Paeds · nephrology-urology-fluids-and-electrolytes
Acute kidney injury
Also known as Paediatric acute kidney injury · AKI in children · Acute renal failure · ATN in children · Paediatric renal failure
Fellowship guide to paediatric acute kidney injury: the KDIGO definition and three-stage classification using creatinine and urine output criteria, the pre-renal, intrinsic and post-renal framework with acute tubular necrosis the leading intrinsic cause in critically ill children, the staged emergency management of hyperkalaemia and fluid overload, the indications and modality choice for renal replacement therapy, and the long-term risk of chronic kidney disease that now mandates nephrology follow-up after every significant AKI episode.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who was making urine and now is not, whose creatinine is climbing and whose potassium is heading toward a danger zone, has acute kidney injury, one of the most time-critical problems on a paediatric ward or intensive care unit. The defining problem is an abrupt fall in the kidney's ability to filter blood and maintain fluid, electrolyte, and acid-base balance, unfolding over hours to days rather than the months of chronic kidney disease. The danger is immediate and biochemical: potassium rises until the heart stops, acid accumulates until it depresses myocardial function, and fluid accumulates until the lungs drown. [1]
The international standard definition is the KDIGO criteria, published in 2012 and summarised by Kellum and Lameire. Acute kidney injury is present when the serum creatinine rises by 0.3 mg per dL or more within 48 hours, or rises to 1.5 times the baseline value or more within seven days, or when the urine output falls below 0.5 mL per kg per hour for six hours. The threshold matters because it is low enough to catch injury early, before the creatinine has doubled and before the complications become irreversible, and because it gives every clinician a single, reproducible standard rather than a subjective judgement of "renal impairment." [1]
The emergency is two-sided. The failing kidney stops clearing potassium, acid, and fluid, so the child develops biochemical and volume problems that can kill within hours. At the same time the cause may be reversible, which is why resuscitation must run in parallel with a hunt for the cause and an early call to paediatric nephrology and intensive care. A child with volume-responsive pre-renal injury can recover within hours of a fluid bolus, while a child with established acute tubular necrosis needs days to weeks of support and a careful watch for the complications that determine survival. [5]
Classification
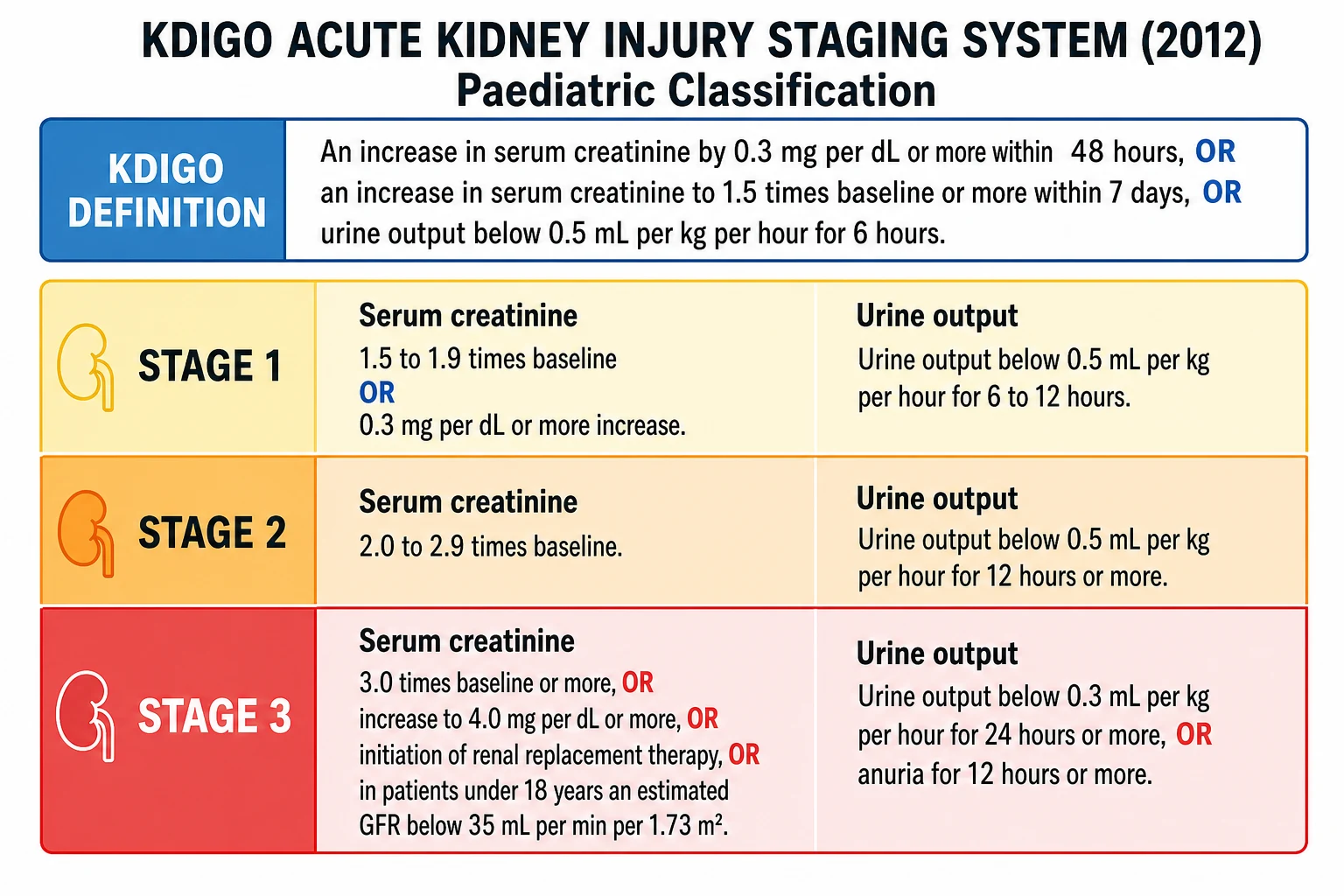
Classification serves two purposes: it confirms the child meets the diagnostic threshold, and it stages the severity, which drives the level of monitoring and the urgency of intervention. KDIGO stages severity into three grades. Stage 1 is a creatinine of 1.5 to 1.9 times the baseline value or a rise of 0.3 mg per dL or more, with a urine output below 0.5 mL per kg per hour for 6 to 12 hours. Stage 2 is a creatinine of 2.0 to 2.9 times baseline with a urine output below 0.5 mL per kg per hour for 12 hours or more. Stage 3 is the most severe: a creatinine of 3.0 times baseline or more, or a rise to 4.0 mg per dL or more, or the initiation of renal replacement therapy, or in a patient under 18 years an estimated GFR below 35 mL per min per 1.73 m2, with a urine output below 0.3 mL per kg per hour for 24 hours or more or anuria for 12 hours or more. [1]
The paediatric pRIFLE classification, derived by Akcan-Arikan and colleagues from the adult RIFLE criteria, is validated for critically ill children and uses the estimated creatinine clearance alongside the urine output. Risk is a 25 percent reduction in the estimated creatinine clearance or a urine output below 0.5 mL per kg per hour for eight hours, injury is a 50 percent reduction, and failure is a 75 percent reduction or an estimated clearance below 35 mL per min per 1.73 m2. The PODIUM consensus conference and the ADQI 26 report endorse KDIGO as the primary definition in children while recognising that pRIFLE remains useful in the intensive care setting. [3]
Stage 1
- Creatinine 1.5 to 1.9 times baseline, or 0.3 mg per dL or more rise
- Urine output below 0.5 mL per kg per hour for 6 to 12 hours
Stage 2
- Creatinine 2.0 to 2.9 times baseline
- Urine output below 0.5 mL per kg per hour for 12 hours or more
Stage 3
- Creatinine 3.0 times baseline or more, or 4.0 mg per dL or more, or renal replacement therapy
- Or in under-18s an estimated GFR below 35 mL per min per 1.73 m2
- Urine output below 0.3 mL per kg per hour for 24 hours or more, or anuria for 12 hours or more
The single most important staging judgement is the baseline creatinine, ideally a value from within the prior three months. Without a baseline, a child with chronic kidney disease may be mislabelled as having acute kidney injury, and a child with a low baseline may have their injury missed. Where no baseline exists, the clinician back-calculates an estimated baseline from the child's age and the assumption of a normal GFR, and stages the injury from there. [5]
Epidemiology & Risk Factors
Acute kidney injury is far more common in hospitalised children than was once believed, and the AWARE study established the modern benchmark. In a prospective cohort of over 4500 critically ill children and young adults, AKI occurred in 26.9 percent, and severe AKI of KDIGO stage 2 or 3 occurred in 11.6 percent. AKI was independently associated with increased mortality and a longer hospital and intensive care stay, with the risk rising steeply through the stages and highest for stage 3 and for children who needed renal replacement therapy. [4]
The risk factors group into the causes and the contexts that injure the kidney. Sepsis and septic shock are the leading precipitants of intrinsic AKI in the intensive care unit, combining inflammatory and haemodynamic injury. Cardiac surgery with cardiopulmonary bypass is a leading cause in infants with congenital heart disease, provoking a systemic inflammatory response that injures the tubules. Nephrotoxic medications, including aminoglycosides, non-steroidal anti-inflammatory drugs, ACE inhibitors, contrast media, and chemotherapy, cause a significant and preventable burden of hospital-acquired AKI, and Moffett and Goldstein showed that increasing nephrotoxic-medication exposure is associated with rising AKI rates even in non-critically ill children. Hypovolaemia from any cause, oncological disease and tumour lysis syndrome, rhabdomyolysis, and pre-existing chronic kidney disease add to the risk. [8]
Neonates are a high-risk group because of their low nephron number and immature renal function, and perinatal asphyxia, congenital heart disease, and nephrotoxic drug exposure all contribute. The AWAKEN study showed that neonatal AKI is common and often recurrent, and recurrent neonatal AKI carries a higher risk of mortality and later chronic kidney disease. Children from lower-resource settings present later and have less access to renal replacement therapy, so the preventable causes carry the greatest yield in those contexts. [11]
Pathophysiology
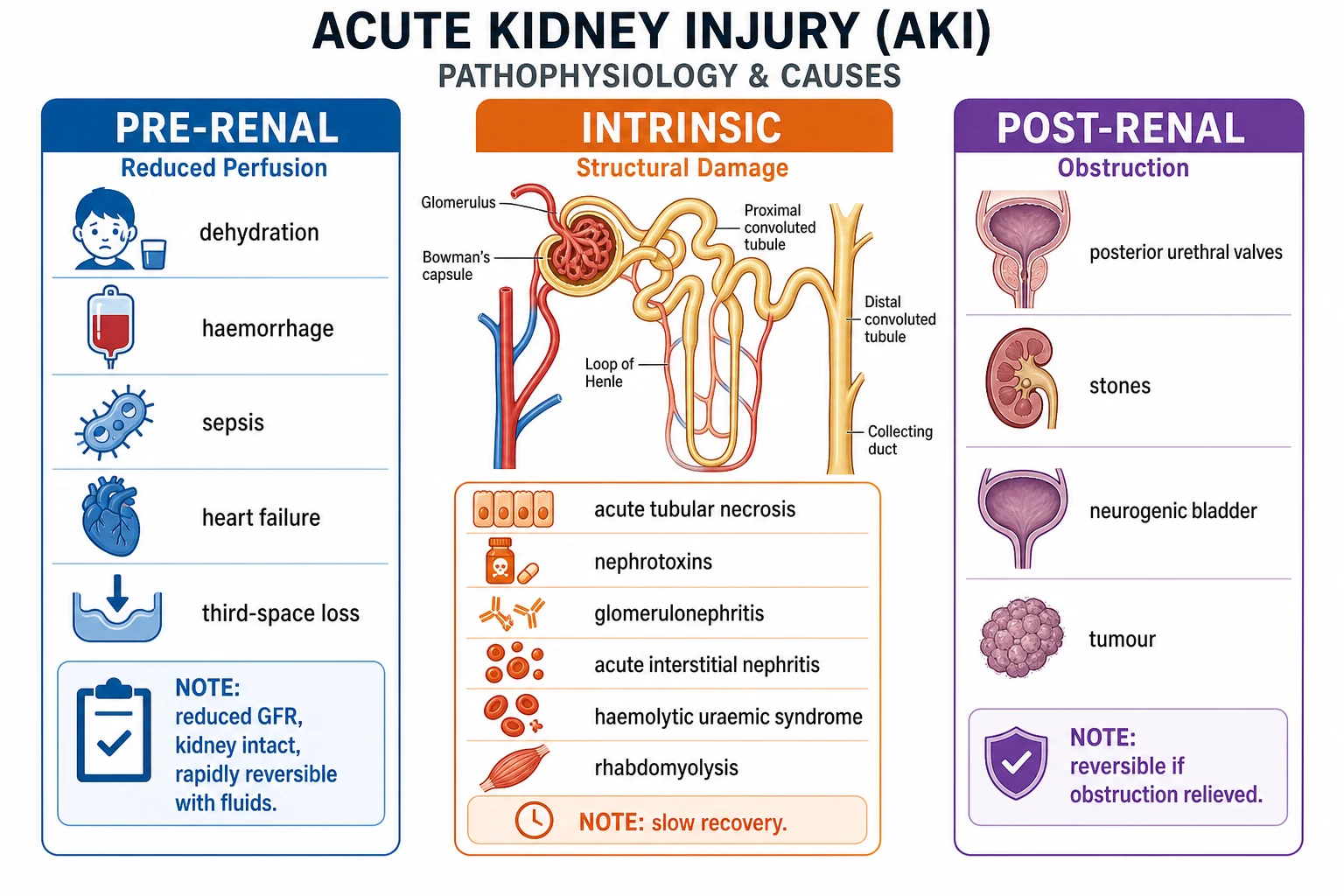
The clearest way to hold the mechanism is the three-part framework of where the injury occurs: pre-renal, intrinsic, and post-renal. Each points to a different treatment, which is why every assessment of a child with AKI asks where the problem lies. Pre-renal injury is reduced effective renal perfusion. The kidney is structurally intact, but the filtration pressure drops because too little blood reaches it, so the GFR falls and the creatinine rises. The causes are anything that reduces effective circulating volume: dehydration, haemorrhage, sepsis with vasodilation, heart failure with low cardiac output, and third-space losses from burns or capillary leak. The crucial point is that pre-renal injury reverses within hours of restoring perfusion, which is why a child with pre-renal AKI can recover dramatically after a fluid bolus. [5]
Intrinsic injury is structural damage to the kidney itself, and acute tubular necrosis from ischaemia or nephrotoxins is by far the most common form in critically ill children. Prolonged pre-renal hypoperfusion progresses to ischaemic acute tubular necrosis, which is why the distinction between the two matters: the pre-renal child recovers with fluids, while the child with established tubular necrosis does not, and the recovery takes days to weeks as the tubular cells regenerate. Other intrinsic causes have characteristic patterns: glomerulonephritis shows haematuria, proteinuria, and casts; acute interstitial nephritis follows drug exposure and shows eosinophiluria; haemolytic uraemic syndrome shows microangiopathic haemolytic anaemia and thrombocytopenia; and rhabdomyolysis and tumour lysis syndrome show pigment and crystal casts. [2]
Post-renal injury is urinary tract obstruction, and it is reversible if the obstruction is relieved promptly. The causes are structural: posterior urethral valves in male infants, stones, neurogenic bladder, and tumours compressing the urinary tract. Obstruction raises the hydrostatic pressure downstream of the block, which lowers the filtration pressure and the GFR. The kidney is structurally intact at first, but prolonged obstruction causes tubular atrophy and irreversible damage, which is why a child with obstruction needs prompt decompression by catheter or nephrostomy. [5]
The renal angina index, developed by Basu and colleagues, combines the risk-factor profile with early signs of renal injury to predict which critically ill child will progress to severe AKI within 72 hours. It is the paediatric equivalent of a cardiac risk score for the kidney, and a score of 8 or more triggers enhanced monitoring and biomarker testing. The index is useful because most AKI unfolds over hours, and early identification allows the team to stop nephrotoxins, optimise perfusion, and involve nephrology before the creatinine has climbed. [7]
Clinical Presentation
The presentation spans the spectrum from a child with oliguria and a rising creatinine who is otherwise stable, to a child in multiorgan failure with a potassium level that is about to stop the heart. The common thread is the abrupt loss of the kidney's excretory and regulatory functions, and the tempo is hours to days rather than the months of chronic kidney disease. [5]
Oliguria is the most visible sign and is defined as a urine output below 0.5 mL per kg per hour. Anuria is more severe, below 0.1 mL per kg per hour or complete absence for 12 hours or more, and signals a greater risk of complications and a higher likelihood of needing renal replacement therapy. The trap is that AKI can be non-oliguric, particularly with nephrotoxic causes such as aminoglycosides, so a normal urine output does not exclude AKI. The clinician must check the creatinine and not be reassured by a child who is still passing urine. [1]
The signs of the precipitating cause dominate the early picture. A child with dehydration is tachycardic with a prolonged capillary refill and dry mucous membranes. A child with septic shock is febrile, tachycardic, and peripherally shut down. A child with haemolytic uraemic syndrome is pale and bruised with hypertension. The biochemical consequences then take over: hyperkalaemia causes no symptom until it produces the peaked T waves and widened QRS that herald cardiac arrest; metabolic acidosis causes tachypnoea as the child tries to blow off carbon dioxide to compensate; and fluid overload causes weight gain, peripheral and then pulmonary oedema, and a rising respiratory rate. [2]
Recognising the deteriorating child with acute kidney injury
Rising serum creatinine over hours to days
Oliguria below 0.5 mL per kg per hour or anuria
Hyperkalaemia with or without ECG changes
Metabolic acidosis with a falling pH and bicarbonate
Fluid overload with weight gain and pulmonary oedema
Uraemic encephalopathy, pericardial rub, or a bleeding diathesis
Signs of severe disease that demand immediate escalation include a rapidly rising creatinine, ECG changes from hyperkalaemia, pulmonary oedema from fluid overload, hypertension from volume excess or renal disease, and uraemic encephalopathy with drowsiness and seizures. These signs mark a child who is heading toward renal replacement therapy, and the team must escalate to intensive care and nephrology before the complications become irreversible. [5]
Differential Diagnosis
The first distinction is between acute kidney injury and chronic kidney disease, because the management and prognosis differ fundamentally. Chronic kidney disease is suggested by a long history of fatigue, poor growth, polyuria, or a known renal abnormality, and by the ultrasound appearance of small, echogenic kidneys. Anaemia, renal osteodystrophy, and a long-standing hypertension point to chronic disease, and a baseline creatinine from the prior months settles the question. A child with chronic kidney disease who acutely decompensates has acute-on-chronic kidney injury, a different entity that combines the two. [5]
Within acute kidney injury, the cause is classified as pre-renal, intrinsic, or post-renal, and the differential within each category is wide. Pre-renal AKI from volume depletion responds rapidly to fluid resuscitation, with a fall in creatinine and a recovery of urine output within hours. The intrinsic causes are distinguished by their patterns, and the urinalysis, urine microscopy, and specific blood tests do most of the work. Post-renal AKI is suggested by a palpable bladder, a history of poor urinary stream, and a renal ultrasound showing hydronephrosis. [2]
Pre-renal
- Mechanism is reduced effective perfusion
- Causes: dehydration, sepsis, heart failure, third-space loss
- Fractional excretion of sodium below 1 percent
- Rapid recovery with fluid resuscitation
Intrinsic
- Mechanism is structural kidney damage
- Causes: acute tubular necrosis, glomerulonephritis, interstitial nephritis
- Fractional excretion of sodium above 1 percent
- Recovery over days to weeks, may be incomplete
Post-renal
- Mechanism is urinary tract obstruction
- Causes: posterior urethral valves, stones, neurogenic bladder
- Ultrasound shows hydronephrosis
- Recovers after decompression if prompt
The key mimics are sepsis with secondary hepatic and renal dysfunction, in which the kidney is injured by the same inflammatory and haemodynamic process that drives the septic shock, and haemolytic uraemic syndrome, which produces a distinctive picture of microangiopathic haemolytic anaemia, thrombocytopenia, and AKI after a diarrhoeal prodrome. Acute glomerulonephritis presents with haematuria, proteinuria, hypertension, and oedema, and is distinguished by its immune-mediated pattern and the low complement level in post-infectious and lupus forms. [5]
Clinical & Bedside Assessment
The assessment is performed in parallel with resuscitation and answers three questions: is the child in immediate biochemical or haemodynamic danger, what is the cause, and is there fluid overload. The airway, breathing, and circulation are assessed and stabilised first, with particular attention to the signs of shock and dehydration that would make the cause pre-renal and the injury volume-responsive. A strict fluid balance chart, a daily weight, and an accurate hourly urine output, by urinary catheter if the child is oliguric, are essential and often the only way to track the trajectory. [5]
The bedside assessment of volume status is the single most important clinical judgement in AKI, because it determines whether the child receives fluid resuscitation or fluid restriction. A hypovolaemic child is tachycardic with a prolonged capillary refill, cool peripheries, and a low jugular venous pressure, and receives isotonic crystalloid. A fluid-overloaded child is hypertensive with a raised jugular venous pressure, a gallop, crackles, and hepatomegaly, and receives fluid restriction and diuretics rather than further boluses. The trap is the child who is both septic and overloaded, in whom the volume assessment must be made with invasive monitoring or repeated bedside reassessment rather than by a single set of observations. [5]
The abdomen is examined for a palpable bladder suggesting obstruction, hepatomegaly suggesting fluid overload, and abdominal masses. The cardiovascular examination seeks hypertension from volume overload or renal disease and a gallop from heart failure. The respiratory examination seeks crackles and a raised respiratory rate from pulmonary oedema. The neurological examination seeks the drowsiness and seizures of uraemic encephalopathy or hyponatraemia. A 12-lead ECG is performed immediately if hyperkalaemia is suspected or confirmed, looking for the progression from peaked T waves through a prolonged PR interval and widened QRS to a sine-wave pattern and cardiac arrest. [2]
Investigations
The investigations confirm AKI, stage it, seek the cause, and detect the complications. The cornerstone is the serum creatinine trend against a baseline value, ideally within the prior three months. KDIGO staging uses the rise relative to baseline, so the baseline creatinine is as important as the current value, and where it is missing the clinician estimates one from the child's age and a normal GFR. The urine output is measured hourly and staged by the KDIGO urine output criteria. [1]
The electrolytes reveal the complications that drive the acute danger. Potassium rises and may reach levels that cause cardiac arrest, so it is checked urgently and rechecked frequently in the severe case. Phosphate rises and calcium falls as the failing kidney cannot excrete phosphate. Sodium is often low from water retention, and a rapid fall causes seizures. A venous or arterial blood gas reveals the metabolic acidosis with a high anion gap, and the lactate adds a measure of tissue perfusion. The full blood count shows anaemia in haemolytic uraemic syndrome or chronic disease, and a high white cell count in sepsis. [2]
The urinalysis and urine microscopy are diagnostic for the intrinsic causes. Haematuria and proteinuria with red cell casts suggest glomerulonephritis, muddy brown granular casts suggest acute tubular necrosis, white cell casts and eosinophiluria suggest acute interstitial nephritis, and a bland urine suggests pre-renal or post-renal disease. The urine electrolytes allow the calculation of the fractional excretion of sodium, which separates a pre-renal from an intrinsic cause, with the fractional excretion of urea preferred when the child is on diuretics. [2]
A renal ultrasound with Doppler is a key investigation that assesses kidney size, hydronephrosis, stones, cysts, and vascular patency. It distinguishes obstruction from intrinsic and pre-renal causes, and it shows the small, echogenic kidneys of chronic disease. Specific cause-directed tests are sent on the basis of the clinical picture: creatine kinase for rhabdomyolysis, urate and phosphate for tumour lysis syndrome, complement C3 and autoimmune markers including antinuclear antibodies and anti-streptolysin O for glomerulonephritis, and a thorough drug history for acute interstitial nephritis. Biomarkers such as neutrophil gelatinase-associated lipocalin add predictive value when combined with the renal angina index, identifying children who will progress to severe AKI before the creatinine has risen. [7]
Management — Resuscitation
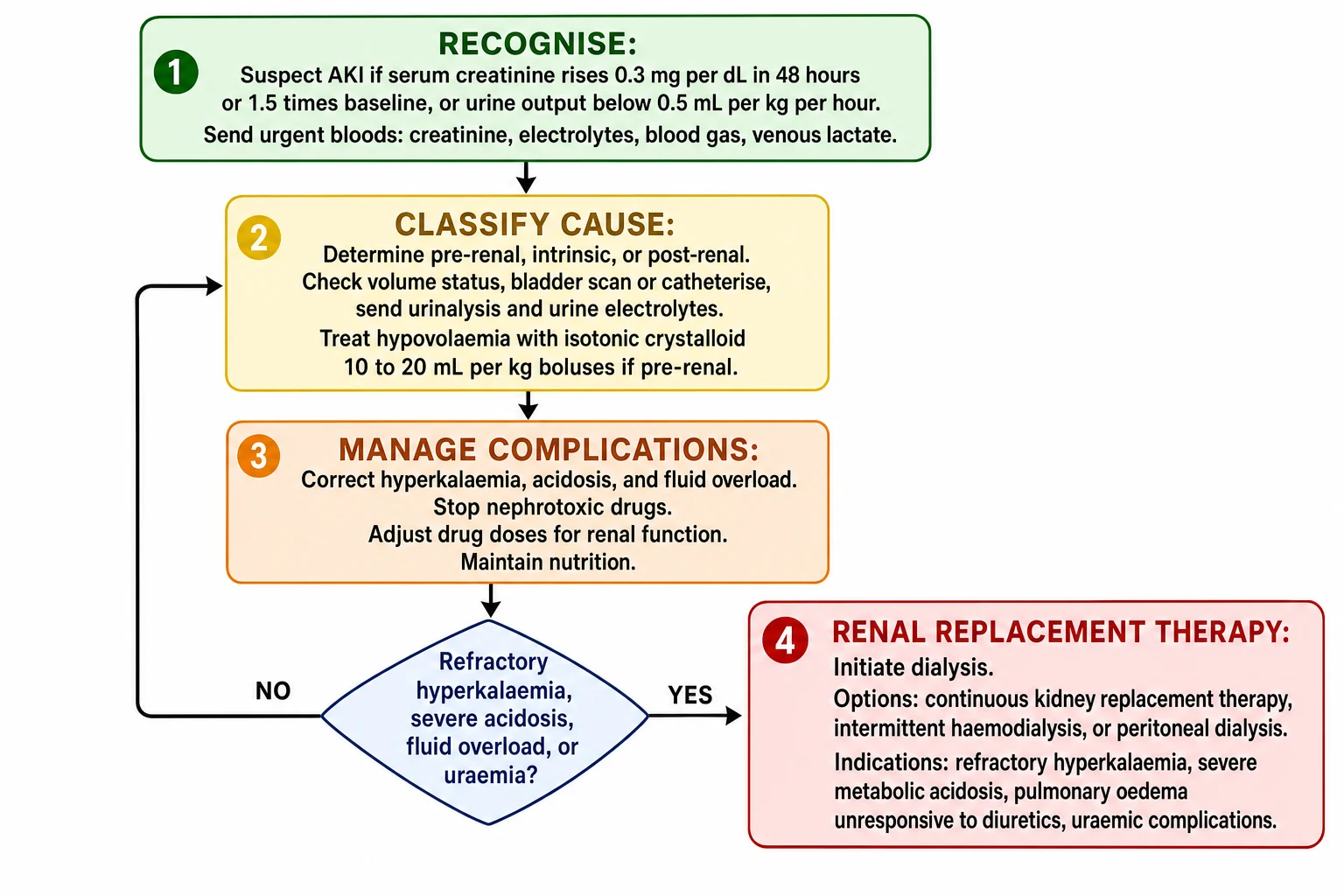
Resuscitation addresses the immediate threats to life and runs in parallel with the diagnostic workup. The airway and breathing are stabilised and intravenous access established. The central decision is the volume status, and it determines the entire resuscitation. A child who is hypovolaemic or in shock receives isotonic crystalloid boluses of 10 to 20 mL per kg with reassessment after each bolus, because restoring perfusion may reverse a pre-renal injury within hours. A child who is fluid overloaded receives fluid restriction and diuretics rather than further boluses, because more fluid will worsen the pulmonary oedema and the outcome. [5]
The choice of resuscitation fluid has been tested directly in children. The PRoMPT BOLUS trial, a large pragmatic randomised trial of over 9000 children with septic shock, found no significant difference in the composite outcome of death, new renal replacement therapy, or persistent kidney dysfunction at 30 days between balanced crystalloids and 0.9 percent saline. Either fluid is therefore acceptable for the initial resuscitation, and the priority is the prompt restoration of perfusion rather than the fluid choice. [10]
Isotonic crystalloid for volume resuscitation in suspected pre-renal AKI
Dose
10 to 20 mL per kg per bolus
Hyperkalaemia is the most immediately lethal complication and is treated as an emergency in a staged approach. The first step is to check a 12-lead ECG, and if there are ECG changes, to give intravenous calcium gluconate to stabilise the myocardial cell membrane. The second step is to shift potassium into the cells with insulin and glucose, a beta-2 agonist such as salbutamol, and sodium bicarbonate in the acidotic child. The third step is to remove potassium from the body with potassium-wearing resins or, in the refractory case, renal replacement therapy. The serum potassium is rechecked after each intervention because the effect is transient. [2]
Calcium gluconate 10 percent for hyperkalaemia with ECG changes
Dose
0.5 mL per kg per dose, up to 20 mL per dose
Metabolic acidosis is treated when it is severe. A pH below 7.1 or a bicarbonate below 12 mmol per litre causes myocardial depression and worsens hyperkalaemia, and may be treated with sodium bicarbonate cautiously, with the risk of volume overload and hypernatraemia weighed against the benefit. Nephrotoxic drugs are stopped, and every drug dose is adjusted to the current estimated GFR, because the standard dose of a renally cleared drug in a child with AKI will accumulate and add to the injury. [2]
Fluid overload is itself a complication and a cause of deterioration. The percentage fluid overload is calculated and tracked, and severe fluid overload causing pulmonary oedema unresponsive to diuretics is an indication for renal replacement therapy. Diuretics such as furosemide are used to achieve euvolaemia, though they improve urine output without changing the renal recovery or the survival. [9]
Management — Definitive & Stepwise
[2]Definitive management is cause-specific where a treatable cause is found, and centred on renal protection and timely renal replacement therapy where the kidney fails to recover. The cause is treated directly: sepsis receives antibiotics and source control, hypovolaemia receives fluids, obstruction receives decompression by catheter or nephrostomy, glomerulonephritis may receive immunosuppression, and tumour lysis syndrome receives rasburicase and hydration. Every nephrotoxic agent is reviewed and stopped where possible, and every drug dose is adjusted to the current estimated GFR. [2]
Fluid management moves through phases as the child recovers or deteriorates. The initial phase is resuscitation for the hypovolaemic child. The middle phase is maintenance, with the fluid tailored to the current output and the insensible losses, and attention to the electrolyte content. The late phase, if the child becomes fluid overloaded or oliguric, is restriction and diuretics to achieve euvolaemia. The percentage fluid overload is tracked because it carries an independent and synergistic effect with AKI on mortality, and severe overload is an indication for renal replacement therapy. [9]
Furosemide for fluid overload in acute kidney injury
Dose
1 to 2 mg per kg per dose, intravenously
Renal replacement therapy is initiated for the complications that cannot be controlled medically. The indications are refractory hyperkalaemia unresponsive to the staged medical therapy, severe metabolic acidosis unresponsive to bicarbonate, fluid overload causing pulmonary oedema unresponsive to diuretics, and uraemic complications such as encephalopathy, pericarditis, and a bleeding diathesis. Selected toxin ingestions are another indication, where dialysis removes the drug. The modality is chosen by the age, the size, the haemodynamic stability, and the centre expertise. [2]
Continuous kidney replacement therapy is preferred for the haemodynamically unstable PICU patient because it provides a slow, steady clearance that does not provoke the blood pressure swings of intermittent dialysis. Intermittent haemodialysis is used for the stable older child and for toxin removal where a rapid clearance is needed. Peritoneal dialysis is used for small infants, for whom vascular access is difficult, and in resource-limited settings where it is simpler and cheaper. The KDIGO summary recommends continuous therapy for haemodynamically unstable patients and notes that the modality does not clearly change survival, so the choice is made on practical grounds. [2]
A paediatric nephrologist is involved early for any child with stage 2 or 3 AKI, for any child with an unclear cause, and for every child who may need renal replacement therapy. Prevention is as important as treatment, and nephrotoxic-medication stewardship programmes reduce the incidence of hospital-acquired AKI by prompting the review and the cessation of unnecessary nephrotoxic agents. [8]
Specific Subtypes & Scenarios
Sepsis-associated AKI is the most common intrinsic AKI in the PICU and combines inflammatory and haemodynamic injury. The systemic inflammation of sepsis produces cytokines that injure the tubular cells directly, and the vasodilation of septic shock reduces the renal perfusion, so the kidney suffers a double insult. These children have a high risk of progression to stage 3 and to multiorgan failure, and they need early and aggressive resuscitation alongside the antibiotic and source-control treatment of the sepsis. [4]
Cardiac surgery-associated AKI following cardiopulmonary bypass peaks within 48 hours and is a leading cause of AKI in infants with congenital heart disease. The injury is driven by the systemic inflammatory response to the bypass circuit, the non-pulsatile flow, and the haemolysis that releases free haemoglobin, and it carries a worse outcome. The renal angina index and the biomarkers are used to stratify the risk early, and the prevention centres on optimising the bypass strategy, avoiding nephrotoxins, and maintaining perfusion. [5]
Nephrotoxic AKI is often non-oliguric and is the most preventable form. Aminoglycosides, non-steroidal anti-inflammatory drugs, ACE inhibitors, contrast media, and chemotherapy each injure the tubule by a distinct mechanism, and the cumulative exposure matters. Moffett and Goldstein showed that increasing nephrotoxic-medication exposure is associated with rising AKI rates even in non-critically ill children, and stewardship programmes that prompt the review and the cessation of these agents reduce the incidence. The clinical implication is that every child with a rising creatinine has their drug chart reviewed and every nephrotoxic agent stopped where possible. [8]
Haemolytic uraemic syndrome is the leading cause of intrinsic AKI in young children and presents with the triad of microangiopathic haemolytic anaemia, thrombocytopenia, and AKI, usually after a diarrhoeal prodrome from Shiga-toxin-producing Escherichia coli. The management is supportive, with careful fluid and electrolyte management and renal replacement therapy for the severe case, because antibiotics and anti-motility agents may worsen the toxin release. Tumour lysis syndrome causes acute uric acid and phosphate crystal nephropathy and is prevented by hydration and rasburicase in high-risk haematological malignancy. Rhabdomyolysis from crush injury, viral myositis, or metabolic disease causes myoglobinuric tubular injury and is treated with aggressive isotonic fluid and an alkaline diuresis. [5]
[5]Complications & Pitfalls
The complications of AKI are the direct causes of death and the targets of intensive monitoring. Hyperkalaemia is the most immediately lethal, causing the ECG changes that progress from peaked T waves through a widened QRS to a sine-wave pattern and asystole, and it is treated as an emergency with calcium, the agents that shift potassium into cells, and dialysis for the refractory case. Fluid overload develops insidiously, and Gist and colleagues showed it carries an independent and synergistic effect with AKI on mortality in critically ill children, worsening the oxygenation, delaying the mechanical ventilation weaning, and impairing the wound healing. [9]
Metabolic acidosis causes myocardial depression and worsens hyperkalaemia, and it is treated with sodium bicarbonate when the pH falls below 7.1. Uraemia causes a bleeding diathesis from platelet dysfunction, a pericardial rub from uraemic pericarditis, and encephalopathy with drowsiness and seizures. Infection is both a cause and a complication, because the uraemic child is relatively immunocompromised and the intensive care interventions create portals for the bacterial and fungal entry. Hyponatraemia from water retention causes seizures, and the correction must be controlled to avoid the osmotic demyelination. [2]
The classic pitfalls are diagnostic and therapeutic. Failing to recognise non-oliguric AKI, because the child is still passing urine, delays the diagnosis and the staging. Treating all oliguria with fluid boluses, without assessing the volume status, worsens the fluid overload in the child who is already overloaded. Failing to stop and to dose-adjust the nephrotoxic drugs adds to the injury. Delaying the renal replacement therapy until the hyperkalaemia has caused a cardiac arrest or the fluid overload has become irreversible is the most dangerous error. And confusing the AKI with chronic kidney disease, because no baseline creatinine was sought, changes the prognostic calculus entirely. [5]
Prognosis & Disposition
The prognosis depends on the cause, the severity at presentation, and the trajectory, and the AWARE study established the modern benchmark for the outcome. AKI independently increases the mortality and the length of stay in critically ill children, with the risk rising steeply through the KDIGO stages and highest for stage 3 and for the children who need renal replacement therapy. Most children with pre-renal AKI recover fully when the cause is treated, and the recovery is within hours. The child with intrinsic AKI from acute tubular necrosis recovers over days to weeks as the tubular cells regenerate, but a proportion are left with chronic kidney disease. [4]
The long-term outcome has shifted the practice. The meta-analysis by Meena and colleagues showed that children who survive an AKI episode have a higher long-term risk of chronic kidney disease, hypertension, and recurrent AKI. This challenges the older belief that paediatric AKI is fully reversible, and it mandates long-term nephrology follow-up after every significant AKI episode, with blood pressure monitoring, serial creatinine, and the avoidance of nephrotoxins. [12]
Disposition is to a paediatric intensive care unit for the stage 2 and 3 AKI, with a paediatric nephrologist involved for the severe or persistent AKI and for every child needing renal replacement therapy. The discharge plan addresses the cause, the medication and monitoring regimen, and the avoidance of nephrotoxins, and it includes nephrology follow-up to confirm the renal recovery and to screen for the long-term complications. The family is counselled on the prognosis honestly, with the emphasis on the likelihood of recovery and the importance of the long-term follow-up. [12]
Special Populations
Neonates are a high-risk group because of their low nephron number, their immature renal function, and their common exposure to perinatal asphyxia, congenital heart disease, and nephrotoxic drugs. The AWAKEN study showed that neonatal AKI is common and often recurrent, and the recurrent neonatal AKI carries a higher risk of mortality and of later chronic kidney disease. The nKDIGO definition uses the age-adjusted creatinine reference values, because the neonatal creatinine in the first days of life reflects the maternal creatinine rather than the neonatal GFR, and the staging must account for this. [11]
Infants after cardiac surgery for congenital heart disease are a particularly high-risk group. The cardiopulmonary bypass provokes a systemic inflammatory response that injures the tubules, and the risk is highest in the youngest infants and those with the most complex surgery. The renal angina index and the biomarkers are used to stratify the risk early, and the prevention centres on the optimisation of the bypass strategy, the avoidance of the nephrotoxins, and the maintenance of the perfusion. [5]
Children with oncological disease and stem-cell transplant recipients face tumour lysis syndrome, the nephrotoxic chemotherapy, and the transplant-related complications. The prevention of tumour lysis syndrome in the high-risk haematological malignancy is with hydration and rasburicase, and the monitoring for the nephrotoxic chemotherapy is with the serial creatinine and the urinalysis. [5]
Children in lower-resource settings present later and have less access to the renal replacement therapy, so the prevention through the hydration, the nephrotoxin stewardship, and the early recognition of the reversible causes carries the greatest yield. Aboriginal and Torres Strait Islander children and other Indigenous populations carry a higher background burden of chronic kidney disease and post-streptococcal glomerulonephritis, so AKI in these children warrants a lower threshold for the nephrology involvement and the long-term follow-up. [5]
[5]Evidence, Guidelines & Regional Differences
The KDIGO 2012 Clinical Practice Guideline for Acute Kidney Injury is the international standard, and its summary by Kellum and Lameire codifies the definition, the staging, the prevention, the pharmacological treatment, and the renal replacement therapy. Part 1 covers the definition, the staging, the risk assessment, the prevention, and the drug therapy, and Part 2 covers the contrast-induced AKI and the renal support. The guideline is applicable to children and adults, with the paediatric nuances captured by the pRIFLE classification and the PODIUM consensus. [1]
The AWARE study by Kaddourah and colleagues is the landmark epidemiological study of paediatric AKI, establishing the 26.9 percent incidence in critically ill children and the independent association with mortality. The ADQI 26 consensus conference report from Sutherland and colleagues provides the current paediatric epidemiology and the research framework, and the PODIUM consensus from Fitzgerald and colleagues standardises the renal dysfunction criteria in the critically ill children. The renal angina index from Basu and colleagues and the fluid-overload outcome data from Gist and colleagues are the high-yield paediatric evidence. [4]
KDIGO Guideline
- 2012: international definition, staging, prevention, renal support
- The current standard, applicable to children and adults
AWARE study
- 2017: 26.9 percent incidence of AKI in critically ill children
- Independent association with mortality and longer stay
pRIFLE
- 2007: paediatric modification of the RIFLE criteria
- Validated for critically ill children
PRoMPT BOLUS
- 2026: no difference between balanced crystalloids and saline
- In children with septic shock
The controversies centre on the role of the diuretics, the timing of the renal replacement therapy, and the choice of the resuscitation fluid. The diuretics improve the urine output without changing the renal recovery or the survival, so they are used for the fluid management rather than for the renal rescue. The optimal timing of the renal replacement therapy is not settled by the randomised trials in children, so the decision is made on the clinical indications. The choice of the resuscitation fluid was tested by the PRoMPT BOLUS trial, which found no difference between the balanced crystalloids and the saline in the children with septic shock, so either is acceptable. The long-term outcome data from the Meena meta-analysis have shifted the practice toward the mandatory nephrology follow-up after the AKI. [10]
Exam Pearls
ABC for the resuscitation priorities in paediatric AKI
References
- [1]Kellum JA, Lameire N, KDIGO AKI Guideline Work Group Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Crit Care, 2013.PMID 23394211
- [2]Lameire N, Kellum JA, KDIGO AKI Guideline Work Group Contrast-induced acute kidney injury and renal support for acute kidney injury: a KDIGO summary (Part 2). Crit Care, 2013.PMID 23394215
- [3]Akcan-Arikan A, Zappitelli M, Loftis LL, Washburn KK, Jefferson LS, Goldstein SL Modified RIFLE criteria in critically ill children with acute kidney injury. Kidney Int, 2007.PMID 17396113
- [4]Kaddourah A, Basu RK, Bagshaw SM, Goldstein SL, AWARE Investigators Epidemiology of Acute Kidney Injury in Critically Ill Children and Young Adults. N Engl J Med, 2017.PMID 27959707
- [5]Sutherland SM, Alobaidi R, Gorga SM, Iyengar A, Morgan C, Ronco C, et al Epidemiology of acute kidney injury in children: a report from the 26th Acute Disease Quality Initiative (ADQI) consensus conference. Pediatr Nephrol, 2024.PMID 37874357
- [6]Fitzgerald JC, Basu RK, Fuhrman DY, Gorga SM, Hassinger AB, Alten JA, et al Renal Dysfunction Criteria in Critically Ill Children: The PODIUM Consensus Conference. Pediatrics, 2022.PMID 34970682
- [7]Basu RK, Zappitelli M, Brunner L, Wang Y, Wong HR, Chawla LS, Goldstein SL Derivation and validation of the renal angina index to improve the prediction of acute kidney injury in critically ill children. Kidney Int, 2014.PMID 24048379
- [8]Moffett BS, Goldstein SL Acute kidney injury and increasing nephrotoxic-medication exposure in noncritically-ill children. Clin J Am Soc Nephrol, 2011.PMID 21212419
- [9]Gist KM, Selewski DT, Brinton J, Menon S, Goldstein SL Assessment of the Independent and Synergistic Effects of Fluid Overload and Acute Kidney Injury on Outcomes of Critically Ill Children. Pediatr Crit Care Med, 2020.PMID 31568240
- [10]Balamuth F, Weiss SL, Long E, Thompson GC, Cruz AT, Nager AL, et al Balanced Fluid or 0.9% Saline in Children Treated for Septic Shock. N Engl J Med, 2026.PMID 42028918
- [11]Rutledge AD, Griffin RL, Vincent K, Askenazi DJ, Segar JL Incidence, Risk Factors, and Outcomes Associated With Recurrent Neonatal Acute Kidney Injury in the AWAKEN Study. JAMA Netw Open, 2024.PMID 38329754
- [12]Meena J, Ali S, Robinson C, Greenberg JH, Kamran D, Kaddourah A, et al Late Outcomes Following Acute Kidney Injury in Children: A Systematic Review and Meta-Analysis. JAMA Pediatr, 2026.PMID 42081220