Paeds · nephrology-urology-fluids-and-electrolytes
Chronic kidney disease and progression
Also known as CKD · Chronic renal failure · Chronic renal insufficiency · Kidney failure progression · CKD-MBD
Fellowship guide to chronic kidney disease and its progression in children: the KDIGO definition (kidney abnormalities or low GFR for over three months), the GFR G1 to G5 and albuminuria A1 to A3 staging grid that drives risk and referral, why congenital CAKUT dominates paediatric causes, the hyperfiltration vicious cycle that makes CKD self-amplifying, the nephroprotective bundle of blood-pressure control below the 50th percentile with ACE inhibitors or ARBs, and the longitudinal management of growth failure, anaemia, acidosis and mineral-bone disease that lets a child reach transplantation in the best possible condition.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A boy born with posterior urethral valves is now seven. His creatinine has crept up over years, his height has fallen from the 50th to the 9th centile, and his blood pressure is above the 95th centile. He has chronic kidney disease: the slow, lasting loss of the kidney's ability to filter blood and maintain balance, present for more than three months and carrying consequences for health. The time frame matters — it separates CKD from the recoverable acute kidney injury that happens over days, and the health consequence matters, because a slightly low filtering rate without any damage marker or any impact is not yet disease. [1]
KDIGO, the international body that sets kidney-disease standards, defines chronic kidney disease as either a glomerular filtration rate below 60 mL per minute per 1.73 square metres for over three months, or markers of kidney damage present for over three months. The damage markers are albuminuria, an abnormal urine sediment, persistent electrolyte and acid-base disturbance from tubular disease, structural abnormalities found on imaging, a history of kidney transplantation, or a cystic or inherited kidney disease. In children the emphasis falls differently from adults: congenital and structural problems dominate, and the kidney is still expected to support a growing body, so even moderate loss of function can derail growth and development. [1]
Classification
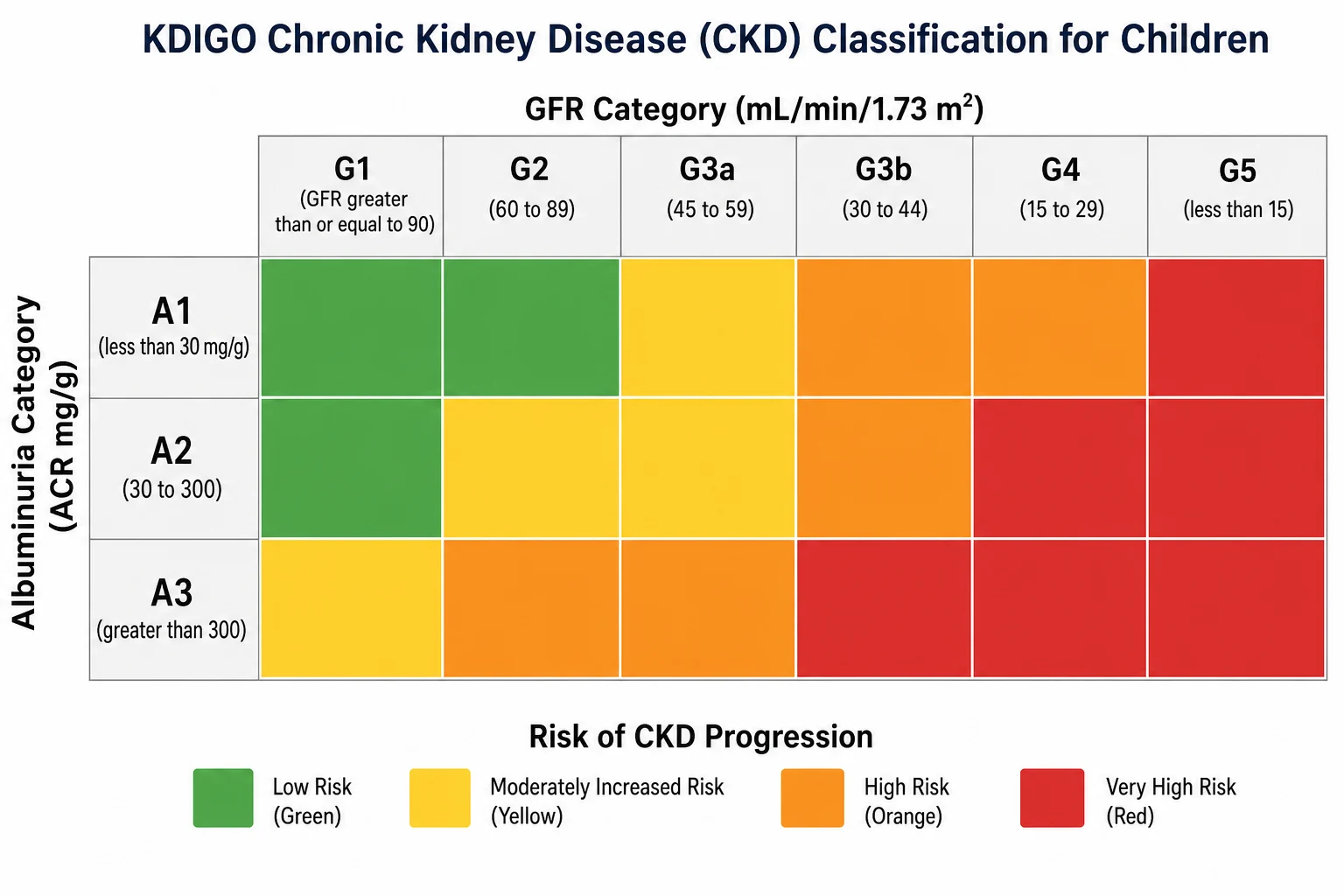
The staging system is worth understanding rather than memorising, because it is built from one simple idea: the risk to the kidney comes from two independent things — how much filtering capacity is left, and how leaky the filter has become. Filtering capacity is captured by the estimated glomerular filtration rate and divided into five categories. Albuminuria, the leakiness, is divided into three. Cross the two on a grid and you get a heat map of risk, which is exactly what the figure shows. A child can be in a reassuring green cell with good function and no albuminuria, or in a dangerous red cell with failing function and heavy proteinuria, and the grid tells you which. [1]
The GFR categories run from G1, where the rate is 90 mL per minute per 1.73 square metres or more, down through G2 at 60 to 89, G3a at 45 to 59, G3b at 30 to 44, G4 at 15 to 29, and G5, kidney failure, at a rate under 15. The albuminuria categories use the albumin-to-creatinine ratio: A1 is under 30 mg per g, A2 is 30 to 300, and A3 is over 300. A single number on its own is less informative than people assume — a GFR of 55 with no albuminuria (G3a, A1) is a far kinder place to be than a GFR of 55 with heavy albuminuria (G3a, A3), because the protein leak itself drives further scarring. That is the clinical value of the grid: it forces you to ask about both axes. [5]
[1]A practical point distinguishes paediatric staging. GFR categories G1 and G2 require markers of kidney damage to count as CKD, because a child with a GFR of 100 and entirely normal kidneys is healthy, not stage-one diseased. This is why a child with reflux nephropathy and a normal GFR still has CKD (structural damage is the marker), while an athlete with a high GFR and no damage does not. The albuminuria cut-off of 30 mg per g is also the level above which cardiovascular and progression risk begins to climb, which is why the grid colours shift at exactly that boundary. [5]
Epidemiology & Risk Factors
The causes of chronic kidney disease in children look nothing like the causes in adults. In adults the dominant drivers are diabetes and hypertension, diseases of later life. In children the dominant driver is being born with a kidney or urinary tract that never formed correctly. These congenital anomalies of the kidney and urinary tract, known as CAKUT, account for roughly half of all paediatric CKD and include renal hypodysplasia, posterior urethral valves and other obstructive uropathies, and reflux nephropathy. The next largest group is inherited glomerular and cystic disease, including focal segmental glomerulosclerosis, Alport syndrome and autosomal recessive polycystic kidney disease. [6]
Several factors mark a child out as likely to progress faster down the GFR categories. Heavy proteinuria at baseline is the single strongest predictor of decline, because albumin leaking through the glomerulus is directly toxic to the tubular cells it reaches. Hypertension comes next: every millimetre of mercury above the normal range accelerates sclerosis inside the glomerulus. Low birth weight and prematurity reduce the nephron endowment a child is born with, leaving fewer units to lose before function fails. Recurrent infections, obstructive episodes and acute kidney injuries on top of the chronic disease each chip away at reserve. The boy with posterior urethral valves carries several of these — a congenital obstruction, reflux, and recurrent infections — which is why his trajectory is downhill unless each factor is actively opposed. [7]
Pathophysiology
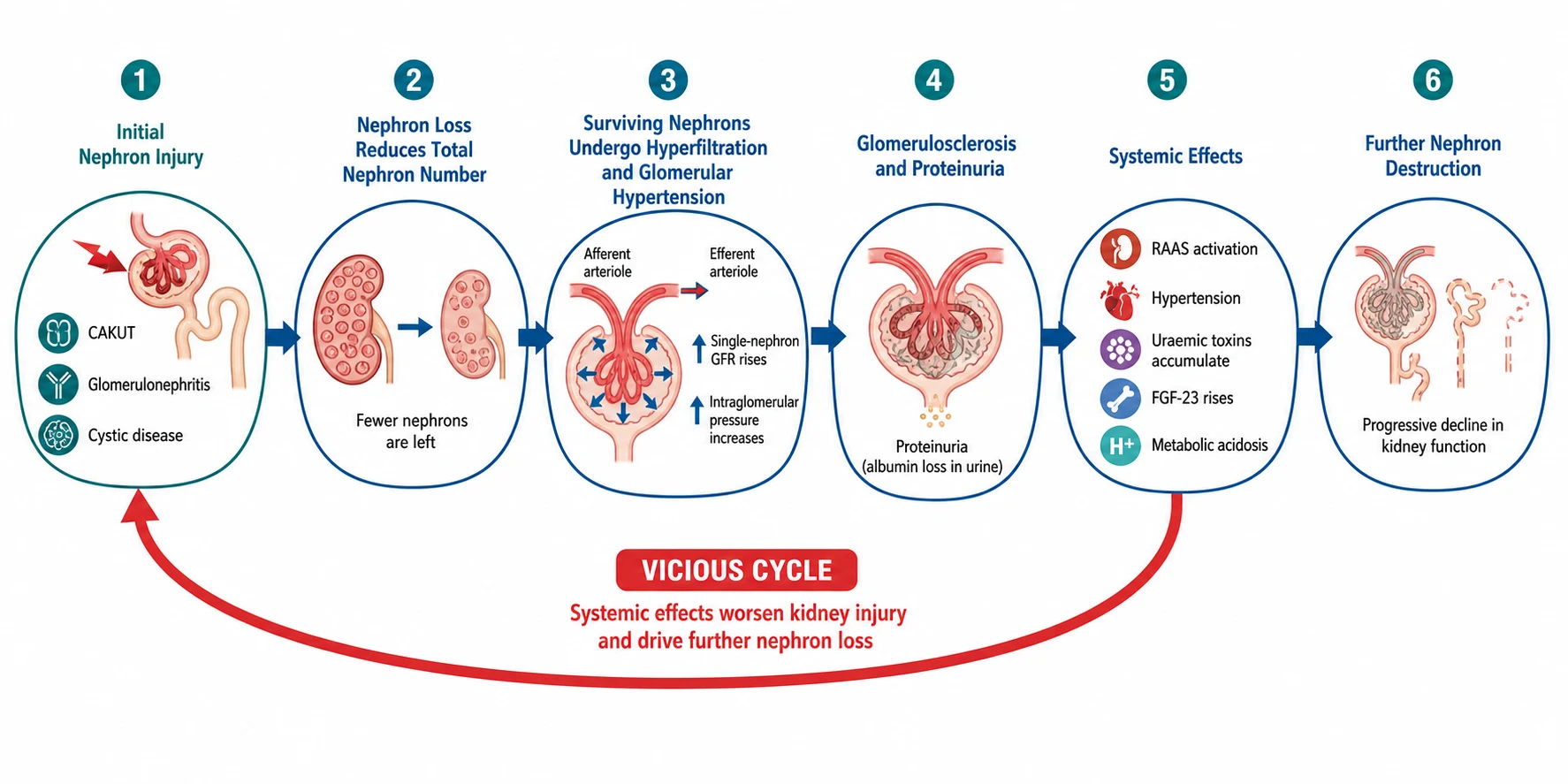
The most important concept in CKD is that the disease feeds itself. When nephrons are lost — to dysplasia, obstruction, inflammation or scarring — the remaining nephrons do not simply do less work. They increase their individual filtration to keep total kidney function up, a phenomenon called hyperfiltration. Each surviving nephron filters more blood at higher pressure, and in the short term this preserves the whole-organ GFR so the child looks better than the underlying nephron loss would predict. The cost is paid later: the high-pressure, high-flow overwork injures the glomerulus, causing focal segmental glomerulosclerosis, and that scarring destroys the very nephrons that were compensating. This is the vicious cycle, and it is why CKD accelerates once it has begun. [7]
The mechanism driving hyperfiltration is the renin-angiotensin-aldosterone system. Angiotensin two constricts the efferent arteriole, the vessel carrying blood out of the glomerulus, more than the afferent arteriole carrying blood in. This raises the pressure inside the glomerular capillary (the intraglomerular pressure), which pushes more filtrate through the surviving nephron. It also damages the glomerular barrier, letting albumin leak through. Proteinuria is therefore both a marker of damage and a mechanism of further damage: albumin and filtered proteins are taken up by proximal tubular cells, triggering inflammation, fibrosis and interstitial scarring. This single insight — that angiotensin two, glomerular hypertension and proteinuria form a self-reinforcing loop — is the rationale for the entire nephroprotective strategy, because blocking angiotensin two breaks the loop. [3]
RAPE
As nephrons fail, the kidney's other jobs unravel in a predictable order. Phosphate retention and falling calcitriol raise fibroblast growth factor 23 early, long before phosphate climbs on a blood test. Reduced erythropoietin production causes a normocytic anaemia. Acid generation exceeds excretion, producing a high-anion-gap metabolic acidosis that dissolves bone and worsens growth failure. The hormonal axis for growth is disrupted, and chronic inflammation and poor nutrition compound it. Each of these is a treatable complication, and treating each one — not just the GFR number — is what lets the child grow, learn and reach transplantation in good condition. [8]
Clinical Presentation
Chronic kidney disease is famously silent in its early stages, which is why so much of paediatric presentation is found through screening rather than symptoms. A child with a known antenatal hydronephrosis, a posterior urethral valve repair, or reflux is followed with blood pressure and creatinine, and the CKD is detected when the numbers drift. The first symptom a family notices is often not renal at all: the child is not growing. Growth failure is one of the commonest presentations of significant CKD in childhood, driven by poor appetite, chronic acidosis, anaemia, mineral-bone disease and resistance to growth hormone, and a child crossing centile lines downward warrants kidney function as part of the work-up. [6]
When symptoms do appear, they tend to reflect the complications rather than the kidney itself. Fatigue, pallor and exercise intolerance point to anaemia. Failure to thrive, recurrent fractures or bone pain point to mineral-bone disease. Headaches, visual disturbance or seizures can reflect hypertension, which is common in obstructive and reflux nephropathy. Polyuria and polydipsia occur when concentrating ability is lost, particularly in dysplastic and obstructive uropathies where the tubules fail early while the GFR is still preserved — a child may pass large volumes of dilute urine and be mislabelled as simply a heavy drinker. Nocturia and secondary enuresis are under-recognised clues. [5]
Atypical and late presentations are the traps an examiner probes. An adolescent may present with apparently new hypertension and turn out to have reflux nephropathy or undiagnosed dysplasia with long-standing CKD. A younger child with rickets refractory to standard vitamin D may have CKD-mineral-bone disorder. A neonate with posterior urethral valves may present with respiratory distress from pulmonary hypoplasia before the renal failure is appreciated. Advanced disease declares itself with the features of uraemia: anorexia, nausea, vomiting, itching, bruising, fluid overload with oedema and pulmonary congestion, and the biochemical emergencies of hyperkalaemia and acidosis. [1]
Differential Diagnosis
The first diagnostic task is to separate chronic kidney disease from acute kidney injury, because the management and prognosis diverge immediately. Acute injury develops over hours to days, is often reversible, and usually shows normal-sized kidneys on ultrasound with no chronic features. Chronic disease evolves over months, is generally irreversible, and classically shows small, echogenic kidneys with loss of corticomedullary differentiation — though dysplastic, cystic or obstructed kidneys may be enlarged or asymmetric. The duration of abnormal function, the imaging appearance, and the presence of anaemia, acidosis and mineral-bone disease all point toward chronicity. [5]
[7]Within chronic disease the differential is the search for the underlying cause, because the cause shapes progression and management. CAKUT (hypodysplasia, obstructive uropathy, reflux nephropathy) is suggested by a history of antenatal hydronephrosis, valve repair, recurrent urinary tract infections, and imaging showing small scarred kidneys or dilated collecting systems. Glomerular disease (focal segmental glomerulosclerosis, Alport syndrome) presents with proteinuria, haematuria and often a family history, with biopsy providing the definitive answer. Cystic disease (autosomal recessive polycystic kidney disease) shows enlarged echogenic kidneys and a family history, often with hepatic fibrosis. Inherited tubular and metabolic disorders round out the list. Identifying the cause is not academic: a child with reflux nephropathy needs infection prevention and blood-pressure control, while a child with focal segmental glomerulosclerosis may need immunosuppression to control the proteinuria that is driving the decline. [6]
Clinical & Bedside Assessment
The bedside assessment of a child with CKD answers four questions at once: how much function remains, how fast it is declining, what complications are present, and how the child is growing and developing. The history establishes the cause — antenatal findings, neonatal course, surgical history, urinary tract infections, family history of renal disease, deafness (Alport) or cystic disease — and the trajectory, by asking about changes in energy, appetite, growth, urine volume and school performance. Growth is measured meticulously: height, weight and body-mass index plotted on the appropriate centile charts, with height velocity, because growth failure is both a complication and a barometer of overall disease control. [6]
Examination looks for the consequences of CKD across systems. Blood pressure is measured with the right cuff and plotted on age, sex and height centiles, and elevated readings must be confirmed; in CKD, ambulatory blood-pressure monitoring is the preferred tool because it captures nocturnal hypertension and the blunted overnight dip that clinic readings miss. Fluid status is assessed for dehydration (which worsens function) or overload (oedema, raised venous pressure, pulmonary crackles). Pallor suggests anaemia, and the pallor of CKD is typically out of proportion to the child's other symptoms. Bone deformities, widened wrists or frontal bossing indicate established renal osteodystrophy. Abdominal examination may reveal enlarged polycystic kidneys, a palpable bladder, or scars from urological surgery. [1]
Neurodevelopment and cognition deserve deliberate attention. Children with CKD, even of moderate severity, have higher rates of attention difficulties, executive-function problems and impaired educational attainment, and these worsen with declining function and during dialysis. Recognising them early allows educational support, and they form part of the indication for timely transplantation rather than prolonged dialysis in young children. A developmental and school history is therefore a required part of the assessment, not an optional extra. [9]
Investigations
The investigation strategy confirms CKD, estimates its severity with the staging grid, and surveys the complications that require treatment. The estimated GFR is the central measurement, and in children it is estimated rather than measured, using a formula based on serum creatinine and height. The updated bedside Schwartz equation is the high-yield formula to know: estimated GFR equals 0.413 multiplied by height in centimetres, divided by serum creatinine in micromoles per litre divided by 88.4 (to convert to mg per dL). The CKiD study also produced a more accurate four-variable equation using creatinine, cystatin C, urea and height, but the bedside Schwartz coefficient of 0.413 is the figure examiners expect, and creatinine must always be interpreted with the child's height, never in isolation. [4]
The albuminuria measurement completes the staging grid. A first-morning urine albumin-to-creatinine ratio is preferred over a random sample because it minimises the standing-effect of daytime activity, and a ratio of 30 mg per g or more sustained on repeat samples defines significant albuminuria. The urine sediment is examined for red cells, casts and dysmorphism that point to glomerular disease. A renal ultrasound establishes kidney size, echogenicity, corticomedullary differentiation, cysts, dilatation and post-void residual, and is essential for defining the structural cause. In selected cases a DMSA scan demonstrates scarring and differential function, a MAG3 or DTPA scan assesses drainage and obstruction, and a renal biopsy is performed when glomerular disease is suspected and histology will change management. [5]
The complication survey runs in parallel. A full blood count and iron studies reveal the anaemia of CKD and guide iron and erythropoiesis-stimulating-agent therapy. Bicarbonate quantifies the metabolic acidosis. Calcium, phosphate, parathyroid hormone and alkaline phosphatase map the mineral-bone disorder, with 25-hydroxyvitamin D measured to guide replacement. Fibroblast growth factor 23 rises early and predicts both progression and cardiovascular risk, though it is not yet a routine clinical test. Lipids, glucose and an echocardiogram assess cardiovascular burden, which becomes the leading cause of long-term mortality in those who survive to adulthood. [8]
Management — Resuscitation
The resuscitation phase applies to the child with CKD who has acutely decompensated, typically with hyperkalaemia, severe acidosis, fluid overload or symptomatic uraemia. Airway, breathing and circulation come first. Hyperkalaemia with electrocardiogram changes is a medical emergency treated immediately with intravenous calcium gluconate for cardiac membrane stabilisation, followed by insulin with dextrose and nebulised salbutamol to shift potassium into cells, and sodium bicarbonate for the accompanying acidosis. Definitive removal of potassium and fluid is achieved with dialysis when medical therapy fails or the child is oliguric. [1]
Fluid management in the decompensated child demands precision. Many children with CKD, particularly those with dysplastic or obstructive uropathies, are polyuric and salt-wasting rather than oliguric, and they can present dehydrated with a rising creatinine that mimics acute-on-chronic failure; cautious rehydration with isotonic saline improves these children. Conversely, a child who is oliguric or anuric must be fluid-restricted to insensible losses plus urine output, because excess accumulates rapidly and causes pulmonary and cerebral oedema. Daily weights and strict input-output charting are the most reliable guides. Severe metabolic acidosis with a pH under 7.1 or bicarbonate under 10 is treated with intravenous bicarbonate while preparing for definitive therapy. [1]
Symptomatic uraemia — pericarditis, encephalopathy, or uncontrollable fluid and biochemical disturbance — is an indication for urgent dialysis. In young children peritoneal dialysis is usually the preferred modality because it is gentler haemodynamically, preserves vascular access for the future, and can be managed at home, though haemodialysis or continuous renal replacement therapy are used in the acutely unstable child. The decision to start kidney replacement therapy, however, should ideally be planned rather than emergency, which is why the definitive management that follows is the part of CKD care that truly changes outcomes. [1]
Management — Definitive & Stepwise
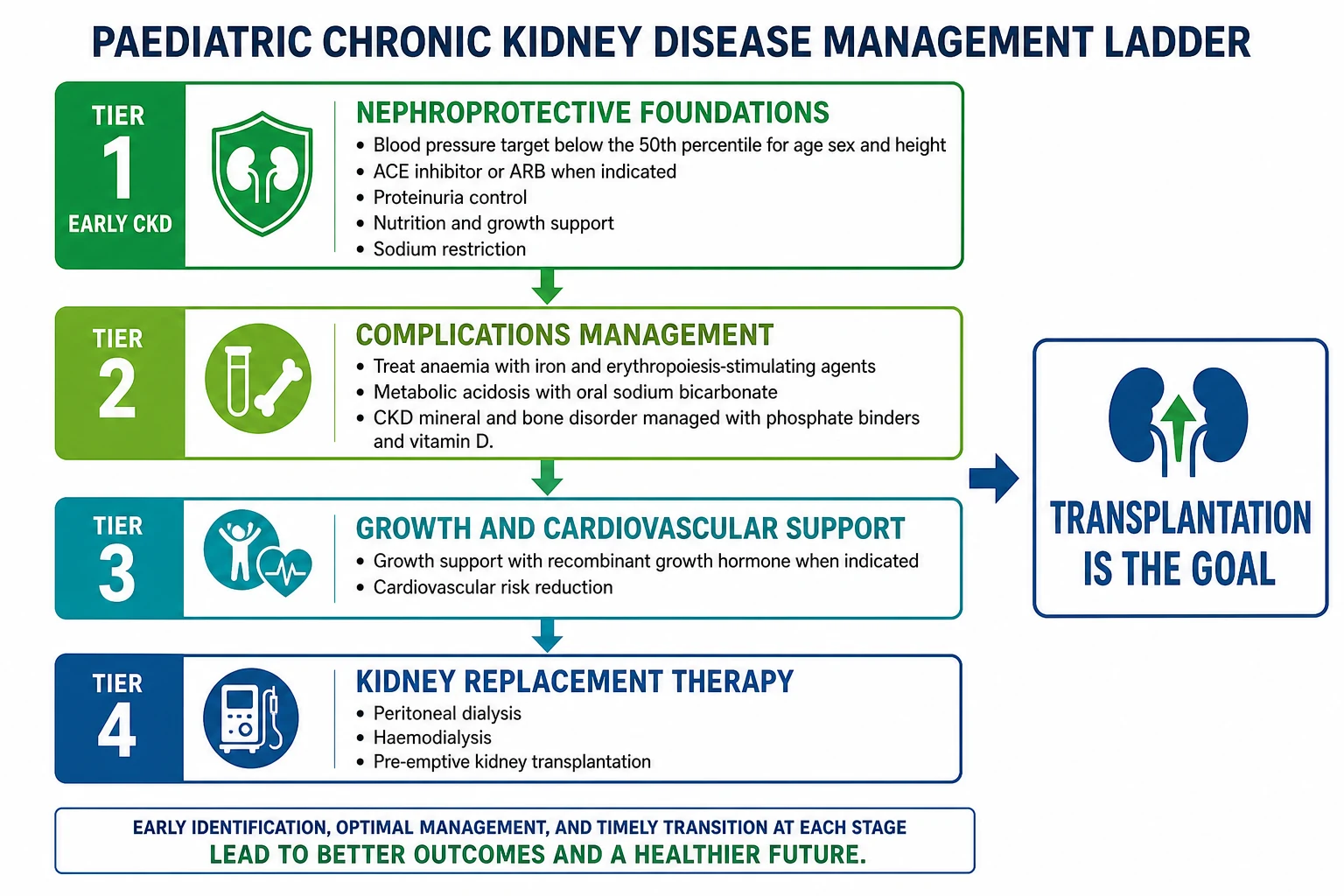
Definitive management of CKD is built on one principle that overrides all others: slow the progression, because every millilitre of GFR preserved is a millilitre the child does not have to make up with dialysis. The nephroprotective bundle has three pillars, and the evidence for each is strong. The first is rigorous blood-pressure control. The ESCAPE trial established that targeting a 24-hour mean arterial pressure below the 50th percentile for age, sex and height slows progression in children with CKD more effectively than a higher target, and this below-50th-percentile goal remains the cornerstone of paediatric nephroprotection, achieved with ambulatory monitoring to confirm it has been reached. [3]
Blood pressure below the 50th percentile
Block the renin-angiotensin system
Eliminate reversible insults
Control the complications
Support growth and the heart
Prepare for kidney replacement therapy
The second pillar is blockade of the renin-angiotensin system, because this directly interrupts the hyperfiltration loop. An angiotensin-converting enzyme inhibitor (for example enalapril starting at 0.1 mg per kg per day, titrated, in two divided doses) or an angiotensin receptor blocker (for example losartan 0.7 mg per kg per day up to 50 mg, titrated) is first-line for hypertension and for proteinuric CKD even when blood pressure is controlled, because these agents lower the efferent arteriolar tone, reduce intraglomerular pressure, and cut albuminuria. Starting or uptitrating an ACE inhibitor causes an expected small rise in creatinine and potassium, which is acceptable and should not trigger automatic cessation, but both must be monitored. These drugs are the single most evidence-supported intervention to slow paediatric CKD progression. [7]
The third pillar is the elimination of reversible insults: treating urinary tract infections promptly, relieving obstruction surgically where it persists, withdrawing non-steroidal anti-inflammatory drugs and other nephrotoxins, and avoiding the intravascular depletion that under-fills the kidney and worsens function. These seem obvious, but they are where preventable progression hides. Beyond nephroprotection, the management ladder controls the treatable complications so the child reaches end-stage kidney disease in the best possible condition rather than wasted by anaemia, bone disease and stunting. [1]
Anaemia is treated with iron and erythropoiesis-stimulating agents. Oral elemental iron at 2 to 3 mg per kg per day corrects absolute deficiency, and intravenous iron is used when oral iron is not tolerated or is insufficient; an erythropoiesis-stimulating agent such as darbepoetin is added when haemoglobin falls despite adequate iron, typically below 100 g per litre, to maintain it in the 100 to 120 g per litre range without overshooting, since higher targets increase thrombotic risk. Metabolic acidosis is corrected with oral sodium bicarbonate, 1 to 3 mmol per kg per day in divided doses, to maintain serum bicarbonate at 22 mmol per litre or above, because chronic acidosis worsens growth failure, dissolves bone and may itself accelerate progression. [8]
Mineral-bone disease is managed across three fronts: phosphate control, calcium balance and vitamin D. Dietary phosphate restriction, phosphate binders (calcium-based such as calcium carbonate in earlier stages, or non-calcium binders such as sevelamer when the calcium-phosphate product is high), and adequate but not excessive calcium intake are combined. Native vitamin D (cholecalciferol) is given to correct 25-hydroxyvitamin D deficiency, and an active vitamin D analogue such as calcitriol or paricalcitol is added to suppress secondary hyperparathyroidism when parathyroid hormone rises above the target range, titrated to keep parathyroid hormone within roughly two to nine times the upper limit of normal for the stage. Maintaining normal vitamin D levels is itself associated with less proteinuria and slower progression. [11]
ACE inhibitor (e.g. enalapril)
Dose
Enalapril 0.1 mg per kg per day starting, titrated to 0.5 to 0.6 mg per kg per day, in two divided doses
Growth failure is one of the most visible and distressing consequences of CKD for families, and it demands a stepped approach. The first steps are always to correct the reversible drivers — optimise nutrition with the help of a renal dietitian, treat acidosis, anaemia and mineral-bone disease, and ensure adequate caloric and protein intake, sometimes with supplementary tube feeding in infants. Only after these are addressed is recombinant human growth hormone considered. The recommended dose is 28 IU per square metre per week, equivalent to about 0.05 mg per kg per day, given as a daily subcutaneous injection, and it improves growth velocity and final height in children with CKD whose growth remains impaired despite optimal conservative management. The decision is made jointly with the family and a paediatric endocrinology-nephrology team. [10]
Specific Subtypes & Scenarios
CAKUT is the subtype the general paediatrician meets most often. It is a spectrum of abnormal kidney and urinary tract development — renal agenesis, hypodysplasia, multicystic dysplastic kidneys, ureteropelvic junction obstruction, posterior urethral valves, vesicoureteric reflux and prune-belly syndrome — and its common thread is that structural abnormality leads to impaired development, infection, obstruction or reflux that cumulatively destroys nephrons. A child with posterior urethral valves repaired in the neonatal period may still lose function over years because the dysplastic renal tissue never recovered and the bladder dysfunction causes high storage pressures that back-pressure the upper tracts. Management therefore includes not just nephroprotection but ongoing urological surveillance of bladder function, sometimes with clean intermittent catheterisation or anticholinergics. [6]
Glomerular diseases that cause CKD — focal segmental glomerulosclerosis, Alport syndrome, and the aftermath of haemolytic uraemic syndrome — present with proteinuria and haematuria and tend to carry heavier albuminuria, placing them in the higher-risk cells of the staging grid. Because the protein leak itself drives progression, aggressive reduction of proteinuria with renin-angiotensin blockade and, where appropriate, immunosuppression is central. Alport syndrome, with its sensorineural hearing loss and ocular signs, illustrates how a renal diagnosis demands a system-wide assessment, and how family screening identifies affected relatives. [6]
Cystic kidney disease, particularly autosomal recessive polycystic kidney disease, presents differently: enlarged echogenic kidneys detected antenatally or in infancy, often with hypertension, polyuria and progressive loss of concentrating ability, frequently accompanied by congenital hepatic fibrosis and portal hypertension. These children may reach end-stage kidney disease in childhood and require coordinated hepatology and nephrology care. Across all subtypes, the trajectory and the complications differ, but the nephroprotective bundle and the commitment to planned transplantation apply to every child. [1]
Complications & Pitfalls
The complications of CKD are exactly the treatable disturbances that the management ladder is designed to control, and they cluster predictably as function declines. Growth failure, anaemia, metabolic acidosis and mineral-bone disorder dominate the middle stages. Cardiovascular disease — left-ventricular hypertrophy, accelerated atherosclerosis and later sudden cardiac death — becomes the leading cause of long-term mortality in survivors, which is why blood-pressure control, lipid attention and echocardiographic surveillance matter even in children. Neurocognitive impairment affects schooling and independence, and infection risk rises with malnutrition, immunosuppression and dialysis access. [9]
The classic pitfalls are the ones that cost function or safety. Treating the blood pressure to a normal-for-the-population target rather than the below-50th-percentile CKD target leaves a child undertreated and progressing. Withdrawing an ACE inhibitor at the first small creatinine rise deprives the child of the drug that most slows decline. Missing the polyuric, salt-wasting child who needs fluid and sodium rather than restriction dehydrates the kidney and worsens function. Failing to plan access and transplant work-up before the child reaches G5 forces an emergency dialysis start, which carries higher morbidity. And under-recognising mineral-bone disease and growth failure leaves a child reaching end-stage kidney disease stunted, frail and less well prepared for transplantation. [7]
Prognosis & Disposition
The prognosis of paediatric CKD is fundamentally a story about progression and its prevention. Without nephroprotection, most children with significant CKD progress to kidney failure, and the rate is determined chiefly by the level of albuminuria and the adequacy of blood-pressure control. With the full nephroprotective bundle, progression slows substantially, and many children gain years or decades of additional native-kidney function. The ultimate destination for those who reach end-stage kidney disease is transplantation, which offers by far the best survival, growth, neurodevelopment and quality of life compared with dialysis, and pre-emptive transplantation before dialysis is begun gives the best outcomes of all. [6]
Severity
CKD G1 to G2 (with damage)
Normal or mildly reduced GFR with kidney damage markers. Focus on diagnosis, nephroprotection and surveillance. Excellent prognosis with control of blood pressure and proteinuria.
Severity
CKD G3 (3a to 3b)
Moderately reduced GFR. Complications of anaemia, acidosis and mineral-bone disease emerge and require active management. Growth and blood pressure need close attention.
Severity
CKD G4 to G5
Severely reduced function to kidney failure. Requires multidisciplinary preparation for kidney replacement therapy, transplant work-up, and management of cardiovascular and growth burden.
Disposition follows the stage. Early CKD is managed jointly by the general paediatrician and a nephrology service with surveillance that matches the risk, typically six- to twelve-monthly for stable early disease and more frequently as function declines. Children approaching end-stage kidney disease are managed in a specialist paediatric nephrology centre with access to dialysis, transplant assessment and a multidisciplinary team including dietitians, nurses, psychologists and social workers. Every adolescent with CKD requires a structured transition to adult nephrology services, because the move from paediatric to adult care is a recognised period of graft loss and disengagement when poorly managed. [1]
Special Populations
Infants and young children are the population in whom CKD has its greatest developmental impact, because the kidney must support growth and the developing brain through a vulnerable period. In infants, particularly those with dysplastic or obstructive uropathies, salt wasting, polyuria and poor intake make sodium supplementation and adequate nutrition — often via nasogastric or gastrostomy feeding — central to growth, sometimes more important than any drug. These young children are also the group in whom early transplantation, sometimes before two years of age, is pursued to protect neurodevelopment, since dialysis in infancy carries the poorest cognitive outcomes. [9]
Adolescents bring the twin challenges of disease acceleration and the transition to adult care. Non-adherence to medication and monitoring rises in adolescence and is a leading cause of graft loss after transplantation, which is why structured transition programmes, peer support and honest conversations about fertility, substance use and self-management are essential. Young people with CKD need counselling about the impact of kidney disease on puberty, fertility and pregnancy planning, and young women on teratogenic drugs such as ACE inhibitors and mycophenolate need specific contraceptive advice. [10]
Children from Indigenous and socioeconomically disadvantaged backgrounds, as documented in Australian and New Zealand registry data, carry a disproportionate burden of kidney disease, often present later with more advanced CKD, and face barriers to the consistent follow-up that nephroprotection requires. Recognising and addressing these inequities — through culturally safe care, outreach and coordination — is part of delivering the nephroprotective bundle equitably rather than only to those who can attend a tertiary clinic. [6]
Evidence, Guidelines & Regional Differences
The KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease is the current global standard for the definition, staging and management of CKD across children and adults, updating and consolidating the landmark 2012 guideline. It confirms the G1 to G5 and A1 to A3 grid, formalises risk-based assessment, and emphasises that rapid progression — a sustained decline in estimated GFR of 5 mL per minute per 1.73 square metres per year or more — warrants intensification of nephroprotection. It also reinforces the place of albuminuria as both a staging and a therapeutic target. [1]
The ESCAPE trial remains the defining evidence in paediatric nephroprotection. It randomised children with CKD to a strict blood-pressure target (24-hour mean arterial pressure below the 50th percentile) against a conventional target (50th to 95th percentile), and showed that strict control slowed the decline in GFR over five years. The finding that the benefit was most evident in proteinuric children cemented the below-50th-percentile target and renin-angiotensin blockade as the twin foundations of paediatric CKD management, and ambulatory blood-pressure monitoring as the tool to confirm the target has been met. [3]
ESCAPE Trial — strict blood-pressure control in paediatric CKD
Key finding
In children with CKD, targeting a 24-hour mean arterial pressure below the 50th percentile for age, sex and height slowed the decline in GFR over five years compared with a higher conventional target, with the benefit concentrated in proteinuric patients. All children received a fixed dose of the ACE inhibitor ramipril.
Practice change
Use ambulatory blood-pressure monitoring to target the below-50th-percentile goal in children with CKD, with ACE-inhibitor or ARB therapy, particularly when albuminuria is present.
In Australia and Aotearoa New Zealand, paediatric CKD is managed through specialist paediatric nephrology centres linked to the ANZDATA registry, which tracks dialysis and transplant outcomes. Care is consistent with KDIGO recommendations, with strong emphasis on early detection of CAKUT through antenatal and postnatal screening, equity-focused outreach for Indigenous communities, and a national transplant programme that prioritises pre-emptive living-donor transplantation. Blood-pressure targets follow the ESCAPE below-50th-percentile standard. [6]
Regional differences exist mainly in the timing of detection and access to transplantation. Systems with universal antenatal ultrasound and postnatal surveillance detect CAKUT early and begin nephroprotection before function is lost, whereas late presentation with advanced CKD remains common where screening is limited. Access to recombinant growth hormone, the full range of phosphate binders and timely transplantation varies with health-system resources, though the clinical principles of nephroprotection are universal. The IPNA (International Pediatric Nephrology Association) provides guidance adapted to settings with fewer resources, emphasising the high-yield, low-cost interventions of blood-pressure control, proteinuria reduction and complication treatment. [1]
Exam Pearls
Chronic kidney disease is defined by kidney damage or a glomerular filtration rate below 60 mL per minute per 1.73 square metres for over three months. The KDIGO grid crosses GFR category G1 (90 or more) through G5 (under 15) with albuminuria category A1 (under 30 mg per g), A2 (30 to 300) and A3 (over 300) to assign progression risk, and albuminuria is the single strongest predictor of decline. The leading cause in children is CAKUT, not diabetes or hypertension as in adults. The bedside Schwartz equation, estimated GFR equals 0.413 times height in centimetres divided by creatinine in mg per dL, is the formula to estimate paediatric GFR. [1]
The mechanism of progression is the hyperfiltration vicious cycle: nephron loss forces surviving nephrons to overwork, angiotensin two raises intraglomerular pressure, and the resulting sclerosis and proteinuria destroy the compensating nephrons. The two evidence-based nephroprotective interventions are blood-pressure control to a 24-hour mean below the 50th percentile (ESCAPE trial) and renin-angiotensin blockade with an ACE inhibitor or ARB, particularly for proteinuric disease. Recombinant growth hormone at 28 IU per square metre per week (about 0.05 mg per kg per day) subcutaneously is added for persistent growth failure once reversible factors are corrected. [3]
Rapid progression is defined as a sustained fall in estimated GFR of 5 mL per minute per 1.73 square metres per year or more, and it is a signal to intensify therapy. Transplantation, ideally pre-emptive and before dialysis, gives the best survival, growth and quality of life for children reaching kidney failure, and is the destination the entire management ladder is engineered to reach. Transition to adult care must be planned and structured, because it is a high-risk period for disengagement and graft loss. [1]
References
- [1]Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int, 2024.PMID 38490803
- [2]Levin A, Ahmed SB, Carrero JJ, Foster B, et al Executive summary of the KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease: known knowns and known unknowns. Kidney Int, 2024.PMID 38519239
- [3]ESCAPE Trial Group, Wühl E, Trivelli A, Picca S, et al Strict blood-pressure control and progression of renal failure in children. N Engl J Med, 2009.PMID 19846849
- [4]Schwartz GJ, Muñoz A, Schneider MF, Mak RH, et al New equations to estimate GFR in children with CKD. J Am Soc Nephrol, 2009.PMID 19158356
- [5]Hogg RJ, Furth S, Lemley KV, Portman R, et al National Kidney Foundation's Kidney Disease Outcomes Quality Initiative clinical practice guidelines for chronic kidney disease in children and adolescents: evaluation, classification, and stratification. Pediatrics, 2003.PMID 12777562
- [6]Wong CJ, Moxey-Mims M, Jerry-Fluker J, Warady BA, et al CKiD (CKD in children) prospective cohort study: a review of current findings. Am J Kidney Dis, 2012.PMID 23022429
- [7]Schaefer B, Wühl E Educational paper: Progression in chronic kidney disease and prevention strategies. Eur J Pediatr, 2012.PMID 22968936
- [8]Fadrowski JJ, Pierce CB, Cole SR, Moxey-Mims M, et al Hemoglobin decline in children with chronic kidney disease: baseline results from the chronic kidney disease in children prospective cohort study. Clin J Am Soc Nephrol, 2008.PMID 18235140
- [9]Gerson AC, Butler R, Moxey-Mims M, Wentz A, et al Neurocognitive outcomes in children with chronic kidney disease: current findings and contemporary endeavors. Ment Retard Dev Disabil Res Rev, 2006.PMID 17061289
- [10]Drube J, Wan M, Bonthuis M, Wühl E, et al Clinical practice recommendations for growth hormone treatment in children with chronic kidney disease. Nat Rev Nephrol, 2019.PMID 31197263
- [11]Shroff R, Aitkenhead H, Costa N, Trivelli A, et al Normal 25-Hydroxyvitamin D levels are associated with less proteinuria and attenuate renal failure progression in children with CKD. J Am Soc Nephrol, 2016.PMID 26069294
- [12]Shroff R, Wan M, Nagler EV, Bakkaloglu S, et al Clinical practice recommendations for treatment with active vitamin D analogues in children with chronic kidney disease Stages 2-5 and on dialysis. Nephrol Dial Transplant, 2017.PMID 28873971