Paeds · nephrology-urology-fluids-and-electrolytes
Antenatal hydronephrosis and postnatal evaluation
Also known as Antenatal hydronephrosis · Prenatal hydronephrosis · Fetal hydronephrosis · Fetal pelvic dilatation · Society for Fetal Urology grading · Urinary tract dilation classification · Postnatal renal ultrasound timing
Fellowship guide to antenatal hydronephrosis and postnatal evaluation. Covers the definition and the Society for Fetal Urology grading system and the Urinary Tract Dilation classification system, the anteroposterior renal pelvic diameter thresholds at the 28-week gestational cutoff, the critical timing of the first postnatal ultrasound at days 5 to 7 to avoid the false negative of neonatal dehydration, the investigation pathway of ultrasound, MCUG, DMSA, and MAG3, the risk stratification that separates transient physiologic dilatation from obstructive uropathy and reflux, the role of prophylactic antibiotics, and the long-term surveillance for the chronic kidney disease risk that the underlying congenital anomaly carries.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Antenatal hydronephrosis is the dilatation of the renal collecting system detected on antenatal ultrasound, and it is the single most common abnormal finding on the routine mid-trimester anomaly scan. The finding spans a spectrum from the harmless transient dilatation that resolves within weeks of birth to the severe obstructive uropathy that threatens the renal and the respiratory survival of the newborn. The clinical task is not to treat the hydronephrosis itself but to separate the benign from the pathological, because the dilatation is a sign and not a diagnosis, and the underlying congenital anomaly of the kidney and urinary tract is what determines the long-term outcome. [6]
The terminology has been refined over three decades. The original Society for Fetal Urology grading system, introduced by Fernbach and colleagues in 1993, graded the hydronephrosis from grade 0 to grade 4 on the basis of the pelvic and calyceal dilatation and the preservation of the renal parenchyma. The 2014 multidisciplinary consensus led by Nguyen introduced the Urinary Tract Dilation classification, which replaced the ambiguous terms hydronephrosis and pyelectasis with a standardised measure of the anteroposterior renal pelvic diameter and a set of additional sonographic features that together stratify the fetus and the child into a low-risk or an increased-risk category. [1]
The clinical importance of antenatal hydronephrosis lies in its role as the gateway finding for congenital anomalies of the kidney and urinary tract, the group of structural malformations that is the single largest cause of paediatric end-stage kidney disease. Lee and colleagues showed in their meta-analysis that antenatal hydronephrosis predicts a postnatal pathology in a significant proportion of cases, with the risk proportional to the degree of the dilatation, which is why the threshold for the postnatal evaluation is deliberately low. [5]
Classification
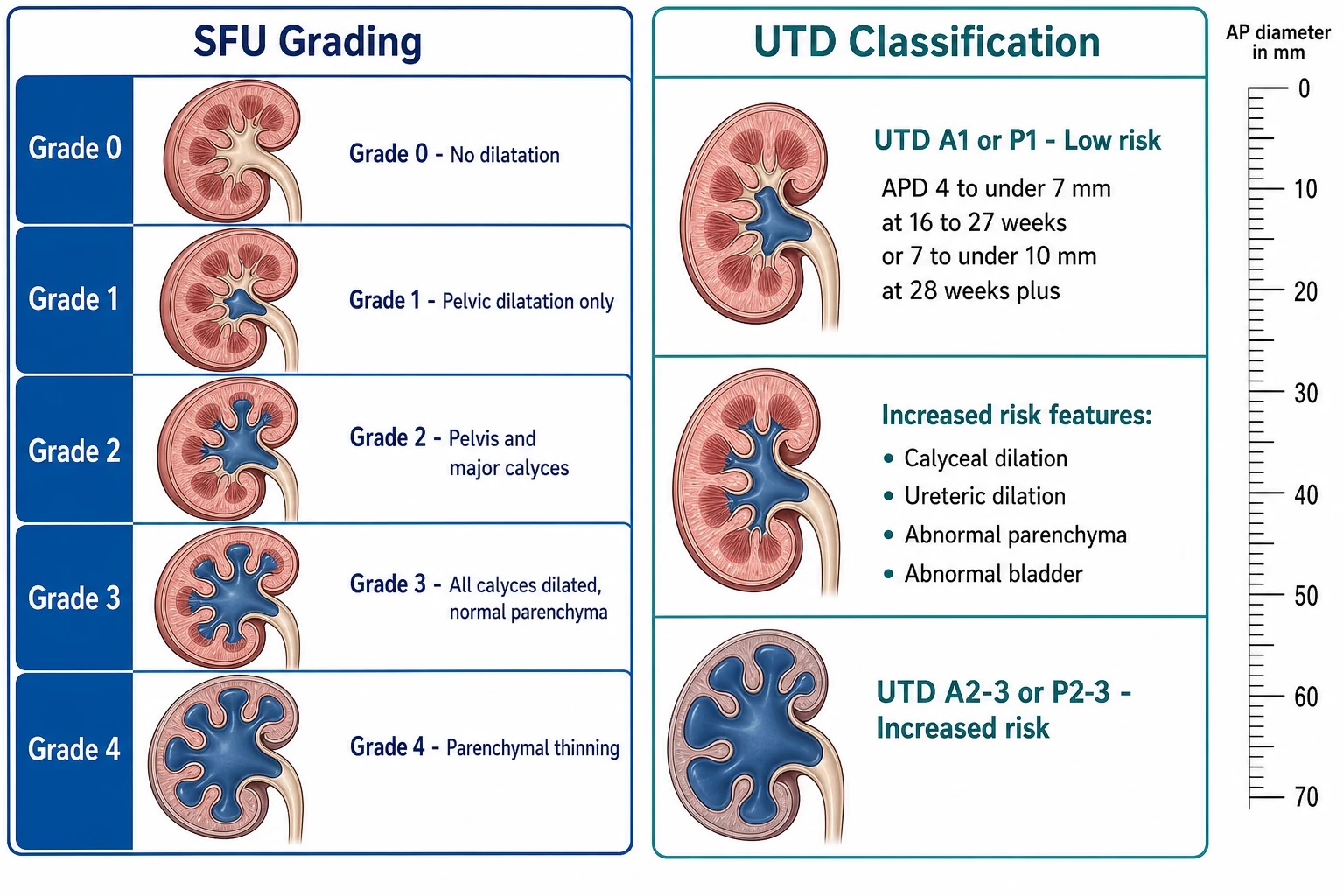
The Society for Fetal Urology grading system, introduced by Fernbach, Maizels, and Conway in 1993, was the first standardised method for grading hydronephrosis on ultrasound, and it remains the most widely taught system in paediatric examinations. The system uses five grades. Grade 0 is a normal kidney with no dilatation. Grade 1 shows dilatation of the renal pelvis only, with no calyceal involvement. Grade 2 shows dilatation of the renal pelvis and the major calyces, with normal renal parenchyma. Grade 3 shows dilatation of the renal pelvis, the major calyces, and the minor calyces, with the renal parenchyma still normal in thickness. Grade 4 shows the same dilatation as grade 3 but with thinning of the renal parenchyma, which signals a chronic or severe obstruction. [3]
The Urinary Tract Dilation classification system was introduced in the 2014 multidisciplinary consensus led by Nguyen, and it superseded the older system in the academic and the guideline literature because it incorporated the quantitative anteroposterior renal pelvic diameter alongside a set of additional sonographic features. The antenatal system uses the prefix A and divides cases into a low-risk category, UTD A1, and an increased-risk category, UTD A2 to A3, with a gestational age cutoff at 28 weeks. The increased-risk category is assigned either by the diameter threshold or by the presence of any of the additional features regardless of the diameter. [1]
The additional sonographic features that upgrade a case to the increased-risk category, regardless of the anteroposterior diameter, are the central or peripheral calyceal dilatation, the abnormal renal parenchyma shown by increased echogenicity or thinning or cortical cysts, the dilatation of the ureter, the abnormal bladder shown by a thickened wall or enlargement, and the unexplained oligohydramnios. These features matter because they indicate a structural anomaly or a chronic obstruction rather than a transient physiologic dilatation, and their presence lowers the threshold for the postnatal investigation. [9]
The postnatal system uses the prefix P and applies the same principle of a low-risk category, UTD P1, and an increased-risk category, UTD P2 to P3. The postnatal system cannot be directly interchanged with the antenatal system, because the kidney is larger and produces more urine after birth, and the postnatal anteroposterior diameter threshold for significance is correspondingly higher. The postnatal increased-risk features are the peripheral calyceal dilatation, the ureteral dilatation, and the abnormal parenchyma shown by increased echogenicity or thinning or cysts, and their presence warrants the further investigation with the MCUG and the functional scans. [8]
SFU grading
- Grades 0 to 4 based on pelvis, calyces, and parenchyma
- Grade 4 defined by parenchymal thinning
- Qualitative and operator-dependent
- Introduced by Fernbach in 1993, still the most taught system
UTD classification
- Quantitative anteroposterior renal pelvic diameter
- 28-week gestational age cutoff for antenatal
- Additional features upgrade to increased risk
- 2014 multidisciplinary consensus, the modern standard
Postnatal UTD
- Prefix P, distinct from the antenatal prefix A
- Higher diameter threshold than antenatal
- P1 low risk versus P2-3 increased risk
- Increased-risk features trigger MCUG and functional scans
Epidemiology & Risk Factors
Antenatal hydronephrosis is the most common abnormality detected on the routine antenatal ultrasound, with a reported incidence of 1 to 5 percent of all pregnancies when any degree of renal pelvic dilatation is included. The widespread use of the routine 18 to 20 week anomaly scan means that the finding is now identified before birth in the great majority of cases, which has shifted the clinical encounter from the acute presentation of a sick neonate to the planned postnatal evaluation of a well-appearing newborn. Liu and colleagues emphasised that the high detection rate has made the postnatal evaluation pathway one of the most common reasons for a paediatric nephrology and urology referral in infancy. [6]
The most reassuring epidemiological fact is that the majority of cases of antenatal hydronephrosis are transient and physiologic, and they resolve spontaneously in the first months of life without any intervention. The meta-analysis by Lee and colleagues showed that the risk of a postnatal pathology is proportional to the degree of the antenatal dilatation, with the mild dilatation resolving in most cases and the severe dilatation carrying a high risk of an obstruction, a reflux, or another congenital anomaly. Nakane and colleagues showed that the antenatal grade 1 and grade 2 hydronephrosis resolves in the majority of cases, and they defined the appropriate timing for the follow-up ultrasound and the criteria for the safe termination of the surveillance. [12]
The risk factors for a pathological outcome are the severity and the bilaterality of the dilatation, the presence of the additional sonographic features, the progression of the anteroposterior diameter across the serial antenatal scans, and the male sex in the context of a dilated bladder. The bilateral severe hydronephrosis with the oligohydramnios is the highest-risk finding, because it signals a lower urinary tract obstruction such as the posterior urethral valves and the risk of the Potter sequence with the pulmonary hypoplasia. A family history of a congenital anomaly of the kidney and urinary tract, the maternal diabetes, and the syndromic features all increase the probability of a pathological finding. [6]
Aboriginal and Torres Strait Islander children and children from the lower-resource settings carry a higher background burden of the chronic kidney disease, which compounds the long-term risk of any confirmed anomaly. The emphasis in these populations is on the early detection through the routine antenatal ultrasound and the prompt postnatal evaluation of any finding, because the late presentation with an advanced chronic kidney disease is more common when the antenatal detection is missed. [11]
Pathophysiology
The pathophysiology of antenatal hydronephrosis divides into three mechanisms, and the distinction drives the postnatal evaluation. The first mechanism is the transient physiologic dilatation, which is the most common and the most benign. The fetal renal pelvis dilates because of the high fetal urine output and the relative compliance of the immature collecting system, and the dilatation resolves after birth as the renal physiology matures and the urine output normalises. There is no structural anomaly, no obstruction, and no reflux, and the long-term renal function is normal. [12]
The second mechanism is the obstruction, in which a structural blockage impedes the flow of the urine and raises the pressure in the collecting system upstream. The ureteropelvic junction obstruction, from a congenital narrowing at the junction of the renal pelvis and the ureter, is the most common cause of a true obstruction and the most common pathological finding in the postnatal evaluation of antenatal hydronephrosis. The posterior urethral valves, the membrane-like folds in the male posterior urethra, cause the lower urinary tract obstruction and the most severe phenotype, with the back-pressure dilating the bladder and the upper tracts and damaging the developing kidneys in utero. [6]
The third mechanism is the vesicoureteral reflux, in which the urine flows retrograde from the bladder into the ureter because of a short or absent intramural tunnel. The reflux dilates the renal pelvis during the voiding and may be intermittent, which explains why the antenatal hydronephrosis from the reflux can vary across the serial scans. The reflux carries the risk of the recurrent urinary tract infection and the renal scarring, and it is the second most common pathological finding in the postnatal evaluation. The multicystic dysplastic kidney and the duplex collecting system are the less common but important causes, and each has a distinctive ultrasound appearance. [6]
Clinical Presentation
The presentation of antenatal hydronephrosis is, by definition, the antenatal ultrasound finding, and the clinical encounter is the planned postnatal evaluation of the well newborn. The severity and the laterality of the antenatal finding, the presence of the additional sonographic features, and the progression across the serial scans together determine the urgency and the intensity of the postnatal evaluation. The minority of cases that are not detected antenatally present after birth with a palpable abdominal mass, a febrile urinary tract infection in infancy, or, later, with a hypertension or a failure to thrive. [2]
The antenatal finding is graded and stratified at the time of the scan. The low-risk category, UTD A1, is an isolated renal pelvic dilatation within the threshold for the gestational age, and it is the most common finding. The increased-risk category, UTD A2 to A3, is either a larger dilatation or the presence of any of the additional features, and it carries a higher probability of a postnatal pathology. The bilateral severe hydronephrosis with the oligohydramnios and the dilated bladder is the highest-risk finding, and it raises the immediate concern for the posterior urethral valves and the Potter sequence. [1]
The modes of presentation across the timeline
Antenatal hydronephrosis on the 18 to 20 week anomaly scan, the most common mode
Serial antenatal scans showing the progression or the resolution of the dilatation
The well newborn in the postnatal evaluation clinic at days 5 to 7
The male neonate with the palpable bladder and the poor stream from the posterior urethral valves
The infant with the febrile urinary tract infection from the reflux or the obstruction
The older child with the hypertension or the incidental finding on imaging
The clinical presentation is shaped by the underlying anomaly. The ureteropelvic junction obstruction presents as a unilateral hydronephrosis that persists or worsens across the serial scans. The vesicoureteral reflux may present as a fluctuating hydronephrosis or as a febrile urinary tract infection in infancy. The posterior urethral valves present in the male neonate with the bilateral hydronephrosis, the dilated thick-walled bladder, the palpable bladder, and the poor urinary stream, and the severe cases present at birth with the respiratory distress from the pulmonary hypoplasia. The multicystic dysplastic kidney presents as a multicystic renal mass with the characteristic non-communicating cysts. [6]
Differential Diagnosis
The first distinction in the differential is between the transient physiologic dilatation and the pathological hydronephrosis, because the management and the prognosis diverge completely. The transient dilatation is the most common finding, and it resolves spontaneously in the first months of life. The pathological hydronephrosis is caused by an obstruction, a reflux, or another congenital anomaly, and it requires the structured postnatal evaluation. Lee and colleagues showed in their meta-analysis that even the mild antenatal hydronephrosis carries a risk of a postnatal pathology, so the clinician cannot assume the transient nature without the postnatal evaluation. [5]
The second distinction is between the causes of a true obstruction. The ureteropelvic junction obstruction is the most common, and it shows a unilateral hydronephrosis with a dilated renal pelvis and the normal-calibre ureter. The posterior urethral valves cause the lower urinary tract obstruction in the male, and they show the bilateral hydronephrosis with the dilated thick-walled bladder and the dilated posterior urethra. The ureterocele and the ectopic ureter in a duplex system cause a focal obstruction, and the neurogenic bladder from a spinal cord lesion causes a functional obstruction. [6]
Transient physiologic
- The most common and benign cause
- Resolves spontaneously in the first months
- No structural anomaly or obstruction
- Confirmed by the resolution on the postnatal ultrasound
Ureteropelvic junction obstruction
- The most common pathological cause
- Unilateral hydronephrosis with a normal ureter
- Confirmed by the MAG3 renogram
- Managed by surveillance or pyeloplasty
Vesicoureteral reflux
- Retrograde urine flow from a short intramural tunnel
- May be fluctuating on the serial scans
- Detected by the MCUG
- Risk of recurrent infection and renal scarring
Posterior urethral valves
- Male lower urinary tract obstruction
- Bilateral hydronephrosis with a dilated bladder
- High risk of chronic kidney disease
- Requires immediate catheterisation and valve ablation
The third distinction is between the hydronephrosis and the other cystic renal masses. The multicystic dysplastic kidney shows the non-communicating cysts of varying size, the grape-cluster appearance, which distinguishes it from the hydronephrosis in which the cystic spaces communicate with the renal pelvis. The autosomal recessive polycystic kidney disease presents with the bilateral enlarged echogenic kidneys, and the autosomal dominant polycystic kidney disease shows the bilateral renal cysts in a child with an affected parent. A dysmorphic child with the renal anomaly warrants the genetics evaluation for a syndromic association. [6]
Clinical & Bedside Assessment
The bedside assessment of the newborn with the antenatal hydronephrosis answers three questions: is the child in the immediate danger, what is the structural anomaly, and what is the renal function. The airway, the breathing, and the circulation are assessed first, because the neonate with the severe bilateral hydronephrosis from the posterior urethral valves may present with the respiratory distress from the pulmonary hypoplasia. The abdomen is examined for the palpable mass, which may be the distended bladder of the posterior urethral valves, a hydronephrotic kidney, or the multicystic dysplastic kidney. [2]
The blood pressure is measured in every newborn with the antenatal hydronephrosis, because the hypertension is both a complication of the underlying anomaly and a sign of the renal dysplasia. The growth parameters are plotted, because the failure to thrive is a feature of the chronic kidney disease from the bilateral dysplasia or the obstructive uropathy. The external genitalia are examined, because the posterior urethral valves occur only in males and the syndromic anomalies may have the genital findings. The spine is examined for the stigmata of the occult spinal dysraphism, because the neurogenic bladder from the tethered cord is a treatable cause of the upper tract damage. [6]
The history should include the antenatal findings in detail, because the severity, the laterality, the additional features, and the progression across the serial scans guide the urgency of the postnatal evaluation. A family history of the congenital anomaly of the kidney and urinary tract, the kidney disease, the hearing loss, or the diabetes raises the possibility of the monogenic or the syndromic cause. The maternal history of the diabetes, the drug exposure, or the oligohydramnios provides the additional context. [2]
Investigations
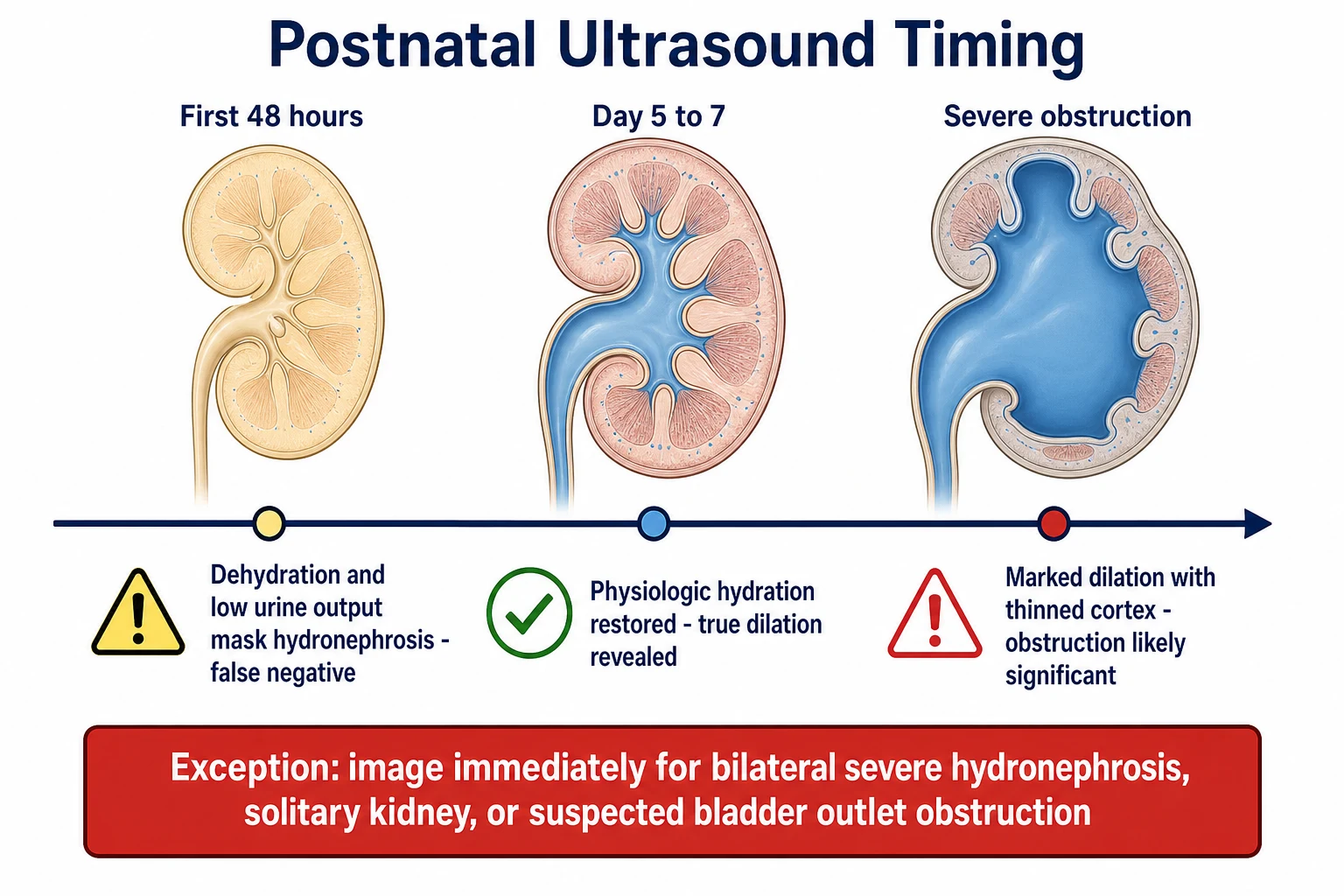
The investigation pathway for the antenatal hydronephrosis is sequential and image-led, with each test answering a specific question, and the timing of the first test is the single most testable point. The first test is always the postnatal renal ultrasound, and it is deferred to at least 48 hours and ideally to days 5 to 7 of life. Wiener and O'Hara established that the neonatal dehydration and the oliguria in the first 48 hours reduce the urine output and underestimate the renal pelvic dilatation, which produces the false negative and the missed diagnosis. [4]
The exception to the deferred timing is the clinical picture that demands the immediate imaging. The bilateral severe hydronephrosis, the solitary kidney, and the suspected bladder outlet obstruction from the posterior urethral valves are the indications for the immediate postnatal ultrasound, because the delay in the diagnosis and the decompression worsens the renal dysplasia and the long-term outcome. In these high-risk cases, the ultrasound is performed in the first hours of life, the urethral catheter is passed if the obstruction is confirmed, and the urgent urology referral is made. [4]
The micturating cystourethrogram, or MCUG, is the gold standard for the detection of the vesicoureteral reflux and the posterior urethral valves. It involves the catheterisation of the bladder, the filling with the contrast, and the imaging during the voiding, and it shows the reflux grade from 1 to 5 and the dilated posterior urethra of the valves. The MCUG is invasive and carries the risk of the urinary tract infection, so it is reserved for the children with the high pre-test probability of the reflux or the obstruction, and the prophylactic antibiotics are given around the procedure. The Swiss consensus by Bahadori and colleagues provided the practical thresholds for the referral and the selection of the children who warrant the MCUG. [11]
The DMSA scan, or the dimercaptosuccinic acid scintigraphy, is the static cortical scan that maps the functioning renal cortex and detects the scars, the dysplasia, and the split renal function. It is performed months after any acute infection to avoid the confusion with the acute pyelonephritis, and it is essential for the long-term surveillance. The MAG3 renogram, or the mercaptoacetyltriglycine scan, is the dynamic scan that shows the uptake, the drainage, and the split function of each kidney, and it is the definitive test for the ureteropelvic junction obstruction. Hodhod and colleagues showed that the postnatal Urinary Tract Dilation classification improves the accuracy of the grading and the selection of the children who need the functional scans. [8]
Blood tests assess the renal function and the complications. The serum creatinine and the estimated glomerular filtration rate are the baseline markers, though the neonatal creatinine reflects the maternal creatinine for the first days of life and must be interpreted with the care. The electrolytes, the acid-base balance, and the full blood count screen for the chronic kidney disease and the infection. The urinalysis and the urine culture are essential in any febrile child, because the urinary tract infection may be the first sign of the underlying anomaly. [6]
Management — Resuscitation
The resuscitation priorities in the newborn with the antenatal hydronephrosis are to secure the airway in the child with the pulmonary hypoplasia, to decompress any obstruction, and to prevent the infection. The neonate with the posterior urethral valves and the respiratory distress from the Potter sequence needs the immediate respiratory support, and the obstruction is decompressed with the urethral catheter as soon as the airway is stable. The catheter is the first therapeutic intervention in any obstructive uropathy, because the relief of the back-pressure improves the renal perfusion and the renal function. [2]
The newborn with the bilateral renal dysplasia or the severe obstructive uropathy may present with the metabolic acidosis, the hyperkalaemia, or the fluid overload from the renal failure. These biochemical disturbances are managed with the standard neonatal acute kidney injury protocols: the correction of the hyperkalaemia, the management of the acidosis, and the fluid restriction if the child is overloaded. The nephrology team is involved early for the child with the significant renal impairment, and the renal replacement therapy pathway is established if the disturbance is severe. [6]
Prophylactic antibiotic for the high-risk antenatal hydronephrosis
Dose
Trimethoprim 2 mg per kg at night
Prophylactic antibiotics are started at the diagnosis for any newborn with the increased-risk category or the high probability of the reflux or the obstruction, to prevent the urinary tract infection and the renal scarring while the definitive investigations are completed. The agent of the first choice is the trimethoprim at 2 mg per kg at night, or the nitrofurantoin or the cephalexin in the neonate. The antibiotics are continued until the MCUG confirms or excludes the reflux and the obstruction, and they are maintained long-term in the child with the high-grade reflux until the spontaneous resolution or the surgical correction. [2]
Management — Definitive & Stepwise
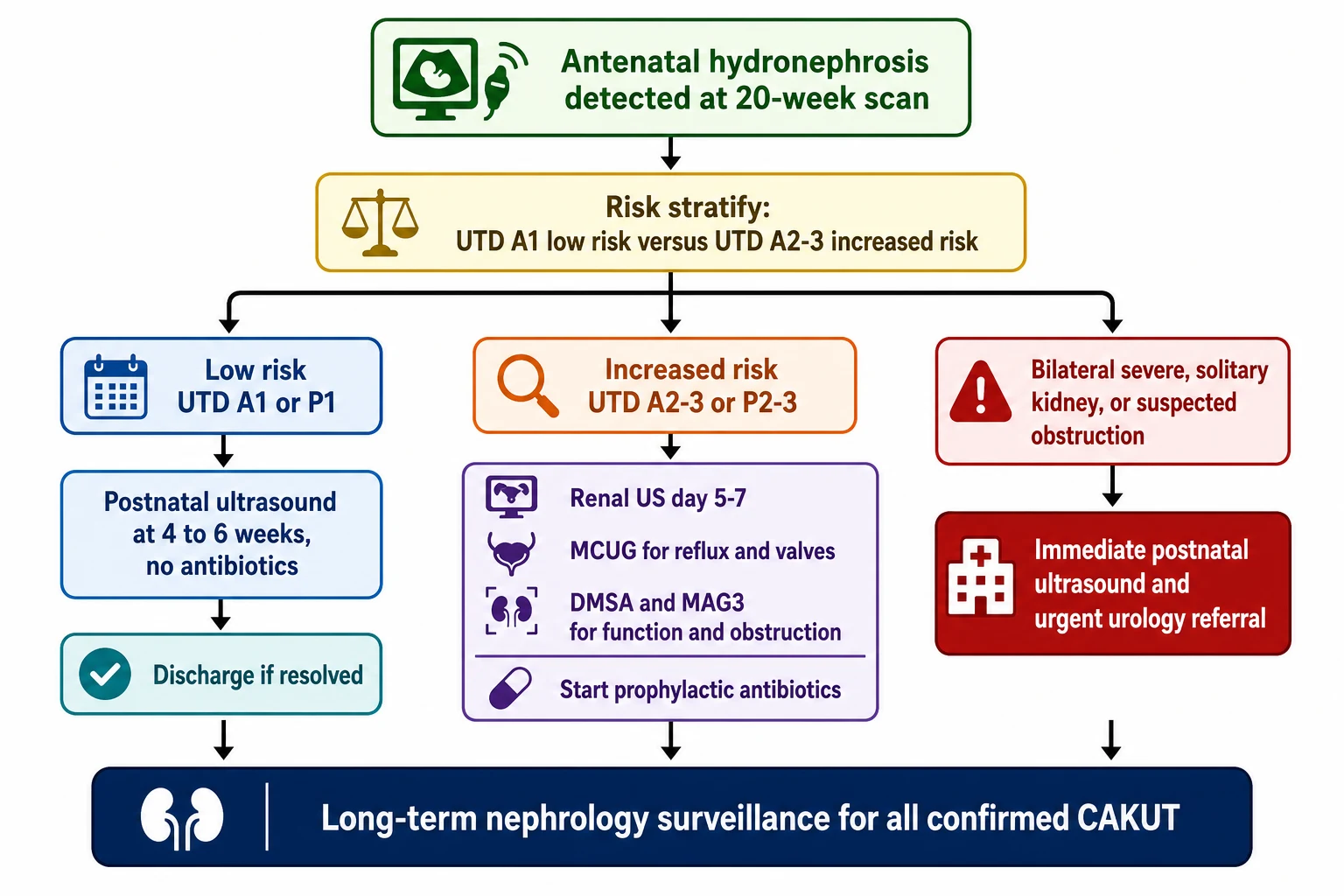
[6]The definitive management is determined by the risk category, the specific anomaly, and the renal function, and the overarching principles are to relieve any obstruction, to prevent the infection, to preserve the renal function, and to monitor for the long-term complications. The Society for Fetal Urology consensus statement by Nguyen and colleagues established the framework that stratifies the postnatal evaluation by the risk category, with the low-risk findings observed and the increased-risk findings investigated. [2]
The low-risk category, the UTD A1 on the antenatal scan and the UTD P1 on the postnatal scan, is managed conservatively. The first postnatal ultrasound is performed at 4 to 6 weeks of age, and no prophylactic antibiotics are given unless the clinical picture changes. If the postnatal ultrasound shows the resolution or the stable mild dilatation, the child is monitored with the serial ultrasounds and discharged when the dilatation resolves. The low-risk pathway applies to the great majority of the cases, because the transient physiologic dilatation is the most common finding. [2]
The increased-risk category, the UTD A2 to A3 on the antenatal scan or the UTD P2 to P3 on the postnatal scan, undergoes the full investigation. The postnatal ultrasound is performed at days 5 to 7, the prophylactic antibiotics are started, and the MCUG and the functional scans are arranged. Melo and colleagues showed that the postnatal Urinary Tract Dilation classification improves the accuracy of the prediction of the kidney injury, which supports the use of the increased-risk features as the trigger for the further investigation. [10]
The severe category, the bilateral severe hydronephrosis with the oligohydramnios or the suspected bladder outlet obstruction, is managed as the emergency. The immediate postnatal ultrasound is performed, the urethral catheter is passed if the obstruction is confirmed, and the urgent urology and nephrology referral is made. The posterior urethral valves are managed by the endoscopic valve ablation once the newborn is stable, and the long-term management focuses on the bladder function and the renal surveillance. The 2021 update by Nguyen and colleagues clarified the common points of confusion in the application of the classification and provided the practical suggestions for the management. [9]
Specific Subtypes & Scenarios
The ureteropelvic junction obstruction is the most common pathological finding in the postnatal evaluation of the antenatal hydronephrosis, and it accounts for the largest proportion of the cases that require the surgical intervention. It presents as the unilateral hydronephrosis with the dilated renal pelvis and the normal-calibre ureter, and it is confirmed by the MAG3 renogram, which shows the impaired drainage and the split renal function. The management is the conservative surveillance if the function is preserved and the pyeloplasty if the function declines or the obstruction is severe. [6]
The vesicoureteral reflux is the second most common pathological finding. It may present as the fluctuating hydronephrosis on the serial antenatal scans, and it is detected by the MCUG in the postnatal evaluation. The low-grade reflux resolves spontaneously in the majority of the children and is managed with the prophylactic antibiotics and the surveillance. The high-grade reflux, the recurrent febrile infection despite the prophylaxis, or the progressive renal scarring may warrant the endoscopic correction or the ureteric reimplantation. [6]
TUMS for the pathological causes of antenatal hydronephrosis
The posterior urethral valves are the most severe and the most testable cause of the antenatal hydronephrosis. They occur only in males, with the incidence of approximately 1 in 4000 to 8000 live male births, and they present with the bilateral hydronephrosis, the dilated thick-walled bladder, the palpable bladder, and the poor urinary stream. The severe cases present at birth with the Potter sequence and the pulmonary hypoplasia, and the mild cases present in infancy with the recurrent infection or the poor growth. The immediate management is the urethral catheterisation and the endoscopic valve ablation, and the long-term management focuses on the bladder function and the chronic kidney disease surveillance. [6]
The multicystic dysplastic kidney presents as the multicystic renal mass with the non-communicating cysts of varying size, the grape-cluster appearance, which distinguishes it from the hydronephrosis. It is managed conservatively in the great majority of the cases, because it involutes over the years and the risk of the hypertension and the malignancy is low. The duplex collecting system is common and may present with the ectopic ureter, the ureterocele, or the reflux to the lower moiety, and the Weigert-Meyer rule places the upper-pole ureter ectopically and distally. [6]
[11]Complications & Pitfalls
The complications of the antenatal hydronephrosis are the complications of the underlying congenital anomaly, and they unfold over the years to the decades. The chronic kidney disease is the most significant, and the trajectory is determined by the initial nephron endowment, the degree of the ongoing injury from the infection and the obstruction, and the hyperfiltration injury in the remaining nephrons. The child with the posterior urethral valves or the bilateral dysplasia carries the highest risk, and the life-long nephrology surveillance is essential. [6]
The recurrent urinary tract infection is the second key complication, because it causes the renal scarring that compounds the existing dysplasia and accelerates the chronic kidney disease progression. The prophylactic antibiotics and the prompt treatment of any confirmed infection are the rationale for the prevention. The hypertension is common and may arise from the dysplastic kidney, the hyperfiltration injury, or the volume overload, and it is often asymptomatic and detected only by the routine blood pressure monitoring. [6]
The classic pitfalls are the diagnostic and the prognostic errors. The first pitfall is the failure to defer the first postnatal ultrasound to at least 48 hours, which produces the false negative and the missed diagnosis. The second pitfall is the failure to investigate the increased-risk finding, on the assumption that the dilatation will resolve, which delays the diagnosis of the obstruction or the reflux and allows the preventable renal scarring. The third pitfall is the failure to recognise the male neonate with the palpable bladder and the poor stream as the posterior urethral valves, which delays the decompression and worsens the renal dysplasia. The fourth pitfall is the underestimation of the long-term chronic kidney disease risk in the child with the unilateral anomaly. [4]
Prognosis & Disposition
The prognosis depends on the risk category, the specific anomaly, the bilaterality, and the renal function at the presentation. The child with the transient physiologic dilatation has the excellent prognosis, with the resolution in the first months and the normal long-term renal function. The child with the unilateral ureteropelvic junction obstruction and the preserved function has the good prognosis, with the surveillance or the pyeloplasty as indicated. The child with the bilateral dysplasia or the posterior urethral valves has the guarded prognosis, with the substantial risk of the progressive chronic kidney disease. [6]
Braga and colleagues compared the Society for Fetal Urology classification and the Urinary Tract Dilation grading system for the prognostication in the prenatal hydronephrosis, and they found that both systems predicted the time to the resolution, with the Urinary Tract Dilation system offering the additional quantitative precision. The prognostic value of the grading reinforces the importance of the accurate classification at the time of the scan, because the category guides the intensity of the postnatal evaluation and the counselling of the family. [7]
The disposition is to the paediatric nephrology and urology service for every child with the increased-risk finding or the confirmed anomaly, with the intensity of the follow-up tailored to the specific condition and the renal function. The child with the resolved transient hydronephrosis may be discharged, but the child with the unilateral dysplastic kidney, the solitary functioning kidney, or the posterior urethral valves needs the life-long surveillance. The transition to the adult nephrology care is planned in the adolescence, because the chronic kidney disease risk persists into the adulthood. [6]
Special Populations
The fetus with the antenatal diagnosis is the fastest-growing special population, because the near-universal antenatal ultrasound has shifted the encounter to before the birth. The antenatal team involves the maternal-fetal medicine specialist, the paediatric nephrologist, and the paediatric urologist in the counselling of the family, and the severity of the finding guides the plan for the place and the mode of the delivery. The most severe cases, such as the bilateral severe hydronephrosis with the oligohydramnios, may be managed with the palliative care or the fetal intervention in the selected centres. [2]
The child with the solitary functioning kidney is a special population because the single kidney carries the entire renal burden. The antenatal hydronephrosis in a fetus with the solitary kidney is the indication for the immediate postnatal imaging, because there is no renal reserve and the obstruction must be excluded at the birth. The child with the solitary functioning kidney needs the life-long surveillance for the hyperfiltration injury, the hypertension, and the proteinuria. [6]
Aboriginal and Torres Strait Islander children and the children from the lower-resource settings present the different challenge. The higher background burden of the chronic kidney disease and the reduced access to the antenatal ultrasound and the specialist services compound the risk, and the late presentation with the advanced chronic kidney disease is more common. The emphasis is on the early detection through the routine antenatal ultrasound, the prompt postnatal evaluation, and the culturally appropriate counselling and surveillance. [11]
The young adult transitioning from the paediatric to the adult care is the final special population. The congenital anomaly does not resolve, and the chronic kidney disease risk persists and may accelerate in the adulthood. The transition plan addresses the blood pressure monitoring, the renal function surveillance, the reproductive and the genetic counselling, and the coordination between the paediatric and the adult nephrology services. [6]
Evidence, Guidelines & Regional Differences
The evidence base for the antenatal hydronephrosis spans the grading systems, the timing of the postnatal ultrasound, the risk stratification, and the long-term outcomes. The 2014 multidisciplinary consensus by Nguyen and colleagues established the Urinary Tract Dilation classification system, which standardised the measurement and the reporting of the urinary tract dilatation across the prenatal and the postnatal periods. The 2021 update by Nguyen and colleagues provided the clarifications, the review of the literature, and the practical suggestions that refined the application of the system. [9]
The original Society for Fetal Urology grading system, introduced by Fernbach and colleagues in 1993, was the first standardised method and remains the most widely taught system. The meta-analysis by Lee and colleagues established the risk stratification that the postnatal pathology risk is proportional to the degree of the antenatal dilatation. The study by Wiener and O'Hara established the rationale for the deferred timing of the first postnatal ultrasound, which is the single most testable point in the topic. [3]
Nguyen 2014
- Journal of Pediatric Urology multidisciplinary consensus
- The Urinary Tract Dilation classification system
- 28-week gestational cutoff and the additional features
Nguyen 2022 update
- Pediatric Radiology 2021 update
- Clarifications and practical suggestions
- Review of the clinical validation
Lee 2006
- Pediatrics meta-analysis on antenatal hydronephrosis
- Risk proportional to the degree of dilatation
Wiener 2002
- Journal of Urology on the postnatal ultrasound timing
- Defer to at least 48 hours, ideally days 5 to 7
Braga 2018
- Journal of Urology comparison of the SFU and UTD systems
- Both predict the time to resolution
The validation studies have strengthened the system. Hodhod and colleagues showed that the Urinary Tract Dilation classification improves the accuracy of the grading of the postnatal hydronephrosis. Melo and colleagues showed that the postnatal classification improves the accuracy of the prediction of the kidney injury. Braga and colleagues compared the Society for Fetal Urology and the Urinary Tract Dilation systems and found that both predicted the time to the resolution. The Swiss consensus by Bahadori and colleagues provided the practical approach and the thresholds for the referral. [8]
The regional differences centre on the access to the antenatal ultrasound and the specialist care. In the high-income settings, the near-universal antenatal detection and the standardised postnatal pathway allow the early intervention and the long-term surveillance. In the lower-resource settings, the later presentation with the advanced chronic kidney disease or the severe infection is more common, and the emphasis shifts to the prevention and the prompt treatment. The international guidelines, including the Society for Fetal Urology consensus and the Swiss consensus, are applicable across the settings, with the intensity of the evaluation tailored to the local resources. [11]
Exam Pearls
ABCDE for the postnatal evaluation of the antenatal hydronephrosis
References
- [1]Nguyen HT, Benson CB, Bromley B, et al Multidisciplinary consensus on the classification of prenatal and postnatal urinary tract dilation (UTD classification system). J Pediatr Urol, 2014.PMID 25435247
- [2]Nguyen HT, Herndon CD, Cooper C, et al The Society for Fetal Urology consensus statement on the evaluation and management of antenatal hydronephrosis. J Pediatr Urol, 2010.PMID 20399145
- [3]Fernbach SK, Maizels M, Conway JJ Ultrasound grading of hydronephrosis: introduction to the system used by the Society for Fetal Urology. Pediatr Radiol, 1993.PMID 8255658
- [4]Wiener JS, O'Hara SM Optimal timing of initial postnatal ultrasonography in newborns with prenatal hydronephrosis. J Urol, 2002.PMID 12352369
- [5]Lee RS, Cendron M, Kinnamon DD, et al Antenatal hydronephrosis as a predictor of postnatal outcome: a meta-analysis. Pediatrics, 2006.PMID 16882811
- [6]Liu DB, Armstrong WR 3rd, Maizels M Hydronephrosis: prenatal and postnatal evaluation and management. Clin Perinatol, 2014.PMID 25155734
- [7]Braga LH, McGrath M, Farrokhyar F, et al Society for Fetal Urology Classification vs Urinary Tract Dilation Grading System for Prognostication in Prenatal Hydronephrosis: A Time to Resolution Analysis. J Urol, 2018.PMID 29198999
- [8]Hodhod A, Capolicchio JP, Jednak R, et al Evaluation of Urinary Tract Dilation Classification System for Grading Postnatal Hydronephrosis. J Urol, 2016.PMID 26527513
- [9]Nguyen HT, Phelps A, Coley B, et al 2021 update on the urinary tract dilation (UTD) classification system: clarifications, review of the literature, and practical suggestions. Pediatr Radiol, 2022.PMID 34981177
- [10]Melo FF, Vasconcelos MA, Mak RH, et al Postnatal urinary tract dilatation classification: improvement of the accuracy in predicting kidney injury. Pediatr Nephrol, 2022.PMID 34453601
- [11]Bahadori A, Wilhelm-Bals A, Caccia J, et al Swiss Consensus on Prenatal and Early Postnatal Urinary Tract Dilation: Practical Approach and When to Refer. Children (Basel), 2024.PMID 39767990
- [12]Nakane A, Mizuno K, Kato T, et al Appropriate timing of performing abdominal ultrasonography and termination of follow-up observation for antenatal grade 1 or 2 hydronephrosis. BMC Urol, 2020.PMID 33143721