turns. It arises from absolute insulin deficiency in type 1 diabetes, producing unrestrained lipolysis and the generation of ketoacids that consume bicarbonate and widen the anion gap. Around a quarter of children present in DKA at first diagnosis of diabetes, and missed DKA remains a leading cause of death in childhood diabetes, which is why every sick child with polyuria, polydipsia, weight loss and vomiting needs a glucose and a gas. [5] [6]
Lactic acidosis is the next commonest high gap acidosis in the acutely unwell child, and it reflects tissue hypoxia from shock, sepsis, severe anaemia or hypoxaemia. It is a marker of illness severity as much as a diagnosis, and a rising lactate with a widening anion gap is a signal to reassess perfusion, not simply to give bicarbonate. Renal failure contributes a uraemic acidosis as the glomerular filtration rate falls and the kidney can no longer excrete the daily acid load, while the toxins and inborn errors of metabolism present in infancy with vomiting, encephalopathy and a high anion gap that demands an expanded newborn-screen and metabolic workup. [3] [7]
The normal anion gap acidoses are dominated by diarrhoea in infants and young children, because stool is rich in bicarbonate and severe gastroenteritis can deplete it faster than the kidney can compensate. Renal tubular acidosis is the other major paediatric cause, presenting in infancy with failure to thrive, and it is the subject of its own topic because the type (distal, proximal or type 4) changes the potassium and the treatment. Iatrogenic normal gap acidosis is increasingly common in hospitalised children: large-volume normal saline drives a hyperchloraemic acidosis by loading chloride, and acetazolamide wastes bicarbonate in the treated child. [4] [9]
Metabolic alkalosis in children is most often the result of gastric acid loss, through vomiting in pyloric stenosis or prolonged nasogastric drainage, or of diuretic therapy that contracts the volume and wastes potassium and hydrogen. Chloride-resistant alkalosis is rarer and points to endocrine disease, including Bartter and Gitelman syndromes and the mineralocorticoid excess of Cushing syndrome or exogenous steroid. The respiratory disorders are almost always a direct read of the work of breathing and the drive to ventilate: a tired infant in bronchiolitis retains carbon dioxide, an adolescent in an asthma attack does the same, and the anxious or painful child hyperventilates. [12] [2]
Pathophysiology
The bicarbonate buffer is the body's first line of defence against a pH change, and the Henderson-Hasselbalch equation expresses it. The pH equals 6.1 plus the logarithm of the bicarbonate concentration divided by 0.03 times the carbon dioxide tension, so the pH depends on the ratio of the two, not on either alone. Doubling the bicarbonate and the carbon dioxide tension together leaves the pH unchanged, which is exactly what compensation achieves: the lung and the kidney move the two variables in the same direction to hold the ratio and defend the pH. [1] [11]
Metabolic acidosis arises when acid accumulates or bicarbonate is lost. When a strong acid enters the extracellular fluid, its hydrogen ion is buffered by bicarbonate, which is consumed and converted to carbon dioxide and water, so the bicarbonate falls and chloride is unchanged; if the acid is an unmeasured anion like lactate or a ketone, the anion gap widens. When bicarbonate is lost directly through diarrhoea or a renal tubular defect, chloride rises to preserve electroneutrality, the anion gap stays normal, and the acidosis is hyperchloraemic. This single distinction is why the anion gap is calculated on every metabolic acidosis, and why it is the second step of the systematic approach. [3] [4]
Metabolic alkalosis arises when hydrogen ion is lost or bicarbonate is generated and then maintained. Gastric acid loss removes hydrogen and chloride, producing a hypochloraemic alkalosis that the kidney cannot correct while chloride and volume remain depleted, because the distal nephron keeps reabsorbing bicarbonate to maintain electroneutrality as sodium is reabsorbed without chloride. The potassium and hydrogen that leak into the distal tubule in this state worsen the alkalosis and the hypokalaemia, which is why chloride, volume and potassium replacement are the treatment of the chloride-responsive alkalosis. [12] [2]
Respiratory acidosis arises when alveolar ventilation falls and carbon dioxide accumulates. Within minutes the bicarbonate buffer absorbs some of the acid load, but the kidney is the real compensator, and over three to five days it generates new bicarbonate to restore the ratio toward normal, which is why the chronic compensation is larger than the acute. Respiratory alkalosis is the mirror image: hyperventilation blows off carbon dioxide, the pH rises, and the kidney excretes bicarbonate over days to compensate. The clinical skill is to compare the measured bicarbonate against the expected compensation for the carbon dioxide tension, because a mismatch means a second disorder is layered on the first. [1] [3]
Clinical Presentation
The presentation of an acid-base disorder is the presentation of its cause, but the acid-base disturbance itself leaves signatures that the bedside clinician should recognise. A metabolic acidosis drives Kussmaul breathing, the deep sighing respirations that attempt to blow off carbon dioxide to compensate, and the child looks unwell, dehydrated and often vomiting. The fruity breath of ketones points to DKA, the cold peripheries and prolonged capillary refill of shock point to lactic acidosis, and the vomiting and tachypnoea of an infant with an inborn error points toward the metabolic workup. [5] [7]
A metabolic alkalosis is subtler and is often found on a gas drawn for another reason. The child with pyloric stenosis presents with projectile non-bilious vomiting, dehydration and a hypokalaemic hypochloraemic alkalosis, and the visible peristalsis and palpable olive mass in the epigastrium make the diagnosis at the bedside. The child on a diuretic or with prolonged nasogastric drainage presents with weakness, polyuria and the same alkalosis. Chloride-resistant alkalosis presents with hypertension when mineralocorticoid excess is the driver, and the combination of alkalosis, hypokalaemia and high blood pressure is the clue to endocrine disease. [12] [2]
A respiratory acidosis presents as the child who is tiring and retaining carbon dioxide. The infant in severe bronchiolitis has marked subcostal and intercostal recession, head bobbing and grunting, and then becomes less reactive and more somnolent as the carbon dioxide rises and the pH falls. The child in a severe asthma attack has a silent chest, fatigue and falling peak flow, and the adolescent with neuromuscular weakness has a weak cough, a rapid fall in vital capacity and morning headaches from nocturnal hypoventilation. Oxygen saturation can be normal while carbon dioxide climbs, so a gas is essential in any tiring child. [2] [7]
A respiratory alkalosis presents as rapid deep breathing without the distress of metabolic compensation. The anxious or painful adolescent hyperventilates with perioral and digital tingling, carpopedal spasm and light-headedness from the acute fall in ionised calcium that the alkalosis causes. The child with early salicylate toxicity hyperventilates because salicylate directly stimulates the respiratory centre, and the picture evolves toward a mixed disorder as the drug produces a metabolic acidosis later. Any child with persistent hyperventilation and a normal lactate and glucose deserves a gas to separate anxiety from a serious drive. [1] [3]
Differential Diagnosis
The differential of a metabolic acidosis is organised by the anion gap, and the mnemonic is worth committing because it covers the causes examiners probe. For a high anion gap metabolic acidosis, the GOLD MARK list covers the glycols (ethylene and propylene), oxoproline from chronic paracetamol, L-lactate and D-lactate, methanol, aspirin, renal failure and ketoacidosis. For a normal anion gap acidosis the list is shorter and paediatric: diarrhoea, renal tubular acidosis, acetazolamide, saline loading and Addisonian adrenal insufficiency. The gap is the first branch, and the clinical context does the rest. [3] [4]
GOLD MARK
The differential of a metabolic alkalosis is organised by the urine chloride, which tells whether the kidney is chloride-hungry (responsive) or chloride-saturated (resistant). A low urine chloride points to vomiting, nasogastric drainage, diuretic use or chloride-losing diarrhoea, all of which correct with saline and potassium. A high urine chloride points to mineralocorticoid excess, Bartter and Gitelman syndromes, or severe hypokalaemia itself, none of which correct with saline because the kidney keeps generating bicarbonate. The blood pressure separates the endocrine causes further: hypertension accompanies primary hyperaldosteronism and Cushing, while normotension accompanies Bartter and Gitelman. [12] [2]
The respiratory acidoses and alkaloses are distinguished by the bedside and the gas together. A high carbon dioxide with acidemia means hypoventilation, and the question is whether the cause is airway obstruction (bronchiolitis, severe asthma, upper airway), central depression (opiates, brainstem lesion) or neuromuscular weakness. A low carbon dioxide with alkalemia means hyperventilation, and the question is whether the drive is central (anxiety, pain, fever, salicylate, CNS lesion), hypoxic (any cause of low oxygen), or pulmonary (early asthma, pneumonia, pulmonary embolism). The key trap is to assume hyperventilation is always anxiety, because hypoxia and early salicylate toxicity are dangerous mimics. [1] [3]
Clinical & Bedside Assessment
Begin with the airway, breathing and circulation, because an acid-base disorder is often an emergency before it is a calculation. Assess the work of breathing and the pattern, because Kussmaul breathing signals metabolic acidosis and the tiring infant signals rising carbon dioxide. Feel the pulse and the perfusion, because shock drives a lactic acidosis and dehydration drives the contraction alkalosis of pyloric stenosis. Take the temperature, because fever raises the respiratory drive and sepsis drives both lactate and the gas toward a high gap acidosis. [2] [7]
The history identifies the cause faster than any calculation. Ask about polyuria, polydipsia and weight loss for diabetes, vomiting and stool pattern for gastroenteritis and pyloric stenosis, and the drug list for diuretics, acetazolamide, salicylates and opiates. Ask about asthma and the inhaler use, neuromuscular diagnoses and overnight ventilation, and the developmental and family history for inborn errors of metabolism. In the infant, ask about feeding, growth and vomiting, because the inherited metabolic and renal tubular causes present in the first months with failure to thrive. [5] [4]
Examine for the features that point to a cause and a type. The deep sighing Kussmaul respirations and ketotic breath of DKA, the cold peripheries and mottled skin of shock, the palpable olive and visible peristalsis of pyloric stenosis, and the weakness, hyporeflexia and ileus of severe hypokalaemia are all bedside signatures of the underlying disorder. In the tiring respiratory child, look for the chest wall recession, grunting and falling conscious level that signal carbon dioxide retention, and remember that oxygen saturation can be normal while the carbon dioxide climbs. [6] [2]
Assess the volume status carefully before any fluid is given, because the dehydrated child with DKA needs a careful fluid deficit correction and the dehydrated child with pyloric stenosis needs chloride and potassium before any attempt at alkalinisation. The child with chronic respiratory acidosis on a ventilator needs the carbon dioxide lowered slowly to avoid post-hypercapnic alkalosis and seizures. The gas is drawn at the bedside as part of the assessment, not after it, because the numbers only make sense when they are tied to the child in front of you. [1] [10]
Investigations
The blood gas is the core investigation, and it is interpreted with the six-step systematic approach. Whether arterial, capillary or venous, the gas gives the pH, the carbon dioxide tension and the bicarbonate, and from these the primary disorder is named. An arterial sample is the standard for the carbon dioxide tension, but a venous or capillary sample is acceptable for the pH and bicarbonate and is safer in the struggling child; the carbon dioxide tension runs roughly 4 to 6 mmHg higher in venous blood. Send the gas with the electrolytes, because the calculated bicarbonate and the measured chloride give the anion gap. [1] [11]
The anion gap is calculated as the serum sodium minus the sum of chloride and bicarbonate, with a normal range around 8 to 12 mmol per litre. It must be corrected for albumin, because albumin carries much of the unmeasured negative charge and a low albumin narrows the gap, hiding a high gap acidosis. The correction is to add 2.5 mmol per litre to the gap for every 10 g per litre the albumin falls below 40, or roughly 0.25 mmol per litre for every 1 g per litre of albumin deficit. A "normal" gap in a hypoalbuminaemic child with a metabolic acidosis is a red flag for a hidden high gap acidosis. [3] [8]
The expected respiratory compensation for a metabolic acidosis is calculated with Winters formula: the expected carbon dioxide tension equals 1.5 times the bicarbonate plus 8, with a range of plus or minus 2. If the measured value falls within that range the respiratory compensation is appropriate and the disorder is simple; if it is higher a respiratory acidosis is also present, and if lower a respiratory alkalosis. For metabolic alkalosis the expected carbon dioxide tension rises by about 0.6 mmHg for every 1 mmol per litre rise in bicarbonate above 24, and a handy check is that it approximates the last two digits of the pH. [1] [3]
The delta gap unmixes disorders when the anion gap is high. The delta ratio is the change in the anion gap divided by the change in the bicarbonate, calculated as the measured gap minus 12 over 24 minus the bicarbonate. A ratio around 1 to 2 indicates a pure high anion gap metabolic acidosis, because each excess anion should consume one bicarbonate. A ratio below 1 means an additional normal gap metabolic acidosis is present, as in a child with DKA who also has severe diarrhoea. A ratio above 2 means an additional metabolic alkalosis is present, as in a child with DKA and persistent vomiting. The delta gap turns a single acid-base picture into a precise count of the disorders at work. [3] [4]
Targeted tests follow the systematic approach and confirm the cause. A glucose and ketones confirm DKA, a lactate quantifies tissue hypoxia, and the urea and creatinine stage renal failure. A toxicology screen identifies salicylate, methanol and ethylene glycol, and the ammonia and metabolic workup identify the inborn errors. The urine anion gap, calculated as the sum of urine sodium and potassium minus urine chloride, separates a renal cause of a normal gap acidosis (positive gap, low ammonium) from a gastrointestinal cause (negative gap, high ammonium), and it is the tool that splits the normal anion gap differential at the bedside. [8] [9]
Management — Resuscitation
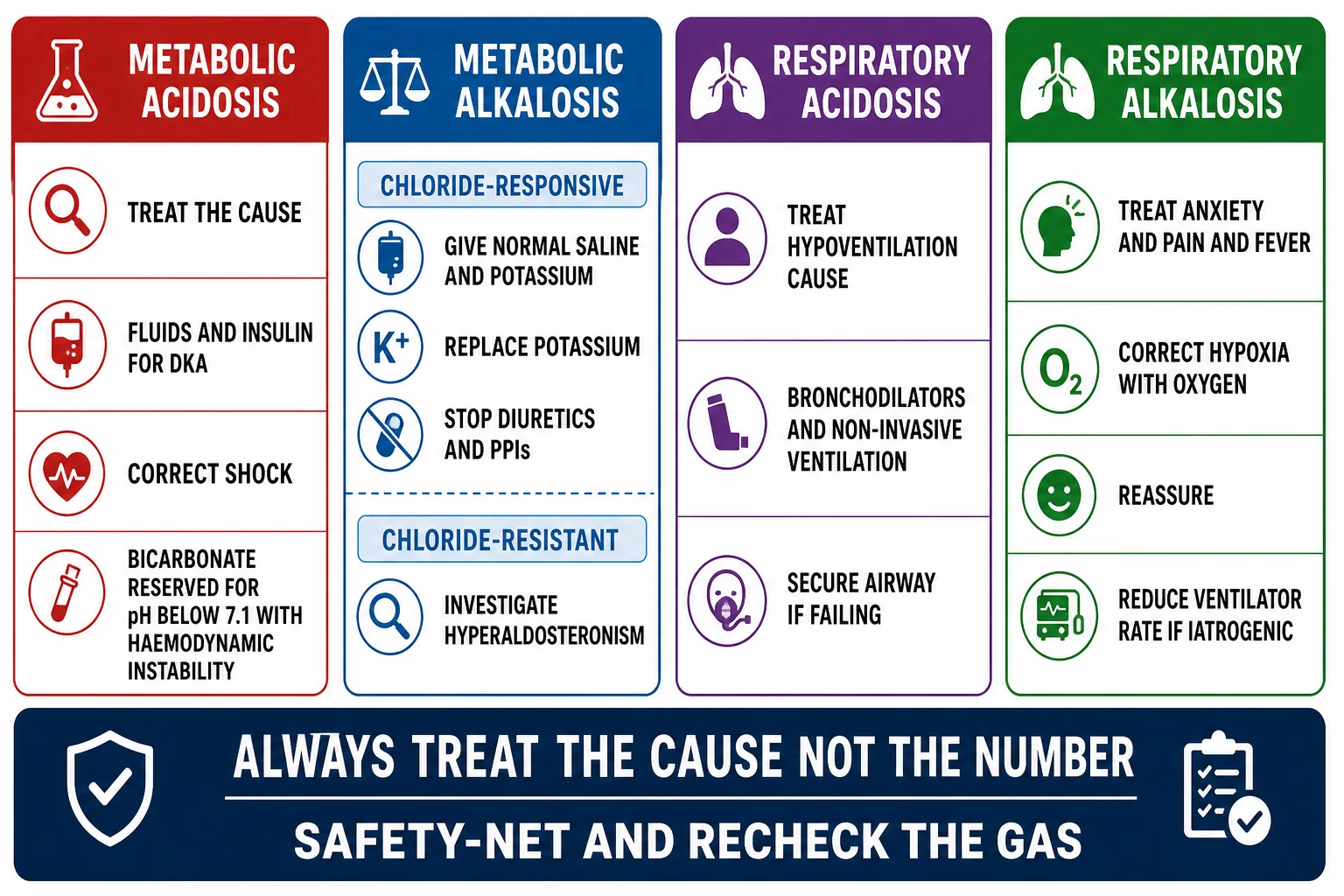
The first principle of resuscitation is to treat the cause, not the number, because an acid-base disorder is a sign of an underlying process and correcting the pH without addressing the cause does not help and often harms. The child in shock gets fluid resuscitation to restore perfusion and clear the lactate, the child in DKA gets fluids and insulin to switch off ketogenesis, and the child with a respiratory acidosis gets airway and breathing support to lower the carbon dioxide. The pH will correct as the cause is treated, and that is the goal. [1] [10]
Intravenous sodium bicarbonate is rarely indicated, and the modern evidence argues against its routine use. The trials in critically ill adults and children with severe metabolic acidosis have not shown a mortality benefit, and bicarbonate therapy in severely acidotic patients has been associated with increased mortality through worsened hypernatraemia, fluid overload and paradoxical intracellular acidosis. The exceptions where bicarbonate is still considered are a pH below 6.9 with haemodynamic instability that is not responding to fluids, life-threatening hyperkalaemia, and certain toxic ingestions such as tricyclic antidepressant or salicylate overdose where alkalinisation of the blood and urine aids clearance. In diabetic ketoacidosis bicarbonate is reserved for the rare child with pH below 6.9 and cardiovascular compromise, and it is given by the specialist team, not routinely. [10] [5]
Address the airway and breathing first in any respiratory disorder, because a rising carbon dioxide from a failing airway is immediately reversible with bag-valve-mask ventilation, high-flow nasal cannula, non-invasive ventilation or intubation. The child with a metabolic acidosis and Kussmaul breathing is moving air effectively and needs no ventilatory support unless the measured carbon dioxide climbs above the Winters expected value, at which point the respiratory muscle fatigue has tipped into failure. In the child with chronic respiratory acidosis from neuromuscular disease, non-invasive ventilation is the definitive support and the carbon dioxide is corrected slowly. [2] [7]
Sodium bicarbonate (severe metabolic acidosis, exceptional use only)
Dose
Reserved for pH below 6.9 with haemodynamic instability unresponsive to fluids, life-threatening hyperkalaemia, or specific toxin (tricyclic, salicylate); given by the specialist team, titrated to a partial not full correction
Management — Definitive & Stepwise
The definitive management of each disorder is cause-specific, and the gas is used to track the response rather than to drive the therapy. For a high anion gap metabolic acidosis from DKA, the management is structured fluid resuscitation followed by a fixed-rate insulin infusion and careful potassium replacement, with the anion gap closing as ketogenesis is switched off. For lactic acidosis the management is restoration of perfusion and oxygen delivery, with the lactate falling as shock is treated. For the toxins the management is the specific antidote or enhanced elimination, and for renal failure the management is dialysis when the acidosis or the complications demand it. [5] [6]
For a normal anion gap metabolic acidosis the management depends on whether the cause is gastrointestinal or renal. Diarrhoea is treated with rehydration and oral or intravenous bicarbonate precursor as needed, and the acidosis resolves as the gut mucosa heals. Renal tubular acidosis is treated with oral alkali, with the dose differing by type: 1 to 4 mEq per kilogram per day for distal RTA and 10 to 20 mEq per kilogram per day for proximal RTA, because the proximal tubule keeps wasting bicarbonate above its lowered threshold. Acetazolamide-induced acidosis resolves with drug cessation, and saline-induced hyperchloraemic acidosis resolves with a balanced salt solution. [4] [9]
For metabolic alkalosis the management hinges on chloride responsiveness. The chloride-responsive alkalosis corrects with normal saline and potassium chloride, because restoring volume and chloride allows the kidney to excrete the excess bicarbonate; vomiting from pyloric stenosis resolves with surgical correction after resuscitation, and diuretic-induced alkalosis resolves with potassium and chloride repletion. The chloride-resistant alkalosis does not correct with saline and requires treatment of the underlying mineralocorticoid excess, with spironolactone or eplerenone for hyperaldosteronism and the specific management of Cushing or Bartter and Gitelman syndromes. [12] [2]
For respiratory disorders the management is to support or reduce the ventilation as the cause demands. The child with respiratory acidosis from bronchiolitis or asthma receives bronchodilators, steroids and respiratory support up to and including intubation for the failing child, and the carbon dioxide is allowed to fall as the airway obstruction resolves. The child with chronic respiratory acidosis from neuromuscular weakness receives non-invasive ventilation, and the carbon dioxide is corrected slowly to avoid the post-hypercapnic alkalosis that causes seizures and arrhythmia from a fall in ionised calcium. The child with respiratory alkalosis receives treatment of the underlying anxiety, pain, fever or hypoxia, and the hyperventilation resolves as the drive is removed. [1] [7]
The six-step systematic approach to any paediatric blood gas
Step 1 — Assess the pH: acidemia below 7.35, alkalemia above 7.45, normal pH with abnormal gases means a mixed or compensated disorder
Step 2 — Identify the primary process: compare pH with pCO2 and bicarbonate to name metabolic versus respiratory
Step 3 — Calculate the anion gap as sodium minus chloride plus bicarbonate, normal 8 to 12, and correct for albumin
Step 4 — Assess compensation with Winters formula for metabolic acidosis (1.5 x HCO3 + 8) or the respiratory rules
Step 5 — Apply the delta gap to unmask mixed disorders when the anion gap is high (delta ratio 1 to 2 is pure)
Step 6 — Tie the numbers to the child at the bedside and treat the cause
Specific Subtypes & Scenarios
Diabetic ketoacidosis is the archetype of a paediatric high anion gap metabolic acidosis and deserves a dedicated handling. The combination of hyperglycaemia, ketosis and a high anion gap metabolic acidosis defines it, and the pathophysiology is absolute insulin deficiency driving unrestrained lipolysis and ketoacid generation. The gas shows a low pH, a low bicarbonate, a low compensating carbon dioxide tension, and a wide anion gap, and the management is structured fluid resuscitation, a fixed-rate intravenous insulin infusion starting after the potassium is known, careful potassium replacement, and close monitoring for the cerebral oedema that is the feared complication. Bicarbonate is reserved for the rare child with profound acidosis and cardiovascular instability. [5] [6]
Pyloric stenosis is the archetype of a paediatric chloride-responsive metabolic alkalosis. The infant, classically three to six weeks old, presents with projectile non-bilious vomiting and develops a hypokalaemic, hypochloraemic metabolic alkalosis with a low urine chloride as the stomach loses acid and chloride. The gas shows a high pH and high bicarbonate, the electrolytes show the characteristic hypokalaemic hypochloraemia, and the ultrasound confirms the hypertrophied pylorus. The management is resuscitation with normal saline and potassium chloride to correct the deficit before any anaesthesia or surgery, because the alkalosis and hypokalaemia are anaesthetic risks. [12] [2]
The inborn errors of metabolism present in infancy with a high anion gap metabolic acidosis, encephalopathy and a metabolic derangement that the systematic approach helps to frame. An expanded newborn screen, plasma amino acids, urine organic acids, ammonia and lactate are sent alongside the gas, and the management is supportive with glucose, the removal of toxic substrates, and cofactor therapy such as vitamin B12 for methylmalonic acidaemia. The high anion gap, the neurological signs and the age at presentation are the pointers, and the acid-base picture is one part of a wider metabolic emergency. [7] [3]
Chronic respiratory acidosis in the child with neuromuscular disease is the archetype of a slowly compensated respiratory disorder. The carbon dioxide rises over weeks as the respiratory muscles weaken, and the kidney generates bicarbonate to compensate, so the pH is near normal and the bicarbonate is high. The danger is iatrogenic: aggressive mechanical ventilation that lowers the carbon dioxide too fast produces a severe post-hypercapnic alkalosis, a fall in ionised calcium, seizures and arrhythmia. The management is non-invasive ventilation titrated to lower the carbon dioxide slowly, with monitoring of the pH, bicarbonate and ionised calcium throughout. [1] [10]
Complications & Pitfalls
The cardinal pitfall is treating the number rather than the cause. Bicarbonate given for a metabolic acidosis from shock, DKA or sepsis does not improve outcome and is associated with harm, because it generates carbon dioxide that diffuses into cells and worsens intracellular acidosis, it raises the sodium and causes fluid overload, and it shifts potassium into cells. The correct response to a severe acidosis is to find and treat the cause, resuscitate the circulation, and reserve bicarbonate for the narrow exceptions. The modern evidence, including the association of bicarbonate with increased mortality in severely acidotic patients, has shifted practice firmly away from routine alkalinisation. [10] [3]
The second pitfall is missing a mixed disorder. A child with DKA and persistent vomiting may have a high anion gap metabolic acidosis layered with a metabolic alkalosis, and the delta ratio above 2 is the clue. A child with chronic obstructive lung disease and sepsis may have a respiratory acidosis layered with a metabolic acidosis, and the carbon dioxide higher than the Winters expected value is the clue. Applying the full systematic approach, including the delta gap and the compensation check, prevents the common error of reading only the headline pH and missing the second process. [1] [4]
The third pitfall is failing to correct the anion gap for albumin. A hypoalbuminaemic child in intensive care may have a deceptively normal calculated gap that hides a significant high gap acidosis, because each fall of 10 g per litre in albumin narrows the gap by about 2.5 mmol per litre. The correction is simple and it changes the diagnosis, so it should be applied to every anion gap calculated in a sick child, particularly those with nephrotic syndrome, liver disease or critical illness where the albumin is low. [3] [8]
The fourth pitfall is over-rapid correction of chronic respiratory acidosis. The kidney has spent days generating bicarbonate to compensate for the high carbon dioxide, and if ventilation suddenly normalises the carbon dioxide, the bicarbonate remains high and the child develops a severe metabolic alkalosis with a fall in ionised calcium that causes seizures, tetany and arrhythmia. The rule in chronic respiratory acidosis is to lower the carbon dioxide slowly, over hours to days, with close monitoring of the pH, bicarbonate and ionised calcium. [1] [2]
Prognosis & Disposition
Prognosis in an acid-base disorder is the prognosis of the underlying cause, but the severity and duration of the disturbance modify it. A high anion gap metabolic acidosis from DKA has an excellent prognosis with structured management, and the mortality is low in centres that follow a protocol, though cerebral oedema remains the feared complication in children. A lactic acidosis from shock carries the prognosis of the shock, and a persistently high lactate is a marker of ongoing tissue hypoxia that demands reassessment. The inborn errors carry the prognosis of the specific disease, and early diagnosis changes the trajectory. [5] [7]
The normal anion gap acidoses have a prognosis governed by their cause. Diarrhoea resolves with rehydration, renal tubular acidosis is controlled with lifelong alkali and has a good prognosis when treated early, and the iatrogenic acidoses from saline or acetazolamide resolve with the change in therapy. The chloride-responsive metabolic alkalosis of pyloric stenosis resolves with resuscitation and surgery. The chronic respiratory disorders carry the prognosis of the underlying neuromuscular or pulmonary disease, and the goal of therapy is to maintain gas exchange and growth rather than to normalise the gas. [9] [12]
Disposition follows the severity and the cause. Any child with a significant metabolic or respiratory acidosis, or with haemodynamic instability, belongs in a high-dependency or intensive care setting for close monitoring and organ support. The child with mild DKA on a protocol may be managed on the ward with close observation, while the child with severe DKA, shock, or a failing respiratory effort needs intensive care. Most children stabilise as the cause is treated and step down to the ward and then home, with follow-up specific to the underlying diagnosis. [6] [7]
The monitoring plan tracks the gas, the electrolytes and the cause. Serial blood gases confirm that the pH, the carbon dioxide and the bicarbonate are moving in the expected direction, and the anion gap and lactate confirm that the underlying process is resolving. Potassium, chloride, sodium and calcium are monitored because they shift as the pH changes, and the child on insulin for DKA needs hourly glucose and potassium. On discharge, give the family a safety-net that names the warning signs of the underlying disease, and ensure the diagnosis is communicated to the primary team for follow-up. [5] [1]
Special Populations
Neonates and infants are the population in which acid-base interpretation is both hardest and most important. The normal values differ, with a lower bicarbonate and carbon dioxide tension than older children, and the buffer capacity is smaller, so the pH falls faster with an acid load. The common disorders differ too: inborn errors of metabolism, congenital adrenal hyperplasia, pyloric stenosis and severe bronchiolitis dominate, and the presentation is often non-specific, with poor feeding, lethargy, vomiting and tachypnoea. A gas is part of the septic and metabolic workup of any sick neonate, and a high anion gap acidosis with a deranged glucose demands an ammonia and a metabolic screen. [7] [2]
Children with complex chronic conditions are especially vulnerable to iatrogenic acid-base disorders. The child on diuretics for cardiac or renal disease develops a metabolic alkalosis, the child on acetazolamide for glaucoma or raised intracranial pressure develops a normal gap metabolic acidosis, and the child resuscitated with large volumes of normal saline develops a hyperchloraemic acidosis. A medication and fluid review is part of every acid-base assessment in this group, and changes should be made one at a time with follow-up gases, because the contribution of each therapy to the acid-base balance is hard to predict in combination. [4] [12]
Children with diabetes present the largest single group, and DKA is the archetypal acid-base emergency of childhood. Education of the family and the young person in sick-day rules, ketone monitoring and insulin adjustment prevents recurrence, and a structured transition to adult diabetes care maintains the vigilance that protects against DKA in adolescence and young adulthood. The acid-base disorder is the acute presentation of a chronic disease, and the prognosis is shaped by the quality of the long-term diabetes care as much as by the management of the acute episode. [5] [6]
Adolescents with eating disorders, self-induced vomiting or laxative abuse present with characteristic acid-base patterns that are easily misattributed. A hypokalaemic hypochloraemic metabolic alkalosis in a young person without an obvious surgical cause should raise an eating disorder in the differential, alongside pyloric stenosis in the infant and the diuretic abuser. The acid-base picture is a window onto the behaviour, and the management is as much psychological as physiological, with careful electrolyte correction and a multidisciplinary approach to the underlying disorder. [12] [2]
Evidence, Guidelines & Regional Differences
The systematic six-step approach to acid-base interpretation is the international standard, and it is articulated in the physiological reviews of Berend and colleagues and the clinical approach of Kraut and Madias. The anion gap, the albumin correction, Winters formula and the delta gap together allow a disciplined interpretation of any gas, and the evidence for their use is drawn from decades of physiological study rather than a single trial. The approach is robust and reproducible, and it is the framework taught in paediatric and adult training worldwide. [1] [3]
The role of intravenous bicarbonate in severe metabolic acidosis is the area where evidence has most changed practice. The early physiological rationale that a low pH impairs cellular function was not borne out in trials, which showed that bicarbonate did not improve outcomes in lactic acidosis, and the observational data in severely acidotic trauma patients found an association with increased mortality. The current consensus, reflected in the surviving sepsis and critical care guidelines, reserves bicarbonate for a pH below 6.9 to 7.0 with haemodynamic instability, life-threatening hyperkalaemia, or specific toxin removal, and it is not used routinely in DKA. [10] [3]
ANZ paediatric practice follows the international evidence for acid-base interpretation and management. The ISPAD-aligned protocols for DKA, used across Australian and New Zealand paediatric diabetes services, reserve bicarbonate for the rare child with profound acidosis and cardiovascular instability, and the fluid and insulin protocols are standardised across units. The systematic approach to the gas is taught in the RACP and RCPCH curricula, and the anion gap, Winters formula and delta gap are expected knowledge at the fellowship examination. Local unit protocols for fluid composition and insulin rates should always be confirmed. [5] [1]
International consensus, as reflected in the ISPAD guidelines for DKA, the surviving sepsis guidance for lactic acidosis, and the physiological reviews of Berend and Kraut and Madias, applies the same systematic approach and the same caution around bicarbonate. Regional differences exist in the choice of resuscitation fluid (balanced crystalloids are increasingly preferred over normal saline to avoid hyperchloraemic acidosis), in the threshold for intensive care admission, and in the availability of point-of-care gas analysers. The framework is common, and the local protocol should be confirmed before prescribing. [4] [7]
The evidence is weakest in three places. The exact pH threshold below which bicarbonate is indicated in paediatric DKA remains debated, and the value of pH 6.9 used by ISPAD is a consensus rather than a trial-derived number. The role of balanced crystalloids versus normal saline in preventing hyperchloraemic acidosis during paediatric resuscitation is supported by physiological studies and adult trials but the paediatric evidence is still maturing. And the optimal rate at which to correct chronic respiratory acidosis is drawn from physiological principle and small observational series rather than trials. These are the corners where specialist discussion is most valuable. [1] [10]
The delta gap and the albumin-corrected anion gap are tools that are increasingly used but whose clinical impact on outcomes is inferred rather than proven. The studies that established their physiological basis are decades old, and the modern application relies on their logical force rather than on contemporary trials. None of this weakens their use at the bedside or in the examination, because they transform a guess about mixed disorders into a calculation, but it does frame the limits of the evidence base and the importance of tying every number to the child in front of you. [3] [4]
Exam Pearls
Commit the six-step systematic approach before anything else, because it is the spine of every acid-base question. Name the pH, identify the primary process, calculate the anion gap with its albumin correction, check the compensation with Winters formula, apply the delta gap for mixed disorders, and tie the numbers to the child. The discipline of the approach prevents the two common errors: reading only the headline pH, and missing a second disorder layered on the first. [1] [2]
The anion gap is the single most examined calculation, and it must be exact. It is the serum sodium minus the sum of chloride and bicarbonate, with a normal range of 8 to 12 mmol per litre, and it is corrected for albumin by adding 2.5 mmol per litre for every 10 g per litre the albumin falls below 40. A high gap means acid gain, a normal gap means bicarbonate loss, and the GOLD MARK mnemonic covers the high gap causes while diarrhoea and renal tubular acidosis cover the normal gap causes. The urine anion gap then splits the normal gap group into renal and gastrointestinal causes. [3] [8]
Winters formula is the compensation check that examiners reward, and it is worth memorising verbatim. The expected carbon dioxide tension in a metabolic acidosis equals 1.5 times the bicarbonate plus 8, with a range of plus or minus 2. If the measured value is higher a respiratory acidosis is also present, and if lower a respiratory alkalosis is present. The respiratory compensation rules are equally worth knowing: in respiratory acidosis the bicarbonate rises 1 mmol per 10 mmHg acutely and 3.5 to 4 chronically, and in respiratory alkalosis it falls 2 acutely and 4 to 5 chronically. [1] [3]
The delta gap is the discriminator that unmixes disorders, and it is the final step in the high-yield answer. The delta ratio is the change in anion gap over the change in bicarbonate, calculated as the measured gap minus 12 divided by 24 minus the bicarbonate. A ratio of 1 to 2 is a pure high gap acidosis, below 1 adds a normal gap acidosis, and above 2 adds a metabolic alkalosis. And never forget that bicarbonate is rarely indicated and is associated with harm, so treat the cause and reserve it for the narrow exceptions. These four facts, with the systematic approach, answer the corners of the topic. [4] [10]
References
- [1]Berend K; de Vries AP; Gans RO Physiological approach to assessment of acid-base disturbances. N Engl J Med, 2014.PMID 25295502
- [2]Carmody JB; Norwood VF A clinical approach to paediatric acid-base disorders. Postgrad Med J, 2012.PMID 22267531
- [3]Kraut JA; Madias NE Metabolic acidosis: pathophysiology, diagnosis and management. Nat Rev Nephrol, 2010.PMID 20308999
- [4]Rastegar M; Nagami GT Non-Anion-Gap Metabolic Acidosis: A Clinical Approach to Evaluation. Am J Kidney Dis, 2017.PMID 28029394
- [5]Dhatariya KK; Glaser NS; Codner E; Umpierrez GE Diabetic ketoacidosis. Nat Rev Dis Primers, 2020.PMID 32409703
- [6]Calimag APP; Chlebek S; Lerma EV Diabetic Ketoacidosis. Disease-a-Month, 2023.PMID 35577617
- [7]Zieg J; Ghose S; Raina R Electrolyte disorders related emergencies in children. BMC Nephrol, 2024.PMID 39215244
- [8]Batlle D; Ba Aqeel SH; Marquez A The Urine Anion Gap in Context. Clin J Am Soc Nephrol, 2018.PMID 29311217
- [9]Giglio S; Montini G; Trepiccione F; Gambaro G Distal renal tubular acidosis: a systematic approach from diagnosis to treatment. J Nephrol, 2021.PMID 33770395
- [10]Wilson RF; Spencer AR; Tyburski JG; Dolman H Bicarbonate therapy in severely acidotic trauma patients increases mortality. J Trauma Acute Care Surg, 2013.PMID 23271076
- [11]Berend K; Duits AJ The role of the clinical laboratory in diagnosing acid-base disorders. Crit Rev Clin Lab Sci, 2019.PMID 30917291
- [12]Luke RG; Galla JH Does chloride play an independent role in the pathogenesis of metabolic alkalosis? Semin Nephrol, 1989.PMID 2772432